G
IRISHL. G
UPTE, A
LASTAIRJ.W. M
ILLARIntestinal Transplantation – an Overview
Przeszczepy jelit – przegląd
Liver Unit, Birmingham Children’s Hospital, United Kingdom Adv Clin Exp Med 2006, 15, 5, 761–766
ISSN 1230−025X
EDITORIAL
The concept of intestinal failure (IF) is relative− ly new compared with the well−established concepts of liver failure and kidney failure. IF is defined as a “critical reduction of functional gut mass below the minimal amount necessary for adequate digestion and absorption to satisfy body nutrient and fluid requirements for maintenance in adults or growth in children” [1, 2]. Prior to the 1960’s, before the avail− ability of parenteral nutrition (PN), patients with IF died from starvation and malnutrition. PN revolu− tionized the outcome of IF, resulting in the current one−year survival rate of 90% and five−year survival rate of 75% [3]. The use of long−term PN can be associated with complications: intestinal failure− associated liver disease (IFALD), impaired venous access due to thrombosis of the major vessels, and recurrent life−threatening infections [4]. For individ− uals with IF who develop life threatening complica− tions, intestinal transplantation (ITx) has, in the past decade, evolved as a life−saving treatment.
Historical Perspective
Intestinal transplantation was attempted in the early 1960’s, but the lack of potent immunosup− pressive agents, inadequate graft preservation, and technical difficulties resulted in poor outcomes [5]. The development of life−threatening complications related to PN and the use of modern immunosup−
pressive agents such as cyclosporine led to rejuve− nated interest in the field of ITx. The first success− ful long−term survivor after ITx, reported from Ontario, Canada, was an adult patient with short bowel syndrome who had a combined liver and small bowel transplant and survived for more than a year following ITx on cyclosporine−based immunosuppression. At that time it was felt that the liver provided some immunological protection to the transplanted intestine [6]. Sporadic reports of success were reported elsewhere in the world in the late 80’s, the most notable being a child who received a graft from a neonate and who remains well today more than 17 years after the transplant [7]. Following the introduction of tacrolimus, the first successful series of five patients was reported from Pittsburgh in 1991 [8]. Since then, approxi− mately 1300 intestinal transplants have been per− formed worldwide in 65 centers spread across 21 countries [9]. This relatively meagre worldwide experience with intestinal transplantation is limited compared with other solid organ transplants.
Indications for Intestinal
Transplantation
The indications for intestinal transplantation proposed by Kaufmann et al. are very well estab− lished [10]: irreversible intestinal failure and one
© Copyright by Silesian Piasts University of Medicine in Wrocław
Abstract
Intestinal transplantation is evolving into a standard of care for children with intestinal failure who no longer can be maintained on PN. Advances in immunosuppression in addition to effective monitoring techniques for oppor− tunistic infections have resulted in achieving improved outcome with less morbidity. This article highlights the evo− lution of intestinal transplantation and current advances (Adv Clin Exp Med 2006, 15, 5, 761–766).
of the following: i) impaired venous access (reduced to two suitable veins for placement of feeding catheters), ii) progressive liver disease with coagulopathy, ascites, and encephalopathy, and iii) life−threatening episodes of catheter sepsis. Contraindications can be divided and subdi− vided into: 1) absolute contraindications, these being: i) profound neurological disabilities, ii) life−threatening and other uncorrectable illnesses not directly related to the digestive system, and iii) non−resectable malignancies, and 2) relative con− traindications, these being: i) severe congenital or acquired immunological deficiencies, ii) multi− system autoimmune diseases, and iii) insufficient vascular patency to guarantee vascular access for up to six months following transplant.
Types of Intestinal
Transplantation
The type of transplant performed depends on the severity of the liver disease (Fig. 1, 2): 1) min− imal or mild liver disease and impaired venous access: isolated small bowel transplantation, mod− ified multi−visceral transplantation; 2) moderate to severe liver disease with evidence of portal hyper− tension: combined liver and small bowel trans− plant, multi−visceral transplant.
There is much debate and controversy in the field of intestinal transplantation about the defini− tion of the term “multi−visceral transplant”. Multi− visceral transplantation is the term applied to any intestinal transplant in which evisceration of the abdominal organs, including the spleen, is done at the time of transplanting the donor organs. The techniques for the different surgical procedures, with some modifications in the last decade, have been described elsewhere [11–13].
Obstacles to Successful
Intestinal Transplantation
The major obstacles in the development and advancement of intestinal transplantation are the immunogenicity of the organ, leading to a high potential for rejection and thus a requirement for increased immunosuppression, late referral with patients in an agonal state, and the shortage of appropriate size−matched donor organs, leading to deaths on the waiting list.
Immunogenicity of the Organ
The intestine contains a huge store of lympho− cytes expressing class II major histocompatibility
antigens, which results in a higher incidence of rejection. In addition, the hollow viscera of the intestine is a reservoir of microorganisms which makes the graft easily susceptible to infection [14]. A failure to achieve the fine balance of enough immune suppression to maintain the health of the graft, but not so much such that the patient suffers from opportunistic infection can lead to the vicious cycle of infection and rejection, resulting in graft failure.
Late Referral and Shortage
of Donor Organs
Fecteau et al. commented upon the importance of the timing of referral for intestinal transplanta− tion [15]. In the Canadian experience, the median waiting time for liver and small bowel transplanta− tion was 212 days, with a mortality of 50% on the waiting list. The high mortality on the waiting list was mainly due to the progressive nature of IFALD in young infants under one year of age. The lack of appropriate size−matched organs fur− ther lessens the chances of a transplant and leads to a worsening of the outcome in young infants. Innovative techniques such as reduced en−bloc combined liver and small bowel transplantation (organs from older children and adults are reduced in size prior to being transplanted into smaller children) have resulted in improved availability of the organs for young recipients (Fig. 3) [16]. Even with the reduced en−bloc technique, abdominal closure in young infants under one year of age may pose a significant challenge. Tight closure of the abdomen can lead to abdominal compartment syndrome, which leads to increased morbidity and mortality [17]. In our center we have adopted the techniques of pre−transplant insertion of tissue expanders and staged abdominal closure of the abdomen in young infants undergoing small bowel transplantation. One center reported the much more aggressive technique in adult patients of abdominal wall transplantation in the management of those patients with a very scarred abdominal wall or involvement with desmoid tumors [18].
Medical and Surgical
Complications
Graft Rejection
able and cannot be easily distinguished from those of viral enteritis. There are currently no reliable noninvasive markers of rejection. Serum citrulline, a marker of mucosal mass, has shown some promise, although the differentiation between rejection and infection can make the levels diffi− cult to interpret [19]. The diagnosis of rejection is
made on histopathological examination of graft tissue from endoscopic biopsies. It is usually grad− ed as mild, moderate, or severe [20]. Mild or mod− erate rejection is treated by optimizing the immunosuppression and with pulsed doses of intravenous methylprednisolone (10–20 mg/kg to a maximum of 400 mg). Severe rejection, charac− terized by diffuse ulcerations and denuded mucosa throughout the graft, is notoriously difficult to treat and is associated with poor prognosis. Treatment strategies with OKT3, thymoglobulin
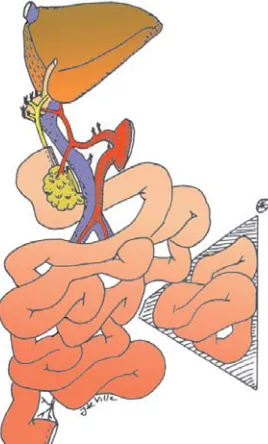
Fig. 1. Isolated intestinal transplantation: a) vascular anastomosis – arterial,
b) superior mesenteric artery of the donor is anasto− mosed to the aorta, usually with an interposition graft of donor iliac artery – venous,
c) donor superior mesenteric vein to the recipient por− tal vein or inferior vena cava,
d) intestinal anastomoses:
– donor jejunum – recipient’s residual duodenum or jejunum,
– distally, the ileum is connected to the native colon in an end−to−end fashion,
– an ileostomy is created proximal to the ileocolic anastomosis by exteriorizing the distal end of the graft using the “chimney” method with the recipi− ent’s ileum or colon anastomosed to the side of the graft below the stoma
Fig. 2. Combined liver and small bowel transplantation: a) venous anastomosis:
– suprahepatic IVC – recipient vena cava, b) arterial anastomosis:
– celiac and SMA – infrarenal aorta (Carrell patch and interposition graft of donor aorta or iliac artery),
c) portacaval shunt in the recipient to decompress portal blood return from the foregut and spleen,
d) intestinal anastomosis:
– donor jejunum – recipient’s residual duodenum or jejunum, – ileum to native colon end−to−end,
– ileostomy
Fig. 3. En−bloc reduced combined liver and small bowel transplantation:
a) reduced segment 2, 3, and 4 of the liver, b) venous anastomosis:
– piggyback triangulated left hepatic vein – recipi− ent vena cava,
c) arterial anastomosis:
– celiac and SMA – infrarenal aorta (Carrell patch and interposition graft),
d) portacaval shunt, e) intestinal anastomosis:
– donor jejunum – recipient’s residual duodenum or jejunum,
and, recently, infliximab (anti−TNF−alpha mono− clonal antibody) have been tried with variable suc− cess [21, 22]. In the last decade, the introduction of induction agents such as IL2 blockers, campath (anti−CD52), and thymoglobulin has decreased the incidence of acute rejection within the first few weeks following intestinal transplantation. This is reflected in the reported improved survival from major intestinal transplant centers in the USA.
Infection
According to the intestinal transplant registry, infection is the most common cause of morbidity and mortality following intestinal transplantation, accounting for 60–70% of the deaths [9]. The high incidence of bacterial infections is likely to be due to bacterial translocation occurring across a com− promised intestinal mucosal barrier because of reperfusion injury, disruption of the lymphocytes, rejection, and potent immunosuppressive agents. Broad−spectrum antibiotics are routinely adminis− tered during the postoperative period along with selective decontamination of the gut with oral antibiotics and antifungal agents.
Post−transplant infectious enteritis, cyto− megalovirus (CMV), and Epstein Barr virus (EBV) related post−transplant lymphoproliferative disease (PTLD) can lead to devastating consequences in the context of heavy immunosuppression following intestinal transplantation. Infectious enteritis is noted in 39% of the population following intestinal transplantation with viruses (adenovirus, rotavirus, and calcivirus) and protozoa (Giardia lamblia,
Cryptosporidium) [23]. The prompt recognition of infectious enteritis can be difficult, as the clinico− pathological picture can mimic acute rejection, but the treatments are diametrically opposite, the one requiring increased immune suppression and the other reduced immune suppression along with directed anti−rejection or anti−microbial medica− tion. Rotavirus and adenovirus enteritis can trigger episodes of acute rejection and can result in graft loss [23]. CMV infection and EBV−related PTLD are seen more commonly in the pediatric intestinal transplant population in the setting of a sero−posi− tive donor to a sero−negative recipient. Different tests (pp antigenemia, viral load) are used to make the diagnosis of CMV infection and effective treat− ment is instituted with the use of IV gancyclovir [24]. The incidence of PTLD following intestinal transplantation, historically, was reported to be as high as 30–40%. The gold standard for the diagno− sis of EBV−related PTLD still remains the histopathological examination of affected tissue. EBV viral load measured by polymerase chain reaction (PCR) is helpful to indicate ongoing EBV
viremia, but does not confirm the diagnosis of PTLD [25]. In children, presentation with recurrent infections, hypoalbuminemia, anemia, thrombocy− topenia, and neutropenia should alert the physician to perform investigations to exclude PTLD. Imaging of the abdomen for abdominal lym− phadenopathy and the chest for mediastinal lym− phadenopathy may be necessary to arrive at the diagnosis. Endoscopic procedures along with EBER (EBVin situhybridization) staining of gut biopsies may be necessary to confirm the diagnosis in children without lymphadenopathy. Preemptive reduction of immunosuppression in the context of EBV viremia has been demonstrated to prevent the progression to PTLD [26]. With the advent of EBV PCR and pre−emptive reduction of immunosup− pression, there has been a considerable improve− ment in the outcome of PTLD [9].
Graft−Versus−Host Disease
Surprisingly, despite the high lymphocyte load within the intestine, the incidence of graft−versus− host disease (GVHD) has been reported to be 8.5% from the largest single center experience, which is less of a problem than expected [27]. Optimization of tacrolimus immunosuppression and steroid administration is the treatment of choice and usually leads to a favorable outcome. Children with immune system dysregulation prior to intestinal transplanta− tion can pose significant challenges in the manage− ment of GVHD and can result in a poor outcome.
Surgical Complications
Intestinal perforation, seen in up to 40% of cases, usually occurs within the first two weeks fol− lowing intestinal transplantation and is notoriously difficult to manage. The symptoms and signs of acute peritonitis can be masked, as the children are on high−dose steroids, thus needing a high index of suspicion. Abdominal imaging and contrast studies may be needed to confirm the diagnosis. Surgical control of the perforation, either by primary closure or by insertion of a T tube into the perforation to create a controlled fistula, is mandatory. Other complications, such as adhesive obstruction, pan− creatitis, development of biliary sludge with partial obstruction, and wound and stomal issues, are fre− quent but can be successfully managed.
Nutritional Outcome
and Quality of Life
tion [9]. The median time to establish children on an oral diet varies, as it is dependent on the pre−trans− plant oral intake. Children with a diagnosis of pseu− do−obstruction who have not eaten normally prior to intestinal transplantation find it extremely difficult to establish oral intake and may need psychological and speech therapeutic input. Few studies exist in the literature addressing the issue of long−term growth in intestinal transplantation. Iyer et al. report− ed on 36 children undergoing intestinal transplanta− tion [28]. The median time to wean them off PN was 29 days. The children were followed up to two years after ITx. The majority of the patients showed sig− nificant retardation of linear growth after transplan− tation and the growth retardation persisted on fol− low−up. In contrast, weight gain continued at the same velocity before and after transplantation [28].
With the recent rapid advances and improved survival following intestinal transplantation, issues regarding the quality of life in long−term survivors have come to the forefront. Sudan et al. have used a Child Health Questionnaire (CHQ) specifically validated for 5–16 year olds and applied it to three patient groups and their parents: i) children under− going intestinal transplantation (n = 21), ii) healthy school children of the same age (n = 232), and iii) children with end−stage renal disease (n = 18) [29]. The CHQ questionnaire addressed 14 domains related to physical functioning, bodily pain, self esteem, parental impact in terms of time and emo− tion, family activities, etc. Overall, the intestinal transplant recipients reported similar scores in all domains compared with normal children. However, younger intestinal transplant recipients (5–10 years) reported significantly lower scores than older recip− ients (11–18 years) in the domains of global health, general health perception, and family activities [29].
Living Related Intestinal
Transplantation
Living related intestinal transplantation is an option to address the deaths on the waiting list and improve the pool of donors [30]. The proponents of the procedure claim the advantages of reduced cold ischemia time, the ability to select recipients in an optimal condition, and the opportunity to plan a tolerance−inducing immunosuppression protocol [14]. However, the graft per se does not offer any immunological advantage and most indi− viduals would still need to be maintained on life− long immunosuppression. Thus, living related ITx has not been widely adapted in major ITx centers and is restricted to select centers in the world.
Outcome
Data from the intestinal transplant registry presented at the IX Small Bowel Transplant Symposium in Brussels reported a one−year sur− vival rate of 90% and a three−year survival rate of around 70–80%. In a univariate and multi− variate analysis conducted within the registry, the poor prognostic variables were: hospitaliza− tion at the time of transplant, age under two years, and centers performing less than 10 trans− plants in total.
In conclusion, the rapid advances in the surgi− cal techniques and immunosuppressive strategies are reflected in an overall improved outcome. ITx in the next 20 years will continue to evolve and has the potential to be considered as an alternative strategy to home PN in selected patients.
Acknowledgement. We would like to thank Prof. Jean de Ville de Goyet for his kind permission to use the illustrations.
References
[1] Irving M: Intestinal failure. J Gastroenterol Hepatol 2000, 15 Suppl, G26–G29.
[2] Goulet O, Ruemmele F, Lacaille F, Colomb V: Irreversible intestinal failure. J Pediatr Gastroenterol Nutr 2004, 38, 250–269.
[3] Holden C: Review of home paediatric parenteral nutrition on the UK. Br J Nurs 2001, 10, 782–788. [4] Goulet O, Revillon Y: Intestinal transplantation. Indian J Pediatr 2003, 70, 737–742.
[5] Reyes J, Mazariegos GV, Bond GM, Green M, Dvorchik I, Kosmach−Park B et al.: Pediatric intestinal trans− plantation: historical notes, principles and controversies. Pediatr Transplant 2002, 6, 193–207.
[6] Grant D, Wall W, Mimeault R, Zhong R, Ghent C, Garcia B et al.: Successful small−bowel/liver transplanta− tion. Lancet 1990, 335, 181–184.
[7] Ruemmele FM, Sauvat F, Colomb V, Jugie M, Jan D, Canioni D et al.: Seventeen years after successful small bowel transplantation: long term graft acceptance without immune tolerance. Gut 2006, 55, 903–904.
[8] Todo S, Tzakis A, Reyes J, Abu−Elmagd K, Casavilla A, Fung JJ et al.: Intestinal transplantation in humans under FK 506. Transplant Proc 1993, 25, 1198–1199.
[9] Grant D, Abu−Elmagd K, Reyes J, Tzakis A, Langnas A, Fishbein T et al.: 2003 report of the intestine trans− plant registry: a new era has dawned. Ann Surg 2005, 241, 607–613.
[11] Kato T, Romero R, Verzaro R, Misiakos E, Khan FA, Pinna AD et al.: Inclusion of entire pancreas in the com− posite liver and intestinal graft in pediatric intestinal transplantation. Pediatr Transplant 1999, 3, 210–214. [12] Kato T, Tzakis AG Selvaggi G Madariaga J: Surgical techniques used in intestinal transplantation. Curr Opin
OrganTransplant 2004, 9, 207–213.
[13] Sudan DL, Iyer KR, Deroover A, Chinnakotla S, Fox IJ, Jr., Shaw BW Jr. et al.: A new technique for com− bined liver/small intestinal transplantation. Transplantation 2001, 72, 1846–1848.
[14] Starzl TE, Murase N, Abu−Elmagd K, Gray EA, Shapiro R, Eghtesad B et al.: Tolerogenic immunosuppres− sion for organ transplantation. Lancet 2003, 361, 1502–1510.
[15] Fecteau A, Atkinson P, Grant D: Early referral is essential for successful pediatric small bowel transplantation: The Canadian experience. J Pediatr Surg 2001, 36, 681–684.
[16] de Ville dG, Mitchell A, Mayer AD, Beath SV, McKiernan PJ, Kelly DA et al.: En block combined reduced− liver and small bowel transplants: from large donors to small children. Transplantation 2000, 69, 555–559. [17] Watson RA, Howdieshell TR: Abdominal compartment syndrome. South Med J 1998, 91, 326–332.
[18] Selvaggi G, Levi DM, Kato T, Madariaga J, Moon J, Nishida S et al.: Expanded use of transplantation tech− niques: abdominal wall transplantation and intestinal autotransplantation. Transplant Proc 2004, 36, 1561–1563. [19] Pappas PA, Saudubray JM, Tzakis AG, Rabier D, Carreno MR, Gomez−Marin O et al.: Serum citrulline as
a marker of acute cellular rejection for intestinal transplantation. Transplant Proc 2002, 34, 915–917.
[20] Lee RG, Nakamura K, Tsamandas AC, Abu−Elmagd K, Furukawa H, Hutson WR et al.: Pathology of human intestinal transplantation. Gastroenterology 1996, 110, 1820–1834.
[21] Abu−Elmagd K, Reyes J, Bond G, Mazariegos G, Wu T, Murase N et al.: Clinical intestinal transplantation: a decade of experience at a single center. Ann Surg 2001, 234, 404–416.
[22] Fishbein TM: The current state of intestinal transplantation. Transplantation 2004, 78, 175–178.
[23] Ziring D, Tran R, Edelstein S, McDiarmid SV, Gajjar N, Cortina G et al.: Infectious enteritis after intestinal transplantation: incidence, timing, and outcome. Transplantation 2005, 79, 702–709.
[24] Bueno J, Green M, Kocoshis S, Furukawa H, Abu−Elmagd K, Yunis E et al.: Cytomegalovirus infection after intestinal transplantation in children. Clin Infect Dis 1997, 25, 1078–1083.
[25] Green M, Bueno J, Rowe D, Mazariegos G, Qu L, Abu−Almagd K et al.: Predictive negative value of persis− tent low Epstein−Barr virus viral load after intestinal transplantation in children. Transplantation 2000, 70, 593–596.
[26] Reyes J, Mazariegos GV, Bond GM, Green M, Dvorchik I, Kosmach−Park B et al.: Pediatric intestinal trans− plantation: historical notes, principles and controversies. Pediatr Transplant 2002, 6, 193–207.
[27] Mazariegos GV, Abu−Elmagd K, Jaffe R, Bond G, Sindhi R, Martin L et al.: Graft versus host disease in intestinal transplantation. Am J Transplant 2004, 4, 1459–1465.
[28] Iyer K, Horslen S, Iverson A, Sudan D, Fox I, Shaw B et al.: Nutritional outcome and growth of children after intestinal transplantation. J Pediatr Surg 2002, 37, 464–466.
[29] Sudan D, Horslen S, Botha J, Grant W, Torres C, Shaw BW Jr. et al.: Quality of life after pediatric intestinal transplantation: the perception of pediatric recipients and their parents. Am J Transplant 2004, 4, 407–413. [30] Testa G, Panaro F, Schena S, Holterman M, Abcarian H, Benedetti E: Living related small bowel transplan−
tation: donor surgical technique. Ann Surg 2004, 240, 779–784.
Address for correspondence:
Girish Gupte
Birmingham Children’s Hospital, Steelhouse Lane, Birmingham B4 6NH, United Kingdom
Tel: +44 121 333 8255 Fax: +44 121 333 8251
E−mail: [email protected]
Conflict of interest: None declared
Received: 8.08.2006 Accepted: 21.09.2006