A Survey of Primary Care Providers’ Knowledge of HPV-associated Head and Neck Cancers: A focus on clinical characteristics, presentation and outcomes
By James Taylor
A Master’s Paper submitted to the faculty of the University of North Carolina at Chapel Hill
in partial fulfillment of the requirements for the degree of Master of Public Health in
the Public Health Leadership Program
Table of Contents
Abstract 3 Introduction 5
Methods 6
Results 7
Demographics and Response Rates 8
Knowledge of Head and Neck Cancer 9
Knowledge of HPV-associated Head and Neck Cancer 9 Knowledge of HPV Infection 9
Discussion 9 Tables 14
References 20 Appendix 26 Title (2) 35
Introduction (2) 36 Methods (2) 37
Results (2) 39 Discussion (2)42
A Survey of Primary Care Providers’ Knowledge of HPV-associated Head and Neck Cancers: A focus on clinical characteristics, presentation and outcomes
Importance: The epidemiology of head and neck cancer has changed in recent years, particularly as related to those associated with human papillomavirus (HPV). Understanding primary care physicians’ (PCPs) current knowledge about HPV-associated head and neck cancers (HNC) will help inform educational efforts on this important topic.
Objective: To assess the knowledge and understanding of PCPs towards the rapidly changing clinical characteristics, presentation and outcomes associated with HPV-positive HNCs
Design, Setting and Participants: Online survey of primary care physicians (pediatricians, general internists and family medicine physicians) at two tertiary academic medical centers in North Carolina between May and July of 2016.
Results: 275 PCPs at two tertiary academic medical centers were invited to participate via email, 95 PCPs completed the survey for a response rate of 34.5%. The majority of respondents were female (67.0%), attending physicians (61.5%), had less than 10 years of practice experience (46.0%), and practiced in an academic setting (85.3%). PCPs correctly answered 56% of
knowledge based questions about HPVs causative role in HNC. 79% of PCPs failed to correctly identify the most common clinical presentation of the HPV-positive patient. Further, only 23% of PCPs correctly identified that HPV is associated with a much improved prognosis in HNC. Survey data indicate that PCPs most commonly consider the HPV-positive patient to be an African American male presenting with a persistent sore throat or non-healing ulcer and to have prior tobacco and alcohol consumption. However, PCPs demonstrated a high degree of
Introduction
Cancer of the head and neck is the sixth most common cancer worldwide with an estimated incidence of 633,000 cases annually.1 Recently in the United States the overall incidence of head and neck cancer (HNC) has declined, paralleling decreases in tobacco use.2 However, despite the overall decline in head and neck cancers, there has been an increase in the incidence of oropharyngeal squamous cell carcinoma (OPSCC) driven by human papillomavirus (HPV) infection.3 It is estimated that the incidence of HPV-associated OPSCC has increased by 225% from 1988-2004.4 Compared to patients with negative HNCs, patients with HPV-positive HNCs tend to be younger, from higher socioeconomic status, have less tobacco and alcohol exposure, and are more likely to be caucasian.5-6 In addition, HPV-positive disease tends to have superior oncologic outcomes and improved response to therapy.7,8 Due to the substantial differences between patients who present with HPV-positive and HPV-negative HNC, it is imperative that primary care physicians are knowledgeable about the rapidly changing
epidemiology, clinical characteristics and outcomes associated with HPV-driven HNC in order to appropriately refer high-risk patients.
of HPV-related HNC. Overall, the rapid changes associated with HPV-positive HNC pose significant clinical challenges for both PCPs and specialists.
The goal of this research is to build upon efforts by the American Head & Neck Society
(AHNS) to help educate providers from multiple specialties on the rapidly changing presentation and outcomes associated with HPV-positive head and neck cancers by identifying areas where additional educational resources would benefit PCPs. In order to gain insight into the knowledge of PCPs with respect to HPV-positive HNC, a survey was developed and distributed at two tertiary academic medical centers in North Carolina.
Methods
We developed a 29-question electronic survey to assess the current knowledge of PCPs in regards to HPV-positive HNC. The survey included a broad assessment of three topics: general knowledge of head and neck cancer, general knowledge about HPV, and specific knowledge about the association of HPV with head and neck cancers. This survey instrument was developed in a collaborative manner with input from head and neck oncology specialists,
radiation oncologists, family physicians, and epidemiologists at the University of North Carolina at Chapel Hill (the full survey is located in the appendix). In addition, relevant literature and practice guidelines were searched and incorporated into the development process. Finally, several questions previously used in a survey of AHNS members on awareness of HPV-associated head and neck cancers were included with permission.12 Content and discriminant validity were assessed by a group of 5 physicians and 5 medical students respectively.
For the purpose of this study, the term “PCPs” included general pediatricians, general internists and family medicine physicians. The survey was made available to these physicians via an online form (Google Forms, Alphabet Inc., Mountain View, CA) between March and July of 2016. No compensation or incentive was provided for participation. The study was approved by the institutional review board at the University of North Carolina at Chapel Hill.
Individual scores were calculated as percent for correct overall and for each category of questions and stratified by specialty. Additionally, overall scores were calculated for each knowledge based question. We compared means with either student’s t-test or ANOVA as appropriate with SAS 9.4 (SAS Institute, Cary, NC).
Results
Demographics and Response Rates
The survey had an overall response rate of 34.5% with 95 of 275 PCPs responding and completing the survey. One respondent answered less than 50% of the survey and was excluded from data analysis. Provider characteristics for respondents can be found in Table 1. Over two-thirds of respondents were female (67%). Pediatricians had the highest proportion of respondents with a 41.7% response rate, followed by family medicine at 36.4%. The majority of respondents were attending physicians (61%) and were practicing in an academic setting (85%). Of
responding attending physicians 46% had less than 10 years of practice experience.
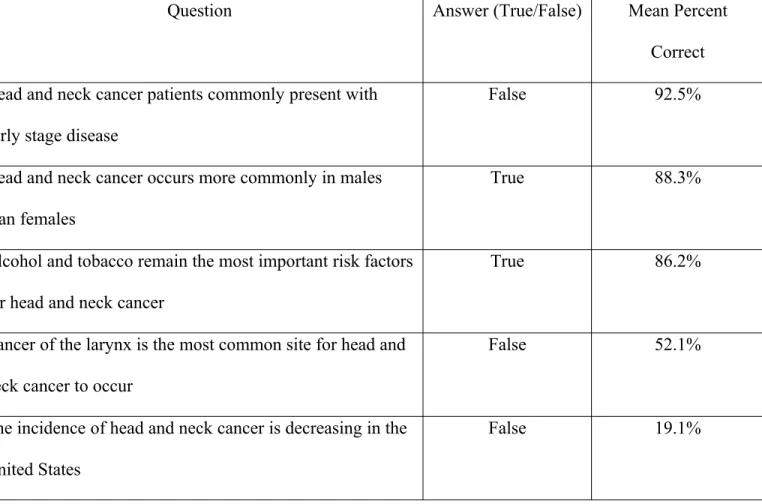
Knowledge about Head and Neck Cancer
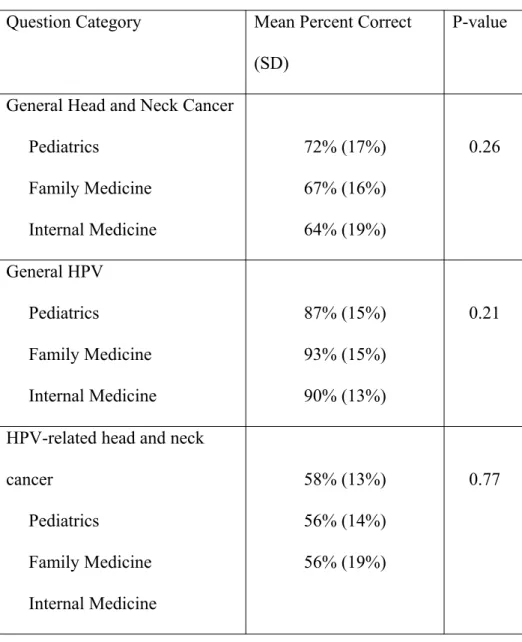
percentage of correct responses for general HNC can be found in Table 2. The most commonly missed question was “the incidence of head and neck cancer is decreasing in the United States” with only 19% responding correctly. When stratified by specialty, pediatricians had the average highest percentage of correctly answered questions (72%) followed by family and internal medicine (67% and 64% respectively). Results stratified by question category and specialty can be found in Table 3.
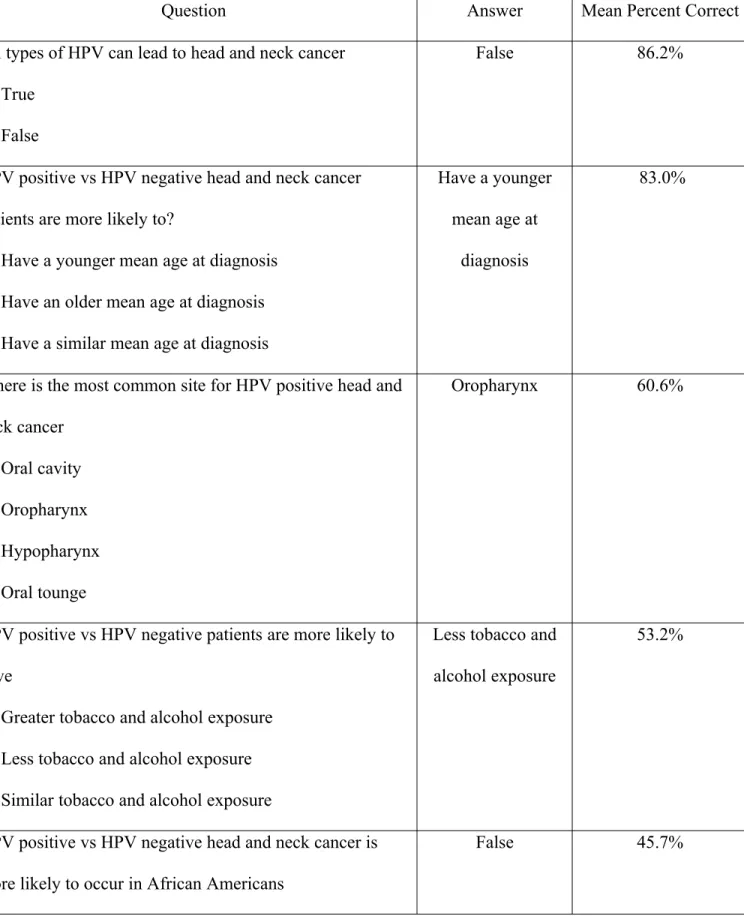
Knowledge about HPV’s Causative Role in HNC
The percentage of correct responses was relatively low for knowledge regarding HPV-driven HNCs at 56% (SD 15%). The corresponding questions and percent correct can be found in Table 4. Only 61% of respondents correctly identified the oropharynx as the most common site for HPV-positive head and neck cancer to occur. Additionally, only 21% correctly identified that a painless neck mass is the most common presentation for HPV-positive OPSCC.
Pediatricians had a 58% correct response rate followed by family medicine and internal medicine at 56% respectively (p-value: 0.77).
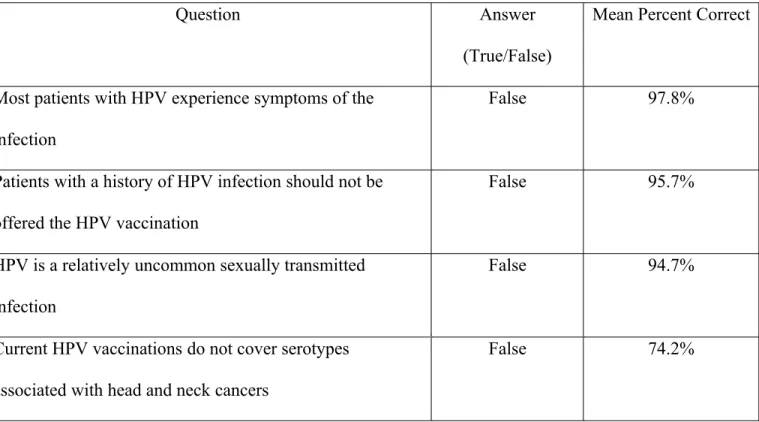
Knowledge about HPV Infection
Overall, accuracy for knowledge about HPV infection was greater than for either general HNC knowledge or knowledge of HPVs causative role in HNC as evidenced by Table 5. Most respondents correctly indicated “most patients with HPV do not experience symptoms of
Discussion
A growing body of literature has demonstrated that patients with HPV-positive OPSCC have distinct risk factors, oncologic outcomes and improved survival compared with non-HPV HNC cancer patients.13 These significant differences between HPV-positive and HPV-negative HNCs indicate that cancers driven by HPV may be biologically and clinically distinct entities from cancers caused by tobacco and alcohol. This rapid change in the incidence of HPV-positive HNCs poses significant clinical challenges. Specifically, for PCPs who are often the first
providers to see a patient with various complaints, the presentation of the “classic” head and neck cancer patient is changing. Correctly identifying high-risk patients among the
approximately 20% of primary care patients with complaints involving the head and neck will require primary care physicians to be aware of clinical presentations and risk factors for HPV-related HNC.10,14
Caucasian male presenting with a painless neck mass without a significant alcohol and tobacco history.15,16 This information indicates that PCPs are not fully aware of the demographic
differences between the HPV-positive and HPV-negative HNC populations. These
misunderstandings hold the potential to lead to delayed initial diagnosis, as well as a decreased likelihood of the providers obtaining a relevant sexual history to evaluate for risk factors for HPV transmission.
Additionally, most PCPs believe that HPV-positive patients respond worse to
chemoradiotherapy and have worse outcomes overall in regards to morbidity and survival. This is the opposite of the clinical picture associated with HPV-positive patients who have improved response to therapy and clinical outcomes.17 Although a detailed understanding of HPV HNC prognosis and treatment is unnecessary in the context of appropriate primary care, basic
awareness of treatment modalities and outcomes can dramatically alter physician approaches to initial patient counseling and referral. For example, the presence of regional lymph node metastasis in HPV-negative HNC patients is considered to be a major indicator of poor
prognosis.15 In contrast, HPV-positive OPSCC patients tend to have more extensive lymph node metastasis at time of diagnosis, but this is not associated with major changes in outcome.18
towards PCPs to increase awareness of the common clinical characteristics and presentations of HPV-positive HNC patients has the potential to improve outcomes through increased
surveillance and early detection.
Despite this clear importance of HNC awareness among PCPs, there is evidence that current levels of HNC and otolaryngology knowledge among this group may be sub-optimal. A 2012 survey found that significant portions of PCPs incorrectly identified common presentations of otolaryngology diseases.20 Furthermore, a study conducted by Jackowska et al in Poland found that general practitioners (GPs) were less knowledgeable regarding the association between HPV and head and neck cancer compared with otolaryngologists.9 A similar study of GPs in Italy found that GPs were considerably less knowledgeable about the association of HPV and HNC, compared to HPV’s role in the development of cervical, vulvar and vaginal cancers.21 Overall, when queried, the vast majority of PCPs subjectively desired further education and training about otolaryngology.22
Overall, we demonstrate the need for increased education among primary care providers with a focus on the HPV-positive patient.
The solutions to this challenge will likely be multifold. One potential avenue is
addressing the knowledge gaps early by incorporating additional otolaryngology education into medical school curriculums in the United States. Currently, less than 2/3 of American medical schools require any clinical otolaryngology experience.23 This gap likely contributes to the fact that several previous studies have shown insufficient HNC knowledge and physical exam skills among medical students, as well as to ongoing HNC knowledge deficits later in these students’ careers.24-22 Additionally, otolaryngology professional societies should continue to encourage primary care providers to attend otolaryngology conferences or work in unison to organize multi-specialty conferences where relevant HNC and HPV research can be presented to both PCP and otolaryngology researchers.
Overall, we believe that our study is the first to objectively measure the awareness of HPV-related trends in HNC among PCPs in the United States and builds upon the AHNS’ recent emphasis on education.12 Strengths of our study include a multidisciplinary team of clinicians and researchers who assisted in the survey development process, a high response rate by
Our study provides evidence that PCPs, although knowledgeable with respect to the “classic” head and neck cancer patient, are less knowledgeable about the HPV-positive head and neck cancer patient. We demonstrate a need for additional education among PCPs with respect to HPV-positive HNCs. Innovative and collaborative efforts, directed at increasing both
Table 1. Provider Characteristics Provider Characteristics Respondents ,% (n=95) Sex Male Female 33.0 67.0 Practice Time (years)
Resident/Fellow 1-10 11-20 >20 41.0 26.3 14.8 17.9 Practice Setting Academic
Table 2. General Knowledge of HNC
Question Answer (True/False) Mean Percent
Correct Head and neck cancer patients commonly present with
early stage disease
False 92.5%
Head and neck cancer occurs more commonly in males than females
True 88.3%
Alcohol and tobacco remain the most important risk factors for head and neck cancer
True 86.2%
Cancer of the larynx is the most common site for head and neck cancer to occur
False 52.1%
The incidence of head and neck cancer is decreasing in the United States
Table 3. Percent correct by question category and specialty
Question Category Mean Percent Correct (SD)
P-value
General Head and Neck Cancer Pediatrics
Family Medicine Internal Medicine
72% (17%) 67% (16%) 64% (19%)
0.26
General HPV Pediatrics
Family Medicine Internal Medicine
87% (15%) 93% (15%) 90% (13%)
0.21
HPV-related head and neck cancer
Pediatrics
Family Medicine Internal Medicine
58% (13%) 56% (14%) 56% (19%)
Table 4. HPV-associated HNC Knowledge
Question Answer Mean Percent Correct
All types of HPV can lead to head and neck cancer True
False
False 86.2%
HPV positive vs HPV negative head and neck cancer patients are more likely to?
Have a younger mean age at diagnosis Have an older mean age at diagnosis Have a similar mean age at diagnosis
Have a younger mean age at
diagnosis
83.0%
Where is the most common site for HPV positive head and neck cancer Oral cavity Oropharynx Hypopharynx Oral tounge Oropharynx 60.6%
HPV positive vs HPV negative patients are more likely to have
Greater tobacco and alcohol exposure Less tobacco and alcohol exposure Similar tobacco and alcohol exposure
Less tobacco and alcohol exposure
53.2%
HPV positive vs HPV negative head and neck cancer is more likely to occur in African Americans
True False
HPV positive head and neck cancers respond worse to chemoradiotherapy
True False
False 45.7%
HPV is associated with a much improved prognosis for patients with head and neck cancer
True False
True 22.6%
What is the most common presenting sign for patient with HPV-positive oropharynx cancer
Non healing ulcer Painless neck mass Dysphagia
Persistant sore throat
Table 5. General knowledge of HPV Infection
Question Answer
(True/False)
Mean Percent Correct
Most patients with HPV experience symptoms of the infection
False 97.8%
Patients with a history of HPV infection should not be offered the HPV vaccination
False 95.7%
HPV is a relatively uncommon sexually transmitted infection
False 94.7%
Current HPV vaccinations do not cover serotypes associated with head and neck cancers
References
1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893-2917. doi:10.1002/ijc.25516.
2. Chai RC, Lambie D, Verma M, Punyadeera C. Current trends in the etiology and diagnosis of HPV-related head and neck cancers. Cancer Med. 2015:n/a - n/a. doi:10.1002/cam4.424.
3. Marur S, D’Souza G, Westra WH, Forastiere AA. HPV-associated head and neck cancer: a virus-related cancer epidemic. Lancet Oncol. 2010;11(8):781-789. doi:10.1016/S1470-2045(10)70017-6.
4. Chaturvedi AK, Engels EA, Pfeiffer RM, et al. Human Papillomavirus and Rising Oropharyngeal Cancer Incidence in the United States. J Clin Oncol. 2011;29(32):4294-4301. doi:10.1200/JCO.2011.36.4596.
5. Gillison ML, D’Souza G, Westra W, et al. Distinct risk factor profiles for human papillomavirus type 16-positive and human papillomavirus type 16-negative head and neck cancers. J Natl Cancer Inst. 2008;100(6):407-420. doi:10.1093/jnci/djn025.
6. Ragin CCR, Taioli E. Survival of squamous cell carcinoma of the head and neck in relation to human papillomavirus infection: Review and meta-analysis. Int J Cancer. 2007;121(8):1813-1820. doi:10.1002/ijc.22851.
Clinical Trial. JNCI J Natl Cancer Inst. 2008;100(4):261-269. doi:10.1093/jnci/djn011.
8. Dayyani F, Etzel CJ, Liu M, Ho C-H, Lippman SM, Tsao AS. Meta-analysis of the impact of human papillomavirus (HPV) on cancer risk and overall survival in head and neck squamous cell carcinomas (HNSCC). Head Neck Oncol. 2010;2:15. doi:10.1186/1758-3284-2-15.
9. Jackowska J, Bartochowska A, Karlik M, Wichtowski M, Tokarski M, Wierzbicka M. The knowledge of the role of papillomavirus - Related head and neck pathologies among general practitioners, otolaryngologists and trainees. A survey-based study. PLoS One. 2015;10(10):1-10. doi:10.1371/journal.pone.0141003.
10. Griffiths E. Incidence of ENT problems in general practice. J R Soc Med. 1979;72(10):740-742. http://www.pubmedcentral.nih.gov/articlerender.fcgi? artid=1437201&tool=pmcentrez&rendertype=abstract.
11. Rourke T, Tassone P, Philpott C, Bath A. ENT cases seen at a local “walk-in centre”: a one year review. J Laryngol Otol. 2009;123(May 2008):339-342.
doi:http://dx.doi.org/10.1017/S0022215108002508.
12. Malloy KM, Ellender SM, Goldenberg D, Dolan RW. A survey of current practices, attitudes, and knowledge regarding human papillomavirus-related cancers and vaccines among head and neck surgeons. JAMA Otolaryngol Head Neck Surg. 2013;139(10):1037-1042. doi:10.1001/jamaoto.2013.4452.
14. Emery JD, Shaw K, Williams B, et al. The role of primary care in early detection and follow-up of cancer. Nat Rev Clin Oncol. 2014;11(1):38-48.
doi:10.1038/nrclinonc.2013.212.
15. Klozar J, Kratochvil V, Salakova M, et al. HPV status and regional metastasis in the prognosis of oral and oropharyngeal cancer. Eur Arch Oto-Rhino-Laryngology. 2008;265(SUPPL. 1). doi:10.1007/s00405-007-0557-9.
16. Boscolo-Rizzo P, Del Mistro A, Bussu F, et al. New insights into human papillomavirus-associated head and neck squamous cell carcinoma. Acta Otorhinolaryngol Ital organo Uff della Soc Ital di Otorinolaringol e Chir Cerv-facc. 2013;33(2):77-87.
http://www.pubmedcentral.nih.gov/articlerender.fcgi? artid=3665382&tool=pmcentrez&rendertype=abstract.
17. O’Rorke MA, Ellison M V., Murray LJ, Moran M, James J, Anderson LA. Human papillomavirus related head and neck cancer survival: A systematic review and meta-analysis. Oral Oncol. 2012;48(12):1191-1201. doi:10.1016/j.oraloncology.2012.06.019.
18. McIlwain WR, Sood AJ, Nguyen S a, Day T a. Initial Symptoms in Patients With HPV-Positive and HPV-Negative Oropharyngeal Cancer. JAMA Otolaryngol Head Neck Surg. 2014;140(5):1-7. doi:10.1001/jamaoto.2014.141.
19. Collins R, Flynn A, Melville A, Richardson R, Eastwood A. Effective health care: management of head and neck cancers. Qual Saf Health Care. 2005;14(2):144-148. doi:10.1136/qshc.2005.013961.
providers. Med Educ Online. 2012;17:17350. doi:10.3402/meo.v17i0.17350.
21. Signorelli C, Odone A, Pezzetti F, et al. Infezione da Papillomavirus umano e
vaccinazione : conoscenze e ruolo dei medici di medicina generale Human Papillomavirus infection and vaccination : knowledge and attitudes of Italian general practitioners. 2014;38(6):3-7.
22. Clamp PJ, Gunasekaran S, Pothier DD, Saunders MW. ENT in general practice: training, experience and referral rates. J Laryngol Otol. 2007;121(6):580-583.
doi:10.1017/S0022215106003495.
23. Chawdhary G, Ho EC, Minhas SS. Undergraduate ENT education: What students want.
Clin Otolaryngol. 2009;34(6):584-585. doi:10.1111/j.1749-4486.2009.02027.x.
24. Mohyuddin N, Langerman A, LeHew C, et al. Knowledge of Head and Neck Cancer Among Medical Students at 2 Chicago Universities. Arch Otolaryngol Neck Surg. 2008;134(12):1294. doi:10.1001/archotol.134.12.1294.
25. Cunningham CT, Quan H, Hemmelgarn B, et al. Exploring physician specialist response rates to web-based surveys. BMC Med Res Methodol. 2015;15:32. doi:10.1186/s12874-015-0016-z.
26. Westra WH. The changing face of head and neck cancer in the 21st century: the impact of HPV on the epidemiology and pathology of oral cancer. Head Neck Pathol. 2009;3(1):78-81. doi:10.1007/s12105-009-0100-y.
1999;10(4):412-418. doi:00001648-199907000-00009 [pii].
28. King T, Agulnik M. Head and Neck Cancer: Changing Epidemiology and Public Health Implications. Oncol J. 2010:6-8. www.cancer.gov/.../HeadandNeck-Snapshot.pdf.
29. Chera BS, Amdur RJ, Tepper J, et al. Phase 2 trial of de-intensified chemoradiation therapy for favorable-risk human papillomavirus-associated oropharyngeal squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2015;93(5):976-985.
doi:10.1016/j.ijrobp.2015.08.033.
30. Barnett ML, Song Z, Landon BE. Trends in physician referrals in the United States, 1999-2009 - with comments. Arch Intern Med. 2012;172(2):163-170.
doi:10.1001/archinternmed.2011.722.
31. Scott JR, Wong E, Sowerby LJ. Evaluating the referral preferences and consultation requests of primary care physicians with otolaryngology – head and neck surgery. J
Otolaryngol - Head Neck Surg. 2015;44(1):57. doi:10.1186/s40463-015-0114-2.
32. Gillison ML, Koch WM, Capone RB, et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. JNatlCancer Inst. 2000;92(9):709-720. http://www.ncbi.nlm.nih.gov/pubmed/10793107.
33. Malloy KM, Ellender SM, Goldenberg D, Dolan RW. A survey of current practices, attitudes, and knowledge regarding human papillomavirus-related cancers and vaccines among head and neck surgeons. JAMA Otolaryngol Head Neck Surg. 2013;139(10):1037-1042. doi:10.1001/jamaoto.2013.4452.
Cancer. Otolaryngol Clin North Am. 2012;45(4):739-764. doi:10.1016/j.otc.2012.04.003.
Appendix
Head and Neck Cancer: A Changing Presentation
Please tell us about your medical practice.
Provider Characteristics
Please choose the most appropriate answer by marking in the oval: In what discipline did you receive your primary training?
Mark only one oval.
o Family Medicine
o Internal Medicine o Pediatrics
o Other
If you answered "other" for the previous question, please provide what you consider your primary discipline:
How many years have you been in practice? Mark only one oval.
o Resident
o Clinical Fellow o 1-5
o 6-10
o 16-20
o >20
In which practice setting do you most commonly practice? Mark only one oval.
o Private Practice
o Academic Setting
o Clinic or Public Hospital o Managed Care Organization
o Other
What gender do you identify with? Mark only one oval.
o Male
o Female
General Knowledge Regarding Head and Neck Cancers
Please indicate either True or False:
The incidence of head and neck cancer is decreasing in the United States. Mark only one oval.
o True
Cancer of the larynx is the most common site for head and neck cancer to occur. Mark only one oval.
o True
o False
Head and neck cancer patients commonly present with early stage disease. Mark only one oval.
o True
o False
Alcohol and tobacco remain the most important risk factors for head and neck cancer. Mark only one oval.
o True
o False
GENERAL KNOWLEDGE OF HUMAN PAPILLOMAVIRUS AND PREVENTION
Please indicate either True or False:
All types of Human Papillomavirus (HPV) can lead to head and neck cancer. Mark only one oval.
o True
HPV-positive head and neck cancers respond worse to chemoradiation therapy. Mark only one oval.
o True
o False
HPV is a relatively uncommon sexually transmitted infection. Mark only one oval.
o True
o False
HPV is associated with a much improved prognosis for patients with head and neck cancer.
Mark only one oval.
o True o False
Head and neck cancer occurs more commonly in males than females. Mark only one oval.
o True o False
o True
o False
Most patients with HPV experience symptoms of the infection. Mark only one oval.
o True
o False
Current HPV vaccinations do not cover serotypes associated with head and neck cancers. Mark only one oval.
o True
o False
Knowledge of HPV Head and Neck Cancer Patients
Please choose the most appropriate answer:
Where is the most common site for HPV positive head and neck cancer? Mark only one oval.
o Oral Cavity
o Oropharynx o Hypopharynx
o Oral Tongue
Mark only one oval.
o Have a younger mean age at diagnosis. o Have an older mean age at diagnosis.
o Have a similar mean age at diagnosis.
What is the most common presenting sign for a patient with HPV positive oropharynx cancer?
Mark only one oval.
o Nonhealing ulcer o Dysphagia
o Painless neck mass
o Persistent sore throat
HPV positive vs HPV negative head and neck cancer is more likely to occur in African Americans.
Mark only one oval.
o True
o False
HPV negative vs HPV positive head and neck cancer patients are more likely to have: Mark only one oval.
o Greater tobacco and alcohol exposure.
o Similar tobacco and alcohol exposure.
Current Practice Trends
Please select the most appropriate answer:
When you discuss alcohol related diseases with patients, how often do you discuss alcohol as a risk factor for head and neck cancer?
Mark only one oval.
o Always
o Often o Sometimes
o Seldom o Never
When you discuss smoking related diseases with patients, how often do you discuss smoking as a risk factor for head and neck cancer?
Mark only one oval.
o Always
o Often o Sometimes
o Seldom
When you discuss smokeless tobacco related diseases with patients, how often do you discuss smokeless tobacco as a risk factor for head and neck cancer?
Mark only one oval.
o Always o Often
o Sometimes o Seldom
o Never
How often do you recommend the HPV vaccination to eligible female patients? Mark only one oval.
o Always
o Often
o Sometimes o Seldom
o Never o N/A
How often do you recommend the HPV vaccination to eligible male patients? Mark only one oval.
o Always o Often
o Seldom
o Never
o N/A
When you discuss the benefits of the HPV vaccination with female patients, how often do you discuss protection from head and neck cancer as a potential benefit?
Mark only one oval.
o Always
o Often
o Sometimes o Seldom
o Never o N/A
When you discuss the benefits of the HPV vaccination with male patients, how often do you discuss protection from head and neck cancer as a potential benefit?
Mark only one oval.
o Always
o Often o Sometimes
o Seldom
Introduction
Cancers of the head and neck are a heterogenous group of malignancies that share common anatomical origins.6 Historically, head and neck cancers (HNCs) have been classified based upon their anatomic locations.26 Recently, due to many clinical and biological differences, a subset of HNCs oropharyngeal squamous cell carcinomas (OPSCC) have been further divided based upon their association with Human Papillomavirus (HPV). 1 In the United States, it is estimated that the incidence of HPV-positive OPSCC has increased by 225% from 1988 to 2004.2,27,4 Several theories have been proposed to explain this trend, yet the causative mechanisms underlying this increase have not been fully elucidated.5 Compared with HPV-negative OPSCC, patients with HPV-positive OPSCC have distinct risk factor profiles, treatment strategies, and clinical outcomes.7,28 Additionally, these patients tend to be younger, from higher socioeconomic status, have less tobacco and alcohol exposure, and are more likely to be
Caucasian.4 positive disease may require less aggressive treatments compared with HPV-negative disease and has demonstrated superior oncologic outcomes and improved response to therapy over various treatment modalities.7,29 Due to these substantial differences, it is imperative that primary care physicians (PCPs) are knowledgeable about the rapidly changing clinical picture of the HPV-positive OPSCC patient.
Currently, limited data exist that detail the present knowledge, attitudes, and beliefs towards HPV-positive OPSCC among primary care physicians (PCPs).9 PCPs form the backbone of the healthcare system and provide the referral base to head and neck surgeons. Therefore, their knowledge of HPV-positive OPSCC plays a critical role in ensuring the timely referral of
patients on preventive health measures, inform their patients of screening recommendations, and aid their patients in shared medical decision making. Additionally, with the advent of the HPV vaccine, there is an added interest in its role in prevention of HPV-positive OPSCC. Therefore, without formal screening guidelines for head and neck cancers, the rapid changing factors associated with HPV-positive OPSCC and the potential for prevention through increased vaccination, it is imperative that PCPs are knowledgeable with respect to this evolving disease.
The purpose of this systematic review is to examine the current literature regarding studies which provide insight into the overall knowledge, attitudes, and beliefs of PCPs (and head and neck surgeons) towards HPV-positive OPSCC. The objectives (key principles) of the review are to (1) examine the current level of knowledge among PCPs on HPV-positive OPSCC (2) examine the practice patterns of PCPs towards HPV-positive OPSCC with a focus on risk factor counseling and (3) examine the beliefs of PCPs towards the HPV-vaccination as a method of prevention for OPSCC.
Methods
Search Criteria
information comparing head and neck surgeons’ knowledge to that of PCPs. The full search strategy for each database can be found in Table 1. Briefly, we used combinations of key terms to search each database based on database specific criteria.
Additionally, to ensure the thoroughness of the search, hand searches were performed on relevant articles returned from the initial search strategy. Articles identified by hand searches were reviewed, critically appraised and, when deemed appropriate, incorporated into the review. Finally, ClinicalTrials.gov was searched to identify any unpublished studies and results. Studies were screened at the abstract level and during full text review. Ultimately, articles were included only if they had relevant information pertaining to (1) oropharyngeal squamous cell carcinoma, (2) head and neck cancer, (3) primary care physicians (pediatricians, internal medicine
physicians and family medicine physicians) or head and neck surgeons, (4) contained data commenting on one of the three principles established for the current review and (5) included information from surveys, questionnaires, or focus groups. For details on inclusion and exclusion criteria see Table 2. Studies were excluded if PCPs knowledge, attitudes, and beliefs were modeled (Table 2). Only English language studies were included in the analysis and any studies published from countries outside of the Organisation for Economic Co-Operation and
Development (OECD) were excluded. Data Extraction
We reviewed all titles and abstracts of studies identified using the defined search
(respondents), type of participants, study design, survey (or questionaire) response rates, survey (or questionaire) questions, location where research was conducted, and study outcomes.
Assesment of Risk of Bias
The quality of each study was assessed by a single reviewer (JT) using a pre-specified critical appraisal and risk of bias template consisting of 15 quality assessment metrics. All studies, regardless of the number of subjects, were considered equally. Due to the types of studies included in the current review (survey based studies), non-responder bias was critically appraised and commented on below.
Results
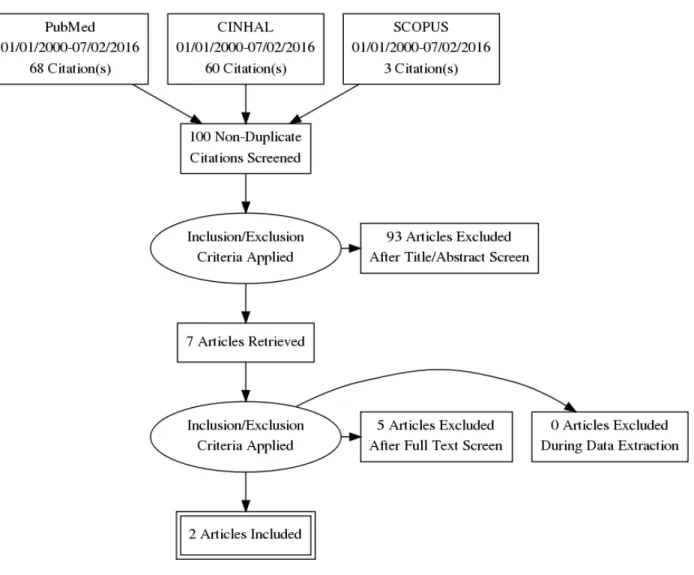
As of July 2nd, 2016, the aforementioned search strategy returned 131 citations. After removing 31 studies identified as duplicates, 100 original studies remained (Figure 1. Prisma Flow Diagram). Of these studies, 93 were excluded during abstract and title review because they did not fulfill the defined selection criteria. Following title and abstract review, seven studies remained and were included in the full text review process. Of the remaining studies, five were excluded because they did not fulfill study criteria and were deemed inappropriate for the current review (Table 3.). In total, two articles were included for review.
al. was published in PLoS ONE, a free online open access journal, and contained information on general practitioners (GPs) as well as otolaryngologists in Poland.9
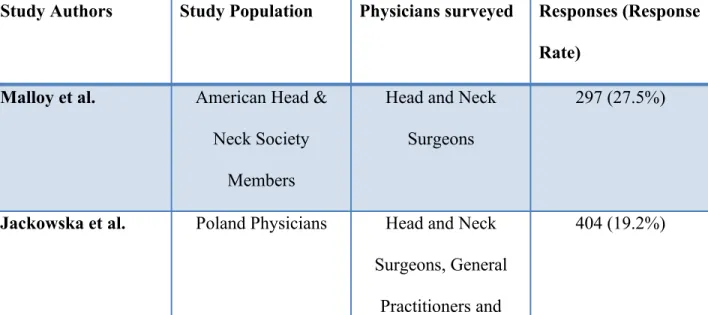
The paper published by Malloy et al. had a response rate of 27.5% while the paper by Jackowska et al. had a response rate of only 19.2%. For details on study characteristics and response rates, see Table 5. Key questions, answers, and responses from the study by Malloy et al. can be found in Tables 6 and 7. Lastly, Table 8 includes key information from the paper by Jackowska et al. The tables do not include an exhaustive list of the questions or answers asked from each survey based study, but instead represent key questions that address one or more of the three principles established for the current review. A rating of moderate has been assigned to each study when assessing for risk of bias. This grade was assigned due to low response rates leading to risk of non-responder bias.
The study by Malloy and colleagues demonstrates that head and neck surgeons are knowledgeable with respect to HPV and its role in head and neck cancers. Table 6 and Table 7 present the results from knowledge and practice pattern based questions respectively.
The paper by Jackowska and colleagues also provides important information into this topic. This survey based study was more in alignment with the goals of the current systematic review. The authors conducted a nationwide survey of GPs, otolaryngologists, and trainees to assess their current knowledge of HPV and head and neck cancer. This study demonstrates that in Poland, otolaryngologists are more knowledgeable with respect to HPV and its association with HNC than are GPs (Table. 8). In addition, the authors also demonstrate that few GPs are knowledgeable about the potential use of the HPV vaccination for the prevention of upper aerodigestive tract tumors (HNCs). When compared with otolaryngologists, PCPs were less aware of a potential benefit of the HPV vaccination for prevention of head and neck cancers.
Discussion
Currently, few studies exist that detail the knowledge, attitudes, and beliefs of PCPs towards HPV-positive OPSCC, and our study supports this claim. We developed three search strateges each tailored to a specific database to identify studies that would provide insight into this topic. After each database was searched, titles and abstracts were screened, and a full text review was completed, only two articles remained. Despite a low yield, we believe important information can be gained from studying these two physician groups.
OPSCC will surpass the incidence of HPV-positive cervical cancer by 2020.34,35 These rapid changes demand that innovative solutions are developed to increase awareness among PCPs and the general population. Increasing educational efforts to PCPs has the potential to improve patient outcomes through increased vaccination efforts, early detection, and timely referral of patients presenting with early signs of malignancy
The paper by Jackowska et al. found that in Poland, GPs are less knowledgeable about HPV and its role in head and neck cancers. Although this study was not conducted in the United States, we believe it demonstrates an important issue; GPs who have the ability to act in a preventive manner through vaccination efforts were less knowledgeable about the potential use of the HPV vaccination for the prevention of HNCs. Although we expect specialists to be more knowledgeable, they are less able to play a preventive role due to most commonly only seeing patients after diseases have developed. Increasing vaccination efforts is predicated upon a strong knowledge base among GPs who have the ability to offer vaccinations to patients at appropriate ages and before diseases have developed. As in the United States, increasing the knowledge base of PCPs may have the largest effect on HPV-positive OPSCC through increased prevention, surveillance, and early detection.
development of educational resources tailored to address these gaps. By identifying areas where knowledge gaps exist and directing resources to address these gaps, educational programs can be maximized.
Our study is limited by the low yield from the search strategy and the potential of non-responder bias to have driven the results of each study. Although we acknowledge these studies may suffer from non-responder bias, similar low response rates for surveys have recently been reported among physicians.25,14. Additionally, title, abstract, and full text review was done by a single author. This could potentially bias the results by failing to include studies that may have been included if dual review was used. Finally, limiting the search to English language articles only could have missed studies published from OECD countries that did not have English translations. Furthermore, our study has several strengths, including a comprehensive search strategy collaboratively developed with the assistance of a professional librarian. Additionally, we searched three databases through two separate electronic libraries to ensure the thoroughness of the search. Although the yield was small and only single review was used, we believe the thoroughness of the search ensures that the majority of relevant articles were assessed.
References
1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893-2917. doi:10.1002/ijc.25516.
2. Chai RC, Lambie D, Verma M, Punyadeera C. Current trends in the etiology and diagnosis of HPV-related head and neck cancers. Cancer Med. 2015:n/a - n/a. doi:10.1002/cam4.424.
3. Marur S, D’Souza G, Westra WH, Forastiere AA. HPV-associated head and neck cancer: a virus-related cancer epidemic. Lancet Oncol. 2010;11(8):781-789. doi:10.1016/S1470-2045(10)70017-6.
4. Chaturvedi AK, Engels EA, Pfeiffer RM, et al. Human Papillomavirus and Rising Oropharyngeal Cancer Incidence in the United States. J Clin Oncol. 2011;29(32):4294-4301. doi:10.1200/JCO.2011.36.4596.
5. Gillison ML, D’Souza G, Westra W, et al. Distinct risk factor profiles for human papillomavirus type 16-positive and human papillomavirus type 16-negative head and neck cancers. J Natl Cancer Inst. 2008;100(6):407-420. doi:10.1093/jnci/djn025.
6. Ragin CCR, Taioli E. Survival of squamous cell carcinoma of the head and neck in relation to human papillomavirus infection: Review and meta-analysis. Int J Cancer. 2007;121(8):1813-1820. doi:10.1002/ijc.22851.
Clinical Trial. JNCI J Natl Cancer Inst. 2008;100(4):261-269. doi:10.1093/jnci/djn011.
8. Dayyani F, Etzel CJ, Liu M, Ho C-H, Lippman SM, Tsao AS. Meta-analysis of the impact of human papillomavirus (HPV) on cancer risk and overall survival in head and neck squamous cell carcinomas (HNSCC). Head Neck Oncol. 2010;2:15. doi:10.1186/1758-3284-2-15.
9. Jackowska J, Bartochowska A, Karlik M, Wichtowski M, Tokarski M, Wierzbicka M. The knowledge of the role of papillomavirus - Related head and neck pathologies among general practitioners, otolaryngologists and trainees. A survey-based study. PLoS One. 2015;10(10):1-10. doi:10.1371/journal.pone.0141003.
10. Griffiths E. Incidence of ENT problems in general practice. J R Soc Med. 1979;72(10):740-742. http://www.pubmedcentral.nih.gov/articlerender.fcgi? artid=1437201&tool=pmcentrez&rendertype=abstract.
11. Rourke T, Tassone P, Philpott C, Bath A. ENT cases seen at a local “walk-in centre”: a one year review. J Laryngol Otol. 2009;123(May 2008):339-342.
doi:http://dx.doi.org/10.1017/S0022215108002508.
12. Malloy KM, Ellender SM, Goldenberg D, Dolan RW. A survey of current practices, attitudes, and knowledge regarding human papillomavirus-related cancers and vaccines among head and neck surgeons. JAMA Otolaryngol Head Neck Surg. 2013;139(10):1037-1042. doi:10.1001/jamaoto.2013.4452.
14. Emery JD, Shaw K, Williams B, et al. The role of primary care in early detection and follow-up of cancer. Nat Rev Clin Oncol. 2014;11(1):38-48.
doi:10.1038/nrclinonc.2013.212.
15. Klozar J, Kratochvil V, Salakova M, et al. HPV status and regional metastasis in the prognosis of oral and oropharyngeal cancer. Eur Arch Oto-Rhino-Laryngology. 2008;265(SUPPL. 1). doi:10.1007/s00405-007-0557-9.
16. Boscolo-Rizzo P, Del Mistro A, Bussu F, et al. New insights into human papillomavirus-associated head and neck squamous cell carcinoma. Acta Otorhinolaryngol Ital organo Uff della Soc Ital di Otorinolaringol e Chir Cerv-facc. 2013;33(2):77-87.
http://www.pubmedcentral.nih.gov/articlerender.fcgi? artid=3665382&tool=pmcentrez&rendertype=abstract.
17. O’Rorke MA, Ellison M V., Murray LJ, Moran M, James J, Anderson LA. Human papillomavirus related head and neck cancer survival: A systematic review and meta-analysis. Oral Oncol. 2012;48(12):1191-1201. doi:10.1016/j.oraloncology.2012.06.019.
18. McIlwain WR, Sood AJ, Nguyen S a, Day T a. Initial Symptoms in Patients With HPV-Positive and HPV-Negative Oropharyngeal Cancer. JAMA Otolaryngol Head Neck Surg. 2014;140(5):1-7. doi:10.1001/jamaoto.2014.141.
19. Collins R, Flynn A, Melville A, Richardson R, Eastwood A. Effective health care: management of head and neck cancers. Qual Saf Health Care. 2005;14(2):144-148. doi:10.1136/qshc.2005.013961.
providers. Med Educ Online. 2012;17:17350. doi:10.3402/meo.v17i0.17350.
21. Signorelli C, Odone A, Pezzetti F, et al. Infezione da Papillomavirus umano e
vaccinazione : conoscenze e ruolo dei medici di medicina generale Human Papillomavirus infection and vaccination : knowledge and attitudes of Italian general practitioners. 2014;38(6):3-7.
22. Clamp PJ, Gunasekaran S, Pothier DD, Saunders MW. ENT in general practice: training, experience and referral rates. J Laryngol Otol. 2007;121(6):580-583.
doi:10.1017/S0022215106003495.
23. Chawdhary G, Ho EC, Minhas SS. Undergraduate ENT education: What students want.
Clin Otolaryngol. 2009;34(6):584-585. doi:10.1111/j.1749-4486.2009.02027.x.
24. Mohyuddin N, Langerman A, LeHew C, et al. Knowledge of Head and Neck Cancer Among Medical Students at 2 Chicago Universities. Arch Otolaryngol Neck Surg. 2008;134(12):1294. doi:10.1001/archotol.134.12.1294.
25. Cunningham CT, Quan H, Hemmelgarn B, et al. Exploring physician specialist response rates to web-based surveys. BMC Med Res Methodol. 2015;15:32. doi:10.1186/s12874-015-0016-z.
26. Westra WH. The changing face of head and neck cancer in the 21st century: the impact of HPV on the epidemiology and pathology of oral cancer. Head Neck Pathol. 2009;3(1):78-81. doi:10.1007/s12105-009-0100-y.
1999;10(4):412-418. doi:00001648-199907000-00009 [pii].
28. King T, Agulnik M. Head and Neck Cancer: Changing Epidemiology and Public Health Implications. Oncol J. 2010:6-8. www.cancer.gov/.../HeadandNeck-Snapshot.pdf.
29. Chera BS, Amdur RJ, Tepper J, et al. Phase 2 trial of de-intensified chemoradiation therapy for favorable-risk human papillomavirus-associated oropharyngeal squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2015;93(5):976-985.
doi:10.1016/j.ijrobp.2015.08.033.
30. Barnett ML, Song Z, Landon BE. Trends in physician referrals in the United States, 1999-2009 - with comments. Arch Intern Med. 2012;172(2):163-170.
doi:10.1001/archinternmed.2011.722.
31. Scott JR, Wong E, Sowerby LJ. Evaluating the referral preferences and consultation requests of primary care physicians with otolaryngology – head and neck surgery. J
Otolaryngol - Head Neck Surg. 2015;44(1):57. doi:10.1186/s40463-015-0114-2.
32. Gillison ML, Koch WM, Capone RB, et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. JNatlCancer Inst. 2000;92(9):709-720. http://www.ncbi.nlm.nih.gov/pubmed/10793107.
33. Malloy KM, Ellender SM, Goldenberg D, Dolan RW. A survey of current practices, attitudes, and knowledge regarding human papillomavirus-related cancers and vaccines among head and neck surgeons. JAMA Otolaryngol Head Neck Surg. 2013;139(10):1037-1042. doi:10.1001/jamaoto.2013.4452.
Cancer. Otolaryngol Clin North Am. 2012;45(4):739-764. doi:10.1016/j.otc.2012.04.003.
35. Gregoire V, Lefebvre J-L, Licitra L, Felip E. Squamous cell carcinoma of the head and neck: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21(Supplement 5):v184-v186. doi:10.1093/annonc/mdq185.
Figure 1. Prisma Diagram detailing article selection process from the three searched databases
Database Key Terms (connected with “AND”)
Expansion Terms (connected with “OR”)
PubMed Carcinoma, Squamous
cell
Otolaryngeal
Head and Neck
Neoplasm Neoplasms
Head and Neck Cancers
Alphapapillomavirus Human papillomavirus
Papillomavirus
infections Human
Papillomaviruses HPV
HPV-6
Primary Care Physicians Education
Early Detection of
Cancer
Practice Patterns,
Physicians
Health Knowledge,
Personnel
Healthcare Surveys
Specialists Surgical
CINHAL Carcinoma, Squamous
Cell
Neoplasms
Malignancy
Human Papillomavirus HPV
Papillomavirus
Alphapapillomavirus
Primary Care Physicians Pediatricians
Family medicine
Internal medicine
surgery
Surveys Medical Surveys
Knowledge
Attitudes
Beliefs
Practice Patterns
SCOPUS Neoplasms Malignancy
Cancer
Head and neck
oropharyngeal
Alphapapillomavirus
Primary Care Providers Family medicine
Internal medicine
pediatrics
Medical Surveys Surveys
Table 2. Key Inclusion and Exclusion Criteria
Key Inclusion and Exclusion Criteria
Key Inclusion Key Exclusion
Information pertaining to HPV-Positive: OPSCC
HNC
Information pertaining to HPV-negative OPSCC
HNC
Information obtained from PCPs
Pediatricians
Inernal Medicine Physicians Family Medicine Physicians Head and Neck Surgeons
Studies Using Modeling to Predict PCPs: Knowledge
Practice Patterns Attitudes
Beliefs
Included 1 of the following 3 key principles: Knowledge of PCPs
Information Obtained From: Surveys
Focus Groups Questionnaires
Information not obtained from: Surveys
Focus Groups Questionnaires
English Language Only Non-English Language Articles
Published in an OECD Country Published outside of an OECD Country
Table 3. Studies excluded during full text review with reasons for exclusion
Study Title Reason for Exclusion
North American Survey on HPV-DNA and p-16 testing for head and neck carcinoma
Survey results did not fulfill one of the 3 key principles of the current review
Human Papillomavirus infection and vaccination: knowledge and attitudes of Italian
general practitioners
Non-English Language Article
Cancers That U.S. Physicians Believe that the HPV Vaccine Prevents: Findings from a
Physician Survey , 2009
Did not include oropharynx or head and neck cancer
Educational value of a medical student-led head and neck cancer screening event
Did not include PCPs or head and neck surgeons
Awareness and knowledge of human papillomavirus-related diseases are still dramatically insufficient in the era of
coverage vaccination programs
Table 4. Article Specifics
Study Authors Journal Study Design Date Published
Malloy et al. JAMA
otolaryngology- head and neck surgery
Online Electronic Survey
August 29,2013
Jackowska et al. Plos ONE Online Electronic Survey
October 26, 2015
Table 5. Study Survey Response Rates
Study Authors Study Population Physicians surveyed Responses (Response Rate)
Malloy et al. American Head & Neck Society
Members
Head and Neck Surgeons
297 (27.5%)
Jackowska et al. Poland Physicians Head and Neck Surgeons, General
Practitioners and
Trainees
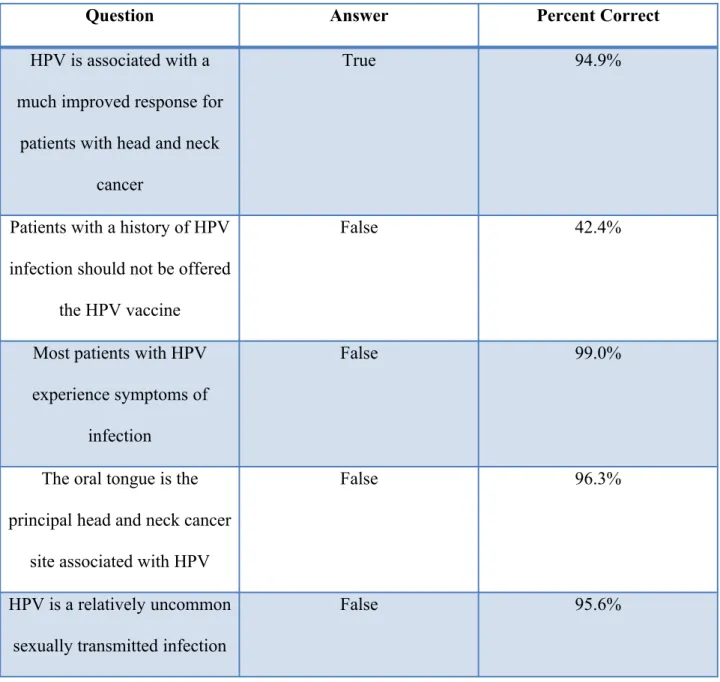
Table 6. Key knowledge questions from Malloy et al.
Question Answer Percent Correct
HPV is associated with a much improved response for
patients with head and neck cancer
True 94.9%
Patients with a history of HPV infection should not be offered
the HPV vaccine
False 42.4%
Most patients with HPV experience symptoms of
infection
False 99.0%
The oral tongue is the principal head and neck cancer
site associated with HPV
False 96.3%
HPV is a relatively uncommon sexually transmitted infection
All types of HPV can lead to head and neck cancer
False 96.3%
Table 7. Key practice questions from Malloy et al.
Question Options with response percentages
I Strongly Agree I somewhat Agree I somewhat Disagree I strongly Disagree
Pediatricians should remain the sole
appropriate source of information regarding the HPV vaccine
8.8% 22.9% 24.6% 44.3%
It is necessary to discuss issues of sexuality before recommending HPV vaccines to patients
23.2% 33.0% 23.2% 20.5%
The efficacy and safety of new vaccines can only be sufficiently established after the vaccine has been on the market for 5 to 10 years.
16.5% 43.1% 28.3% 12.1%
My patients are sufficiently informed of the risks of becoming infected with HPV and the
potential consequences of such an infection.
Table 8. Key questions and answers from Jackowska et al.
Question Answer with Response Percentage
General Practitioners Otolaryngologists
Have you heard about the impact of vaccination on the reduction of cervical cancer incidence?
Yes 100.0% No 0.0% Yes 100.0% No 0.0%
Have you heard about the potential value of HPV vaccination in preventing oropharyngeal cancer?
Yes 23.4% No 76.6% Yes 44.4% NO 55.6%
Have you heard about the association between HPV and upper aerodigestive tract tumors?