THE IMPACT OF PROSTHODONTIC TREATMENT ON A NORTH CAROLINA HUMAN IMMUNIDEFICIENCY VIRUS (HIV) COHORT
Gabrielle R Jackson
A thesis submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master in Science in the School of Dentistry
(Prosthodontics).
Chapel Hill 2019
Approved by:
Jennifer Webster-Cyriaque Ingeborg De Kok
ABSTRACT
Gabrielle R Jackson: The impact of prosthodontic treatment on the Human Immunodeficiency Virus (HIV) cohort
(Under the direction of Jennifer Webster, Ryan Cook, Ingeborg De Kok)
Background: Among people living with human immunodeficiency virus (HIV), oral care is among the highest unmet needs affecting quality of life and overall wellness. The impact of prosthodontic treatment on HIV patients has not been comprehensively documented.
Objective: The purpose of this study is to investigate the relationship between prosthodontic rehabilitation and different quality of life measures in HIV-positive subjects before and after
prosthodontic treatment.
Methods: A convenience sample of HIV positive subjects (n=22) were rehabilitated with removable prostheses: complete dentures, immediate dentures, cast or acrylic partial dentures; mean age 46; 78% men. Four validated questionnaires were administered at 6-month intervals over a 24-month period: OHIP-14 (Oral Health Impact Profile), SF-8 (Medical Outcomes Short Form 8), SADS (Social Avoidance and Anxiety) and FAY (Feelings About Yourself). Wilcoxon signed-rank tests compared average questionnaire responses before treatment to average questionnaire responses after treatment.
ACKNOWLEDGEMENTS
To my family and friends who have supported me emotionally, financially and spiritually throughout my journey. Your love, kindness humor and patience have been indispensable during this time. Dad and brother and sister, who have supported me throughout my journey.
I wish to acknowledge my mentor, Jennifer Webster DDS, PHD for her caring, patience, wisdom and encouragement that has guided me to the completion of this
project. We have met on many after-hour coffee appointments, typing, writing, searching, editing and theorizing the major concepts of this important project. I thank her for the opportunity to partake in this meaningful journey, as it has made me a better researcher and better clinician.
My most sincere gratitude to my thesis committee members: Dr. Ingeborg DeKok DDS, MS one of my first female role models and mentors at UNC School of Dentistry. Thank you for your constant support and encouragement in addition to your contributions and
TABLE OF CONTENTS
LIST OF TABLES ... x
LIST OF FIGURES ... xi
LIST OF ABBREVIATIONS ... xii
CHAPTER 1: INTRODUCTION ... 1
Role of prosthodontics in oral health and QoL: an overview ... 1
Defining dental prosthetic rehabilitation ... 2
Defining QoL, HRQoL and OHRQoL ... 2
Validated metrics used in QoL, general health and overall wellbeing assessments ... 5
Oral Health Impact Profile (OHIP-14) ... 5
Short Form Health Survey 8 (SF-8) ... 5
Social Avoidance and Anxiety (SADS) ... 6
Feelings About Yourself (FAY) ... 7
Measuring oral disease status and its impact on QoL ... 7
Clinical/objective measures of oral disease ... 8
Subjective measures of oral disease ... 12
Objective and subjective consequences in the HIV patient ... 13
Statement of Purpose ... 16
Chapter II: THE IMPACT OF PROSTHODONTIC TREATMENT IN AN HIV
COHORT ... 17
Introduction ... 17
Prosthodontic treatment and OHRQoL in the HIV negative cohort ... 18
Prosthodontic treatment and OHRQoL in the HIV positive cohort ... 19
Defining prosthodontic rehabilitation in the HIV population ... 20
MATERIALS & METHODS ... 21
Study Design and Population ... 21
Prosthodontic Sub-cohort ... 22
Recruitment, Data Collection, and Inclusion Criteria ... 23
STATISTICAL ANALYSES ... 23
General Analysis ... 23
Analysis for Factors Affecting Oral Health ... 24
Periodontal Disease Analysis ... 25
Analyses for Questionnaires ... 25
Analyses for Denture Subgroup Comparison ... 26
RESULTS ... 27
Oral Health over the Course of the Study ... 27
Qualitative outcomes after prosthodontic treatment in an HIV cohort ... 28
Qualitative differences between complete denture recipients and partial denture recipients. ... 29
CONCLUSIONS ... 30
LIST OF TABLES
LIST OF FIGURES
Figure 1. General Study Design. ... 38
Figure 2. Oral health at baseline for pros versus non-pros cohort. ... 39
Figure 3. Response to Periodontal Therapy in an prosthetic HIV Cohort. ... 41
Figure 4. (a-f): Qualtative Impact of Prosthodontic Treatment in a HIV Cohort ... 42
LIST OF ABBREVIATIONS
AAP American Academy of Periodontology ACP American College of Prosthodontics ADA American Dental Association
AL Attachment loss
ART Antiretroviral combination therapy BOP Bleeding on probing
BiPD-Q Burdens in Prosthetic Dentistry Questionnaire CAL Clinical attachment loss
CDC Center for Disease Control
DMFT Decayed-missing-filled teeth index FAY Feelings about yourself
HAART Highly active anti-retroviral therapy HRQoL Health-related quality of life
HIV Human immunodeficiency virus
HRSA Health resources and service administration MRPD Metal removable partial dentures
OHRQoL Oral health related quality of life OHIP Oral health impact profile OHI Oral hygiene index
PD Probing depth
PLWH People living with HIV QoL Quality of life
SPNS Special Projects of National Significance
VL Viral load
CHAPTER 1: INTRODUCTION Role of prosthodontics in oral health and QoL: an overview
Prosthodontics is a dental specialty recognized by the American Dental Association (ADA) that pertains to the diagnosis, treatment planning, rehabilitation and maintenance of oral function, comfort, esthetics and health of patients with clinical conditions associated with missing teeth and/or jaw structures3. Prosthodontists often work with general dentists, other dental specialists and other healthcare specialists in a team-based approach, playing a principal role in the interplay between tooth loss, restoration type and treatment effects on oral health, general health and overall quality of life (QoL).
The beginnings of the prosthodontic discipline date back to the early nineteenth century. Following its establishment as a dental specialty in 1947, prosthodontics has evolved to include areas of research, education and clinical practice. The concept of prosthodontic rehabilitation originated from the theory that the restoration of an individual’s occlusion would improve the functional state of supporting structures and thereby oral health. 4–7 The need for treatment with dental prostheses may arise as a consequence of sustained poor oral health status and/or
Defining dental prosthetic rehabilitation
Dental prosthetic rehabilitation involves restoring missing teeth, parts or structures of an individual’s mouth with an artificial prosthesis where the primary goal is to reestablish oral comfort, function and esthetics. Rehabilitation may be accomplished using a number of methods and prostheses types. A fixed dental prosthesis (FDP) refers to any prosthesis that is securely fixed or attached to a natural tooth or teeth, or one or more dental implants/implant abutments which cannot be removed by the patient8. Removable dental prostheses refers to a removable complete or partial denture, overdenture, or maxillofacial prosthesis that replaces some or all missing teeth which can be readily removed by the patient.8 And lastly, an implant-supported dental prostheses (ISDP) can refer to prostheses that are fixed or removable in nature.
Relying on functional indicators alone to quantify the comprehensive effects of prosthetic interventions to replace missing teeth is inadequate. Assessing the psychosocial impact of treatment on the patient is equally important. Within the literature, the impact of prosthodontic outcomes has been studied from both the objective clinical perspective and the also the
subjective patient-reported viewpoint. Understanding the psychosocial, esthetic, functional, and emotional effects of prosthodontic treatment on quality of life is an important component of informed consent. Therefore, an exploration of the evidence that assesses the comprehensive impact of our restorative efforts across treatment modalities and specific populations is indicated.
Defining QoL, HRQoL and OHRQoL
Dentistry was behind in this realization. As stated earlier, the aim of prosthodontic treatment is to improve oral health, function and esthetics for individuals and populations through the use of different dental prostheses. The degree to which this goal is achieved through treatment from the patient’s perspective is quality of care. The quality of care we provide patients can have drastic and long-term effects on an individual’s quality of life.
What follows is an overview of the terms quality of life, health-related quality of life (HRQoL) and oral health-related quality of life (OHRQoL) including their implementation in population surveillance studies which have helped expand our understanding of the patient, provider, and treatment dynamic from a prosthodontic lens.
QoL is defined as an individuals’ perceptions of their position and satisfaction in life in the context of their physical and mental health, family, education, employment, and safety, in relation to the culture and value systems in which they live. With regard to physical health, medical providers have traditionally measured disease severity and impact using clinical
indicators. Today, the relationship among clinical indicators of health and disease, treatment and the related impacts on quality of life is better understood.
of disease (2) The functional capability of an individual and (3) The way an individual perceives his/her situation in life.
Historically, oral health and general health were understood to be separate entities. This division placed an undue burden on of oral disease on vulnerable populations in the US who faced many barriers related to access to oral care. In the early 1980’s, researchers like Locker, Slade and others suggested that there was high value in understanding the socioenvironmental components of oral health.11–13 Subsequently, a more specified derivative of HRQoL was birthed, termed oral health related quality of life (OHRQoL). In 1988, Locker’s13 conceptual model for measuring oral health, based on the World Health Organization’s (WHO)
classification of disease has been fundamental to the development of modern-day dental research.
OHRQoL is a multifaceted concept that includes a subjective evaluation of a person’s oral health, function, emotional and social wellbeing, satisfaction with oral care, and sense of self. In 1995, quality of life, was identified by the WHO as a valid parameter of patient assessment in not only medicine, but oral health as well.14 Just five years later, the Surgeon General’s report of 2000 identified OHRQoL a priority in public health policy. This redefining of oral health was timely and vital to the planning of oral healthcare programs specifically targeting at-risk populations such as children and people living with HIV/AIDS.
With this new comprehensive paradigm shift in the framework of our health model, there was pronounced growth in the development and testing of patient-based assessments which focused specifically on measuring oral health outcomes in a cross-sectional approach.
implications for research-based clinical dentistry. Over the past three decades, a variety of validated instruments have been utilized to measure these outcomes.15–17
Validated metrics used in QoL, general health and overall wellbeing assessments
Oral Health Impact Profile (OHIP-14)
The most frequently used validated questionnaire used in dental research to assess patient-reported outcomes is the Oral Health Impact Profile (OHIP), first described by Slade and Spencer in 1994.15 The original instrument consisted of 49 questions and uses a frequency-based approach. Since its introduction, several shortened versions have been developed and show a high level of agreement with the original instrument. Today, it is still the most sensitive method for detecting dissatisfaction with prosthetic rehabilitation.1819
The OHIP questionnaire provides a comprehensive measure of self-reported dysfunction, discomfort and disability attributed to oral conditions. Specifically, it focuses 7 domains
dimensions: functional limitation, pain, social disability, psychological discomfort, and handicap. The OHIP-14, consists of 14 questions which can be scored on a likert-type scale and has the following 5 impact response options20: “hardly ever” (score 1), “occasionally” (score 2), “fairly often” (score 3) and “very often” (score 4). The response “never” (score 0) implies the total
absence of impact. The outcome variable ranges from 0-56 with higher scores indicating higher
levels of dysfunction, discomfort and disability attributable to oral conditions.
Short Form Health Survey 8 (SF-8)
derived. SF questionnaires measure QoL, functional health and well-being on two major scales: physical health and mental health. The physical health score is derived from the patient’s perception of his or her overall health, limitations due to physical health issues, difficulty with daily work due to physical health issues, and bodily pain in the prior four weeks. The mental health score is derived from the patient’s perception of personal energy, the impact of physical or emotional problems on social activity, the impact of emotional problems on daily life activities.
The SF-8 developed by Quality Metric, Incorporated (QMI) consists of only 8 questions, four from each major scale and takes about 1-2 minutes to complete. The ability to measure general and physical health populations suffering from chronic disease such as PLWH, is
important to help detect health variances between population subgroups and the impact of health-related interventions. Previous studies suggest that the SF is a reliable and valid measure of health status for diverse groups of people infected with HIV.21
Social Avoidance and Anxiety (SADS)
psychosocial impact within two populations: patients with developmental dental defects and the cleft lip and palate cohort, both of which prosthodontists often rehabilitate.
Feelings About Yourself (FAY)
Self-esteem is an important social psychological construct that has been conceptualized as an influential predictor of certain outcomes. For example, self-esteem is known to be a protective factor of mental health and also may have beneficial effects on physical health.23 A number of self-esteem theories converge on its potential to buffer the effects of stress, anxiety and also symptoms of disease.24 Interest in the connections between self-esteem and general health started to grow in the 1970’s. The Feelings About Yourself (FAY) scale, created in 1979, is a validated instrument used for measuring self-esteem and is a combination of the Pearlin Mastery Scale and Rosenberg Self-Esteem scales. The Pearlin Mastery Scale was designed to measure an individual’s level of mastery in life which is defined as “the extent to which one regards one’s life-chances as being under one’s own control in contrast to being fatalistically ruled”.25 The Rosenberg Self-Esteem Scale measures global feelings of worth or
self-acceptance.26 The questionnaire consists of 17 items with higher scores indicating higher feelings of one’s life.
Measuring oral disease status and its impact on QoL
Within the prosthodontic literature, studies have reported on changes in quality of life scores in patients treated with various treatments from single crowns2728, to fixed dental
patients who received FPDs, RPDs, and complete dentures over a 12-month period. The OHIP means were compared to the OHRQoL mean level in the generation population. Improvements in OHRQoL was observed in 96% of subjects where an initial increase from pre-treatment scores within the first 6 months of treatment followed by a decrease from 6-12 months. The largest improvement was observed for patients with fixed prosthodontics.
Montero et al32evaluated the self-perceived changes in OHRQoL reported by 153 subjects treated with CDs, metal removable partial dentures (M-RPDs), and acrylic removable partial dentures (ADs) and metal-ceramic fixed dental prostheses (FDPs). The OHIP-14 questionnaire was utilized to assess the difference between baseline impact scores and post treatment scores when compared with the reference population. Patients perceived benefits in their chewing ability, esthetics and treatment satisfaction after receiving their prosthesis. Specifically, the metal removable partial denture group showed the highest patient satisfaction and thus, highest therapeutic improvement although pain/discomfort of appliance is a noted drawback described in other studies as well.33
Clinical/objective measures of oral disease
Tooth loss is the ultimate consequence of oral disease and is normally the result of multiple risk factors at play. In addition to local disease, there are other risk factors such as poor diet, poor oral hygiene, tobacco use, non-regular dental care, and systemic disease which may exacerbate disease progression further complicating the decision-making process. The use of clinical
Oral hygiene status has been measured through a number of metrics such as the Oral Hygiene Index (OHI).34 Introduced by Green and Vermillion in 1960, the OHI is classified based on the combined scores of plaque/debri and calculus per buccal and lingual tooth surface for a total of 12 surfaces per arch. The simplified index35 (S-OHI) differs from the original in that it only assesses 6 surfaces total per arch-4 posterior teeth and two anterior teeth. Plaque and gingival indices36 have also been widely used.
There is an understood relationship between oral health status or oral hygiene and oral disease experience, specifically caries and periodontal disease. We understand caries to be a multifactorial result of bacterial microflora, refined carbohydrates, the patients host response, and time. Caries experience, as recommended by the World Health Organization has been frequently assessed using the decayed-missing-filled teeth (DMFT) index. The index is applied to permanent dentition and is expressed as the number of tooth surfaces decayed, missing or restored. Studies have shown higher DMFT scores to correlate positively with low or poor oral hygiene status.3738
Periodontal disease status has been most widely measured via periodontal pocket depths referred to as probing depths (PDs), bleeding on probing (BOP), bone loss and clinical attachment loss (CAL) indices and is commonly categorized based on location and severity. Described by Armitage41 and adapted by the American Academy of Periodontology42 (AAP), the most widely used classification of periodontal disease is based on clinical attachment loss and is. For epidemiologic purposes, it has also been classified based on probing depths and clinical attachment levels43. And lastly, as used in this study, the biofilm-gingival interface (BGI) is another classification system based on probing depths and bleeding on probing reflecting presence of active disease vs historical disease status. 44
As previously mentioned, acute and chronic disease progression can lead to tooth loss. There is an established direct relationship between tooth loss and masticatory function, also referred to as chewing ability.45 Chewing ability is related to the number and location of remaining
functional units. A tooth should occlude with another tooth in the opposing jaw to be considered a functional unit.46 With this understanding, it makes sense that an individuals’ ability to chew is also related to their nutritional intake. Several studies have found impaired dentition status to be associated with poor nutritional intake.474849 People with impaired dentitions may follow certain dietary restrictions which can compromise their nutritional status.
procedures. In 1964, Kapur studied chewing performance in 140 subjects and found the chewing efficiency of the denture wearer to be less than one-sixth that of a dentate subject.50 In 1990, James Leake realized the need for a reliable and validated index of chewing ability as a measure of dental health and carried out a study to develop and test his index on 43 participants.
Individuals were scored from 0 to 5 based on their self-reported ability to chew five foods after 20 strokes: fresh carrots, salad, steak, boiled vegetables and apples. In his analysis, among the dentate subjects, several clinical dental health status measures appeared to influence chewing ability--the absence of functioning opposing pairs of natural posterior teeth and the need for urgent care/presence of pain had the largest influence.51 A 2014 systematic review explored the relationship between functional tooth units and chewing ability in older adults across 18 studies. Although there was conflicting results regarding the minimal number of remaining functional tooth units to maintain adequate oral function, it revealed that chewing ability is closely related to the number and location of remaining teeth.52
A 2004 study by Gilbert et al quantified the incidence of tooth loss, prosthodontic dental restoration and chewing difficulty onset during 24months of follow-up and effect of tooth loss and the effect of tooth loss and prosthodontic restoration on chewing difficulty onset.53 The study evaluated the chewing index of 873 subjects. People who reported tooth loss were 2.7 times more likely to report chewing difficulty onset than people without tooth loss. A positive
association between number of occluding pairs with chewing ability and improved general health was observed. People who had received and completed removable prosthodontic treatment were much less likely to have reported chewing difficulty onset than those who had not received
Subjective measures of oral disease
Most oral pathology is not lethal, even in immune compromised populations like those living with HIV. However, it is often associated with some morbidity along with function, physical, psychosocial, emotional and social effects impacting QoL; these include pain, and difficulty eating, chewing, smiling and communicating. 5455 The presence of oral disease can impact “people’s comfort when eating, sleeping and engaging in social interaction; their self-esteem; and their satisfaction with respect to their oral health” as stated in the Surgeon General’s Report of 2000.56
As discussed earlier, oral disease, including tooth loss, can significantly impact an individual’s ability to eat comfortably. This in turn has the potential to affect an individual’s likelihood of eating in social settings. A study by Teófilo et al examined 211 patients’ self-perceived impacts and prosthodontic needs at the time of extraction and 3 months post treatment finding an association between the position of teeth lost and perceived functional limitation.57 Tooth loss in the maxillary arch was found to be associated with a worsened appearance and increased desire for prosthodontic treatment. Patients identified financial limitation as the most important factor influencing access to treatment.
We live in an increasingly more social media driven world where our interactions with others is largely influenced by our appearance. Dentists frequently witness the emotional and psychological effects of tooth loss when treating the partially or completely edentulous patient. Tooth loss with or without prosthodontic treatment can impact an individual’s ability to
lowered self-confidence, dislike of appearance, altered self-image, and altered behavior in socializing and forming close relationships to name a few. Following tooth loss is it is not uncommon for patients to be restricted in social activity mainly due to functional limitations and even sometimes experience symptoms of depression.60
In addition to what has already been discussed, certain social determinants are known to have a strong association with tooth loss and are an important link in understanding the existing disparities in oral health. African Americans and those of low SES are less likely to obtain dental care and more likely to experience tooth loss.61 Poor oral health is also associated with
environmental impacts such as decreased school6263and job performance.64
More recent studies have also reported a self-perceived improvement in general health
following prosthodontic treatment.6566Prosthodontics is one of the dental specialties where these
psychosocial effects are most frequently observed and secondarily treated. Prosthodontic intervention may therefore, provide a standard of care that improves general health and overall wellbeing in the edentulous population.
Objective and subjective consequences in the HIV patient
In the HIV-positive population where immunosuppression plays a large role, patients are known to have a greater prevalence of oral disease in general. Oral manifestations are one of the earliest clinical indicators of HIV infection and progression in children. Specifically, this cohort is at higher risk for the two most common oral diseases, caries6768 and periodontal disease6970 ultimately leading to greater tooth loss71 than the systemically healthy patient.
treatment. The federally funded Ryan White HIV/AIDS program, played a pivotal role in the introduction of combination therapy, also known as highly active anti-retroviral therapy (HAART) therapy which ultimately led to a significant decrease in mortality rates related to AIDS.
Xerostomia and decreased salivary flow are known side effects of HAART therapy. These two effects together have a positive synergistic influence on caries risk, particularly cervical and root caries. Comorbidity is also common in those living with the virus which through polypharmacy exacerbates the already xerostomic condition secondarily, increasing caries risk72. Resultant caries often progresses rapidly if untreated, deeming a tooth non-restorable and ultimately ending in tooth loss.73
In a more direct relationship, HIV patients’ systemic immunosuppression is often manifested orally through periodontal diseases, amongst others. Most recently, It has been documented that periodontal disease prevalence is 75% in the HIV positive population74 some studies reporting up to 85%7576 compared to 47% prevalence in the general population.77 HIV infected individuals may experience unique forms of periodontal and gingival disease including necrotizing ulcerative periodontitis (NUP), necrotizing ulcerative gingivitis (NUG), necrotizing ulcerative stomatitis (NUS) and linear gingival erythema (LGE).78 There is also a higher prevalence and incidence of fungal infections like oral candidiasis, viral-associated mucosal pathology such as Kaposi’s sarcoma, herpes simplex virus lesions, human papilloma virus wart lesions, and also oral hairy leukoplakia, all of which have become much less common since the introduction of HAART but are still observed and treated clinically.78
socioeconomic status (SES) are closely related to the more direct objective measures of disease we observe clinically in both HIV-positive and HIV negative groups. However, it is a known fact that African Americans and people of low SES are disproportionately infected with the
virus. African Americans account for a higher proportion of new HIV cases, those living with HIV, and those who have ever received an AIDS diagnosis, compared to other
races/ethnicities.79The 2019 CDC HIV Surveillance report states that although African
Americans account for only 13% of the US population, they accounted for 43% (16,694) of the 38,739 new HIV diagnoses in 2017.80 From 2010-2016 the infection rate among African Americans decreased 12% compared to 8% overall within the US supporting that even with accelerating progress, a large gap still remains.80
When it comes to SES, commonly assessed metrics include education, annual household income, poverty level, employment, and homeless status. HIV prevalence rates in urban poverty-stricken areas are inversely related to annual household income81. In addition to being more common in low-income households, HIV infection was also more common among those who were unemployed and had less than a high school education82. With a better understanding of the HIV population general demographics, it makes sense that this cohort faces large barriers related to income and insurance coverage which also influences use of dental services83. Since HIV patients often lack access to regular dental care84, this again puts them at higher risk for tooth loss85 and other significant impacts on QoL8687.
by a number of factors including those which are biological such as periodontal status and caries rate and patient-related factors such as cost.
Statement of Purpose
The primary objective of this study is to bridge the research gap focusing on the impact of oral health care, specifically with removable prosthodontics on the HIV-positive cohort. The findings of this study should reinforce the need for continued federal and statewide advocacy and support for oral health programs targeting people living with HIV. The ultimate goal is to reduce disparities in access to effective preventive and dental treatment services that would hopefully be extended to other vulnerable populations.
Hypothesis
Chapter II: THE IMPACT OF PROSTHODONTIC TREATMENT IN AN HIV COHORT Introduction
Systemic and oral health are intimately intertwined, especially in people living with HIV
(PLWH). The HIV population faces potential compromised oral health as a consequence of their compromised immune function. For over a decade now, oral care has been identified as one of the highest unmet needs among PLWH 9091, noted as being twice as prevalent as the unmet need for medical care. 92,93 In general, oral disease has be associated with pain, malnutrition, weight loss, poor medication adherence, lower self-esteem, increased anxiety, social isolation and unemployment. 94–96 Financial factors related to income and insurance coverage have been found to limit access to, and influence use of oral health care services by people infected with human immunodeficiency virus, or HIV.91 The repercussions from these unmet needs may have exacerbating negative effects on the overall health and quality of life in PLWH. Long-term retention and adherence to antiretroviral combination therapy (ART) has extended the life expectancy of people living with HIV dramatically since the 1980’s.
Despite advances in dentistry, edentulism still remains a predominant public health problem in the US and worldwide. 97 Complete and partial edentulism is known to have a
pronounced impact on daily living, leading directly to functional limitations and impairment with physical, psychological, and social components.98,99 The impact of oral health on overall health has been understudied in the PLWH population in general, but even more so within the
disease and problems with access to dental care and are thus thought to have a larger impact on quality of life and wellness when compared to HIV negative individuals. 100101 Dental prostheses such as partials or dentures serve to replace missing teeth and are perceived as an integral part of the body. Thus, prosthodontic treatment may be a vital component in bridging the gap between the unmet oral care needs of edentulous patients living with HIV.
Historically, disease diagnosis and treatment were largely based on objective clinical measures. Patient-reported outcomes have since come to hold a higher level of importance in the more comprehensive assessment of disease status and prognosis as it relates to overall health and oral health. We now understand that the objective measure of disease provides very little insight into the impact of oral disease on daily living and quality of life, especially in those who are medically compromised.54,102 Therefore, a patient-centered approach has become the driving force in treatment assessment today. Because the psychosocial effects of tooth loss are very commonly observed by prosthodontists, prosthodontic intervention may therefore provide a standard of care that improves general heath and overall well-being in the edentulous population.
Prosthodontic treatment and OHRQoL in the HIV negative cohort
Numerous quality of life studies related to prosthodontic treatment have supported the positive effects of oral rehabilitation on perceived oral health in the general population.29,65,103 In 2007, Özhayat et al 104 assessed the impact of partial edentulism and removable partial denture wearing on quality of life utilizing a visual analog scale and a direct weighting
These include the patient’s age, number of occluding dental units replaced, replacement of anterior teeth and nature of the opposing arch.105 In sum, the consensus of this review was consistent with that of previous studies, in that there is little evidence supporting any association between patient-reported QoL and satisfaction as it relates to RPD therapy.
Studies have also compared different types of prosthetic restorations. One such study compared patient satisfaction and oral-health related QoL in a total of 86 completely edentulous patients with either fixed implant-supported prostheses (n=29), removable implant-supported prostheses (n=27) and complete dentures (n=30).106 A significant increase in OHRQoL following prosthetic treatment was observed in all three groups however the fixed and removable treatment provided significantly greater improvement than the complete denture treatment.
Prosthodontic treatment and OHRQoL in the HIV positive cohort
North Carolina consistently ranks 47th among the fifty states with a dentist-population ratio of 4.1 dentists per 10,000.107 As this already presents an initial barrier to access to care, additionally PLWH also experience the barrier of discrimination by dentists and other types of providers 65,108. Prosthodontists frequently treat patients who have experienced significant stigma related to their oral health status similar to the stigma PLWH face regarding their HIV status.
A recently published 2018 cross-sectional study evaluated HRQoL in 120 HIV positive individuals using the Short Form Health Survey (SF-36) and the DMFT index. The relationship between the mental component summary (MCS) and DMFT was analyzed where they found a significant increase in MCS for each unit increase in DMFT. They also evaluated the impact of depression on these variables and found that depressed patients showed worse oral health indicators (DMFT index, missing teeth).111 When it comes to more invasive treatments, like dental implant therapy, there is no current consensus on their use in HIV positive patients. A 2018 systematic review on implant survival in the HIV patient evaluated success rates, marginal bone loss and complications concluding that dental implants are suitable for the rehabilitation of HIV-positive patients with controlled risk factors and normal CD4+ cell counts. 112
Defining prosthodontic rehabilitation in the HIV population
Traditionally, HIV patients have been treated with a combination of fixed prostheses, removable prostheses and more recently dental implants; all of which are the same treatment options available to HIV negative patients. The largest biological factor affecting dental
MATERIALS & METHODS
Study Design and Population
The UNC Oral Health Demonstration Project, was one of 15 demonstration sites funded through the US Health Resources and Service Administration (HRSA) Special Projects of National Significance (SPNS) Innovations in Oral Health Care Initiative to develop innovative 5-year models of care providing oral health care services to underserved populations living with HIV in both urban and non-urban settings. The SPNS Oral Health Initiative parent study, conducted by HRSA included 2, 178 HIV positive individuals and covered 12 US states, including rural and urban districts, and 1 US territory.91 Fifteen study sites were located in New York, New York; San Francisco, California; Miami, Florida; New Orleans, Louisiana; Chapel Hill, North Carolina; Eugene, Oregon; US Virgin Islands; Lane County, Oregon; Norwalk, Connecticut; Provincetown, Massachusetts; Chester, Pennsylvania; Jefferson, South Carolina; Tyler, Texas; and Green Bay, Wisconsin.
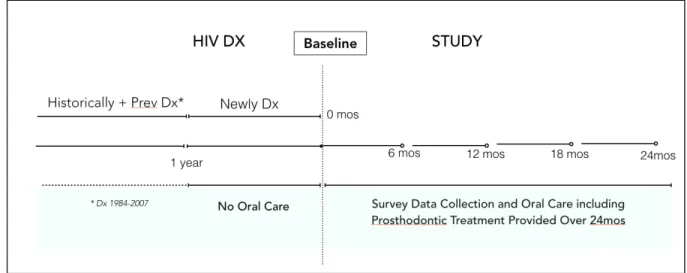
Baseline data included of a number of indices relating to periodontal status, caries experience and HIV status in addition to the completion of the 4 previously mentioned questionnaires. Most participants were unemployed, high school educated, African American (64.28%) males (76.19%) with a mean age of 44, and a mean income of $851 per month. Participants were characterized into 1of 3 HIV diagnostic categories: (1) Newly Diagnosed: <1 year since HIV diagnosis with no history of regular dental care for at least 12 months; (2) Previously Diagnosed: >1 year since HIV diagnosis with no history of dental care for at least 12 months; (3) Historically Diagnosed: >1 year since HIV diagnosis with history of regular dental care within the last 12 months (Figure 1). Within the entire cohort, there was a relatively equal number of patients within each category. Baseline data on viral load, mean CD4 count and ART status was also obtained and most participants (77%) were on HAART therapy (Table 1).
Prosthodontic Sub-cohort
Treatments were provided through collaboration with the UNC Hospitals’ Dental Clinic and its providers. Of the 196 enrolled participants at the UNC site, 22 were in need of prosthodontic care. This study focuses on the data analysis of this prosthodontic sub-cohort. Removable dental prostheses provided included immediate dentures, complete dentures, and removable partial dentures. For analysis purposes, 4 prosthetic groups were established according to the type of prostheses received per arch (Figure 2) (1) CD: complete denture; (2) ID: immediate denture (3) M-RPD: metal-based removable partial denture; (4) ADs: acrylic partial denture (Figure 2). For simplification of analysis, immediate dentures were included with complete dentures.
Recruitment, Data Collection, and Inclusion Criteria
The recruitment and data collection techniques and inclusion criteria have been
previously published. 91 The North Carolina study site recruited subjects through direct outreach, in collaboration with social services and HIV case managers, and through referrals from HIV clinics. The four utilized questionnaires were provided to participants at baseline, 6, 12, 18 and 24 months. Inclusion criteria required participants to be HIV positive and over the age of 18. The majority (73%) of the prosthodontic sub-cohort had not received dental treatment within the past 12 months prior to treatment.
STATISTICAL ANALYSES
General Analysis
Given the small nature of this sub-study, exact methods which do not rely on large sample assumptions are used for statistical inference and are always presented with
Analysis for Factors Affecting Oral Health
Factors affecting oral health were summarized for the entire cohort at the first exam visit. On occasion, the first exam visit was not performed at the baseline visit however, the majority of patients had data (or relatively complete data) at baseline. Values are presented as means and ranges using stratification by no/mild, moderate, and severe disease for periodontal disease (PD) and attachment loss (AL) and yes (generalized bleeding)/ no (local bleeding) for bleeding on probing (BOP). A Kruskal Wallis test was used to test for a difference across the groups.
Of the original 22 patients, a total of 16 patients were evaluated for an extent of periodontal disease ≥3 mm with BOP and/or attachment loss ≥3 mm with BOP. These variables measured the probing depth exceeding 3 mm across the entire mouth (all sites). We realize that statistical tests for change may falsely identify improvement in these variables over time if the number of sites being evaluated decreases due to dental extractions. In order to control for this, we divided the PD and AL variables by the total number of sites that met the ≥3 mm BOP criteria. This provides a standardized estimate of the extent of disease that is directly comparable to an estimate at any point in time.
Patients with an extent of 0 mm at the first visit were not included in the analyses, as they did not worsen over time and could not be evaluate for improvement. Patients were also excluded if they had only a single periodontal examination. This left N=13 evaluable patients with complete PD data and N=14 evaluable patients with complete AL data. The smallest and largest duration between initial and final examination was 6 and 24 months, respectively, with a median of 9 months. Relationship of final examination date to prosthodontics procedure date was not considered. Testing is reported using an exact, two-sided Wilcoxon signed-rank test.
summary, even if they did not have the procedure codes of interest (see Supplementary Material for List of Procedure Codes). A difference in the distribution of the groups was tested using a two-sided Wilcoxon rank-sum test.
Periodontal Disease Analysis
A total of 17 patients were included in our periodontal analysis as the 5 remaining participants were either edentulated prior to their baseline visit or were diagnosed to have a terminal dentition. Three of the 17 patients did not exhibit a change in periodontal status as determined by probing depth measurement and were thus excluded from analysis as they could not be evaluated for improvement. Three additional patients who were evaluated for periodontal disease at only one clinic visit were also excluded. The remaining 11 patients were used for periodontal analyses. Exam intervals varied from 6 and 24 months, with a median of 18 months. Relationship of final examination date to prosthodontics procedure date was not considered.
For graphical displays, patients are categorized by their periodontal status at initial examination.Patients with probing depth ≥ 4 mm with bleeding on probing (BOP) were classified as having periodontal disease. However, due to sample size limitations, statistical testing was done without stratification by disease using an exact, two-sided Wilcoxon signed-rank test.
Analyses for Questionnaires
outcome. The rescaling is accomplished by assigning the mean SF-36 v2 scale score from the 2000 general U.S. population (n=7472) to each response category measuring the same concept (Table 4.1, A Manual for Users of the SF-8 Health Survey, 2001). For example, for the question regarding Physical Functioning, the Likert values (0, 1, 2, 3, 4) are translated to (54.05, 48.33, 40.07, 30.31, 21.46) respectively. Thus, on the new scale, higher scores indicate better health.
Values for the other questionnaires, FAY, SADS and OHIP, are summarized on the original, Likert scale. For FAY and SADS, optimal outcomes for item responses were not unidirectional (i.e., 1 was optimal for certain items and 4 was optimal for other items). We reverse coded applicable responses so that a score of 1 is optimal and corresponds to higher self-worth (FAY), comfortability in social situations (SADS), and self-perceived oral health (OHIP). Mean SF-36 scale scores were not available for these questionnaires, so we were unable to rescale the values. The change in questionnaire score following prosthodontics was partially censored at zero due to the discrete nature of the Likert scale, and thus, an exact, two-sided Wilcoxon signed-rank test was used for within-arm comparison.
Analyses for Denture Subgroup Comparison
RESULTS
Oral Health over the Course of the Study
Of the 196 participants, a convenience sample of 22 HIV positive subjects were
rehabilitated with removable prostheses. The pros cohort was compared to the non-pros cohort. The majority of the prosthodontic cohort consisted of African American (77%) males (82%) , with a mean age of 44, mean CD4 count of 451 cells/uL and mean HIV viral load of 318 copies/mL (Table 1).
At baseline, the pros cohort had fewer sound teeth with a mean number of 21.25 teeth compared to 25.25 sound teeth in the non-pros cohort (Mann Whitney, p=0.06). There were fewer decayed coronal and root surfaces and fewer root fragments in the pros cohort compared to the non-pros group, however these difference were not statistically significant (Figure 2a). The pros cohort required more extractions than the non-pros cohort with a mean number 6.09 teeth extracted over the course of the study compared to a mean number of 1.87 teeth that need to be extracted in the non-pros cohort (Wilcoxon rank sum, p=0.01) (Figure 2b).
Regardless of prosthetic status, the majority of subjects had moderate to severe
periodontal disease (PD) at baseline with a mean extent PD (probing depths (pd)>3 with bleeding on probing) of 28.77 in the pros group and 29.52 in the non-pros group (not significant).
Likewise, measures related to attachment loss were not different between the groups. All
Qualitative outcomes after prosthodontic treatment in an HIV cohort
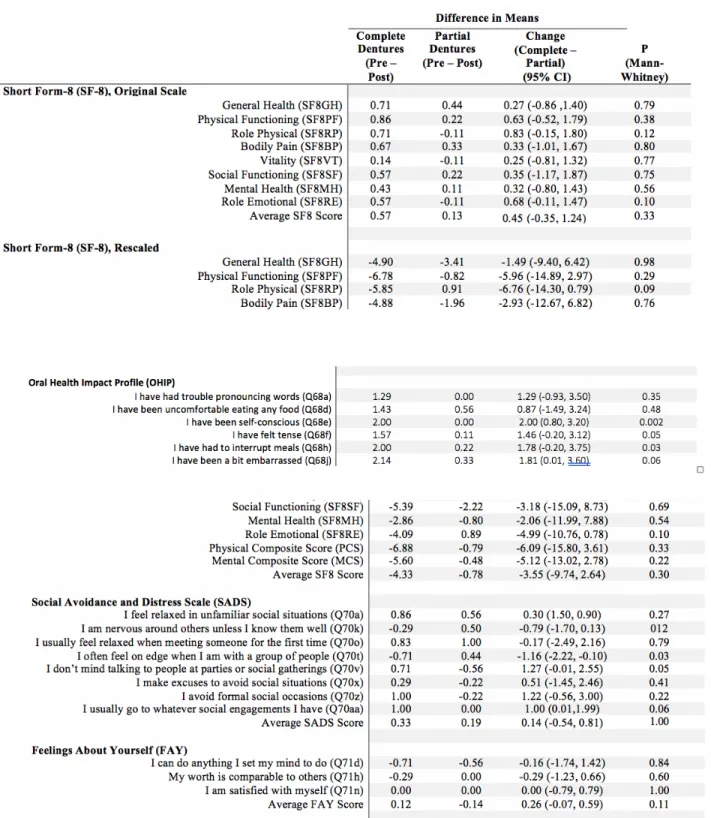
In order to assess the qualitative impact of prosthodontic treatment, four validated instruments were assessed that allowed assessment of overall wellness (SF8), oral health quality of life (OHIP), self-esteem (FAY) and social avoidance (SADS). For each of the four qualitative instruments, improvements were detected before and after treatment (Table 2, Figure 4a). Average median responses on the Likert scale before and after prosthodontic intervention were as follows: OHIP-14 – (1.07, 1.86 ns); SADS- (2.85,3.11 ns) FAY- (2.53, 2.59 ns); and SF-8 mental component (49.53, 54.96 p=0.01). Statistically significant improvements were detected for one of the four instruments overall (Figure 4a). However, there were some statistically significant findings for specific questions within the remaining surveys. The Short Form-8 (SF-8) is a measure of self-reported mental and physical wellness represented by mental component score (MCS) and the physical component score (PCS). SF8 scores are presented on the original, Likert scale (top) and rescaled (second table) using mean scores from the 2000 general U.S. Population (see Statistical Methods). General health and physical functioning were two of the eight health domains that showed a statistically significant improvement pre to
post-prosthodontic treatment (p=0.03 and p=0.05 respectively) (Fig 4f, Table 2). Overall, while not statistically significant, an increase in both PCS and MCS was observed (Figure 4e, Table 2.) Average median response on the Likert scale before and after prosthodontic intervention for SADS scale was 2.85 and 3.11 respectively- these differences were not significant. (Figure 4b, Table 2) However, individual item responses within the validated instrument did reveal differences with treatment. Three of the item responses showed a statistically significant
social engagements I have (Wilcoxin signed rank p= ≤ 0.05) (Figure 4b). For the OHIP
questionnaire, two items showed significant differences before and after prosthodontic treatment 1) I’ve been self-conscious 2) I’ve been a bit embarrassed (Wilcoxin signed rank p= ≤ 0.05) (Figure 4d). While not significant, item responses for FAY “I can do anything I set my mind to” and “My work is comparable to others” also revealed overall improvements before and after prosthodontic treatment.
Qualitative differences between complete denture recipients and partial denture recipients.
A qualitative analysis of outcome differences between prosthodontic treatment groups was performed. The difference in the means from pre to post-prosthodontic treatment between the CD group and RPD group revealed statistically significant differences for specific questions within two of the questionnaires, OHIP and SADS (Table 3, Figure 5).
In regard to social avoidance and anxiety participants rehabilitated with CDs felt “more on edge in a group of people” (Q70t) before treatment compared to RPD recipients (Mann Whitney, p=.03). There was also a significant difference in response to the statement “I don’t mind talking to people at parties or social gatherings (Q70v) where CD wearers exhibited a much greater difference in their response post-treatment (Mann Whitney, p=0.05).
CONCLUSIONS
This sub-study provides a comprehensive perspective on the interrelation between HIV, patient-reported outcomes, prosthodontics, oral and general health. There has not been a study in the literature to date which comprehensively assesses the impact of prosthodontic treatment using validated instruments within an HIV cohort. Secondary to the introduction of highly active antiretroviral therapy, HIV has now become a chronic disease. As such, the number of HIV positive people with these prosthetic needs will continue to increase. In the context of HIV, where feelings of stigma and shame are common117, patient-reported measures serve as a critical component to understanding to totality of the impact of care provision. It is clear that quality of life metrics can be poorer for PLWH, in fact HIV-infected women averaged 10% poorer OHRQOL than HIV-uninfected women (Mulligan, 2008). Overall, in this sub-study, there was a higher burden
of oral disease detected at baseline in patients requiring prosthodontic rehabilitation. We have shown that prosthodontic intervention leads to qualitative improvement in general health and wellness (SF-8, p=0.02) but we also observed improvements in select item responses related to OHRQoL and social avoidance and anxiety. In the setting of HIV, prosthodontic care was associated with improved self-perception of overall wellness; patients were less self-conscious and embarrassed. Similar to the general population, there was greater improvement in QoL in patients restored with complete dentures compared to partial dentures.
toward people with HIV.115 The fear of being judged often prevents people from doing many things in life including things related to self-care and overall quality of life. This study reinforces the fact that we can make real, tangible impacts and alter these patients lives for the good.
We understand that people with HIV may be more likely to seek preventive dental care if financial barriers are removed, they are actively taking ART medications, and are satisfied with their overall oral health.116These findings may impact policy making which is vital to the
planning of oral healthcare programs. Our group is in the process of modifying state and national HIV guidelines to include oral healthcare. Prosthetic intervention in an HIV positive population allows qualitative improvement in QoL as determined by SF8, and OHIP trending toward that of an HIV negative nationally representative sample.
Future directions of this study may include stratifying outcomes based on ART status, CD4 count, HIV viral load and diagnosis. Also, the utilization of a more prosthetically focused instruments such as the Burdens in Prosthetic Dentistry questionnaire (BiPD-Q)118 or the Prosthetic Esthetic Index (PEI)119might be more useful.
There is no existing research in understanding how these types of prosthodontic treatments impact the oral microbial status within the context of oral health and disease in this immune-compromised cohort which may be a future area of interest. The inclusion of other prosthodontic treatment types such as fixed restorations and those supported or retained by implants would be beneficial.
We have shown that improvements in oral health translate to improvements in self perceived systemic health. The growing number of people living with HIV much longer requires more effort to increase and strengthen integrated oral health promotion and disease prevention. These changes observed in the HIV positive cohort are similar to findings in the general population. In addition to those living with HIV, other groups such as the elderly, the
TABLE INDEX Pros Sub-cohort (n=22) Age Mean (yr) 44.64 (100%) Gender
Male 18 (82%)
Female 4 (18%)
Race/Ethnicity
Black or African American
(not Hispanic) 17 (77%) White (not Hispanic) 5 (23%)
CD4
Mean (cells/uL)
451.55 (100%)
HIV VL
Undetectable
(<50 copies/mL) 10 (45%) Detectable (≥50 copies/mL) 12 (55%) Self-Reported ART
Yes 20 (91%)
No 2 (9%)
Tobacco Use
(Smoking + Chewing Days)
None 9 (41%) 1-29 1 (5%)
30+ 12 (55%) Employment Status
Employed 10 (45%)
Unemployed 12 (55%)
Prosthesis Type
Complete (max or mand) 8 (36%) Immediate (max or mand) 2 (9%)
Table 1 Prosthodontic cohort demographics categorized according to HIV diagnosis.
Table 2 Health-Related Quality of Life Pre- and Post-Prosthodontics intervention in an HIV+ cohort.
Table 3. Qualitative assessments in HIV+ participants who received complete versus partial dentures.
FIGURES INDEX
Figure 1. General Study Design.
The multisite study enrolled a total of 2, 178 HIV positive individuals who were at different stages of disease progression. After study enrollment, initial oral exam completion, and baseline data collection, patients went through initial phase one treatment (caries control,
A.
B.
N Min Max Median Mean
Pros Cohort 22 0 32 1 6.09
Non-Pros
Cohort 175 0 25 0 1.87
C.
First Visit Last Visit Change (First-Last) (95% CI)
P
Probing Depth (PD) & Bleeding = Yes Extent PD ≥3 mm w
BOP
28.77 9.04 19.73 (10.36,
29.10)
<0.001 Attachment Loss (AL) & Bleeding = Yes
Extent AL ≥ 3 mm w BOP
8.30 1.51 6.79 (2.02, 11.55) <0.001
Figure 2. Oral health at baseline for pros versus non-pros cohort.
Figure 3. Response to Periodontal Therapy in a prosthetic HIV Cohort.
Horizontal limits of each box represent first quartile (25th percentile), median, and third quartile (75th percentile), respectively. The marker inside each box indicates the mean. ***p ≤ 0.001, **p ≤ 0.01, *p ≤ 0.05, Wilcoxon signed-rank test (testing is exact and two-sided).
Figure 4. (a-f): Qualitative Impact of Prosthodontic Treatment in a HIV Cohort
a) Self-perceived overall wellness according to averages of item responses for each questionnaire.
each box represent first quartile (25th percentile), median, and third quartile (75th percentile), respectively. The marker inside each box indicates the mean. ***p ≤ 0.001, **p ≤ 0.01, *p ≤ 0.05, Wilcoxon signed-rank test (testing is exact and two-sided). b) Item reponse for Social Avoidance and Distress Scale (SADS) pre- and post-prosthodontics. Horizontal limits of each box represent first quartile (25th
0.01, *p ≤ 0.05, Wilcoxon signed-rank test (
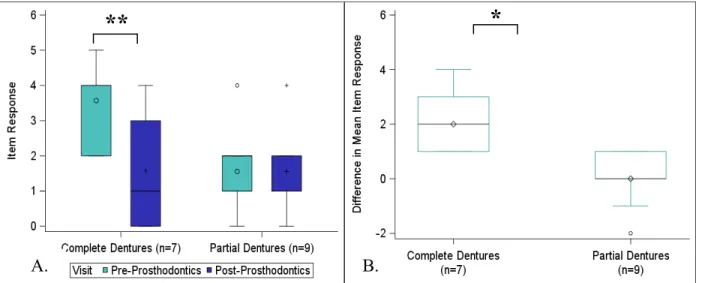
Figure 5. Complete denture recipients were more self-conscious than partial wearers “I have been self-conscious.”
A. Item response pre- and post-prosthodontics for patients who received complete dentures (complete maxillary or complete mandibular) versus patients who received partial dentures (acrylic RPD or cast metal RPD). B) Difference in mean item response pre- and
post-prosthodontics for each procedure group. Lower scores indicate positive self-worth, with an optimal score being zero. Horizontal limits of each box represent first quartile (25th
percentile), median, and third quartile (75th percentile), respectively. The marker inside each box indicates the mean. **p < 0.005, *p < 0.05, Wilcoxon signed-rank test for within and Wilcoxon rank-sum test for between procedure groups (testing is exact and two-sided).
**
*
REFERENCES
1. Health-Related Quality of Life (HRQOL) | CDC. https://www.cdc.gov/hrqol/index.htm. Accessed February 27, 2019.
2. Jeanty Y, Cardenas G, Fox JE, et al. Correlates of unmet dental care need among HIV-positive people since being diagnosed with HIV. Public Heal Rep. 2012;127 Suppl:17-24. doi:10.1177/00333549121270S204
3. What Is a Prosthodontist and the Dental Specialty of Prosthodontics?; 2018.
https://www.prosthodontics.org/assets/1/7/1.What_is_a_Prosthodontist_and_the_Dental_S pecialty_of_Prosthodontics__-_approved1.pdf. Accessed February 27, 2019.
4. GOLDMAN I. Practicing mouth rehabilitation successfully. N Y J Dent. 1949;19(12):415-422. http://www.ncbi.nlm.nih.gov/pubmed/24536288. Accessed February 16, 2019.
5. McLean JW. Full mouth reconstruction. Quintessence Int Dent Dig. 1978;9(11):41-47. http://www.ncbi.nlm.nih.gov/pubmed/397513. Accessed February 16, 2019.
6. FRANKS AST. The concept of oral rehabilitation. J Oral Rehabil. 1976;3(1):1-8. doi:10.1111/j.1365-2842.1976.tb00924.x
7. Rosenstiel SF, Land MF, Fujimoto J. Contemporary Fixed Prosthodontics.
8. Ferro K et al. The Glossary of Prosthodontic Terms 9th Ed. J Prosthet Dent. 2017;117(5S):e40.
9. Torrance GW. Utility approach to measuring health-related quality of life. J Chronic Dis. 1987. doi:10.1016/0021-9681(87)90019-1
10. Wilson IB. Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA J Am Med Assoc. 1995. doi:10.1001/jama.273.1.59
12. Slade GD. Assessing change in quality of life using the Oral Health Impact Profile.
Community Dent Oral Epidemiol. 1998;26(1):52-61. doi:10.1111/j.1600-0528.1998.tb02084.x
13. LOCKER, D. Concepts of oral health, disease and quality of life. Meas oral Heal Qual life. 1997. https://ci.nii.ac.jp/naid/10010687436/. Accessed February 17, 2019.
14. The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc Sci Med. 1995.
doi:10.1016/0277-9536(95)00112-K
15. Slade GD, Spencer JA. Development and evaluation of the oral health impact profile.
Community Dent Health. 1994;11:3-11.
16. Broder HL, Slade G, Caine R, Reisine S. Perceived impact of oral health conditions among minority adolescents. J Public Health Dent. 2000. doi:10.1111/j.1752-7325.2000.tb03326.x
17. McGrath C, Broder H, Wilson-Genderson M. Assessing the impact of oral health on the life quality of children: Implications for research and practice. Community Dent Oral Epidemiol. 2004. doi:10.1111/j.1600-0528.2004.00149.x
18. Preciado A, Del Río J, Suárez-García MJ, Montero J, Lynch CD, Castillo-Oyagüe R. Differences in impact of patient and prosthetic characteristics on oral health-related quality of life among implant-retained overdenture wearers. J Dent. 2012.
doi:10.1016/j.jdent.2012.07.006
19. Montero J, LÓpez JF, Galindo MP, Vicente P, Bravo M. Impact of prosthodontic status on oral wellbeing: A cross-sectional cohort study. J Oral Rehabil. 2009. doi:10.1111/j.1365-2842.2009.01968.x
20. Slade GD. Derivation and validation of a short-form oral health impact profile.
Community Dent Oral Epidemiol. 1997. doi:10.1111/j.1600-0528.1997.tb00941.x
21. Han C, Pulling CC, Telke SE, Hullsiek KH, C TBCP. Assessing the utility of five domains in SF-12 Health Status Questionnaire in an AIDS clinical trial. Aids. 2002;16(3):431-439. doi:10.1097/00002030-200202150-00015
1969;33(4):448-457. doi:10.1037/h0027806
23. Mann M, Hosman CMH, Schaalma HP, De Vries NK. Self-esteem in a broad-spectrum approach for mental health promotion. Health Educ Res. 2004. doi:10.1093/her/cyg041
24. Taylor SE, Kemeny ME, Reed GM, Bower JE, Gruenewald TL. Psychological resources, positive illusions, and health. Am Psychol. 2000. doi:10.1037/0003-066X.55.1.99
25. Pearlin LI, Schooler C. The structure of coping. J Health Soc Behav. 1978.
26. Winch RF, Rosenberg M. Society and the Adolescent Self-Image. Soc Forces. 2006. doi:10.2307/2575639
27. Goshima K, Lexner MO, Thomsen CE, Miura H, Gotfredsen K, Bakke M. Functional aspects of treatment with implant-supported single crowns: A quality control study in subjects with tooth agenesis. Clin Oral Implants Res. 2010. doi:10.1111/j.1600-0501.2009.01809.x
28. AlZarea BK. Oral health related quality-of-life outcomes of partially edentulous patients treated with implant-supported single crowns or fixed partial dentures. J Clin Exp Dent. 2017. doi:10.4317/jced.53661
29. John MT, Slade GD, Szentpétery A, Setz JM. Oral health-related quality of life in patients treated with fixed, removable, and complete dentures 1 month and 6 to 12 months after treatment. Int J Prosthodont. 2004;17(5):503-511.
30. Alzarea BK. Assessment and evaluation of quality of life (OHRQOL) of patients with dental implants using the oral health impact profile (OHIP-14) - A clinical study. J Clin Diagnostic Res. 2016. doi:10.7860/JCDR/2016/18575.7622
31. John MT, Slade GD, Szentpetery A, Setz JM. Oral health–related quality of life in patients treated with fixed, removable, and complete dentures 1 month and 6 to 12 months after treatment. J Prosthet Dent. 2005. doi:10.1016/j.prosdent.2005.02.013
32. Montero J, Castillo-Oyagüe R, Lynch CD, Albaladejo A, Castaño A. Self-perceived changes in oral health-related quality of life after receiving different types of conventional prosthetic treatments: A cohort follow-up study. J Dent. 2013.
33. Øzhayat EB, Gotfredsen K. Patient-reported effect of oral rehabilitation. Journal of Oral Rehabilitation. 2019.
34. Greene JC, Vermillion JR. The oral hygiene index: a method for classifying oral hygiene status. J Am Dent Assoc. 1960;61(2):172-179. doi:10.14219/JADA.ARCHIVE.1960.0177
35. GREENE JC, VERMILLION JR. THE SIMPLIFIED ORAL HYGIENE INDEX. J Am Dent Assoc. 1964. doi:10.14219/jada.archive.1964.0034
36. Löe H. The Gingival Index, the Plaque Index and the Retention Index Systems. J Periodontol. 2015. doi:10.1902/jop.1967.38.6_part2.610
37. Ferizi Shabani L, Begzati A, Dragidella F, Hysenaj Hoxha V, Hysenaj Cakolli V, Bruçi B.
The Correlation between DMFT and OHI-S Index among 10-15 Years Old Children in Kosova.; 2015.
38. Vakani F, Basaria N, Katpar S. Oral hygiene KAP assessment and DMFT scoring among children aged 11-12 years in an urban school of Karachi. J Coll Physicians Surg Pakistan. 2011.
39. Offenbacher S. Periodontal Diseases: Pathogenesis. Ann Periodontol. 1996;1(1):821-878. doi:10.1902/annals.1996.1.1.821
40. Löe H. Experimental Gingivitis. J Periodontol. 1965. doi:10.1111/j.1600-051X.2011.01710.x.Endotoxemia
41. Armitage GC. Development of a classification system. Ann Periodontol. 1999. doi:10.1097/00006199-197401000-00014
42. Wiebe CB, Putnins EE. The periodontal disease classification system of the American Academy of Periodontology - An update. J Can Dent Assoc (Tor). 2000.
43. Eke P, Page R. Update of the case definitions for population-based surveillance of periodontitis. J …. 2012. doi:10.1902/jop.2012.110664
44. Singer RE, Williams RC, Moss K, Barros SP, Offenbacher S, Beck JD. Periodontal Disease at the Biofilm–Gingival Interface. J Periodontol. 2007.
45. Witter DJ, Palenstein Helderman WH, Creugers NHJ, Käyser AF. The shortened dental arch concept and its implications for oral health care. Community Dent Oral Epidemiol. 2010. doi:10.1111/j.1600-0528.1999.tb02018.x
46. Hildebrandt GH, Dominguez BL, Schork MA, Loesche WJ. Functional units, chewing, swallowing, and food avoidance among the elderly. J Prosthet Dent. 1997.
doi:10.1016/S0022-3913(97)70100-8
47. HUNG H-C, WILLETT W, RIMM E, ROSNER BA, ASCHERIO A, JOSHIPURA KJ. Tooth loss and dietary intake. J Am Dent Assoc. 2014.
doi:10.14219/jada.archive.2003.0353
48. Joshipura KJ, Willett WC, Douglass CW. The impact of edentulousness on food and nutrient intake. J Am Dent Assoc. 1996;127(4):459-467.
doi:10.14219/jada.archive.1996.0237
49. Gaewkhiew P, Sabbah W, Bernabé E. Does tooth loss affect dietary intake and nutritional status? A systematic review of longitudinal studies. J Dent. 2017;67:1-8.
doi:10.1016/j.jdent.2017.10.012
50. Kapur KK, Soman SD. Masticatory performance and efficiency in denture wearers. J Prosthet Dent. 2006;95(6):407-411. doi:10.1016/j.prosdent.2006.03.012
51. LEAKE JL, HAWKINS R, LOCKER D. Social and functional impact of reduced posterior dental units in older adults. J Oral Rehabil. 1994;21(1):1-10.
doi:10.1111/j.1365-2842.1994.tb01119.x
52. Naka O, Anastassiadou V, Pissiotis A. Association between functional tooth units and chewing ability in older adults: A systematic review. Gerodontology. 2014.
doi:10.1111/ger.12016
53. Gilbert GH, Meng X, Duncan RP, Shelton BJ. Incidence of tooth loss and prosthodontic dental care: Effect on chewing difficulty onset, a component of oral health-related quality of life. J Am Geriatr Soc. 2004;52(6):880-885. doi:10.1111/j.1532-5415.2004.52253.x
54. Locker D, Slade GD. Association between clinical and subjective indicators of oral health status in an older adult population. Gerodontology. 1994;11(2):108-114.
doi:10.1111/j.1741-2358.1994.tb00116.x
Dent Oral Epidemiol. 2004. doi:10.1111/j.0301-5661.2004.00144.x
56. Satcher D. Oral Health in America: A Report of the Surgeon General. Vol 28.; 2000. doi:10.1002/yd.20021
57. Teófilo LT, Leles CR. Patients’ self-perceived impacts and prosthodontic needs at the time and after tooth loss. Braz Dent J. 2007;18(2):91-96.
doi:10.1590/S0103-64402007000200001
58. Saintrain MV de L, de Souza EHA. Impact of tooth loss on the quality of life.
Gerodontology. 2012;29(2):e632-e636. doi:10.1111/j.1741-2358.2011.00535.x
59. Fiske J, Davis DM, Frances C, Gelbier S. The emotional effects of tooth loss in edentulous people. Br Dent J. 1998. doi:10.1038/sj.bdj.4809551
60. Shah R, Diwan F, Diwan M, Chauhan V, Agrawal H, Patel G. A study of the emotional effects of tooth loss in an edentulous Gujarati population and its association with depression. J Indian Prosthodont Soc. 2016. doi:10.4103/0972-4052.161564
61. Gilbert GH, Duncan RP, Shelton BJ. Social determinants of tooth loss. Health Serv Res. 2003.
62. Seirawan H, Faust S, Mulligan R. The impact of oral health on the academic performance of disadvantaged children. Am J Public Health. 2012;102(9):1729-1734.
doi:10.2105/AJPH.2011.300478
63. Blumenshine SL, Vann WF, Gizlice Z, Lee JY. Children’s school performance: Impact of general and oral health. J Public Health Dent. 2008.
doi:10.1111/j.1752-7325.2007.00062.x
64. Maharani DA, Adiatman M, Rahardjo A, Burnside G, Pine C. An assessment of the impacts of child oral health in Indonesia and associations with self-esteem, school performance and perceived employability. BMC Oral Health. 2017. doi:10.1186/s12903-017-0358-5
65. Reissmann DR, Schierz O, Szentpétery AG, John MT. Improved perceived general health is observed with prosthodontic treatment. J Dent. 2011;39(4):326-331.