A CASE CONTROL STUDY TO IDENTIFY THE RISK GROUP
OF PRECANCEROUS ORAL LESIONS AND TO CORRELATE
WITH PRE-DISPOSING FACTORS AND TO IMPLEMENT A
NEED BASED AWARENESS PROGRAMME ON ORAL
CANCER AMONG ADULTS RESIDING IN SELECTED
RURAL SETTINGS AT MADURAI DISTRICT
A Thesis
Submitted to The Tamil Nadu Dr.M.G.R Medical University,
Chennai
for the award of the Degree of
Doctor of Philosophy in Nursing
By
Y.JOHN SAM ARUN PRABU, M.Sc(N).,M.Sc(Psy).,M.Phil.,
Professor
C.S.I Jeyaraj Annapackiam College of Nursing, Madurai
Under the Guidance of
PROF.DR.B.T. BASAVANTHAPPA, M.Sc(N).,Ph.D(N).,
Research Guide
C.S.I Jeyaraj Annapackiam College of Nursing
Madurai
A CASE CONTROL STUDY TO IDENTIFY THE RISK GROUP
OF PRECANCEROUS ORAL LESIONS AND TO CORRELATE
WITH PRE-DISPOSING FACTORS AND TO IMPLEMENT A
NEED BASED AWARENESS PROGRAMME ON ORAL
CANCER AMONG ADULTS RESIDING IN SELECTED
RURAL SETTINGS AT MADURAI DISTRICT
Signature of the Guide: ______________________________
PROF.DR.B.T. BASAVANTHAPPA,M.Sc(N)., Ph.D(N)., RESEARCH GUIDE
C.S.I JEYARAJ ANNAPACKIAM COLLEGE OF NURSING
MADURAI
A Thesis
Submitted to The Tamil Nadu Dr.M.G.R Medical University,
Chennai
for the award of the Degree of
A CASE CONTROL STUDY TO IDENTIFY THE RISK GROUP
OF PRECANCEROUS ORAL LESIONS AND TO CORRELATE
WITH PRE-DISPOSING FACTORS AND TO IMPLEMENT A
NEED BASED AWARENESS PROGRAMME ON ORAL
CANCER AMONG ADULTS RESIDING IN SELECTED
RURAL SETTINGS AT MADURAI DISTRICT.
Signature of the Guide: ______________________________
PROF.DR.B.T.BASAVANTHAPPA, M.Sc(N) Ph.D(N)., RESEARCH GUIDE
C.S.I JEYARAJ ANNAPACKIAM COLLEGE OF NURSING
MADURAI
Signature of the Co-Guide: ______________________________
PROF.DR.C. JOTHI SOPHIA, M.Sc(N)Ph.D.N. RESEARCH CO-GUIDE
C.S.I JEYARAJ ANNAPACKIAM COLLEGE OF NURSING
MADURAI
A Thesis
Submitted to The Tamil Nadu Dr.M.G.R Medical University, Chennai for the award of the Degree of
CERTIFICATE BY GUIDE
This is to certify that the thesis entitled
“A case control study to
identify the risk group of precancerous oral lesions and to correlate
with pre-disposing factors and to implement a need based awareness
programme on oral cancer among adults residing in selected rural
settings at Madurai District”
, submitted by
Y.JOHN SAM ARUN
PRABU,
who registered for Ph.D in 2009 is a bonafide record of the
research done by her during the period of study under my supervision and
guidance and that it is not formed on any basis for the award of any other
Degree, or Diploma, Associate ship, Fellowship or any other similar title
or any other Universities.
I also certify that this thesis is her original independent work. I
recommend this thesis should be placed before the examiners for the
award of Ph.D degree.
---
PROF.DR.B.T. BASAVANTHAPPA,
M.Sc(N).,
Ph.D(N).,
RESEARCH GUIDE
C.S.I JEYARAJ ANNAPACKIAM COLLEGE OF NURSING
CERTIFICATE BY CO-GUIDE
This is to certify that the work embodied in the thesis entitled
“A
case control study to identify the risk group of precancerous oral
lesions and to correlate with pre-disposing factors and to implement
a need based awareness programme on oral cancer among adults
residing in selected rural settings at Madurai District”
, submitted by
Y.JOHN SAM ARUN PRABU,
for the award of the Degree of Doctor
of Philosophy in Nursing is a bonafide record of research done by her
during the period of study under my supervision and guidance that it has
not formed the basis for the award of any Degree, Diploma. Associate
ship, Fellowship or any other similar title in this university or any other
university or institution of higher learning.
I also certify that this thesis is her original independent work. I
recommend this thesis should be placed before the examiners for the
award of Ph.D degree.
---
PROF.DR.C. JOTHI SOPHIA, M.Sc(N).,Ph.D.,
RESEARCH CO-GUIDE
C.S.I JEYARAJ ANNAPACKIAM COLLEGE OF NURSING
DECLARATION BY THE CANDIDATE
I hereby declare that this thesis entitled
“A case control study to
identify the risk group of precancerous oral lesions and to correlate
with pre-disposing factors and to implement a need based awareness
programme on oral cancer among adults residing in selected rural
settings at Madurai District”
, is an original work done by me under
the guidance of
Prof. Dr.B,T.Basavanthappa, M.Sc(N).,Ph.D.,
and has
not been submitted elsewhere, either partially or fully for the award of
any other Degree, or Diploma Diploma. Associateship, Fellowship or any
other similar title.
---
Y.JOHN SAM ARUN PRABU, M.Sc(N).,M.Sc(Psy).,M.Phil.,
PROFESSOR
ACNOWLEDGMENT
First and foremost, I praise and thank God Almighty for his abundant grace and blessings showered upon me throughout my study to complete it successfully
I wish to express my sincere appreciation and deep gratitude to all those who helped me in accomplishing this task successfully.
I am fortunate to express my sincere thanks and heartfelt gratitude to my guide Dr. B.T. Basavanthappa,M.N.,Ph.D(N)., Professor and Principal, Rajarajeswari College of
Nursing, Bangalore, for his suggestions, encouragement and valuable guidance , professional competence throughout my study.
My heartfelt thanks and respect to my co-guide Prof. Dr .C .Jothi Sophia, Ph.D(N)., Principal, C.S.I. Jeyaraj Annapackiam College of Nursing, Madurai, for her direction and valuable guidance offered to complete this studyand for her keen interest, scholarly guidance, valuable timely help and suggestions throughout my study.
I express my heartfelt gratitude to my clinical guide Dr.N.Gururaj, MDS., Professor in oral pathology, C.S.I. College of Dental Sciences and Research, Madurai for his expertise , inspiration, immense interest, support and suggestions in helping me to accomplish this task.
I owe my special thanks to Dr.Sivakumar, MBBS., B.M.O, Block PHC, for permitting me to conduct the study under Thiruparankundram Block .
It is my pleasure and privilege to express my deep sense of gratitude to Prof. Mrs.Merlin Jeyapal, vice principal, C.S.I. Jeyaraj Annapackiam College of Nursing, Madurai for her constant support, suggestions and encouragement.
It is my pleasure and privilege to express my gratitude to Prof.Dr.Rajalakshmi, Research Guide , C.S.I. Jeyaraj Annapackiam College of Nursing, Madurai for her valuable, suggestions and constant support in helping me to accomplish this task.
I thank from the bottom of my heart to all my colleagues and community health department faculty, C.S.I. Jeyaraj Annapackiam College of Nursing for providing all help in getting this work completed on time.
I am immensely thankful to Miss.C.Udayakumari, M.A., M.Ed., M.Phil., Headmistress, O.C.P.M Girls Higher Secondary school ,Madurai, for her exhaustive contribution towards English editing work .
I am indeed to express my gratitude to Mrs. Emelda, M.A., B.Ed., Retired Tamil Teacher, C.S.I Girls higher Secondary School, Pasumalai , Madurai, for Tamil editing work.
I render my gratitude to Mr.John, for his printing work throughout my study.
I extremely grateful to Mary Anne Charity Trust Chennai, for their valuable materials for this study.
Without the continues prayers and support of my family , this study would never have been the outcome it is today, I am beholden deeply to my parents Rev.A.Yovan, Mrs.S.SelvamaniYovan and my Aunt Mrs.W.RubellavathyManoharan for their love, prayers and encouragement which were of most importance to me.
I am deeply indebted to my better half Mrs.Praveena Kiruba Bai and my Children Master. Praiselin and Miss. Praisee who has been my shoulder and unceasing support and who has always believed and brought out the best in me.
Most importantly, this Journey would not have been the same without all my Brothers, Brother-in-laws, sister and sister-in-law especially, Mr.Raja, Mr.John, Mr.Gideon, Mr.Robin, Mr.Selvin, Mrs.Christy, Mrs.Shalini, Mrs.Sofia. I am grateful for their overwhelming kind co-operation, unconditional love and support during this study.
Above all its my pleasure and privilege to express my heartfelt gratitude to my beloved kutties Master. Kingsly, Miss Angel, Master Franklin and Master Benjamin. My special prayers for their bright future.
I thank my entire dear and near ones who has prayed for me to complete my study.
I once again extend my heartfelt gratitude to all who directly and indirectly helped me to accomplish my Journey Successfully.
With a thankful heart
ABSTRACT
BackgroundCancer is a universal and non communicable disease that affects people without
regard to race, gender, socio economics status or culture1. Cancer is the second most
common killer disease in the world.2. Oral health is a state of being free from mouth and
facial pain, oral and throat cancer, oral infection and sores, periodontal (gum) disease,
tooth decay, tooth loss, other diseases and disorders that limit individual’s capacity in
biting, chewing, smiling, speaking, and psychosocial wellbeing. The most common oral
diseases are oral cancer, dental cavities, periodontal (gum) disease, oral infectious
diseases, trauma from injuries, and hereditary lesions4. Researchers in oral cancer believe
that early diagnosis of oral carcinoma greatly increases the probability of cure and survival
rates in addition to minimizing impairment and deformity52.
Statement of the problem
A case control study to identify the risk group of precancerous oral lesions and to
correlate with pre-disposing factors and to implement a need based awareness programme
on oral cancer among adults residing in selected rural settings at Madurai district
Objectives of the study
1. To identify the prevalence of precancerous lesions among adults residing at
selected rural settings at Madurai.
2. To describe the predisposing factors of pre cancerous oral lesions among tobacco
using adults in cases and controls groups.
3. To find correlation between precancerous oral lesions and pre disposing factors
among adults in cases and controls.
4. To implement a need based awareness programme on oral cancer among adults
Methods
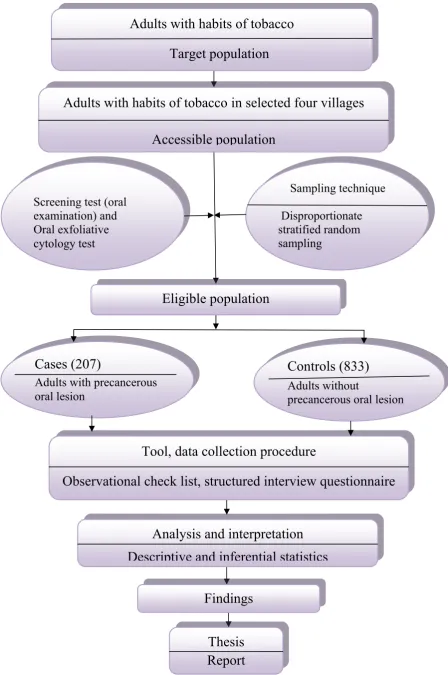
The research design adopted for this study is Quasi- Experimental Case Control
Design. The study was conducted in the rural settings of Madurai District in south Tamil
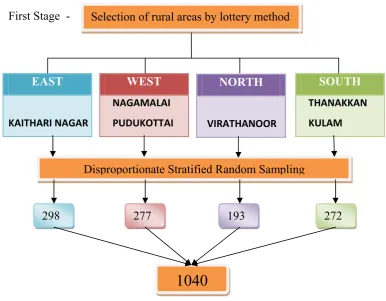
Nadu. The sample size was made using Power Analysis and was 1040. According to
Cytological results 207 samples were identified with precancerous oral lesions. They were
considered as Cases. Remaining 833 samples were considered as controls.
Disproportionate stratified random sampling method was used to select samples.
Observational check list was used to identify the risk group of precancerous oral lesions
through oral examination. Questionnaire was used to identify the pre-disposing factors on
oral cancer among adults. knowledge was assessed by using a questionnaire and the
attitude was measured on a 3 point Likert scale and modified Fagerstrom Addiction Scale
were used to find the level of dependence among adults with precancerous oral lesions
(cases). The data were analyzed based on the objectives of the study using descriptive and
inferential statistics.
Results
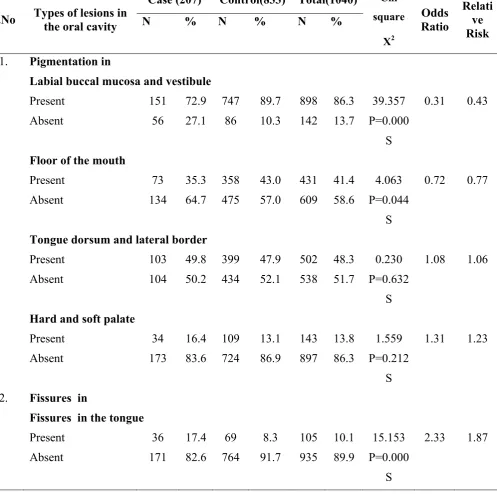
Totally 207 (100%) of cases had leukoplakia which is one of the ideal precancerous
lesions. Majority 72.9% of Cases and 89.7% of Controls were having
Pigmentation in the labial buccal mucosa and vestibule.
High majority of the cases (90.3%) using biddies smoking and controls (78.9%)
using cigarette smoking. Almost all of the cases (97.1%) and controls (96.6%) used
below 5 packets of smokeless tobacco per day and the onset of smokeless tobacco
were at the age of 25 and above in both the cases and controls.
Level of knowledge on oral cancer before the structure teaching programme was
generally inadequate 134 (100%), the level of attitude was moderately favorable
39(29.1%) and low favorable 95 (70.9%). After structured teaching programme the
adequate level 90 (67.2%) and the level of attitude has highly increased to high
favorable 134 (100%).
Level of dependence in smoking before the structure teaching programme among
adults were moderately high 69(51.5%) and high 30(22.4%) and in smokeless
tobaccowere low 92 (68.7) and moderately high 14(10.4%) and high
28(20.9%).After structured teaching programme the level of dependence has
deliberately decreased to low level 134 (100%)
Interpretation and conclusion
The main conclusion of the present study is that many adults with the habit of
smoking, smokeless tobacco, alcoholism and other substance abuse were unknowingly
affected with pre cancerous oral lesions. If it is detected earlier prevention from oral
cancer is possible. Identification and rectification of pre disposing factors will reduce the
risk of oral cancer.
The structured teaching programme could effectively increase the knowledge and
Attitude of adults with pre cancerous oral lesions (cases) regarding oral cancer which help
the adults to reduce the level of dependence in smoking and smokeless tobacco and also
acceptance of treatment and thus reduce the prevalence of oral cancer.
Key words: precancerous oral lesions, Oral Health, smoking, smokeless tobacco,
leukoplakia, pigmentations, Pre-disposing factors, knowledge, attitude, dependence and
TABLE OF CONTENTS
CHAPTER TITLE PAGE
CHAPTER I INTRODUCTION
1.1 Background of the study
1.2 Significance and need for the study 1.3 Statement of the problem
1.4 Aim and objectives 1.5 Hypotheses
1.6 Operational definition 1.7 Limitations
1.8 Projected outcomes
1 4 8 8 9 9 11 11
CHAPTER II REVIEW OF LITERATURE
2.1 Studies on predisposing factors on Oral Cancer 2.2 Studies on knowledge regarding oral cancer 2.3 Studies on case control design.
2.4 Studies on Oral exfoliative cytology 2.5 Studies on structured teaching programme 2.6 Conceptual frame work
12 14 17 20 23 26
CHAPTER III METHODOLOGY
3.1 Research approach 3.2 Research design 3.3 Setting
3.4 Population
3.5 Sample and sample size 3.6 Sampling technique 3.7 Selection of cases
3.8 Diagnostic criteria
3.9 Criteria for sample selection 3.10 Selection of controls 3.11 Measurement of exposure 3.12 Instrument
3.13 Scoring
3.14 Reliability and validity 3.15 Pilot study
3.16 Method for data collection 3.17 Data collection process 3.18 Schedule for data collection 3.19 Plan for data analysis 3.20 Protection of human rights
34 35 35 35 36 38 39 40 40 42 42 43
CHAPTER IV STUDY FINDINGS 44
CHAPTER V DISCUSSION 125
CHAPTER VI SUMMARY AND RECOMMENDATIONS
6.1 Summary of the study
6.2 Summary of the study findings 6.3 Conclusions
LIST OF TABLES
TABLE TITLE PAGE
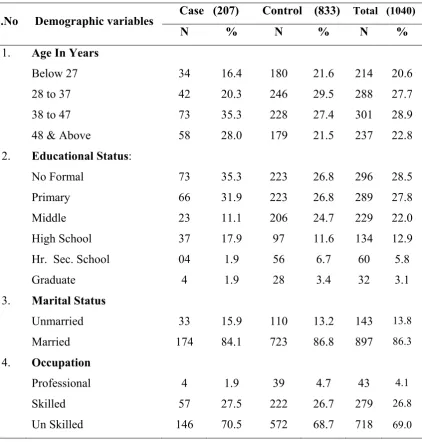
1.1 Distribution of frequency and percentage of cases and controls regarding their demographic variables such as age, educational status,
marital status and occupation. 46
1.2 Distribution of frequency and percentage of cases and controls regarding their demographic variables such as personal monthly income, type of family, religion ,food habit and source of information.
50
1.3 Distribution of frequency and percentage of cases and controls regarding their demographic variables such as source of information to stop using tobacco, family history of first degree relatives and physical health problems.
55
2.1 Distribution of prevalence of risk group of pre cancerous oral lesions
among cases and controls. (Present only illustrated). 59 2.2 Distribution of prevalence of risk group of pre cancerous oral lesions
in oral cavity among cases and controls. (present only illustrated). 60 2.3 Distribution of mean, standard deviation and statistical value on
examination of buccal cavity among cases and controls. 63 2.4 Distribution of prevalence of oral disorders in teeth among cases and
controls. (present only illustrated). 64
2.5 Distribution of mean, standard deviation and statistical value on
examination of teeth among cases and controls. 66
2.6 Distribution of mean, standard deviation and statistical value on total
screening score among cases and controls. 67
3.1 Distribution of habit of smoking regarding pre-disposing factors among
cases and controls. 68
3.2 Distribution of mean, standard deviation and statistical value on habit
3.3 Distribution of habit of smokeless tobacco regarding pre-disposing
factors among cases and controls. 72
3.4 Distribution of mean, standard deviation and statistical value on habit
of smokeless tobacco among cases and controls. 74
3.5 Distribution of expenses regarding pre-disposing factors among cases
and controls. 75
3.6 Distribution of mean, standard deviation and statistical value on
expenses among cases and controls. 76
3.7 Distribution of reason for quitting tobacco regarding pre-disposing
factors among cases and controls. 77
3.8 Distribution of mean, standard deviation and statistical value on reason
for quitting tobacco among cases and controls. 79
3.9 Distribution of reason for relapse regarding pre-disposing factors
among cases and controls. 80
3.10 Distribution of mean, standard deviation and statistical value on reason
for relapse among cases and controls. 82
3.11 Distribution of habit of alcohol and other substances regarding
Pre-disposing factors among cases and controls. 83
3.12 Distribution of mean, standard deviation and statistical value on habit
of alcohol and other substances among cases and controls. 85 3.13 Distribution of practice of oral hygiene regarding
Pre-disposing factors among cases and controls. 86
3.14 Distribution of mean, standard deviation and statistical value on
practice of oral hygiene among cases and controls. 87 3.15 Distribution of mean, standard deviation and statistical value on total
pre-disposing factors among cases and controls. 88
4.1 Relationship between risk group of precancerous oral lesion and
pre-disposing factors among cases only. 89
5.1 Frequency and percentage distribution of cases regarding their demographic variables such as age, educational status, marital status and occupation
5.2 Frequency and percentage distribution of cases regarding their demographic variables such as personal monthly income, type of family, religion, food habit and source of information.
92
5.3 Frequency and percentage distribution of cases regarding their demographic variables such as source of information to stop using tobacco, family history of first degree relatives and physical health problems.
94
6.1 Distribution of existing knowledge of adults with pre cancerous oral
lesions regarding oral cancer. 95
6.2 Distribution of paired‘t’ test value between pre test and post test
knowledge scores. 97
7.1 Distribution of level of attitude regarding oral cancer among adults
with pre cancerous oral lesions. 98
7.2 Distribution of paired‘t’ test value between pre test and post test
attitude scores. 99
8.1 Distribution of level of dependence regarding habit of smoking among
adults with pre cancerous oral lesions. 100
8.2 Distribution of paired ‘t’ test value between pre test and post test
scores on level of dependence in smoking. 101
8.3 Distribution of level of dependence regarding habit of smokeless
tobacco among adults with pre cancerous oral lesions. 102 8.4 Distribution of paired ‘t’ test value between pre test and post test
scores on level of dependence in smokeless tobacco. 10 9.1 Relationship between knowledge attitude and level of dependence
(smoke and smokeless tobacco users) of adults with pre cancerous oral lesions.
104
10.1 Distribution of association between the post test level of knowledge and selected demographic variables such as age in years, educational status, marital status and occupation.
10.2 Distribution of association between the level of knowledge and selected demographic variables such as personal monthly income, type of family and religion.
106
10.3 Distribution of association between the level of knowledge and
selected demographic variables such as source of information. 107 10.4 Distribution of association between the level of knowledge and
selected demographic variables such as source of information to stop using tobacco and family history of first degree relatives.
108
11.1 Distribution of association between the level of attitude and selected demographic variables such as age in years, educational status, marital status and occupation.
110
11.2 Distribution of association between the level of attitude and selected demographic variables such as personal monthly income, type of family and religion.
111
11.3 Distribution of association between the level of attitude and selected
demographic variables such as source of information. 112 11.4 Distribution of association between the level of attitude and selected
demographic variables such as source of information to stop using tobacco and family history of first degree relatives.
113
12.1 Distribution of association between the level of dependence among habit of smoking and selected demographic variables of adults with precancerous oral lesion.
115
12.2 Distribution of association between the level of dependence among habit of smokers and selected demographic variables such as personal monthly income, type of family and religion.
116
12.3 Distribution of association between the level of dependence among habit of smokers and selected demographic variables such as source of information.
12.4 Distribution of association between the level of dependence among habit of smokers and selected demographic variables such as source of information to stop using tobacco and family history of first degree relatives.
118
12.5 Distribution of association between the level of dependence among habit of smokeless tobacco and selected demographic variables such as age in years, educational status, marital status and occupation.
120
12.6 Distribution of association between the level of dependence among habit of smokeless tobacco and selected demographic variables such as personal monthly income, type of family and religion.
121
12.7 Distribution of association between the level of dependence among habit of smokeless tobacco and selected demographic variables such as source information.
122
12.8 Distribution of association between the level of dependence among habit of smokeless tobacco and selected demographic variables such as source of information to stop using tobacco and family history of first degree relatives.
LIST OF FIGURES
FIGURE TITLE PAGE
1. Modified conceptual frame work based on web of causation – mac mohan
& thomas pugh (1970). 28
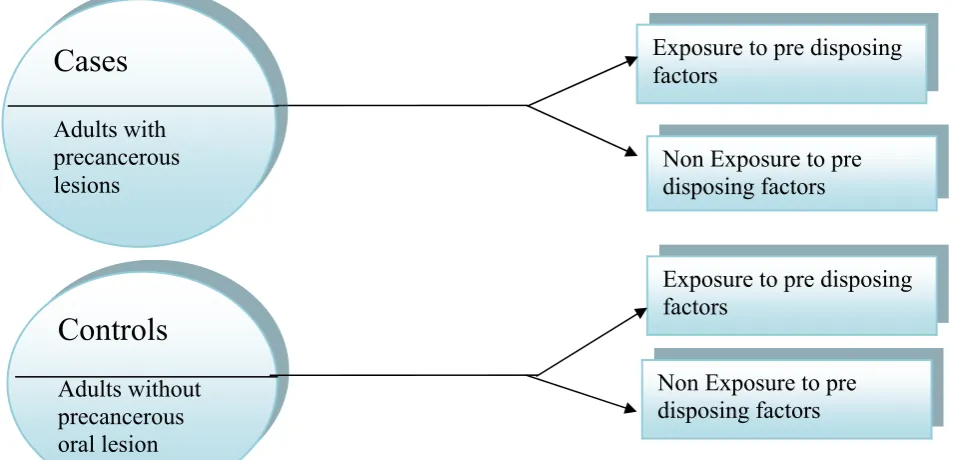
2. Concept of case control design. 29
3. Schematic representation of case control research design. 30
4. Selection of samples 32
5. Data collection process 40
6. Frequency and percentage of cases and controls according to age. 48 7. Frequency and percentage of cases and controls according to educational
status. 48
8. Frequency and percentage of cases and controls according to marital
status. 49
9. Frequency and percentage of cases and controls according to occupation. 49 10. Frequency and percentage of cases and controls according to personal
monthly income. 52
`11. Frequency and percentage of cases and controls according to type of
family. 52
12 Frequency and percentage of cases and controls according to religion . 53 13 Frequency and percentage of cases and controls according to food habit. 53 14 Distribution of frequency and percentage of cases and controls
according to source of information. 54
15 Frequency and percentage of cases and controls according to source of
information to stop using tobacco. 57
16 Frequency and percentage of cases and controls according to family
17 Frequency and percentage of cases and controls according to physical
health problems. 58
18 Distribution of existing knowledge on oral cancer among adults with pre
cancerous oral lesions. 96
19 Distribution of level of attitude on oral cancer among adults with pre
cancerous oral lesions. 98
20 1distribution of level of dependence regarding habit of smoking among
adults with pre cancerous oral lesions. 100
21 Distribution of level of dependence regarding habit of smokeless tobacco
LIST OF APPENDICES
APPENDIX TITLE
A Letter requesting permission for conducting the main study
B Letter requesting permission for conducting the main study
C Result of the cytological study
D Madurai district map
E Institutional ethical committee clearance certificate
F Letter seeking expert opinion for the content validity of tool
G Criteria checklist for validation of the tool
H Certificate of tool validation
I List of experts who validated the tool
J Informed consent English
K Informed consent Tamil
L Tool used for data collection
M Structured teaching programme
N Research milestone
O Exfoliative cytology procedure
P Mass health education
Q Distributed booklet on prevention of oral cancer in saloons of study area
R Booklet on prevention of oral cancer
S Pamphlet on prevention of oral cancer
LIST OF ABBREVIATIONS
1. < Less than
2. > More than
3. χ2 Chi-square
4. % Percentage
5. df Degree of freedom
6. OR Odds ratio
7. RR Relative risk
8. SD Standard deviation
9. PHC Primary health centre
10. STP Structured teaching programme
11. S Significant
12. NS Non significant
13. WHO World health organization
14. SCC Squamous cell carcinoma
15. ICMR Indian Council of Medical Research
16. NCD Non Communicable Disease
17. NFHS National Family Health Services
18. DDHS Deputy Directorate of Health Services
19. ACS American Cancer Society
1
CHAPTER – I
INTRODUCTION
“YOU ARE THE TEMPLE OF GOD……FOR THE TEMPLE OF GOD IS HOLY”“HEALTHY ADULTS FOR A WEALTHY NATION”
1.1 Background of the study
Cancer is a universal and non communicable disease that affects people
irrespective of race, gender, socio economics status or culture1. It can occur at any site or
tissue of the body and involves any type of cells. There are wide variations in the
distribution of cancer through out the world. Cancer is the second most common killer
disease in the world.2It is a major disease with high incidence and mortality rate and
increasingly recognized to be a global problem, not limited to the industrialized nations.
India entered in to “population explosion” era in 1920 and after 1940 mortality rate started
declining3.
Oral health is essential to general health and quality of life. It is a state of being
free from mouth and facial pain, oral and throat cancer, oral infection and sores,
periodontal (gum) disease, tooth decay, tooth loss, other diseases and disorders that limit
individual’s capacity in biting, chewing, smiling, speaking, and psychosocial wellbeing.
The most common oral diseases are oral cancer, dental cavities, periodontal (gum) disease,
oral infectious diseases, trauma from injuries, and hereditary lesions4.
Cancer of the oral cavity occurs when malignant tumors are found in the tissue of
the lip or mouth. More than 90% of cancers of oral cavity occur in the squamous cells that
line the mucosal surfaces in the mouth and throat. In the oral cavity, these include Lips,
2
mouth, upper and lower gums (gingiva), bony roof of the mouth (hard palate), area behind
the wisdom teeth (retro molar tongue) 5
The WHO’s oral health program has outlined the need for careful oral screening as
an important public health measure for all clients of all ages in order to reduce common
oral health problems, including dental caries, and ensure early identification of serious oral
health conditions, such as oral cancer and HIV disease6.
Oral cancer is the third most common cancer in developing nations and the fifth
most common cancer in world 7, according to the National Institutes of Health, The
American Cancer Society (ACS) estimates that 22,040 cases of oral cancers diagnosed in
the united states in 2006. According to WHO, 2004 incidence of oral cancer in USA was
31,2002 per expected population of 293,655,405, In India 113,163 per expected
population of 1,065,070,6078.
According to World Cancer Report (2004), cancer rates are expected to raise by
50% leading to 50 million new cancer patients by 2020. WHO states that death due to
cancer is expected to increase 14% with largest increase (70%) to occur among people
living in developing countries by 20209.
Cancer of the oral cavity, which may occur in any part of the mouth or throat, is
curable if discovered early10 .Oral cancer may occur on the lips or anywhere within the
mouth, like tongue, floor of the mouth, buccal mucosa, hard and soft palate, Pharyngeal
walls and tonsils11.
Although the oral cavity lesions constitute only a small minority of pathological
conditions, they are of great significance, as they have a potential to jeopardize health and
3
constituting 40% of all cancer cases registered in India, 90% of which are squamous cell
carcinomas. It occupies a very important place on the global cancer score board. It is a
common cancer in South-East Asia, where more than 100,000 new cases are reported
every year 13. Whereas it accounts for about 2% to 3% of total malignant tumors in the
United Kingdom and the United States of America14. This marked difference is because of
environmental factors and life styles of the people. Several workers from India reported
that the high incidence is due to the wide spread habit of tobacco chewing 15,16& 17 along
with smoking18&19, alcoholism20, poor oral hygiene and ill-fitting dentures21. Of these,
tobacco habit holds a strong suspicion as carcinogenic agent.
The most common type of oral cancer is squamous cell carcinoma, 60% of oral
cancer are well advanced by the time they are detected. It is still increasing as a leading
killer across the globe, especially in the developing countries. In 2000, there were an
estimated 10 million new cancer cases and 6 million cancer deaths throughout the
world,even through physicians and dentist frequently examine the oral cavity22.
Oral cancer begins as leukoplakia a white patch (lesion), red patches,
(Erythroplakia) or non healing sores that have existed for more than 14 days. In the United
States, Oral cancer accounts for about 8% of all malignant growths. Men are affected
twice as often as women, particularly men older than 40/60. In Indian subcontinent oral
sub mucosa fibrosis is very common23. This condition is characterized by limited opening
of mouth and burning sensation on eating of spicy food. This is a progressive lesion in
which the opening of the mouth becomes progressively limited and later on even normal
eating becomes difficult. It occurs almost exclusively in India and Indian communities
4
Smoking is one of the most important risk factors for developing oral cancers 25&26.
Oral cancer is currently a major global health issue27. In developing countries, oral cavity
cancer is estimated to be the third most common malignancy after cancer of the cervix and
stomach28. Oral cancer is emerging as an important public health problem and it is
responsible for killing approximately one person every hour. It is the sixth most common
cancer in men and the fourteenth most common cancer in women in sex-wise occurrence
in India29.
No significant advancement in the treatment of oral cancer has been found in
recent years. Although better combinations of multidiscipline approach have improved the
quality of life in oral cancer patients, the over all survival rate has not improved much
over the past decades30. Therefore, primary prevention such as cessation of tobacco
smoking and alcohols drinking along with early detection is necessary to control
procedures and to improve the prognosis of oral cancer 31.
1.2 SIGNIFICANCE AND NEED FOR THE STUDY
Tobacco use is a global problem. The long history of disease, the epidemic of
tobacco attributable morbidity and mortality is a relatively recent phenomenon. Recent
trends indicate an earlier age of initiation to tobacco use and raising smoking prevalence
rates among growing children and healthy adolescence. If this pattern continues tobacco
use will result in the deaths of 250 million of the people who are children and adolescence
today, many of them in the developing countries. Indian council of medical research
(ICMR) says that nearly 1, 60,000 people developed cancer in India, each year as a result
5
Nearly two-third of world’s smokers live in just ten countries and more than 40%
live in just two countries i.e. China and India. India bears around 10% share of total
smokers in the world33. According to NFHS –III, in India, 55.8% male, 10.8% female in
the age group of 12 to 60 years have been found to be consuming tobacco. Among males,
32.7% smokers and 36.5% tobacco chewers are reported, while among females, It is
reported to be 1.4 and 8.4%, respectively34.The Government’s most recent National
sample survey indicates that there are 1,194 Million consumers in India with tobacco use,
differing greatly from the rest of the world. Some 96 million people use smokeless tobacco
and while 20% consumed cigarettes, nearly 40% smoke beedi which deliver more nicotine
than cigarettes. The remaining 40% chew tobacco and tobacco containing products such as
snuff, betal quid, zarda, pan masala, mava/khaa/gutkha, gudakhu, kimam. According to
WHO by 2020 tobacco will be solely responsible for 13.3% of death in India35.
During the process of growing ,drying and curing smokeless tobacco, it acquires
28 different carcinogens (National Cancer Institute 2003).The amount of nicotine received
through smokeless tobacco is 3 to 4 times higher than the nicotine received through a
cigarette, and it remains in the system longer. Adolescents who believe that the smokeless
tobacco is “safer” to use than cigarette is sadly mistaken. Smokeless tobacco use increases
the risk of mouth, lip, cheek, and tongue cancer. National Cancer Institute (2003) has been
associated with the presence of “smokeless tobacco lesions” on the oral mucosa which are
similar to those observed in patients with oral cancer with pre-existing oral lesions36.
As per WHO (2003) one of the greatest concern among adolescence today is
“tobacco addiction”. Nearly 20 million children are using tobacco. Global rate of
conception of tobacco will increase from 3 million to 10 million in the year 2010.
6
tobacco related diseases, about 1,60,000 to 2,00,000 people develop cancer every year due
to tobacco use37.
Health professionals including nurses and other health workers have an important
role in prevention and control of oral cancer. Nurses in the community can play a vital role
in creating awareness in people through education due to the frequent interaction with the
individuals. They can also effectively screen oral cancer and the precancerous lesions in
high risk population aiding in appropriate prevention in the early stages. Globally, about,
5, 75,000 new cases and 3, 20,000 deaths occur every year from oral cancer38.
It is essential to establish an accurate diagnosis to initiate optimal therapy for oral
cavity lesions. An adequate incision biopsy taken from an area representative of the lesion
can provide over 98% diagnostic accuracy as to whether the lesion is malignant or not,
when routine pathological techniques are used39.
A programme on Non Communicable Disease is conducted in Primary Health
Center to prevent and control common NCDs through behaviour and life style changes.
They have introduced the Colposcopy investigation in the district level hospital to identify
the cervical cancer among females. Now it is extended to community level 40. But there
was no Provision to identify the pre cancerous oral lesions which leads to oral cancer. The
oral exfoliative cytology is quick, simple, less technically demanding, painless, non-
invasive yet quite dependent laboratory procedure for the microscopic investigations and
diagnosis of different kinds of oral diseases, especially suspected malignant and
pre-malignant lesions. As a diagnostic cytology it has got an immense value in the field of
7
Despite the fact that oral cancer can be cured if treated early enough45, the 5 years
survival (about 35%)46 has not really improved with advances in surgery, radiotherapy,
and chemotherapy47. The main reason is probably the late presentation of these
tumours48&49. In turn this may be due to: (i) the asymptomatic nature of the early lesion47;
(ii) lack of self examination by patients50,51; (iii) misdiagnosis by clinician48-50 and (iv) the
patients fear49,50. These obstacles have to be overcome if the prognosis is to improve45.
Researchers in oral cancer believe that early diagnosis of oral carcinoma greatly
increases the probability of cure and survival rates in addition to minimizing impairment
and deformity.52,53 Despite recent advances in the diagnosis and treatment of cancer,
visual accessibility to oral mucosa and easy early detection,the prognosis of oral cancer
has yet to change. The proportion of oral cancer cases diagnosed at an early and localized
stage is still less than approximately 50%.54,55Since at least two-thirds of all cases are due
to life style factors, such as tobacco and alcohol abuse, these behaviours are changeable by
the use of effective primary prevention programmes.56,57 One of the main causes seems to
be the lack of awareness about oral cancer,both among the general population and some
health care professionals. The number of countries that have implemented oral cancer
control programmein minimal is comparison to those for other cancers such as
breast,cervical, and prostate.52,5358,59
The investigator working in the community found that many people are addicted to
the usage of tobacco products and many precancerous lesions are unnoticed which lead to
oral cancer and many studies suggested visual accountability to oral mucosa and easy
early detection. Hence the present study was undertaken with a view to study to estimate
8
and to create a need based awareness programme on hazards of deleterious habits as well
as control the occurrence of oral cancer.
1.3 STATEMENT OF THE PROBLEM
A case control study to identify the risk group of precancerous oral lesions and to
correlate with pre-disposing factors and to implement a need based awareness programme
on oral cancer among adults residing in selected rural settings at Madurai district.
1.4 AIM AND OBJECTIVES
Aim
To determine the precancerous lesion among adults with the habits of smoking ,
chewing tobacco and alcoholism
To find out cytological changes in the oral cavity through Oral exfoliative cytology
investigation.
To refer the identified cases of precancerous lesion to C.S.I Dental college hospital
for further treatment.
To create awareness among adults with the habits of smoking , chewing tobacco
and alcoholism relating to oral cancer
Objectives of the study
1. To identify the prevalence of precancerous lesions among adults residing at
selected rural settings at Madurai.
2. To describe the predisposing factors of pre cancerous oral lesions among tobacco
using adults in cases and controls groups.
3. To find correlation between precancerous oral lesions and pre disposing factors
9
4. To implement a need based awareness programme on oral cancer among adults
residing in selected rural settings at Madurai district.
1.5 HYPOTHESES
H1: There is a significant association between pre disposing factors and pre
cancerous oral lesions among cases and controls.
H2 : There is a significant difference between pre- test and post- test knowledge
scores on oral cancer among cases.
H3 : There is a significant difference between pre- test and post- test attitude
scores on oral cancer among cases.
H4 : There is a significant difference between pre- test and post- test level of
dependence scores among cases.
H5 : There is a significant association between knowledge , attitude and level of
dependence scores and their selected demographic variables.
1.6 OPERATIONAL DEFINITION
Identify :
It refers to detect the precancerous oral lesions by doing oral examination
and oral Exfoliative cytology test.
Precancerous oral lesions:
Leukoplakia -A wide range of white oral lesions which cannot be
rubbed off .
sub mucous fibrosis - Deposition of fibrous tissue in the sub mucosal
layer of the pharynx, palate, cheek and lips.
Erythroplasia - A flat red patch or lesion in the mouth that cannot be
10
These lesions can be identified through observational check list on oral
examination and cytology test.
Pre-disposing factors:
It refers to the causative factors for adults to develop oral cancer such as
habits of tobacco (smoking and smokeless tobacco) and usage of alcohol
and other substances, expenses towards tobacco habits, quit and relapse and
their oral hygiene practices as elicited by questionnaire.
A need based health awareness programme on oral cancer:
It refers to group and mass health education programme with appropriate
audio-visual aids designed for adults to provide information regarding
definition, causes, diagnosis, signs and symptoms, treatment and
prevention of oral cancer.
Adults:
It refers to male adults with the age group of 18 to 60 years with the habits
of tobacco in all forms and alcohol usage.
Correlation:
It refers to the relationship between the adults with precancerous oral
lesions and their pre-disposing factors.
Oral cancer:
It refers to the appearance as a growth or sore in the mouth that does not go
away which includes cancers on the lips, tongue, cheeks, floor of the
mouth, hard and soft palate, sinuses and pharynx(throat), which can be life
11 1.7 LIMITATIONS
This study is limited to male adults with the age group of 18 to 60 years.
[Early adults – 18 to 40 years; late adults – 40 to 60 years]
1.8 PROJECTED OUTCOME
1. The findings of the study would help the community health nurses to identify the
precancerous oral lesions and to create awareness on oral cancer and referral
services.
2. The findings will help to identify the Pre-disposing factors that are caused to
develop oral cancer.
3. The findings of the study will create awareness among people with precancerous
lesions for early identification and treatment and to protect them from oral cancer.
4. Knowledge of oral cancer will enhance the healthy lifestyle (behavioral
modification) of adults.
5. Early detection and prompt treatment of precancerous oral lesions will lead to
12
CHAPTER II
REVIEW OF LITERATURE
Review of literature is a key step in any research process. Review of literature
refers to an extensive, exhaustive and systematic examination of publications relevant to
the research. It generally helps to put a research problem in proper perspective or to
identify gaps and weakness in prior studies so as to justify a new investigation.
The review of literature for the present study is arranged under the following sections:
1. Studies on predisposing factors on Oral Cancer
2. Studies on knowledge regarding oral cancer
3. Studies on case control design.
4. Studies on Oral Exfoliative cytology
5. Studies on structured teaching programme
2.1 STUDIES ON PRE DISPOSING FACTORS ON ORAL CANCER
The study was carried out in surrounding 11 villages of the Kasturba Rural
Health Training Centre, Anji during January 2008. 385 adolescents were selected by
simple random sampling and interviewed through house to house visits. After survey, six
focus group discussions were undertaken with adolescent boys. About 68.3% boys and
12.4% girls had consumed any of the tobacco products in last 30 days. Out of the boys
who had consumed tobacco, 79.2% consumed kharra, and 46.4% consumed gutka. Among
boys, 51.2% consumed it due to peer pressure, 35.2% consumed tobacco as they felt
better, and 5% consumed tobacco to ease abdominal complaints and dental problem.
Among girls, 72% used dry snuff for teeth cleaning, 32% and 20% consumed tobacco in
the form of gutka, tobacco& lime respectively. The reasons for non use of tobacco among
13
was the fear of cancer (58.6%), poor oral health (44.8%) and fear of getting addiction
(29.3%). According to FGD respondents, few adolescent boys taste tobacco by 8-10 years
of age, while girls do it by 12-13 years.61
Among the 119 patients with oral cancer, information on chewing habits and
smoking was obtained in 92 patients (77.3%). There were 70 tobacco chewers (76.1%), 55
quid chewers (59.8%), and 22 smokers (23.9%). Simultaneous chewing of tobacco and
quid was found in 48 cases (52.2%). The present survey has disclosed for the first time
that oral SCC is the most frequent cancer in this study area in Yemen, and that the high
relative frequency of oral SCC may be related to the habits of chewing tobacco61
Fifty eight percent of the global head and neck cancers occur in South and
Southeast Asia, where chewing of betel, areca and tobacco are common. This study was
carried out to establish the pattern of use of Paan, Chaalia, Gutka, Niswar, Tumbaku and
Naas among population of squatter settlement of Karachi and to determine the perceptions
and knowledge regarding their role in the etiology of head and neck cancers. Through
systematic sampling, 425 subjects [a male and female from a household] were interviewed
with a structured questionnaire. The prevalence of the disease was 2.46 times higher
among males than females and 1.39 times higher among adolescents than adults. At least
79% of the participants were classified as having poor knowledge about the
carcinogenicity of each of these items. Knowledge increased with age and level of
education. Health hazards of these items were poorly recognized and about 20% perceived
at least one of these items to be beneficial.62
A 5-year retrospective study (1994-97 and 1999) on the prevalence of oral
cancer was conducted using patients' records at the Dental Department in the Solomon
14
relationship between smoking and betel nut chewing in patients with oral cancer. There
were 48 cases of oral cancer reported at the hospital over the 5-year period. Males aged 45
years and above were mostly affected with the distribution showing 31.5% of the cases
from Malaita, 20.8% from Temotu and 14.6% from the Western Provinces. Ninety percent
(90%) of the oral cancer patients practice both smoking and betel nut chewing, compared
to those who only practice one habit and this was highly significant (p<0.001). This study
has shown that the combinations of tobacco smoking and chewing of betel quid are the
main risk factors for oral cancer. Therefore, these factors are to be emphasized in the
public and preventive education to be given to communities in the Solomon Islands63.
The study conducted on adverse effects of tobacco use on the health of an
individual is well known. It is essential to identify factors leading to tobacco use to plan
strategies to limit its use. Education is known to influence the prevalence of tobacco use.
We aimed to determine the prevalence and patterns of tobacco use in a rural community
with a high literacy rate and to examine the socioeconomic and demographic variables
that correlate tobacco consumption in the area. Our findings in this rural community
suggest that improvement in the educational and socioeconomic status may lead to a
decline in the use of tobacco. Health education to improve dental hygiene may also help to
reduce tobacco use in this community as it is predominantly used in the chewing form 64.
2.2 STUDIES RELATED TO KNOWLEDGE REGARDING ORAL CANCER
The study was conducted to assess awareness of oral cancer, knowledge of its
major risk factors and clinical signs, and oral cancer examination experiences among
Florida adults aged 40 years and older. A sample size was selected and computer assisted
telephone survey was conducted in 2002. Data from 1773 respondents were weighted to
15
knowledge of oral cancer. The result shows that in Florida, 15.5% of adults aged 40 years
and older had never heard of oral cancer and another 40.3% reportedly knew little or
nothing about it. About one-half of adults did not think that oral white or red patches or
bleeding could indicate oral cancer and 27.6% correctly identified three of oral cancers
major risk factors. The study was concluded that there is widespread lack of awareness
and knowledge in Florida regarding oral cancer and low levels of reported examination,
particularly among groups experiencing disproportionately high incidence and later stage
diagnosis.65
The study was conducted to determine public awareness and knowledge of oral
cancer in Great Britain. The sample size is 1894 members of the public over the age of 16
years .They were asked in face-to-face interviews their knowledge relating to cancer, with
particular reference to oral cancer, its causes and those with high risk and general attitudes
to cancer. The results shows that the oral cancer was one of the least heard of cancers by
the public with only 56% of the participants being aware, whereas 96% had heard of skin
cancer, 97% lung cancer and 86% cervical cancer. There was a 76% awareness of the link
between smoking and oral cancer but only 19% were aware of its association with alcohol
misuse. The study was concluded that this survey highlights a general lack of awareness
among the public about mouth cancer and a lack of knowledge about its causation
especially the excess risk associated with alcohol 66.
The study was conducted to determine the attitudes and practice of Florida nurse
practitioners on oral cancer prevention. A sample size of 448 Florida nurse practitioners
were selected .A statewide mail-based survey was conducted to assess the independent
relationship between nurse practitioners attitudes and their practices in oral cancer
16
practice behaviors were significantly affected by their attitudes. The study proved that the
effective strategies should be implemented to enhance positive attitudes about oral cancer
early detection among Florida nurse practitioners 67.
The study was focused on teaching cancer prevention and detection which is
important in health professional education. It is desirable to select a comprehensive
framework for teaching oral cancer prevention and detection skills. A sample size of 104
persons are selected and the precede-proceed model was used to design a randomized
pretest and posttest study of the oral cancer prevention and detection skills of dental
students. Oral cancer knowledge, opinions, and competencies were evaluated. The result
shows that the second year students in the intervention group were more competent than
those in the control group. The study was concluded that the novel use of precede-proceed
sets a precedent for designing a standardized oral cancer curriculum for a wide range of
health professional disciplines 68.
A study was conducted to determine knowledge of risk factors for oral cancer and
signs and symptoms of oral cancer among 916 Maryland 18 years old adult and older.
Overall, level of knowledge about risk factors and signs and symptoms of oral cancer was
low; misinformation was high. Although 85% of them reported that they heard about oral
cancer, only 28% of the respondents reported that they had undergone oral cancer
examination. These results demonstrate a need for interventions designed to increase
knowledge levels at risk factors, sign, and symptoms of oral cancer and the need for oral
cancer examination69.
An investigation was undertaken to assess the knowledge, attitudes and beliefs of
South Asian adults (n= 367) regarding the risk factors and signs of oral cancer. Tobacco
17
difference (p<0.001) was seen in betel- squid chewing habit among the age groups with
42.2% of adults in the 50-80 year age group practising this habit as compared to only 5.3%
in the 16- 29 year age group70.
A study was conducted to assesses knowledge of oral cancer risk factors, clinical
signs, and oral cancer examination experience among North Carolina adults. A state wide
random digit dial, computer assisted telephone interview was conducted in 2002. Data
from 1,096 respondents, where analysed and it proved that risk factor knowledge was
high for 56% and associated in a logistic regression model with younger age, feeling
personal factors cause cancer, and non use of snuff. One sign of oral cancer (sore/ lesion,
red or white patch in mouth, and bleeding in the mouth) was correctly identified by 53%
with significantly more correct responses from younger people, nonsmokers, and some
college education. Although there is moderate knowledge of signs and risk factors for oral
cancer among North Carolina adults, knowledge deficits remain71.
2.3 STUDIES ON CASE CONTROL DESIGN
The role of tobacco chewing, smoking and alcohol drinking patterns on the risk
of cancer of the oral cavity was evaluated using a nested case-control design on data from
a randomized control trial conducted between 1996 and 2004 in Trivandrum, India. Data
from 282 incident oral cancer cases and 1410 matched controls were analyzed using
multivariate conditional logistic regression models. Tobacco chewing was the strongest
risk factor associated with oral cancer. Effects of chewing pan with or without tobacco on
oral cancer risk were evaluated for both sexes. Beedi smoking increased the risk of oral
cancer in men (OR=1.9, 95%CI=1.1-3.2). Given the relatively poor survival rates of oral
cancer patients, cessation of tobacco and moderation of alcohol use remain the key
18
A multi centric case-control study conducted in India included 513
hypopharyngeal cancer cases, 511 laryngeal cancer cases and 718 controls. we
investigated smoking and chewing tobacco products as risk factors for these cancers.
Among never-smokers, tobacco chewing was a risk factor for hypopharyngeal cancer, but
not for laryngeal cancer. In particular, the risk of hypopharyngeal cancer increased with
the use of Khaini (OR 2.02, CI 0.81-5.05), Mawa (OR 3.17, CI 1.06-9.53), Pan (OR 3.34,
CI 1.68-6.61), Zarda (OR 3.58, CI 1.20-10.68) and Gutkha (OR 4.59, CI 1.21-17.49). A
strong dose-response relationship was observed between chewing frequency and the risk
of hypopharyngeal cancer (p(trend) < 0.001). An effect of alcohol on cancer of the
hypopharynx and supraglottis was observed only among daily drinkers (OR 2.22, CI
1.11-4.45 and OR 3.76, CI 1.25-11.30, respectively). In summary, this study shows that
chewing tobacco products commercially available in India are risk factors73
A case-control study was conducted in Rajah Muthiah Dental College and
Hospital, Annamalainagar, Annamalai University, Chidambaram, Tamil Nadu, India
during the period 1991-2003. The study included 388 oral squamous cell carcinoma cases
and an equal number (388) of age and sex-matched controls. The combination of chewing
and smoking together with alcohol drinking showed very high relative risk (OR 11.34). A
positive association was observed between non-vegetarian diet, poor oral hygiene and
poor dentition with the risk of oral squamous cell carcinoma74.
Forty oral cancer patients identified consecutively in Changhua Christian Hospital
between 1990 and 1992 were compared with 160 population-based controls, matched for
sex, age, area of residence, and educational background. Betel quid chewing was
positively associated with the risk of oral cancer with adjusted odds ratio of 58.4 (95% CI:
19
oral cancer; the adjusted odds rations were 12.9, 93.7 and 397.5 for < 21, 21-40, and > 40
years of betel chewing as compared with the non-users. The risk also increased with the
quantity chewed per day; the odds ratios for those chewing < 10, 10-20 and > 20 quid /day
were 26.4, 51.2 and 275.6, respectively. These odds ratio estimates were all statistically
significantly different from the null value of unity75.
A case control study conducted in Chennai and Trivendrum in South India to
assess the effect of different pattern of smoking, chewing and alcohol drinking in the
development of the 3 neoplasms i.e., oral, pharyngeal and esophageal cancer. They
observed a significant dose response relationship for duration, amount of consumption of
the 3 habits with the development of the 3 neoplasms. Tobacco chewing emerged as the
strongest risk factor for oral cancer with highest odds ratio of 5.05 the strongest risk factor
for pharyngeal and Oesophageal cancer, tobacco smoking with add ratio of 4.00 and 2.83
respectively76.
The incidence of oral cancer amongst young adults is increasing in many European
and high incidence countries. The aim of this study was to evaluate the major risk factors
for oral cancer in young adults using a case-control design. A sample of 116 patients aged
45 years and younger, diagnosed with squamous cell carcinoma of the oral cavity between
1990 and 1997 from the south east of England were included. Two-hundred and seven
controls who had never had cancer, matched for age, sex and area of residence, were
recruited. The self-completed questionnaire contained items about exposure to the
following risk factors: tobacco products, cannabis, alcohol and diet. Conditional logistic
analyses were conducted adjusting for social class, ethnicity, tobacco and alcohol habits.
All tests for statistical significance were two-sided. The majority of oral cancer patients
20
age. The estimated risks associated with tobacco or alcohol were low (OR range: 0.6–2.5)
among both males and females. Only smoking for 21 years or more produced significantly
elevated odds ratios (OR=2.1; 95% CI: 1.1–4.0).77
A Case control study was conducted onTobacco Smoking and Oral Cancer
,Several epidemiological studies suggest that tobacco smoking increases the risk of oral
cancer. They undertook a meta-analysis of epidemiological studies investigating the
magnitude relationship between tobacco smoking and oral cancer. Primary studies were
identified through a computerized literature search of Medline. Articles abstracted were all
epidemiological studies published as original articles in English during 1990-2007
provided the summary estimates of odds ratios (OR) of tobacco smoking for oral cancer
compared to that of non-smokers. A total of 15 case-control studies were used for this
meta-analysis. Summary of OR was calculated based on random effects model.The
combined odds ratio for tobacco smoking related to oral cancer was 4.65 (95%CI,
3.19-6.77). Also, the highest combined odds ratio belonged to American continents (OR= 7.65;
95%CI,5.11-11.45) and the lowest was in Asia (OR= 1.88; 95%CI, 0.95-3.71).the results
clearly indicate that tobacco smokers are at increased risk of oral cancer. The cancer risk
can be reduced by controlling of tobacco smoking in different countries.78
2.4 STUDIES ON ORAL EXFOLIATIVE CYTOLOGY
A study was conducted on the use of Oral exfoliative cytology in the Early
Diagnosis of Oral Pemphigus Vulgaris by Dr. VivekK et,al., Oral exfoliative cytology is
an important diagnostic device. It is quick, simple, less painful and bloodless procedure.
Considerable interest has been developed in the use of oral exfoliative cytology for
diagnosis of oral lesions; especially oral carcinomas. It is also proved to be useful in the
early diagnosis of disease like Pemphigus Vulgaris, Herpes Simplex, Herpes Zoaster and
21
Cytological smears were obtained from fourteen patients of oral pemphigus vulgaris. All
the smears of the selected group were taken from surface of the oral cavity for 3-4 times
with a wooden spatula. Smears were then fixed in cytofix. After fixation the smears were
stained with hematoxylin and eosin stain and papanicoloue stain.79
A study was focused on AgNOR count in oral exfoliative cytology of normal
buccal mucosa. The purpose of this study was to compare the AgNOR count of cells
collected from normal buccal mucosa by oral exfoliative cytology in smokers and
non-smokers. Of 40 smokers and non-smokers were selected for the study, 22 patients were
males and 18 females. These patients were attending the dental school of the federal
university of minas gerais for routine dental treatment. The patients ages ranged from
41-77 (mean 57) in the non smoking group and from 40-76 (mean 53) in the smoking group.
The smokers used a minimum of 20 cigarettes per day for at least 15 years. Patients in
neither group had medical problems, and both groups were matched for age and sex. The
smears were taken from the clinically normal buccal mucosa.80
The study was conducted on Oral exfoliative cytology of normal oral mucosa .
Smears were taken from four oral sites (buccal mucosa, hard palate, ventral tongue) using
the cytobrush (medscandcolgue medical ltd Berkshire, England) in 28 patients attending
the Dundee dental hospital. In all cases mucosa appeared clinically normal. 14 males and
14 females consented to the smear procedure and formed part of a control group for a
study proved by the medical ethics committed.81
The study was conducted to cytomorphometric analysis of exfoliated normal
buccal mucosa cells. Oral exfoliative cytology is the study of superficial cells which has
been exfoliated from mucous membranes, renal tubes, and so on: and it also includes the
22
may also be found in body fluids; for example, sputum, peritoneal fluid, etc. These cells
are stained by papanicolaou stain. It is painless, which causes little discomfort to the
patient. For these reasons, the procedure can be repeated a number of times for diagnosis,
follow up and research purposes. Smears from the buccal mucosa were taken from 160
subjects attending the outpatient department, Meenakshi Ammal dental college, Chennai,
who did not give history of any systemic illness, tobacco use or alcohol habits 82.
The study was conducted by oral exfoliative cytology and electron microscopy in
the diagnosis of hairy leukoplakia. Thirty patients with oral lesions suggestive of HC were
controlled in the study. They included 28 men and women with a mean age of 39.7 years.
The patients were seen at the oral medicine clinic of the B. C. cancer agency, Paul’s
hospital, and the Vancouver hospital and health cancer centre, Canada review of medical
records showed that 20 patients were HIV seropositive and 10 had developed AIDS 83.
A study was focused to oral oral exfoliative cytology in the diagnosis of
paracoccidioidomycosis, Ten patients with a clinical suspicion of paracocidioidomycosis
were included in the study. All patients were males with ages ranging from 29.0 to 54.0
years. The patients presented with symptoms and signs of paracocidioidomycosis
underwent a clinical examination and pulmonary radiography. All patients exhibited oral
lesions clinically compatible with paracocodioidomycosis presenting as chronic, painful
mulberry like ulcerations. Frequently more than one oral site was affected. Six patients
had generalized oral lesions, three had lesions in the gingival and oropharynx and one
patient had only involvement of the buccal mucosa. Pulmonary lesions were observed in
23
The study was focused on radiotherapy using a source to skin distance of 100cm.
Most patients received parallel opposing fields and required wedges. Smears were
obtained from normal buccal mucosa which was in the field of exposure for the irradiation
of malignant tumours. These smears were taken before 1.2 wks into and at one month
following completion of radiotherapy on oral cancer mucosa. A wooden assessed by
quantitative oral exfoliative cytology. A wooden tongue spatula was scraped firmly across
the mucosa and the scrapings transferred to glass slides. The smears for DNA estimation
were fixed in methanol formalin acetic acid 85: 10: 5 and then underwent feulgen
hydrolysis. The smears for cytomorphological assessment ( measurement of nuclear area
and cytoplasmic area) were fixed in equal parts 95% ethanol and diet hylet her and then
stained with the papanicolaou stain 85.
2.5 STUDIES ON STRUCTURED TEACHING PROGRAMME IN GENERAL
The quasi experimental study was carried out to assess the effectiveness of
Structured Teaching Programme (STP) regarding tobacco consumption among the
subjects attending Rural Health Centre (RHC) at south Pitchavaram in the year 2006- 2007
by making comparison between pre-test and post-test among the subjects. A teaching
module for health education on Tobacco consumption and the structured tool for data
collection was prepared. Sixty subjects who fulfilled the criteria were selected as samples
and pre-test was conducted. After that STP was given with appropriate audiovisual aids.
After one month of STP, post-test was conducted and data were analyzed. There was
significant increase in the level of knowledge, attitude, but there was a significant
reduction in the practice of the subjects between pre-test and post-test. There was a
significant increase in the level of knowledge and attitude. There was a positive
relationship between knowledge and attitude level of the subjects and the demographic
24
their behaviour.Out of 28 tobacco chewers 15 (53.6%) had highest level of readiness to
quit their behaviour of chewing tobacco. The study finding indicates that there is a need
for STP to improve the knowledge, attitude and to decrease the practice level of the
subjects.86
The study was conducted regarding the effectiveness of structured teaching
programme on cancer cervix ,regarding the knowledge and attitude among married women
residing in selected urban and rural areas of Karnataka. Research design used in this study
was quasi experimental design with one group pretest and posttest. the multistage
sampling technique was used .The findings of the study reveal that most of married
women 84% in urban area and 76% in rural areas had moderate knowledge. The posttest
score for all the married women was 100% in urban and 92% in rural area .The study
showed that there was significant improvement between pretest and posttest, so it is
concluded that the structure teac