Students’ Acquisition and Use of School Condoms in a High School
Condom Availability Program
Mark A. Schuster, MD, PhD*‡; Robert M. Bell, PhD*; Sandra H. Berry, MA*; and David E. Kanouse, PhD*
ABSTRACT. Objectives. To determine what students know about a condom availability program in their high school, how they react to the program, whether they obtain condoms from it, and what they do with these condoms.
Design. Self-administered anonymous survey con-ducted 1 year after the program began.
Setting. An urban California school district.
Participants. A total of 1112 students, 9th through 12th grade, 59% of eligible students present on the survey day.
Main Outcome Measures. History of obtaining con-doms from the program, use of these concon-doms, knowl-edge about the program, and attitudes toward the pro-gram.
Results. Forty-eight percent of students had person-ally taken school condoms, and another 5% had gotten them from someone else, for a total of 53% who had obtained school condoms. Seventy percent of nonvirgins and 38% of virgins obtained condoms. Males were more likely than females to have obtained condoms (60% vs 45%). Fifty-four percent of students who had obtained school condoms had used them for sexual activity: 52% had used them for vaginal intercourse, 7% for anal inter-course, and 4% for fellatio. Students also explored school condoms without having sex, eg, removing them from the packet, putting them on fingers, or putting them on their penis or a partner’s penis. Thirty-four percent of students who had used a condom for vaginal intercourse during the previous year had obtained the condom they last used from school, with more males than females reporting the school as their source (41% vs 26%).
Eighty-eight percent of students knew that all students were allowed to obtain condoms, and 74% knew that parental permission was not required. Students generally supported the condom program: 88% thought the school should give out condoms, and 79% thought that if the school were to require parental permission for students to get condoms, students would get them less often than with the present system (which does not require permis-sion). Thirteen percent agreed and 71% disagreed that “having condoms available at school makes it harder for someone who doesn’t want to have sex to say no.”
Conclusions. Providing high school students with di-rect access to condoms leads to widespread use of school condoms, both for sexual activity and for exploratory activities that familiarize students with condoms.
Con-doms are of interest to both students who have and students who have not engaged in sexual activities for which condoms are recommended. Pediatrics 1997;100:
689 – 694;adolescents, condom availability programs, high school students, risk reduction, sexual behavior.
D
uring the past several years, school districts have been establishing condom availability programs to prevent the spread of human immunodeficiency virus and other sexually trans-mitted diseases and to reduce the number of unin-tended pregnancies among their students.In contrast to programs that provide various forms of contraception at school-based clinics, condom pro-grams provide only condoms and generally make them available at sites other than (or in addition to) clinics. The American Academy of Pediatrics,1 the American College of Obstetricians and Gynecolo-gists,2and the American School Health Association3 have stated that schools are an appropriate site for condom availability programs, and the American Academy of Pediatrics has called for research on the subject.1
As of June 1995, at least 37 school districts or individual schools in the United States had approved condom availability programs, and schools in at least 19 districts (but probably many more) were making condoms available through school-based health clin-ics. At least 55 other school districts had rejected condom programs.4
Condom availability programs differ in ways that can greatly influence how community members react to them and whether students use them. Some re-quire written parental permission to participate (ac-tive consent), some allow all students to participate unless parents sign a written refusal (passive con-sent), and others do not offer parents the option to refuse (no consent). Schools that require active or passive consent must authorize an adult (eg, teacher, school nurse) to check a list or card before giving out condoms. Schools without consent requirements have more flexibility. They can make condoms avail-able in unattended sites, let staff provide them with-out checking names, and sell them through vending machines. Some schools require staff to provide counseling to students who ask for condoms, and some institute formal educational programs.5
Because of the variety of approaches used in im-plementing condom availability programs, it is nec-essary to study different types of programs to gain a full appreciation of their potential impact. In partic-ular, it is important to study programs that do not
From *RAND, Santa Monica, California; and ‡the Department of Pediatrics, University of California at Los Angeles, Los Angeles, California. The opinions expressed are those of the authors and do not necessarily reflect the opinions of their institutional affiliations or the funding agencies. Received for publication Nov 15, 1996; accepted Mar 17, 1997.
Reprint requests to (M.A.S.) RAND, 1700 Main St, Box 2138, Santa Monica, CA 90407-2138.
restrict access to condoms so that we can gain an understanding of what the maximal impact is likely to be. A study that measured the number of condoms distributed per student in schools across the United States found that programs with easier access (eg, condoms available in bowls) distributed the largest number of condoms.6 Although there have been some preliminary studies of programs that require students to obtain condoms from staff7–9 and some studies of students’ attitudes toward condom pro-grams in schools without a program,10,11 we have found no published studies that have been con-ducted in programs with unrestricted access or that have reported data on multiple aspects of program impact.
We studied a high school condom program that makes male condoms available to all students; no parental consent is required, and no gatekeepers check identification cards or dispense condoms. In this article, we report on what students know about the condom program, how they react to it, and which students make use of it.
METHODS Program
The condom availability program is located in an urban high school that serves a racially and socioeconomically diverse com-munity in Los Angeles County.
The school district put together plastic packets containing two male condoms, an instruction sheet, and a card printed with the following message: “Condoms are not 100% effective in prevent-ing AIDS/HIV, sexually transmitted diseases or pregnancy durprevent-ing sexual intercourse. Abstinence is! Not all teenagers are sexually active. THINK BEFORE YOU ACT! The consequences may be for a lifetime.”
Packets were available in baskets in four classrooms and out-side the nurse’s office; some of these sites were accessible at times when other people generally would not be around. A sign asked students to leave a quarter for each packet in a can next to the basket of packets. During the first year of the program, between 1800 and 2000 packets were taken per school month and almost no money was collected.
The district had a 9th grade health curriculum that already covered sexual behaviors and risk prevention and an annual AIDS Awareness Week with assemblies and other educational pro-grams. No new educational programs were added.
Study Design
The program began in April 1992. The data for this article come from a survey of students in grades 9 through 12, conducted 1 year after the program was initiated.
Survey Content
This article covers knowledge, perceptions, and use of the condom availability program; history of sexual activities; and demographics. All terms and concepts used in the survey were part of the district’s 9th grade health curriculum.
Items covering attitudes and other nonbehavioral questions generally had Likert scale response alternatives. For the response alternatives that included “strongly agree,” “sort of agree,” “un-certain,” “sort of disagree,” and “strongly disagree,” we generally combined “strongly” and “sort of” when reporting results for “agree” and “disagree.” For a question on the potential impact of requiring parental permission to obtain school condoms, answer options included “more often,” “the same as before,” “less often,” and “uncertain.”
The survey covered history of various sexual activities during the previous year. It also covered lifetime history of vaginal inter-course (nonvirginity) but not lifetime history for other activities. For analytic purposes, we divide the students into virgins and
nonvirgins, but of course, virgins can engage in other sexual activities for which condoms are generally recommended.12
Administration and Survey Response Rates
Respondents completed the anonymous self-administered sur-vey during a regular class period and sealed it in an opaque envelope. Survey administrators unaffiliated with the school dis-trict proctored the classes. RAND’s Human Subjects Protection Committee approved consent and administration procedures.
Parents were required to sign a form providing permission for their children to participate (active consent), and this was ex-plained in letters and information sheets for parents and students. Respondents supplied oral assent, and the names of respondents completing the survey were not recorded. Respondents were in-structed to skip questions they preferred not to answer.
A group of parents contended that specific questions about students’ sexual activities were inappropriate and that the in-formed-consent process was inadequate. They sought a temporary restraining order against the survey. The controversy also prompted news media attention about the study. After hearing the case, the court ruled that the informed-consent and privacy pro-cedures offered appropriate protection for the rights of parents and students, and the survey was administered as planned.
Sample
Approximately 2500 students were enrolled in the school. Stu-dents in classes teaching English as a second language (;16% of the student body) and students in intensive special education classes were excluded from the study at the request of the princi-pal. An alternative school for;125 students considered at high risk for dropping out of school was not included in the evaluation. Fifteen percent of eligible students were absent. Of 1878 eligible students present, 1112 (59%) turned in usable surveys, 764 (41%) did not take the survey, and 2 turned in unusable surveys. Al-though the controversy undoubtedly influenced some parents’ and students’ decisions about participation, the magnitude of influence is not clear, given that comparable response rates have been reported for other school surveys on sensitive topics (pri-marily drug use behaviors) conducted with active consent.13–15
Weights
In addition to the 1-year follow-up survey covered by this article, we had conducted a survey just before the condom avail-ability program was introduced. The same eligibility criteria were used for both surveys; however, the consent procedures were different. For the baseline survey, parents received a letter from the school district informing them of the study and giving them the opportunity to sign a form withholding permission for their children to participate (passive consent). (This procedure was selected by the school district superintendent in consultation with the school board, because it was the standard approach to school surveys in the district. At follow-up, after discussions with parents who preferred active consent, the research team modified the consent procedures with approval from the superintendent.)
The baseline survey achieved a response rate of 98% of eligible students present on survey day. Therefore, we were able to use data from the two surveys to construct weights to adjust for the effects of selective participation resulting from the active consent procedures and local controversy. We developed analysis weights so that the weighted follow-up sample would represent the base-line sample in terms of several characteristics that should not have been affected by the program but may have been related to non-response at follow-up: gender, race/ethnicity, mother’s education, father’s education, grade, age relative to grade, educational expec-tations, self-reported grades, importance of religion in the respon-dent’s life, and presence of two parents in the household. Char-acteristics that could have been affected by the condom program (eg, sexual history) were not used for creating weights.
We used logistic regression to generate the weights. The sample consisted of all surveys collected at baseline or follow-up, the dependent variable identified the survey wave, and the predictor variables were ones collected at each wave. We imputed wave-specific means for all missing values. The logistic regression pro-duced predicted probabilities Pˆithat an observation was obtained
re-sponse rates rˆi5Pˆi/(12Pˆi) that measured the probability that a
student would respond at follow-up. The follow-up weights are reciprocals of the predicted follow-up response rates–that is, wi5
1/rˆi. Because most analyses are performed separately for males
and females, the weights were computed separately by gender.
Data Quality
Analysis of multiple questions about experience with certain sexual behaviors indicated that inconsistencies were rare. For example, among adolescents who indicated that they had engaged in vaginal intercourse one or more times during the previous year, ,2% of respondents reported that they had never had vaginal intercourse (more than 10 items earlier).
Statistical Tests
We report results of weighted cross-tabulations (includingf coefficients) and weighted logistic regression. All statistical infer-ence accounts for the weights through the use of linearization methods that produce asymptotically consistent standard errors.16
Computations were performed by the hreg and hlogit commands in Stata, version 3.1.17
RESULTS Characteristics
Fifty-one percent of respondents were male. The sample was distributed evenly by grade: 9th grade, 25%; 10th, 27%; 11th, 25%; 12th, 23%. Eight percent described themselves as African-American, 10% Asian and Pacific Islander, 27% Latino, 48% white, and 7% Other. Fifty-six percent had at least one parent who was a college graduate; 71% reported that English was the language most often spoken at home; 47% were living in a two-parent household; 18% expected not to graduate from college, 31% ex-pected to graduate from college, and an additional 51% expected to attend graduate or professional
school. Fifty-one percent had had vaginal intercourse (were nonvirgins). Forty-nine percent had had vagi-nal or avagi-nal intercourse during the previous year.
Awareness of the School’s Condom Availability Program
Respondents had an accurate perception of the school’s condom availability program. Eighty-eight percent agreed that “students of all ages and in all grades are allowed to get condoms at my school.” Seventy-four percent knew that the school does not require parents’ permission to take condoms, and most of the rest (19%) were uncertain.
Experience With School Condoms
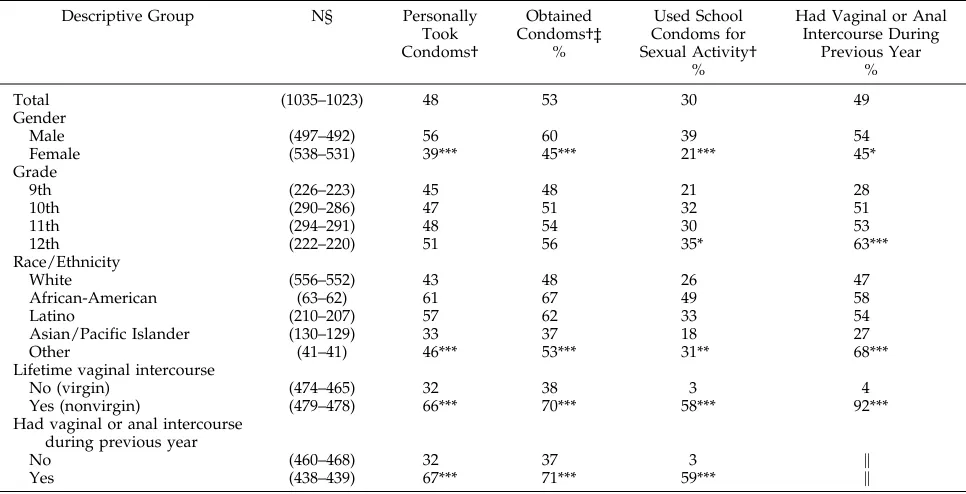
Forty-eight percent of the students had personally taken school condoms during the school year, and an-other 5% had not personally taken them but had ob-tained them from someone else, for a total of 53% who had obtained school condoms (Table 1). Males were more likely than females to have obtained condoms, and the likelihood of obtaining them increased with grade. Among racial/ethnic groups, African-Ameri-cans were the most likely to have obtained school con-doms and Asians and Pacific Islanders were the least likely. Nonvirgins were much more likely to have ob-tained condoms than virgins (70% vs 38%, P,.001,f
5 2.32). Students who had had vaginal or anal inter-course during the previous year were much more likely to have obtained condoms than those who had not (71% vs 37%, P,.001,f5 2.34).
Among adolescents who had personally picked up school condoms during the school year, 31% had
TABLE 1. Receipt and Use of School Condoms and Sexual Activity After Implementation of a Condom Availability Program
Descriptive Group N§ Personally
Took Condoms†
Obtained Condoms†‡
%
Used School Condoms for Sexual Activity†
%
Had Vaginal or Anal Intercourse During
Previous Year %
Total (1035–1023) 48 53 30 49
Gender
Male (497–492) 56 60 39 54
Female (538–531) 39*** 45*** 21*** 45*
Grade
9th (226–223) 45 48 21 28
10th (290–286) 47 51 32 51
11th (294–291) 48 54 30 53
12th (222–220) 51 56 35* 63***
Race/Ethnicity
White (556–552) 43 48 26 47
African-American (63–62) 61 67 49 58
Latino (210–207) 57 62 33 54
Asian/Pacific Islander (130–129) 33 37 18 27
Other (41–41) 46*** 53*** 31** 68***
Lifetime vaginal intercourse
No (virgin) (474–465) 32 38 3 4
Yes (nonvirgin) (479–478) 66*** 70*** 58*** 92***
Had vaginal or anal intercourse during previous year
No (460–468) 32 37 3 \
Yes (438–439) 67*** 71*** 59*** \
* P,.05 for statistical test (Pearson’sx2) that the percentages reporting a column outcome differ for descriptive groups.
** P,.01. *** P,.001.
§ The number of respondents varied slightly among items. † During the school year (previous 8 months).
‡ Took school condoms personally or obtained them through someone else.
taken 1 packet (each packet contained 2 condoms), 40% had taken 2 to 5, 13% had taken 6 to 10, 9% had taken 11 to 19, and 7% had taken 20 or more. Most students who had not had vaginal or anal intercourse during the previous year took only 1 condom packet (49%) or 2 to 5 packets (43%).
Fifty-seven percent agreed that “it’s fairly easy to take condoms at school without someone seeing you.” Adolescents who had personally taken con-doms were more likely to consider it easy than those who had not taken them (71% vs 44%, P,.001,f5
2.28). (Fourteen percent of the former group were uncertain, compared with 33% of the latter group.)
Forty-six percent “would be embarrassed if some-one saw me taking condoms at school.” Potential embarrassment was more likely to be reported by virgins than by nonvirgins (53% vs 38%, P,.001,f
5 2.15) and by adolescents who had not taken school condoms than by those who had (55% vs 36%, P,.001,f5 .19). Females also were more likely to be embarrassed than males (51% vs 42%, P 5 .020,
f5 2.08).
Seventy-nine percent agreed that “it’s OK to take them without paying if you don’t have the money.” Among students who had obtained condoms, 77% had read the accompanying information sheets. Among students who had read the sheets, 17% “didn’t learn anything,” 46% “learned a little,” 23% “learned a lot,” and 14% did not “remember much about what they [the information sheets] say.” Thirty-three percent of students who had not gotten condoms had also read the information sheets. Eigh-teen percent of these students “didn’t learn any-thing,” 46% “learned a little,” 14% “learned a lot,” and 22% did not “remember much.”
Use of School Condoms
Thirty percent of all students (Table 1), 54% of students who had obtained school condoms, and 78% of nonvirgins who had obtained school con-doms had used them for sexual activity. Specifically, among students who had obtained condoms, 52% had used them for vaginal intercourse, 7% for anal intercourse, and 4% for fellatio.
Among students who had used school condoms for sexual activity, 31% had used a school condom 1 time, 37% 2 to 5 times, 16% 6 to 9 times, 10% 10 to 19 times, and 6% 20 or more times.
Students also used condoms for other activities, with virgins reporting more exploratory use than nonvirgins (Table 2).
Among students who had had vaginal intercourse in the previous year, 55% had used school condoms for vaginal intercourse. For male–female fellatio with ejaculation and male–female anal intercourse, the comparable percentages were 5% and 25%, respec-tively.
Adolescents who had used a condom for vaginal intercourse during the previous year obtained them from a variety of sources. Thirty-five percent of stu-dents who had used a condom for vaginal inter-course during the previous year had obtained the condom they last used for vaginal intercourse from school, with more males than females reporting the
school as their source (42% vs 26%, P 5 .006, f 5
2.17). Thirty-three percent had obtained the condom from a store, 14% from a friend, 4% from a parent, and the remaining 14% from other sources.
For the subsample that had used a condom for vaginal intercourse during the previous year, male gender was the only characteristic in a logistic re-gression that significantly predicted that the student had obtained the condom last used for vaginal inter-course from school (odds ratio: 2.56, 95% confidence interval: 1.53– 4.29, P, .001). The other variables in the regression, including grade, race/ethnicity, num-ber of parents in the household, language spoken at home, and parental education, were also not signif-icant in bivariate analyses.
Attitudes About the Condom Program
Students generally supported the condom pro-gram. Eighty-eight percent of the students thought the school should give out condoms, with 75% of these students reporting they liked the way the school organized its program. Sixty-five percent would like condoms to be available in more locations at school, such as in the gym and in more classrooms, and 68% thought they should be available through vending machines in restrooms.
Students strongly opposed the idea that parental permission be required to obtain condoms. In re-sponse to the question, “Do you think that a parent’s permission should be required for a student to get condoms at school?,” 75% answered “definitely not” and another 10% answered “probably not.” The rest were evenly split between those who had “no opin-ion” and those who “definitely” or “probably” sup-ported a requirement for parental permission. This finding varied somewhat by whether the students had or had not gotten school condoms (probably or definitely not: 90% vs 81%, P 5 .002, f 5 2.12) or whether they were virgins (82% vs 90%, P5.005,f
5.11). However, high percentages opposed parental permission in all subgroups.
If the school were to require parental permission for students to get condoms, 79% thought students would get them less often than with the present system (which does not require permission). There were no statistically significant differences based on whether students had obtained school condoms (78%
TABLE 2. Percentage of Students Who Used School Condoms for Activities Other Than Penetrative Sex, Among Students Who Obtained School Condoms
Male Female
Virgin (N591)
Nonvirgin (N5181)
Virgin (N583)
Nonvirgin (N5147)
Removed from packet
47 24 42 30
Gave to someone 29 37 48 49
Saved it 47 47 54 45
Lost it or threw it away
22 17 27 11
Put it on fingers, banana
11 3 15 10
Put it on penis, but no sex
vs 80%, P 5 .436,f 5 .03) or were virgins (78% vs 81%, P 5 .391, f 5 .03). Fifty-seven percent of re-spondents thought that students would use condoms less often if parental permission were required, 21% thought condom use would be unchanged, 9% thought they would use condoms more often, and the rest were uncertain. Seventy-four percent be-lieved that there would not be a change in how often students would have vaginal intercourse, 9% thought the frequency would increase, and 7% thought it would decrease. Thirty-five percent thought there would be no change in the frequency with which students would discuss sexual issues with their parents, 28% thought they would discuss sexual issues less often, and 15% thought they would discuss sexual issues more often.
Perceived Impact of Program on Peer Environment Thirteen percent agreed and 71% disagreed that “having condoms available at school makes it harder for someone who doesn’t want to have sex to say no.” Seventy-six percent of students who had ob-tained school condoms and 79% of those who had used them for sexual activity disagreed as well. Fe-males were more likely to disagree than Fe-males (77% vs 66%, P5.002,f5.12). Sixty-two percent agreed and 13% disagreed that “having condoms available at school makes it easier to talk with your sex partner about using them.” There were no significant differ-ences in the percentage of males and females who agreed (63% vs 61%, P 5 .598, f 5 .02). Seventy percent of students who had obtained school con-doms and 76% of those who had used them for sexual activity agreed.
DISCUSSION
High school condom availability programs were introduced only recently into schools in the United States. Despite much controversy and debate over these programs,5,18 –23 little scientific information is available about them. In particular, little is known about how students react to these programs and the extent to which they make use of condoms.
Our study demonstrates widespread use of the program. Students knew the program existed and had an accurate view of how it functions. Approxi-mately half had taken school condoms, and many were using them for sexual activities. Approximately half of nonvirgins had used school condoms for vag-inal intercourse, indicating broad impact of the in-tervention.
However, school condoms were not being used for all forms of intercourse. Among students who had engaged in fellatio with ejaculation and anal inter-course during the previous year, very few had used school condoms for these activities. School condoms were lubricated, making it unlikely that they would be used for fellatio. (If schools want to encourage use of school condoms for fellatio, they may need to provide unlubricated condoms in addition to or in-stead of lubricated condoms, along with education about their proper use.)
Results from this study reinforce previous findings suggesting that condom availability programs
re-ceive high levels of support from students.7,10,11 How-ever, the students would have preferred condoms to be available in more places, such as bathroom vend-ing machines. Embarrassment and concern about be-ing seen obtainbe-ing condoms (whether from a store or school program) have been noted in other studies as one reason adolescents do not obtain them.7,24 –26Our study supported these findings, with many of the students reporting that they would be embarrassed if they were seen taking condoms. This suggests that programs would reach more students if condoms were made available in a discreet manner.
As had been found in previous studies,7,9 male students were more likely than female students to have taken school condoms. Male students were also nearly twice as likely to report having used school condoms for sexual activity, even though they were only;20% more likely to report having engaged in vaginal or anal intercourse during the previous year. Consistent with these findings, female students were more likely than male students to report that they would feel embarrassed if seen taking condoms at school. Condoms have been traditionally considered a male form of contraception, and our findings may indicate that condom programs will have more of a direct effect on males in a school. Nonetheless, it may be possible to create an atmosphere in which females who want to use the program will feel more com-fortable doing so. Efforts may be necessary to ad-dress issues that may inhibit females’ use of the program, such as embarrassment, discomfort pro-posing condom use to sexual partners, and selection of methods that prevent pregnancy rather than preg-nancy and disease.
More than two thirds of 9th graders who had had vaginal or anal intercourse in the previous year had used school condoms for sexual activity, compared with slightly more than half of comparable 12th graders. Although this could indicate less contracep-tive use by older students, it could also reflect that 12th graders have greater access to obtaining con-doms outside of the school or that they are more likely to use other forms of contraception. Regardless of the reason, our results suggest that a school con-dom program may be used more by younger stu-dents, who have less access to other sources of any form of contraception.
Few previous studies have examined or docu-mented use of condoms (from any source) by stu-dents who are virgins. We found that some virgins engaged in exploratory use of school condoms with-out having intercourse, raising questions abwith-out the long-term consequences. Greater familiarity with condoms could lead to greater likelihood of their use by virgins who later engage in intercourse, especially at first intercourse. The opportunity to become famil-iar with condoms in advance of actual use could also result in more students using condoms properly. These possibilities are worth addressing in prospec-tively designed studies in the future.
stu-dents in our study had taken condoms, compared with students at a school where condoms were made available through faculty members.9 One concern raised about programs that make condoms freely available without adult monitoring is that a few stu-dents may empty baskets of all the condoms and leave none for other students. The widespread acqui-sition and use of school condoms documented in our study suggests otherwise.
Although we weighted the data using demo-graphic and other variables, some other characteris-tic (eg, sexual history) may have influenced the prob-ability of participating in the survey as well as reactions to the condom program. Variables such as sexual history could not be used for weighting the data, because they could have been changed by the condom program. Local factors and specific program details can affect reactions to any new program, and generalizing to other school districts must always be done with caution.
We report on data collected 1 year after the con-dom availability program began. Response to any new program may vary from the period of novelty just after implementation until later, when it may become an unremarkable feature of school life. This is particularly true in a high school, where within 4 years there will be almost no students remaining who remember a time when the program did not exist. Additional research is needed to determine how students will react to condom availability pro-grams in the long run.
ACKNOWLEDGMENTS
This study was supported by Grant HS08055-1, Agency for Health Care Policy and Research, Rockville, MD; the American Foundation for AIDS Research, Los Angeles, CA; the Brotman Foundation of California, Encino, CA; the California Wellness Foundation, Woodland Hills, CA; and the Robert Wood Johnson Clinical Scholars Program, Los Angeles, CA.
We thank the students, parents, school and district personnel, and school board members who contributed to this study, and Robert H. Brook, MD, ScD; Rebecca Collins, PhD; Phyllis L. El-lickson, PhD; Arleen Leibowitz, PhD; Linda G. Martin, PhD; Mar-tin F. Shapiro, MD, PhD; and our anonymous reviewers for their comments on drafts of this article. We also thank Jennifer Hawes-Dawson, BA; Ron D. Hays, PhD; Beverly A. Weidmer, MA; and the staff of the RAND Survey Research Group for their assistance with this study.
REFERENCES
1. American Academy of Pediatrics, Committee on Adolescence. Condom availability for youth. Pediatrics. 1995;95:281–285
2. ACOG Committee Opinion Number 154. Condom Availability for
Adoles-cents. Washington, DC: American College of Obstetrics and
Gynecologists; 1995
3. American School Health Association, Council on Sexuality Education.
Latex Condom Availability Programs in Schools. ASHA Compendium of
Resolutions. II. Position Papers and Policy Statements. Kent, OH: Amer-ican School Health Association; 1992
4. Advocates for Youth. Cities With Schools Offering Condom Availability
Programs. Identified as of 7/3/95. Washington, DC: Advocates for Youth;
1995
5. Stryker J, Samuels SE, Smith MD. Condom availability in schools: the need for improved program evaluations. Am J Public Health. 1994;84: 1901–1906
6. Kirby DB, Brown NL. Condom availability programs in US schools. Fam
Plann Perspect. 1996;28:196 –202
7. Guttmacher S, Lieberman L, Wai HC, et al. Gender differences in attitudes and use of condom availability programs among sexually active students in New York City public high schools. J Am Med
Women’s Assoc. 1995;50:99 –102
8. Hagedorn S. Student views of the school nurse’s role in a secondary school condom availability program. J School Health. 1993;63:358 –360 9. Wolk LI, Rosenbaum R. The benefits of school-based condom
availability: cross-sectional analysis of a comprehensive high school-based program. J Adolesc Health. 1995;7:184 –188
10. Fanburg JT, Kaplan DW, Naylor KE. Student opinions of condom distribution at a Denver, Colorado, high school. J School Health. 1995; 65:181–185
11. Sikand A, Fisher M, Friedman SB. AIDS knowledge, concerns, and behavioral changes among inner-city high school students. J Adolesc
Health. 1996;18:325–328
12. Schuster MA, Bell RM, Kanouse DE. The sexual practices of adolescent virgins: genital sexual activities of high school students who have never had vaginal intercourse. Am J Public Health. 1996;86:1570 –1576 13. Kearney KA, Hopkins RH, Mauss AL, Weisheit RA. Sample bias
result-ing from a requirement for written parental consent. Public Opin Q. 1983;47:96 –102
14. Lueptow L, Mueller SA, Hammes RR, Master LS. The impact of in-formed consent regulations on response rate and response bias. Soc
Methods Res. 1977;6:183–204
15. Severson H, Ary D. Sampling bias due to consent procedures with adolescents. Addict Behav. 1983;8:433– 437
16. Binder DA. On the variances of asymptotically normal estimators from complex surveys. Int Stat Rev. 1983;51:279 –292
17. Stata Corporation. Stata Reference Manual: Release 3.1. 6th ed. College Station, TX: Stata Corporation; 1993
18. Blair J. Condom availability in schools. J Adolesc Health. 1993;14:565–568 19. English A. Condom distribution in the schools. J Adolesc Health. 1993;
14:562–564
20. Guttmacher S, Lieberman L, Ward D, Radosh A, Rafferty Y, Freuden-berg N. Parents’ attitudes and beliefs about HIV/AIDS prevention with condom availability in New York City public high schools. J School
Health. 1995;65:101–106
21. Kerr DL. Condoms availability in New York City schools. J School
Health. 1991;61:279 –280
22. Mahler K. Condom availability in the schools: lessons from the court-room. Fam Plann Perspect. 1996;28:75–77
23. Samuels SE, Smith MD, eds. Condoms in the Schools. Menlo Park, CA: Henry J. Kaiser Family Foundation; 1993
24. Hingson RW, Strunin L, Berlin BM, Heeren T. Beliefs about AIDS, use of alcohol and drugs, and unprotected sex among Massachusetts ado-lescents. Am J Public Health. 1990;80:295–299
25. MacDonald NE, Wells GA, Fisher WA, et al. High-risk STD/HIV be-havior among college students. JAMA. 1990;263:3155–3159
DOI: 10.1542/peds.100.4.689
1997;100;689
Pediatrics
Mark A. Schuster, Robert M. Bell, Sandra H. Berry and David E. Kanouse
Availability Program
Students' Acquisition and Use of School Condoms in a High School Condom
Services
Updated Information &
http://pediatrics.aappublications.org/content/100/4/689 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/100/4/689#BIBL This article cites 21 articles, 1 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/contraception_sub Contraception
icine_sub
http://www.aappublications.org/cgi/collection/adolescent_health:med Adolescent Health/Medicine
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.100.4.689
1997;100;689
Pediatrics
Mark A. Schuster, Robert M. Bell, Sandra H. Berry and David E. Kanouse
Availability Program
Students' Acquisition and Use of School Condoms in a High School Condom
http://pediatrics.aappublications.org/content/100/4/689
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.