ARTICLE
Failure of Ductus Arteriosus Closure Is Associated
With Increased Mortality in Preterm Infants
Shahab Noori, MDa, Michael McCoy, MS, ARNPa, Philippe Friedlich, MD, MS, Epib, Brianna Bright, MAa,c, Venugopal Gottipati, MDa, Istvan Seri, MD, PhDb, Kris Sekar, MDa
aDepartment of Pediatrics, Neonatal-Perinatal Medicine, Children’s Hospital, andcDepartment of Biostatistics and Epidemiology, College of Public Health, University of
Oklahoma Health Sciences Center, Oklahoma City, Oklahoma;bDepartment of Pediatrics, Division of Neonatology, Childrens Hospital Los Angeles, Keck School of
Medicine, University of Southern California, Los Angeles, California
The authors have indicated they have no financial relationships relevant to this article to disclose.
What’s Known on This Subject
PDA is associated with increased morbidity in VLBW infants; however, because the standard of care has been to close the PDA, data on the outcome of patients with a persistent PDA are scarce.
What This Study Adds
After adjustments for potential confounders, we demonstrated an eightfold increase in mortality in patients with a persistent PDA. Although our finding does not establish the PDA as the cause of the increased mortality, it does raise this possibility.
ABSTRACT
OBJECTIVE.Because the standard of care has been to attempt to close the patent ductus arteriosus in preterm neonates, there is a paucity of information on the outcome of patients with a persistent patent ductus arteriosus. Our objective was to compare the mortality of preterm infants with and without a persistent patent ductus arteriosus.
METHODS.This was a single-center, retrospective study. Very preterm infants (birth weightⱕ1500 g and gestational ageⱕ29 weeks) who survived beyond the first 3 postnatal days and did not undergo surgical ligation were included in the primary analysis. Mortality of neonates with a persistent and a closed patent ductus arteriosus was compared during the initial hospitalization by using the2test. Cox proportional
hazard regression and logistic regression were used to take into account the time until death and assess the independent effect of each risk factor on mortality. We also performed 3 secondary analyses by excluding patients who died during the first 7 and 14 postnatal days and including patients who underwent surgical ligation by using different group assignments. A persistent patent ductus arteriosus was defined as a failure of either spontaneous or pharmacologic ductal closure during the initial hospitalization.
RESULTS.Patients with a persistent patent ductus arteriosus (n⫽41) had lower birth weight and were less mature than those with a closed ductus (n⫽260). Unadjusted mortality rate was higher in patients with a persistent (70.7%) than with a closed (11.2%) ductus. After adjustment for perinatal factors, level of maturity, disease severity, and morbid pathologies, the hazard for death in neonates with a persistent ductus was eightfold higher than in those with a closed ductus. Exclusion of patients who died during the first 2 weeks or inclusion of those who underwent ductal ligation did not change the findings.
CONCLUSION.Failure of ductal closure is associated with an increase in mortality in very preterm infants.Pediatrics2009;123:e138–e144
I
N THE PAST decades, closure of the patent ductus arteriosus (PDA) has been the standard of care for preterm infants.1In these patients, closure of the PDA is usually first attempted by the administration of a cyclooxygenase(COX) inhibitor, such as indomethacin or ibuprofen, and if pharmacologic closure is unsuccessful, then the ductus is surgically ligated in the vast majority of cases. The primary rationale for this strategy is the physiologic plausibility that left-to-right shunting across the PDA results in deleterious systemic and pulmonary hemodynamic effects manifesting as systemic hypoperfusion and pulmonary overcirculation, respectively. Indeed, a large number of studies have found an association between PDA and major complications of prematurity where abnormal pulmonary and systemic hemodynamics may play a contributory role. These morbidities include bronchopulmonary dysplasia (BPD),2–4 intraventricular hemorrhage (IVH),5,6 and necrotizing enterocolitis (NEC).7–9 Furthermore, findings of
studies in developing animals lend support to the notion that PDA plays a role in the pathogenesis of these complications.10,11
www.pediatrics.org/cgi/doi/10.1542/ peds.2008-2418
doi:10.1542/peds.2008-2418
Key Words
ibuprofen, indomethacin, ligation, neonate, patent ductus arteriosus
Abbreviations
PDA—patent ductus arteriosus COX— cyclooxygenase BPD— bronchopulmonary dysplasia IVH—intraventricular hemorrhage NEC—necrotizing enterocolitis VLBW—very low birth weight GA— gestational age
OUHSC—Oklahoma University Health Sciences Center
CRIB— clinical risk index for babies CI— confidence interval
Accepted for publication Oct 3, 2008 Address correspondence to Shahab Noori, MD, Neonatal Perinatal Medicine, Department of Pediatrics, University of Oklahoma, College of Medicine, 1200 Everett Dr, 7th Floor North Pavilion, Oklahoma City, OK 73104. E-mail: [email protected]
The rationales for ductal closure have recently been challenged12–15 because data from randomized clinical
trials on the benefits of ductal closure are scarce8 and
indomethacin, the COX inhibitor most commonly used for the closure of the ductus arteriosus, is associated with significant short-term and possibly long-term adverse effects.16–18 In fact, some authors have recommended a
conservative approach to the treatment of the preterm neonate with a PDA so that pharmacologic and/or sur-gical closure would be reserved for exceptional cases only.13Because the standard of practice has been to close
the PDA, there is a paucity of information on the out-come of patients with a persistent PDA.
METHODS
The objective of this retrospective study was to investi-gate the possible impact of the failure of ductal closure on mortality in very low birth weight (VLBW) infants who were born atⱕ29 weeks’ gestational age (GA). The institutional review board at the University of Oklahoma Health Sciences Center (OUHSC) approved the study, and informed consent was waived.
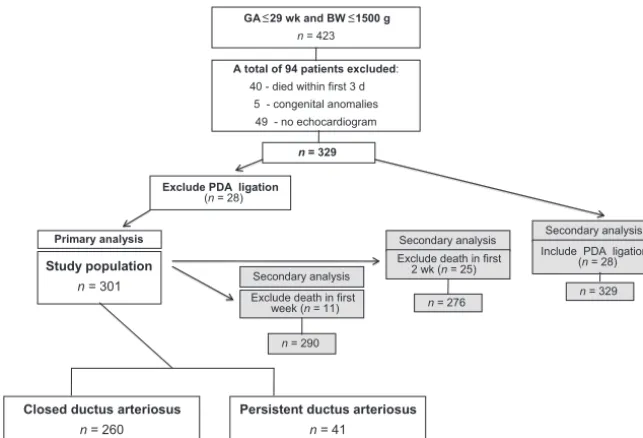
VLBW infants who were born atⱕ29 weeks’ GA, had a birth weight of ⱕ1500 g, and were admitted to the NICU of the OUHSC Children’s Hospital from January 2005 to August 2007 were included in the study. Elec-tronic medical charts were reviewed. Figure 1 depicts the study population. Because shunting across the PDA is a normal phenomenon during postnatal transition, we ex-cluded patients who died during the first 3 postnatal days. Patients with major congenital anomalies were also excluded. In addition, because the status of ductal patency cannot be objectively verified without the use of echocardiography, we excluded patients who did not have at least 1 echocardiographic study performed. Fi-nally, because surgical ligation of the ductus in our pa-tient population took place over a wide range of post-natal ages and because the impact of ligation on mortality and morbidity is complex and difficult to
as-sess, we excluded from the primary analysis patients who had undergone ligation (n ⫽ 28); however, to assess the potential impact of ligation on mortality, we included these neonates in our secondary analyses (Fig 1). Of the 423 patients screened, 301 were included in the primary analysis. These patients were divided into 2 groups: closed ductus and persistent ductus. The closed ductus group (n⫽260) comprised patients whose duc-tus closed either spontaneously or in response to expo-sure to COX inhibitors. The persistent ductus group (n⫽
41) comprised patients whose ductus was open (ie, blood flow detected by color Doppler) on the last echo-cardiogram obtained before discharge or death regard-less of treatment status. Patency of the ductus on the last echocardiogram in the patients who were enrolled in this group was not attributed to reopening of the PDA as a result of clinical deterioration caused by sepsis or other pathology. The size of the PDA on the last echocardio-gram varied from small (ⱕ1.5 mm;n⫽22), to moderate (1.6 –2.5 mm; n ⫽ 13) to large (⬎2.5 mm; n ⫽ 6). Patients in the persistent ductus group had not been exposed to COX inhibitors because of the presence of a clinically “nonsignificant” PDA (n⫽12) or had received either a partial (n ⫽ 3) or a complete (n⫽ 15) single course (3 doses of a COX inhibitor) or prolonged or multiple courses (n⫽11) of COX inhibitors but failed to achieve complete ductal closure at the time of discharge or death. Among the 29 patients in the persistent ductus group who received treatment with a COX inhibitor, the primary reasons for not proceeding with surgical ligation were a ductal diameter of ⬍2 mm without hemody-namic instability (n ⫽ 13), having received a COX in-hibitor at the time of death (n ⫽ 7), change in the direction of ductal shunting from left-to-right to right-to-left (n ⫽ 7), thought to be unstable to tolerate the procedure (n⫽3), and documented sepsis (n⫽2).
As per the clinical protocol in the NICU at OUHSC, the diagnosis of a PDA in very preterm infants needs to be confirmed by echocardiography. Accordingly, a
GA ≤29 wk and BW ≤1500 g n = 423
Study population
n = 301
A total of 94 patients excluded: 40 - died within first 3 d
5 - congenital anomalies 49 - no echocardiogram
n = 329
Primary analysis
Exclude PDA ligation
(n = 28)
Secondary analysis
Secondary analysis Secondary analysis
Exclude death in first week (n = 11)
Exclude death in first 2 wk (n = 25)
n = 290
n = 276
Closed ductus arteriosus
n = 260
Persistent ductus arteriosus
n = 41
Include PDA ligation (n = 28)
n = 329
FIGURE 1
screening echocardiogram is usually obtained for these patients on postnatal days 2 to 4. Occasionally, however, when the patient receives no or only minimal respira-tory support and has no evidence of hemodynamic in-stability, the neonatologist may forego obtaining an echocardiogram. As mentioned previously, in this study, we excluded all patients without at least 1 echocardio-gram documenting the status of the PDA. A PDA is treated when it is considered hemodynamically signifi-cant on the basis of the ductal size and/or clinical symp-toms attributed to ductal shunting. When a PDA is con-sidered not significant, the patient is followed by serial echocardiograms until discharge and then followed by a cardiologist as an outpatient. A significant PDA is treated with either indomethacin or ibuprofen lysine according to the neonatologist’s preference. Ductal response to COX inhibitor is evaluated by echocardiography after each treatment course. If the patient fails to respond to 2 to 3 courses of COX inhibitor treatment with complete closure of the ductus, a significant PDA is ligated, whereas a nonsignificant PDA is followed as described. For the purposes of this study, significant PDA is defined as a PDA with a ductal diameter of ⱖ1.5 to 2.0 mm and/or clinical signs and symptoms of significant left-to-right ductal shunting such as an active precordium, bounding pulses, wide pulse pressure, and systemic hy-potension.
To adjust for the effects of disease severity on out-come, we used the clinical risk index for babies (CRIB) score.19,20We also collected data on patient
characteris-tics and diseases that have been shown to affect mortal-ity. These data include GA, birth weight, antenatal ste-roid exposure, Apgar score at 5 minutes, gender, IVH grades III to IV, NEC (Bell stages II–III), and culture-proven sepsis.
GA and birth weight between the groups were com-pared using 2-tailed Student’sttest. Nonparametric test (Mann-Whitney) was used to compare data with non-Gaussian distribution. Binomial parameters between the
groups were compared with 2or Fisher’s exact test as
appropriate. Univariate logistic regression was used to predict the effect of selected variables on mortality. These variables included GA, antenatal steroid exposure, Apgar score at 5 minutes, gender, CRIB score, IVH III to IV, NEC II to III, sepsis, and exposure to COX inhibitors. Variables withP⬍.1 in the univariate logistic regression analyses were used simultaneously as potential con-founders in multivariate logistic regression models to define the odds of mortality in case of a persistent PDA. Finally, Cox proportional hazard regression was used to take into account time until death and assess the inde-pendent effect of each risk factor on mortality. The time to event was defined as birth to the identification of death.
In addition, we performed a number of secondary data analyses. First, we excluded patients who died dur-ing the first week and then those who died durdur-ing the first 2 weeks of postnatal life. In addition, we included patients who underwent ductal ligation in the analysis by using 3 different scenarios. First, we included the ligated patients in the closed ductus group and then in the persistent ductus group. Finally, using the median age of death in patients in the persistent ductus group as the cutoff point (14 days), a patient with a ligated PDA was considered to belong to the closed or the persistent ductus group when ligation was performed before or after the cutoff point, respectively.
RESULTS
The study population that underwent the primary anal-ysis comprised 301 VLBW infants who were born atⱕ29 weeks’ GA (Fig 1). There were 260 patients in the closed ductus group and 41 patients in the persistent ductus group (Table 1). Patients with a persistent ductus had a lower birth weight, were less mature, had a higher CRIB score and higher incidence of IVH grades III to IV, and were more likely to receive a COX inhibitor than those in the closed ductus group (Table 1). Mortality rate was
TABLE 1 Clinical Characteristics of the Study Population
Characteristic Closed Ductus
Persistent Ductus
Ligated Ductus
P
Closed vs Persistent
Closed vs Ligated
Persistent vs Ligated
n 260 41 28
GA, mean⫾SD, wk 27.3⫾1.6 26.0⫾2.0 26.6⫾1.8 .0002 .0564 .2111 Birth weight, mean⫾SD, g 971⫾247 842⫾296 909⫾219 .0027 .2039 .3082
Antenatal steroid, % 81.9 77.8 71.4 .5500 .1810 .5610
Apgar at 1 min, median (range) 5 (0–9) 5 (1–9) 5 (1–8) .3315 .8591 .4431 Apgar at 5 min, median (range) 7 (1–9) 6 (1–9) 7 (1–9) .0580 .7262 .3082
AGA, % 91.9 85.4 89.3 .1720 .6310 .6350
CRIB score, median (range) 4 (0–17) 8 (1–19) 3 (0–18) .0013 .8681 .0301
RDS, % 87.6 92.7 100.0 .3470 .0480 .1430
IVH grades III–IV, % 14.2 34.1 25 .0020 .1320 .4170
NEC stages II–III, % 5.8 7.3 14.3 .6980 .0850 .3460
Sepsis, % 7.3 9.8 32.1 .5830 ⬍.0001 .0200
Exposure to COX inhibitors, % 50.0 71.0 96.4 .0130 ⬍.0001 .0070
Mortality, % 11.2 70.7 7.1 ⬍.0001 .5150 ⬍.0001
Mortality DOL, median (range) 22 (5–182) 14 (4–140) 168 (164–172) .0184 .0298 .0195
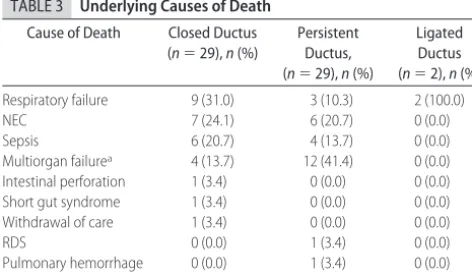
higher among patients with a persistent ductus (29 of 41 [70.7%]) compared with those with a closed ductus (29 of 260 [11.2%]; P⬍ .0001; Tables 1 and 2). On addi-tional analysis of the persistent ductus group, mortality rates were found to be 55% (12 of 22) in patients with a small PDA (ductal diameterⱕ1.5 mm) compared with 89% (17 of 19) in those with a moderate or large PDA (ductal diameterⱖ1.6 mm) on the last echocardiogram (P⫽.014). Table 3 lists the causes of death in the closed and persistent ductus groups as well as in patients who underwent ligation. It is of note that more patients died from multiorgan failure in the persistent ductus group compared with the other 2 groups.
Univariate logistic regressions of potential confound-ers that affect mortality in the primary analysis between the closed and persistent ductus groups are shown in Table 4. After adjusting for GA, Apgar score at 5 minutes, CRIB score, IVH III to IV, NEC stages II to III, sepsis, and exposure to COX inhibitors in multiple logistic regres-sion models, the odds for mortality were significantly higher when the PDA persisted (odds ratio: 16.79 [95%
confidence interval [CI]: 6.05– 46.61]; P ⬍ .0001). By using the Cox proportional hazard regression model to incorporate the effect of time until death while control-ling for other significant covariates, the hazard for death for the patients in the persistent ductus group remained significantly higher than in the closed ductus group (hazard ratio: 8.34 [95% CI: 4.30 –16.06]; P ⬍ .0001; Table 5).
Patients who were treated with COX inhibitors in the closed and persistent ductus groups (n⫽159) received indomethacin (n ⫽120), ibuprofen (n ⫽ 35), or both (n ⫽ 4). Exposure to indomethacin or ibuprofen was similarly associated with an increased mortality in uni-variate regression analysis (data not shown).
On additional analysis, excluding patients who died during the first postnatal week, the persistent ductus group had a higher mortality rate (22 of 34 [64.7%]) compared with the closed ductus group (25 of 256 [9.8%]; P ⬍ .0001; Table 2). Similarly, excluding pa-tients who died during the first 2 weeks, papa-tients in the persistent ductus group had a higher mortality rate (13 of 25 [52%]) than those in the closed ductus group (20 of 251 [8%];P⬍.0001). Adjusting for the confounders, the odds for mortality and the hazard for death remained higher when PDA persisted (Table 5).
Among the 28 patients who had undergone PDA ligation and thus were excluded from the primary anal-ysis, 2 died during their initial hospitalization. To inves-tigate whether exclusion of these patients affected the observed difference in mortality between the closed and persistent ductus groups, we included them in the sec-ondary analyses by using 3 different scenarios (see “Methods”). Regardless of the group assignment of the patients with a surgically ligated ductus arteriosus, the confounder-adjusted odds for mortality and hazard for death remained higher for patients who were assigned to the persistent ductus group (Table 5).
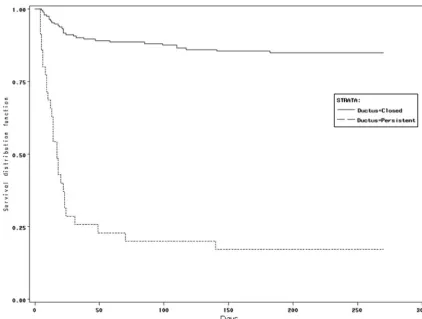
Survival data at 9 months of age were available for 227 of the 301 patients who were enrolled in the pri-mary analysis. The Kaplan-Meier curve for this subset showed significant difference in mortality patterns be-tween the 2 groups (log-rank testP⬍.0001; Fig 2). Data
TABLE 2 Unadjusted Mortality Rates
Parameter Persistent
Ductus, %
Closed Ductus, %
P
Primary analysis
PDA ligation excluded 70.7 11.2 .0001
Secondary analyses
Patients survived⬎1 wka 64.7 9.8 .0001
Patients survived⬎2 wkb 52.0 8.0 .0001
Ligation as closed ductusc 70.7 10.8 .0001
Ligation as open ductusd 44.9 11.2 .0001
Ligation⬎14 d as open ductuse 50.0 10.9 .0001
aPatients were included in the analysis only when they survived⬎1 week after delivery. bPatients were included in the analysis only when they survived⬎2 weeks after delivery. cPatients with surgically ligated PDA included in the closed ductus group.
dPatients with surgically ligated PDA included in the persistent ductus group.
ePatients with surgically ligated PDA were included in the persistent ductus group when
liga-tion was performed after 14 days of postnatal life, whereas patients with a surgically ligated PDA were included in the closed ductus group when ligation was performed on or before 14 days of postnatal life.
TABLE 3 Underlying Causes of Death
Cause of Death Closed Ductus (n⫽29),n(%)
Persistent Ductus, (n⫽29),n(%)
Ligated Ductus (n⫽2),n(%)
Respiratory failure 9 (31.0) 3 (10.3) 2 (100.0)
NEC 7 (24.1) 6 (20.7) 0 (0.0)
Sepsis 6 (20.7) 4 (13.7) 0 (0.0)
Multiorgan failurea 4 (13.7) 12 (41.4) 0 (0.0)
Intestinal perforation 1 (3.4) 0 (0.0) 0 (0.0) Short gut syndrome 1 (3.4) 0 (0.0) 0 (0.0) Withdrawal of care 1 (3.4) 0 (0.0) 0 (0.0)
RDS 0 (0.0) 1 (3.4) 0 (0.0)
Pulmonary hemorrhage 0 (0.0) 1 (3.4) 0 (0.0)
PPHN 0 (0.0) 2 (6.9) 0 (0.0)
The cause of death was assigned by 1 of the authors, who was masked to the PDA status of the patients. RDS indicates respiratory distress syndrome; PPHN, persistent pulmonary hyperten-sion of newborn.
aMore than 2 organ system failures without identification of cause, such as sepsis, pneumonia,
or NEC.
TABLE 4 Univariate Logistic Regression of Potential Confounders That Affect Mortality in the Primary Analysis Between the Closed and Persistent Ductus Groups
Confounder OR 95% CI P
GA 0.52 0.43–0.64 .0001
Antenatal steroid 0.69 0.33–1.43 .3200
Apgar score at 5 min 0.80 0.70–0.91 .0001
Male gender 1.55 0.87–2.78 .1400
CRIB 1.28 1.18–1.39 .0001
IVH grades III–IV 5.65 2.92–10.90 ⬍.0001
NEC stages II–III 7.89 2.91–21.41 ⬍.0001
Sepsis 3.69 1.53–8.90 .0054
Exposure to COX inhibitors 2.55 1.38–4.74 .0021
Persistent ductus 19.25 8.86–41.81 ⬍.0001
on the fate of the PDA were available only on 7 of the 12 patients who were discharged from the hospital with a persistent ductus. Five of the 7 patients had their PDA still open on follow-up visit in the clinic (ages of 66, 113, 121, 158, and 365 days), whereas the remaining 2 pa-tients had a closed ductus on the follow-up visit at 88 and 251 days of postnatal life, respectively.
DISCUSSION
In this retrospective study, we found that failure of ductal closure in VLBW neonates who were born atⱕ29 weeks’ GA was associated with an increase in mortality. This association remained significant after adjustment for the degree of immaturity; initial disease severity; and morbid pathologies such as severe IVH, NEC, and sepsis. The hazard for death for patients in the persistent ductus group was eightfold higher compared with the closed ductus group. Furthermore, this association persisted even when patients who died in the first week or first 2 weeks of postnatal life were excluded and when ligated patients were included in the analysis. The reasons for the increased mortality are unknown but may be, at least in part, related to the pathophysiology of the PDA.
Left-to-right shunting across the PDA significantly af-fects both the pulmonary and the systemic circulation, resulting in pulmonary overcirculation and decreased systemic perfusion, respectively.21–26 Pulmonary
over-flow can lead to pulmonary edema, increased need for ventilatory support, maldevelopment of the alveolar structure, and ultimately BPD.21–23The associated
com-promised systemic blood flow and hypotension can af-fect tissue oxygen delivery and result in abnormal organ function and tissue injury.24–26From this standpoint, it is
an interesting finding that the most common cause of death in persistent ductus group was multiorgan failure. An alternative explanation for the association between increased mortality and persistent PDA is that persistent ductus may be only a marker of disease severity; how-ever, a possible contributory role of ductal shunting in the observed increased mortality might be supported by our finding that patients with a moderate to large PDA had higher mortality than those with a small ductus arteriosus.
Because there is a lack of randomized clinical trials comparing outcomes in neonates who are treated for a PDA with those who do not receive pharmacologic treat-ment or surgical closure, some authors have questioned the justification for administering COX inhibitors or per-forming surgical ligations to close the PDA.12–14Because
of the growing concerns about the potential harmful effects of surgical ligation of the ductus, the criticism of the present approach to the treatment of the PDA has especially targeted ligation. Indeed, surgical closure of the PDA leads to an impairment of cardiovascular func-tion.27,28Although transient, the documented
deteriora-tion in the cardiovascular status and the suspected de-terioration in pulmonary function after surgical ligation may have long-term implications, especially because there is an association between PDA ligation and BPD and poor neurodevelopmental outcome.29,30 Although
PDA ligation may be only a marker rather than the cause of these complications, because of the lack of random-ized trials, a cause– effect relationship cannot be ruled out. As a consequence, some investigators have sug-gested a conservative approach to the treatment of PDA whereby surgical closure is reserved for patients in in-tractable heart failure13; however, it is unclear whether
the prolonged exposure to pulmonary overcirculation and compromised systemic perfusion is less harmful than surgical ligation. Along these lines, we found that inclusion of patients who had undergone surgical liga-tion into the closed or persistent ductus group or choos-ing their group assignment accordchoos-ing to the median time of death in the persistent ductus group did not affect the finding of the primary analysis, because a persistent PDA remained associated with a significantly higher mortality in these secondary analyses; therefore, surgical ligation in this patient population does not seem to have played an appreciable role in influencing mortality.
Because the common practice has been to close the PDA pharmacologically or surgically, data on the out-come of preterm infants with a persistent ductus are scarce. To our knowledge, only 1 other study addressed this issue and reported a fourfold increase in the
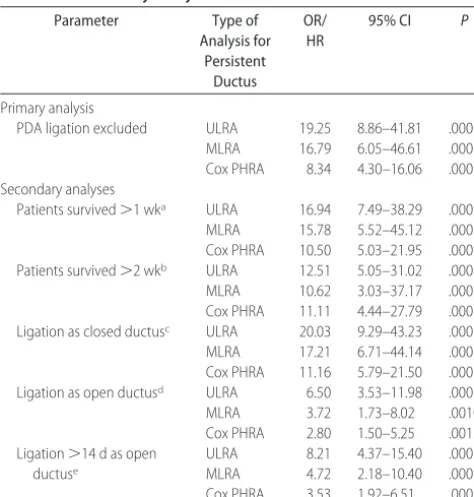
mor-TABLE 5 Odds and Hazard Ratios for Death in the Primary and Secondary Analyses
Parameter Type of
Analysis for Persistent
Ductus
OR/ HR
95% CI P
Primary analysis
PDA ligation excluded ULRA 19.25 8.86–41.81 .0001 MLRA 16.79 6.05–46.61 .0001 Cox PHRA 8.34 4.30–16.06 .0001 Secondary analyses
Patients survived⬎1 wka ULRA 16.94 7.49–38.29 .0001
MLRA 15.78 5.52–45.12 .0001 Cox PHRA 10.50 5.03–21.95 .0001 Patients survived⬎2 wkb ULRA 12.51 5.05–31.02 .0001
MLRA 10.62 3.03–37.17 .0002 Cox PHRA 11.11 4.44–27.79 .0001 Ligation as closed ductusc ULRA 20.03 9.29–43.23 .0001
MLRA 17.21 6.71–44.14 .0001 Cox PHRA 11.16 5.79–21.50 .0001 Ligation as open ductusd ULRA 6.50 3.53–11.98 .0001
MLRA 3.72 1.73–8.02 .0010 Cox PHRA 2.80 1.50–5.25 .0013 Ligation⬎14 d as open
ductuse
ULRA 8.21 4.37–15.40 .0001 MLRA 4.72 2.18–10.40 .0001 Cox PHRA 3.53 1.92–6.51 .0001
Median day of death for open ductus (no ligation included): 14. Variables withP⬍.1 in the univariate logistic regression analysis (ULRA; data not shown) were used simultaneously as potential confounders in multivariate logistic regression analysis (MLRA) and Cox proportional hazard regression analysis (Cox PHRA) models. OR/HR indicates odd ratio (for ULRA and MLRA) or hazard ratio (for Cox PHRA).
aPatients were included in the analysis only when they survived⬎1 week after delivery. bPatients were included in the analysis only when they survived⬎2 weeks after delivery. cPatients with surgically ligated PDA included in the closed ductus group.
dPatients with surgically ligated PDA included in the persistent ductus group.
ePatients with surgically ligated PDA were included in the persistent ductus group when
tality of preterm infants with a persistent PDA.31 The
finding of an eightfold increase in the mortality of VLBW neonates with a persistent PDA in our study strongly supports and extends the observations of the previous study.31
Patients who were discharged from the hospital with a persistent ductus remained asymptomatic at the fol-low-up outpatient cardiology clinic visits during the first postnatal year. This observation is consistent with the findings of a recent study that demonstrated that none of the 21 VLBW infants who were included in this study and discharged from the hospital with a PDA developed congestive heart failure by the time of the follow-up visit.32
Our study suffers from several limitations. Given its retrospective nature, the 2 groups were not similar in many of their clinical characteristics. We adjusted for the identified differences by using multivariate logistic and proportional hazard regression models, yet certain dif-ferences may have remained unidentified and thus not adjusted for by our analysis. Another limitation is that the persistent ductus group included patients with and without exposure to COX inhibitors; however, because we were interested in the effect of failure of closure of the ductus as an independent variable regardless of the cause, this heterogeneity is likely of less importance. In addition, we corrected for the effect of COX inhibitor exposure in the regression models. Finally, it is of note
that the CIs for the odds for mortality and, to a lesser extent, the hazard for death were relatively wide; how-ever, the finding that the lower limits of these CIs are 6.05 and 4.30, respectively, is reassuring and lends sup-port for the validity and potential clinical significance of our observations.
CONCLUSIONS
We found a significant increase in mortality in very preterm infants when the ductus arteriosus remained open. It is important to emphasize that our findings do not establish the persistent ductus arteriosus as the cause of the observed increased mortality; nevertheless, it does raise this possibility. Although the controversy regarding medical and/or surgical closure of PDA can be settled only by appropriately designed and powered random-ized studies, the finding of an increased mortality in patients with a persistent PDA in this study provides additional information and can be of help in the design of future prospective clinical trials.
REFERENCES
1. Van Overmeire B. Patent ductus arteriosus: how aggressive should we be?Neonatology.2007;91(4):318
2. Rojas MA, Gonzalez A, Bancalari E, Claure N, Poole C, Silva-Neto G. Changing trends in the epidemiology and pathogenesis of neonatal chronic lung disease. J Pediatr. 1995;126(4): 605– 610
FIGURE 2
3. Marshall DD, Kotelchuck M, Young TE, Bose CL, Kruyer L, O’Shea TM. Risk factors for chronic lung disease in the surfac-tant era: a North Carolina population-based study of very low birth weight infants. North Carolina Neonatologists Associa-tion.Pediatrics.1999;104(6):1345–1350
4. Oh W, Poindexter BB, Perritt R, Lemons JA, Bauer CR, Ehren-kranz RA, Stoll BJ, Poole K, Wright LL; Neonatal Research Network. Association between fluid intake and weight loss during the first ten days of life and risk of bronchopulmonary dysplasia in extremely low birth weight infants.J Pediatr.2005; 147(6):786 –790
5. Dykes FD, Lazzara A, Ahmann P, Blumenstein B, Schwartz J, Brann AW. Intraventricular hemorrhage: a prospective evalu-ation of etiopathogenesis.Pediatrics.1980;66(1):42– 49 6. Evans N, Kluckow M. Early ductal shunting and
intraventric-ular haemorrhage in ventilated preterm infants.Arch Dis Child Fetal Neonatal Ed.1996;75(3):F183–F186
7. Ryder RW, Shelton JD, Guinan ME. Necrotizing enterocolitis: a prospective multicenter investigation. Am J Epidemiol. 1980; 112(1):113–123
8. Cassady G, Crouse DT, Kirklin JW, et al. A randomized, con-trolled trial of very early prophylactic ligation of the ductus arteriosus in babies who weighed 1000 g or less at birth.N Engl J Med.1989;320(23):1511–1516
9. Dollberg S, Lusky A, Reichman B. Patent ductus arteriosus, indomethacin and necrotizing enterocolitis in very low birth weight infants: a population-based study.J Pediatr Gastroenterol Nutr.2005;40(2):184 –188
10. Clyman RI. Mechanisms regulating the ductus arteriosus.Biol Neonate.2006;89(4):330 –335
11. Bancalari E, Claure N, Gonzalez A. Patent ductus arteriosus and respiratory outcome in premature infants.Biol Neonate.
2005;88(3):192–201
12. Laughon MM, Simmons MA, Bose CL. Patency of the ductus arteriosus in the premature infant: is it pathologic? Should it be treated?Curr Opin Pediatr.2004;16(2):146 –151
13. Bose CL, Laughon MM. Patent ductus arteriosus: lack of evi-dence for common treatments.Arch Dis Child Fetal Neonatal Ed.
2007;92(6):F498 –F502
14. Knight DB, Laughon MM. Evidence for active closure of patent ductus arteriosus in very preterm infants. J Pediatr. 2008; 152(3):446 – 447
15. Clyman RI, Chorne N. Patent ductus arteriosus: evidence for and against treatment.J Pediatr.2007;150(3):216 –219 16. Herrera C, Holberton J, Davis P. Prolonged versus short course
of indomethacin for the treatment of patent ductus arteriosus in preterm infants. Cochrane Database Syst Rev. 2007;(2): CD003480
17. Schmidt B, Roberts RS, Fanaroff A, Davis P, Kirpalani HM, Nwaesei C, Vincer M; TIPP Investigators. Indomethacin pro-phylaxis, patent ductus arteriosus, and the risk of bronchopul-monary dysplasia: further analyses from the Trial of Indometh-acin Prophylaxis in Preterms (TIPP). J Pediatr.2006;148(6): 730 –734
18. Attridge JT, Clark R, Walker MW, Gordon PV. New insights
into spontaneous intestinal perforation using a national data set: (1) SIP is associated with early indomethacin exposure.J Perinatol.2006;26(2):93–99
19. International Neonatal Network. The CRIB (clinical risk index for babies) score: a tool for assessing initial neonatal risk and comparing performance of neonatal intensive care units. Lan-cet.1993;342(8865):193–198
20. Sarquis AL, Miyaki M, Cat MN. The use of CRIB score for predicting neonatal mortality risk [in Portuguese].J Pediatr (Rio J).2002;78(3):225–229
21. Kluckow M, Evans N. Ductal shunting, high pulmonary blood flow, and pulmonary hemorrhage. J Pediatr. 2000;137(1): 68 –72
22. Alpan G, Scheerer R, Bland R, Clyman R. Patent ductus arte-riosus increases lung fluid filtration in preterm lambs.Pediatr Res.1991;30(6):616 – 621
23. McCurnin D, Seidner S, Chang LY, et al. Ibuprofen-induced patent ductus arteriosus closure: physiologic, histologic, and biochemical effects on the premature lung. Pediatrics. 2008; 121(5):945–956
24. Clyman RI, Mauray F, Heymann MA, Roman C. Cardiovascu-lar effects of patent ductus arteriosus in preterm lambs with respiratory distress.J Pediatr.1987;111(4):579 –587
25. Kluckow M, Evans N. Low superior vena cava flow and intra-ventricular haemorrhage in preterm infants.Arch Dis Child Fetal Neonatal Ed.2000;82(3):F188 –F194
26. Lemmers PM, Toet MC, van Bel F. Impact of patent ductus arteriosus and subsequent therapy with indomethacin on ce-rebral oxygenation in preterm infants.Pediatrics.2008;121(1): 142–147
27. Moin F, Kennedy KA, Moya FR. Risk factors predicting vaso-pressor use after patent ductus arteriosus ligation.Am J Peri-natol.2003;20(6):313–320
28. Noori S, Friedlich P, Seri I, Wong P. Changes in myocardial function and hemodynamics after ligation of the ductus arte-riosus in preterm infants.J Pediatr.2007;150(6):597– 602 29. Chorne N, Leonard C, Piecuch R, Clyman RI. Patent ductus
arteriosus and its treatment as risk factors for neonatal and neurodevelopmental morbidity. Pediatrics. 2007;119(6): 1165–1174
30. Kabra NS, Schmidt B, Roberts RS, Doyle LW, Papile L, Fanaroff A; Trial of Indomethacin Prophylaxis in Preterms Investigators. Neurosensory impairment after surgical closure of patent duc-tus arteriosus in extremely low birth weight infants: results from the Trial of Indomethacin Prophylaxis in Preterms.J Pe-diatr.2007;150(3):229 –234
31. Brooks JM, Travadi JN, Patole SK, Doherty DA, Simmer K. Is surgical ligation of patent ductus arteriosus necessary? The Western Australian experience of conservative management.
Arch Dis Child Fetal Neonatal Ed.2005;90(3):F235–F239 32. Herrman K, Bose C, Lewis K, Laughon M. Spontaneous closure
DOI: 10.1542/peds.2008-2418
2009;123;e138
Pediatrics
Gottipati, Istvan Seri and Kris Sekar
Shahab Noori, Michael McCoy, Philippe Friedlich, Brianna Bright, Venugopal
Preterm Infants
Failure of Ductus Arteriosus Closure Is Associated With Increased Mortality in
Services
Updated Information &
http://pediatrics.aappublications.org/content/123/1/e138
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/123/1/e138#BIBL
This article cites 30 articles, 9 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2008-2418
2009;123;e138
Pediatrics
Gottipati, Istvan Seri and Kris Sekar
Shahab Noori, Michael McCoy, Philippe Friedlich, Brianna Bright, Venugopal
Preterm Infants
Failure of Ductus Arteriosus Closure Is Associated With Increased Mortality in
http://pediatrics.aappublications.org/content/123/1/e138
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.