KNOWLEDGE AND POST-TRAUMATIC STRESS DISORDER
REGARDING CHILD ABUSE AMONG SCHOOL CHILDREN
- A MIXED METHOD APPROACH.
THESIS
Submitted to
THE TAMIL NADU Dr. M.G.R. MEDICAL UNIVERSITY, CHENNAI
for the award of the degree of
DOCTOR OF PHILOSOPHY
IN
NURSING
By
Mrs. RUTH RANI PRINCELY.J , M.Sc. (NURSING)
KNOWLEDGE AND POST-TRAUMATIC STRESS DISORDER
REGARDING CHILD ABUSE AMONG SCHOOL CHILDREN
- A MIXED METHOD APPROACH.
THESIS
Submitted to
THE TAMIL NADU Dr.M.G.R. MEDICAL UNIVERSITY, CHENNAI
for the award of the degree of
DOCTOR OF PHILOSOPHY
IN
NURSING
By
Mrs. RUTH RANI PRINCELY.J, M.Sc. (NURSING)
Guided by
Dr. S. KANCHANA, M.Sc. (N), Ph.D (N), POST DOC.(RESEARCH), PRINCIPAL & Ph.D (N) RESEARCH GUIDE,
OMAYAL ACHI COLLEGE OF NURSING, PUZHAL, CHENNAI-600 066.
KNOWLEDGE AND POST-TRAUMATIC STRESS DISORDER
REGARDING CHILD ABUSE AMONG SCHOOL CHILDREN
- A MIXED METHOD APPROACH.
THESIS
Submitted to
THE TAMIL NADU Dr.M.G.R. MEDICAL UNIVERSITY, CHENNAI
for the award of the degree of
DOCTOR OF PHILOSOPHY
IN
NURSING
By
Mrs. RUTH RANI PRINCELY .J, M.Sc. (NURSING)
Under the guidance of
Dr. S. KANCHANA, M.Sc. (N), PhD. (N), POST DOC.(RESEARCH), PRINCIPAL & Ph.D (N) RESEARCH GUIDE,
OMAYAL ACHI COLLEGE OF NURSING, PUZHAL, CHENNAI – 600 066.
I hereby declare that this thesis entitled “EFFECT OF STAY SAFE NURSING
CARE PACKAGE ON KNOWLEDGE AND POST-TRAUMATIC STRESS DISORDER REGARDING CHILD ABUSE AMONG SCHOOL CHILDREN– A MIXED METHOD APPROACH” is my own work carried out under the Guideship of
Dr. S. KANCHANA, M.Sc. (N), Ph.D (N), Post Doc. (Research), Principal & Ph.D(N) Research Guide, Omayal Achi College of Nursing and is approved by the Research Committee, The Tamil Nadu Dr. M.G.R. Medical University, Guindy, Chennai.
I further declare to the best of my knowledge that the thesis does not contain any part of work which has been submitted for the award of any degree either in this University or in any other University / Deemed University, without proper citation.
Mrs. RUTH RANI PRINCELY.J ,M.Sc. (N) RESEARCH SCHOLAR
This is to certify that this thesis entitled “EFFECT OF STAY SAFE NURSING CARE PACKAGE ON KNOWLEDGE AND POST-TRAUMATIC STRESS DISORDER REGARDING CHILD ABUSE AMONG SCHOOL CHILDREN– A MIXED METHOD APPROACH.” submitted by Mrs. RUTH RANI PRINCELY.J, M.Sc. (N) for the award of the Degree of Doctor of Philosophy in Nursing, is a bonafide record of research done by her during the period of study, under my supervision and guidance and that it has not formed the basis for the award of any other Degree, Diploma, Associateship, Fellowship or other similar title. I also certify that this thesis is her original independent work. I recommend that this thesis should be placed before the
examiners for their consideration for the award of Ph.D Degree in Nursing.
RESEARCH GUIDE
Dr. S. KANCHANA, M.Sc. (N), Ph. D (N), POST DOC.(RESEARCH), PRINCIPAL & Ph. D (N) RESEARCH GUIDE, OMAYAL ACHI COLLEGE OF NURSING, 45, AMBATTUR ROAD, PUZHAL, CHENNAI – 66 Place :
We cannot do great things on this Earth, only small things with great love Mother Teresa
This research work was executed with effort of a number of people whose contributions for this thesis deserves a special mention. It is a pleasure to convey my gratitude to all of them through this acknowledgement.
I completely surrender myself in the glorious hands of Almighty Lord, the owner of all things, for his immeasurable mercy, unconditional grace, wisdom and magnificent blessings throughout the journey of this thesis.
I desire to express my gratitude to the Vice Chancellor, Registrar,
Controller of Examination, Academic Officer, HODs and other officials of the Research Department of the Tamil Nadu Dr. M.G.R. Medical University, Guindy, Chennai for granting me an opportunity to undergo the Ph.D (Nursing) programme in this prestigious University.
I express my sincere and heartfelt gratitude to Mrs.ValliAlagappan, Managing Trustee and Chairperson ofthe Governing Council,
MBBS, FRSH(London), Research Coordinator, International Centre for Collaborative Research (ICCR) and Governing Council Member, Omayal Achi College of Nursing, for confirming the research statement during research proposal, funded me to complete a course on cognitive behavioural therapy and being a great inspiration to conduct this study.
I wish to thank and express my profound gratitude, indebtedness and appreciation to an exemplar Dr. S. Kanchana, M.Sc.(N), Ph.D (N), Post Doc. Research, Research Director, ICCRand Principal, Omayal Achi College of Nursing for being my Research Guide. She is the best director of this research work as she laid strong foundation in every phase of this study. She was always supportive, compassionate, brilliant and a scholarly person who guided and helped me in all time of this research and writing this thesis. I could not have imagined having a better advisor and mentor for my Ph.D study.
I am obliged to express my sincere thanks to my Doctoral Advisory Committee Members, Dr.Vasanthakumari, M.Sc (N), Ph.D (N), Child Health Nursing Dept, and Dr.Pamavathy Kamaraj, M.Sc (N),Ph.D(N), Vice Principal, Madras Medical Mission College of Nursing , Chennai, for their expertise and valuable suggestions in refining this research study.
support had always kept me going ahead.
I express my earnest gratitude to Mrs.Gifta Prabha Vedaselvi M.Sc.(N), In-Charge, Omayal Achi Community Health Centre, Arakambakkam, for her excellent motivation and guidance to conduct this study in selected schools.
I take this opportunity to thank the Chief Educational Officer, Thiruvallur District for granting me permission to conduct this study in Government higher secondary schools in Thiruvallur District.
My sincere gratitude to Dr.Vengatesan Satish, Ph.D, Biostatistician, who tirelessly and with great effort helped me to complete the statistical analysis and provided excellent guidance to complete both the phases of the study.
My sincere thanks to Mrs. M.N Pushpa Chandrasekar, Retired Education Officer, Government Museum, Chennai, for editing the tools and this thesis for English and Tamil language appropriateness, and back to back translations respectively.
complete a certified course in cognitive behavioural therapy and having guided me in planning the intervention for these special children.
I also express my heartfelt gratitude to my departmental faculties
Mrs.Sorna Daya Rani, Assistant Professor, Mrs.Rubin Selvarani, Nursing Tutor and Mrs.Betsy, Nursing Tutor who encouraged me throughout my study.
I also extend my sincere thanks to Mrs.Mythiliy, Assistant Professor for designing my IEC and my colleague Mrs.Amutha, Associate Professor, for stimulating discussions and Mrs. Bagavathy, Associate Professor for the help extended in the final compilation of the manuscript.
I would like to express my sincere thanks to Mrs. Chandralekha, Nurse Facilitator, Dr. Mohan Diabetic Research Foundation, Mrs.Uma Nursing Tutor who helped me to complete the study successfully. .
I am immensely grateful to the Administrative Staff, and the Librarians for all moral and technical support with preparation of the tool and the thesis.
shared their precious time during the process of interviewing and who actively participated in the interventions.
I express my gratefulness to Mr. G.K.Venkataraman, Elite Computers, for his technical expertise in shaping the manuscript into its final form.
I would like to express a deep sense of gratitude and love to my parents Late Mr. B.Jeyaraj and especially my mother Mrs. Suseela Rukmani.T who was my pillar and strength in all times and provided continuous encouragement throughout the study and this accomplishment would not have been possible without her support.
My heartfelt thanks to my in-laws Late Mr. Masillamani and Mrs. Pushabai for their constant encouragement throughout the study.
I feel grateful to share my thanks to my most lovable brother Mr. Balaselvin Job.J, Sister-in-law Mrs.Anitha. D, nieces B. Nithin, B. Alvin and my ever loving and adorable sister Mrs.Jaya Prabha.J, brother-in-law Mr.Suresh.V and daughters Ms. Sadhana Suresh, and S.Angel for all their love and support.
I extend my gratitude to all my friends especially Mr.Kaviyarasan.K, who helped me during the difficult phases of this study.
ANOVA - Analysis of Variance
APA - American Psychiatric Association
CAPTA - Child Abuse Prevention and Treatment Act CBT - Cognitive Behavioural Therapy
CINHAL - Cumulative Index to Nursing & Allied Health
CPTSD-I - Children’s Post Traumatic Stress Disorder Inventory
CSA - Child Sexual Abuse
DHHS - The Department of Health and Human Services
DSM-IV-TR - Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition-Text Revision
EMDR - Eye Movement Desensitization and Reprocessing
ERASE-Stress - Extended Enhancing Resiliency Amongst Students Experiencing Stress
MEDLINE - Medical Literature Analysis and Retrieval System
NCRB - National Crime Records Bureau
PMRT - Progressive Muscle Relaxation Therapy
POCSO - Protection of Children against Sexual Offences Act PTSD - Post Traumatic Stress Disorder
RCTs - Randomized Controlled Trials
TAU - Treatment As Usual
TF-CBT - Trauma-Focused Cognitive Behavioral Therapy
CHAPTER
NO. TITLE
PAGE NO.
1 INTRODUCTION 1
1.1 Background of the study 6
1.2 Significance and Need for the study 17
1.3 Conceptual framework 29
2 AIMS AND OBJECTIVES 40
2.1 Title 40
2.2 Statement of the problem 40
2.3 Research questions 40
2.4 Objectives 40
2.5 Operational definitions 41
2.6 Null hypotheses 43
2.7 Assumptions 44
2.8 Delimitations 44
3 REVIEW OF LITERATURE 45
3.1 Overview of child abuse and its and the underlying changes among children.
47
3.2 Impact of child abuse among children, family and society 53
3.3 Overview of PTSD related to child abuse 55
3.4 Summary 67
3.5 Gaps in the reviewed literature 68
4 MATERIALS AND METHODS 69
4.1 Research Methodology 69
4.2 Research approach 69
4.3 Research designs 69
4.4 Phase -1 Qualitative approach 70
4.4.1 Research designs 70
4.4.2 Research setting 71
4.4.4 Data Generation 72
4.4.5 Ethical Considerations 74
4.4.6 Qualitative Transcription 74 4.4.7 Aggregate of the exploration in to cluster for the developing
stay safe nursing care package
75
4.4.8 Thematic analysis of the transcribed data 77
4.4.10 Interim phase
80
4.5 Quantitative Approach 81
4.5.1 Variables 81
4.5.2 Research Design 82
4.5.3 Research setting 82
4.5.4 Population 83
4.5.5 Sample 83
4.5.6 Sample size 83
4.5.7 Sampling technique 84
4.5.8 Sampling criteria 84
4.5.9 Development of the tool 85
4.5.10 Content validity 87
4.5.11 Reliability of the tool 87
4.5.12 Ethical considerations 87
4.5.13 Pilot study 90
4.5.14 Data collection Procedure 92
5 RESULTS AND ANALYSIS 96
5.1 Description of child abuse among children 98 5.2 Exploration of the lived in experience of children with abuse
using phenomenological approach
102
5.3 Description of demographic variables of the children in study and control group
5.4 Assessment and comparison of pre and post test knowledge and post traumatic stress disorder among children in study and control group
122
5.5 Effectiveness of stay safe nursing care package on knowledge and post traumatic stress disorder scores among children.
127
5.6 Correlation of mean differed knowledge with post traumatic stress disorder scores among children in the study and control group
139
6 DISCUSSION 140
7 SUMMARY, CONCLUSION, IMPLICATIONS,
RECOMMENDATIONSAND LIMITATIONS
164
8 REFERENCES 177
TABLE
NO. TITLE
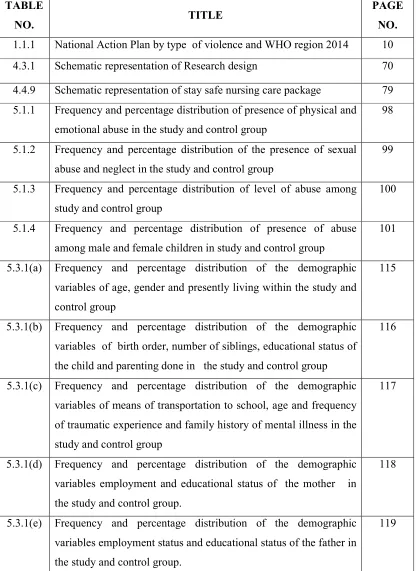
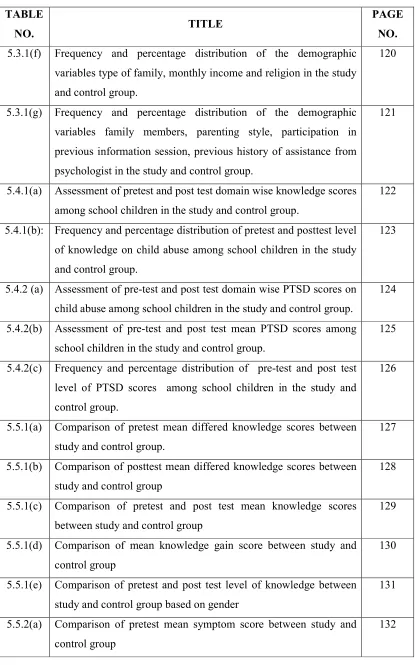
PAGE NO. 1.1.1 National Action Plan by type of violence and WHO region 2014 10
4.3.1 Schematic representation of Research design 70
4.4.9 Schematic representation of stay safe nursing care package 79 5.1.1 Frequency and percentage distribution of presence of physical and
emotional abuse in the study and control group
98
5.1.2 Frequency and percentage distribution of the presence of sexual abuse and neglect in the study and control group
99
5.1.3 Frequency and percentage distribution of level of abuse among study and control group
100
5.1.4 Frequency and percentage distribution of presence of abuse among male and female children in study and control group
101
5.3.1(a) Frequency and percentage distribution of the demographic variables of age, gender and presently living within the study and control group
115
5.3.1(b) Frequency and percentage distribution of the demographic variables of birth order, number of siblings, educational status of the child and parenting done in the study and control group
116
5.3.1(c) Frequency and percentage distribution of the demographic variables of means of transportation to school, age and frequency of traumatic experience and family history of mental illness in the study and control group
117
5.3.1(d) Frequency and percentage distribution of the demographic variables employment and educational status of the mother in the study and control group.
118
5.3.1(e) Frequency and percentage distribution of the demographic variables employment status and educational status of the father in the study and control group.
[image:15.612.110.526.138.709.2]5.3.1(f) Frequency and percentage distribution of the demographic variables type of family, monthly income and religion in the study and control group.
120
5.3.1(g) Frequency and percentage distribution of the demographic variables family members, parenting style, participation in previous information session, previous history of assistance from psychologist in the study and control group.
121
5.4.1(a) Assessment of pretest and post test domain wise knowledge scores among school children in the study and control group.
122
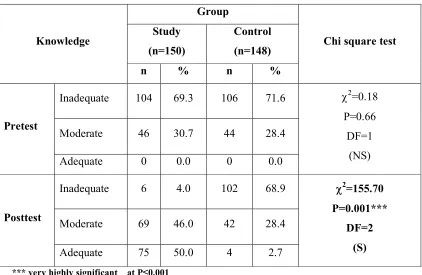
5.4.1(b): Frequency and percentage distribution of pretest and posttest level of knowledge on child abuse among school children in the study and control group.
123
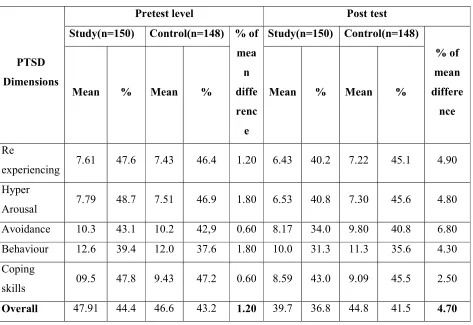
5.4.2 (a) Assessment of pre-test and post test domain wise PTSD scores on child abuse among school children in the study and control group.
124
5.4.2(b) Assessment of pre-test and post test mean PTSD scores among school children in the study and control group.
125
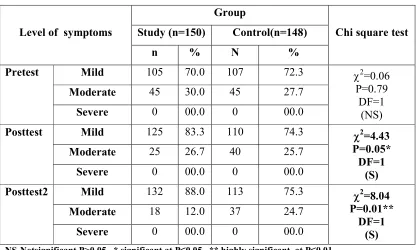
5.4.2(c) Frequency and percentage distribution of pre-test and post test level of PTSD scores among school children in the study and control group.
126
5.5.1(a) Comparison of pretest mean differed knowledge scores between study and control group.
127
5.5.1(b) Comparison of posttest mean differed knowledge scores between study and control group
128
5.5.1(c) Comparison of pretest and post test mean knowledge scores between study and control group
129
5.5.1(d) Comparison of mean knowledge gain score between study and control group
130
5.5.1(e) Comparison of pretest and post test level of knowledge between study and control group based on gender
131
5.5.2(a) Comparison of pretest mean symptom score between study and control group
[image:16.612.110.525.61.726.2]5.5.2(b) Comparison of post test 1 mean PTSD symptom score in study and control group
133
5.5.2(c) Comparison of post test2 mean PTSD symptom score in study and control group
134
5.5.2(d) Comparison of mean PTSD symptom scores between study and control group
135
5.5.2(e) Comparison of pretest, post test 1, post test2 PTSD symptom scores between study and control group
136
5.5.2(f) Comparison of pretest, post test 1 and post test 2 mean reduction score of PTSD between study and control group
137
5.5.2(g) Comparison of pre and post test mean PTSD symptom scores between study and control group based on gender
138
5.6.1 Correlation of mean differed knowledge score with PTSD symptom score in study and control group
[image:17.612.110.527.67.386.2]FIGURENO. TITLE
1.1.1 Types of child abuse among children in U.S in 2014 1.1.2 Number of child abuse in the U.S in 2014
1.1.3 Number of cases of child abuse in U.S, 2014 1.1.4 Prevalence of child abuse in Chennai
1.1.5 Prevalence of PTSD among children 1.3.1 Child Health Promotion Model
1.3.2 Integrated theory of Child Health Promotion Model and Wiedenbach Prescriptive theory
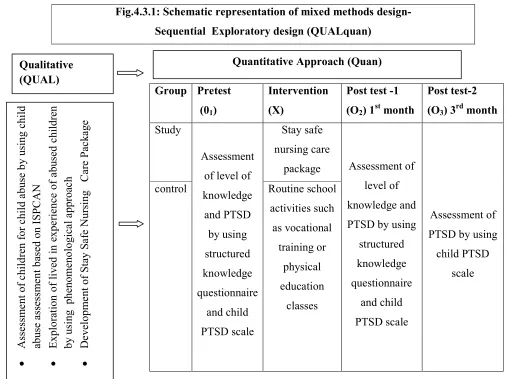
4.3.1 Schematic representation of mixed methods design
5.5.1(a) BOX-PLOT compares the pretest and posttest knowledge score between experiment and control group of children
5.6.1(a)
Scatter diagram between the mean knowledge gain score with symptom reduction score in study group5.7.1(a)
Association of the selected demographic variables (Age, Gender and Birth order) with mean differed knowledge score5.7.1(b)
Association of the selected demographic variables with mean knowledge score5.7.1(c)
Association of the selected demographic variables with mean differed knowledge score5.7.1(d)
Association of the selected demographic variable with mean differed of knowledge score5.7.2(a)
Association of selected demographic variable with mean differed of PTSD symptom score5.7.2(b)
Association of selected demographic variable with mean differed PTSD symptom score5.7.2(c)
Association of selected demographic variable with mean differed PTSD symptom scoreS.No. TITLE
A Provisional Registration Certificate for the Award of Ph.D B Confirmation of Provisional Registration
C Ph D Execution Plan-Gantt Chart D Ethical Clearance Certificate E IEC Approval Certificate F Setting Permission Letter G Plagiarism Analysis Report H Certificates
I Research publications
J List of Content Validity Experts
K Certification for cognitive behavioural therapy L Consent letter from the lawyer
M Certificates of English and Tamil Editing N Informed Consent (English and Tamil) O Informed Assent
P Data Collection Tool (English and Tamil) Q Intervention Tool (English and Tamil) R Ph.D Synopsis Submission Application form S Ph.D Thesis Submission Application form T Photos
Effect of Stay Safe Nursing Care Package on Knowledge and Post-Traumatic Stress Disorder Regarding Child Abuse Among School Children - A Mixed Method Approach.
Background: Childhood is an important phase in every human life as they are the future asset of the society. Child abuse is one of the most desolate and increasing social problem today. A child of any age can be abused as they are dependent on adults and they are vulnerable to be abused due to their developmental stages and the rearing environment. These effects can affect the physical, psychological, social status of the child, family and the society .
Aim of the study: To explore the lived in experience of children with child abuse and to assess the effectiveness of stay safe nursing care package on level of knowledge andPost Traumatic Stress Disorder (PTSD) among school children.
Materials and Methods: The study was conducted using a mixed methods approach, using sequential exploratory research design in which qualitative study was done using phenomenological approach to explore the lived in experience of children with child abuse and quantitative approach was conducted by using a quasi experimental research design. Five participants for qualitative, two hundred and ninety eight children who had been abused and with PTSD symptoms were selected for quantitative approach by using non probability purposive sampling technique. Data was collected using interview guide for the qualitative component and structured knowledge questionnaire was used to assess the knowledge and Post Traumatic Stress Disorder symptom scores was assessed by Child PTSD scale.
Results: The qualitative data derived the themes based on the lived in experience of children regarding child abuse, contributing factors, types of abuse, impact of abuse and reporting of abuse. Based on this report and experts suggestions, stay safe nursing care package was designed and tested for its effectiveness among children with abuse .The comparison between the mean differed knowledge score between the groups revealed a high level of statistical significance at P<0.001.The mean differed PTSD symptom reduction score was 19.6 after intervention. Statistically significant correlation was observed between knowledge and PTSD symptom scores. Statistically significant association of selected demographic variables with mean differed knowledge and PTSD symptom scores was identified in the study group thus indicating that stay safe nursing care package was effective and viable in reducing the symptoms of PTSD among children.
Conclusion : The stay safe nursing care package was found to be a need based nursing intervention for school children to promote awareness about child abuse and reduced the symptoms related to PTSD which occurred due to abuse .The Mixed Methods approach had helped the researcher to identify the children needs before framing the stay safe nursing care package.
Childhood is a crucial period focusing on health, developmental needs and their rights, as it is the time in which children gain knowledge, skills, learn to manage emotions, relationships which are essential to assume adult role .It’s a time of discovery and disorientation as it brings also the issues related to independence and self-identity as they face difficult task of school work, romantic interests, appearance, peer groups and their involvement in social life. Childhood involves most rapid phases of human development as the changes appear universal as it depends on their rearing nature of the parents, nutrition, socioeconomic status and gender of the child.They are the young people aged between 10 to 19 years in which early adolescence were from 10-14 years, middle adolescence from15-17 years and late adolescence and young adults were from18-24years. According to CAPTA (Child Abuse Prevention And Treatment Act), the term child is someone who has not reached the age of 18; or (except in the case of sexual abuse) the age specified by the child protection law of the State in which the child resides.
serious harm.”
Children are too young or too vulnerable to disclose their experience or to protect themselves. The lack of adequate data on the issue is likely compounding the problem by fuelling the misconception that violence remains a marginal phenomenon, affecting only certain categories of children and perpetrated solely by offenders with biological predispositions to violent behaviour. One of the limitations inherent in any attempt to document violence against children is what it leaves out: the presumably large numbers of children unable or unwilling to report their experiences. Considering the evidence regarding the impact of childhood maltreatment upon development of the child, the present study aimed to answer the following Research questions
• How exposure to child abuse does affect the child?
• What is the impact of stay safe nursing care package on knowledge and level of PTSD among children?
To investigate this issue, the researcher explored the unknown factors about the impact of abuse, lived in experiences among children with abuse, which can help the researcher to frame nursing care focused intervention which is to be given in schools.
Objectives of the study:
• To identify children with abuse among children at selected schools.
traumatic stress disorder symptom among children in study and control group.
• To assess the effectiveness of stay safe nursing care package on knowledge and Post-Traumatic Stress Disorder symptom among children.
• To correlate the mean differed knowledge score with Post-Traumatic Stress Disorder symptom score among children in study and control group.
• To associate the selected demographic variable with the mean knowledge and Post-Traumatic Stress Disorder symptom score among children in study and control group.
The Null hypotheses formulated for the study are
NH1- There is no significant difference in pre and post-test level of knowledge and
Post-Traumatic Stress Disorder symptom score among children with abuse between study and control group at p<0.05 level .
NH2- There is no significant correlation between the mean differed knowledge with
Post-Traumatic Stress Disorder symptom score among children with abuse in the study and control group at p<0.05 level.
NH3- There is no significant association of selected demographic variables with mean
differed knowledge and Post-Traumatic Stress Disorder symptom score in study and control group at p<0.05 level
A Mixed method research approach with sequential exploratory research design was chosen to conduct this study. The Qualitative study was conducted by using phenomenological approach and quantitative approach was conducted using quasi experimental research design. The dependent variable was the level of knowledge and PTSD among children while the independent variable was stay safe nursing care package.
In the phase 1 of the study, children of 12 -17 years were screened for risk of child abuse by using modified child assessment tool based on ISPCAN (International Society for Prevention of Child abuse and Neglect), children who had severe child abuse were selected as participants for qualitative component of the study .They were explored to know their lived in experience of being abused using descriptive phenomenological approach.
After obtaining suggestions from experts and with adequate reviews the designed intervention has been tested for its effectiveness in enhancing the level of knowledge and PTSD regarding child abuse. Structured knowledge questionnaire and Child PTSD scale was used to assess knowledge and PTSD respectively.
package was designed based on the themes derived from the qualitative study. The interventions were planned and tailored in sessions based on literature reviews and experts opinion.
In the phase 2 the quantitative approach was conducted by selecting 300 samples, chosen by purposive sampling technique from three Government schools at Thiruvallur District. The required sample size of 125 samples per group was calculated by power analysis. Hence the investigator had enrolled 150 samples in each group. Considering the possibility of attrition, the final sample size on completion of the study was 298 school children with 150 in study group and 148 in control group. Equal number of boys and girls were proportionately selected for study and control group. The tool was translated into regional language Tamil and administered by self report method, following validation by speciality and Tamil language experts. The reliability of the tool was high and was established through test for stability and internal consistency. Hence these tools were appropriate for assessing the level of knowledge and PTSD among school children in selected schools.
respect for human dignity and justice throughout the study period.
RESULTS AND DISCUSSION
Data was analysed using Statistical Package for Social Science / PC+ Version.20. Results derived from phase 1 of qualitative study was utilised to frame the nursing intervention called as stay safe nursing care package that comprised of tailored interventions based on the themes derived from the study. The effectiveness of the intervention was tested by comparing the level of knowledge and PTSD between study and control group.
The comparison between the mean differed knowledge score between the groups revealed that calculated unpaired ‘t’ test value was 19.16 which was found to be highly statistically significant at P<0.001.The mean differed level of PTSD symptom reduction score in the study group was 19.16 in post test 1 and 17.8 in post test 2, however in control group the reduction score was from 03.0to 02.7. The calculated F value by repeated measures of ANOVA in study group was 947.24 which was found to be highly statistically significant at P<0.001 level which indicated that stay safe nursing care package was effective in reducing the symptoms of PTSD among children .
CONCLUSION
CHAPTER 1
CHAPTER – 1
INTRODUCTION
Childhood is an important phase in every human life as they are the future asset
of the society.1 They are like buds, which need to be properly nourished, nursed so that
they bloom fully.2 Childhood is the best time for the development of physical,
psychological, social, intellectual and emotional aspects of an individual. As the child
approach the transition from a child to adolescence thus faces various challenges in
different dimensions. 3
Childhood is a crucial period focusing on health, developmental needs and their
rights, as it is the time in which children gain knowledge, skills, learn to manage
emotions, relationships which are essential to assume adult role.4 It’s a time of discovery
and disorientation as it brings also the issues related to independence and self identity as
they face difficult task of school work, romantic interests, appearance, peer groups and
their involvement in social life. Childhood involves most rapid phases of human
development as the changes appear universal as it depends on their rearing nature of the
parents, nutrition, socioeconomic status and gender of the child.5 They are the young
people aged between 10 to 19 years in which early adolescence were from 10-14 years,
middle adolescence from15-17 years and late adolescence and young adults were from
18-24years.5The United Nations Convention on the Rights of the child defines Child as
"a human being below the age of 18 years unless under the law applicable to the child,
Childhood is a time of rapid development in body systems that are critical to
health including the brain, nervous, endocrine and immune systems. These systems are
under construction even before birth from the earliest moments of life, a child’s
experience and environment exert powerful influences on his or her development and
functioning. Poorly constructed systems have an impact on health in early life, and these
effects may be magnified as children grow in to adulthood. Some children are vulnerable
to experience violence, sexual abuse, child labour and child abuse due to their nature,
family circumstances and the environment.
Child abuse is one of the most desolate and increased social problem today. A
child of any age can be abused as they are dependent on adults and they are vulnerable to
be abused due to their developmental stages and the rearing environment.7Children are
often exposed to different forms of abuse in their home or at schools with regard to
physical, emotional, sexual or neglect.8 According to WHO (World Health Organization),
Child abuse also refers to any act or failure to act that violates the rights of the child that
endangers his or her optimum health, survival and development.9 CAPTA (Child Abuse Prevention and Treatment Act)also defines Child abuse and neglect as “at a minimum,
any recent act or failure to act on the part of a parent or caretaker, which results in death,
serious physical or emotional harm, sexual abuse or exploitation, or an act or failure to
act which presents an imminent risk of serious harm.”11
Child abuse is the common phenomenon among children that may occur in four
forms such as physical abuse, emotional abuse, sexual abuse and neglect.10 The WHO
defines physical abuse as an intentional use of physical forces against the child that
development or dignity. Physical abuse is when a child has been physically harmed due
to some interaction or lack of interaction by another person, which could have been
prevented by any person in a position of responsibility, trust or power. Example of
physical abuse includes hitting, beating, kicking, shaking, biting, strangling, scalding,
burning and poisoning.12
WHO also states that emotional abuse can be seen as a failure to provide a
supportive environment and primary attachment figure for a child so that they may
develop a full and healthy range of emotional abilities. Forms of emotional abuse
includes patterns of belittling such as spreading rumors, blackmailing a child,
denigrating, blaming, scaring, discriminating or ridiculing.13 Child Sexual Abuse (CSA)
is a form of child abuse in which an adult or older adolescent abuses a child for sexual
stimulation. Sexual abuse refers to the participation of a child in a sexual act aimed
toward the physical gratification or the financial profit of the person committing the act.
Sexual abuse is engaging a child in any sexual activity that he or she does not understand
or cannot give informed consent for or is not physically, mentally or emotionally
prepared for. This includes using a child for pornography, sexual materials, prostitution
and unlawful sexual practices.12
Neglect is the failure to meet a child’s basic needs. These needs include housing,
food, clothing, education, and access to medical care. Child neglect can include physical
neglect such as failing to provide food, clothing, shelter, or other physical necessities,
emotional neglect such as failing to provide love, comfort, or affection, or medical
Some of the warning symptoms of child abuse among children is exhibited as
withdrawal from friends or usual activities, changes in behavior such as aggression,
anger, hostility or hyperactivity or changes in school performance, depression, anxiety or
unusual fears or a sudden loss of self-confidence, frequent absences from school,
reluctance to leave school activities, attempts at running away, rebellious or defiant
behavior, attempts at suicide.16 Specific signs of physical abuse include unexplained
injuries, such as bruises, fractures or burns, injuries that don't match the given
explanation, untreated medical or dental problems. Signs and symptoms of sexual abuse
includes sexual behavior or knowledge that's inappropriate for the child's age, pregnancy
or a sexually transmitted infection, blood in the child's underwear, statements that he or
she was sexually abused, trouble walking or sitting or complaints of genital pain .17
Children also exhibits signs and symptoms of emotional abuse such as delayed or
inappropriate emotional development, loss of self-confidence or self-esteem, social
withdrawal or a loss of interest or enthusiasm, depression, headaches or stomachaches
with no medical cause, avoidance of certain situations, such as refusing to go to school
desperately seeks affection, a decrease in school performance or loss of interest in
school, loss of previously acquired developmental skills.17
Individuals exposed to maltreatment present significant impairment in important
developmental aspects such as emotion regulation, the development of attachment,
autonomy, peer relationships, adaptation to school, and self-esteem. Furthermore,
because they are more likely to suffer more than one type of impairment during early
problems and psychological disorders both during childhood and the remainder of their
development.18
Exposure of children to abuse results in problems related to attachment and
interpersonal relationships, learning and developmental disabilities also results in youth
suicide, mental health problems, alcohol and drug abuse, aggression, violence, criminal
activity, and teenage pregnancy.18 However exposure to this type of abuse among
children can also result in Post Traumatic Stress Disorder (PTSD) but there is very
limited research on the relationship between maltreatment and the severity of PTSD
symptoms. Research exploring the relationship between childhood abuse and severity of
PTSD symptoms is rare. Studies largely focus on prevalence of abuse among children.
Limited amount of research is available that focuses on the severity of PTSD symptoms
resulting from this type of trauma.19
It is not always easy to recognize when a child has been abused. Children who
have been mistreated are often afraid to tell anyone, because they think they will be
blamed or that no one will believe them. Sometimes they remain quiet because the
person who abused them is someone they love very much, or because of fear, or both.
Parents also tend to overlook signs and symptoms of abuse, because they don’t want to
face the truth. This is a serious mistake. A child who has been abused needs special
support and treatment as early as possible. The longer they continues to be abused or is
1.1 BACKGROUND OF TH The age group of 12
biological and hormonal char
behavioural and sexual matur
in the Prevalence of many of
phase of rapid growth and
behavioural changes occur.21
21% of Indian population. Mo
due to preventable causes. Y
of awareness about physica
and the ill health affecting t
constitutes holistic health of
[image:34.612.116.522.403.622.2]physical abuse are increasing
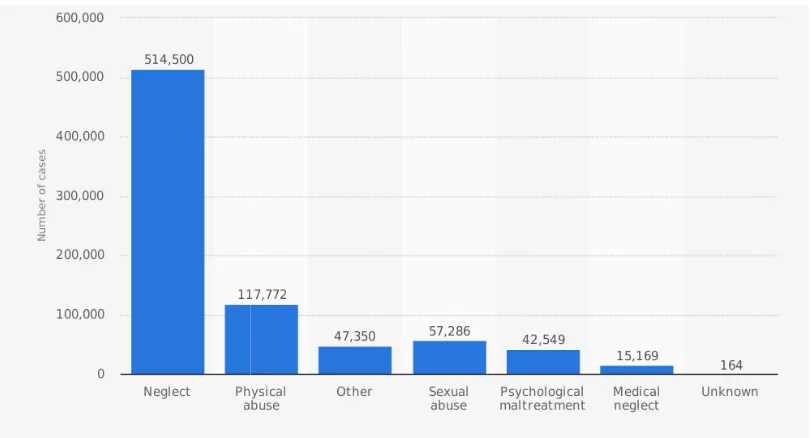
Fig 1.1.1: Types of child abu
Source:Child trends data ban
F THE STUDY
12 -17 years is characterized by rapid changes in t
l characters of the individual resulting into her/his ps
maturation. This phase is characterized by a remarka
ny of the threats to children, including violence and a
and development during which physical, physio
21
They constitute more than 1.2 billion worldwid
on. Morbidity and mortality occurring in this age grou
ses. Young and growing children have poor knowled
sical and psychological changes that occurs during
ting them. Apart from physical health, a positive s
lth of the children. Prevalence of sexual abuse, v
asing among the children.22
abuse among children in U.S (2014)
ta bank indicator66
es in the physical,
his psychological,
markable upswing
and abuse. It is a
physiological and
ldwide, and about
e group is mostly
owledge and lack
uring adolescence
itive social health
The above figure 1.1
abuse reveals that in 2014
abuse and 514,500 cases of ne
public health and social prob
includes all forms of physica
negligent treatment and explo
life-long consequences. In sp
income countries, data from
maltreatment indicate that ne
physical abuse as a child, 36
physical neglect, with no sig
lifetime prevalence rate of ch
gender – 18% for girls an
maltreatment include impaire
[image:35.612.116.506.458.682.2]and job and relationship diffic
Fig 1.1.2: Number of
Source:Child trends d
re 1.1.1 shows the global statistics of different for
4, 117,772 cases of physical abuse, 57,286 case
s of neglect were reported in the U.S. Child abuse is a
al problem in the worldwide. According to WHO
hysical and/or emotional ill-treatment, sexual abuse,
exploitation. Child maltreatment is a global problem
. In spite of recent national surveys in several
low-a from mlow-any countries low-are still llow-acking. Estimlow-at
hat nearly a quarter of adults (22.6%) worldwide
ild, 36.3% experienced emotional abuse and 16.3%
no significant differences between boys and girls. H
of childhood sexual abuse indicates more marked dif
rls and 7.6% for boys. The lifelong consequenc
paired physical and mental health, poorer school p
difficulties.23
ber of victims of child abuse in U.S (2016) ends data bank indicator 66
nt forms of child
6 cases of sexual
is a recognized
HO, child abuse
buse, neglect and
blem with serious
- and
middle-stimates of child
ide suffered with
6.3% experienced
irls. However, the
ked differences by
quences of child
The above figure 1.1.2
in 2016, by race and ethnicit
children of Hispanic origin an
the last decade, recognition o
children has grown. Still,
underreported. This can be att
forms of child abuse agains
perceived as being abusive. 24
Fig 1.1.3: Number of cases o
Source:Child trends data ba
The above figure 1.1
during 2014 revealed that ch
majority of the children wer
adolescents have also suffere
in their study reported about t
e 1.1.2 indicates the number of victims of child abuse
thnicity revealed that about 269,252 children of Wh
igin and 5,686 children of Asia were reported to be a
ition of the pervasive nature and impact of child ab
Still, the phenomenon remains largely undocum
be attributed to a variety of reasons, including the fa
against children are socially accepted, tacitly condo
24
ases of child abuse in U.S(2014)
ata bank indicator66
re 1.1.3 indicates the number of cases of child ab
hat children of all age group are at risk of abuse, e
n were in the age of 2-5 years including school c
uffered with abuse. Fang X, Fry A Deborah, Brown
bout the burden of child abuse in the East Asia and Pa
abuse in the U.S.
of White, 147,719
o be abused. Over
hild abuse against
documented and
the fact that some
condoned or not
ild abuse in U.S.
, even though
hool children and
rown Derek et al,
as they addressed a significant gap in the current evidence base in the field of child
abuse. Systematic reviews and meta-analyses were conducted to estimate the prevalence
of child physical abuse, sexual abuse, emotional abuse, neglect, and witnessing parental
violence, identified that the economic burden of child maltreatment in the East Asia and
Pacific region is substantial, indicating the importance of preventing and responding to
child maltreatment in this region.25
It is estimated that, worldwide, at least 1 in 10 girls and 1 in 20 boys experience some
form of sexual abuse in childhood. Those who are sexually abused as children are more
susceptible to depression, eating disorders, suicidal behaviour, or drug and alcohol problems
later in life, and are more likely to become victims of sexual assault as adults. In many
countries, children are taught how to recognize, react to, and report abuse situations through
school-based programmes designed to help prevent sexual abuse.26
The Cochrane researchers reviewed data from 24 trials in which a total of 5,802
children took part in school-based prevention programmes in the US, Canada, China,
Germany, Spain, Taiwan, and Turkey. Schools involved in the trials used a variety of
methods to teach children about sexual abuse, including teaching of safety rules, body
ownership, and who to tell through films, plays, songs, puppets, books, and games. In
children who did not receive the intervention, around 4 in 1,000 children disclosed some form
of sexual abuse. This contrasts with 14 in 1,000 children in the intervention groups, who
In Kenya and even in many other countries, data on the prevalence of child abuse
is still scarce. A Kenyan study showed that violence against children was very high, with
31.9% and 17.5% female and male, respectively reporting having been exposed to sexual
violence, 65.8% and 72.9% female and male respectively to physical violence.
In the same study, 18.2% and 24.5% female and male, respectively had been
abused prior to attaining 18 years of age, and only 23.8% female and 20.6% male
reported not having experienced any form of violence during childhood. Recently, some
studies have investigated child abuse in different cities of Iran, but there is not an overall
estimation of child abuse in the whole country.27 Most of these studies focus on any
types of child abuse except sexual abuse due to cultural issues. For example, a study
conducted in Tehran, the capital city of Iran, revealed the prevalence of 17.5% for
physical abuse and prevalence of 36.4% and 49.46% for neglect and emotional abuse,
respectively, 29 another study showed that the prevalence of emotional abuse, physical
abuse and neglect was 78%, 56% and 39% in Zanjan, respectively .30
Table 1.1.1: National action plan by type of violence and WHO Region, 2014
Type of violence African region% Region of Americas% Eastern Mediterranean region% European region% South East Asia region% Western pacific region% All countries% Child
maltreatment 56 91 69 78 88 55 71
Prevention
Home
visiting 07 52 31 51 13 30 35
Parent
education 11 57 44 46 13 40 38
Child sexual abuse prevention
44 62 31 29 0 35 37
Source: Regional Action Plan for Violence and Injury Prevention in the Western
The above table 1.1.1 illustrates the percentage of child abuse prevalence in
South East Asian Countries, identified that in America and South East Asian Countries
and European regions the child abuse is more common .However preventive strategies
like home visiting, parental education regarding child abuse an child sexual abuse
prevention is been effectively practiced in other countries except South East Asian
countries.31
India is the home to 19 percent of the world’s children, that is, nearly 440 million
people in India are under the age of 18 years. This is 5-times higher than the population
of children in the US, and is in fact higher than the total population of the US.More
recently, a report by the National Crime Records Bureau (NCRB) for 2016 reported that
8,800 cases of rape on children were registered across the country under the Protection of
Children against Sexual Offences Act (POCSO), and also identified that 25.3 per cent of
child abuse involves offenders as employers or co-workers. The data revealed that
abusers of 35.8 % is neighbors in 2015.32In over 10 per cent of cases last year, children
were subjected to rape by their own family members or relatives,94.8 per cent of cases,
children were subjected to rape by someone known to them and 14,913 cases were
registered under POCSO in 2015.It also reported that Uttar Pradesh led the highest
number of child abuse cases (3.078), followed by Madhya Pradesh (1,687 cases), Tamil
Nadu (1,544cases), Karnataka(1480 cases) and Gujarat (1,416 cases).33
In Chennai cases of child sexual abuse have been causing a major concern with
several new instances being reported and the accused going scot free. There seems to be
no follow up on the complaints, as in most of the cases child abusers are habitual
abuse cases are low in Chennai even after the enactment of the POCSO , a child line
source also revealed that in many cases the abuse among children remain unreported as
they too scared to come out and complaint to the school level vigilance committees have
also not been functioning effectively as the reputation of the schools may be lost.35
As per Childline data, physical torture of children is also very much prevalent in
the city. From April 2015 to March 2016, there were 27 cases of child sexual abuse,
including 10 rape cases and 96 complaints of physical abuse of children were also been
reported an in the last four months alone, there were 11 cases of child sexual abuse in
Chennai and 5 of them were rape cases and 26 complains on physical abuse. Police
official also reported that in many cases the victims and parents do not like to pursue the
complaint as they lose interest and request to settle the case out of court due to fear of
losing dignity. 34
Recently Tulir, also reported that in Chennai 35% of children were below the age
group of 18 years, abuse is more common among 11-15 years age group and 45% of
abuse is more common among children.35
Fig 1.1.4: Prevalence of abuse in Chennai
Source:Tulir, (NGO) Chennai35
0 20 40 60 80 100
Sexually abused severely abused
The above figure 1.1.5 depicts that even though severely abused is less common
among children but most of the boys and girls were sexually abused. The effects of
exposure to child maltreatment on self-esteem, social competence, relationships with
peers, and school performance have been widely investigated by international studies.
However, in India, studies about the relationship between these variables are scarce.
National studies have focused on aspects such as the prevalence and consequences of
abuse, especially sexual abuse, in certain situations and their related factors, the risk of
developing mental illness in individuals exposed to maltreatment and the development of
group interventions for victims of sexual abuse. Furthermore, most of these published
studies did not compare groups with the presence and absence of childhood
maltreatment.36
Child abuse is often accompanied by verbal violence which consists in denying
children their personality, hurling abusive words at them or forbidding them to enquire
about their rights and/or to carry out their activities. This psychological violence results
in discrediting and depriving the child and can lead child towards delinquency. The
ensuing traumas could be medical, causing physical wounds, shock or serious lesions.
They could also be psychiatric, leaving behind emotional memories of a painful event
deep-rooted in the brain. All forms of child abuse has serious consequences such as
fear, anxiety, depression as well as disorders relating to behavior, sleep, feeding, and
speech, and may even result in suicide, or suicide attempt. 37
There are two distinct types of violence experienced by children defined by the
United Nations as child maltreatment by parents and caregivers in children aged 0-14,
These different types of violence can be prevented by addressing the underlying causes
and risk factors specific to each type, a WHO study in 2010, estimated that the lifetime
impact of child sexual abuse accounts for approximately 6% of cases of depression, 6%
of alcohol and drug abuse/dependence, 8% of suicide attempts, 10% of panic disorders
and 27% of post traumatic stress disorders. Other studies have also linked child physical
abuse, sexual abuse and other childhood adversities to excessive smoking, eating
disorders, and high-risk sexual behavior, which in turn are associated with some of the
leading causes of death including cancers and cardiovascular disorders.39
The statistics on physical child abuse are alarming. It is estimated that hundreds
of thousands of children are physically abused each year by a parent or close relative.
Thousands actually die as a result of the abuse. For those who survive, the emotional
trauma remains long after the external bruises have healed. Communities and the courts
recognize that these emotional “hidden bruises” can be treated. Early recognition and
treatment is important to minimize the long term effect of physical abuse. Whenever a
child says he or she has been abused, it must be taken seriously and immediately
evaluated.40
The exposure to conditions of abuse and neglect during childhood has been
associated with an increased risk of psychological, social, and behavioral impairment.
Studies suggest that degree of impairment depends on the type of abuse involved as well
as its severity. There is also evidence that abused children are generally exposed to more
than one type of maltreatment. Therefore, to better understand the impact of
maltreatment on child development, specific instruments and analyses must be developed
The impact of exposure to maltreatment on psychological adjustment has been
investigated through the variables that make up this construct, such as academic
performance, self esteem and social competence. Relationships among exposure to
maltreatment, academic failure, and development of psychopathology have been reported
in a number of studies. Children who are victims of maltreatment tend to have lower
grades in school, exhibit impairment in standardized tests, and display poorer academic
performance as compared to children who were not maltreated Even in school,
disadvantages in relation to their peers are found. 43Children who experienced abuse and
neglect tend to react with greater aggressiveness toward peers or sometimes stay socially
isolated.
Despite the limited research in this area, the studies that have been done so far
offer some sense of the trends in this area. Multiple Researchers Ford, Wasser, and
Connor looked at a sample of children in a psychiatric outpatient setting who had
experienced polyvictimization, exposure to multiple types of maltreatment and domestic
based traumas, and found that polyvictimization was associated with severe
parent-reported externalizing issues and clinician parent-reported psychosocial issues and that PTSD
was the only psychiatric diagnosis associated with polyvictimization.44
Wechsler-Zimring and Kearney’s also studied among adolescents who
experienced different types of maltreatment found that almost 90% of their sample fit
criteria for PTSD and that adolescents who had experienced physical and or sexual abuse
had higher mean scores for each of the symptoms observed by the Children’s PTSD
experienced neglect and physical and/or sexual abuse and the lowest scores were found
in adolescents who had only experienced neglect.45
The lack of research on maltreatment makes it difficult to draw conclusions about
a relationship between this type of trauma and the severity of symptoms. The
information that is available suggests that a relationship does indeed exist but there is not
enough research available to draw any further conclusions. Children are too young or too
vulnerable to disclose their experience or to protect themselves. The lack of adequate
data on the issue is likely compounding the problem by fuelling the misconception that
violence remains a marginal phenomenon, affecting only certain categories of children
and perpetrated solely by offenders with biological predispositions to violent behaviour.
46
One of the limitations inherent in any attempt to document violence against children is
what it leaves out, the presumably large numbers of children unable or unwilling to
report their experiences.
Considering the evidence regarding the impact of childhood maltreatment upon
development of the child, the present study aimed to answer the following research
question, how does exposure to childhood abuse affects the child? To investigate this
issue, the researcher explored the unknown factors about the impact of abuse, lived in
experiences among children with abuse, which can help the researcher to frame a set of
1.2 SIGNIFICANCE AND NEED FOR THE STUDY
Childhood is the period of means 'to emerge' to achieve 'identity'. The term
“childhood” means “to grow” or “to grow to maturity”. Maturing involves not only
physical but also mental growth. It is a period, which fills the gap between childhood and
adulthood.48 Generally, this period is termed as “youth” which includes the often
neglected but equally important aspects, which are emotional or psychological, social
and spiritual. The time of growing up from child to adulthood is known as the childhood
period. It is a period of physical growth.49 However, it is more than that. It is a time for
the maturing of mind and behaviors as well. The length of time for this period of
development varies. On the one hand reaching out towards adult roles and on the other
still needing the love and protection of parents. It is a time when children undergo a
crisis of identity.48
Late childhood period is often believed to be a difficult period and very critical
stage of transition because of various qualitative shift that they pass through at that
moment of life and this conflicts with breaking away from the old self and interest of the
childhood memories and all these periods are accompanied by significant changes of
various degrees for instance, all the characteristics involved in puberty such as menstrual
cycle in girls and hair growth in certain part of the body in boys as well as deepening of
the voice.50
Child abuse is threatening and disruptive to normal child development. The very
persons charged with the care and nurturing of a child, and to whom the child turns for
food, love, and safety, can cause the child pain and injury. The child then learns to
characteristics and behaviors. Most common among these are anger, acting out,
depression, anxiety, aggression, social withdrawal, low self-esteem, and sleep
difficulties. 51
At the extreme end, abuse can cause a child to dissociate and develop disorders
such as schizophrenia, amnesia, and personality disorder. Personality disorder is a mental
disorder that affects a person's ability to function in everyday activities such as work,
school, and interpersonal relationships. Borderline personality disorder is a frequent
diagnosis for children who are victims of abuse or neglect. Symptoms can include
paranoia, lack of impulse control, limited range of emotions, and inability to form close
and lasting relationships.51
A common problem found in children who have been physically abused is
disruptive disorders. It has been shown that at least 30% of people who have been
physically abused have lifetime disruptive disorder diagnosis, such as oppositional
defiant disorder or conduct disorder higher aggressive and delinquent behaviours.
Research has also indicated that physically abused children tend to be less popular and
liked and had fewer friendships. As well, physically abused children showed less
intimacy and more conflict and negative affect towards their close friends in comparison
to the non-abused group.52 These children also tend to be shyer and inhibited in
interpersonal contacts than the non-abused group
Emotional abuse is the most poorly understood and the least well researched;
despite a growing awareness of the harmful outcomes it can have in later life. Emotional
• Rejection, which may take the form of continual criticism or undermining a child’s self-esteem
• Isolation, so that the child is kept from seeing family and friends from child
• Ignoring, which may involve not responding a child’s efforts to seek attention or failing to acknowledge achievements
• Terrorizing, such as threatening to harm a child or abandon them, Corruption, especially involving a child in crime
• Exploitation, such as forcing a child to work to provide family income and look after sibling.53
This was also supported by a study conducted by Ba-Saddik, A. S. S., & Hattab,
A. S. among pupils in basic education schools in Yemen revealed that children reported
high rates of emotional abuse 55.2% at least once in their school lifetime. Male pupil’s
had higher prevalence of emotional abuse 72.6% than females 26.1%. Teachers
constituted the highest proportion of perpetrators 45.6%. Odds Ratio (95% confidence
interval) showed statistically significant association between emotional abuse and pupils'
gender, family type and father’s education respectively.54
Sexual abuse also has long-lasting negative effects on children. Sexually abused
children have a higher prevalence of psychiatric disorders. This has been illustrated in
several studies (Moylan CA, Herrenkohl TI, Sousa C, Tajima EA, Herrenkohl RC, Russo
MJ, 2013, Zhu, Gao E, Chuang YL, Zabin L S, Emerson MR, Lou C identified the
relationship of child sexual abuse among adolescents in Taipei, revealed that the overall
proportion of CSA was 5.15%, with more females (6.14%) than males (4.16%) likely to
after adjusting other factors, such as age, residence, economic status, education,
employment status, and household instability. Both male’s and female’s with CSA
experience were more likely to report drinking, gambling, and suicidal ideation
compared with those who had no history of CSA. However, the significant association
between CSA and smoking, fighting, and suicidal attempt was not observed among
female’s. 55
Children who were abused often vary in the nature of their responses to traumatic
experiences. The reactions of children may be influenced by their developmental level,
ethnicity or cultural factors, previous trauma exposure, available resources, and
preexisting child and family problems. However, all children and adolescents express
some kind of distress or behavioral change in the acute phase of recovery from a
traumatic event. Not all short-term responses to trauma are problematic and some
behavior changes may reflect adaptive attempts to cope with difficult or challenging
experience. Some children can exhibit symptoms of the development of new fears, sleep
disturbance, nightmares, and sadness, loss of interest in normal activities, reduced
concentration and decline in schoolwork, anger, somatic complaints and irritability.
Although most return to baseline functioning, a substantial minority of children
develop severe acute or ongoing psychological symptoms (including PTSD symptoms)
that bother them, interfere with their daily functioning, and warrant clinical attention.
Some of these reactions can be quite severe and chronic. PTSD in children and
adolescents occurs as a result of a child’s exposure to one or more traumatic events,
actual or threatened death, serious injury, or sexual violence. The victim may experience
repeated or extreme exposure to aversive details of the event. Potentially traumatic
events include physical or sexual assaults, natural disasters, and accidents
Fig.1.1.5: Lifetime Prevalence and distribution of PTSD among children
Source: Lifetime prevalence of mental disorders in U.S66
The above figure 1.1.5 illustrates the presence and distribution of a symptom
among children in U.S which revealed that PTSD symptoms were 6.6% common among
females when compared with male children, 5.8% of children with age group 17-18
years were affected common than other children National Co-morbidity Survey
Replication- Adolescent Supplement is a nationally representative sample of over 10,000
adolescents aged 13-18. Results indicate that 5% of adolescents have met criteria for
PTSD in their lifetime. Prevalence is higher for girls than boys (8.0% vs. 2.3%) and
increase with age. Current rates (in the past month) are 3.9% overall.66 There are no
definitive studies on prevalence rates of PTSD in younger children in the general
Psychological First Aid (PFA) has been used in schools which involves providing
comfort and support, teaches calming and problem solving skills. Trauma Focused
psychotherapies have the most empirical support for children and adolescents .Cognitive
therapy for PTSD focuses on teaching children how to identify, evaluate, and reframe the
dysfunctional cognitions related to the specific trauma and its sequelae that contribute to
the intense negative emotions and behavioral reactions. Cognitive Behavior Therapy
(CBT) includes a range of approaches that have been shown to be effective in treating
PTSD. Cognitive behavioral methods have also demonstrated to be significantly
effective in demonstrating positive outcomes with child sexual abuse victims in children
and in adult survivors.56 CBT methods stem from the central principle that an
individual’s cognitions play a significant and primary role in the development and
maintenance of emotional and behavioral responses to life situations. The manner in
which individuals emotionally and cognitively process a traumatic experience
contributes to the development and maintenance of PTSD. A central theme contributing
to the onset and persistence of PTSD is a perception of ongoing threat, even when the
trauma occurred in the distant past.
Trauma-focused cognitive behavioral therapy (TF-CBT) developed by Cohen,
Mannarino, and Deblinger, is a psychosocial treatment model designed to treat
post