“EFFECTIVENESS OF JABALPUR SCORE IN PREDICTING MORTALITY AND MORBIDITY IN PATIENTS WITH PERITONITIS
CAUSED BY PEPTIC ULCER PERFORATION”
THE DISSERTATION SUBMITTED TO
THE TAMILNADU DR.M.G.R MEDICAL UNIVERSITY In partial fulfillment of the regulations for the award of the degree of
M.S. GENERAL SURGERY – BRANCH I
DEPARTMENT OF GENERAL SURGERY
COIMBATORE MEDICAL COLLEGE AND HOSPITAL THE TAMILNADU DR.M.G.R MEDICAL UNIVERSITY
CERTIFICATE
This is to certify that this is the bonafide dissertation done by DR. VIGNESH SHANKAR S and submitted in partial fulfillment of the requirement for the Degree of M.S. General Surgery, Branch I of the Tamilnadu Dr. M.G.R. Medical University, Chennai.
DATE: UNIT CHIEF
DATE: PROFESSOR & HOD
Department of General Surgery
DATE: DEAN
DECLARATION
I solemnly declare that the dissertation titled “EFFECTIVENESS OF JABALPUR SCORE IN PREDICTING MORTALITY AND MORBIDITY IN PATIENTS WITH PERITONITIS CAUSED BY PEPTIC ULCER PERFORATION” was done by me from July 2017 to July 2018 under the guidance and supervision of PROFESSOR. DR. V. LEKSHMINARAYANI, M.S, D.G.O.
This dissertation is submitted to the Tamilnadu Dr. M.G.R Medical University towards the partial fulfillment of the requirement for the award of M.S Degree in General Surgery (Branch I).
PLACE:
ACKNOWLEGDEMENT
I owe my reverential gratitude and humble thanks to Lord God Almighty for all his mercy, for being with me and showering abundant blessing upon me throughout the course of the study.
I am obliged to record my immense gratitude and thanks to DR. B. ASHOKAN Mch, The Dean, Coimbatore Medical College Hospital for providing all the facilities to conduct the studies.
I express my deep sense of gratitude and heartfelt thanks to Professor DR. V. ELANGO, M.S, Head of Department of General Surgery for his dynamic guidance, constant help and encouragement throughout the study.
I express my respectful gratitude and indebtedness to my guide Professor DR. V. LEKSHMINARAYANI M.S, D.G.O, for her valuable guidance and support.
I would like to express my sincere thanks to Professor Dr.D.N. Renganathan M.S, Professor Dr. Nirmala M.S, Professor Dr.Ganesh Babu M.S and Professor Dr. Srinivasan M.S.
I acknowledge my gratitude to our Registrar Dr. RAVI M.S, D.L.O and all my assistant professors of Department of surgery for their encouragement and support.
I am thankful to The ETHICAL COMMITTEE of Coimbatore Medical College for permitting me to proceed with this dissertation.
Lastly I am grateful to all the patients whose cooperation made this work possible.
DATE:
TABLE OF CONTENTS
S.NO CONTENTS PAGE NO
1. INTRODUCTION
1
2. AIMS AND OBJECTIVES
3
3. REVIEW OF LITERATURE
4
4. METHODOLOGY
41
5. OBSERVATION AND ANALYSIS
45
6. STATISTICS
65
7. DISCUSSION
83
8. CONCLUSION
85
9. BIBLIOGRAPHY
86
10. ANNEXURES
PROFORMA
89
CONSENT FORM
91
ABSTRACT
BACKGROUND:
Many prognostic systems have been developed to stratify perforative peritonitis patients. Many are complex and cannot be used in developing countries as the prognostic system depends on sophisticated investigations. So, a simpler scoring system is developed to stratify those patients.
PATIENTS AND METHOD:
Our study included 50 patients who presented with features of peritonitis due to peptic ulcer perforation and underwent emergency laparotomy for the same in Coimbatore medical college hospital.
RESULTS:
Mortality and morbidity steadily increases with increase in the Jabalpur score. All the parameters in Jabalpur score are individually significant in predicting the outcome. For a score of 9, sensitivity is 87.5%, specificity is 83.3%, positive predictive value is 50% and negative predictive is 97.2%.
CONCLUSION:
Jabalpur score is a simple and effective scoring system to predict the mortality and morbidity in peptic ulcer perforation patients.
KEY WORDS:
1
INTRODUCTION
Perforative peritonitis is the most common case seen in emergency department by the surgeons all around the world especially in developing countries. Perforation leads to seepage of gastrointestinal contents in to the peritoneal cavity which causes an inflammatory process involving the peritoneal layer of abdomen resulting in the cascade of events. The increased morbidity and mortality that attributes to this condition is due to electrolyte disturbance, septic shock that leads to multi organ failure.
Mostly it may be due to abdominal trauma or peptic ulcer perforation or typhoid infected case or even sometimes it may be non infectious too. The severity of bacterial contamination of the peritoneal region depends on the site of localization of the injury. Perforations due to peptic ulcer disease are commonly encountered in first part of duodenum along with pylorus of the stomach.
2
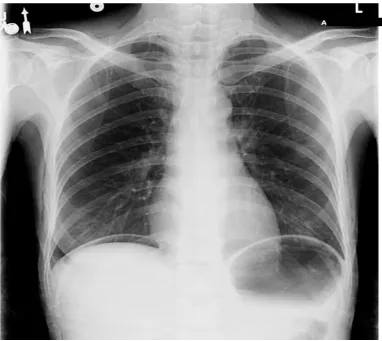
The clinical features include acute abdominal pain, abdominal tenderness, and guarding that is exacerbated by movement of the abdomen that bring visceral organ in contact with the peritoneum, leukocytosis, acidosis and hypernatremia with hypokalemia may be incidental findings. X rays reveal pneumoperitoneum with or without dilated intestines as a sign of paralytic ileus. CT scan helps to differentiate this from other causes. Despite of surgical advances in management and prompt post operative antimicrobial therapy along with antacids the mortality and morbidity is high.
In the view of evaluating the prognostic outcome of patients suffering from this condition multiple scoring system and indexes have been put forth by numerous investigators over the period of time, but many of these scoring grades fall short in aim by requiring lab investigations that are far too complex to obtain in the stipulated period of critical time.
3
AIM AND OBJECTIVES
AIM:
Aim of the study is to find the efficacy of the Jabalpur scoring system in predicting the mortality and morbidity in patients with peritonitis due to peptic ulcer perforation.
OBJECTIVES:
Analysis of physical parameters and blood workup as early as possible to every patient diagnosed with perforative peritonitis.
Incorporation of Jabalpur scoring system in identifying the high risk group of patients in those diagnosed with perforative peritonitis.
Watchful monitoring of those patients with high score to anticipate early complications and for the application of early treatment.
4
REVIEW OF LITERATURE
Perforation refers to sudden breach in the gut wall through which the bowel contents leak out and lead to dreadful complication. It is a life threatening complication unless managed at right time.
Perforation may occur in a patient with chronic peptic ulcer disease. Sometimes it may occur even without any proceeding symptoms.
EPIDEMIOLOGY:
SEX : Perforation occurs most commonly in men than in women
AGE : Most common age group affected include 30-50 years of age
OCCUPATION: Occurs in low socio -economic status
ETIOLOGY AND RISK FACTORS:
The most common etiology for perforation include
Peptic ulcer disease
5 RISK FACTORS:
1. NSAID
2. Excessive alcohol intake 3. Cigarette smoking
4. Emotional/ Physical stress 5. Beverages-tea, coffee 6. Genetic factors
7. blood group
NSAID's – excess intake inadvertently may increase the chance of perforation 5 to 8 times
Excess alcohol intake cause peptic ulcer disease followed by increased chances of perforation
Beverages such as coffee, tea increase acid secretion causing peptic ulcer disease
Cigarette smoking prevent healing of peptic ulcer
6 OTHER FACTORS:
CUSHING ULCER – occurs following head injury, associated with hyper gastric acid secretion
CURLING ULCER - occurs in patients with burns, during convalescence period the mucosal blood flow to the stomach is reduced leading to ulcers
ZOLLINGER ELLISON SYNDROME - causing hypergastrinemia and excess gastric acid secretion
PATHOLOGY
Acute perforation
Sub-acute perforation
Chronic perforation
ACUTE ULCER PERFORATION:
7
Duodenal ulcer is a saddle type of ulcer. Posteriorly may penetrate into the pancreas and anteriorly may perforate. The size of perforation in duodenal ulcer is about 3 mm to 1 cm. Most common cause of perforation is duodenal ulcer.
DUODENAL ULCER
Anterior (90%) Posterior (10%)
Perforation Bleeding
2) GASTRIC ULCER - most commonly found in the
Antrum
Lesser curvature
Very large ulcer on the lesser curvature may penetrate posteriorly and perforate anteriorly. It causes simultaneous bleeding and perforation
8
PATHOPHYSIOLOGY OF PERFORATION:
PERFORATION
Contents of stomach and duodenum leak out
Chemically mediated peritonitis
Extravasation of peritoneal fluid and extra peritoneal oedema
Sequestration of fluid
As soon as the perforation occurs, the contents of the stomach or the duodenum escape into the peritoneal cavity. Contents leaking may be gastric acid, bile, pancreatic enzymes, and bacteria. This leads to chemical peritonitis.
9
Peritoneum as a result of perforation secretes lots of fluids to neutralize the contents leaked from the stomach or duodenum. This leads to temporary reduction of pain. The fluid loss if uncorrected may lead to hypovolemia and shock.
The bacteria from the Gastrointestinal tract enters into the peritoneal cavity through the site of perforation causing diffuse bacterial peritonitis which leads to septicaemia and circulatory failure.
SUBACUTE PERFORATION:
Perforation in which the contents do not leak out because of immediate sealing mechanism. In sub acute perforation patient usually have sudden onset of acute abdominal pain which lasts usually less than 2 hours due to immediate sealing effect of the perforation.
CHRONIC PERFORATION:
10 PEPTIC ULCER DISEASE
It includes
Gastric ulcer
Duodenal ulcer
It refers to the erosion in the gastric or duodenal mucosa. It may extend into the muscularis mucosa
Peptic ulcer disease most commonly presents with upper gastrointestinal hemorrhage. Bleeding is the principal cause of death in peptic ulcer disease. PATHOGENESIS:
The pathogenesis of peptic ulcer disease related to
Increase in Aggressive factors
Decrease in the Defensive factors AGGRESSIVE FACTORS INCLUDE
HCl secretion
Pepsin
Smoking
Alcohol
11
Ischemia
NSAID’s
Hypoxia
DEFENSIVE FACTORS INCLUDE:
Mucosal bicarbonate secretion
Mucus production
Blood flow
Cell renewal
Growth factors
Endogenous prostaglandins
HELICOBACTER PYLORI:
It is a spiral shaped gram negative microaerophilic bacilli.
H.pylori resides in the Gastric epithelium, underneath the mucosa layer. It can live in gastric epithelium since it posses the adherence receptors. Other than gastric mucosa, H.pylori may be found in sites with heterotopic gastric mucosa. They include:
Proximal esophagus
12
Gastric metaplasia in duodenum
Meckel’s diverticulum
Rectum
The bacteria grows well at 37° C in microaerophilic conditions
Medium used for bacterial culture include – Skirrow’s medium, Chocolate agar
Biochemical reactions- catalase +ve, oxidase +ve, urease +ve
Virulence factors include – Vac A cytotoxin, Group of gene CagPAI
MECHANISM BY WHICH H.PYLORI INDUCES GI INJURY:
1. Production of toxin products:
Urea broken down to ammonia and bicarbonate
Cytotoxins
Phospholipases
2. Induction of local immune response
3. Increase gastric acid levels and gastric metaplasia in duodenum
4. Interruption of inhibiting vagal reflexes
13 H.pylori associated with:
About 85-90% of duodenal ulcer
75% of Gastric ulcer
Increased risk of Gastric Adenoma and Gastric MALToma
CAG-A positive strain leads to Squamous cell carcinoma of Esophagus, but protective for Adenocarcinoma of Esophagus
H.PYLORI DISEASE MANIFESTATION:
Antral predominant Gastritis- Duodenal ulcer
Atrophic Gastritis – Gastric ulcer, Gastric Adenocarcinoma
Non atrophic Chronic superficial Gastritis – Gastric MALToma
DIAGNOSIS:
1. Gold standard/ Diagnostic for H.pylori – Histologic investigation Stains used – Silver, Giemsa, Warthin starry
2. Rapid urease test 3. Serology
14 NON-INVASIVE TESTS:
Urea breath test
Stool Antigen test
Serological Assay
INVASIVE TESTS:
Endoscopy and Biopsy
TREATMENT:
The treatment for H.pylori includes:
H.Pylori eradication
Reduce gastric acid secretion
Increase mucosal protective barrier function
1. ANTACIDS - Decrease gastric acidity by reaction with Gastric Hcl – leading to Salt formation and increase Gastric pH
2. SUCRALFATE – It is aluminium salt of sulphated sucrose. It polymerises and binds to protein in the ulcer. A protective coating is formed and it lasts for about 6 hours
3. H2 RECEPTOR ANTAGONISTS – Famotidine is the most potent H2 blocker
15 TRIPLE THERAPY:
Proton Pump Inhibitors and ANTIBIOTICS - usually Amoxicillin 1 gm bid or Clarithromycin 500 mg bid. If allergic to penicillin, Metronidazole 500mg bid used.
MANAGEMENT FOR H.PYLORI INDUCED COMPLICATIONS:
Peptic ulcer disease – Parietal cell vagotomy with or without Antrectomy
Bleeding – Oversewing of bleeding vessel with H.pylori treatment
Perforation – Patch closure with H.pylori treatment
Obstruction- To rule out malignancy and if required, Gastrojejunostomy with H.pylori treatment
GASTRIC ULCER:
Gastric ulcer refers to the erosion in the lining of the gastric mucosa leading to ulcer formation.
ETIOLOGY:
75% of gastric ulcers are associated with H.pylori infection
NSAID’s
Smoking
16
Low socio-economic status
Atrophic gastritis
Duodenogastric bile reflux
Gastric stasis
[image:25.595.110.554.310.642.2] Any abnormality in acid and pepsin secretion.
17
Incidence is equal in both male and female. Nowadays incidence is becoming more common among females. Peak incidence is in the age group of 55-60 years. Acid will be ulcerogenic even to the normal gastric mucosa and these patients usually associated with normochlorhydria or hypochlorhydria.
Most common site of gastric ulcer is lesser curvature along the Incisura angularis. Ulcer of size more than 3 cm is called as giant gastric ulcer.
MODIFIED JOHNSON’S CLASSIFICATION OF GASTRIC ULCER
TYPE OF GASTRIC ULCER
LOCATION ACID
SECRETION MANAGEMENT I Lesser curvature Low Distal Gastrectomy with
reconstruction II Body of stomach and
duodenum
High Truncal vagotomy/ Antrectomy
III Prepyloric High Truncal Vagotomy/
Antrectomy
IV High on lesser curvature Normal Schoemaker’s procedure Pouchet’s procedure Keley- Medlener Csendes procedure
18
Fig 2: Types of gastric ulcer.
CLINICAL PRESENTATION:
Pain in the epigastrium after taking food, relieved by vomiting
Loss of appetite
Loss of weight
Hemetemesis/ Malena
19
CHARACTERISTIC OF GASTRIC ULCER:
BENIGN MALIGNANT
Less common Most common
Smooth radiating folds with Hampton line of collar
Interrupted nodular/clubbed folds with Lasman Kirklin complex
Overhanging margins Eccentric with everted margins
Penetrating sign Carman meniscus sign
Huge base Necrotic base
Preserved peristalsis No peristalsis
Heals in 8 –10 weeks No healing
INVESTIGATION:
Endoscopy helps in direct visualisation of gastric ulcer. Biopsy from the ulcer can be taken to rule out malignancy
Barium meal shows–
o Niche in lesser curvature / Notch on Greater curvature
o Spoke wheel pattern
o Overhanging mucosa with Hampton’s line
20
COMPLICATIONS OF GASTRIC ULCER:
Perforation- most commonly into the Lesser sac
Hour glass contracture
Tea-pot stomach
Malignant transformation
DUODENAL ULCER ETIOLOGY:
85-90% of duodenal ulcers associated with H.pylori infection
Anxiety and Stress
Steroids
NSAID’s
Smoking
Alcohol
O+ve blood group
Vitamin deficiencies
Endocrine disorders – Zollinger Ellison Syndrome, MEN-I, Cushing’s syndrome
Hyperparathyroidism
Incidence – most common in males than females Most common site of ulcer – First part of duodenum
21
Fig 3: Picture showing perforated duodenal ulcer.
CLINICAL FEATURES:
Abdomen pain - most commonly in the early morning, pain decreases after food intake
Pain common during night
Malena
Good appetite
22 INVESTIGATIONS:
Upper GI Radiology – Barium meal shows deformed Duodenal Cap (due to spasm), Appearance of infoliate duodenum due to surrounding Duodenal diverticula
Flexible upper GI endoscopy – Most valuable method for Diagnosis H.pylori testing – Invasive / Non- invasive
COMPLICATION OF DUODENAL ULCER:
Bleeding – Most commonly in the posterior wall – Gastroduodenal Artery
Perforation – Most commonly in the anterior wall CLINICAL FEATURES OF PERITONITIS:
The most common presenting symptom is the sudden onset of abdominal pain, more intense in the epigastric region. The pain may be radiated to scapula or lower abdomen region
Abdominal distension
Guarding and rigidity of abdominal muscle
Decreased bowel sounds
Low grade fever
23
Hypotension and Tachycardia
Decreased urine output
Obliteration of liver dullness LAB INVESTIGATIONS:
1. Complete blood count – Leucocytosis with shift to left
2. Chest X ray /Abdomen Xray erect – reveals evidence of free air 3. Usg abdomen and pelvis
[image:32.595.126.508.362.703.2]4. CT scan – rarely required
24 TREATMENT APPROACH:
Perforated peritonitis due to peptic ulcer disease is usually managed by emergency surgery. In certain patients who presents with sealed perforation and without pneumoperitoneum can be managed non operatively. Non operative management is not generally adopted and has been restricted to patients who are unfit for undergoing emergency laparotomy.
NON OPERATIVE MANAGEMENT INCLUDES:
Nasogastric tube decompression
Fluid resuscitation
Proton pump inhibitors
Broad spectrum antibiotics
Serial abdominal examination
Subsequent endoscopy
H.pylori treatment
Non operative management should not be done in patients with
Failure of symptoms improvement after12-24 hours
Peritoneal sepsis
Increasing abdomen tenderness
25
PERFORATED PEPTIC ULCER
PERITONITIS PRESENT LOCALIZED PAIN
NO GENERALIZED PERITONITIS
CARDIOVASCULAR RADIOGRAPH WITH ORAL OR NG TUBE,
STABILITY WATER SOLUBLE CONTRAST
EMERGENCY NON CONTAINED CONTAINED
LAPAROTOMY PERFORATION PERFORATION
NON OPERATIVE
OMENTAL PATCH SURGERY IV FLUIDS & ANTIBIOTICS
NG TUBE
26 OPERATIVE MANAGEMENT
GRAHAM’S PATCH CLOSURE:
It is the simple method of closure of perforated duodenal ulcer by three absorbable sutures on interrupted fashion through the ulcer and a part of omentum is placed in order to produce sealing effect.
Abdomen is opened by vertical midline laparotomy incision. Peritoneal cavity entered. Free fluid in the peritoneal cavity is aspirated and 10 ml of fluid is taken for culture and sensitivity. Visualization of stomach, small intestines, ileocaecal junction, appendix, large intestines done. Solid organs visualized. Perforation identified. Peritoneal lavage is done using 3 litres of warm normal saline.
Primay closure of the perforation is done by taking full thickness stitches from the stomach or duodenal wall 1 cm away from the edge of perforation. Usually 3 to 4 stay stitches taken and then primary closure of the perforation is done. Live omental patch kept over the site and secured.
27
Fig 5: Abdomen painted and draped
[image:36.595.213.458.410.699.2]28
Fig 7: Picture showing preperitoneal fat bulging through rectus sheath
[image:37.595.114.560.445.701.2]29
Fig 9: Peritoneal wash being given
[image:38.595.123.561.453.696.2]30
Fig 11: Picture showing primary closure of perforation
[image:39.595.147.537.454.735.2]31
Fig 13: Bilateral tube drain kept
[image:40.595.203.429.455.696.2]32
Fig 15: Skin closed with staplers
DEFINITIVE PROCEDURES:
Definitive procedures are usually not done in emergency setup, but if the patient has minimal upper abdominal contamination, hemodynamically stable and doubtful compliance for medical therapy definitive procedures can be done.
Large perforation >2cm – may require thal’s patch or rarely Vagotomy, Antrectomy, Billroth II reconstruction
33 Those patients who had
Chronic ulcer symptoms- H.pylori negative
NSAID’s dependent
Previous H.pylori treatment failure
Previous ulcer complications These patients may require
Patch closure
Parietal cell vagotomy
Pyloroplasty
Ulcer excision
OUTCOME AND PROGRESSION: Factors affecting prognosis include
Patient in shock at the time of admission
Delay in initiation of surgery >12 hours of presentation
>70 years of age
Cirrhosis
Concurrent medical illness
34 JABALPUR SCORING SYSTEM
Jabalpur scoring system developed by Mishra et al at Jabalpur district of Madhya Pradesh. This study was formulated for easy analysis of prognosis of patients diagnosed with perforation peritonitis for developing nations. It initially encompassed 10 factors of these 6 parameters were taken ideally as Jabalpur peritonitis index.
The factors that were incorporated into this study are easily obtainable that doesn’t involve time consuming investigations make this scoring system an easily applicable one. The initial data are collected from patients during their hospital admission. After obtaining thorough and complete physical examination and systematic examination patients were subjected to routine investigation along with x–ray abdomen, chest x-ray and ultrasound abdomen. Prior consent is mandatory before subjecting them to all investigations and surgical procedures. The parameters that are included in this study are,
PERFORATION OPERATION INTERVAL:
35 MEAN SYSTOLIC BLOOD PRESSURE:
The second parameter that is taken into consideration is preoperative mean systolic blood pressure with score of 0 of 70-109 mmHg the next score skips 1 to land at 2 that ideally involves both ends of spectrum with mean systolic pressure of 50- 69/110-129, Score 3 is given to systolic of 130-159 and Score 4 to BP less than 49 and more than 160 mmhg.
HEART RATE:
The third parameter is heart rate that ranges from 0/70-109 BPM to score 2 that includes rate from 55-69/110-139/score 3 of rate 40-54/140-179 and finally score4 of heart rate less than 39 or more than 180 BPM
SERUM CREATININE:
The next parameter is serum creatinine which is obtained by lab investigations. It also ranges from score 0 including values of 0.6-1.4, score 2 that includes values of 1.5-1.9, score 3 that incorporates values from 2.0-3.4 and finally score of 4 for all the values above 3.5.
AGE:
36 COMORBID ILLNESS:
Co-morbid illness is incorporated along with age. A score of 5 is given for age if the patient has any co-morbid illness.
The co-morbid illnesses considered in this study are,
diabetes mellitus,
systemic hypertension,
bronchial asthma,
liver dysfunction,
coronary artery disease,
seizure disorder,
chronic kidney disease,
Thyroid disorder.
37
JABALPUR PROGNOSTIC SCORING SYSTEM FOR PEPTIC PERFORATION
FACTOR
SCORE
0 1 2 3 4 5 6
P-0 Interval
(Hours) < 24 25-72 73 – 96 97-120 > 120 - - Mean Systolic
BP (mmHg) 70 - 109 -
50 - 69 or
110 – 129 130 – 159
< 49 or
> 160 - -
Heart Rate (Per
Minute) 70 - 109 -
55 - 69 or 110 – 139
40 – 54 or 140 – 179
< 39 or
>180 - -
Serum Creatinine
(mg/dl)
0.6 - 1.4 - 1.5 - 1.9 2.0 – 3.4 > 3.5 - -
Age* (Years) < 45 - 45 – 54 55 - 64 - 65 - 74 75 or more
38 OUTCOME MEASUREMENTS: MORTALITY:
Mortality is considered as death in the hospital during the same admission of perforative peritonitis.
MORBIDITY:
Various morbidities that can occur are
Superficial wound infection
Complete wound dehiscence
Septic shock
Peritoneal abscess
Acute respiratory distress syndrome
Acute kidney injury
Enterocutaneous fistula due to leak
Multiorgan dysfunction
VARIOUS SCORING SYSTEM FOR PERITONITIS: POSSUM SCORE:
39
ACUTE PHYSIOLOGICAL AND CHRONIC HEALTH EVALUATION (APACHE II) SIMPLIFIED ACUTE PHYSIOLOGY SCORE.
It comprises of parameters like age , health rate, systolic blood pressure , temperature , GCS , mechanical ventilation / CPAP, PaO, FiO2, urine output, BUN, sodium ,potassium, bicarbonate bilirubin white blood cell, chronic diseases, Type of admission It is an ICU scoring system that is used in predicting morbidity and mortality of patients.
MANHAEIM PERITONITIS INDEX :
Developed by wacha and linder in 1983 based on retrospective analysis of data. Patients can have maximum score of 47 with score exceeding 26 are said to be having high mortality rate. Factors included are age, duration of peritonitis, organ failure, diffuse peritonitis, site of perforation, level of exudates in peritoneal fluid
THE SEPSIS SCORE:
40 BOEY SCORE:
This is one of the scores that is easily available in clinical practice parameters like concomitant medical illness , preoperative shock ( SBP <90mmhg) duration of perforation more than 24 hours are included scores ranging from 0-3.
CHARLSON COMORBIDITY INDEX:
It predicts ten years mortality of patients who may have range of total 22 co-morbid conditions. This index is incorporated into parametric study of peritonitis and influences that effect of these conditions in predicting the mortality and morbidity of the diesease.
HACETTEPE SCORE:
Predicts 30 days mortality in patients in PPU and it includes serious medical illness, acute renal failure, WBC count, male gender as prognostic factors.
PULP II SCORE:
41
METHODOLOGY
STUDY DESIGN:
Prospective cohort study
PLACE WHERE STUDY CONDUCTED:
Department of general surgery
Coimbatore medical college and hospital
STUDY PERIOD:
July 2017 to July 2018
STUDY POPULATION:
Patients came to emergency department and admitted with acute abdominal pain whose clinical symptoms and investigations leads to the diagnosis of perforative peritonitis and all the patients underwent emergency laparotomy.
SAMPLE SIZE:
42 INCLUSION CRITERIA:
Patients above the age of 18.
Patients undergoing emergency laparotomy with features of peritonitis due to peptic ulcer perforation.
EXCLUSION CRITERIA:
Patient less than age of 18.
Pregnant patients.
Psychiatric patients.
Patients with HIV and TB.
PRE – OPERATIVE EVALUATION:
43 PREOPERATIVE PREPARATION:
Patients who were diagnosed as case of perforative peritonitis and planned for emergency laparotomy were put on nil per oral as soon as the patient received in emergency department. Intravenous catheterization done and fluid resuscitation given. Nasogastric tube aspiration and Foleys catheterization done. Preoperative Intravenous antibiotics, antacids were given 1 hour before the surgery.
ANESTHESIA: General anesthesia.
POSITION: Supine position.
OPERATIVE PROCEDURE:
44 POSTOPERATIVE CARE:
After surgery patient is shifted to surgical intensive care unit or post anesthetic care unit for close monitoring of vitals and early detection of complications and its intensive management. Patient kept on nil per oral till the bowel motility returns which was assessed by auscultating bowel sounds and history of passing flatus and stools postoperatively. Patients were given intravenous fluids, antibiotics, analgesics, antacids. Input output monitoring done. Early ambulation done. Patient started on oral diet once the bowel motility returns. Drain removal done 24 hrs after the patient is on oral diet. Patient on discharge is advised to take anti helicobacter pylori kit.
FOLLOW UP:
Follow up were done at 10th day,1 month and 3 months post laparotomy.
LIMITATIONS:
45
OBSERVATION AND ANALYSIS
OBSERVATION:
Patients presented with acute abdominal pain in emergency evaluated to have perforative peritonitis due to peptic ulcer perforation. All the patients underwent emergency laparotomy for the same. All the parameters were noted and Jabalpur score calculated preoperatively and the outcome of the patient observed postoperatively.
ANALYSIS:
SEX WISE DISTRIBUTION:
The incidence is more common in males than females. In our study, males comprised 96% of the study population and the females comprise only 2% of the study population.
TABLE 1: SEX FREQUENCY TABLE
SEX NO.OF PATIENTS PERCENTAGE
Male 48 96.0
Female 2 4.0
46
TABLE 2: SEX DISTRIBUTION
PATIENTS CURED EXPIRED
MALE 41 7
FEMALE 1 1
Fig 16: PIE CHART FOR SEX DISTRIBUTION
47 SITE OF PERFORATION:
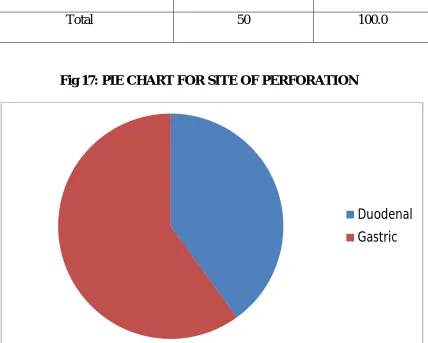
In our study, 60% of the patients had perforation in the stomach that too in the pyloric region of the stomach and the remaining 40% of the patients had perforation in the first part of duodenum.
TABLE 3: SITE OF PERFORATION
SITE OF PERFORATION NO.OF PATIENTS PERCENTAGE
Duodenal 20 40.0
Gastric 30 60.0
[image:56.595.107.535.331.674.2]Total 50 100.0
Fig 17: PIE CHART FOR SITE OF PERFORATION
48 AGE DISTRIBUTION:
In our study group, 64% of the patients are less than 45 years of age and 36% of the patients are more than 45 years of age. The mortality increases with increase in age group. In less than 45 years the mortality rate is 6.25% and the mortality rate is 33.33% in patients more than 45 years. In patients more than age of 65 the mortality rate raises to 60%.
TABLE 4: AGE FREQUENCY TABLE
AGE NO.OF PATIENTS PERCENTAGE
Below 45yrs 32 64.0
45 to 54yrs 6 12.0
55 to 64yrs 7 14.0
65 to 74yrs 5 10.0
49
TABLE 5: AGE WISE DISTRIBUTION
AGE CURED EXPIRED TOTAL
<45 30 2 32
45-54 4 2 6
55-64 6 1 7
65-74 2 3 5
>75 NIL NIL NIL
Fig 18: BAR CHART FOR AGE WISE DISTRIBUTION
0 8 15 23 30 38
<45 45-54 55-64 65-74 >75
[image:58.595.106.539.338.653.2]50 HEART RATE:
In our study, 68% of the patients at the time of presentation have heart rate between 70 to 109 beats/min and the remaining 38% of the patient have heart rate between 110 to 139 beats/min. The mortality rate increases with increase in heart rate. Here, the patients having heart rate between 110 to 139/min has a mortality rate of 50%.
TABLE 6: HEART RATE FREQUENCY TABLE
HEART RATE NO. OF PATIENTS PERCENTAGE
70 to 109 34 68.0
110 to 139 16 32.0
51
TABLE 7: RELATIONSHIP BETWEEN HEART RATE AND OUTCOME
HEART RATE CURED EXPIRED TOTAL
50-69 NIL NIL NIL
70-109 34 NIL 34
110-139 8 8 16
Fig 19: BAR CHART SHOWING RELATIONSHIP BETWEEN HEART RATE AND OUTCOME
0 10 20 30 40
50-69 70-109 110-139
52
PERFORATION – OPERATION INTERVAL:
In our study, 66% of the patients get admitted with perforation – operation interval between 1 to 3 days. Mortality increases with increase in perforation to operation interval. 70% mortality is seen in the study group if the perforation to operation interval is ≥ 4 days.
TABLE 8: P – O INTERVAL FREQUENCY TABLE
P-O INTERVAL NO. OF PATIENTS PERCENTAGE
<1day 7 14.0
1 to 3days 33 66.0
3 to 4days 8 16.0
>4days 2 4.0
53
TABLE 9: RELATIONSHIP BETWEEN P- O INTERVAL AND OUTCOME
P-O INTERVAL CURED EXPIRED TOTAL
< 1 DAY 7 NIL 7
1-3 DAYS 32 1 33
≥ 4 DAYS 3 7 10
Fig 20: BAR CHART SHOWING RELATIONSHIP BETWEEN P- O INTERVAL AND OUTCOME
0 10 20 30 40
< 1 DAY 1 - 3 DAYS ≥ 4 DAYS
54 MEAN SYSTOLIC BLOOD PRESSURE:
In our study, about 72% of the patients presented with mean systolic blood pressure of 70 to 109 mm Hg, 18% of the patients presented with mean systolic blood pressure of 50 to 69 mm Hg and the remaining 10% of the patients has mean systolic blood pressure of 110 to 129 mm Hg. The mortality is high when the patient has hypotension at the time of presentation.
TABLE 10: MEAN SBP FREQUENCY TABLE
MEAN SYSTOLIC BP NO.OF PATIENTS PERCENTAGE
50 to 69 9 18.0
70 to 109 36 72.0
110 to 129 5 10.0
55
TABLE 11: RELATIONSHIP BETWEEN MEAN SYSTOLIC BLOOD PRESSURE AND OUTCOME
MEAN SYSTOLIC BP CURED EXPIRED TOTAL
50-69 4 5 9
70-109 33 3 36
110-129 5 NIL 5
130-159 NIL NIL NIL
Fig 21: BAR CHART SHOWING RELATIONSHIP BETWEEN MEAN SYSTOLIC BLOOD PRESSURE AND OUTCOME
0 10 20 30 40
50 - 69 70 - 109 110 - 129 130 - 159
56 SERUM CREATININE:
In our study group, serum creatinine is measured once the patient gets admitted. 32% of the patients had serum creatinine value between 0.6 to 1.4 and 36% of the patients had serum creatinine value between 2.0 to 3.4. Mortality increases with increase in serum creatinine value.
TABLE 12: SERUM CREATININE FREQUENCY TABLE
SERUM CREATININE NO.OF PATIENTS PERCENTAGE
0.6 to 1.4 16 32.0
1.5 to 1.9 11 22.0
2.0 to 3.4 18 36.0
Above 3.5 5 10.0
57
TABLE 13: RELATIONSHIP BETWEEN SERUM CREATININE AND OUTCOME
SERUM CREATININE CURED EXPIRED TOTAL
0.6-1.4 16 NIL 16
1.5-1.9 11 NIL 11
2.0-3.4 14 4 18
Fig 22: BAR CHART SHOWING RELATIONSHIP BETWEEN SERUM CREATININE AND OUTCOME
0 4 8 12 16 20
0.6 - 1.4 1.5 - 1.9 2.0 - 3.4 > 3.5
58 CO MORBID ILLNESS :
[image:67.595.113.546.383.680.2]In our study, only 16% of the study population had co morbidites. Remaining 84% of the study population doesnot have any co morbidities.
TABLE 14: COMORBID ILLNESS
CO MORBIDITY NO.OF PATIENTS PERCENTAGE
Yes 8 16.0
No 42 84.0
Total 50 100.0
Fig 23: PIE CHART SHOWING DISTRIBUTION OF CO MORBID ILLNESS
59
TABLE 15: RELATIONSHIP BETWEEN CO MORBID ILLNESS AND MORTALITY
CO MORBIDITY NO.OF PATIENTS MORTALITY
Yes 8 3
No 42 5
Total 50 8
Fig 24: BAR CHART SHOWING RELATIONSHIP BETWEEN CO MORBID ILLNESS AND MORTALITY
0 5 10 15 20 25 30 35 40 45
Yes No
60
TABLE 16: RELATIONSHIP BETWEEN CO MORBIDITY AND MORBIDITY
CO MORBIDITY NO.OF PATIENTS MORBIDITY
Yes 8 5
No 42 12
Total 50 8
Fig 25: BAR CHART SHOWING RELATIONSHIP BETWEEN CO MORBIDITY AND MORBIDITY
0 5 10 15 20 25 30 35 40 45
Yes No
61 JABALPUR SCORE:
Jabalpur score is obtained by summation of marks obtained in each factors such as age, co morbid illness, heart rate, mean systolic blood pressure, serum creatinine, perforation – operation interval. 46% of the patients have jabalpur score ≤4. 26% of the patients have jabalpur score between 5 and 9. 28% of the patients have jabalpur score >9. No patients died who had score between 0 and 4 and 100% mortality if patient had score more than 14.
TABLE 17: JABALPUR SCORE FOR MORTALITY
JABALPUR SCORE CURED EXPIRED TOTAL
0-4 23 NIL 23
5-9 12 1 13
10-14 7 3 10
62
Fig 26: RELATIONSHIP BETWEEN JABALPUR SCORE AND MORTALITY
MORBIDITY:
In our study, out of 50 patients 17 patients had developed complications. Out of which some patient had more than one complication. Out of 14 patients who had Jabalpur score >9 11 patients developed complications. 6 patients had developed complications out of 36 patients who had score <9. Superficial wound infection was developed by 7 patients. Multiple organ dysfunction syndrome was developed by 5 patients. Acute kidney injury was developed by 10 patients. ARDS was developed by 3 patients.
0 8 15 23 30
0 to 4 5 to 9 10 to 14 15 to 21
63
TABLE 18: JABALPUR SCORE FOR MORBIDITY
JABALPUR SCORE NO
MORBIDITY MORBIDITY TOTAL
0-4 21 2 23
5-9 9 4 13
10-14 3 7 10
15-21 NIL 4 4
Fig 27: BAR CHART SHOWING RELATIONSHIP BETWEEN JABALPUR SCORE AND MORBIDITY
0 5 10 15 20 25
0 to 4 5 to 9 10 to 14 15 to 21
64
RELATIONSHIP OF JABALPUR PROGNOSTIC SCORING SYSTEM WITH MORBIDITY AND MORTALITY
Among the 23 patients who had Jabalpur score between 0 and 4 only 2 patients develop morbidity and there were no mortality.13 patients have scored between 5 and 9 among that 1 patient expired and 4 patients develop morbidity.10 patients have score between 10 and 14 among which 7 patients develop morbidity and 3 patients died. 4 patients scored above 14 and all the patients have both morbidity and mortality.
TABLE 19: RELATIONSHIP OF JABALPUR SCORING SYSTEM WITH MORBIDITY AND MORTALITY
SCORE ( RANGE )
NO. OF PATIENTS
MORBIDITY (n{%})
MORTALITY (n{%})
0 – 4 23 2 -
5 – 9 13 4 1
10 – 14 10 7 3
65
STATISTICS
SENSITIVITY:
Sensitivity is the ability to identify correctly all the true positives. Cut off score is considered as 9 for calculating sensitivity and specificity.
TABLE 20: SENSITIVITY AND SPECIFICITY OF JABALPUR PROGNOSTIC SCORE 9 FOR MORTALITY
JABALPUR
PROGNOSTIC SCORE EXPIRED CURED TOTAL
>9 7 7 14
<9 1 35 36
=
+ 100
= 7
7 + 1 100
= 87.5%
66 SPECIFICITY:
Specificity is the ability to identify correctly all the true negatives.
SENSITIVITY = True Negative
True Negative + False Positive x 100
SENSITIVITY = 35
35 + 7 x 100
= 83.33%
Specificity of Jabalpur score in predicting the mortality is 83.33%.
POSITIVE PREDICTIVE VALUE:
Ability of Jabalpur score to identify correctly all those who expired, out of all those who have increased Jabalpur Score
Positive Predictive Value = True Positive
True Positive + False Positive x 100
SENSITIVITY = 7
7 + 7 x 100
= 50%
67 NEGATIVE PREDICTIVE VALUE:
Ability of Jabalpur score to identify correctly all those who expired, out of all those who have low Jabalpur Score
Negative Predictive Value = True Negative
True Negative + False Negative x 100
SENSITIVITY = 35
1 + 25 x 100
= 97.2%
NEGATIVE PREDICTIVE VALUE of Jabalpur score is 97.2 %
PERCENTAGE OF FASLE POSITIVE:
% False Positive = False Positive
False Positive + True Negative x 100
SENSITIVITY = 7
7 + 25 x 100
= 16.6%
68 PERCENTAGE OF FASLE NEGATIVE:
% =
+ 100
= 1
7 + 7 100
= 12.5%
% FALSE NEGATIVE of Jabalpur score is 12.5%.
DESCRIPTIVE STATISTICS
In our study, statistical analysis of each parameter is done. Since, perforation operation interval is calculated in range descriptive statistics could not be done. As age is considered, the lowest age of the patient who presented with perforative peritonitis is 18 and the highest age is 80. Mean value of age is 40.5 and the standard deviation is 15.2.
69
TABLE 21: DESCRIPTIVE STATISTICS FOR EACH PARAMETER MIN. MAX. MEAN S.D
AGE 18 70 40.50 15.236
MEAN SBP 60 114 86.68 14.505
HR 80 124 102.52 10.332
Sr.CREATININE .80 3.80 2.0000 .85762
JABALPUR SCORE 0 16 5.88 4.628
In our study, the lowest heart rate of the patient who presented with perforative peritonitis is 80beats/min and the highest heart rate is 124beats/min. The mean value is 102.5 and the standard deviation is 10.3.
In our study, the lowest value of serum creatinine of the patient who presented with perforative peritonitis is 0.8 mg/dl and the highest heart rate is 3.80 mg/dl. The mean value is 2.0 and the standard deviation is 0.8.
70 AGE:
[image:79.595.102.533.369.626.2]On statistical analysis of the parameter age in our study group 25% (2 patients) of the patient expired are below the age of 45 and the remaining 75% (6 patients) of the patients died are above 45 years. 71.4% of the patients are cured who are below 45 years of the age and only 28.6% who are above 45 years of age are cured. On application of chi square test and t test p value is found to be <0.05 and age is independently significant parameter for predicting the mortality and morbidity of the perforative peritonitis patient.
TABLE 22: CHI-SQUARE TEST FOR AGE
AGE
OUTCOME
STATISTICAL INFERENCE CURED EXPIRED TOTAL
n % N % N %
Below 45yrs 30 71.4% 2 25.0% 32 64.0%
X2=10.822 Df=3 .013<0.05 Significant 45 to 54yrs 4 9.5% 2 25.0% 6 12.0%
71
TABLE 23: T TEST FOR AGE
AGE N MEAN S.D
STATISTICAL INFERENCE
Cured 42 37.79 14.070 T=-3.136 Df=48
.003<0.05 Significant
Expired 8 54.75 13.750
SEX:
In our study, sex of the patient is statistically insignificant in predicting the outcome.
TABLE 24: CHI-SQUARE TEST FOR SEX
SEX
OUTCOME
STATISTICAL INFERENCE CURED EXPIRED TOTAL
n % n % n %
Male 41 97.6% 7 87.5% 48 96.0% X2=1.792 Df=1 .181>0.05 Not Significant
Female 1 2.4% 1 12.5% 2 4.0%
72 SITE OF PERFORATION:
Site of perforation is statistically insignificant in predicting the mortality and morbidity. P value is 0.08 which is greater than 0.05.
TABLE 25: CHI-SQUARE TEST FOR SITE OF PERFORATION
SITE OF PERFO-RATION
OUTCOME
STATISTICAL INFERENCE CURED EXPIRED TOTAL
N % n % n %
Duodenal 19 45.2% 1 12.5% 20 40.0% X2=3.001 Df=1 .083>0.05 Not Significant Gastric 23 54.8% 7 87.5% 30 60.0%
73 CO MORBID ILLNESS:
In our study, among expired patients 37.5% of the patients have co morbidities and 62.5% of the patient does not have any co morbidities. Among cured patients 11.9% of the patients have co morbidities and the remaining 88.1% does not have any co morbidities. Statistically co morbid illness is not significant in predicting the outcome since the P value is 0.07 (>0.05).
TABLE 26: CHI-SQUARE TEST FOR CO MORBID ILLNESS
CO-MOR-BIDILLNESS
OUTCOME
STATISTICAL INFERENCE CURED EXPIRED TOTAL
N % n % N %
Yes 5 11.9% 3 37.5% 8 16.0% X2=3.276 Df=1 .070>0.05 Not Significant
No 37 88.1% 5 62.5% 42 84.0%
74
PERFORATION OPERATION INTERVAL:
[image:83.595.89.545.474.720.2]In our study, patients with Perforation operation interval <1 day had no mortality and <3 days had 3.1% mortality rate and p – o interval between 3 – 4 days had mortality rate of 60% and with p – o interval >4 days had 100% mortality rate. Among cured patients 82.9% patients had p – o interval <3 days and 7.9% patients had p – o interval above 3 days. Among expired patients 87.5% patients had p – o interval greater than 3 days and the remaining 12.5% hand p – o interval less than 3 days. Perforation operation interval is statistically significant independently since the p value is < 0.05. T test could not be done as it is calculated in range.
TABLE 27: CHI-SQUARE TEST FOR PERFORATION OPERATION INTERVAL
P-O INTER-VAL
OUTCOME STATISTICAL
INFERENCE CURED EXPIRED TOTAL
n % n % N %
X2=29.834 Df=3 .000<0.05 Significant
<1day 7 16.7% 0 .0% 7 14.0%
1 to 3days 32 76.2% 1 12.5% 33 66.0% 3 to 4days 3 7.1% 5 62.5% 8 16.0%
>4days 0 .0% 2 25.0% 2 4.0%
75 MEAN SYSTOLIC BLOOD PRESSURE:
[image:84.595.103.529.324.543.2]In our study, among cured ones 78.6% of the patients have mean systolic between 70 to 109 mm Hg. 9.5% of the patients have mean systolic blood pressure between 50 to 69 mm Hg and 11.9% of the patients have mean systolic blood pressure between 110 t0 129 mm Hg.
TABLE 28: CHI-SQUARE TEST FOR MEAN SYSTOLIC BLOOD PRESSURE
MEAN SBP
OUTCOME
STATISTICAL INFERENCE CURED EXPIRED TOTAL
N % n % n %
50 to 69 4 9.5% 5 62.5% 9 18.0%
X2=13.004 Df=2 .002<0.05 Significant 70 to 109 33 78.6% 3 37.5% 36 72.0%
110 to 129 5 11.9% 0 .0% 5 10.0% Total 42 100.0% 8 100.0% 50 100.0%
76
TABLE 29: T TEST FOR MEAN SYSTOLIC BLOOD PRESSURE
MEAN SBP N MEAN S.D
STATISTICAL INFERENCE
Cured 42 90.38 12.464 T=5.070 Df=48
.000<0.05 Significant
Expired 8 67.25 7.005
HEART RATE:
In our study, among cured patients 89% of the patients have heart rate between 70 to 109 beats/ min and the remaining 19% of the patients have heart rate between 110 to 139 beats/min. All expired patients have heart rate between 110 to 139 beats/min. Chi square test and T test applied. P value identified and found to be less than 0.05. Hence, heart rate is independently significant and determine the outcome of the patient with perforative peritonitis.
TABLE 30: CHI-SQUARE TEST FOR HEART RATE
HR
OUTCOME
STATISTICAL INFERENCE CURED EXPIRED TOTAL
n % n % N %
70 to 109 34 81.0% 0 .0% 34 68.0% X2=20.238 Df=1 .000<0.05 Significant 110 to 139 8 19.0% 8 100.0% 16 32.0%
77
TABLE 31: T TEST FOR HEART RATE
HR N MEAN S.D
STATISTICAL INFERENCE
Cured 42 99.67 8.496 T=-5.759 Df=48
.000<0.05 Significant Expired 8 117.50 4.375
SERUM CREATININE:
Among cured patients, 38.1% of the patients have serum creatinine value between 0.6 to 1.4 mg/dl, 26.2% of the patients have serum creatinine value between 1.5 to 1.9 mg/dl, 33.3% of the patients have serum creatinine value between 2.0 to 3.4 mg/dl and 2.4% of the patients have serum creatinine value above 3.5 mg/dl.
TABLE 32: CHI-SQUARE TEST FOR SERUM CREATININE
Sr. CREATININE
OUTCOME
STATISTICAL INFERENCE CURED EXPIRED TOTAL
N % n % N %
0.6 to 1.4 16 38.1% 0 .0% 16 32.0%
X2=20.899 Df=3 .000<0.05 Significant 1.5 to 1.9 11 26.2% 0 .0% 11 22.0%
78
There was no mortality when the serum creatinine value is less than 2.0 mg/dl. 50% of the expired patients have serum creatinine value between 2.0 to 3.4 mg/dl and remaining 50% of the patients have value greater than 3.5 mg/dl. Chi square test and T test applied. P value found to be less than 0.05. Statistical significance of serum creatinine in predicting the outcome is identified.
TABLE 33: T TEST FOR SERUM CREATININE
Sr.CREATININE N MEAN S.D
STATISTICAL INFERENCE
Cured 42 1.7452 .65563 T=-6.560 Df=48
.000<0.05 Significant
Expired 8 3.3375 .44381
JABALPUR SCORE:
Among cured patients 83.4% of the patients have Jabalpur score less than 9 in which 54.8% of the patient have Jabalpur score between 0 and 4. And the remaining 16.6% of the cured patients have score between 10 and 14. No patients who are cured does not have score more than 14.
79
Among expired patients 50% have Jabalpur score more than 15. Statistical analysis done using chi square and T test. P value is less than 0.05. Jabalpur score is statistically significant in predicting the mortality and morbidity of the patients with perforative peritonitis.
TABLE 35: CHI-SQUARE TEST FOR JABALPUR SCORE
JABALPUR SCORE
OUTCOME
STATISTICAL INFERENCE CURED EXPIRED TOTAL
N % n % N %
0 to 4 23 54.8% 0 .0% 23 46.0%
X2=27.507 Df=3 .000<0.05 Significant 5 to 9 12 28.6% 1 12.5% 13 26.0%
10 to 14 7 16.6% 3 37.5% 10 20.0% 15 to 21 0 .0% 4 50.0% 4 8.0%
Total 42 100.0% 8 100.0% 50 100.0%
TABLE 35: T TEST FOR JABALPUR SCORE JABALPUR
SCORE
N MEAN S.D
STATISTICAL INFERENCE
Cured 42 4.60 3.676 T=-5.811 Df=48
.000<0.05 Significant
80
RELATIONSHIP BETWEEN MORBIDITY AND MORTALITY:
Out of 42 cured patients 10 (23.8%) of the patients have morbidity. 76.2% of the cured patients do not have any morbidity. 12.5% of the expired patients does not have any morbidity and the remaining 87.5% of the expired patients have morbidity. Chi square test done. P value is less than 0.05. Jabalpur score is statistically significant in predicting the morbidity and morbidity increases the mortality of the patients.
TABLE 36: CHI SQUARE TEST FOR MORBIDITY AND MORTALITY
MORBIDITY
OUTCOME
STATISTICAL INFERENCE CURED EXPIRED TOTAL
n % n % N %
Absent 32 76.2% 1 12.5% 33 66.0% X2=12.148 Df=1 .000<0.05 Significant Present 10 23.8% 7 87.5% 17 34.0%
81
ROC CURVE
CASE PROCESSING SUMMARY OUTCOME Valid N (listwise)
Positivea 8
Negative 42
Larger values of the test result variable(s) indicate stronger evidence for a positive actual state.
82
AREA UNDER THE CURVE
Test Result
Variable(s) Area
Std. Errora
Asymptotic Sig.b
Asymptotic 95% Confidence Interval
Lower Bound Upper Bound
AGE .814 .080 .005 .656 .972
MEAN SBP .061 .034 .000 .000 .127
HR .970 .022 .000 .927 1.000
Sr.CREATININE .973 .021 .000 .933 1.000
JABALPUR SCORE .951 .034 .000 .885 1.000
The test result variable(s): AGE, MEAN SBP, HR, Sr.CREATININE, JABALPUR SCORE has at least one tie between the positive actual state group and the negative actual state group. Statistics may be biased.
83
DISCUSSION
Perforative peritonitis is one of the challenging and demanding surgical emergency that requires immediate management which can be life saving at all situations. The emphasis on triaging the patients prior to management is aimed at significantly decreasing the morbidity and mortality of the patient.
All the patients undergoing this study were diagnosed with perforative peritonitis with proper radiological and clinical evidence. The study confirmed that this ideal scoring system improves the clinical efficiency in management. Though variety of scoring system has been proposed and devised for assessment of the severity, none of the scoring system is complete. Many scoring systems are complex. The parameters that are included in this study are easily obtainable and taken without delay in bringing out the score.
84
There were no death if the patient had perforation to operation interval less than 24 hrs and there is 100% mortality if the P – O interval is greater than 96 hrs. There were no deaths if Jabalpur score is less than 4 and 100% mortality if the score is above 14. All the parameters such as age, perforation operation interval, mean systolic blood pressure, serum creatinine and heart rate are independently and statisitically significant in predicting the mortality and morbidity of the patients with perforative peritonitis.
According to this score, one can plan their management and assess the complications that are anticipated along the treatment so that the overall survival improves. just because the score is low doesn’t necessarily mean they can be ignored or compromised in any way. The significant increase in score can lead to bad prognosis and acts as early marker for shifting the focus to such patients and active intervention.
Mishra et al studied 140 patients with perforative peritonitis the sensitivity is 87% and specificity is 85% that is more than any other scoring system applied for this specific study. Comparison of Jabalpur scoring system to other scoring systems in practice also proves it as an effectively favorable one. In country like India were one cannot expect sophisticated investigation to be readily available in time. Considering various factors the use of easily available parameters is the most promising reason for the success of this study.
85
CONCLUSION
86
BIBLIOGRAPHY
1. 1.Mishra A, Sharma D, Raina VK. A simplified prognostic scoring system for peptic ulcer perforation in developing countries. Indian J Gastroenterol. 2003;22(2):49–53.
2. 2.Singh H, Mishra A, Sharma D, Somashekar U. A simple prognostic scoring system for typhoid ileal perforation peritonitis. Tropical doctor. 2010;40(4):2037
3. Boey J, Choi SK, Poon A, Alagaratnam TT. Risk stratification in perforated duodenal ulcers. A prospective validation of predictive factors. Annals of surgery. 1987;205(1):22.
4. Altaca G, Sayek I, Onat D, Cakmakci M,Kamiloğlu S. Risk factors in
perforated peptic ulcer disease: comparison of a new score system with the Mannheim Peritonitis Index.The European journal of surgery= Actachirurgica. 1992;158(4):217-21.
5. Jagdeesh TS, Mishra A, Saxena A, Sharma D. Eosinopenia as a prognostic marker in patients with peritonitis. ISRN Infectious Diseases 2012; 28:2013.
87
7. Koc M, Yoldas O, Kilic YA, Gocmen E, Ertan T, Dizen H, Tez M: Comparison and validation of scoring systems in a cohort of patients treated for perforated peptic ulcer. Langenbecks Arch Surg 2007, 392(5):581–585.
8. Makela JT, Kiviniemi H, Ohtonen P, Laitinen SO: Factors that predict morbidity and mortality in patients with perforated peptic ulcers.Eur J Surg 2002, 168(8–9):446–451.
9. Boey J, Wong J, Ong GB. A prospective study of operative risk factors in perforated duodenal ulcers. Ann Surg 1982;195: 265-9.
10. 10.Kim JM, Jeong SH, Lee YJ, Park ST, Choi SK, Hong SC, et al. Analysis of Risk Factors for Postoperative Morbidity in Perforated Peptic Ulcer. J Gastric Cancer 2012; 12: 26-35.
11. Thorsen K, Søreide JA, Søreide K. Scoring systems for outcome prediction in patients with perforated peptic ulcer. Scand J Trauma ResuscEmerg Med 2013 Apr 10; 21: 25.
88
13. Subedi SK, Afaq A, Adhikary S, Niraula SR, Agrawal CS: Factors influencing mortality in perforated duodenal ulcer following emergency surgical repair. JNMA J Nepal Med Assoc 2007, 46(165):31–35.
14. Ersumo T, W/Meskel Y, Kotisso B. Perforated peptic ulcer in Tikur Anbessa Hospital: a review of 74 cases. Ethiop Med J 2005; 43: 9-13.
15. 15.Buck DL, Vester-Andersen M, Møller MH. Accuracy of clinical prediction rules in peptic ulcer perforation: an observational study. Scand J Gastroenterol 2012; 47: 28-35.
16. Arici C, Mesci A, Dincer D, Dinckan A, Colak T: Analysis of risk factors predicting (affecting) mortality and morbidity of peptic ulcer perforations. Int Surg 2007, 92(3):147–154.
89 PROFORMA
SI No : Ipd No : Name : DOA : Age : DOD : Sex : Occupation : Address :
Presenting Symptoms:
Abdominal pain
Vomiting/Nausea
Abdominal distension
Constipation/ obstipation
Past history:
Medical history
Surgical history Personal history:
90 SYSTEMIC EXAMINATION:
Cardiovascular system Respiratory system Central nervous system Per Abdomen:
Inspection
Palpation
Auscultation
Percussion CLINICAL IMPRESSION:
INVESTIGATIONS Basic investigations Radiological- X-ray chest X-ray abdomen erect Final diagnosis: Laparotomy findings Intervention done:
91
CONSENT FORM
I ………, do hereby volunteer and consent to participate in this study being conducted by Dr. Vignesh Shankar .S on “EFFECTIVENESS OF JABALPUR SCORE IN PREDICTING MORTALITY AND MORBIDITY IN PATIENTS WITH PERITONITIS CAUSED BY PEPTIC ULCER PERFORATION ". I have read and understood the consent form or it has been read and explained to me in my own language. The study has been fully explained to me and I may ask questions at any time.
Signature / Left Thumb Impression of the Volunteer Date:
Place: Signature and Name of witness