Gastrointestinal Tract
Raman Sreedharan, MD*, and Devendra I. Mehta, MD‡
ABSTRACT. The developing gastrointestinal tract from conception to adolescence is in constant direct in-teraction with an increasingly complex environment. This sets up the potential for unrecognized acute as well as chronic disorders, some of which may be difficult to pinpoint in a developing infant and child, given the wide variations that exist. It is startling to note how early some environmental toxins can come into contact with the developing human, where vulnerability may be height-ened and maturation of detoxifying pathways may be incomplete. Although the complex process of recogniz-ing, detoxifyrecogniz-ing, and avoiding the toxic substance by the body has presumably evolved over a substantial period of time, in this rapidly changing world, the array of novel toxins that make their way into the gastrointestinal tract is increasing. There remain many gaps in understanding the effects of environmental toxins on all of the devel-opmental stages from conception to adolescence. Al-though threshold levels have typically been derived from adult or animal data, factors such as size, relative differ-ences in consumption in proportion to size especially in infancy, and variable physiologic maturation of meta-bolic pathways are not well understood. The vulnerabil-ity may be further accentuated by physical factors that alter with maturity, such as permeability and critical times during organogenesis or organ maturation. Also of concern is how little is known about low-dose, long-term exposure, as well as any interplay with common ill-nesses. This article focuses on environmental toxins that have been shown to have toxic effects on the gastrointes-tinal tract. Pediatrics 2004;113:1044 –1050; development, intestinal mucosa, toxins.
ABBREVIATIONS. GI, gastrointestinal; CYP, cytochrome P450.
T
he gastrointestinal (GI) tract, like the skin and
the respiratory system, is in constant direct
interaction with the environment. The
func-tions of the GI tract as a protective barrier are as
important as its functions of digestion and
absorp-tion but vary with age and maturity. The large
sur-face area and prolonged exposure time increase risk
of toxin-mediated damage, and increased
permeabil-ity in early infancy may augment this further.
Com-plex processes of recognizing, detoxifying, and
avoiding toxic substances also undergo physiologic
maturation. In addition to recognized environmental
toxic agents, in this rapidly changing world, the
ar-ray of novel toxins that make their way into the GI
tract poses significant threats and needs to be better
understood.
ROUTES OF ENTRY
Environmental toxins taken orally may be
modi-fied in the GI tract by gastric pH, digestive enzymes,
or even bacteria that live in the intestines.
Environ-mental toxins that are internalized by skin
absorp-tion or by inhalaabsorp-tion may be secreted into the lumen
through the biliary system and lead to toxicity. Also,
toxins suspended in air make their way into the
intestinal tract by drainage from the sinuses into the
pharynx and esophagus.
Mucosal Factors
A thin preepithelial water layer (“unstirred water
layer”) and a mucous layer cover the intestinal
mu-cosa and limit absorption to toxins that can diffuse.
Lipid solubility will increase the absorption, as will
smaller particle size. The intestinal luminal pH plays
a role by altering the ionization of molecules so that
nonionized forms of the weak bases and acids are
absorbed more rapidly than the ionized forms. The
mucous binding and absorption of metals such as
cobalt, zinc, lead, and iron are pH dependent.
The rapid turnover of the intestinal mucosa helps
to protect the mucosa and the body against toxic
injuries. The regenerative capacity after injury and
damage are remarkable because of the mucosa’s
ca-pacity for rapid turnover and has been studied
ex-tensively with the dog ileum after interruption of
blood supply. The lower two thirds of the crypts
form the proliferative compartment of the mucosa
and, because of their location, are protected from the
reach of toxic substances. This could explain the low
incidence of small intestinal carcinoma despite its
large area. The presence of cytotoxic substances
stim-ulates exfoliation of the cells into the lumen. Also,
studies have demonstrated that during the periods of
cytotoxic exposure, glucose absorption and enzyme
activities are decreased.
Detoxification
The detoxification mechanism that exists in the
intestinal mucosa serves as a second-line barrier and
has been studied well in animal models and also to
an extent in humans. Regional differences are also
From the *Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania; and ‡Nemours Children’s Clinic, Wilmington, Alfred I. duPont Hospital for Children, Wilmington, Delaware.
Received for publication Oct 7, 2003; accepted Oct 20, 2003.
Reprint requests to (D.I.M.) Division of Gastroenterology, NCC-Wilming-ton, Alfred I. duPont Hospital for Children, Box 269, WilmingNCC-Wilming-ton, DE 19899. E-mail: [email protected]
noted, with most enzymes diminishing in expression
in distal small bowel. Studies conducted in rat small
intestines have shown that cytochrome P450 (CYP),
NADPH-CYP reductase, p-nitroansole
o-demethyl-ase, and benzpyrene hydroxylase activities are
ex-pressed 3 to 10 times more in the upper villous cells
of the proximal small bowel.
1This may represent an
evolutionary adaptation as the highest
concentra-tions of environmental toxins are presented to the
upper small bowel.
Pharmacokinetic differences may play a part in the
age-related differences in the incidence of adverse
effects of environmental toxins. Phase I reactions
depend predominantly on CYP enzymes,
particu-larly as most drugs are lipophilic. Specific CYP
en-zymes are developmentally regulated and affect
pro-duction of metabolites, including possibly toxic ones,
as well as efficacy of drug therapy. Thus, CYP2D6
activity is
⬍1% of the adult level and remains low
until after 28 days of age. Drugs that use these
path-ways, such as

-blockers and tricyclic
antidepres-sants, could result in toxicity, including
anticholin-ergic gastrointestinal side effects.
2Conversely,
CYP3A, used to metabolize a large number of drugs,
is present in significant amounts in the fetal liver.
Extraintestinal CYP3A may be the most important
enzyme for orally administered drugs, although the
ontogeny has not been evaluated.
3Indeed, the
activ-ity of these enzymes is greater in infants and children
compared with adolescents and adults. In children,
CYP-catalyzed metabolism is increased, and uridine
diphosphate-glucuronosyltransferase– catalyzed
me-tabolism is not significantly different from that in
adults.
4Phase II enzymes also show developmental
regu-lation that affect drug metabolism. N acetyl
trans-ferase 2 activity is low in infants and children
younger than 3 years, essentially making them
phe-notypically resemble slow metabolizers. By
extrapo-lation, slow metabolizers are at greater risk of
toxic-ity, including toxic epidermal necrolysis and
Stevens-Johnson syndrome.
5In contrast, higher red
blood cell thiopurine methyltransferase activity
ob-served in newborn infants may have therapeutic
im-plications in terms of levels of azathioprine and
6-mercaptopurine and hence efficacy and toxicity,
but no data to date indicate how long this higher
activity is maintained.
6In general, pharmacokinetic
studies in infants and children have been used to
provide inferential information on the impact of
de-velopment on the activity of drug-metabolizing
en-zymes. Because different pathways often metabolize
these drugs, the information obtained provides only
an overview. In some cases, these enzyme systems
may instead activate toxins, such as carbon
tetrachlo-ride, which then dissociates into toxic free radicals in
the lumen. Finally, the different processes involved
in absorption, such as diffusion, nonionic diffusion,
facilitated diffusion, specific active transport, and
toxins, might usurp solvent drag, and mechanisms to
counter these with respect to a particular toxin may
be useful therapeutically.
DIFFERENTIAL VULNERABILITIES AND CRITICAL WINDOWS OF EXPOSURE OF THE GI TRACT:
FROM CONCEPTION TO ADOLESCENCE
Antenatal
Maternal diet is the major factor governing
expo-sure at conception and in utero. The rapidly growing
fetus is susceptible, but the placenta acts as barrier.
Although transplacental transport of environmental
toxins, such as lead and mercury, is recognized,
tox-ins in amniotic fluid, such as nicotine and cotinin,
have been poorly studied for possible absorption by
either the skin or the GI tract.
7Specific GI effects of
maternal smoking are cleft lip and palate and
post-natal growth retardation.
Postnatal Changes
The postnatal maturing GI tract undergoes several
changes that may significantly alter risk of toxicity
(Table 1). Changes in vulnerability to toxins as a
result of many of these factors have largely been
studied only in animal models and may not be
ap-plicable. Mucosal permeability to macromolecules
diminishes in the first few days of life in humans but
diminishes much later in animals. In addition,
influ-ence of GI disease, more common in infancy and
early childhood, may alter absorption by changes in
motility, mucosal integrity, or surface area. Lead
(Table 2) and cadmium absorption is markedly
in-creased in early childhood. Absorption of both
met-als increases in iron deficiency states as the number
of carriers shared by all 3 metals increases in the
duodenum.
8Low gastric acid production in infants may lead to
increased small bowel bacterial overgrowth.
Methe-moglobinemia in infants may have resulted from
conversion of nitrate from contaminated well water
to nitrite.
9The disposition of drugs and other environmental
toxins varies at different stages of child
develop-ment. Generally, absorption is slower in younger
children. The extracellular volume is higher, and the
extent of protein binding is lower. Renal excretion is
lower, and environmental toxin metabolic pathways
that depend on glucuronidation activity in the liver
may increase concentration of toxins. Animal studies
show diminished or absent hydrolase, reductase, or
demethylase activity at birth in the rabbit and lack of
uridine diphosphate– glucuronyl transferase in the
guinea pig but not in the rabbit.
10Interspecies
differ-ences highlight the dangers of extrapolation to
hu-mans.
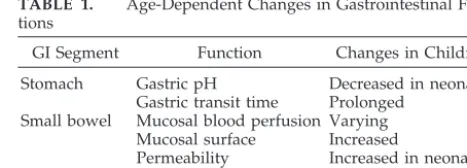
TABLE 1. Age-Dependent Changes in Gastrointestinal Func-tions
GI Segment Function Changes in Children
Stomach Gastric pH Decreased in neonates Gastric transit time Prolonged
Small bowel Mucosal blood perfusion Varying Mucosal surface Increased
Permeability Increased in neonates Intestinal flora Digestion/nutrients Increased
Pancreas Digestive enzymes Decreased in infancy
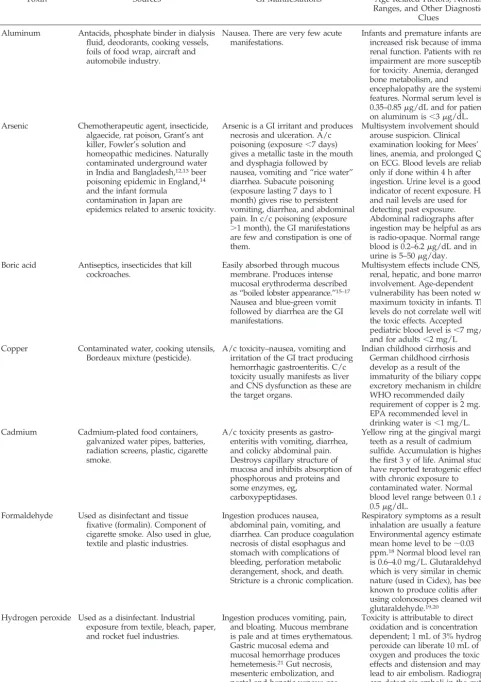
TABLE 2. Some Specific Environmental Toxins
Toxin Sources GI Manifestations Age-Related Factors, Normal
Ranges, and Other Diagnostic Clues
Aluminum Antacids, phosphate binder in dialysis fluid, deodorants, cooking vessels, foils of food wrap, aircraft and automobile industry.
Nausea. There are very few acute manifestations.
Infants and premature infants are at increased risk because of immature renal function. Patients with renal impairment are more susceptible for toxicity. Anemia, deranged bone metabolism, and
encephalopathy are the systemic features. Normal serum level is 0.35–0.85g/dL and for patients on aluminum is⬍3g/dL. Arsenic Chemotherapeutic agent, insecticide,
algaecide, rat poison, Grant’s ant killer, Fowler’s solution and homeopathic medicines. Naturally contaminated underground water in India and Bangladesh,12,13beer poisoning epidemic in England,14 and the infant formula
contamination in Japan are epidemics related to arsenic toxicity.
Arsenic is a GI irritant and produces necrosis and ulceration. A/c poisoning (exposure⬍7 days) gives a metallic taste in the mouth and dysphagia followed by nausea, vomiting and “rice water” diarrhea. Subacute poisoning (exposure lasting 7 days to 1 month) gives rise to persistent vomiting, diarrhea, and abdominal pain. In c/c poisoning (exposure
⬎1 month), the GI manifestations are few and constipation is one of them.
Multisystem involvement should arouse suspicion. Clinical examination looking for Mees’ lines, anemia, and prolonged QTc on ECG. Blood levels are reliable only if done within 4 h after ingestion. Urine level is a good indicator of recent exposure. Hair and nail levels are used for detecting past exposure. Abdominal radiographs after ingestion may be helpful as arsenic is radio-opaque. Normal range in blood is 0.2–6.2g/dL and in urine is 5–50g/day. Boric acid Antiseptics, insecticides that kill
cockroaches.
Easily absorbed through mucous membrane. Produces intense mucosal erythroderma described as “boiled lobster appearance.”15–17 Nausea and blue-green vomit followed by diarrhea are the GI manifestations.
Multisystem effects include CNS, renal, hepatic, and bone marrow involvement. Age-dependent vulnerability has been noted with maximum toxicity in infants. The levels do not correlate well with the toxic effects. Accepted pediatric blood level is⬍7 mg/dL and for adults⬍2 mg/L
Copper Contaminated water, cooking utensils, Bordeaux mixture (pesticide).
A/c toxicity–nausea, vomiting and irritation of the GI tract producing hemorrhagic gastroenteritis. C/c toxicity usually manifests as liver and CNS dysfunction as these are the target organs.
Indian childhood cirrhosis and German childhood cirrhosis develop as a result of the immaturity of the biliary copper excretory mechanism in children. WHO recommended daily requirement of copper is 2 mg. EPA recommended level in drinking water is⬍1 mg/L. Cadmium Cadmium-plated food containers,
galvanized water pipes, batteries, radiation screens, plastic, cigarette smoke.
A/c toxicity presents as gastro-enteritis with vomiting, diarrhea, and colicky abdominal pain. Destroys capillary structure of mucosa and inhibits absorption of phosphorous and proteins and some enzymes, eg,
carboxypeptidases.
Yellow ring at the gingival margin of teeth as a result of cadmium sulfide. Accumulation is highest in the first 3 y of life. Animal studies have reported teratogenic effect with chronic exposure to contaminated water. Normal blood level range between 0.1 and 0.5g/dL.
Formaldehyde Used as disinfectant and tissue fixative (formalin). Component of cigarette smoke. Also used in glue, textile and plastic industries.
Ingestion produces nausea, abdominal pain, vomiting, and diarrhea. Can produce coagulation necrosis of distal esophagus and stomach with complications of bleeding, perforation metabolic derangement, shock, and death. Stricture is a chronic complication.
Respiratory symptoms as a result of inhalation are usually a feature. Environmental agency estimates mean home level to be⬃0.03 ppm.18Normal blood level range is 0.6–4.0 mg/L. Glutaraldehyde, which is very similar in chemical nature (used in Cidex), has been known to produce colitis after using colonoscopes cleaned with glutaraldehyde.19,20
Hydrogen peroxide Used as a disinfectant. Industrial exposure from textile, bleach, paper, and rocket fuel industries.
Ingestion produces vomiting, pain, and bloating. Mucous membrane is pale and at times erythematous. Gastric mucosal edema and mucosal hemorrhage produces hemetemesis.21Gut necrosis, mesenteric embolization, and portal and hepatic venous gas have been reported.22, 23
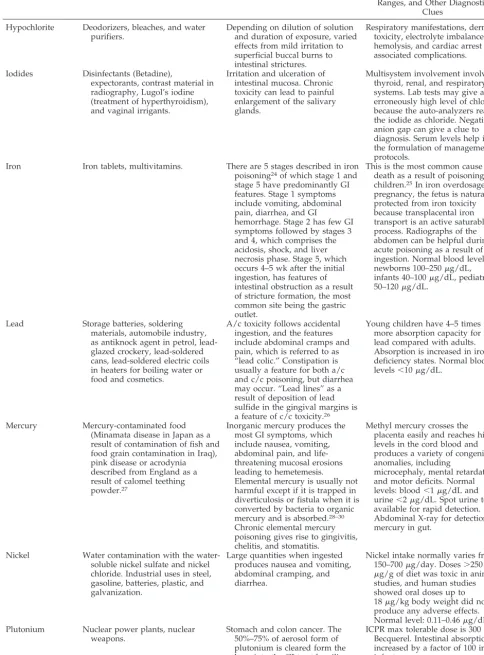
TABLE 2. Continued
Toxin Sources GI Manifestations Age-Related Factors, Normal
Ranges, and Other Diagnostic Clues
Hypochlorite Deodorizers, bleaches, and water purifiers.
Depending on dilution of solution and duration of exposure, varied effects from mild irritation to superficial buccal burns to intestinal strictures.
Respiratory manifestations, dermal toxicity, electrolyte imbalances, hemolysis, and cardiac arrest are associated complications.
Iodides Disinfectants (Betadine),
expectorants, contrast material in radiography, Lugol’s iodine (treatment of hyperthyroidism), and vaginal irrigants.
Irritation and ulceration of intestinal mucosa. Chronic toxicity can lead to painful enlargement of the salivary glands.
Multisystem involvement involving thyroid, renal, and respiratory systems. Lab tests may give an erroneously high level of chloride because the auto-analyzers read the iodide as chloride. Negative anion gap can give a clue to diagnosis. Serum levels help in the formulation of management protocols.
Iron Iron tablets, multivitamins. There are 5 stages described in iron poisoning24of which stage 1 and stage 5 have predominantly GI features. Stage 1 symptoms include vomiting, abdominal pain, diarrhea, and GI
hemorrhage. Stage 2 has few GI symptoms followed by stages 3 and 4, which comprises the acidosis, shock, and liver necrosis phase. Stage 5, which occurs 4–5 wk after the initial ingestion, has features of intestinal obstruction as a result of stricture formation, the most common site being the gastric outlet.
This is the most common cause of death as a result of poisoning in children.25In iron overdosage in pregnancy, the fetus is naturally protected from iron toxicity because transplacental iron transport is an active saturable process. Radiographs of the abdomen can be helpful during acute poisoning as a result of ingestion. Normal blood levels: newborns 100–250g/dL, infants 40–100g/dL, pediatric 50–120g/dL.
Lead Storage batteries, soldering materials, automobile industry, as antiknock agent in petrol, lead-glazed crockery, lead-soldered cans, lead-soldered electric coils in heaters for boiling water or food and cosmetics.
A/c toxicity follows accidental ingestion, and the features include abdominal cramps and pain, which is referred to as “lead colic.” Constipation is usually a feature for both a/c and c/c poisoning, but diarrhea may occur. “Lead lines” as a result of deposition of lead sulfide in the gingival margins is a feature of c/c toxicity.26
Young children have 4–5 times more absorption capacity for lead compared with adults. Absorption is increased in iron deficiency states. Normal blood levels⬍10g/dL.
Mercury Mercury-contaminated food (Minamata disease in Japan as a result of contamination of fish and food grain contamination in Iraq), pink disease or acrodynia described from England as a result of calomel teething powder.27
Inorganic mercury produces the most GI symptoms, which include nausea, vomiting, abdominal pain, and life-threatening mucosal erosions leading to hemetemesis. Elemental mercury is usually not harmful except if it is trapped in diverticulosis or fistula when it is converted by bacteria to organic mercury and is absorbed.28–30 Chronic elemental mercury poisoning gives rise to gingivitis, chelitis, and stomatitis.
Methyl mercury crosses the placenta easily and reaches high levels in the cord blood and produces a variety of congenital anomalies, including
microcephaly, mental retardation, and motor deficits. Normal levels: blood⬍1g/dL and urine⬍2g/dL. Spot urine tests available for rapid detection. Abdominal X-ray for detection of mercury in gut.
Nickel Water contamination with the water-soluble nickel sulfate and nickel chloride. Industrial uses in steel, gasoline, batteries, plastic, and galvanization.
Large quantities when ingested produces nausea and vomiting, abdominal cramping, and diarrhea.
Nickel intake normally varies from 150–700g/day. Doses⬎250
g/g of diet was toxic in animal studies, and human studies showed oral doses up to 18g/kg body weight did not produce any adverse effects. Normal level: 0.11–0.46g/dL. Plutonium Nuclear power plants, nuclear
weapons.
Stomach and colon cancer. The 50%–75% of aerosol form of plutonium is cleared form the lung into the GI tract by ciliary movement.
Infancy
Maternal diet remains an important source of
en-vironmental toxins in breastfed infants. Many
envi-ronmental toxins, including halogenated pesticides
such as polychlorinated biphenyls and dioxins, may
be concentrated significantly in the milk fat. Because
milk is typically the main diet, constant exposure
over several months may occur. Currently, however,
there is no evidence that these concentrations reach
thresholds that are harmful, and breast milk is still
recommended by the American Academy of
Pediat-rics as the best choice. Milk formulas from cow milk
may be less concentrated, especially as the fat source
is nondairy. However, possible risks of other
con-taminants such as antibiotics warrant additional
study, as the amounts ingested are large over a
sus-tained period of months.
Childhood
Several environmental factors affect exposure to
toxins in childhood. Household powders and liquids
may be ingested and lead to caustic esophageal
in-juries. These injuries markedly increase the risk of
esophageal cancer in later life.
11Toxic plants, such as
Dieffenbachia
, including mother-in-law’s tongue and
berries such as holly berries (Table 3), can lead to
severe oral and GI disturbances and are most
com-mon in childhood. Schools, child care facilities, and
playgrounds expose children to a wide array of
en-vironmental toxins ranging from lead to herbicides,
heavy metals, and pesticides. Outdoor play areas
such as wooden playground equipment may be a
source of arsenic or chromium if ingested.
A child’s diet is typically less varied than in
ado-lescents or adults but may contain proportionally
more fruits and vegetables. This exposes them to
greater amounts of pesticides. Common childhood
disorders, such as constipation, may significantly
in-crease toxin absorption because of delayed transit
time.
The environmental toxin metabolic pathways
con-tinue to change, as exemplified by peak theophylline
metabolism occurring at this age and leading to
dif-ferent urinary metabolite levels than in infancy.
Adolescence
Risk-taking behaviors such as smoking, ingestion
of intoxicants, or part-time manual jobs affect
expo-sure to environmental toxins. Smoking is a risk factor
for peptic ulcer disease. Hormonal changes lead to
growth and differentiation of tissues, making these
more vulnerable to toxins. A change in the metabolic
rate of environmental toxins pathways occurs,
lead-ing to reduced CYP expression, and theophylline
metabolism decreases to adult levels.
Specific Environmental Toxins
Minor GI symptoms are common in many toxic
exposures, although other organs may be more
in-volved. In Table 2, environmental toxins for which
GI symptoms either are common or may be the major
presenting signs are listed. Age-specific features are
noted. In Table 3, some biological toxins for which GI
symptoms predominate are listed.
CHILDHOOD GI DISORDERS FOR WHICH ENVIRONMENTAL TOXINS MAY BE CONSIDERED
Acute exposures may lead to nausea, vomiting,
and diarrhea and may be difficult to identify, as
infectious causes are more common. However,
addi-tional features, such as excessive drowsiness,
involv-ing other organs should raise suspicion. Ginvolv-ingivitis,
edema, and erythema of oral mucosa; dysphagia;
and GI hemorrhage also may suggest environmental
toxin exposure, especially heavy metals. Copper,
pokeweed, and toxalbumins may lead to bloody
di-arrhea, mimicking acute colitis. Indeed, in
inflamma-tory bowel disease, environmental toxins such as
ultrafine particles of titanium oxide have been
pos-tulated as causes.
46CONCLUSION
Changes in diet and exposure to environmental
toxins vary tremendously with age. Developmental
stages of protective mechanisms such as mucosal
permeability also lead to age-specific risks. Although
many gaps in understanding effects of
environmen-tal toxins on all of the developmenenvironmen-tal stages from
conception to adolescence remain, it is clear that the
TABLE 2. Continued
Toxin Sources GI Manifestations Age-Related Factors, Normal
Ranges, and Other Diagnostic Clues
Thallium Rhodenticide, pesticide, semiconductor industry, pyrotechny, thermometer industry, cardiac scanning.
Nausea, vomiting, and diarrhea. Paralytic ileus, duodenitis, and constipation have been reported. Parotid gland, pancreas, and liver involvement also are documented.
Symptoms are dose related. Neurologic manifestations are the hallmark of the disease. Also dermatologic manifestations and sudden cardiac death as a result of autonomic disturbances can occur as late manifestations. Normal blood range: 0.5g/dL. Tin Food stored in tin containers,
antiseptics, fungicides, insecticide, and molluscacide. Occupational exposure in polyvinyl chloride, silicon, and polyurethane industries.
Inorganic form of tin: a/c toxicity is rare and c/c toxicity is unknown. Organic form of tin: pancreatic and liver dysfunction.
Toxic effects with food containing
⬎1400 ppm of tin. Age-dependent vulnerabilities have not been studied.
various age groups need to be considered separately.
The GI tract, despite being an important
detoxifica-tion site, is also vulnerable because of its specific
features that allow optimal digestion and absorption.
The vulnerability is further accentuated by
develop-mental factors such as permeability and the critical
timing for many target organs. Low dose, long-term
exposure and high-dose, short-term exposure both
need to be studied, and the impact of common
ill-nesses on toxicity needs to be evaluated.
Further-more, although safe threshold levels have been
de-rived from adult or animal data, factors such as size,
relative differences in consumption, and different
maturity of metabolic pathways suggest that these
could be misleading. Little is known about specific
changes and risks during adolescence, and caution
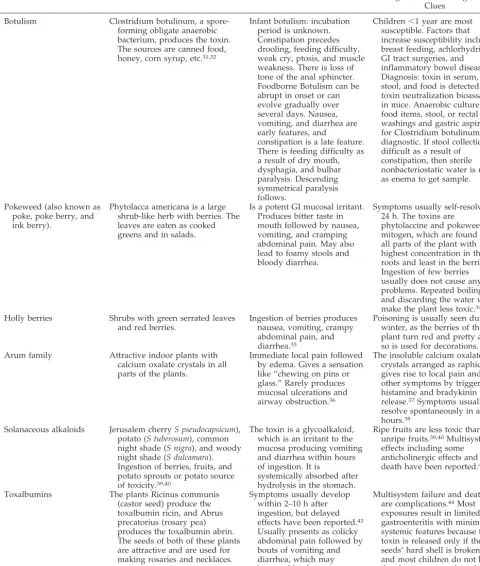
TABLE 3. Some Specific Biological Toxins
Toxin Sources GI Manifestations Age-Related Factors, Normal
Ranges, and Othe Diagnostic Clues
Botulism Clostridium botulinum, a spore-forming obligate anaerobic bacterium, produces the toxin. The sources are canned food, honey, corn syrup, etc.31,32
Infant botulism: incubation period is unknown. Constipation precedes drooling, feeding difficulty, weak cry, ptosis, and muscle weakness. There is loss of tone of the anal sphincter. Foodborne Botulism can be abrupt in onset or can evolve gradually over several days. Nausea, vomiting, and diarrhea are early features, and
constipation is a late feature. There is feeding difficulty as a result of dry mouth, dysphagia, and bulbar paralysis. Descending symmetrical paralysis follows.
Children⬍1 year are most susceptible. Factors that increase susceptibility include breast feeding, achlorhydria, GI tract surgeries, and inflammatory bowel disease. Diagnosis: toxin in serum, stool, and food is detected by toxin neutralization bioassay in mice. Anaerobic culture of food items, stool, or rectal washings and gastric aspirate for Clostridium botulinum is diagnostic. If stool collection is difficult as a result of
constipation, then sterile nonbacteriostatic water is used as enema to get sample.
Pokeweed (also known as poke, poke berry, and ink berry).
Phytolacca americana is a large shrub-like herb with berries. The leaves are eaten as cooked greens and in salads.
Is a potent GI mucosal irritant. Produces bitter taste in mouth followed by nausea, vomiting, and cramping abdominal pain. May also lead to foamy stools and bloody diarrhea.
Symptoms usually self-resolve in 24 h. The toxins are
phytolaccine and pokeweed mitogen, which are found in all parts of the plant with the highest concentration in the roots and least in the berries.33 Ingestion of few berries usually does not cause any problems. Repeated boiling and discarding the water will make the plant less toxic.34 Holly berries Shrubs with green serrated leaves
and red berries.
Ingestion of berries produces nausea, vomiting, crampy abdominal pain, and diarrhea.35
Poisoning is usually seen during winter, as the berries of this plant turn red and pretty and so is used for decorations. Arum family Attractive indoor plants with
calcium oxalate crystals in all parts of the plants.
Immediate local pain followed by edema. Gives a sensation like “chewing on pins or glass.” Rarely produces mucosal ulcerations and airway obstruction.36
The insoluble calcium oxalate crystals arranged as raphide gives rise to local pain and other symptoms by triggering histamine and bradykinin release.37Symptoms usually resolve spontaneously in a few hours.38
Solanaceous alkaloids Jerusalem cherryS pseudocapsicum), potato (S tuberosum), common night shade (S nigra), and woody night shade (S dulcamara). Ingestion of berries, fruits, and potato sprouts or potato source of toxicity.39,40
The toxin is a glycoalkaloid, which is an irritant to the mucosa producing vomiting and diarrhea within hours of ingestion. It is
systemically absorbed after hydrolysis in the stomach.
Ripe fruits are less toxic than unripe fruits.39,40Multisystem effects including some anticholinergic effects and death have been reported.40–42
Toxalbumins The plants Ricinus communis (castor seed) produce the toxalbumin ricin, and Abrus precatorius (rosary pea) produces the toxalbumin abrin. The seeds of both of these plants are attractive and are used for making rosaries and necklaces.
Symptoms usually develop within 2–10 h after ingestion, but delayed effects have been reported.43 Usually presents as colicky abdominal pain followed by bouts of vomiting and diarrhea, which may become bloody.
should be used when applying adult-based
thresh-old values.
REFERENCES
1. Hoensch H, Woo CH, Raffin SB, Schmid R. Oxidative metabolism of foreign compounds in rat small intestine: cellular localization and de-pendence on dietary iron.Gastroenterology. 1976;70:1063–1070 2. Nemeroff CB, DeVane CL, Pollock BG. Newer antidepressants and the
cytochrome P450 system.Am J Psychiatry. 1996;153:311–320
3. Paine MF, Shen DD, Kunze KL, et al. First-pass metabolism of midazo-lam by the human intestine.Clin Pharmacol Ther. 1996;60:14 –24 4. Anderson GD. Children versus adults: pharmacokinetic and
adverse-effect differences.Epilepsia.2002;43(suppl 3):53–59
5. May DG. Genetic differences in drug disposition. J Clin Pharmacol. 1994;34:881– 897
6. McLeod HL, Krynetski EY, Wilimas JA, Evans WE. Higher activity of polymorphic thiopurine S-methyltransferase in erythrocytes from neo-nates compared to adults.Pharmacogenetics. 1995;5:281–286
7. Van Vunakis H, Langone JJ, Milunsky A. Nicotine and cotinin in the amniotic fluid of smokers in the second trimester of pregnancy.Am J Obstet Gynecol. 1974;20:64 – 66
8. Schumann K, Elsenhans B, Richter E. Gastrointestinal tract. In: Mar-quardt H, Schafer SG, McClellan R, Welsch F, eds. Toxicology. San Diego, CA: Academic Press; 1999:573–585
9. Luyens JN. The legacy of well-water methemoglobinemia.JAMA. 1987; 257:2793–2795
10. Lucier GW, Sonawane BR, McDaniel OS. Glucuronidation and deglu-curonidation reactions in hepatic and extrahepatic tissues during peri-natal development.Drug Metab Dispos. 1977;5:279 –287
11. Appleqaist P, Salno M. Lye corrosion carcinoma of the esophagus: a review of 63 cases.Cancer. 1980;45:2655
12. Rahman M, Tondel M, Ahmed SA, Chowchury IA, Faruquee MH, Axelson O. Hypertension and arsenic exposure in Bangladesh. Hyper-tension. 1999;33:74 –78
13. Subramanian KS, Kosnett MJ. Human exposure to arsenic from con-sumption of well water in West Bengal, India.Int J Occup Environ Health. 1998;4:217–230
14. Keynack TN, Kirby W, et al. Arsenical poisoning from beer drinking.
Lancet.1900:1600 –1603
15. Wong LC, Heimbach, Trucott DR, Duncan BD. Boric acid poisoning: report of 11 cases.Can Med Assoc J. 1964;90:1018 –1023
16. Restuccio A, Mortensen ME, Kelly MT. Fatal ingestion of boric acid in an adult.Am J Emerg Med. 1992;10:545–547
17. Rubenstein AD, Mushner DM. Epidemic boric acid poisoning simulat-ing staphylococcal toxic epidermal necrolysis of the newborn infant: Ritters disease.J Pediatr.1970; 884 – 887
18. Imbus HR. Clinical evaluation of patients with complaints related to formaldehyde exposure.J Allergy Clin Immunol. 1985;76:831– 840 19. Durante L, Zulty JC, Israel E, et al. Investigation of an outbreak of
bloody diarrhea: association with endoscopic cleaning solution and demonstration of lesions in an animal model. Am J Med. 1992;92: 476 – 480
20. West AB, Kuan SF, Bennick M, Lagarde S. Glutaraldehyde colitis fol-lowing endoscopy: clinical and pathological features and investigation of an outbreak.Gastroenterology. 1995;108:1250 –1255
21. Giberson TP, Kern JD, Pettigrew DW 3rd, Eaves CC Jr, Haynes JF Jr.
Near fatal hydrogen peroxide ingestion. Ann Emerg Med. 1989;18: 778 –779
22. Luu TA, Kelley MT, Strauch JA, Avradopoulos K. Portal vein gas embolism from hydrogen peroxide ingestion.Ann Emerg Med. 1992;21: 1391–1393
23. Rackoff WR, Merton DF. Gas embolization after ingestion of hydrogen peroxide.Pediatrics. 1990;85:593–594
24. Banner W Jr, Tong TG. Iron poisoning.Pediatr Clin North Am.1986;33: 393– 409
25. Litovitz T, Manoguerra A. Comparison of pediatric poisoning hazards: an analysis of 38 million exposure incidents.Pediatrics. 1992;89:999 –1006 26. Bruggenkate CM, Lopes Cardozo E, Maaskant P, van der Waal I. Lead poisoning with pigmentation of the oral mucosa.Oral Surg. 1975;39: 747–753
27. Troen P, Kaufman SA, Katz KH. Mercuric bichloride poisoning.N Engl J Med.1951;244 –259
28. Canady R, Rabe CS, Gan K. Toxicological profile for mercury. Atlanta, GA: Department of Public Health Service; 1994:66 –259
29. Bredfeldt JE, Moeller DD. Systemic mercury intoxication following rupture of a Miller-Abbott tube.Am J Gastroenterol. 1978;69:478 – 480 30. Mayer O, Cantor MD. Mercury lost in the gastrointestinal tract.JAMA.
1951;146 –560
31. Spika JS, Shaffner N, Hargrett-Bean N, et al. Risk factors for infant botulism in the United States.Am J Dis Child. 1989;143:828 – 832 32. Kothare SV, Kassner EG. Infant botulism: a rare cause of colonic ileus.
Pediatr Radiol.1995;25:24 –26
33. Litovitz TL, Klein-Schwartz W, Dyer KS, et al. 1997 annual report of the American Association of Poison Control Centers Toxic Exposure Sur-veillance System.Am J Emerg Med. 1998;16:443– 497
34. Roberge R, Brader E, Martin ML, et al. The root of evil—pokeweed intoxication.Ann Emerg Med. 1986;15:470 – 473
35. Rodriques TD, Johnson PN, Jefferey LP. Holly berry ingestion: case report.Vet Hum Toxicol. 1984;26:157–180
36. Evans CRH. Oral ulceration after contact with the houseplant Dieffen-bachia.Br Dent J. 1987;162:467– 468
37. Rauber A. Observation on the idioblasts of Dieffenbachia.J Toxicol Clin Toxicol. 1985;23:79
38. Mrvos R, Dean BS, Krenzelok EP. Philodendron/Dieffenbachia ingestion: are they a problem?J Toxicol Clin Toxicol. 1991;29:485– 491 39. Dalvi RR. Toxicology of solanine: an overview.Vet Hum Toxicol. 1983;
25:13–15
40. Hornfeldt CS, Collins JE. Toxicity of nightshade berries (Solanum dul-camara) in mice.J Toxicol Clin Toxicol. 1990;28:185–192
41. McMillan M, Thompson JC. An outbreak of suspected solanine poison-ing in schoolboys.Q J Med. 1979;48:227–243
42. Nishie K, Gumbmann MR, Keyl AC. Pharmacology of solanine.Toxicol Appl Pharmacol. 1971;19:81–92
43. Schneider SM. Toxic plant ingestions: optimizing the course of treat-ment.Emerg Med Rep. 1992;13:141–142
44. Balint GA. Ricin: the toxic protein of castor oil seeds.Toxicology. 1974; 2:77–102
45. Challoner KR, McCarron MM. Castor bean intoxication.Ann Emerg Med. 1990;19:1177–1183