Working to keep school children healthy:
the complementary roles of school staff and
school nurses
Jane Lightfoot and Wendy Bines
Abstract
BackgroundAgainst a background of future uncertainty for school nursing and little previous research, this study aimed to identify and describe the distinctive role of the school nurse in working to keep school children healthy. Particular attention was paid to the ‘interface’ between nursing and the health-related work of teachers. The research was carried out in four health authority areas in England.
Methods Seventy-eight semi-structured interviews were carried out with a range of respondents: school nurses, school Heads and teachers, health authority purchasers and NHS Trust managers. Seven focus group discussions were held with parents and eight with young people of secondary school age.
Results Four key elements of the school nurse role were identified: safeguarding the health and welfare of children; health promotion; a pupils’ confidante; and family support. In each of these aspects of work, nurses and teachers had shared or complementary roles. An over-arching role for the school nurse as ‘health adviser’ to pupils, parents and teachers was also identified. Despite these common ele-ments, emphasis in the practice of individual school nurses varied widely. Difficulties for school nurses in developing their role were identified. Parents and young people saw school as an appropriate setting for health-related work.
ConclusionThe research identified key components of the school nursing role and the complementary roles of nurses and school staff. To optimize school nurses’ contribution to child health, a more strategic approach is required, in partnership with education, along with research into the effectiveness of school nursing interventions.
Keywords:school-age children, role of school nurse
Introduction
BackgroundSchool is a setting for health-related work in which education and health professionals both play a part. School staff undertake a variety of health-related roles, for some of which they have formal responsibility, such as health education and wider health promotion. In addition, research shows that at least some school staff take on an extended role in child health, including the detection of health-related needs, such as hearing problems,
and – through pastoral care – responding to emotional concerns of children.1
Health professionals have a long tradition of working in schools. Growing concern over high rates of infant and child mortality and of infectious disease at the turn of the century prompted the creation of a universal School Medical Service, in 1907, to carry out periodical medical ‘inspection’ of school children.2 These threats to the survival of children have now receded, and been replaced by other concerns, in particular poor mental health,3unhealthy lifestyles4and the needs of increasing numbers of children who survive and are managing a range of chronic illness and disabilities.5Although periodic ‘inspection’ remains the only statutory function of the National Health Service (NHS) with regard to school-age children (NHS Act 1977), in line with changes in patterns of child health, routine medical examinations of all children have now largely been abandoned, with doctors focusing on developing a more targeted paediatric service for individual children. In turn, school nurses have ‘expanded their role in health appraisal and health education and emerged as the key profession for the whole school population’ (Ref. 6, p. 18).
Recent developments offer apparently contradictory pro-spects for the future of school nursing. The Green Paper on public health, Our healthier nation,7reinforced the position of school as a site for health work, identifying school as ‘the key setting’ for a multidisciplinary approach to improving the health of the nation’s children. In doing so, attention was drawn to the role of the school nurse ‘in ensuring that schools . . . keep a clear focus on health’ (Ref. 7, paragraph 3.77). How such a focus might best be secured is as yet unclear under the new arrangements for a primary care driven NHS.8Guidance from the Department of Health on good practice in community child health services9acknowledges that legislation does not require a
qFaculty of Public Health Medicine 2000
Printed in Great Britain
Social Policy Research Unit, University of York, Heslington, York YO10 5DD.
Jane Lightfoot, Research Fellow
Royal Marsden NHS Trust, Fulham Road, London SW3 6JJ.
Wendy Bines, Staff Nurse
health service in school and that children could be ‘inspected’ elsewhere; for example, in a primary care setting. Although a ‘continuing and evolving role’ for the school health service (SHS) is advocated (Ref. 9, paragraph 8.4), clearly its future is neither prescribed nor guaranteed. Meanwhile, a number of health authorities have reduced their investment in school nursing services.10Other commentators have drawn attention to the ‘invisibility’ of the SHS in both policy and professional terms11,12and argued that, as its activities are poorly recorded and little researched, there are inevitable difficulties in assessing its contribution to child health.
Aims of the study
Against this background of challenge to the SHS and of little previous research into the role of school nursing, this paper reports findings of an empirical research study to identify the role of the nurse in school. The focus of the study was the role of nursing in meeting health needs potentially common to all children. Meeting the additional, special, needs of pupils with an illness or disability fell outside its scope. Given the increasing focus of the work of school doctors on children with special health needs, the study did not explore the relationship between the school nurse and school doctor. Instead, the study sought to describe the distinctive contribution of the nurse through investigating the ‘interface’ between nursing and the health-related work of teachers. Much of the work of school nurses is governed by the contractual obligations of NHS Trusts to provide programmes of school child health surveillance and immunizations. We set out to describe this work commonly expected of nurses and also to attempt to uncover any less well-recognized aspects of the school nursing role. We did not, however, seek to present a picture of the ‘typical’ day or week in the life of the school nurse. Rather our objective was to shed light on the field of work covered by the school nurse in meeting ‘ordinary’ health needs.
Methods
SamplingThis study did not set out to generalize the findings statistically to the population of nurses: systematic, non-probabilistic sampling13 was used in selecting health authority research ‘sites’ and in recruiting schools and respondents – particularly nurses – to capture variation in factors likely to influence the nursing role. The research was carried out in one pilot and four main stage ‘sites’, chosen to reflect differences in the context within which nurses work, such as: the socio-economic circumstances of the local population; urban–rural variation; geographical spread (within England); organization and management of local child health services (we included a combined hospital and community Trust, a hospital Trust, a Trust providing all non-acute services and a Trust providing
only community services); and variation in the extent to which nursing services for children had been subject to recent review and/or service development.
Variation among schools was secured in relation to: type and age range of pupils (primary, secondary and special schools were represented); numbers on roll; socio-economic character-istics of the local population; geographical location (urban, suburban or rural); proximity to local amenities, such as health clinics; and the amount of time spent in school by the school nurse. Variation among the sample of school nurses was sought in relation to nursing qualifications, length of service as a school nurse and working hours.
Data collection
Qualitative methods were used, given the exploratory nature of the research. Data were collected during 1995–1996 by semi-structured interviews with a range of health and education staff with a role in meeting the health needs of school-age children; and through focus groups with parents and with pupils, to obtain the perspective of service users.
Semi-structured interviews
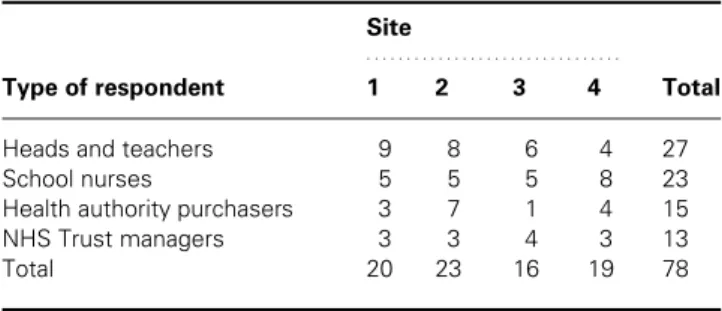
This paper draws on 78 interviews, which were used to collect data from a range of respondents, to capture a variety of perspectives on school nursing and to enhance the validity of the findings through identifying patterns of convergence.13A breakdown of the types and numbers of these respondents across the four research sites is given in Table 1. Heads and teachers represented 16 schools (from 20 approached) across the four sites: six first and primary schools, eight middle and secondary schools; and two special schools. Schools were drawn from the caseloads of the school nurses in the study, from whom we obtained the information relevant to our sampling criteria.
Topics covered in the interviews varied according to the type of respondent. Purchasers (whose remit covered children) and NHS Trust managers (managers of children’s services, of community nursing, and of school nursing) were asked about strategy and context: any local health needs assessment for school-age children; local strategy and priority-setting arrange-ments for child health; arrangearrange-ments for school health contract monitoring and any outcomes measurement; plans for devel-oping services for school-age children; and views of the future role of nursing in respect of school-age children. In addition, purchasers were asked about the commissioning process for children’s services, and Trust managers were asked for their views on the role of the SHS and, in particular, of school nursing.
School nurses were asked about their professional back-ground, education and training as a school nurse, and about their caseload (overall size, number of schools and ages of pupils covered). The interviews focused on four health needs as a device for gathering data on the nursing role in depth:
assessment of general health, both at the level of the individual child and the school population; health education (using sexual health education as an exemplar); management of common health problems (using asthma as an exemplar); and the emotional well-being of pupils. In each area, nurses were asked to describe their role, including role boundaries with other staff, particularly those in school. Nurses were also asked for their views on the extent of their professional autonomy, influences on their role, and prospects for the future of school nursing.
In most of the schools, we interviewed the Head (for a strategic perspective) and a teacher with responsibility for pastoral care and/or health education (for a practitioner perspective). In some schools, one person was able to talk to us about both policy and practice. School staff were asked for their views on factors influencing the health of children, and about the part school staff played in meeting health-related needs. They were also asked about: how they saw the role of the SHS, in particular that of the school nurse; any ways in which school staff and school nurses worked together; any liaison between schools and the NHS about the service to be provided by the school nurse; and any other work they would like to see school nurses do.
Focus groups
Seven focus group discussions were held with parents and eight with young people of middle or secondary school age. Parents were recruited to the focus groups through school staff. Three groups were held for parents of children in first and primary schools, two for middle and secondary schools, and two for special schools. All but one of the participants were mothers and attendance was low (as predicted by school staff), ranging between two and five parents.
Young people from six middle and secondary schools were recruited to focus group discussions, with the help of teachers, who asked for volunteers. In line with good ethical practice when carrying out research with children and young people, we obtained consent both from parents and from the young participants.14 The distribution of young people’s focus groups by site and school year groups is shown in Table 2. Each group comprised between four and six young people from
the same class and was held during the school day. We were guided by each school on the preferred sex composition of the groups: three groups were of mixed sex, whereas the other five comprised either girls or boys.
Topics for discussion were similar for parents and young people: what it means to be ‘healthy’; where responsibility lies for keeping children healthy; where parents or young people obtain support for young people’s health-related needs, including their views on what nursing has to offer; and views on how professional support for young people’s health might be improved.
Analysis
Interviews and group discussions were tape-recorded, with the respondents’ consent. Analysis was carried out using an established staged process for analysing qualitative data.15 The researchers used the tapes to agree an initial thematic framework for analysis, drawn both from a priori issues in the topic guides and from emergent issues raised by respondents. This framework was then used to chart the data systematically, followed by a process of identifying patterns and associations so as to arrive at a description of the contribution of the school nurse to health-related work in school. A number of issues concerned with maximizing the potential of this work were also identified.
Results
Results are presented in three sections: the current role of the school nurse; obstacles to developing the role of school nursing; and the views of teachers, pupils and parents on the appropriateness of school as a setting for nursing work.
The role of the school nurse
Taking together the perceptions of nurses, school staff, parents and young people, four key elements of the current school nurse role were identified: safeguarding the health and welfare of children; health promotion; a confidante; and family support. In addition, nurses drew attention to an over-arching role as ‘health adviser’ to school staff, parents and pupils.
Table 1 Types and numbers of respondents interviewed across the four research sites
Site
. . . .
Type of respondent 1 2 3 4 Total
Heads and teachers 9 8 6 4 27
School nurses 5 5 5 8 23
Health authority purchasers 3 7 1 4 15
NHS Trust managers 3 3 4 3 13
Total 20 23 16 19 78
Table 2 Young people’s discussion groups by research site and school year group
Site Year 8 Year 9 Year 10 Year 11 Total
1 1 – 2 – 3
2 – – – 2 2
3 1 – 1 – 2
4 – 1 – – 1
Total 2 1 3 2 8
Year 8, age 12–13; Year 9, age 13–14; Year 10, age 14–15; Year 11, age 15–16.
Safeguarding the health and welfare of children
Nurses and teachers had a shared role in safeguarding children’s health through identifying and referring on health problems. School nurses were responsible under their NHS Trust’s contract with the local health authority for carrying out a variety of ‘traditional’ school health tasks, including health screening, surveillance checks and immunization of the school population. Although the timing and content of these programmes varied between the Trusts, nurses reported spending the majority of their time on this work. Through these activities school nurses had a key role in referring pupils for a medical by the school doctor. In some sites, school nurses were also able to refer directly to other health professionals, such as speech therapists and audiologists. School nurses also played a part in child protection, through referring to social services departments, preparing health reports for case conferences and carrying out additional health surveillance work.
Teachers saw their part in safeguarding health as part of an informal caring role, their regular contact with the same groups of pupils – particularly in primary schools – placing them in a good position to spot health problems. However, teachers readily acknowledged that their scope for action was limited, both by their lack of expertise in health matters and by their obligations as teachers to the whole class. Routine visits to school from the nurse for health surveillance activities were seen by both nurses and teachers as efficient opportunities for school staff to pass on any health concerns about individual children, for instance, hearing problems.
Health promotion
Nurses and teachers had a shared role in health promotion. Although the health education curriculum was the responsi-bility of schools, a health policy emphasis on health promo-tion16meant that most – although not all – of the school nurses drew attention to health education as an increasingly important part of their work. Nurses saw access to a ‘captive’ audience in school as a good opportunity for promoting healthy lifestyles. Although not necessarily formally trained to teach, most nurses were involved in classroom health education sessions, either by providing resources or by participating directly in teaching.
Teachers and pupils identified five ways in which nurses made a distinctive and positive contribution to sexual health education: expert and up-to-date knowledge; an informal teaching style, conducive to discussing sensitive topics; comfortable when talking about the body; a non-judgemental approach; and being ‘a bit of an outsider’ to whom young people could put questions on sensitive or controversial matters without fear of repercussions in school: ‘They (nurses) bring a dimension which is so different from teachers ... they’re unmoralizing, unshockable and not perceived by children as having moral authority over them’ (deputy head, high school). Depending on the ethos and level of existing health-related knowledge among a school’s staff, school nurses reported that
they might be approached by teachers to take part in school-wide health promotion efforts, such as ‘health weeks’, and for general advice; for example, on healthy eating where a school wished to provide breakfast for pupils.
A confidante for children and young people
Parents, teachers and nurses emerged as having a shared role in listening to young people’s worries and concerns. However, school nurses could be not only an additional adult to approach, but also a trusted alternative when neither parent nor teacher was appropriate: ‘The school nurse offers a link for a child who’s got worries. Perhaps they can’t go to their parent. They know there’s someone approachable that they can go to who isn’t a teacher – some children don’t like to go to teachers’ (parent of child in high school).
Different rules for teachers and for nurses about confidenti-ality – with teachers less able to guarantee it – emerged as crucial in highlighting the special relationship possible between nurses and pupils: ‘In teaching there’s a line you can’t go beyond . . . so it’s difficult for teachers to help without telling anyone’ (teacher, high school). ‘You expect them [nurses] to keep your privacy . . . it’s what they’re meant to do’ (female pupil, age 13).
In response to these needs, and to provide health-related advice, many of the nurses mentioned that they either had set up or were developing confidential ‘drop-in’ sessions for pupils, typically on a weekly basis at lunch time, in secondary or high schools. Some nurses expressed concerns about their limited skills in counselling and supporting pupils with mental health problems, particularly where there were long waiting lists for local child and adolescent psychiatry services. A couple of nurses spoke about collating self-reported health needs of pupils and presenting these (anonymized) findings to teachers so as to develop school-based action. For example, when one nurse discovered that four pupils in one secondary school had recently attempted suicide, she worked with a teacher to develop and run a programme of personal and social education (PSE) sessions aimed at improving pupils’ self-esteem.
Family support
Both nurses and teachers, despite their prime focus on the child at school, talked about having a role in family support. However, not all nurses were prepared to offer such support, owing to a lack of training in family-focused work compared with health visitors. School nurses who did offer support talked about giving both practical help – for example, liaison with social services departments – and emotional support to parents coping with children with behaviour problems and other difficulties in family life.
Teachers reported two key problems with their own efforts to support families. First, teachers believed that some parents misconstrued as criticism their offers of support. Second, teachers reported a tension between wanting to remain on good terms with parents and wishing to put the child’s needs first.
Teachers saw nurses as less likely to be perceived by parents as threatening or judgemental and therefore someone who could act as a mediator between school and family.
Obstacles to developing the role of school nursing
Although the research was able to identify a distinctive contribution of school nursing, a number of obstacles limited its potential. Three areas of particular concern emerged: health needs assessment; role ambiguity; and ‘gatekeeping’ schools.
Health needs assessment
Purchasers reported a gap in strategic focus by health authorities on services for children. This gap was attributed to: difficulties posed by a fragmented development of services for children; little prescriptive national guidance; and relatively low national policy priority. As a result, purchasers reported that needs assessment for school-age children was in its infancy compared with other client groups, hence the historical focus on surveillance in contracts which left nurses little time to respond to other needs. Only one health authority had a post-holder with dedicated responsibility for developing a child health strategy, although purchasers and provider managers in all four sites were aware of growing pressure for a more strategic approach. Pressures stemmed from the requirements to contribute to inter-agency Children’s Services Plans and, organizationally, to develop a primary care-led approach.
Although school nurses themselves were arguably well placed to assess needs at school population level, nurses in only one of the four sites routinely carried out such ‘school health profiling’. Evidence from these nurses and their managers suggested that this practice helped target nursing work, both between and within schools.
Role ambiguity
Despite identifying common elements of the school nursing role, the research found wide variation in the practice of individual nurses. A corollary of highly individual patterns of work was that an overall sense of the role of ‘the school nurse’ was unclear. Potential users of school nursing services – pupils, teachers and parents – spoke about their difficulties in understanding what the nurse could offer. Purchasers and managers acknowledged that they knew little of the scope of school nursing practice, not least because information systems captured their activities inadequately. Even nurses themselves did not share a consensus about how their role should best develop; for example, in respect of teaching and family support. Nurses did not consider that existing formal school nurse education programmes captured the essence of their role, as the content of courses was not keeping pace with the current needs of children and young people; for example, in mental health. In practice, it appeared that nurses attempted to secure additional training – for instance, in teaching or counselling – in response to identified needs and their own areas of interest.
The small size of the school nursing workforce meant that nurses carried large caseloads of pupils and were required to spread their time across a number of schools. For pupils, this posed problems of low awareness of the school nurse and a possible reluctance to approach the nurse with their worries in a ‘drop-in’ session, as familiarity with the person would be needed, along with the opportunity to develop a relationship of trust: ‘You wouldn’t feel comfortable talking to a stranger’ (male student, age 15). ‘If you don’t know the school nurse it would be hard to tell her secrets’ (female student, age 16).
‘Gatekeeping’ schools
Schools are formally required to facilitate only routine health screening, surveillance and immunization programmes. In nurses’ accounts of negotiating access for additional work in schools, it was clear that the ethos of the school and attitudes of key staff were a strong influence on the pattern of nursing practice, both between and within schools. Lack of co-operation by a minority of what nurses called ‘difficult’ schools was reported as central to two key difficulties: targeting services on schools whose pupils have greatest needs, and ensuring equal access to nursing services by children and young people. For example, nurses reported that some schools would not permit a nurse-led confidential drop-in service, or that they might be permitted to offer sexual health education in some primary schools to girls, but not to boys.
For their part, some school staff reported uncertainty as to the scope of the school nurse’s role. Teachers with experience of more than one school nurse spoke about different nurses having different emphases in their work. In general, teachers saw as pragmatic a need to negotiate input at school with their school nurse, although one Head voiced concerns about the apparently individualistic character of the service and argued vigorously for a more strategic approach: ‘We haven’t got a clue what’s on offer ... We don’t know what her [school nurse’s] position is at all, if she can deliver what she’s interested in, or whether she even should be. Health [managers] should say what’s on offer and see if that’s what schools want or whether other things are more important. We’re the customer in effect, but no one is saying ‘‘Is this what you want?’’ (Head, middle school).
School as a setting for nursing work
In the group discussions with parents and young people, school emerged as occupying a central position in everyday life and as a natural location for health-related work. Parents in particular expected staff in schools to play a part in safeguarding their children’s health, and both parents and young people felt that school either was or could be a potentially important source for information, advice and support in relation to health. School was seen as an appropriate setting for activities such as health screening and surveillance, and for health promotion work.
Heads and teachers affirmed their own health-related role, both as part of a holistic approach to education and as caring
professionals. However, school staff regarded their own influence as constrained both by increasing pressure to give priority to academic attainment and by the greater influence of parents, not all of whom were thought to seek a healthy lifestyle for their children. Where the relationship with their school nurse was reported as working well, school staff spoke of the nurse as integrated into school life; for example, describing the nurse as ‘part of the furniture’ or ‘part of the family’. Here, blurring role boundaries between nurse and teacher – for example, in relation to teaching – were seen by teachers in a positive light, as evidence of teamwork. Aside from the direct contribution of the nurse in school, teachers valued the school nurse as a ‘bridge’, helping them to obtain access to other parts of the NHS for information and advice.
The young people in the study valued the opportunity to have on-site independent access to confidential advice from the school nurse. However, they wanted the nurse to spend more time in school, so as to become better acquainted with her. The degree of privacy in the accommodation used by nurses in school also needed improving.
Despite valuing health-related services in school, parents and young people thought a choice of setting important, especially for pupils who may not want to take up a school-based service. In addition, school nurses themselves reported that their caseloads were based on school rolls: few had responsibility for excluded pupils. However, many of the young people in the study reported limited availability of suitable services outside school. General practitioner’s surgeries were avoided, as it was likely that a young person could ‘bump into’ an adult relative. Where young people’s clinics were available these were liked on account of being designed with young people in mind; for example, having convenient times and offering both confidentiality and anonymity.
Discussion
This study used qualitative methods to identify and describe the distinctive role of the school nurse in work aimed at keeping children healthy. Although these findings are not necessarily representative of all school nurses, the broad themes are consistent with other recent research.17–19This study generated new knowledge about the complementary roles of school staff and school nurses, and drew attention to factors inhibiting nurses from realizing their potential in the school setting.
At the heart of school nursing achieving its potential is the need for a more strategic approach to the service. A 1996 survey of NHS Trusts providing SHS (response rate 79 per cent) found that 32 per cent had no strategy for school health services.20 Our own evidence of key constraints on school nursing – lack of needs assessment, role ambiguity, and ‘gatekeeping’ schools – all point to limits on practice when such an approach is lacking or weak. In turn, a strategic approach requires systematic assessment of the health needs of children and young people today, without which school nursing
contracts continue to reflect historical priorities. School nurses themselves are arguably well placed to contribute to local population needs assessment through ‘school health profiling’ at individual school level. Aggregating school health profiles would establish a knowledge base, which could inform purchasing decisions21 and help to target practice.18 A particular advantage of nurses carrying out health needs assessment is that they are in a position to access the views of children themselves on their needs and service preferences. There is a considerable gap in existing knowledge about children’s views as (actual or potential) users of the SHS, despite the policy drive to include the views of users in health services development.22
Uncertainty about the role of the school nurse on the part of users inevitably limits the potential of nurses. Our evidence of the complementary nature of school staff and school nursing work suggests there would be value in schools and NHS Trusts working more closely together. Yet Bagnall and Dilloway’s 1995 survey of Trusts20found that, among those that did have a strategy for SHS, less than half had involved education services. A possible model is provided by ‘service level agreements’ between the SHS and individual schools, which the Department of Health has piloted with reported success in encouraging a pro-active and joint approach to targeting needs, planning and carrying out interventions, which in turn raised the profile in schools of both health and the potential role of the school nurse.23 However, as the young people in our study made clear, school-based health services must be seen as part of a broader strategic response to the health needs of children and young people, as they cannot reach those who are unwilling – or unable – to obtain access to services in school.
School nursing has been the subject of relatively little research. Research to date, including our own, has necessarily been exploratory in character, aiming to describe the role of the school nurse. There is now a need to develop research aimed at ensuring the effectiveness of school nursing work. Our study points to the value of further research in a number of areas. Variation in the content and timing of surveillance and screening programmes in the study sites points to the importance of research to establish an evidence-based pro-gramme, as these tasks take up the majority of time of school nurses and so prevent them from doing other work. Models of any joint working between schools, school nurses and their managers might yield useful data for developing a more strategic approach, as would evaluation of developments in practice, such as school health profiling and confidential ‘drop-in’ services. Evaluation of services should include the views of pupils themselves.
Finally, it is important to acknowledge the need for school-based support to meet the additional, special, needs of pupils with an illness or disability, which fell outside the scope of the study presented here. One of the authors and colleagues have since carried out a separate study24 into the views of young people, parents and teachers on needs for and experiences of
service support for this group of pupils, which indicates that this is another area where careful needs assessment and clarity of professional roles – both of health professionals and of teachers – are needed.
Acknowledgements
The authors would like to thank the respondents who took part in the study. The research was carried out when both authors were Research Fellows at the Social Policy Research Unit, University of York. The study was funded by the Department of Health, although the views represented here are those of the authors and not necessarily of the Department. Dr Patricia Sloper made helpful comments on an earlier draft of this paper, as did two anonymous referees.
References
1 Mayall B. Negotiating health: children and home and primary school. London: Cassell, 1994.
2 Harris B. The health of the schoolchild: a history of the school medical
service in England and Wales. Buckingham: Open University Press,
1995.
3 Health Select Committee. Fourth report, child and adolescent mental
health services. London: The Stationery Office, 1997.
4 Woodroffe C, Glickman M., Barker M, Power, C. Children, teenagers
and health: the key data. Buckingham: Open University Press, 1993.
5 Botting B, Crawley R. Trends and patterns in childhood mortality and morbidity. In: Botting B, ed. The health of our children: decennial
supplement. London: HMSO, 1995: 61–81.
6 British Paediatric Association. Health needs of school age children. London: BPA, 1995.
7 Department of Health. Our healthier nation: a contract for health. Cm 3852. London: The Stationery Office, 1998.
8 Department of Health. The new NHS: modern, dependable. Cm 3807. London: The Stationery Office, 1997.
9 Department of Health. Child health in the community: a guide to good
practice. London: NHS Executive, 1996.
10 Anon. School nursing services savaged. Health Visitor 1997; 70(4): 129. 11 Harrison A, Gretton J. School health: the invisible service. In: Harrison A, Gretton J, eds. Health care UK 1986. Hermitage: Policy Journals, 1986: 25–32.
12 While AE, Barriball LL. School nursing: history, present practice and possibilities reviewed. J Adv Nursing 1993; 18: 1202–1211. 13 Mays N, Pope, C. Rigour and qualitative research. Br Med J 1995; 311:
109–112.
14 Alderson P. Listening to children: children, ethics and social research. Ilford: Barnardos, 1995.
15 Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Bryman A, Burgess RG, eds. Analyzing qualitative data. London: Routledge, 1994: 173–194.
16 Department of Health. The health of the nation: a strategy for health in
England. Cm 1986. London: HMSO, 1992.
17 Health Visitors’ Association. School nursing: here today for tomorrow. London: HVA, 1996.
18 Bagnall P, Dilloway M. In a different light: school nurses and their role
in meeting the needs of school age children. London: Department of
Health–The Queen’s Nursing Institute, 1996.
19 DeBell D, Everett G. In a class apart: a study of school nursing. Norwich: The Research Centre, City College, 1997.
20 Bagnall P, Dilloway M. In search of a blueprint: a survey of school
health services. London: Department of Health–The Queen’s Nursing
Institute, 1996.
21 Department of Health. Change, challenge, opportunity: school nurses
in the new health service structure. London: DoH, 1995.
22 NHS Executive. Patient partnership: building a collaborative strategy. London: DoH, 1996.
23 Department of Health. Negotiating school health services. London: DoH, 1994.
24 Lightfoot J, Wright S, Sloper P. Service support for children with a
chronic illness or physical disability attending mainstream schools.
York: Social Policy Research Unit, University of York, 1998.