STAFF NURSE DECISIONAL INVOLVEMENT IN SOUTH KOREA: THE CONCEPT, MEASUREMENT, AND INFLUENCE OF NURSE DECISIONAL INVOLVEMENT ON NURSE JOB SATISFACTION, ORGANIZATIONAL COMMIMENT, AND TURNOVER
INTENTION
Jumi Lee
A dissertation submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the School
of Nursing.
Chapel Hill 2016
Approved by:
Havens, Donna S
Lynn, Mary R
Schwartz, Todd A
Sherwood, Gwen
© 2016 Jumi Lee
ABSTRACT
Jumi Lee: Staff Nurse Decisional Involvement in South Korea: The Concept, Measurement, and Influence of Nurse Decisional Involvement on Nurse Job Satisfaction, Organizational
Commitment, and Turnover Intention (Under the Direction of Donna S. Havens)
Improving the nurse work environment is essential to address the issue of increased staff
nurse turnover. Staff nurse decisional involvement has been studied in terms of improving the
nurse work environment and reducing staff nurse turnover. Thus, nursing management’s
involving staff nurse in decisions at their working unit level would be a good strategy to improve
the nurse work environment and reduce staff nurse turnover.
This dissertation is composed of three separate studies:
The purpose of chapter two was to define the concept, theoretical framework, and related
factors of staff nurse decisional involvement and to identify knowledge gaps in staff nurse
decisional involvement in English-speaking, Western versus non-English-speaking, Asian
countries. A total of 16 articles were selected from 102 articles originally retrieved to fill the
knowledge gaps in staff nurse decisional involvement using the PRISMA method. The
conceptual framework of staff nurse decisional involvement based on the content and context of
nursing practice framework was defined, and the findings showed that staff nurses actually were
less involved in decisions than they preferred to be both Western and Asian countries.
The purpose of chapter three was to translate the English version of the Decisional
Involvement Scale (DIS) (Havens & Vasey, 2003) into Korean (K-DIS) for use in South Korea.
Support Staff, Collaboration/Liaison Activities, Professional Practice Scope and Workforce for
Quality of Care, RN Recruitment, and Leadership. The instrument demonstrated good reliability,
but its validity was not strongly supported. Thus, further research on assessing the construct
validity of the K-DIS is necessary.
The purpose of chapter four was to examine the influence of staff nurse decisional
involvement on nurse job satisfaction, organizational commitment, and turnover intention. A
descriptive correlational design was used to analyze data (n=300) from staff nurses working in two
university hospitals (i.e., two urban, academic medical centers) in South Korea. The results show
that Korean staff nurses preferred more decisional involvement than they actually experienced.
The dissonance between the actual and preferred levels was negatively correlated with nurse job
satisfaction (rs= -.33, p<.0001) and organizational commitment (rs= -.24, p<.0001). In addition, it
was positively correlated with staff nurse turnover intention (rs= .30, p<.0001). Staff nurses’ low
decisional involvement in actuality means that staff nurses’ opinions are not reflected in nursing
administration decisions to improve the nurse work environment and nursing policies; this may
influence nurse turnover.
The clarity of the conceptual framework of the DIS will guide nurse administrators and
researchers to apply the results of the K-DIS in nursing administration in South Korea. Further
study is necessary to improve the construct validity of the K-DIS and to identify positive
To my family and friends, especially my parents, I could not have done this without your
ACKNOWLEDGEMENTS
I would like to express my sincere gratitude to the countless people who have supported
me throughout this journey. This pursuit would not have been possible without the support and
guidance of many people.
My thesis committee helped make this thesis a reality and I am grateful for their generous
support. Thank you to my dissertation chair and mentor, Dr. Donna Havens, You have believed
in me, taught me so much, and you have challenged me to do my best work. Thank you to my
committee members, Dr. Mary Lynn, Dr. Todd Schwartz, Dr. Gwen Sherwood, and Dr.
Young-Hee Yom, for their guidance and thoughtful review of this dissertation. All your support and
guidance over the last 5 years has been immeasurable. I truly can’t express what you all have
meant to me.
I especially appreciate the staff nurses who participated as subjects, nurse managers and
faculties who helped my research in South Korea. I could not have done this research without
your participation and help.
Thank you to my dear friends, Vicky Yeh and Chifundo Zimba. Your friendship and
support have helped me to stay motivated through challenging days in my doctoral study.
Special thanks you to my great mentor, Katherine Moore and my guardian angel. I'm
deeply impressed with your support and love from your thoughtful mind. You influence me
keep becoming a better person.
Nursing (2012), Glaxo Fellowship Fund Scholarship at the University of North Carolina School
of Nursing (2013), Global Health Scholar Award Scholarship at the University of North
Carolina School of Nursing (2015), and Teaching Assistant Scholarship at the University of
North Carolina School of Nursing (2014-2015).
And last but not least, I must thank my family. Especially my parents, Youngil and
TABLE OF CONTENTS
LIST OF TABLES ...x
LIST OF FIGURES ... xi
LIST OF ABBREVIATIONS ... xii
Chapter 1: Introduction ...1
Background and Significance ...1
Overview of the Key Concepts ...7
Theoretical Framework...9
Aims ...13
Prepared Manuscripts ...14
References ...17
Chapter 2: From an Integrative Literature Review to a Conceptual Framework for Staff Nurse Decisional Involvement….……….……….21
Introduction ...21
Methods ...23
Findings ...25
Conclusion ...44
References ... 51
Chapter 3: Use of the Decisional Involvement Scale (DIS) to Measure Staff Nurse Decisional Involvement in South Korea….……….…57
Results ... 69
Discussion ...72
Conclusion ...76
References ...84
Chapter 4: The Influence of Staff Nurse Decisional Involvement on Job Satisfaction, Organizational Commitment, and Turnover Intention in South Korea…..…89
Introduction ... 89
Methods ... 95
Results ...104
Discussion ...108
Conclusion ...114
References ...125
Chapter 5: Synthesis of Findings and Implications….………...129
Background ...129
Summary of Findings ...130
Strengths of Dissertation ...132
Limitations ...133
Implications for Nursing Management and Research ...134
Conclusion ...136
LIST OF TABLES
1.1 Comparison of PES-NWI scores in the USA and South Korea ...16
1.2 Comparison of the Ratio of Nurses to Patients (based on Medical Unit) ...16
2.1 Descriptive Characteristics of Reviewed Studies ...46
3.1 Revised K-DIS Factor Loadings and Reliabilities ...78
3.2 Revised K-DIS Mean (SD) Subscale Scores and Test-Retest Reliabilities ...79
3.3 Spearman Rank Correlations for Overall Revised K-DIS with IWS and ILS. ...79
3.4 Spearman Rank Correlations Between Revised K-DIS Subscales and the IWS Subscale ...80
3.5 Spearman Rank Correlations Between Revised K-DIS Subscales and ILS Subscales ...80
3.6 Items on the Original and Revised K-DIS ...81
3.7 Pearson Correlations Between Subscales of the Revised K-DIS ...82
3.8 Pearson Correlations Between Revised K-DIS 19 items ...83
4.1 Tests of Normality ... 116
4.2 Multiple Regression Results across Transformations of ILS ... 116
4.3 Multiple Regression Results across Transformations of K- DIS ... 117
4.4 Multiple Regression Results across Transformations of OCQ ... 117
4.5 Finding of Demographics ... 118
4.6 Descriptive Statistics and t-test for Actual and Preferred Level of K-DIS ... 119
4.7 Kappa Statistics for Agreement Test ... 120
4.8 Means and SD for the Actual, Preferred, and Dissonance Scores of K-DIS by Demographics ... 121
4.10 Multiple Regressions for the Staff Nurse Intention to Leave with Dissonance
of K-DIS, IWS, and OCQ ... 122
4.11 Main Effects of Multiple Regression Model for the Staff Nurse Intention to
Leave with Dissonance of K-DIS, IWS, and OCQ ... 123
4.12 ANCOVA for the Staff Nurse Intention to Leave with Dissonance of K-DIS,
IWS, and OCQ According to Demographic Characteristics ... 123
LIST OF FIGURES
1.1 The Theoretical Framework of Decisional Involvement Scale ...13
2.1 The Search and Retrieval Process of Literature ...25
2.2 The Theoretical Framework of the Combination of Scott’s Structure model of Hospital Work for Professionals and Aydelotte’s Professional Nursing Departments Model ...29
2.3 The Theoretical Framework of Kanter’s Structural Theory of Power in Organizations ...30
2.4 The Synthesized Conceptual Framework for Decisional Involvement ...32
2.5 The Conceptual framework of Staff Nurse Decisional Involvement...39
4.1 The Diagram for Hypothetical Relationship ...94
4.2 Sample Size Calculation ...97
4.3 A Model of Spearman Rank Correlation for Research Question 6 ...103
4.4 A Multiple Regression Model for Research Question 7 ...103
LIST OF ABBREVIATIONS
ANCOVA Analysis of Covariance
ANOVA Analysis of Variance
BT Back Translation
CFA Confirmatory Factor Analysis
CFI Comparative Fit Index
CONP Control over Nursing Practice
CVI Index of Content Validity
DIS Decisional Involvement Scale
EFA Exploratory Factor Analysis
GFI Goodness of Fit Model
GLM General Linear Model
IFI Incremental Fit Index
ILS Intention to Leave Scale
IWS Index of Work Satisfaction
K-DIS Korean Version of Decisional Involvement Scale
KMO Kaiser-Meyer-Olkin
MLE Maximum Likelihood Estimation
OCQ Organizational Commitment Questionnaire
PAF Principal Axis Factoring
PCA Principal Component Analysis
PDAQ Participation in Decision Activities Questionnaire
RMR Root Mean Square Residual
RMSEA Root Mean Square of Error of Approximation
RN Registered Nurse
rs Spearman Rank Correlations
CHAPTER 1: INTRODUCTION Background and Significance
The most important contemporary issues in health care organizations are ultimately
related to the ability of the health care system and its practitioners to provide safe high-quality
care. However, in South Korea, nurse turnover issues threaten patient safety and capacity to
deliver quality nursing care.
Nurses are the largest group (over 50%) of health care professionals providing direct
patient care in South Korean hospitals (Ministry of Health & Welfare in South Korea, 2013).
Thus, maintaining adequate nurse staffing is very important because the quality of patient care
is strongly linked to the performance of staff nurses at the patient bedside (J. Kim & M. Kim,
2011; Yoon & Kim, 2010). However, hospitals in South Korea are experiencing a severe nurse
turnover problem. According to the Hospital Nurse Association (2013) in South Korea, in 2013
nurse turnover was 16.9%, surpassing Jones’s (1992) recommendation to keep turnover below
15% to maintain stability in the nursing workforce. In addition, when comparing the number of
nurses in South Korea with other Organization for Economic Cooperation and Development
(OEDC) countries, the ratio of nurses to population is 4.7 to 1,000 in South Korea and 8.7 to
1,000 in OECD countries (Statistics Korea, 2013). This ratio again demonstrates the potential
for increased longed turnover which could lead to work overloads and burnout for the
remaining staff nurses, as well as adverse effects on patient care.
organizational factors, and national factors. First, the individual factors are age, education,
position, marriage status, pay, and career advancement and so forth (J. Kim & M. Kim).
Findings from this study relating to individual factors which have been relatively consistent
over time will be addressed in the third dissertation manuscript. Second, there is a myriad of
variables included in the organizational factors that may lead to increased staff nurse turnover:
work overloads, burnout, unsupportive nursing work environment, and low autonomy as
professionals and so forth. These may reduce nurse job satisfaction and organizational
commitment (Kang, 2012; Kwon & Kim, 2012; Kim & Han, 2013; Kim & Seomun, 2013;
Sung, Choi, & Chun, 2011; Sung, Keum, Roh, & Song, 2013). Korean staff nurses reported the
lowest scores on the Staffing and Resource Adequacy scale among the five subscales of the
Practice Environment Scale of Nursing Work Index (PES-NWI) (Cho, Choi, Kim, Yoo, & Lee,
2011; Kang, 2012) (see Table 1.1). This result may be due to the high nurse to patient ratio.
The legal standard recommended by the Korean Ministry of Health Welfare for the ratio of
nurses to patients in South Korea is 1 to 12 (You, 2013). However, only 7.1 % of the hospitals
observe this ratio, and 59.1% of the hospitals maintain the ratio of 1 to 15-16 (Korean Hospital
Nurse Association, 2013; You, 2013) (see Table 1.2). According to You’s (2013) study,
comparing this ratio of 1 to 12 in South Korea with 1 to 3 in Japan (Japanese Nursing
Association, 2009) and 1 to 4 in the (National Nurses United, n. p) implies that Korean nurses
are overworked. In addition, based on the new scoring methods to identify the favorability of
nurse practice environments (i.e. unfavorable (scores below 2.5 on one subscale), mixed
(scores above 2.5 on 2–3 subscales), and favorable (scores- over 2.5 on 4-5 subscales) (Lake &
Friese, 2006), the average score 2.58 on 5 subscales of Korean nurses would suggest a
average score of 2.65 for nurses working at the non-magnet hospitals in the USA, and even
less than the mean score of 2.95 for nurses working at Magnet hospitals in the USA (Cho et al.,
2011; Lake, 2002) (see Table 1.1). In
particular, the scores on the subscales of Nurse Participation in Hospital Affairs and Staffing
and Resource Adequacy were lower than 2.5 (Cho et al., 2011), suggesting that nurses in South
Korea do not have enough opportunities to participate in hospital affairs to advocate to improve
their staffing and resource adequacy issues.
Adding insult to injury, due to the heavy workloads (J. Kim & M. Kim, 2011; Yoon &
Kim, 2010), even though nurses are professionals, they report having low autonomy and low
control over nursing practice. Autonomy and control over nursing practice (CONP) refer to the
freedom, power, and authority to make decisions related to professional practice (Weston, 2009).
Autonomy can be differentiated into two discrete concepts-clinical and work autonomy:
Clinical autonomy means the authority, freedom, and discretion to indicate clinical nursing
judgments in the context of an interdependent practice for patient care (Weston, 2008). In
contrast, work autonomy was defined as freedom and discretion in work scheduling, work
methods, and work criteria to evaluate and achieve goals within the existing structures and
operations (Breaugh, 1985; Van der Doef & Maes, 1999; Weston, 2009). Unlike clinical and
work autonomy, CONP was defined as freedom, authority, and discretion of nurses to make
decisions in the context of nursing practice including organizational structures, governance,
rules, policies, and operations (Weston, 2008).
Most staff nurses know well the importance of clinical autonomy and work autonomy and
also want to have full status of the both autonomy as professionals. However, they easily
rather than organizational structures, governance, rules, policies, and operations (Weston, 2008),
which may cause adverse effects to establish the full status of clinical autonomy and work
autonomy in South Korea. Especially, under the heavy workloads (J. Kim & M. Kim, 2011;
Yoon & Kim, 2010), staff nurses may not have time or energy for decisional involvement for
nursing policy and administration. According to the study “Experience of Nurse Turnover,”
staff nurses have said that they frequently feel burned out because of the work overload (Lee &
Kim, 2008). Staff nurses do not want to join in other activities in hospitals because they feel that
they are already too busy to finish routine assignments and tasks of the day (Kim & Han, 2013;
Kim & Seomun, 2013; Sung et al., 2013).
Moreover, these working conditions may influence other issues, such as other health
professionals’ and the administration’s thoughts about recognizing that the nurse is a
professional. They view staff nurses as employees just carrying out the routine jobs of nursing,
so they exclude staff nurses from decisional involvement in hospitals about patient care and
hospital administration and policy (Wandelt, Pierce, & Widdowson, 1981; Lee & Kim, 2008).
As a result, Korean staff nurses have conflicting feelings about themselves as professionals,
because they do not have full clinical autonomy and work autonomy in their hospitals (Lee &
Kim, 2008). This result may lead to adverse consequences such as high nurse turnover in South
Korea. Aydelotte (1983) also said that “The inability to exercise control over clinical practice
may produce feelings of career stagnation. This career stagnation and related factors have
caused nurses to leave nursing and remain outside the workforce. The end of this result has
been a nurse shortage” (p. 836). Not only that, lack of recognition for professional nurses by
other influential groups may lead to nurses’ being excluded from decisional involvement in
unsupportive for professional nursing policy and the nursing work environment, so the vicious
cycle for nurse turnover continues in South Korea (B. Kim et al., 2013; You, 2013).
Third, the national factors are Korean cultural issues, organizational culture, and
unsupportive Korean national healthcare policy for nursing workforce stability (B. Kim et al.,
2013; S. Kim & J. Kim, 2012; Y. Kim, S. Kim, & J. Kim, 2013; You, 2013). The Korean
culture (i.e., conservatism), influences organizational culture. Especially, as representative
organizations that maintain a conservative tendency, hospitals in South Korea have hierarchical
atmospheres (Han, 2002; Korean Hospital Nurses Association, 2010; K. Park, S. Park, & Yu,
2014). The current organizational structure of hospitals tends to be flat because of
reorganization to reduce the superstructure. However, staff nurses still report hierarchical and
authoritative organizational cultures of managers and administrators, which stems from the
Asian conservatism-retaining bureaucracy (Im, Kim, Ko, &Lee, 2012; K. Kang, Han, & S.
Kang, 2012; Liu, Hus, & Chen, 2015; Park, & Lee, 2011). Gender disparity related to male
physician power also exists (Kim, Yim, Jeong, & Jo, 2009; Lee & Kim, 2008). Moreover,
Korean nurses typically have a relationship-oriented culture (i.e., collectivism), so they show a
tendency to avoid conflicts with silence and to pretend that they maintain affiliation (K. Kang et
al., 2012; Lee & Kim, 2008; Sung et al., 2011). Thus, speaking about problems may be seen as
breaking the order and affiliation (K. Kang et al., 2012; Lee & Kim, 2008; Liu et al., 2015).
Regarding issues of healthcare policy in South Korea, the current Korean national
medical law for nurse staffing shows no in-depth analysis of the reasons for nurse turnover and
no deep knowledge about professional nursing practice (B. Kim et al., 2013). Most policies that
have been developed have focused only on how to increase the number of nurses (B. Kim et al.,
in nursing schools and compensating hospitalization fees to hospitals based on their nurse
staffing levels. These tend to be plausible to increase nurse staffing, but this cannot lead
hospitals to set adequate staffing for nursing workforce stability (S. Kim & J. Kim, 2012; You,
2013). The reason is that the current healthcare policies for such as hospitalization, health
insurance, and DRG fees do not consider nurse employment costs. Thus except for a few large
hospitals, most hospitals of small and middle size are just trying to keep the middle or lower
level of nurse staffing (S. Kim & J. Kim, 2012). Also, there is no sanction for staffing violations,
thus, even so many small and middle-sized hospitals (78.9%) do not report their nurse staffing
(You, 2013). As a result, these policies motivated hospitals to decrease nurse staffing grades
because cost reduction is better than compensation (Y, Kim, S, Kim, & J, Kim, 2013). Currently,
over 25% of the young nurses of the whole body of licensed nurses do not work in nursing
(Korean Hospital Nurse Association, 2013). Nevertheless, the Korean government is still
suggesting facile policies to increase the number of nurses without considering nursing care
quality and the expertise of the nurses (Korean Hospital Nurse Association, 2013; You, 2013).
To resolve high staff nurse turnover in South Korea, we need to track why this situation
happens. According to Yu (2007), the most critical reason causing the high staff nurse turnover
is the exclusion of staff nurses’ practical opinions and ideas in the decision-making that governs
nursing practice policy and administration. Even though staff nurses are at the frontline of
hospitals for patient care, they are left out of decisions for improving professional nursing
practice and the nursing work environment in South Korea. Therefore, we need a paradigm shift
to solve these problems in relation to the current nursing fields of South Korea by going back to
staff nurses’ decisional involvement. Thus staff nurses’ DI should be the top priority for nursing
leave and reduce turnover, (b) to improve the nursing work environment and nursing policy, and
(c) to attain full professional status for nurses.
The Key Concepts
As a key strategy to increase nurse satisfaction, patient safety, safe quality patient
outcomes, the importance of the staff nurse participation in decision-making that fosters
autonomy and control over nursing practice (CONP) have been supported by nursing literature
on Magnet hospitals and patient safety (Weston, 2008). However, the concepts of decisional
involvement, shared governance, autonomy, CONP have frequently been confused and
commingled in the nursing literature (Weston, 2008). Thus, this confusion makes it more
difficult to understand hindering the synthesis of knowledge and application of these concepts
in practice. Therefore, to clearly analyze and interpret this study, the key concepts of these
terms were defined.
Staff Nurse Decisional Involvement
Havens and Vasey (2003) defined Decisional involvement as “the pattern of distribution
of authority for decisions and activities that govern nursing practice policy and the practice
environment” (p. 332). Thus, staff nurse decisional involvement means the staff nurse has
authority and responsibility in governance for nursing practice policy and the practice
environment.
Governance
Governance indicates “the maintenance of social, political, and economic arrangement by
which practitioners maintain control over their practice, self-discipline, working conditions, and
professional affairs, so without governance, there is no autonomy and full professional status is
professional status, autonomy must be exercised within its defined area of practice. Thus, staff
nurse decisional involvement in governance is essential to have full professional status and
autonomy.
Shared Governance
Shared Governance is regarded as a structural model which enhances staff-manager
partnership on shared decision making that is for improving nursing practice policy and the
practice environment) (Porter-O’Grady, 2003). Thus, through the shared governance structure,
“nurses can express and manage their practice with a higher level of professional autonomy”
(Porter-O’Grady, 2003, p. 251). The professional autonomy entails accountability and
responsibility for improving nursing practice quality and patient safety.
Autonomy: Clinical Autonomy and Work Autonomy
Autonomy is defined as “freedom, power, and authority to make decisions related to
professional practice,” which is usually differentiated into two discrete concepts, clinical
autonomy and work autonomy (Weston, 2009, p87). Clinical autonomy means the authority,
freedom, and discretion to indicate clinical nursing judgments in the context of an
interdependent practice for patient care (Weston, 2008). In contrast, work autonomy was defined
as freedom and discretion in work scheduling, work methods, job process, and work criteria to
evaluate work and achieve goals within the existing structures and operations (Breaugh, 1985;
Van der Doef & Maes, 1999; Weston, 2009).
Control over Nursing Practice (CONP)
Unlike clinical and work autonomy, Control over Nursing Practice (CONP) is defined as
structures, governance, and policies in the context of nursing practice, rather than individual
decisions related to clinical practice or work (Weston, 2008).
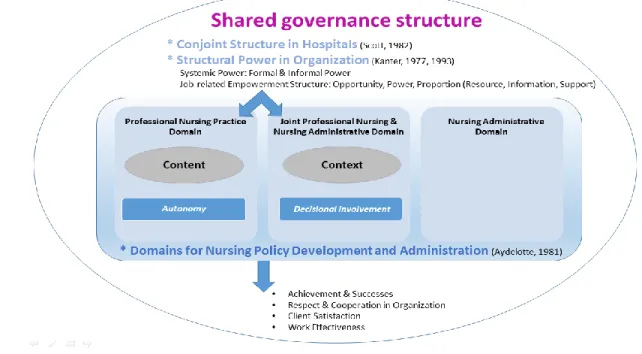
Theoretical Framework
A combination of the professions model (Scott, 1982) and the professional nursing
department model (Aydelotte, 1981) provides a theoretical framework for understanding
professional organization structures and policy development and administration for professional
nurses. This framework is the premise to understand the domains of needed participation of
staff nurses in decision making in hospitals and to encourage staff nurse decisional involvement
regard to their autonomy and control over nursing practice (CONP) as professional nurses in
hospitals. An overview of the key concepts of the combination of the two models will be
presented as well as a conceptualization of autonomy and CONP within this theoretical
framework.
Professions Model
Based on a sociological point of view, Scott (1982) suggested three organizational models
for structuring the work of professional participants within hospitals: the autonomous, the
heteronomous, and the conjoint professional organizational structure. He discussed each of
these structures by describing the relationship between physicians and administrators as a way
to explain the models. In the autonomous structure, because of the specialty and great social
value, professionals (e.g., physicians) have sole authority and responsibility, and organizational
administrators delegate responsibility to the professional group for defining, setting,
implementing, and maintaining performance and standards (Scott, 1982). Thus, the professional
group has governance and organizes itself to have political, economic, and legal support (Scott,
individual patients (i.e., micro care), peer controls are relatively ineffective and sometimes
cause ethical issues (Scott, 1982). In contrast to the autonomous structure, in the heteronomous
structure, organizational administrators have solitary authority and responsibility, and
professional participants are clearly subordinated to an administrative framework (Scott, 1982).
Under this structure, the administrators need to solve conflicts between professionals and other
healthcare professionals (indispensable contributors) to deliver care and also consider problems
of diluting personal responsibility and limited resources for distribution (Scott, 1982). Thus, for
the overall shape of the desired outcome distribution for patients (i.e., macro care),
administrators prefer macro care in conditions of cost constriction, which brings a cost-quality
trade-off (Scott, 1982). To complement for the weakness of both structures, Scott (1982)
suggested the conjoint structure, which is a potentially ideal model for structuring professional
work in health organizations. In the conjoint structure, professionals and administrators have an
equal distribution of power, and professional and administrators have considerable
differentiation in their functions (Scott, 1982). For example, healthcare professionals and other
care practitioners specialize in the delivery of micro care for patients, and administrators and
managers engage in the delivery of macro care (Scott, 1982).
Under the structure of a hospital, as one professional group of the substructures, nurses’
groups also should be able to influence their professional nursing practice under the conjoint
structure for nursing care quality. Thus, the conjoint structure of health organizations should be
a precondition for the realization of the professional nursing department model in South Korea.
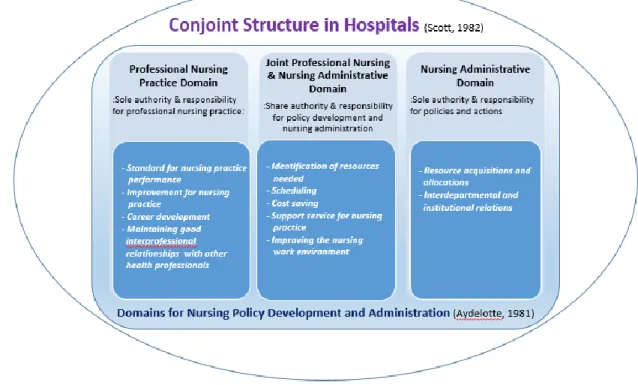
Professional Nursing Department Model
In the professional nursing department model, Aydelotte (1981) suggests three domains
practice policy and administration as following: (a) the professional nursing practice domain
where professional nursing practice staff have sole authority and responsibility for professional
nursing practice, such as nursing practice performance standards and improvement, their career
development as professionals, and maintaining good interprofessional relationships with other
health professionals (Aydelotte, 1981). In contrast to this, (b) the nursing administrative domain
where nursing administrative staff have sole authority and responsibility for policies and actions
related to resource acquisition, allocations, and interdepartmental and institutional relations
(Aydelotte, 1981). The third, (c) joint professional nursing practice and nursing administrative
domain where the two share authority and responsibility for policy development and nursing
administration, such as identification of resources needed, scheduling, cost saving, support
service for nursing practice, and improving the nursing work environment (Aydelotte, 1981).
Related to question “How staff nurses can be involved in decisions (i.e., how) as
professionals under healthcare organizations (e.g., hospitals), Scott’s (1982) professional model
gives guidance for the ideal structure of professional work in hospitals by suggesting the
conjoint structure. On the other hand, Aydelotte’s model addresses more specific aspects related
to the professional nursing department for encouraging staff nurse decisional involvement—(a)
Why staff nurses (i.e., who)? (b) Why is decisional involvement important (i.e., why)? (c) How
can staff nurses be involved in decisions (i.e., how)? (d) What fields need the staff nurses’
decisional involvement (i.e., what and where)?—which are also related to clinical autonomy,
work autonomy, and control over nursing practice (CONP). First, to address (a) and (b): Staff
nurses provide bedside care and can detect a patient’s status and problems most quickly; thus,
reflecting staff nurses’ ideas and opinions for supporting staff nurses is fundamental in
professional having professional qualifications, such as —professional education curriculum,
license, a code of ethics, and standards of nursing practice (Aydelotte, 1983). Thus, based on
professional nursing knowledge and skills, each professional nurse is qualified to have
authority and responsibility for doing professional nursing practice (i. e., clinical autonomy &
work autonomy), as well as they should be able to develop policy and administration, to
advance the work environment and identify nursing resources needed (i.e. CONP) (Aydelotte,
1983). Second, to address (c) and (d): Actually, instituting a correct balance reflecting staff
nurses’ and administrators’ authority and responsibility for hospital strategic goals can be
challenging (Houston, Leveille, Luquire, Fike, Ogola, & Chando, 2012). In terms of this,
Aydelotte’s model (1983) clearly shows which domains need shared authority and
responsibility of professional nursing staff and nursing administrations for policy development
and nursing administration such as identification of resources needed, scheduling, cost saving,
support service, general personnel policies, and nursing work environment. Thus, this like
shared governance.
Therefore, the combination of the two models for hospital work structure for professionals
and professional nursing departments can be conceptualized with the concepts of autonomy and
control over nursing practice within the theoretical framework shown in the following diagram
Figure 1.1 The theoretical framework of Decisional Involvement Scale.
Aims
This dissertation is composed of three manuscripts that each contributes to the literature
with regards to staff nurses’ decisional involvement in practice and policy in South Korean
hospitals. Specifically, the aims are to:
1. Present a literature review to define the concept of nurse decisional involvement with
relating factors—attributes, antecedents, and consequences—based on the theoretical
framework of decisional involvement, and to identify the knowledge gaps in staff nurse
decisional involvement in English-Speaking, Western versus Non-English-Speaking,
Asian Countries.
2. Measure the current status of staff nurses’ decisional involvement in South Korea, by
South Korea, and then reporting psychometric assessments of the Korean version of
Decisional Involvement Scale (K-DIS).
3. Evaluate the influence of nurse decisional involvement on job satisfaction,
organizational commitment, and turnover intention of staff nurses in South Korea.
Manuscripts
The three manuscript option was chosen in lieu of a traditional dissertation. Chapter one
provides an introduction to the significance of staff nurse decisional involvement in South
Korea about the issues of high staff nurse turnover and the importance of nurse autonomy and
control over nursing practice. The theoretical framework, key concepts, and aims of the three
studies have been described. Chapters two through four of this dissertation present three
manuscripts, which will be prepared for publication. Chapter five provides a discussion of the
manuscripts, implications of the findings from this work for nursing education, administration
and policy in South Korea, and the plans for future study.
Chapter two is titled “From an Integrative Literature Review to a Conceptual Framework
for Staff Nurse Decisional Involvement.” The purpose of this component is to identify
knowledge gaps in staff nurse decisional involvement to provide evidence for the necessity of
the Decisional Involvement Scale (DIS) in South Korea based on the theoretical framework.
Chapter three focuses on the revision and application of the Decisional Involvement Scale
(DIS) developed by Havens and Vasey (2003), so this chapter three is titled “Use of the
Decisional Involvement Scale (DIS) to Measure Staff Nurse Decisional Involvement in South
Korea.” The purpose of this study is psychometric testing of the Korean version of DIS (K-DIS)
Chapter four is titled “The Influence of the staff Nurse Decisional Involvement on Job
Satisfaction, Organizational Commitment, and Turnover Intention in South Korea.” The
purpose of this study is to examine whether the nurse decisional involvement at the nursing
unit-level affects the job satisfaction, organizational commitment, and turnover intention of staff
Table 1.1
Comparison of PES-NWI Scores in the USA and South Korea
Mean a ± SD of Nurses in
Magnet Hospitals in the USA(Lake, 2002)
(n=1,610)
Non-Magnet Hospitals in the USA(Lake, 2002)
(n=689)
Hospitals in South Korea(Cho et al., 2011)
(n=733) Nurse Participation in
Hospital Affairs
2.76 ±0.47 2.44b±0.44 2.45±0.47
Nursing Foundation for Quality of Care
3.09±0.39 2.83b±0.36 2.86±0.43
Nurse Manager Ability, Leadership, and Support of Nurses
3.00±0.59 2.68b±.60 2.68±0.57
Staffing and Resource Adequacy
2.88±0.62 2.49b±0.62 2.20±0.59
Collegial Nurse-Physician Relations
2.99±0.52 2.65b±0.37 2.54±0.58
Composite 2.95±0.40 2.65b±0.37 2.58±0.42
Note. a Potential score range for the mean is 1–4. Higher scores indicate more: Values above 2.5 indicate agreement, values below 2.5 indicate disagreement (Lake & Friese, 2006).
b Is significantly less than the corresponding subscale means in the magnet hospitals (p < .0001).
Table 1.2
Comparison of the Ratio of Nurses to Patients a
Grade
South Korea (You, 2013)
USA** Japan***
Current Criteria (RN: BOR*)
Ratio of RN to Patients
Ratio of RN to Patients
Ratio of RN to Patients
1 1: Less 2.5 1:12
1:5 1:7
2 1: 2.5~ less3.0 1:13~1:14 3 1: 3.0~ less3.5 1:15~1:16 4 1: 3.5~ less4.0 1:17~1:19 5 1: 4.0~ less4.5 1:20~1:21 6 1: 4.5~ less6.0 1:22~1:29
7 1: 6.0 1:30
Note. a Comparison based on medical units *BOR: the average bed occupancy rate per year
REFERENCES
Aydelotte, M. (1981). Structure of nursing practice departments: Governance and
professionalization. In J. McCloskey & H. K. Grace (Eds.), Current issues in nursing (2nd ed., pp. 394–404). Boston: Blackwell Scientific Publications.
Aydelotte, M. (1983). Professional nursing: The drive for governance. In N. Chaska (Ed.), The nursing profession: A time to speak (pp. 830–842). New York: McGraw-Hill Book Company.
Breaugh, J. A. (1985). The measurement of work autonomy. Human Relations, 38, 551–570.
Cho, E., Choi, M., Kim, E. Y., Yoo, I. Y., & Lee, N. J. (2011). Construct validity and reliability of the Korean version of the practice environment scale of nursing work index for Korean nurses. Journal of Korean Academy of Nursing, 41(3), 325–332.
Han, S. J. (2002). A Study on the relationship between nursing organizational culture and organizational performance. Journal of Korean Academy of Nursing Administration, 8(3), 441–456.
Havens, D. S., & Vasey, J. (2003). Measuring staff nurse decisional involvement: The decisional involvement scale. Journal of Nursing Administration, 33(6), 331–336.
Houston, S., Leveille, M., Luquire, R., Fike, A., Ogola, G. O., & Chando, S. (2012). Decisional involvement in Magnet®, Magnet-aspiring, and non-Magnet hospitals. Journal of Nursing Administration, 42(12), 586–591.
Im, S. B., Kim, S. Y., Ko, Y., & Lee, M. Y. (2012). Clinical nurses' perceptions on nursing organizational culture and differences in their perceptions according to age groups. Journal of Korean Clinical Nursing Research, 18(2), 215–227.
Japanese Nursing Association (2009). On public health nurses, midwives and nurses act '60 history: History and development of the nursing of nursing administration.
Japanese Nursing Act '60 History Compilation Committee ed. Japanese Nursing Association Publishing Company.
Jones, C. B. (1992). Calculating and updating nursing turnover costs. Nursing Economics, 10(1), 39–45.
Kang, K. H., Han, Y. H., & Kang, S. J. (2012). Relationship between organizational communication satisfaction and organizational commitment among hospital nurses. Journal of Korean Academy of Nursing Administration, 18(1), 13–22.
Kim, B. H., Chung, B. Y., Kim, J. K., Lee, A., Hwang, S. Y., Cho, J. A., & Kim, J. A. (2013). Current situation and the forecast of the supply and demand of the nursing workforce in Korea. Journal of Korean Academy of Adult Nursing, 25(6), 701–711.
Kim, H. S., Yim, H. W., & Jeong, S. H., & Jo, S. J. (2009). An association among verbal abuse, social support and turnover intention for special unit nurses in a hospital. Korean Journal of Occupational and Environmental Medicine, 21(4), 388–395.
Kim, J. K., & Kim, M. J. (2011). A review of research on hospital nurses' turnover intention. Journal of Korean Academy of Nursing Administration, 17(4), 538–550.
Kim, K. S., & Han, Y. H. (2013). A study on intention to quit and job overload, role ambiguity, burnout among nurses in the general hospital. Korean Journal of Occupational Health Nursing, 22(2), 121–129.
Kim, M. R., & Seomun, G. (2013). Relationships among burnout, job satisfaction,
organizational commitment and turnover intention to resign in hospital nurses. Korean Journal of Occupational Health Nursing, 22(2), 93–101.
Kim, S., & Kim, J (2012). A proposal to improve nursing fee differentiation policy for general hospitals using profitability: Analysis in the national health insurance. Journal of Korean Academy of Nursing, 42(3), 351–360.
Kim, Y. M., Kim, S. Y., & Kim, J.Y. (2013). Development of the DRG fee adjustment mechanism reflecting nurse staffing grades. Journal of Korean Clinical Nursing Research, 19(3), 321–332.
Korean Hospital Nurses Association. (2010). Research on nursing organizational culture. Seoul: Author.
Korean Hospital Nurse Association (2013). The annual report: Status of hospital nursing workforce in South Korea. Seoul: Korean Hospital Nurse Association. Retrieved from http://www.khna.or.kr/web/information/resource.php
Kwon, J. O., & Kim, E.Y. (2012). Impact of unit-level nurse practice environment on nurse turnover intention in the small and medium-sized hospitals. Journal of Korean Academy of Nursing Administration, 18(4), 414–423.
Lake, E. T. (2002). Development of the practice environment scale of the nursing work index. Research in Nursing & Health, 25(3), 176–188.
Lake, E. T., & Friese, C. R. (2006). Variations in nursing practice environments: Relation to staffing and hospital characteristics. Nursing Research, 55(1), 1–9.
Liu, Y., Hsu, H., & Chen, H. (2015). Staff nurse decisional involvement: An internet mixed- method study in Taiwan. Journal of Nursing Management, 23, 468–478.
n/an/a.doi:10.1111/jonm.12154
Ministry of Health & Welfare in South Korea. (2013). Ministry of health and welfare yearbook 2013. Retrieved from
http://stat.mw.go.kr/front/statData/mohwAnnalsWpView.jsp?menuId=14&bbsSeq=1&ntt Seq=21132&nttClsCd=01&searchKey=&searchWord=&nPage=1
National Nurses United. (n. p). The National campaign for safe RN-to-patient staffing ratios- proposed RN ratio. Retrieved from
http://www.nationalnursesunited.org/issues/entry/ratios
Park, J., & Lee, M. (2011).The effect nursing organizational culture on job satisfaction and turnover intention tin general hospital: The Mediation effect of empowerment. The Korean Journal of Health Service Management, 5(3), 1–11.
Park, K., Park, S., & Yu, M. (2014). Review of research in nursing organizational culture in Korea. The Journal of the Korea Contents Association, 14(2), 387–395.
Porter-O'Grady, T. (2003). Researching shared governance: A futility of focus. Journal of Nursing Administration. 33(4), 251–252.
Scott, R. (1982). Managing professional work: Three models of control for health organizations. Health Services Research, 17(3), 213–240.
Statistics Korea (2013). Korea statistical information service: Healthcare personnel in Korea. Retrieved from http://kosis.kr/wnsearch/totalSearch.jsp
Sung, M. H., Choi, W. J., & Chun, H. K. (2011). The relationship of negative emotion, emotion suppression, and job satisfaction to organizational commitment in hospital nurses.
Journal of Korean Academy Fundamental Nursing, 18(2), 258–266.
Sung, M. H., Keum, E. J., Roh, H. J., & Song, M. H. (2013).The relationship among job overload, self-efficacy, emotional exhaust and turnover intention in clinical nurses. Korean Journal of Occupational Health Nursing, 22(2), 130–139.
Van der Doef, M., & Maes, S. (1999). The job demand-control (-support) model and
psychological well-being: A review of 20 years of empirical research. Work & Stress, 13, 87–114.
Wandelt, M. A, Pierce, P. M, Widdowson, R. R. (1981).Why nurses leave nursing and what can be done about it. American Journal of Nursing, 81(1), 72–77.
Weston, M. J. (2008). Defining control over nursing practice and autonomy. Journal of Nursing Administration, 38(9), 404–408.
Yoon, G. S., & Kim, S. Y. (2010). Influences of job stress and burnout on turnover intention of nurses. Journal of Korean Academy of Nursing Administration, 16(4), 507–516.
You, S. J. (2013). Policy implications of nurse staffing legislation. The Journal of the Korea Contents Association, 13(6), 380–389.
CHAPTER 2: FROM AN INTEGRATIVE LITERATURE REVIEW TO A CONCEPTUAL FRAMEWORK FOR STAFF NURSE DECISIONAL INVOLVEMENT
Introduction
Nurses are not only the frontline workforce for direct patient and family care, but also the
essential links, who collaborate with physicians, interact with allied health personnel, supervise
assistive personnel, and coordinate patient care among disparate health care professions for the
provision of patient care (Miller & Apker, 2002). Thus, in the middle of a rapidly changing and
complex healthcare system and environment maintaining, an adequate nursing staff is becoming
an increasingly important global issue (Bina et al., 2014; Ugur, Scherb, & Specht, 2015).
Maintaining an adequate nursing staff does not simply mean having a sufficient number of
nurses. It means maintaining an adequate number of qualified nurses who are empowered with
professional authority, autonomy, responsibility, and accountability for improving patient care
and the professional practice environment (Institute of Medicine, 2004). This implies that the
healthcare organization has to be decentralized with shared governance to support staff nurses so
they can demonstrate their fullest potential in providing safe, high-quality patient care (Institute
of Medicine, 2004; Scherb, Specht, Loes, & Reed, 2011). The standards for Magnet designation
also consider the importance of shared governance in healthcare organizations with an emphasis
on staff nurses' decisional involvement (Kowalik & Yoder, 2010). Based on the notion of shared
governance, staff nurses’ decisional involvement is a key component, which has contributed to
improving the nursing work environment and increasing nurse recruitment and retention
Decisional involvement was defined by Havens and Vasey (2003) as “the pattern of
distribution of authority for decisions and activities that govern nursing practice policy and the
practice environment” (p. 332). However, the concept of decisional involvement has frequently
been confused with decision making only in clinical situations for patient care and sometimes
commingled with the concepts of autonomy and control over nursing practice (CONP) in the
nursing literature (Weston, 2008). Moreover, the definition of the combined term “decisional
involvement” is not included in the dictionary, which could lead to difficulties in understanding
and utilizing the concept, especially for those in non-English-speaking countries. The application
to other countries with different languages and cultures could mislead nursing management
research, perhaps promoting wrong interpretations and unexpected consequences for nursing
administration. Thus, defining the concept of nurse decisional involvement may be the first step
in applying it globally in nursing management to encourage staff nurse decisional involvement
for improving the nursing work environment and thus, patient care. Especially, as an Asian
country, South Korea experiences a high increase in staff nurse turnover, threatening nursing
care quality and patient safety (Korean Hospital Nurse Association, 2013).Thus, reviewing the
Korean literature may provide useful information to other Asian countries in a similar situation
and with similar organizational cultures by tracking what the status of nurse decisional
involvement is.
The purpose of this literature review is to define the concept of nurse decisional
involvement with relating factors—attributes, antecedents, and consequences—based on the
theoretical framework of decisional involvement, and to identify the knowledge gaps in nurse
decisional involvement in English-speaking, Western versus non-English-speaking, Asian
The detailed process of this review involves (1) sorting nursing literature on nurse
decisional involvement; (2) defining the concept of decisional involvement with its attributes,
antecedents, and consequences in terms of content and context of nursing practice; (3) exploring
the theoretical frameworks of nurse decisional involvement used most frequently in nursing
literature and identifying common factors; (4) developing a nurse decisional involvement
conceptual framework by synthesizing its attributes, antecedents, and consequences with the
common factors of the theoretical frameworks; and (5) identifying the knowledge gaps in nurse
decisional involvement status in English-speaking Western versus non-English-speaking Asian
countries based on the conceptual framework organized.
Methods
Data Sources, Search Strategy, and Inclusion/Exclusion Criteria
To conduct this integrative review, English and Korean language databases were selected to understand nurse decisional involvement status in English-speaking, Western versus
non-English-speaking, Asian countries.
The databases used were Cumulative Index to Nursing & Allied Health Literature
(CINAHL), PubMed, Web of Science, Korean Nursing Database, Research Information Sharing
Service (RISS), KoreaMed, National Digital Science Library (NDSL), and the Google Scholar
database. The search terms used were “nurse AND decisional involvement,” and “nurse AND
participation AND decentralization OR shared governance”.
The search strategy was to find nursing research published in English or Korean in
peer-reviewed journals. There were no limitations for the date of publication to find the research
articles because this is the first integrative literature review for nurse decisional involvement;
three-step search strategy was used. An initial limited search was undertaken to identify optimal
search terms, followed by an analysis of text words contained in the titles and abstracts and of
the index terms used to describe the article. A second extensive search was undertaken with all
identified keywords and index terms. The third step consisted of a search of the reference lists of
all identified articles for additional key literature.
The inclusion criteria for selecting articles were: (a) studies dealing with the concept of
nurse decisional involvement in governance; (b) studies dealing with similar concepts, such as
nurse participation in decentralized or shared governance.
Criteria for excluding studies included (a) studies that were not written in English or
Korean; (b) conference proceedings and abstracts only; (c) studies that did not match with the
concept of nurse decisional involvement in administrative decisions (i.e., control over context of
nursing practice), such as nurses’ decision making in clinical care or ethical dilemmas; (d) nurses’
decision-making style, process, and competency.
From the eight databases enumerated above, 76 English and 26 Korean articles were
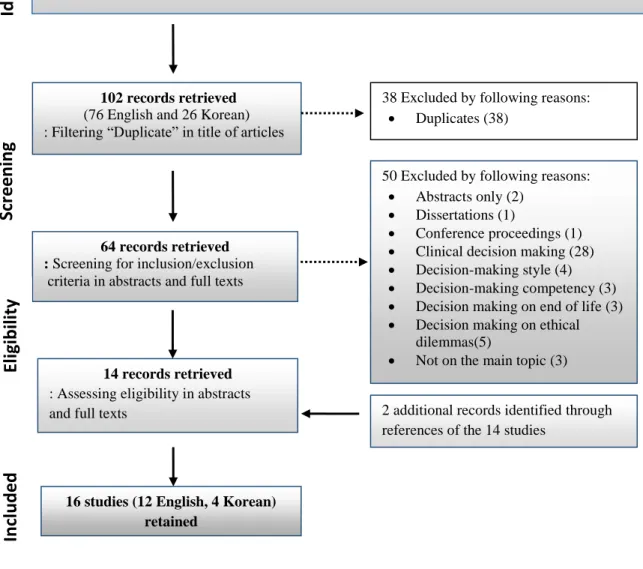
initially identified. The total yield from the search was 12 English and 4 Korean articles. A
summary of the search-and-retrieval process, the exclusion criteria, and the number of articles
included is presented in the Appendix as a PRISMA flow diagram (Figure. 2.1).
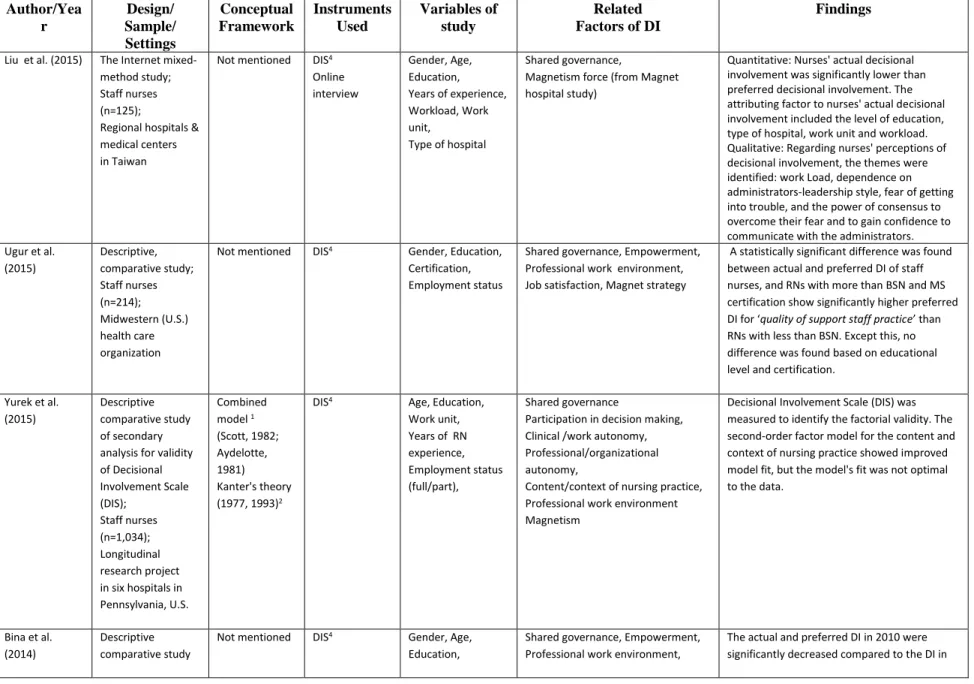
Data Extraction
The following data were extracted from the sixteen studies selected: Author (year),
design/sample/setting, theoretical or conceptual framework, instruments, independent and
Figure 2.1 Search and retrieval process of literature
Findings Descriptive Characteristics of Reviewed Studies
A total of 16 articles (twelve English and four Korean articles) were selected from the
original 102 articles identified. The sampling and settings from 11 of the articles were from the
Search Terms
“Nurse AND decisional involvement”
“nurse AND participation AND decentralization OR shared governance"
Data bases
CINAHL, PubMed, Web of Science, Google Scholar,Korean Nursing Database, Korean Research Information Sharing Service (RISS), Koreamed, Korean National Digital Science Library (NDSL)
2 additional records identified through references of the 14 studies
64 records retrieved : Screening for inclusion/exclusion criteria in abstracts and full texts
14 records retrieved : Assessing eligibility in abstracts and full texts
16 studies (12 English, 4 Korean) retained
50 Excluded by following reasons: Abstracts only (2)
Dissertations (1)
Conference proceedings (1) Clinical decision making (28) Decision-making style (4) Decision-making competency (3) Decision making on end of life (3) Decision making on ethical
dilemmas(5)
Not on the main topic (3) 38 Excluded by following reasons:
Duplicates (38)
102 records retrieved
(76 English and 26 Korean) : Filtering “Duplicate” in title of articles
U.S. (i.e., English-speaking, Western countries). The other five articles from
non-English-speaking Asian countries: the one English article is from Taiwan and the four Korean articles
from South Korea.
The 16 articles selected included seven non-experimental descriptive studies, three
psychometric assessment studies, one concept analysis, four secondary analyses, and one
mixed-method study (see Table 2.1).
The theoretical frameworks used most frequently were (a) the combined two models for
hospital work structure for professionals (Scott, 1982) and professional nursing departments
(Aydelotte, 1981); (b) structural theory of power in organizations (Kanter, 1977, 1993) (see
Table 1). Although ten studies did not identify a theoretical framework, for their studies, five
studies used the Decisional Involvement Scale (DIS) (Havens & Vasey, 2003, 2005) based on
the combined models of Scott (1982) and Aydelotte (1981).
The Decisional involvement scale (DIS) was most frequently used to measure nurse
decisional involvement status—actual and preferred levels— in 10 articles (Bina et al., 2014;
Havens & Vasey, 2003, 2005; Houston et al., 2012;Liu, Hsu, & Chen, 2015; Mangold et al.,
2006; Scherb et al., 2011; Ugur et al., 2015; Yurek, Havens, Hays, & Hughes, 2015)(see Table
2.1).
Each document was read in its entirety and then examined line-by-line to identify the
factors related to decisional involvement. The factors are: shared governance (or decentralization
or participative management), formal/informal power, empowerment structure, clinical /work
autonomy, professional/organizational autonomy, content/context of nursing practice, control
over nursing practice, accountability, responsibility, distribution of authority, collaboration,
fulfillment, work engagement, work effectiveness, organizational commitment, nurse retention
and recruitment, patient outcome, and organizational outcome, which are briefly summarized in
Table 2.1.
Defining the Concept of Decisional Involvement
The concept of decisional involvement is derived from the combined terms decision and
involvement. The definition of decision is “judgement that you make after thinking and talking
about what is the best thing to do” or “the process of deciding something” (Decision, n.d.) and
involvement “involves something, that thing is an important or necessary part or result of it”
(Involvement, n. d.) or “take part in it or are affected by it” (Involvement, n. d.). Thus, decisional
involvement can be defined as “taking part in the process of deciding something important or
necessary, that decision affects the result.”
Researchers have not only differentiated between the involvement in clinical and
administrative decisions, but they have also conceptualized involvement into a two-dimensional
construct that relates to the content and context of nursing practice (Houston et al., 2012;
Kowalik & Yoder, 2010; Laschinger, Sabiston, & Kutszcher, 1997; Yurek et al., 2015).Clinical
decision making has frequently been called decision-making in the nursing literature, which is
linked to involvement in decisions about nursing care activities (i.e., the content of nursing
practice) for patient care. On the other hand, administrative decisions have been called
decisional involvement, which is connected with involvement in decisions about organizational
process and operating systems (i.e., context of nursing practice) to deliver care that ultimately
Based on this content-context framework, we can present conceptual clarity between the
two domains of decisions and permit implementation of management interventions to improve
nursing practice and the nursing work environment.
Theoretical Frameworks for Staff Nurse Decisional Involvement
In the literature, the most frequently used theoretical framework for staff nurse decisional
involvement was based on a combination of the professions model (Scott, 1982) and the
professional nursing department model (Aydelotte, 1981). These both served as the framework
for the development of the Decisional Involvement Scale (Havens & Vasey, 2003, 2005).This
theoretical framework provides an understanding of the organization of professional work and
professional nurse control over the contents and contexts of nursing practice (see Figure 2.2).
Scott (1982) suggested three models for structuring the work of professionals who work in
healthcare organizations: (a) the autonomous model, in which professionals have solitary
authority because administrators delegate the control of most of the professional activities to the
professionals; (b) the heteronomous model, in which administrators have solitary authority to
control over most professional activities with elaborate sets of rules, regulations, and routine
supervision. Thus, professionals are clearly subordinate to the administration with minimal
autonomy; and (c) the conjoint model, in which professionals and administrators share authority
and have equal power by serving as the dominant force in certain areas. For example,
professionals maintain responsibility and authority for patient care, and administrators provide
the resources to shape the optimal work environment for professionals to be able to meet patient
care goals. In this arrangement, professionals and administrators can coexist in a state of
collaboration, interdependence, and mutual influence, which promotes recognizing the autonomy
nursing department model by identifying three domains for policy development and
administration in nursing: (a) the professional nursing practice domain, in which professional
nurses have sole authority and responsibility for patient care; (b) the nursing administrative
domain, in which nursing administrators have sole authority and responsibility for policies and
actions for resource acquisition, allocations, and interdepartmental and institutional relations; and
(c) the joint professional nursing practice and nursing administrative domain, in which both
share authority and responsibility for developing nursing policy and administration, such as
identification of resources needed, scheduling, cost saving, support service for nursing practice,
and improving the nursing work environment.
Figure 2.2 The theoretical framework of the combination of Scott’s structure model of hospital work for professionals and Aydelotte’s professional nursing departments model 1
1Note.The joint professional nursing practice and nursing administrative domain need staff nurse decisional
Another theoretical framework related to decisional involvement is Kanter’s (1977, 1993)
theory of structural power in the organization. Kanter’s theory (1977, 1993) is based on
relationships between perceptions of work empowerment and two facets of work decision
involvement, that is, control over the content and the context of nursing practice (Laschinger et
al., 1997) (see Figure 2.3).
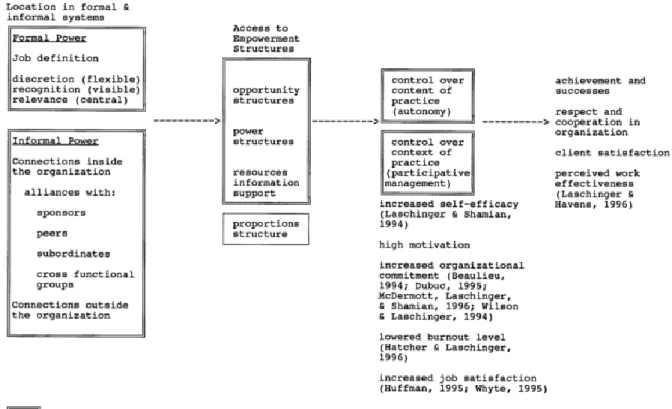
Figure 2.3 The theoretical framework of Kanter’s structural theory of power in organizations.2
According to Kanter (1977, 1993), behaviors and attitudes are shaped primarily in
response to an individual’s position and the situations that arise in an organization. Employee
2Note. A general representation of relationships among concepts in Kanter’s (1977, 1993) structural theory of
empowerment evolves from both the formal and informal systems of the organization (Kanter,
1977, 1993): formal power results from jobs that allow discretion, provide recognition, and are
relevant to key organizational goals, and informal power is derived from relationships and
alliances with people (e.g., sponsors, peers, subordinates, and cross-functional groups) in the
organization. People with formal and informal power are in a position to access job-related
empowerment structures (Kanter, 1977, 1993): (a) the structure of opportunity (e.g., promotion
and career development), (b) the structure of power (e. g., source of power for access to
information, support, and resources), and (c) the structure of proportions (e.g., the social
composition of people in approximately the same situation and position, such as males and
females). These three structures are important attributes contributing to the overall empowerment
of the staff nurse (Laschinger et al., 1997; Mangold et al., 2006; Scherb et al., 2011; Ugur et al.,
2015). Nurses who have access to opportunity, information, support, and resources are
empowered, and they have control over the content and context of professional nursing practice,
which makes their actions possible to improve their autonomy related to patient care and also
encourages nurses to be involved in participative management (i.e., shared governance) related
to work conditions and work environment (Laschinger et al., 1997; Mangold et al., 2006). In
addition, these empowered nurses, in turn, motivate and empower others by sharing the sources
of power, resulting in improved organizational effectiveness (Kanter, 1977, 1993; Laschinger et
al., 1997).
In summary, Scott (1982) and Aydelotte’s (1981) combined model, the joint professional
nursing practice and nursing administrative domain (i.e., the conjoint structure) includes the
aspects of the context of nursing practice, and the professional nursing practice domain points to
organizations also follows predictive patterns similar to Scott and Aydelotte’s combined models
framework. Kanter’s (1977, 1993) theory shows that organizational empowerment structures
under shared governance increased nurses’ empowerment, leading toincreased nurses’ control
over both the content and context of their practice. This Kanter’s (1977, 1993) theory suggests
that increased nurse autonomy in patient care and increased decisional involvement in
management have positive impacts on healthcare organizations by improving work effectiveness,
nurses’ job satisfaction, and patient satisfaction (Laschinger et al., 1997; Mangold et al., 2006).
Based on the common key concepts, such as shared governance, the content of nursing practice
(i.e., autonomy in patient care), and the context of nursing practice (i.e., decisional involvement
in the administrative realm), these two frameworks could be combined and synthesized as one
conceptual framework (see Figure 2.4).
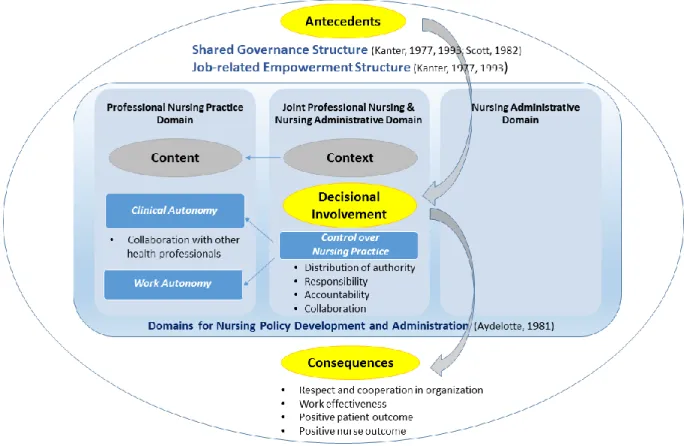
Figure 2.4 The synthesized conceptual framework for decisional involvement.3
3Note.The combination of the two models for hospital work structure for professionals (Scott, 1982) and
Defining Antecedents, Attributes, and Consequences of Decisional Involvement
The identified relating factors of decisional involvement were classified into antecedents,
attributes, and consequence based on the conceptual framework that was synthesized from Scott
and Aydelotte’s combined models and Kanter’s theory.
Antecedents. Antecedent, as cited in the Oxford Dictionary Online, is “a thing that existed
before or logically precedes another” (Antecedent, n. d.).The concept of decisional involvement
has antecedents such as following: (a) shared governance structure, (b) job-related empowerment
structure.
Although there are many definitions of “shared governance,” the core definition is a
decentralized management approach that gives staff nurses greater authority and control over
their practice and work environments (Kowalik & Yoder, 2010; O’May & Buchan, 1999; Scherb
et al., 2011; Ugur, et al., 2015). Shared governance originated from the education, business, and
management literature, such as the philosophy of Walton’s Deming Management Method (1986)
and Kanter’s (1977, 1993) structural theory (Laschinger & Havens, 1996; O’May & Buchan,
1999). Shared governance is often oversimplified and misunderstood as just “giving power to
employees.” However, shared governance requires all nurses and management to understand the
principles, process, and behaviors of shared governance (O’May & Buchan, 1999;
Porter-O’Grady, 2012). According to Kanter (1982), the “building and nurturing shared governance of a
collaborative team that is more fully consulted, more fully informed than the ordinary and one
that shares responsibility for planning and reaching outcomes” (p. 6). Thus, to implement,
disseminate, and enculturate shared governance, the organizational structure has to shift away
from a hierarchical, centrally controlled management style to a decentralized management style