Cardiovascular Calcification and Bone:
A Comparison of The Effects of Dietary and
Serum Calcium, Phosphorous, Magnesium
and Vitamin D
Rachel Nicoll
1, John McLaren Howard
2and Michael Y Henein
11 Department of Public Health and Clinical Medicine and Heart Centre Umea University, Umea, Sweden
2 Acumen Lab, Tiverton, Devon, UK
Introduction
Osteoporosis and atherosclerosis are leading causes of
morbidity and mortality in the Western world. Although
these conditions commonly co-occur in older adults,
growing evidence suggests an association between vascular
calcification and skeletal fragility that is independent of age and
other shared risk factors. Older adults with the greatest bone
loss have the greatest progression of vascular calcification
1,2and the incidence of cardiovascular (CV) events is greater
in women with lower bone mass
3and in men with higher
levels of bone resorption
4,5. The association between both
pathologies also depends on the mechanisms involved in the
regulation of bone and CV metabolism
5. We have previously
shown that the nutrients and micronutrients that benefit the
CV system generally also benefit bone
6-8. In this article we
discuss the effect and interactions of the principal dietary bone
minerals (calcium, phosphorus, magnesium) and vitamin D on
CV calcification and bone health in principally older adults.
Where these studies also investigated other aspects of CV
health, we report these as well. Although other minerals, such
as potassium, sodium, selenium and zinc are known to be
involved in bone health, there are no human or animal studies
investigating their association with CV calcification, so we have
not included them. We have taken an effect on bone to mean an
effect on at least one skeletal site but not necessarily all sites.
Calcium
Calcium fulfils vital roles in the body, particularly with respect
to cell signalling functions; for this reason it is critical that
serum calcium be maintained in a very narrow range. There
are two modes of intestinal calcium absorption: active
transcellular absorption, mediated by 1,25(OH)2D binding to
the intestinal vitamin D receptor (VDR), and passive paracellular
absorption, dependent on the calcium gradient, with high intake
stimulating increased absorption independent of 1,25(OH)2D
9,10.
Active calcium absorption decreases when serum 25(OH)
D concentration is <20nmol/L and consequently low calcium
intake aggravates the consequences of vitamin D deficiency
9.
1,25(OH)2D also increases renal reabsorption of calcium
and upregulates bone resorption by facilitating osteoclast
maturation, thereby increasing serum calcium
11. Animal studies
demonstrate that maintaining normocalcaemia takes priority
over skeletal integrity because of calcium’s multiple intracellular
and extracellular roles
12. Dietary sources of calcium are mainly
dairy products, fish, legumes, grains and vegetables
13,14.
CV calcification
Observational studies generally show little association of
calcium intake, dietary or supplemental, with coronary artery
calcification (CAC) or abdominal aortic calcification (AAC)
incidence or extent in older adults
4,15-18, although a large
study showed that calcium intake was significantly higher in
postmenopausal men and women without AAC at baseline
and in women only after five years
19. Koreans with the highest
calcium intake (>840mg/d) also had improved serum lipid
profiles
20. Many studies of serum calcium show no association
with calcification
21-25, although some show a positive correlation
with presence, extent and progression of AAC in older
Abstract
210
Reviews | ICF November 2014 – Issue 5
adults
19,26-27, with mixed results for presence of CAC, although
there may be an association with extent or progression
18-19,28-29.
Serum calcium was an independent predictor of calcified
and mixed plaque but not non-calcified plaque
29and higher
concentrations were associated with lower in-hospital mortality
among MI patients
30. Nevertheless, serum calcium levels often
bear little relationship to intake, as is evidenced by the study by
Wang et al, where higher serum calcium was associated with
increased AAC but a higher calcium intake was found in those
with no AAC
19. Nunes has suggested that it is the deranged
metabolism of calcium and phosphorus, rather than the intake,
which may be promoting CV calcification, particularly in CKD
31.
Animal studies have shown that low calcium intake induces
higher nephrocalcinosis and aortic calcium content, while high
calcium intake is not generally associated with calcification in
health
32-34but in rats with chronic kidney disease (CKD) and
secondary hyperparathyroidism calcium supplementation
increased arterial calcification
35.
In view of the recent concern by Bolland et al that elevated
serum calcium or calcium supplementation, but not dietary
calcium, might increase CV events
36-38, a review and subsequent
studies found no evidence of any significant effect of calcium
supplementation on the risk of coronary artery disease
(CAD), stroke, CVD events
15,17,39. In fact, a systematic review
showed a strong association between calcium malnutrition
and risk of hypertension and CV events
40, while 1g/d calcium
supplementation was associated with lower CVD and CHD
risk after four years
41and reduced mortality in women after
10 years
42, with calcium supplementation protecting against
vascular disease by lowering serum cholesterol level and blood
pressure
43-44.
Bone
Although osteoporosis appears to have little association with
serum calcium
45, a review of observational studies found an
association of low calcium intake and osteoporosis risk
40, with
an intake threshold of <400mg/d
46. This may only be a
short-term association, possibly suggesting adaptation to a low
calcium intake
47. As with CV calcification, several recent
meta-analyses and systematic reviews of studies of healthy adults
have concluded that the evidence for an association between
calcium intake and BMD or fracture risk was insufficiently
clear
48-51, although a Cochrane Review and recent studies
have shown an effect of calcium supplementation on BMD
but not fracture incidence in postmenopausal women, with an
effective mean intake being >800mg/d
17,52-53, although much
higher intakes have reduced fracture risk in other studies
17,54-55.
Postmenopausal women possibly require a total intake of
>1100mg/d
56-58, although calcium may only be effective in the
first five postmenopausal years
59. Some of the inconsistent
results may be due to the fact that few studies measure
baseline calcium intake or status; supplementation in replete
subjects is unlikely to have a benefit
9. Furthermore, race may
account for some of the mixed results; among postmenopausal
women, there was a positive association between BMD and
calcium intake in white but not Hispanic, black or
Mexican-American women
60, whereas among older men there was a
correlation between BMD and calcium intake in blacks but not
whites
61. Where calcium intake has been found predictive of
BMD, the necessary intake for bone health appears to be >800
mg/day.
Phosphorus
Phosphate is critical for bone mineralisation but also for cell
signalling and energy storage in the form of ATP, requiring
strict control over blood concentrations, as with calcium
62.
The main dietary sources of organic phosphorus are animal
and plant proteins
63, while inorganic phosphorus is mostly
seen in food preservatives or as phosphoric acid in colas;
phosphoric acid may also bind with calcium in the intestine,
so preventing calcium absorption
64. Although up to 100%
of inorganic phosphorus may be absorbed, only 40-60%
of organic phosphorus is absorbed. Furthermore, much
of plant phosphorus is in the form of phytate (myo-inositol
hexakisphosphate), found principally in unrefined cereals and
legumes, which can inhibit absorption of several minerals by
forming non-digestible mineral complexes
65-66. As with calcium,
there are two mechanisms of phosphorus absorption: an active
1,25(OH)2D-dependent process, utilising sodium phosphate
co-transporters, and a passive diffusional process dependent on
the phosphorus gradient
62,66-69. Phosphorus restriction can also
increase synthesis of 1,25(OH)2D
70. There are growing concerns
that excess phosphorus intake from food additives and colas,
with concomitant decrease in calcium intake from vegetables,
in the general population may be a risk factor for CV disease,
osteoporosis and mortality, possibly through induction of
secondary hyperparathyroidism, even when serum phosphate
remains within the normal range
71.
CV calcification
In the few studies of the effect of dietary phosphorus on human
CV calcification there is no association in older Koreans
18,
although animal studies show a positive association between
phosphorus intake and aortic and renal calcification and
atheroma incidence
71-72. Two large studies by Linefsky et al
Low serum Ca
2+Increased resorption, releasing Ca
PTH
Low 1,25(OH)2D
R
Increased reabsorption of Ca + Mg
Increases PTH secretion
25(OH)D
1,25(OH)2D
Ca + Mg
PTH inhibition
Increased Ca + Mg absorption
Increased Ca, Mg and 1,25(OH)2D
Circulation
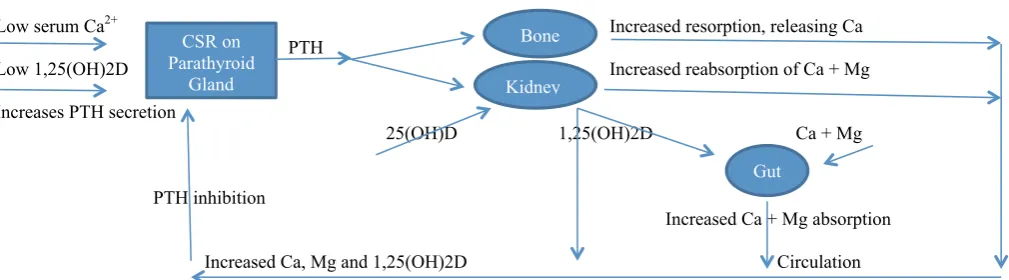
Figure 1. Mechanism by which low serum calcium (Ca), magnesium (Mg) or 1,25(OH)2D impacts the parathyroid gland, bone, kidney and the gut to
raise serum Ca
High serum P
PTH
Reduced reabsorption of P
PTH inhibition
High Ca
Low P
High 1,25(OH2D
Circulation
Figure 2. Mechanism by which high serum phosphate (P) impacts the parathyroid gland and kidney to lower serum P
CSR on
Parathyroid
Gland
Kidney
Bone
Gut
Parathyroid
Gland
Kidney
211
ICF November 2014 – Issue 5 | Reviews
found a significant association between baseline mean serum
phosphate levels (>1.292mmol/l vs ≤0.969mmol/l) and baseline
aortic valve calcification (AVC), mitral annulus calcification
(MAC) and AAC presence but not with extent, progression or
new development after a mean of 2.4 years; the association
with AAC lost significance after adjustment
25,73. These studies
demonstrate that even a serum phosphate value within
the reference range (0.8-1.4mmol/l) is associated with CV
calcification, as well as increased CV risk [66]. Studies of older
adults and CKD patients also found a significant association
between higher serum phosphate and presence and extent
of calcification
18,21,22,26,28,29, with each 0.0323mmol/l rise in
serum phosphorus being associated with 6.1% higher odds
of having CAC
21. Wang et al found a gender difference; in
postmenopausal women, serum phosphate was significantly
higher (1.15 vs 1.17 mmol/l) in subjects with AAC, while in older
men there was no association
19. Elevated serum phosphate
was also associated with coronary obstructive lesions and CV
events, although results for mortality were mixed
21,74-75. A similar
association with arterial and valvular calcification and increased
carotid intima/media thickness (cIMT) is generally seen in CKD,
although the serum phosphate levels tend to be considerably
higher
23,76-79and are due to failure to excrete excess phosphate,
which may be the driver for ectopic calcification
80. In CKD,
arterial calcification can be suppressed by reducing serum
phosphate levels, even in the presence of high serum calcium
and 1,25-dihydroxyvitamin D levels
81. CKD rats showed
phosphorus intake-dependent increases in markers of
inflammation and oxidative stress as well as CV calcification
and mortality
82, while VSMCs cultured in normal levels of
phosphorus do not calcify
79but high inorganic phosphorus
can induce calcification, endothelial dysfunction and increased
markers of inflammation
21,79,82,83.
Bone
Results of adult human studies show mixed results for
associations between total phosphorus intake and osteoporosis
or fractures
84-86, although inorganic phosphorus intake from
colas induced a higher incidence of osteopenia and lower BMD
among women only; since this was not seen with other soft
drinks it is likely to be attributable to phosphoric acid
64. Among
healthy women, dietary and serum phosphorus were generally
not associated with BMD or markers of bone formation or
resorption
45,85,87. Phosphorus supplementation in young women
resulted in decreased markers of bone formation and increased
markers of resorption
88but had no adverse effect on young
men
89. A further intervention study found that the adverse
effects of high phosphorus supplementation could be negated
by high calcium supplementation
90. Animal studies show that
diets creating either a phosphorus excess or deficiency lower
BMD and bone mineralisation
71,91.
Magnesium
Magnesium is an essential mineral, acting as cofactor in more
than 300 enzymatic reactions. It is a natural calcium channel
blocker and plays an important role in CV, neurological and
metabolic functions, although approximately 60% of body
magnesium is found in bone
92. Dietary sources include legumes,
vegetables, nuts, seeds, fruits, grains, fish and dairy foods
93. As
with calcium and phosphorus, there is a vitamin D-dependent
intestinal absorption and gradient-driven absorption
94.
Ectopic calcification
The principal intake study found that CV calcification was
lowest in the quartile with intake ranging from 384-669mg/d
95,
while higher intake was inversely associated with stroke risk
39,
diabetes incidence and hypertension
96. The only studies of
blood concentrations involve dialysis patients and show a clear
association between lower serum magnesium (1.1056mmol/l
vs 1.241mmol/l) and peripheral artery calcification
97-98and
MAC
99, the protective amount being above the reference
range (upper limit 1.2mmol/l), although this should not be
extrapolated to non-renal patients. Serum magnesium was
also inversely correlated with cIMT and aortic pulse wave
velocity in renal and non-renal patients
100. In animals, a low
magnesium diet increased cardiac magnesium and calcium
deposition
72,100-102but the CV and renal calcification was
worse when low magnesium intake was combined with high
phosphorus
102-103. Experimental magnesium deficiency also
induced arterial damage, hypertriglyceridaemia and a decrease
in HDL cholesterol transport
104. A high magnesium intake,
however, was associated with a reduction in plasma cholesterol
and triglycerides in rats
105. There are no trials of magnesium
supplementation on CV calcification in humans but in renal
patients supplementation resulted in significantly lower cIMT
106,
while in animals supplementation dose-dependently lowered
myocardial, carotid and aortic calcium content
107,108. Similarly, in
vitro studies showed that increasing magnesium concentration
reduced calcification in VSMC
83,100.
Bone
Dietary and serum, but not red cell, magnesium were generally
lower among the elderly with osteoporosis
45,86,109and among
healthy older adults, magnesium intake was positively
associated with BMD, BMC and bone mass
86,110-111, with an
intake of >422.5mg/d vs <206.5 mg/d improving BMD
110. A
large multiethnic study found that this association may apply
to older whites but not blacks
112. Some studies also found an
association with BMD in younger women
113-114. Study results are
mixed with respect to intake and fracture risk
84,110,115and among
Japanese subjects low serum magnesium was associated with
increased fracture incidence
116. Short term intervention studies
Increases PTH secretion
25(OH)D
1,25(OH)2D
Ca + Mg
PTH inhibition
Increased Ca + Mg absorption
Increased Ca, Mg and 1,25(OH)2D
Circulation
Figure 1. Mechanism by which low serum calcium (Ca), magnesium (Mg) or 1,25(OH)2D impacts the parathyroid gland, bone, kidney and the gut to
raise serum Ca
High serum P
PTH
Reduced reabsorption of P
PTH inhibition
High Ca
Low P
High 1,25(OH2D
Circulation
Figure 2. Mechanism by which high serum phosphate (P) impacts the parathyroid gland and kidney to lower serum P
Gut
Parathyroid
Gland
Kidney
212
Reviews | ICF November 2014 – Issue 5
show that 1830mg/d magnesium citrate significantly decreased
levels of urinary deoxypyridinoline (a marker of bone resorption)
in postmenopausal osteoporotic women with normal baseline
serum magnesium and calcium, while concentrations of serum
osteocalcin (a marker of bone turnover) were increased
117but there was no effect in young women
118. Longer studies
of postmenopausal women with low BMD showed that
magnesium supplementation increased BMD
119-120.
Vitamin D
Vitamin D is a steroid hormone which has multiple roles in the
body, in particular an autocrine function, which acts to promote
skeletal health, and an endocrine function, which includes
maintenance of serum calcium within a narrow range
121. Since
serum calcium homeostasis is of vital importance, the endocrine
function can often operate to the detriment of the autocrine
function
122, which may account for the lack of clear results in
vitamin D studies. Low serum calcium or phosphate triggers the
synthesis of the vitamin D metabolite 1,25(OH)2D in kidney and
bone, which in turn binds to the intestinal vitamin D receptor
(VDR) and increases intestinal calcium
10,123, phosphorus
62,67-69and magnesium
94absorption and renal reabsorption but also
inhibits bone mineralisation
62and upregulates bone resorption
by facilitating osteoclast maturation to release calcium and
phosphate, thereby increasing serum concentrations
11.
Active calcium absorption decreases when serum 25(OH)
D concentration is <20nmol/L and consequently low calcium
intake aggravates the consequences of vitamin D deficiency
123.
There is a decreasing ability with age to synthesise either
25(OH)D or 1,25(OH)2D as well as intestinal resistance to its
action
124-125; it appears that the optimal level of serum 25(OH)
D for calcium absorption is >80nmol/l in postmenopausal
women
126. Vitamin D also has key roles in CV health, as
indicated by the presence of the VDR in cardiomyocytes,
vascular endothelial cells and VSMCs
127. The principal source
of vitamin D is sunlight on skin but foods such as egg yolk,
offal, oily fish and shellfish also provide some intake, as well as
fortified foods
124,125.
Ectopic calcification
There are no human intake studies with respect to CV
calcification, probably because dietary vitamin D provides
only a relatively small contribution to serum 25(OH)D. Animal
studies, however, show that high vitamin D intake can induce
CV calcification and impair endothelial function
128,129but
they also show that a vitamin D deficient diet can induce an
increase in calcified lesions
130-132, indicating that both excess
and deficiency are detrimental. Several epidemiological
studies measuring serum 25(OH)D demonstrate an absence
of association with presence or extent of CAC, MAC, cIMT,
degree of carotid stenosis or mean arterial pressure
22,133-135,
although patients with calcific aortic stenosis
136and poor
coronary collateral circulation
137had significantly lower serum
25(OH)D. After three years serum 25(OH)D was associated
with new CAC development, but not CAC progression, with
those with serum 25(OH)D of <37.55nmol/l having increased
risk
133. The association is usually clearer in those with previously
diagnosed disease. In CKD patients, arterial calcification was
significantly inversely associated with serum 25(OH)D
24and
a high peripheral arterial calcification score was significantly
associated with lower 25(OH)D concentrations
138. Similarly in
type 1 diabetics, serum 25(OH)D <49.9nmol/l was associated
with the presence and development of CAC after 3 years
139,
with valvular calcification in dilated cardiomyopathy patients
(serum 25(OH)D <75nmol/l)
140and with the calcification score
in peripheral arterial disease
27. Likewise with respect to serum
1,25(OH)2D, some studies show no association with CAC
extent or progression
133,141, although in subjects at risk for CHD,
serum 1,25(OH)2D was inversely correlated with the extent of
calcification
142.
There have been few intervention studies of vitamin D alone
but in CKD patients the incidence of aortic calcification
was significantly lower in treated patients
143, while in heart
failure, 4000IU/d for six months significantly improved
the left ventricular ejection fraction
144. Trials of vitamin D
supplementation combined with calcium showed that up to
1000g/d calcium plus 400 IU/d vitamin D3 did not affect CAC
scores or incidence of myocardial infarction (MI), CHD mortality
or stroke in postmenopausal women
145-146, although there was
an improvement in dyslipidaemia
147; this lack of result may be
because the vitamin D dose was low. Nevertheless, although
a 2011 systematic review found that serum 25(OH)D was not
significantly associated with mortality, MI or stroke
148, a
meta-analysis of RCTs found that vitamin D supplementation for at
least three years significantly decreased all-cause mortality
149.
Bone
A 2006 systematic review and more recent studies of older
adults showed that a vitamin D intake of ≥400 IU/d was
associated with reduced bone loss
150-152but with respect to
fracture incidence, there appears to be little association with
vitamin D intake
115. Two large reviews found that in older adults,
serum 25(OH)D was positively associated with BMD but there
was inconsistent evidence for an association with fractures
153.In elderly postmenopausal women, those with serum 25(OH)
D levels <50 nmol/L had increased fracture risk, bone loss and
mortality, leading to recommendations that 50nmol/L should be
the minimum level to ensure optimum bone health, below which
supplementation is recommended at 800-1000IU/d but above
High serum P
FGF23
Reduced reabsorption of P
PTH inhibition
Decreased synthesis
Low serum Ca
of 1,25(OH)2D decreases
Low serum P
intestinal P absorption
Circulation
Figure 3. Mechanism by which high serum phosphate (P) triggers release of FGF23 to lower serum P
Bone
Kidney
except in fragile elderly subjects, for whom serum 25(OH)
D should be ≥75nmol/l
154. Recent Korean studies confirm the
positive association, which may not be linear
155and indicate
that BMD increases until 25(OH)D ≥70mmol/l in men and 50
nmol/l in women
156. Ethnicity may have a bearing on the effect
of vitamin D. A prospective study showed that higher
25(OH)D levels were associated with a lower risk of fracture in
white women but a higher risk in black and Asian women and
no association in Hispanic or Native American women
157; the
NHANES study showed that mean 25(OH)D levels were highest
in whites and lowest in blacks yet blacks had the highest BMD
and whites had the lowest
158.
When additionally considering calcium intake, the combination
of higher vitamin D and calcium were associated with higher
BMD in young adults
159and reduced osteoporosis risk in
postmenopausal women
47, with the optimum dose for fracture
reduction being 700-800IU/d vitamin D3 with 500-1200mg/d
calcium
153. Animal studies confirm that a diet deficient in
calcium and vitamin D lowers BMD and increases urinary
excretion of markers of bone resorption, not seen in calcium or
vitamin D deficiency alone
160. In humans, BMD and BMC loss
and fracture risk were more consistently inversely associated
with calcium intake and serum 25(OH)D taken together among
all agegroups than either nutrient taken alone
150,155. Three recent
reviews and meta-analyses of intervention studies found that
vitamin D supplementation alone did not prevent fractures or
increase BMD; the two reviews found a protective effect of
vitamin D with calcium but results of the meta-analysis depend
on the authors’ ‘futility boundary’
161-163. A further meta-analysis
found that in older adults, supplementation of 800IU/d could
significantly reduce hip fractures and associated deaths over
one year
164.
Other multinutrient interactions
Lappe and Heaney point out that nutrient trials may fail because
of inadequate attention to co-nutrient optimisation, including
protein
165. One of the most important mineral partnerships is
that of calcium and phosphorus, with the calcium/phosphorus
ratio in bone being 2.2:1
166. An intake ratio of <1.0 was
associated with nephrocalcinosis in rats but increasing the ratio
to 1.3 inhibited calcification development
167, while a low intake
ratio increased osteoporosis risk in Koreans
168and increased
bone resorption markers
169but a ratio of at least ≥0.74 benefited
bone among younger females
87,170. Although phosphorus
restriction increases serum ionised calcium
70, phosphorus
supplementation was also associated with decreased urinary
calcium excretion
126,171, suggesting that calcium is retained
to bind the phosphorus. There is also a strong interaction
between calcium and magnesium, with low magnesium intake
in animals increasing serum calcium, the calcium/phosphate
ratio and calcium deposition in bone
172-173but with high calcium
intake, serum and tissue magnesium was lower, suggesting
decreased absorption
174. High magnesium intake in calcium
sufficiency, however, significantly improved all bone parameters
compared to calcium insufficiency and when supplemented
together, there was a significant improvement to all bone
parameters
175. There is competitive inhibition of
gradient-dependent intestinal absorption, not only between magnesium
and calcium
67,94but also between magnesium and phosphorus
provided calcium is adequate but magnesium absorption may
increase at the expense of phosphorus when serum calcium
is low
94. Magnesium depletion is associated with increased
serum ionised magnesium and calcium and decreased ionised
phosphate
101,102. Magnesium also interacts with vitamin D, such
even during dietary calcium deprivation
176and can lead on to
resistance to 1,25(OH)2D
177.
Mechanisms
As well as vitamin D, additional regulators of CV calcification
and bone mineralisation include parathyroid hormone (PTH)
178and fibroblast growth factor 23 (FGF23), a phosphotonin
secreted from bone, which appears to be a counter-regulatory
hormone for vitamin D
179. Figures 1-3 demonstrate how all three
are involved in the regulation of serum calcium, phosphate and
magnesium. Optimal PTH concentrations have been found
when 25(OH)D ≥80nmol/l
180,181, while elevated FGF23 was
associated with the CAC score in haemodialysis patients
182and even among healthy subjects, the highest FGF23 quartile
was associated with higher CAC scores and greater risk of
heart failure and CHD
183. Elevated serum phosphate can impair
endothelial function, as evidenced by decreased vasodilatation,
and may promote transdifferentation of VSMCs to
osteoblast-like cells
71.
Discussion
Although most studies show little association between calcium
intake and CV calcification or BMD and fracture risk, the large
study showing a positive correlation between higher intake
and absence of AAC and the review showing an association
between low intake and osteoporosis indicate that a higher
intake is preferable. BMD studies indicate that this should
be >800mg/d, with 1100mg/d for postmenopausal women,
although larger doses were required for fracture prevention.
Possibly the studies show a lack of association because even
in the higher quartiles, intake is still too low. Serum calcium
studies also generally show no association with CV calcification
or bone, although a few show a positive association with AAC,
but an association between serum calcium and bone would
not be expected, since bone is a calcium reservoir to maintain
serum levels. Bone studies also highlight the fact that ethnicity
may distort results, which may be equally applicable to CV
studies. There is no evidence that calcium supplementation
increases CV risk; in fact calcium appears beneficial for
prevention of CV events and mortality and can lower cholesterol
and blood pressure.
214
Reviews | ICF November 2014 – Issue 5
Although human observational studies for vitamin D intake and
CV calcification are lacking, animal studies show a U-shaped
dose/response curve for intake, while bone studies found that
intake of >/=400IU/d is required to reduce bone loss. Serum
25(OH)D is generally not correlated with CV calcification, except
in CKD and other already-diagnosed conditions, where it is
inversely associated, but in bone, serum 25(OH)D is positively
associated with BMD. Intervention studies show reduced CV
calcification in CKD, improved ventricular function in heart
failure and lower mortality in longer term studies but no effect
on CV calcification in healthy postmenopausal women, either
alone or when accompanied by calcium, although the vitamin
D dose was low (400IU/d). The vitamin D/calcium combination
is beneficial to bone, however, provided the vitamin D dose
is adequate. Bone studies indicate that supplementation of
>/=800IU/d is required to bring serum 25(OH)D up to 50nmol/l
in healthy adults or >/=75nmol/l in the fragile elderly. Ethnicity
may again affect results, with higher 25(OH)D giving a higher
fracture risk in black and Asian women. It is difficult to assess
the CV or bone effects of vitamin D alone, since its predominant
function is to maintain serum calcium homeostasis and it will do
this to the detriment of bone or arteries if necessary; baseline
serum calcium is seldom measured in these studies.
These studies highlight the interactions between the different
micronutrients and point up the need for a calcium phosphorus
intake in the ratio of >1 for bone health, which may also
translate to arteries. Because of the competitive inhibition of
absorption if intake of one mineral is imbalanced, it is important
that adequate, but not excessive, intake of all bone minerals is
maintained for both artery and bone health.
Conclusion
This review has firstly demonstrated that a mineral and
vitamin D intake that is beneficial for bone is also generally
protective against CV calcification. In principal this involves
ensuring an adequate intake through diet or supplementation
of each mineral and, in particular, supplementing sufficient
calcium to balance any increased phosphorus intake to avoid
upregulating PTH and to prevent a catabolic effect of vitamin
D supplementation on bone to maintain serum calcium. These
relationships may, however, not hold among African Americans
and Asians. It has secondly shown the striking inter-relationship
between the three bone minerals and vitamin D. This is
particularly true with calcium, magnesium and vitamin D, where
one can, to a certain extent, substitute for the other in the short
term in maintaining bone health. Bone studies show limited
effect when considering calcium and vitamin D separately but
when supplemented together there is a significant protective
effect. The competitive inhibition of absorption between all
three minerals further emphasises that the diet should contain
adequate levels of all three. The concern over the effect of
supplemental calcium and CV events appears unnecessary
since there is no evidence of any significant detrimental effects,
whereas calcium supplementation may in fact be protective.
Correspondence to:
Rachel Nicoll MSc
Department of Public Health and Clinical Medicine and Heart
Centre
Umea University
Sweden
E-mail: [email protected]
References:
1 Kiel DP, Kauppila LI, Cupples LA, Hannan MT, O’Donnell CJ, Wilson PW. Bone loss and the progression of abdominal aortic calcification over a 25 year period: the Framingham Heart Study. Calcif Tissue Int 2001;68:271–6 2 Zhou R, Zhou H, Cui M, Chen L, Xu J. The Association between Aortic
Calcification and Fracture Risk in Postmenopausal Women in China: The Prospective Chongqing Osteoporosis Study. PLoS One. 2014 May 9;9(5):e93882
3 Samelson EJ, Kiel DP, Broe KE, Zhang Y, Cupples LA, Hannan MT, Wilson PW, Levy D, Williams SA, Vaccarino V. Metacarpal cortical area and risk of coronary heart disease: the Framingham Study. Am J Epidemiol 2004;159:589–95
4 Samelson EJ, Booth SL, Fox CS, Tucker KL, Wang TJ, Hoffmann U, Cupples LA, O’Donnell CJ, Kiel DP. Calcium intake is not associated with increased coronary artery calcification: the Framingham Study. Am J Clin Nutr. 2012 Dec;96(6):1274-80
5 Szulc P. Association between cardiovascular diseases and osteoporosis-reappraisal. Bonekey Rep. 2012 Aug 8;1:144
6 Nicoll R, McLaren Howard J, Henein M. Cardiovascular and renal calcification and bone: A comparison of the effects of dietary fatty acids. International Cardiovascular Forum. 2014; 3: 127-131
7 Nicoll R, McLaren Howard J, Henein M. Ectopic calcification and bone: A comparison of the effects of dietary carbohydrates, sugars and protein. International Cardiovascular Forum. 2014; 4: In press
8 Nicoll R, McLaren Howard J, Henein M. Cardiovascular calcification and bone: A comparison of the effects of dietary antioxidants. International Cardiovascular Forum. 2014; 5: In press
9 Lips P. Interaction between vitamin D and calcium’. Scand J Clin Lab Invest Suppl. 2012; 243: 60-4
10 Dawson-Hughes B, Bischoff-Ferrari HA. ‘Therapy of osteoporosis with calcium and vitamin D’. J Bone Miner Res. 2007; 22 (Suppl 2): V59-V63 11 Weaver CM. ‘2003 W.O. Atwater Memorial Lecture: Defining Nutrient
Requirements from a Perspective of Bone-Related Nutrients’. Am Soc Nutr Sci. 2003; 133: 4063-6
12 Brown EM. Role of the calcium-sensing receptor in extracellular calcium homeostasis. Best Pract Res Clin Endocrinol Metab. 2013 Jun;27(3):333-43
13 Cook AJ, Friday JE. Food mixture or ingredient sources for dietary calcium: shifts in food group contributions using four grouping protocols. J Am Diet Assoc. 2003
14 Ishida H. Nutrition and bone health. Calcium-rich foods and bone. Clin Calcium. 2009 Nov;19(11):1670-7
15 Spence LA, Weaver CM. Calcium intake, vascular calcification, and vascular disease. Nutr Rev. 2013 Jan;71(1):15-22
16 Kim JH, Yoon JW, Kim KW, Lee EJ, Lee W, Cho SH, Shin CS. Increased dietary calcium intake is not associated with coronary artery calcification. Int J Cardiol. 2012 Jun 14;157(3):429-31
17 Radford LT, Bolland MJ, Mason B, Horne A, Gamble GD, Grey A, Reid IR. The Auckland calcium study: 5-year post-trial follow-up. Osteoporos Int. 2014 Jan;25(1):297-304
18 Kwak S, Kim JS, Choi Y, Chang Y, Kwon MJ, Jung JG, Jeong C, Ahn J, Kim HS, Shin H, Ryu S. Dietary Intake of Calcium and Phosphorus and Serum Concentration in Relation to the Risk of Coronary Artery Calcification in Asymptomatic Adults. Arterioscler Thromb Vasc Biol. 2014 Jun 12. [Epub ahead of print]
19 Wang TK, Bolland MJ, van Pelt NC, Horne AM, Mason BH, Ames RW, Grey AB, Ruygrok PN, Gamble GD, Reid IR. Relationships between vascular calcification, calcium metabolism, bone density, and fractures. J Bone Miner Res. 2010 Dec;25(12):2777-85
20 Kim JH, Yoon JW, Kim KW, Lee EJ, Lee W, Cho SH, Shin CS. Increased dietary calcium intake is not associated with coronary artery calcification. Int J Cardiol. 2012 Jun 14;157(3):429-31
21 Cancela AL, Santos RD, Titan SM, Goldenstein PT, Rochitte CE, Lemos PA, dos Reis LM, Graciolli FG, Jorgetti V, Moysés RM. Phosphorus is associated with coronary artery disease in patients with preserved renal function. PLoS One. 2012;7(5):e36883
22 Park KS, Chang JW, Kim TY, Kim HW, Lee EK, Kim HS, Yang WS, Kim SB, Park SK, Lee SK, Park JS. Lower concentrations of serum phosphorus within the normal range could be associated with less calcification of the coronary artery in Koreans with normal renal function. Am J Clin Nutr. 2011 Dec;94(6):1465-70
23 Srivaths PR, Goldstein SL, Silverstein DM, Krishnamurthy R, Brewer ED. Elevated FGF 23 and phosphorus are associated with coronary calcification in hemodialysis patients. Pediatr Nephrol. 2011 Jun;26(6):945-51
24 García-Canton C, Bosch E, Ramírez A, Gonzalez Y, Auyanet I, Guerra R, Perez MA, Fernández E, Toledo A, Lago M, Checa MD. Vascular calcification and 25-hydroxyvitamin D levels in non-dialysis patients with chronic kidney disease stages 4 and 5. Nephrol Dial Transplant. 2011 Jul;26(7):2250-6
study. J Am Coll Cardiol. 2011 Jul 12;58(3):291-7
26 Figueiredo CP, Rajamannan NM, Lopes JB, Caparbo VF, Takayama L, Kuroishi ME, Oliveira IS, Menezes PR, Scazufca M, Bonfá E, Pereira RM. Serum phosphate and hip bone mineral density as additional factors for high vascular calcification scores in a community-dwelling: the São Paulo Ageing & Health Study (SPAH). Bone. 2013 Jan;52(1):354-9
27 Zagura M, Serg M, Kampus P, Zilmer M, Eha J, Unt E, Lieberg J, Cockcroft JR, Kals J. Aortic stiffness and vitamin D are independent markers of aortic calcification in patients with peripheral arterial disease and in healthy subjects. Eur J Vasc Endovasc Surg. 2011 Nov;42(5):689-95
28 Tuttle KR, Short RA. Longitudinal relationships among coronary artery calcification, serum phosphorus, and kidney function. Clin J Am Soc Nephrol. 2009 Dec;4(12):1968-73
29 Shin S, Kim KJ, Chang HJ, Cho I, Kim YJ, Choi BW, Rhee Y, Lim SK, Yang WI, Shim CY, Ha JW, Jang Y, Chung N. Impact of serum calcium and phosphate on coronary atherosclerosis detected by cardiac computed tomography. Eur Heart J. 2012 Nov;33(22):2873-81 30 Lu X, Wang Y, Meng H, Chen P, Huang Y, Wang Z, Zhou N, Li C, Wang
L, Jia E, Yang Z. Association of Admission Serum Calcium Levels and In-Hospital Mortality in Patients with Acute ST-Elevated Myocardial Infarction: An Eight-Year, Single-Center Study in China. PLoS One. 2014 Jun 13;9(6):e99895
31 Nunes JP. The case for dietary calcium restriction in patients with atherosclerosis. Med Hypotheses. 2005;65(3):521-4
32 Agata U, Park JH, Hattori S, Iimura Y, Ezawa I, Akimoto T, Omi N. ‘The effect of different amounts of calcium intake on bone metabolism and arterial calcification in ovariectomised rats’. J Nutr Sci Vitaminol (Tokyo). 2013; 59(1): 29-36
33 Phillips JC, Bex C, Mendis D, Gangolli SD. Studies on the mechanism of diet-induced nephrocalcinosis: calcium and phosphorus metabolism in the female rat. Food Chem Toxicol. 1986 Apr;24(4):283-8
34 Hsu HH, Culley NC. Effects of dietary calcium on atherosclerosis, aortic calcification, and icterus in rabbits fed a supplemental cholesterol diet. Lipids Health Dis. 2006 Jun 23;5:16
35 Moe SM, Chen NX, Newman CL, Gattone VH 2nd, Organ JM, Chen X, Allen MR. A Comparison of Calcium to Zoledronic Acid for Improvement of Cortical Bone in an Animal Model of CKD. J Bone Miner Res. 2014 Apr;29(4):902-10
36 Bolland MJ, Barber PA, Doughty RN, et al. Vascular events in healthy older women receiving calcium supplementation: randomised controlled trial. BMJ. 2008;336(7638):262–6.
37 Bolland MJ, Avenell A, Baron JA, et al. Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ 2010;341: c3691
38 Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR. Calcium supplements with or without vitamin d and risk of cardiovascular events: reanalysis of the women’s health initiative limited access dataset and meta-analysis. BMJ 2011;342:d2040
39 Sluijs I, Czernichow S, Beulens JW, Boer JM, van der Schouw YT, Verschuren WM, Grobbee DE. Intakes of Potassium, Magnesium, and Calcium and Risk of Stroke. Stroke. 2014 Feb 11. [Epub ahead of print] 40 Peterlik M, Kállay E, Cross HS. Calcium nutrition and extracellular calcium
sensing: relevance for the pathogenesis of osteoporosis, cancer and cardiovascular diseases. Nutrients. 2013 Jan 22;5(1):302-27
41 Paik JM, Curhan GC, Sun Q, Rexrode KM, Manson JE, Rimm EB, Taylor EN. Calcium supplement intake and risk of cardiovascular disease in women. Osteoporos Int. 2014 May 7. [Epub ahead of print]
42 Langsetmo L, Berger C, Kreiger N, Kovacs CS, Hanley DA, Jamal SA, Whiting SJ, Genest J, Morin SN, Hodsman A, Prior JC, Lentle B, Patel MS, Brown JP, Anastasiades T, Towheed T, Josse RG, Papaioannou A, Adachi JD, Leslie WD, Davison KS, Goltzman D; CaMos Group. Calcium and vitamin D intake and mortality: results from the Canadian Multicentre Osteoporosis Study (CaMos). J Clin Endocrinol Metab. 2013 Jul;98(7):3010-8
43 Reid IR, Mason B, Horne A et al. Effects of calcium supplementation on serum lipid concentrations in normal older women: a randomized controlled trial. Am J Med, 112 (5) (2002), pp. 343–347
44 Griffith LE, Guyatt GH, Cook RJ, Bucher HC, Cook DJ. The influence of dietary and nondietary calcium supplementation on blood pressure: an updated metaanalysis of randomized controlled trials. Am J Hypertens 1999;12(1 Pt 1):84–92
45 Okyay E, Ertugrul C, Acar B, Sisman AR, Onvural B, Ozaksoy D. Comparative evaluation of serum levels of main minerals and postmenopausal osteoporosis. Maturitas. 2013 Dec;76(4):320-5 46 Kung AW, Lee KK, Ho AY, Tang G, Luk KD. Ten-year risk of osteoporotic
fractures in postmenopausal Chinese women according to clinical risk factors and BMD T-scores: a prospective study. J Bone Miner Res. 2007 Jul;22(7):1080-7
47 Nieves JW, Barrett-Connor E, Siris ES, Zion M, Barlas S, Chen YT. Calcium and vitamin D intake influence bone mass, but not short-term fracture risk, in Caucasian postmenopausal women from the National
May;19(5):673-9
48 Papaioannou A, Kennedy CC, Cranney A, Hawker G, Brown JP, Kaiser SM, Leslie WD, O’Brien CJ, Sawka AM, Khan A, Siminoski K, Tarulli G, Webster D, McGowan J, Adachi JD. Risk factors for low BMD in healthy men age 50 years or older: a systematic review. Osteoporos Int. 2009 Apr;20(4):507-18
49 Moyer VA; on behalf of the US Preventive Services Task Force. ‘Vitamin D and calcium supplementation to prevent fractures in adults: US Preventive Services Task Force Recommendation Statement’. Ann Intern Med. 2013; Epub ahead of print
50 Waugh EJ, Lam MA, Hawker GA, McGowan J, Papaioannou A, Cheung AM, Hodsman AB, Leslie WD, Siminoski K, Jamal SA; Perimenopause BMD Guidelines Subcommittee of Osteoporosis Canada. Risk factors for low bone mass in healthy 40-60 year old women: a systematic review of the literature. Osteoporos Int. 2009 Jan;20(1):1-21
51 Bischoff-Ferrari HA, Dawson-Hughes B, Baron JA, Buckhardt P, Li R, Spiegelman D et al. ‘Calcium intake and hip fracture risk in men and women: a meta-analysis of prospective cohort studies and randomised controlled trials’. Am J Clin Nutr. 2007; 86(6): 1780-90
52 Shea B, Wells G, Cranney A, Zytaruk N, Robinson V, Griffith L, Hamel C, Ortiz Z, Peterson J, Adachi J, Tugwell P, Guyatt G; Osteoporosis Methodology Group; Osteoporosis Research Advisory Group. Calcium supplementation on bone loss in postmenopausal women. Cochrane Database Syst Rev. 2004;(1):CD004526
53 Nakamura K, Saito T, Kobayashi R, Oshiki R, Kitamura K, Oyama M et al. ‘Effect of low-dose calcium supplements on bone loss in perimenopausal and postmenopausal Asian women: a randomised controlled trial’. J Bone Mineral Res. 2012; 27(11): 2264-70
54 Dionyssiotis Y, Paspati I, Trovas G, Galanos A, Lyritis GP. Association of physical exercise and calcium intake with bone mass measured by quantitative ultrasound. BMC Womens Health. 2010 Apr 7;10:12 55 Babaroutsi E, Magkos F, Manios Y, Sidossis LS. Body mass index,
calcium intake, and physical activity affect calcaneal ultrasound in healthy Greek males in an age-dependent and parameter-specific manner. J Bone Miner Metab. 2005;23(2):157-66
56 Ho SC, Chen YM, Woo JL, Lam SS. High habitual calcium intake attenuates bone loss in early postmenopausal Chinese women: an 18-month follow-up study. J Clin Endocrinol Metab. 2004 May;89(5):2166-70
57 Uusi-Rasi K, Kärkkäinen MU, Lamberg-Allardt CJ. Calcium intake in health maintenance - a systematic review. Food Nutr Res. 2013 May 16;57 58 Nordin BE. The effect of calcium supplementation on bone loss in
32 controlled trials in postmenopausal women. Osteoporos Int. 2009 Dec;20(12):2135-43
59 Anderson JJ, Roggenkamp KJ, Suchindran CM. Calcium intakes and femoral and lumbar bone density of elderly U.S. men and women: National Health and Nutrition Examination Survey 2005-2006 analysis. J Clin Endocrinol Metab. 2012 Dec;97(12):4531-9
60 Wang MC, Dixon LB. Socioeconomic influences on bone health in postmenopausal women: findings from NHANES III, 1988-1994. Osteoporos Int. 2006 Jan;17(1):91-8
61 Jaime PC, Latorre Mdo R, Florindo AA, Tanaka T, Zerbini CA. Dietary intake of Brazilian black and white men and its relationship to the bone mineral density of the femoral neck. Sao Paulo Med J. 2006 Sep 7;124(5):267-70
62 Civitelli R, Ziambaras K. ‘Calcium and phosphate homeostasis: concerted interplay of new regulators’. J Endocrinol Invest. 2011; 34 (7 Suppl): 3-7 63 Kremsdorf RA, Hoofnagle AN, Kratz M, Weigle DS, Callahan HS, Purnell
JQ et al. ‘Effects of a high protein diet on regulation of phosphorus homeostasis’. J Clin Endocrinol Metab. 2013; Epub ahead of print 64 Tucker KL. Osteoporosis prevention and nutrition. Curr Osteopor Rep.
2009; 7: 111-117
65 Gibson RS, Bailey KB, Gibbs M, Ferguson EL. ‘A review of phytate, iron, zinc and calcium concentrations in plant-based complementary foods used in low-income countries and implications for bioavailability’. Food Nutr Bull. 2010; 31 (2 Suppl): S134-46
66 McCarty MF, DiNicolantonio JJ. Bioavailable dietary phosphate, a mediator of cardiovascular disease, may be decreased with plant-based diets, phosphate binders, niacin, and avoidance of phosphate additives. Nutrition. 2014 July - August;30(7-8):739-747
67 Levine BS, Walling MW, Coburn JW. ‘Effect of vitamin D sterols and dietary magnesium on calcium and phosphorus homeostasis’. Am J Physiol. 1981; 241(1): E35-41
68 Kurabayashi M. Role of calcium and phosphate in atherosclerosis and vascular calcification. Clin Calcium. 2013 Apr;23(4):489-96
69 Christakos S. ‘Recent advances in our understanding of
1,25-dihydroxyvitamin D3 regulation of intestinal calcium absorption’. Arch Biochem Biophys. 2012; 523: 73-76
216
Reviews | ICF November 2014 – Issue 5
71 Calvo MS, Uribarri J. Public Health impact of dietary phosphorus excess on bone and cardiovascular health in the general population. Am J Clin Nutr. 2013; Epub ahead of print.
72 Ritskes-Hoitinga J, Lemmens AG, Beynen AC. Nutrition and kidney calcification in rats. Lab Anim. 1989 Oct;23(4):313-8
73 Linefsky JP, O’Brien KD, Sachs M, Katz R, Eng J, Michos ED, Budoff MJ, de Boer I, Kestenbaum B. Serum phosphate is associated with aortic valve calcification in the Multi-ethnic Study of Atherosclerosis (MESA). Atherosclerosis. 2014 Jan 21;233(2):331-337
74 Håglin L, Törnkvist B, Bäckman L. Prediction of all-cause mortality in a patient population with hypertension and type 2 DM by using traditional risk factors and serum-phosphate,-calcium and-magnesium. Acta Diabetol. 2007 Sep;44(3):138-43
75 Cubbon RM, Thomas CH, Drozd M, Gierula J, Jamil HA, Byrom R, Barth JH, Kearney MT, Witte KK. Calcium, phosphate and calcium phosphate product are markers of outcome in patients with chronic heart failure. J Nephrol. 2014 Mar 11. [Epub ahead of print] Done
76 Sharma VK, Dwivedi P, Dubey AK. Correlation of serum phosphate with carotid intimal-medial thickness in chronic kidney disease patients. Indian J Nephrol. 2014 Jan;24(1):15-9
77 Adeney KL, Siscovick DS, Ix JH, Seliger SL, Shlipak MG, Jenny NS, Kestenbaum BR. Association of serum phosphate with vascular and valvular calcification in moderate CKD. J Am Soc Nephrol. 2009 Feb;20(2):381-7
78 Rroji M, Seferi S, Cafka M, Petrela E, Likaj E, Barbullushi M, Thereska N, Spasovski G. Is residual renal function and better phosphate control in peritoneal dialysis an answer for the lower prevalence of valve calcification compared to hemodialysis patients? Int Urol Nephrol. 2014 Jan;46(1):175-82
79 Nishizawa Y, Jono S, Ishimura E, Shioi A. Hyperphosphatemia and vascular calcification in end-stage renal disease. J Ren Nutr. 2005 Jan;15(1):178-82
80 Craver L, Dusso A, Martinez-Alonso M, Sarro F, Valdivielso JM, Fernández E. A low fractional excretion of Phosphate/Fgf23 ratio is associated with severe abdominal Aortic calcification in stage 3 and 4 kidney disease patients. BMC Nephrol. 2013 Oct 12;14:221
81 Razzaque MS. Phosphate toxicity and vascular mineralization. Contrib Nephrol. 2013;180:74-85
82 Yamada S, Tokumoto M, Tatsumoto N, Taniguchi M, Noguchi H, Nakano T, Masutani K, Ooboshi H, Tsuruya K, Kitazono T. Phosphate overload directly induces systemic inflammation and malnutrition as well as vascular calcification in uremia. Am J Physiol Renal Physiol. 2014 Jun 15;306(12):F1418-28
83 Louvet L, Buchel J, Steppan S, Passlick-Deetjen J, Massy ZA. ‘Magnesium prevents phosphate-induced calcification in human aortic vascular smooth muscle cells’. Nephrol Dial Transplant. Epub ahead of print
84 Pinheiro MM, Schuch NJ, Genaro PS, Ciconelli RM, Ferraz MB, Martini LA. Nutrient intakes related to osteoporotic fractures in men and women--the Brazilian Osteoporosis Study (BRAZOS). Nutr J. 2009 Jan 29;8:6 85 Farrin N, Ostadrahimi AR, Mahboob SA, Kolahi S, Ghavami M. Dietary
intake and serum bone related chemistry and their correlations in postmenopausal Iranian women. Saudi Med J. 2008 Nov;29(11):1643-8 86 Tranquilli AL, Lucino E, Garzetti GG, Romanini C. ‘Calcium, phosphorus
and magnesium intakes correlate with bone mineral content in postmenopausal women’. Gynecol Endocrinol. 1994; 8(1): 55-8 87 Ito S, Ishida H, Uenishi K, Murakami K, Sasaki S. The relationship
between habitual dietary phosphorus and calcium intake, and bone mineral density in young Japanese women: a cross-sectional study. Asia Pac J Clin Nutr. 2011;20(3):411-7
88 Kemi VE, Karkkainen MU, Lamberg-Allardt CJ. ‘High phosphorus intakes acutely and negatively affect Ca and bone metabolism in a dose-dependent manner in healthy young females’. Br J Nutr. 2006; 96(3): 545-52
89 Whybro A, Jagger H, Barker M, Eastell R. ‘Phosphate supplementation in young men: lack of effect on calcium homeostasis and bone turnover’. Eur J Clin Nutr. 1998; 52(1): 29-33
90 Kemi VE, Kärkkäinen MU, Karp HJ, Laitinen KA, Lamberg-Allardt CJ. Increased calcium intake does not completely counteract the effects of increased phosphorus intake on bone: an acute dose-response study in healthy females. Br J Nutr. 2008 Apr;99(4):832-9
91 Koshihara M, Katsumata S, Uehara M, Suzuki K. Effects of dietary phosphorus intake on bone mineralization and calcium absorption in adult female rats. Biosci Biotechnol Biochem. 2005 May;69(5):1025-8
92 Bonjour JP, Gue´guen L, Palacios C, Shearer MJ, Weaver CM. ‘Minerals and vitamins in bone health: the potential value of dietary enhancement’. British Journal of Nutrition. 2009; 101: 1581–1596
93 Nieves JW. ‘Osteoporosis: the role of micronutrients’. Am J Clin Nutr. 2005; 81(5): 1232S-1239S
94 Hardwick LL, Jones MR, Brautbar N, Lee DB. ‘Magnesium absorption: mechanisms and the influence of vitamin D, calcium and phosphate’. J Nutr. 1991; 121(1): 13-23
95 Hruby A, O’Donnell CJ, Jacques PF, Meigs JB, Hoffmann U, McKeown NM. Magnesium intake is inversely associated with coronary artery calcification: the framingham heart study. JACC Cardiovasc Imaging. 2014 Jan;7(1):59-69
96 Hoorn EJ, Zietse R. Disorders of calcium and magnesium balance: a physiology-based approach. Pediatr Nephrol. 2013; 28: 1195-1206 97 Ishimura E, Okuno S, Kitatani K, Tsuchida T, Yamakawa T, Shioi A, Inaba M, Nishizawa Y. Significant association between the presence of peripheral vascular calcification and lower serum magnesium in hemodialysis patients. Clin Nephrol. 2007 Oct;68(4):222-7 98 Meema HE, Oreopoulos DG, Rapoport A. Serum magnesium level
and arterial calcification in end-stage renal disease. Kidney Int. 1987 Sep;32(3):388-94
99 Tzanakis I, Virvidakis K, Tsomi A, Mantakas E, Girousis N, Karefyllakis N, et al. Intra- and extracellular magnesium levels and atheromatosis in haemodialysis patients. Magnes Res 2004; 17(2):102–8
100 Salem S, Bruck H, Bahlmann FH, Peter M, Passlick-Deetjen J, Kretschmer A, Steppan S, Volsek M, Kribben A, Nierhaus M, Jankowski V, Zidek W, Jankowski J. Relationship between magnesium and clinical biomarkers on inhibition of vascular calcification. Am J Nephrol. 2012;35(1):31-9 101 Zimmermann P, Weiss U, Classen HG, Wendt B, Epple A, Zollner
H, Temmel W, Weger M, Porta S. The impact of diets with different magnesium contents on magnesium and calcium in serum and tissues of the rat. Life Sci. 2000 Jul 14;67(8):949-58
102 Planells E, Llopis J, Perán F, Aranda P. Changes in tissue calcium and phosphorus content and plasma concentrations of parathyroid hormone and calcitonin after long-term magnesium deficiency in rats. J Am Coll Nutr. 1995 Jun;14(3):292-8
103 van den Broek FA, Beynen AC. The influence of dietary phosphorus and magnesium concentrations on the calcium content of heart and kidneys of DBA/2 and NMRI mice. Lab Anim. 1998 Oct;32(4):483-91
104 Rayssiguier Y. Role of magnesium and potassium in the pathogenesis of arteriosclerosis. Magnesium. 1984;3(4-6):226-38
105 Takeda R, Nakamura T. Effects of high magnesium intake on bone mineral status and lipid metabolism in rats. J Nutr Sci Vitaminol (Tokyo). 2008 Feb;54(1):66-75
106 Mortazavi M, Moeinzadeh F, Saadatnia M, Shahidi S, McGee JC, Minagar A. ‘Effect of magnesium supplementation on carotid intima-media thickness and flow-mediated dilatation among hemodialysis patients: a double-blind, randomised, placebo-controlled trial’. Eur Neurol. 2013; 69(5): 309-16
107 Pen JX, Li L, Wang X, Zhang YH, Li XF, Wu SY. The effect of the magnesium supplementation on vascular calcification in rats. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2012 Jan;28(1):20-3
108 Nagase N, Saijo Y, Nitta H, Tamura Y, Orino S, Akaike Y, Mori H. Myocardial disorders caused by magnesium deficiency in diabetic KK mice. Magnesium. 1989;8(5-6):307-15
109 Reginster JY, Strause L, Deroisy R, Lecart MP, Saltman P, Franchimont P. Preliminary report of decreased serum magnesium in postmenopausal osteoporosis. Magnesium. 1989;8(2):106-9
110 Orchard TS, Larson JC, Alghothani N, Bout-Tabaku S, Cauley JA, Chen Z, Lacroix AZ, Wactawski-Wende J, Jackson RD. Magnesium intake, bone mineral density, and fractures: results from the Women’s Health Initiative Observational Study. Am J Clin Nutr. 2014 Apr;99(4):926-33
111 Tucker KL, Hannan MT, Chen H, Cupples LA, Wilson PW, Kiel DP. ‘Potassium, magnesium and fruit and vegetable intakes are associated with greater bone mineral density in elderly men and women’. Am J Clin Nutr. 1999; 69(4): 727-36
112 Ryder KM, Shorr RI, Bush AJ, Kritchevsky SB, Harris T, Stone K et al. ‘Magnesium intake from food and supplements is associated with bone mineral density in healthy older white subjects’. J Am Geriatr Soc. 2005; 53(11): 1875-80
113 Macdonald HM, New SA, Golden MH, Campbell MK, Reid DM. ‘Nutritional associations with bone loss during the menopausal transition: evidence of a beneficial effect of calcium, alcohol and fruit and vegetable nutrients and of a detrimental effect of fatty acids’. Am J Clin Nutr. 2004; 79(1): 155-65 114 Kim MH, Yeon JY, Choi MK, Bae YJ. Evaluation of magnesium intake and
its relation with bone quality in healthy young Korean women. Biol Trace Elem Res. 2011 Dec;144(1-3):109-17
115 Yaegashi Y, Onoda T, Tanno K, Kuribayashi T, Sakata K, Orimo H. ‘Association of hip fracture incidence and intake of calcium, magnesium, vitamin D and vitamin K’. Eur J Epidemiol. 2008; 23(3): 219-25
116 Saito N, Tabata N, Saito S, Andou Y, Onaga Y, Iwamitsu A, Sakamoto M, Hori T, Sayama H, Kawakita T. Bone mineral density, serum albumin and serum magnesium. J Am Coll Nutr. 2004 Dec;23(6):701S-3S
117 Aydin H, Deyneli O, Yavuz D, Gözü H, Mutlu N, Kaygusuz I, Akalin S. Short-term oral magnesium supplementation suppresses bone turnover in postmenopausal osteoporotic women. Biol Trace Elem Res. 2010 Feb;133(2):136-43
two year controlled trial of peroral magnesium in osteoporosis’. Magnes Res. 1993; 6(2): 155-63
120 Abraham GE, Grewal H. ‘A total dietary program emphasising magnesium instead of calcium. Effect on the mineral density of calcaneous bone in postmenopausal women on hormonal therapy’. J Reprod Med. 1990; 35(5): 503-7
121 Turner AG, Hanrath MA, Morris HA, Atkins GJ, Anderson PH. The local production of 1,25(OH)2D3 promotes osteoblast and osteocyte maturation. J Steroid Biochem Mol Biol. 2013 Oct 12
122 Leiben L, Masuyama R, Torrekens S, Van Looveren R, Schrooten J, Baatsen P et al. ‘Normocalcemia is maintained in mice under conditions of calcium malabsorption by vitamin D-induced inhibition of bone mineralisation’. J Clin Invest. 2012; 122(5): 1803-15
123 Lips P. Interaction between vitamin D and calcium’. Scand J Clin Lab Invest Suppl. 2012; 243: 60-4
124 Heaney RP, Carey R, Harkness L. ‘Roles of vitamin D, n-3 polyunsaturated fatty acid and soy isoflavones in bone health’. J Am Diet Assoc. 2005; 105(11): 1700-2
125 Lamberg-Allardt C. ‘Vitamin D in foods and as supplements’. Prog Biophys Mol Biol. 2006; 92(1): 33-8
126 Rafferty K, Heaney RP. ‘Nutrient effects on the calcium economy: emphasising the potassium controversy’. J Nutr. 2008; 138: 166S-171S 127 Adamczyk A, Stolarz-Skrzypek K, Wesołowska A, Czarnecka D. Vitamin D and Vitamin D Receptor Activators in Treatment of Hypertension and Cardiovascular Disease. Cardiovasc Hematol Disord Drug Targets. 2014 Feb 28. [Epub ahead of print]
128] Kang YH, Jin JS, Yi DW, Son SM. Bone morphogenetic protein-7 inhibits vascular calcification induced by high vitamin D in mice. Tohoku J Exp Med. 2010 Aug;221(4):299-307
129 Tang FT, Chen SR, Wu XQ, Wang TQ, Chen JW, Li J, Bao LP, Huang HQ, Liu PQ. Hypercholesterolemia accelerates vascular calcification induced by excessive vitamin D via oxidative stress. Calcif Tissue Int. 2006 Nov;79(5):326-39
130 Ellam T, Hameed A, Ul Haque R, Muthana M, Wilkie M, Francis SE, Chico TJ. Vitamin d deficiency and exogenous vitamin d excess similarly increase diffuse atherosclerotic calcification in apolipoprotein e knockout mice. PLoS One. 2014 Feb 19;9(2):e88767
131 Schmidt N, Brandsch C, Kühne H, Thiele A, Hirche F, Stangl GI. Vitamin D receptor deficiency and low vitamin D diet stimulate aortic calcification and osteogenic key factor expression in mice. PLoS One. 2012;7(4):e35316
132 Schmidt N, Brandsch C, Schutkowski A, Hirche F, Stangl GI. Dietary Vitamin D Inadequacy Accelerates Calcification and Osteoblast-Like Cell Formation in the Vascular System of LDL Receptor Knockout and Wild-Type Mice. J Nutr. 2014 May;144(5):638-46
133 de Boer IH, Kestenbaum B, Shoben AB, Michos ED, Sarnak MJ, Siscovick DS. 25-hydroxyvitamin D levels inversely associate with risk for developing coronary artery calcification. J Am Soc Nephrol. 2009 Aug;20(8):1805-12
134 Michos ED, Streeten EA, Ryan KA, Rampersaud E, Peyser PA, Bielak LF, Shuldiner AR, Mitchell BD, Post W. Serum 25-hydroxyvitamin d levels are not associated with subclinical vascular disease or C-reactive protein in the old order amish. Calcif Tissue Int. 2009 Mar;84(3):195-202 135 Walker MD, Cong E, Kepley A, Di Tullio MR, Rundek T, Homma S, Lee
JA, Liu R, Young P, Zhang C, McMahon DJ, Silverberg SJ. Association between serum 25-hydroxyvitamin d level and subclinical cardiovascular disease in primary hyperparathyroidism. J Clin Endocrinol Metab. 2014 Feb;99(2):671-80
136 Linhartová K, Veselka J, Sterbáková G, Racek J, Topolcan O, Cerbák R. Parathyroid hormone and vitamin D levels are independently associated with calcific aortic stenosis. Circ J. 2008 Feb;72(2):245-50
137 Sahin I, Okuyan E, Ungör B, Kaya A, Avcı II, Biter HI, Cetin S, Enhos A, Avsar M, Dinçkal MH. Lower vitamin D level is associated with poor coronary collateral circulation. Scand Cardiovasc J. 2014 Jun 30:1-19. [Epub ahead of print]
138 Lee SY, Kim HY, Gu SW, Kim HJ, Yang DH. 25-hydroxyvitamin D levels and vascular calcification in predialysis and dialysis patients with chronic kidney disease. Kidney Blood Press Res. 2012;35(5):349-54
139 Young KA, Snell-Bergeon JK, Naik RG, Hokanson JE, Tarullo D, Gottlieb PA, Garg SK, Rewers M. Vitamin D deficiency and coronary artery calcification in subjects with type 1 diabetes. Diabetes Care. 2011 Feb;34(2):454-8
140 Dishmon DA, Dotson JL, Munir A, Nelson MD, Bhattacharya SK, D Cruz IA, Davis RC, Weber KT. Hypovitaminosis D and valvular calcification in patients with dilated cardiomyopathy. Am J Med Sci. 2009 May;337(5):312-6
141 Arad Y, Spadaro LA, Roth M, Scordo J, Goodman K, Sherman S, Lerner G, Newstein D, Guerci AD. Serum concentration of calcium, 1,25 vitamin D and parathyroid hormone are not correlated with coronary calcifications. An electron beam computed tomography study. Coron Artery Dis. 1998;9(8):513-8
Demer LL. Active serum vitamin D levels are inversely correlated with coronary calcification. Circulation. 1997 Sep 16;96(6):1755-60 143 Yokoyama K. Study on vascular calcification in patients on continuous
ambulatory peritoneal dialysis (CAPD): special reference to active vitamin D (VD) treatment. Nihon Jinzo Gakkai Shi. 1993 Oct;35(10):1171-80 144 Dalbeni A, Scaturro G, Degan M, Minuz P, Delva P. Effects of six months
of vitamin D supplementation in patients with heart failure: A randomized double-blind controlled trial. Nutr Metab Cardiovasc Dis. 2014 Mar 5. [Epub ahead of print]
145 Manson JE, Allison MA, Carr JJ, Langer RD, Cochrane BB, Hendrix SL, Hsia J, Hunt JR, Lewis CE, Margolis KL, Robinson JG, Rodabough RJ, Thomas AM; Women’s Health Initiative and Women’s Health Initiative-Coronary Artery Calcium Study Investigators. Calcium/vitamin D supplementation and coronary artery calcification in the Women’s Health Initiative. Menopause. 2010 Jul;17(4):683-91
146 Hsia J, Heiss G, Ren H, Allison M, Dolan NC, Greenland P, Heckbert SR, Johnson KC, Manson JE, Sidney S, Trevisan M; Women’s Health Initiative Investigators. Calcium/vitamin D supplementation and cardiovascular events. Circulation. 2007 Feb 20;115(7):846-54
147 Schnatz PF, Jiang X, Vila-Wright S, Aragaki AK, Nudy M, O’Sullivan DM, Jackson R, Leblanc E, Robinson JG, Shikany JM, Womack CR, Martin LW, Neuhouser ML, Vitolins MZ, Song Y, Kritchevsky S, Manson JE. Calcium/vitamin D supplementation, serum 25-hydroxyvitamin D concentrations, and cholesterol profiles in the Women’s Health Initiative calcium/vitamin D randomized trial. Menopause. 2014 Mar 3. [Epub ahead of print]
148 Elamin MB, Abu Elnour NO, Elamin KB, Fatourechi MM, Alkatib AA, Almandoz JP, Liu H, Lane MA, Mullan RJ, Hazem A, Erwin PJ, Hensrud DD, Murad MH, Montori VM. Vitamin D and cardiovascular outcomes: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2011 Jul;96(7):1931-42
149 Zheng Y, Zhu J, Zhou M, Cui L, Yao W, Liu Y. Meta-analysis of long-term vitamin D supplementation on overall mortality. PLoS One. 2013 Dec 3;8(12):e82109
150 Nakamura K, Iki M. Efficacy of optimization of vitamin D in preventing osteoporosis and osteoporotic fractures: A systematic review. Environ Health Prev Med. 2006 Jul;11(4):155-70
151 Snellman G, Byberg L, Lemming EW, Melhus H, Gedeborg R, Mallmin H, Wolk A, Michaëlsson K. Long-term dietary vitamin D intake and risk of fracture and osteoporosis: a longitudinal cohort study of Swedish middle-aged and elderly women. J Clin Endocrinol Metab. 2013 [Epub ahead of print]
152 Bergink AP, Uitterlinden AG, Van Leeuwen JP, Buurman CJ, Hofman A, Verhaar JA, Pols HA. Vitamin D status, bone mineral density, and the development of radiographic osteoarthritis of the knee: The Rotterdam Study. J Clin Rheumatol. 2009 Aug;15(5):230-7
153 Cranney A, Horsley T, O’Donnell S, Weiler H, Puil L, Ooi D et al. ‘Effectiveness and safety of vitamin D in relation to bone health’. Evid Rep Technol Assess. 2007; 158: 1-235
154 Rizzoli R, Boonen S, Brandi ML, Bruyère O, Cooper C, Kanis JA, Kaufman JM, Ringe JD, Weryha G, Reginster JY. Vitamin D supplementation in elderly or postmenopausal women: a 2013 update of the 2008 recommendations from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Curr Med Res Opin. 2013 Apr;29(4):305-13
155 Joo NS, Dawson-Hughes B, Kim YS, Oh K, Yeum KJ. ‘Impact of calcium and vitamin D insufficiencies on serum parathyroid hormone and bone mineral density: analysis of the fourth and fifth Korea National Health and Nutrition Examination Survey (KNHANES IV-3, 2009 and KNHANES V-1, 2010)’. J Bone Miner Res. 2013; 28(4): 764-70
156 Min Kim K, Hee Choi S, Lim S, Hoon Moon J, Hee Kim J, Wan Kim S, Chul Jang H, Soo Shin C. Interactions between Dietary Calcium Intake and Bone Mineral Density or Bone Geometry in a Low Calcium Intake Population (KNHANES IV 2008-2010). J Clin Endocrinol Metab. 2014 [Epub ahead of print]
157 Cauley JA, Danielson ME, Boudreau R, Barbour KE, Horwitz MJ, Bauer DC, Ensrud KE, Manson JE, Wactawski-Wende J, Shikany JM, Jackson RD. ‘Serum 25-hydroxyvitamin D and clinical fracture risk in a multiethnic cohort of women: the Women’s Health Initiative (WHI)’. J Bone Miner Res. 2011 Oct;26(10):2378-88
158 Bischoff-Ferrari HA, Dietrich T, Orav J, Dawson-Hughes B. ‘Positive association between 25-hydroxy vitamin D levels and bone mineral density: a population-based study of younger and older adults’. Am J Med. 2004; 116: 634-8
159 Zhou W, Langsetmo L, Berger C, Poliquin S, Kreiger N, Barr SI, Kaiser SM, Josse RG, Prior JC, Towheed TE, Anastassiades T, Davison KS, Kovacs CS, Hanley DA, Papadimitropoulos EA, Goltzman D; CaMos Research Group. Longitudinal changes in calcium and vitamin D intakes and relationship to bone mineral density in a prospective population-based study: the Canadian Multicentre Osteoporosis Study (CaMos). J Musculoskelet Neuronal Interact. 2013 Dec;13(4):470-9