COMPARISON OF ACCURACY OF 3 DIFFERENT METHODS OF WORKING LENGTH DETERMINATION IN LOWER PREMOLARS IN-VIVO AND BY USING
CBCT AND MAGNIFYING LOUPE EX-VIVO
A dissertation submitted
In partial fulfillment of the requirements For the degree of
MASTER OF DENTAL SURGERY
BRANCH IV
CONSERVATIVE DENTISTRY AND ENDODONTICS
THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY CHENNAI 600032
"No one who achieves success does so without acknowledging the help of others. The wise and confident acknowledge this help with gratitude."
Foremost, I want to offer this endeavour to The Almighty, for the wisdom he has bestowed upon me, the strength and good health in order to finish this dissertation.
I thank our Chairman Prof. Dr. K. R. Arumugam, & Vice Chairman A. Babu Dhandapani for the facilities provided to carry out the work at the Institute.
I extend my sincere gratitude to our respected Principal Prof. Dr. K.S. Prem Kumar M.D.S, Head of the Department of Orthodontics, for allowing me to perform my study in orthodontic patients and also for his support.
I am grateful to Prof. Dr. P. Hemalatha M.D.S., Head of the Department of Conservative Dentistry and Endodontics, for her invaluable guidance. I thank her for having trust in me and providing me with this wonderful clinical study. It was a great privilege to work and perform the study under her supervision.
Acknowledgement
I shall always be indebted to all the Teachers and PGs of the Department of Orthodontics and the Department of Oral and Maxillofacial Surgery for the timely help rendered by them throughout the study period.
My profound gratitude to my other Fellow Post Graduates for their valuable support and
togetherness. A very special thanks to my juniors Dr.D.S. Venkataramanan and Dr. G. Sudharsan for helping me by being the second observers in this dissertation.
I owe my sincere gratitude to Dr. Sangeetha Chavan M.D.S. Reader, Department of Community and Public Health Dentistry and to my dear friend, Dr. Vidhya Raghu for their great support in the biostatistics and helped me to present my results in a very unique way.
No research is possible without The Library, the Centre of learning resources. I take this time to express my gratitude to the library staffs for their great support.
Above ground, I am indebted to my family, My Parents and My Sister whose values helped me to only grow with age. And finally, I acknowledge My Husband and My Lovely Daughter who served as my inspiration to pursue this undertaking.
AIM:
The aim of the study was to determine the accuracy of working length determination using Tactile Sensation method, Digital Radiographic Method (RVG) and Electronic Apex Locator (PROPEX II) in lower premolars in-vivo, and to compare the lengths so measured to the actual working length after extraction, measured using CBCT and Magnifying Loupe, ex-vivo.
MATERIALS AND METHODS:
30 mandibular premolars scheduled for orthodontic extraction were selected. After informed consent from the patient, under local anaesthesia, access cavity was prepared, canal located and pulp extripated. The working length was determined by Tactile Sensation method, Digital Radiographic Method (Radiovisiography) and Electronic Apex Locator using PROPEX II apex locator. The values were measured and tabulated. All the 3 methods were performed by 2 operators after blinding. After determining the working length in vivo, the teeth were extracted and the samples were then subjected to Cone beam computed tomography and the CBCT working length was determined. Now a K- file was inserted into the root canal until the file tip is visible at the apical foramen which was confirmed using a Magnifying loupe and these readings were measured as the actual working length of the tooth. and cross evaluated with all other working length values. The reliability analysis was also done to analyze the level of reliability of each group with the Actual Working Length values obtained using Magnifying loupe after extraction.
RESULTS:
Abstract
measurement using CBCT and Electronic apex locator are the most reliable method followed by radiographic method and tactile sensation respectively. Based on the correlation values on reliability, CBCT method have more positive correlation with actual working length measured using Magnifying loupe, followed by Electronic apex locator and then by RVG and tactile sensation.
CONCLUSION:
Within the limitations of the present study, it is concluded that
1. Comparison of working that length measurement with Magnifying Loupe, CBCT, and other 3 conventional in vivo methods showed a significant difference in measurement. 2. Radiographic working length determination using RVG, can be considered as reliable tool
when combined and confirmed with electronic working length measurement.
3. The EAL values of working length showed more positive correlation with the AWL values measured using magnifying loupe. Keeping other potential advantages in consideration, we conclude that the use of EAL technique clinically is useful in root canal treatment for measuring working length which correlates more positively with the AWL.
4. CBCT scans can be used as an alternative method for ascertaining the WL. If a patient has a preexisting CBCT scan, the clinician should take advantage of this technique as an alternative, reliable method for determining the WL.
LIST OF ABBREVIATIONS
No. Acronym Abbreviation
1 CDJ Cemento-dentinal junction
2 AC Apical constriction
3 AF Apical foramen
4 IOPA Intra oral periapical radiography
5 RVG Radiovisiography
6 CCD Charge coupled device
7 CBCT Cone beam computed tomography
8 MPR Multiplanar reformation
9 FOV Field of view
10 CMOS Complementary metal oxide semiconductor
11 DDR Direct digital radiography
12 TWL Tactile working length
13 RWL Radiographic working length
14 EAL Electronic apex locator working length
15 OPG Orthopantamography
16 CBCTWL Cone beam computed tomography working length
17 PSP Photostimulable phosphor plate
18 EDTA Ethylene diamine tetra acidic acid
19 MDCT Multidetector computed tomography
20 SPSS Statistical package for the social sciences
LIST OF FIGURES
No.
Description of Figures
Page No.
1 Working mechanism of RVG 4
2 Working principle of EAL 7
3 Flat panel detectors in CBCT 11
4 Mechanism of image production in CBCT 12
5 Carl Zeiss magnifying loupe 190mm (8.0x) 14
6 Pre-operative OPG 36
7 (A) Consent form -English 39
7 (B) Consent form - Tamil 39
8 Anatomy of the root apex 53
9 (A) Injection of Local Anesthesia 40
9 (B) Rubber dam isolation 40
9 (C) Access cavity preparation 40
10 Working length determination using Tactile
sensation method
41
11 Working length determination by RVG 42
12 Working length determination using electronic apex locator
43
14 Extracted premolar 44
15 CBCT model 44
16
CBCT working length measurement using
DICOM software
45
17 (A) Evaluation of AWL using magnifying loupe 46
17 (B) Position of the file tip at the minor diameter seen through the apical foramen
46
17 (C) Measurement using digital caliper 46
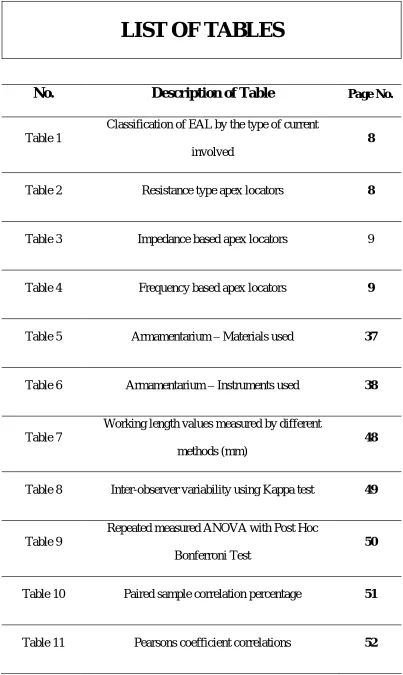
LIST OF TABLES
No.
Description of Table
Page No. [image:17.595.122.525.89.764.2]Table 1
Classification of EAL by the type of current
involved
8
Table 2 Resistance type apex locators 8
Table 3 Impedance based apex locators 9
Table 4 Frequency based apex locators 9
Table 5 Armamentarium Materials used 37
Table 6 Armamentarium Instruments used 38
Table 7
Working length values measured by different
methods (mm)
48
Table 8 Inter-observer variability using Kappa test 49
Table 9
Repeated measured ANOVA with Post Hoc
Bonferroni Test
50
Table 10 Paired sample correlation percentage 51
Table 12 Studies of the position of the apical constriction 54
Table 13 Summary of various RVG studies
57
Table 14
Various comparative studies on different methods
of working length determination with EAL
TABLE OF CONTENTS
No.
Contents
Page No.
1
Introduction
1
2
Review of Literature
15
3
Aim and Objectives
35
4
Materials and Methods
36
5
Statistical Analysis
47
6
Results
48
7
Discussion
53
8
Summary
68
Introduction
1
The long-term success of root canal treatment depends upon the relationship between
instrumentation and obturation procedures and the complex anatomy of the apex.1 Determination of working length is one of the most critical steps of endodontic therapy and a
clear understanding of the morphology of the root canal system, including the apex, is
imperative. The cleaning, shaping and obturation of the root canal system cannot be
accomplished accurately unless the working length is determined precisely.2
WORKING LENGTH is defined in The distance
from a coronal reference point to the point at which canal preparation and obturation
The anatomical apex is the tip or the end of the root determined morphologically, whereas the
radiographic apex is the tip or the end of the root determined radiographically. It is well
established that root morphology, root aberrations, anatomical variations and radiographic
distortion may cause the location of the radiographic apex to vary from the anatomical apex. 3
The dentin cementum junction has been recommended as an ideal apical termination for root
canal preparation4. The position of this histologic entity varies around the internal
circumference of the canal by up to 3 mm across opposing walls. It is located approximately
1 mm away from the apical foramen.5
An apical constriction usually occurs in the region of the dentin cementum junction and
often forms a natural apical matrix. It is the narrowest portal of entry of the pulpal
vasculature from the periapical tissues and would be the smallest wound following pulp
removal. The topography of the apical constriction is variable and undetectable
2
Kuttler investigated the root apices of teeth and provided a dimensional analysis of the apical
morphology. He noted that the distance from the apical constriction to the vertex of the root
increased with age and was recorded as between 0.5 and 0.6 mm. This distance was
considered as a measurement to subtract from the radiographic apex to approximate the
location of the apical constriction.6 Working length, the apical extent of canal preparation and
obturation, is often the main variable in determining success or failure. Seltzer et al. were the
first to report greater success in terminating cleaning and obturating the root canal system just
short of the radiographic apex.7
Sjogren et al. investigated endodontic outcomes over an 8- to 10-year period in over 350
patients. They reported the best outcome was when the root canal filling was between 0 to 2
mm short of the radiographic apex. Distances beyond the radiographic apex, or more than 2
mm short of this point, resulted in significantly lower success rates. These findings are in
agreement with research conducted by other investigators and most recently by
meta-analysis of the literature.8
Chugal found variations in success rate of teeth root filled at different levels. Teeth with
normal preoperative pulps and periapical tissues enjoyed a higher success rate when filled
over 1 mm from the radiographic apex. On the other hand, teeth with necrotic pulps and
apical periodontitis showed greater success when the canal filling was closer to the level of
the radiographic apex. From all the evidence cited, it is clearly prudent to be able to
accurately prepare and fill root canals to a predetermined location in the canal short of the
Introduction
3
METHODS OF DETERMINING WORKING LENGTH:
The requirements of an ideal method for determining working length include rapid location
of the apical constriction in all pulpal conditions and all canal contents; easy measurement,
even when the relationship between the apical constriction and the radiographic apex is
unusual; rapid periodic monitoring and confirmation; patient and clinician comfort; minimal
radiation to the patient; ease of use in special patients such as those with severe gag reflex,
reduced mouth opening, pregnancy, pacemakers, implants etc, and cost effectiveness.10To achieve the highest degree of accuracy in working length determination, a combination of
several methods should be used. This is important in canals for which working length
determination is difficult11.
THE MOST COMMON METHODS ARE.
i. Patient Response.
ii. Tactile Sense Method
iii. Paper Point Measurement.
iv. Radiographic Methods.
v. Electronic Methods.
vi. Audiometric Method.
Of these methods 3 clinically more reliable methods - Tactile Sense Method, Radiographic
Method and Electronic Method have been chosen for this study.
TACTILE SENSATION METHOD:
The tactile perception because of the simplicity of the technique and its virtual effectiveness
are factors that motivate a few clinicians in endodontic practice to still follow this technique.
This method is considered as supplementary to high-quality, carefully aligned, parallel,
4
constricted, an experienced clinician may detect an increase in resistance as the file
approaches the apical 2 to 3 mm.12 Following access, when interferences in the coronal third of the canal are removed, the observant clinician can detect a sudden increase in resistance as
a small file approaches the apex. Careful study of the apical anatomy discloses two facts that
make tactile identification possible:
(1) the unresorbed canal commonly constricts just before exiting the root, and
(2) it frequently changes course in the last 2 to 3 mm.
The awareness of these variations may be enhanced by the use of a file that is larger than the
expected constricture. As preparation develops space in the coronal two-thirds (i.e., radicular
access), the quality of tactile information improves. At that point files bind only in the apical
area, and resistance must be in that region. 13Hence in this clinical study, tactile sense method is used to determine the working length in-vivo.
RADIO VISIO GRAPHY. (RVG)
One of the direct digital radiographic techniques used in dentistry is radio visiography (RVG)
which was introduced to dentistry by Francis Mouyen. This system is based on digital image
capture using a charged coupled device (CCD) which is capable of image enhancement using
[image:24.595.163.432.577.738.2]up to 256 shades of gray.14
Introduction
5
By means of a solid-state radiation detector more sensitive than conventional silver halide
films, the system presents intra oral radiographic images immediately after exposures. One of
the advantage of this digital radiographic technique over conventional radiographs is the
possibility of quantifying the distance between two points on a given image. Ong et al in
1995 stated that RVG is the on -screen measurement utility which allows for rapid additive
multiple point measurement points on screen to a tenth of a millimeter. This is one of the
great advantages of the use of this system in endodontics. 15
In vitro study by Dina Al-Sudani 2002 showed that digital radiography is of equal value to
conventional radiograph for imaging root canal system. However, the radiovisiography has
the advantage of being rapid, low dose imaging technique, besides the image can be stored. 16 Other advantages of this digital technique include immediate image display, the ability to
improve the clarity of the image whilst reducing the radiation dose and accurate working
length estimation even in roots demonstrating severe apical curvature. Hence in this study
RVG has been selected as one of the methods for the in-vivo determination of working
length.17
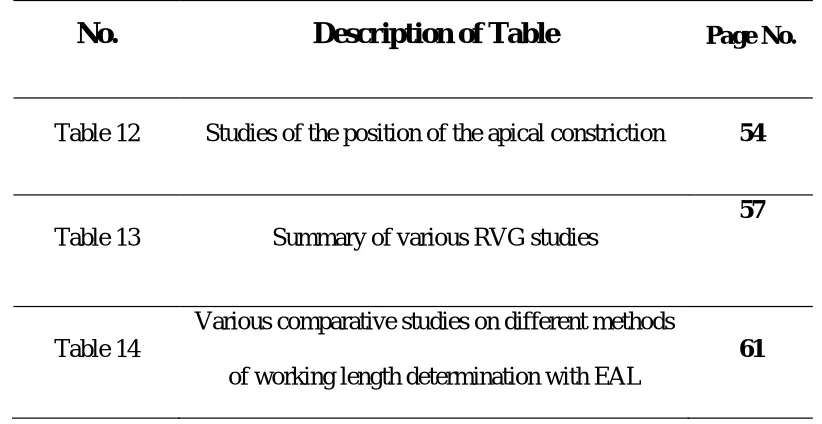
DETERMINATION OF WORKING LENGTH BY ELECTRONICS
Electronic apex locators (EALs) have been one of the major breakthroughs in the traditional
practice of endodontics, as they operate on the electrical impedance at the apical foramina
rather than by a visual inspection of the radiographic apex. EALs are convenient for the
patient and operator, eliminate radiation exposure, save time, and can be used during
6
In 1918, CUSTER was the first to report the use of electric current to determine working
length
In 1942, SUZUKI, reported his study on iontophoresis of ammoniated silver nitrate in the
teeth of dogs. The silver solution was placed in the root canals and then totally dispersed by a
negative electrode in contact with the oral mucous membrane. The conclusion of this
experiment was that the electrical resistance between the root canal instrument inserted into a
root canal and an electrode applied to the oral mucous membrane registered a consistent
value of approximately 6.5 kilo ohms (kW).
In 1960, GORDON, was the second to report the use of clinical device for electrical
measurement of root canals.
In 1962, SUNADA, adopted the principle reported by Suzuki and was the first to describe the
detail of a simple device to measure working length in patients. He used a simple direct
current ohm meter to measure a constant resistance of 6.5 (kW) between oral mucous
membrane and periodontal ligament regardless of age of the patient or the shape and type of
the teeth which became the basis for most apex locators.18
circuit one side
the patients hand. The electrical circuit is complete when the endodontic instrument is
advanced apically inside the root canal touches the PDL. The display on the apex locator
Introduction
[image:27.595.128.486.86.384.2]7
FIG 2: WORKING PRINCIPLE OF EAL
Classification20
The classification of apex locators was given by Mc Donald (1992)based on Type of current flow (operating principle)
8
Depending upon type of current involved
(Table 1)
Resistance type apex locators (Table 2): These apex locators has a built in resistance value
of 6.5 kilo Ohms. The apex locators are attached to the patient's lip on one side and the other
side is attached to the file. The file is then advanced into the canal until it touches the
periodontal tissue at the apex which then completes the circuit.
Impedance type apex locator (Table 3): Operate on the principle that there is electrical
impedance across the walls of the root canal due to the presence of the transparent dentin.
The tooth exhibits increasing electrical impedance across the walls of the root canal, which is
Introduction
9
unit detects the sudden change and indicates it on the analogue meter. To overcome the
problem of a wet environment, insulated probes are utilized.
Frequency based apex locators (Table 4): Operate very similarly to the impedance type
because it measures the impedance of tooth at two different frequencies. In the coronal
portion of the canal, the impedance difference between the frequencies is constant. As the file
advanced apically, the difference in the impedance value begins to differ greatly with
maximum differences at the apical area.
Propex II (Densply-Maillefer, Tulsa) apex locator was used in this study, as some
of the earlier studies in permanent teeth have found it to be better when compared with other
10
principle that uses multiple frequencies to determine the root canal length. Rather than using
the amplitude of the signal as for all EALs, it measures the energy of the signal with multi
signal frequencies. Hence, Propex II is reportedly less affected by potential interferences in
the root canal. Propex II works by calculating the ratio of the impedances measured
simultaneously at frequencies of 0.5 and 8.0 kHz.21
Endodontic Working Length Measurement with Cone-Beam
Computed Tomography Scanning
Cone-beam imaging, sometimes referred to as digital volume tomography, is one of the most
exciting developments in dental and maxillofacial radiology and, owing to its versatility.
CBCT allows the c
-dimensional images in the coronal, sagittal and even oblique or curved image planes a
process referred to as multiplanar reformation (MPR).Dental CBCT technology first emerged
in 1995 when Italian inventors Attilio Tacconi and Piero Mozzo introduced the first
maxillofacial imaging device, the NewTom DVT 9000. 22
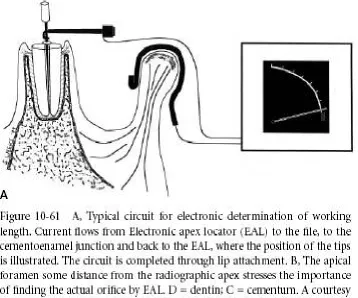
Working mechanism:
Dental CBCT utilises a cone- or pyramid-shaped X-ray beam which is directed on the
pursued maxillofacial field-of-view (FOV). Most of the modern CBCT scanners use flat
panel detectors (FPD) comprising of a pixel array of amorphous silicon thin-film transistors
(TFT) or complementary metal oxide semiconductors (CMOS). For both of these, X-rays are
first converted to light photons by a scintillator material which may consist of thallium doped
caesium iodide (CsI:Tl) or terbium activated gadolinium oxysulphide (Gd2O2S:Tb).
Introduction
11
array to compile a projection raw-data digital image. Flat panel detectors offer higher spatial
resolution and greater dynamic range, and are less bulky and complicated compared to image
intensifiers (II) and charge coupled devices (CCD) which have gradually become obsolete as
[image:31.595.138.459.193.415.2]CBCT detectors.23
FIG 3: FLAT PANEL DETECTORS IN CBCT
The pre-processing steps of the acquired projection raw-data vary between manufacturers for
flat-panel detectors. Typical steps include adjustments related to detector dark-current, gain
and pixel defects by applying offset and gain corrections.
A possible latent image signal from the previous projection read-out also has to be erased by
after glow correction, especially if higher frame-rates are applied. Other processing methods
can be utilised based on the physical properties of the acquisition system, such as X-ray beam
12
Once the X-ray measurements are acquired, they are transferred to a computer where they are
processed to obtain a image volume. This process is called image reconstruction. Once image reconstruction has been performed, the computer components of the system make the CT
[image:32.595.148.445.216.431.2]image volume available for display in some sort of image viewing software.22
FIG 4:MECHANISM OF IMAGE PRODUCTION IN CBCT
In CBCT imaging, voxels are usually isotropic and range from 0.4 mm3 to as small as 0.075
mm3. This superior spatial resolution is one of the most attractive qualities of CBCT imaging
and is largely the result of flat panel technology and isotropic data acquisition. Small FOV
(55 mm_37 mm) CBCT with a 0.076-mm3 voxel size had the potential to improve the spatial
resolution of root canal anatomy in any chosen viewing plane. Working length measurements
obtained by different CBCT FOVs and voxels were clinically acceptable and correlated with
Introduction
13
Liang et al. 2013 found CBCT-based root-canal length measurements are accurate and
reliable, when compared with a gold standard, as actual length. In addition, Janner et al. in
2015 reported that an existing CBCT is as successful as an EAL. Connert et al. in 2016 found
69% accuracy with the CBCT, compared with AL, and concluded that CBCT images can be
used to accurately determine WL. 42
Ela Youti et al in 2009 described that in cases with inconsistent EAL measurements, the
possibility of obtaining root canal measurements from CBCT images could lead to a more
precise evaluation of working length and improved success rates for endodontic treatment.
On the other hand, teeth with metallic reconstructions are prone to problems with EAL
measurements because of electrical short circuits. For 3D imaging using computed
tomography, acquisition artifacts such as beam hardening, scatter, noise, and streak artifacts
caused by metal reconstructions have been described, with CBCT showing less prevalence of
this kind of image distortion. Hence this CBCT working length determination is taken as one
of the parameters in this study.25
Measurement of actual length of tooth after extraction using
Magnifying loupe:
The anatomical variables should be important for accurate working length determination.
The minor diameter of the canal represents the transition between the pulpal and the
periodontal tissues where the canal instrumentation and obturation should terminate.
Microscopic studies estimate the distance of the minor diameter to be from 0.5 to 1.0mm
from the external foramen or major diameter.
When the anatomic apex and apical foramen do not coincide, radiographic estimation of
working length becomes more questionable, and other methods of working length
determination become more important. The larger the distance between these two points, the
14
more significant when treating premolars and molars where there is a higher probability of
inconsistency in foramen position. It was demonstrated that the apical foramen is located
laterally in 78 to 93% of posterior teeth. 26
The actual working length measurement after extraction should be done by taking histologic
sections for locating the minor diameter. But the reliable and feasible method is by inserting
a file into the canal, until the tip can be seen through the major foramen and adjusted for its
position at the level of the coronal-most boundary of the major foramen. The visual
evaluation could be done using magnifying glass, stereomicroscope, surgical operating
microscope or using magnifying loupes.
The magnifying loupe used in this study has 8X magnification which gives an accurate
visualization of the file tip at the minor diameter with great precision. The actual length (AL)
of the tooth is considered as a gold standard in the present study and was measured after
[image:34.595.184.413.536.672.2]evaluation under Magnifying loupe.27
15
1.
Shanmugaraj, et al (2007)This comparative ex- vivo study was done to determine the accuracy in measuring the
working length of root canal using tactile method, electronic apex locator and radiographic
method, in vivo, and comparing the lengths so measured to the actual working length, ex
vivo, after extraction. Thirty single-rooted teeth scheduled for extraction were selected for the
study. After obtaining the consent from patients, a preoperative radiograph was taken and
access opening was done. Working length was determined by ta
radiographic method and by using a Foramatron-IV digital apex locator in vivo. The teeth
were then extracted and the actual working length was determined by placing an endodontic
file in the root canal 0.5 mm short of the apex. The results indicated that among the three
methods, the electronic apex locator showed the highest accuracy and the highest reliability
for working length determination.28
2.
Sharma and Arora (2010):The purpose of the present study was to compare the accuracy of frequency based apex
locator Root ZX and conventional radiographic method under clinical conditions. The
accuracy of the the working length by microprocessor controlled impedance quotient apex
locator was compared using single canal single rooted teeth (incisor, canine and lower
premolar teeth) that were to be extracted for periodontal or orthodontic reasons. An intraoral
periapical (IOPA) radiograph was taken. The tooth was then extracted under local anaesthesia
along with the file in the tooth. The distance of the file tip from the apex was measured under
3X magnification and the reading recorded. It was observed that the radiographic method had
a significant variation from the electronic method when compared to the actual measurement
Review of literature
16
method as compared to radiographic method for determination of working length of the root
canal.29
3.
Luigi Cianoni 2010:This ex vivo study compared the accuracy of three different electronic apex locators (EALs)
in detecting the apical foramen and the accuracy of digital radiography and EALs in
determining the working length (WL) with visible control under a microscope; and the
precision of #10, #15, and #20 K-files in electronic measurements. The length of 101
extracted human teeth was measured with three different EALs (Endex , ProPex II and Root
ZX ), with radio videography (RVG) and compared with the actual length. An endodontic
training kit was used during the experimental procedures. Statistical analysis showed that
Endex and ProPex II were more accurate than Root ZX in determining the WL and no
significant difference between the three different K-file sizes measurements. EALs showed to
be more accurate in determining the WL than RVG and Instrument sizes of hand files did not
affect the accuracy of EALs.30
4.
Shohreh Ravanshad et al (2010)This clinical study was done to compare the effect of working length determination using
electronic apex locator or working length radiograph on the length adequacy of final working
length as well as the final obturation. In 84 patients with 188 canals who were randomized
into two groups; in group 1, the working length was determined by working length
radiograph, whereas in group 2, it was determined by the Raypex5 electronic apex locator.
The results of endodontic treatment using the electronic apex locator are quite comparable, if
not superior, to the radiographic working length measurement regarding the rates of
acceptance of cases. In addition to reducing the radiographic exposure, electronic apex
17
5.
John F. Sherrard 2010This study evaluated the accuracy and reliability of tooth-length and root-length
measurements derived from cone-beam computed tomography (CBCT) volumetric data.
Using the Dolphin imaging software the CBCT scans were oriented twice for each tooth
using the mesial, distal, labial, and lingual cementoenamel junctions as reference points.
Root and tooth lengths were derived from these points and compared with actual
measurements of the teeth made with digital calipers after all surrounding bone had been
carefully removed. Within-trial method errors were almost 2 times greater for the
periapical radiographs than for the CBCT scans. Between trial method errors were
greatest for the 0.4-mm CBCT scans, which were within 0.1 mm of the periapical
radiograph method errors. The intraclass correlations for the periapical and CBCT
measurements were allabove 0.995. CBCT scans are at least as accurate and reliable as
periapical radiographs32
6.
Denis Gonçalves Real, 2011The objectives of this study were to assess the accuracy of working length determination
using 3 electronic apex locators and direct digital radiography and to compare the results with
those obtained using the visual method. The results suggested that electronic apex locators
are useful in determining the ideal working length for root canal preparation, obturation and
also in locating the cemento-dentino-canal junction. These devices become more precise,
especially in the presence of deviation of the apical foramen from the anatomic root apex, in
which the radiographic method yields poor results. In this study, Root ZX and Elements
Review of literature
18
7.
Parekh V. et. al. (2011) :The purpose of this study was to compare the ability of radiographic and electronic methods
to determine reliably the location of the apical constriction. An ex vivo study was conducted
on 20 premolars with intact single straight root canal. After the coronal flaring and irrigation,
the radiographic working length was determined with a k- file and electronic length using
(EL-Root-ZX) 3rd generation apex locator. After extraction of all the premolars,
stereomicroscope was used to confirm and compare radiographic and electronic apex locator
working length values.34
8.
Vieyra et. Al. (2011) :The aim of this in vivo study was to evaluate the accuracy of the Root ZX,
Elements-Diagnostic, Precision AL and Raypex 5 electronic apex locators when compared to
radiographs for locating the apical constriction. Under clinical conditions EALs identified the
AC with greater accuracy than radiographs. In addition, only 0.6% (average) of the EAL
measurements were 1.0 mm through the AC whereas with radiographs it was 31.4%. A WL
1.0 mm through the AC will, in some cases, results in instrumenting and filling beyond the
foramen. A WL 0.5 mm short of, or at the radiographic apex, would further increase the
likelihood of this happening. EALS can increase the accuracy of WL determination.35
9.
Vaiyapuri Ravi et al (2012)This in vitro study compared the conventional and direct digital radiography (DDR) in
working length measurement of the root canal and assessed the significance of the different
enhancement modes provided by the software to visualize the file length. Both conventional
19
radiography must be of size 15 or greater. The enhancement feature of DDR greatly
improves the visual perception, resulting in more accurate measurements. The positive and
colorize enhancement modes were found to be more closely associated with the actual file
length than the control group and other groups.36
10.
Nanda Kishore et al (2012):They compared the working length determination done using three methods, namely, apex
locator (Foramatron D-10, Parkell), radiovisiography (Planmeca) and conventional
radiography (Prostyle intra, Planmeca). The results revealed that all the three methods located
the apex nearly as accurately as the actual root canal length obtained by histological ground
sectioning, and among three methods apex locator being the closest to the actual root canal
length. The study concludes that all the three techniques are equally effective in determining
working length.37
11.
Franziska B. Jeger 2012This prospective, controlled clinical study was to analyze endodontic working length
measurements in preexisting cone-beam computed tomography (CBCT) scans and to
compare them with clinical root canal length determination by using an electronic apex
locator (EAL). All included patients had received a CBCT scan independent of the present
study and needed root canal treatment. Clinically, the root canal length was measured with an
EAL by an endodontist. This measurement was compared with the root canal length as
measured on vestibulooral and mesiodistal CBCT sections by an examiner not involved in the
endodontic treatment. The measurements in both slices (r = 0.97). The mean discrepancy
between RRL and CRL was 0.51 mm (median, 0.36 mm), with a range from 0.02 1.83 mm
Review of literature
20
endodontic working length measurement with a precision similar to measurements done by
EAL.38
12.
Vijay Singh 2012:The in vivo study was aimed at evaluating the accuracy of electronic apex locator, to
determine the working length of root canal, and it was compared with the radiographic
method of working length determination. After access cavity preparation, working length was
determined using radiographic method and electronic apex locator, after which the file was
fixed with a light cured composite resin. The tooth was then extracted and was then
longitudinally grounded using straight fissure diamond bur until the root canal and the tip of
the file were visible. The distance of file from the minor constriction was measured using a
stereomicroscope. The electronic working length determination of root canal was found to be
more accurate than the radiographic method.39
13.
Lucena et al (2013)This in vitro study compared the accuracy of working length (WL) determination using the
Raypex 6® electronic apex locator and cone-beam computed tomography (CBCT). 150
extracted human teeth were decoronated and randomly assigned to five groups (n = 30). WL
conditions (group 1) or with 2.5% NaOCl, distilled water or Ultracain® (groups 2 4). The
radiological WL (group 5) was calculated from bucco-lingual and mesio-distal CBCT
sections. CBCT measurements were an average of 0.59 mm shorter than AL. Electronic
measurements were more reliable than CBCT scans for WL determination. The Raypex 6®
was more accurate in locating the major foramen than the apical constriction under the
21
14.
Kalyan Vinayak 2013The objective of this in vitro study was to compare the accuracy of radiographic method and Propex II apex locator. Thirty single canal extracted human teeth with patent apical foramen
were selected. Access cavities were prepared. Anatomic length (AL) was determined by
inserting a K-file into the root canal until the file tip was just visible at the most coronal
aspect of the apical foramen; subsequently 0.5 mm was deducted from this measured length.
II apex locator was used to determine the electronic working length (EL). The percentage
accuracy of RL and Propex II apex locator was 76.6% and 86.6%, respectively. The results
showed that Propex II was more accurate than the radiographic method in determining
working length. Apex locator can reduced the overestimation observed in radiographic
method.41
15.
Mithun Mohan 2013To evaluate clinical studies on the accuracy of different methods used for working length
determination in endodontics. Search was conducted on Pub med central, Medline and Mesh
data base for the related topic from 1991 to 2012. Articles were selected, if they met the
following criteria: clinical trials, clinical studies, randomized controlled trials and controlled
clinical trials.There is no significant difference between conventional methods and electronic
apex locators in the accuracy of working length determination. But electronic apex locators
and digital radiographic methods were found to be beneficial from the perspective of
radiation dose reduction.Electronic apex locators are not superior to radiographs in
determining working length. Long term follow up studies evaluating post operative success
comparing electronic apex locators and radiographic methods are needed to appreciate the
Review of literature
22
16.
Yu Hong Liang 2013The aim of this in vitro study was to determine the accuracy of root canal length
measurements performed with cone beam computed tomographic (CBCT) scans using a gold
standard. Methods: A total of 162 teeth (198 root canals) in 16 dry human dentulous
mandibles were scanned using a 3DX-Accuitomo CBCT scanner (Morita 3DX; J Morita Mfg
Corp, Kyoto, Japan). The root canal length was measured with CBCT data. All teeth were
extracted atraumatically and endodontically accessed; the root canal length was measured
blindly using a #10 K-file and served as the gold standard. The mean absolute difference of
the CBCT-based root canal length from the gold standard was 0.46 mm (95% confidence
interval, 0.41 0.50 mm). Only in 9 of 198 (4.5%) roots did the difference between the
CBCT-based root canal length and the gold standard exceed 1 mm. CBCT-CBCT-based root canal length
measurements are accurate and reliable when compared with a gold standard. 43
17.
Iyer Krishnan et al (2013)This in vitro study was done to compare the root canal length determination by electronic
apex locator and conventional radiography, and comparing it with the actual length
measurement done by direct visualization. The accuracy of EAL and radiographic methods
were 92% and 72% respectively when compared to the actual length. Hence, EAL proved to
be more accurate in determining the root canal length than the conventional radiographic
method.44
18.
Maria Elissavet Metska,2014This study was to compare the precision of root canal length determination on cone-beam
computed tomographic (CBCT) scans and periapical radiographs (PAs) with the actual root
canal length. The secondary aim was to examine the influence of tooth type anterior and
23
canal length measurement was performed by a consensus panel (2 examiners) on CBCT
scans and digital PAs. After access opening, a #15 file was fixated in every root canal at the
length measured on CBCT scans. All teeth were extracted, and the root canal containing the
file was uncovered. Measurements made on images taken with a digital camera linked to a
stereo-zoom microscope were used as the actual root canal length. The root canal length
measurements of posterior maxillary teeth, they were significantly more accurate than Pas
when CBCT images were used.45
19.
Connert et al (2014)This in vitro study was done to evaluate the accuracy of working length determination
using cone beam computed tomography. The results showed that using a simplified method,
CBCT images of 0.2mm voxel size can be used to accurately determine the endodontic
working length.46
20.
Tadas Venskutonis et al 2014This article reviewed the use of CBCT imaging in the diagnosis, treatment planning, and
assessing the outcome of endodontic complications. Intraoral radiography is the imaging
technique of choice for the management of endodontic disease, but CBCT appears to provide
a superior validity and reliability in the detection of periapical lesions. The superior accuracy
of CBCT imaging helps in the early detection of periapical lesions and may help to determine
their exact locations and extents. CBCT imaging can potentially become the first choice for
endodontic treatment planning and outcome assessment, especially when CBCT with lower
radiation doses and better resolutions become available. However, endodontic cases should
Review of literature
24
information from conventional imaging systems may not yield adequate amounts of
information to allow for the successful management of endodontic problems.47
21.
Anil Dhingra 2015The aim of this clinical study was to compare the effect of working length determination
using radiovisiography (RVG) and two-dimensional (2D) and three-dimensional (3D)
measurements using cone-beam computed tomography (CBCT).Thirty mandibular teeth were
taken and three groups of 10 each were made.The root canal length was determined using
RVG, CBCT measurement method 2D, and CBCT measurement method 3D. The difference
between CBCT measurements, RVG, and the actual canal length were compared to evaluate
the accuracy of each method. No significant statistically difference was seen with 3D
measurements and actual measurements. Measurements with RVG were better than CBCT
2D. CBCT 3D measurements are accurate than RVG and CBCT 2D in the determination of
root canal length.48
22.
Rakesh Mittalet al (2015)In this ex- vivo study of evaluating the accuracy of WL determination by using conventional radiography, digital radiography, and EALin working length (WL) determination. Ability to
measure WL was detected precisely and in acceptable range that is ± 0.5 mm of actual
WL.The mean value of differences between three experimental methods length and the actual
WL were statistically significant. EAL gave the most accurate readings out of all the
experimental groups, with 100% accuracy within the acceptable range where as digital
radiography gave the least accurate reading. The electronic method (Justy II apex locator)
25
23.
Tooba Ghazal 2015The aim of this study was to compare the accuracy of working length measured by electronic
apex locator and periapical radiograph. Thirteen teeth with 23 canals were selected. Working
lengths of all canals were measured using K file with apex locator and periapical radiographs.
Access opening was filled with restorative GIC with the files present in canals. Teeth were
then subjected to extraction. All extracted teeth were evaluated by sectioning the lower half
or lower one third of the apices longitudinally. The distance of the file tip from the minor
constriction was measured and recorded. The results of the study showed that accuracy of
apex locator were 65% (n=15) with the file tip at minor constriction, while 22% (n=5) for
periapical radiograph. Thus it was concluded that electronic apex locator is more accurate and
reliable then periapical radiograph.50
24.
Ali Bagherpour 2015The aim of this study was to compare digital and conventional radiography in determining the
working length of dilacerated canals.Thirty nine human extracted single-rooted teeth with
root curvature more than 35 degrees were included in this study. The true canal length was
determined for each canal. Then, teeth were mounted in acrylic blocks and canal length was
estimated by using on-screen digital radiography with both 3- and 6-clicks measurement and
from conventional radiography by conforming a preserved file on the image of the root canal.
There were no significant differences in measurement accuracy between the true canal length
and conventional radiographic length, but there were significant difference between both
digital radiographic techniques with true canal length. There was no significant correlation
Review of literature
26
canals, the accuracy of determination of working length by using conventional radiography is
higher than digital radiography.51
27. André Luiz Gomide de Morais 2016
The purpose of this clinical study was to compare the accuracy of working length (WL)
determination using cone-beam computed tomography (CBCT), conventional periapical
radiographies and electronic apex locator. 19 patients with a total of 30 single-rooted teeth
diagnosed with apical periodontitis were selected for this study. After taking the initial
parallel periapical radiographs, the initial file was advanced into the canal until the WL was
detected by the Root ZX apex locator and measured. WL radiographs were taken with the file
set in the canal. Afterwards, CBCT images were acquired and actual working length was
measured. The mean values for WL determination by electronic apex locator, periapical
radiograph and CBCT images were 22.25, 22.43 and 22.65, respectively which was not
statistically significant. The determination of the working length of root canal using CBCT
images was precise when compared to radiographic method and electronic apex locator.52
28. Jhadye Alves Carneiro 2016
The objective of this ex vivo study was to evaluate the accuracy of electronic apex locator for teeth were used in this study. After coronal access, manual measurement of the real working
length o
exceeding of the file in the apical foramen. The file was retracted by 1 mm, and its extension
was measured to determine the real working length. The electronic measurement of the
working length was performed in the same teeth using the Joypex 5 electronic apex locator.
27
and manual methods (P > 0.05). the electronic device for measuring the root canal length
53
29. Yakup Ustun, 2016
This study evaluates the endodontic working-length measurements in teeth with large
periapical lesions and persistent intracanal exudate by using preexisting cone-beam computed
tomography (CBCT). It compares the measurements with clinical root canal lengths
determined by using 2 electronic apex locators. Seventy-three teeth with single roots and
canals were studied. The working length of each canal was measured with 2 different
electronic apex locators- Propex pixi and Raypex 6. The measurements were repeated 3 times
by using a digital caliper, and the mean was recorded. This mean was compared with the root
canal length as measured on CBCT sections. The median values for CBCT, Raypex 6, and
Propex Pixi measurements were 21.10, 21.36, and 21.55, respectively. Statistical analysis
showed no significant difference between the Raypex 6, Propex Pixi, and CBCT evaluations.
in teeth with a large periapical lesion with intracanal exudate, CBCT images with a voxel size
of 0.125 mm show comparable results with measurements made with the Raypex 6 and
Propex Pixi devices.54
30. Swapna et al. (2017)
In this study they combined the application of correction factors and the use of IOPA grid to
obtain the radiographic working length values and have further compared them to the
working length values obtained by the apex locator (Morita ZX) to determine the success
rates of the radiographic technique in cases where apex locators cannot be used or are not
Review of literature
28
showed 1 mm as the correct correction factor to be deducted from the tooth length measured
by the IOPA grid.55
31.Mohammad Mahdi Yaghooti Khorasani 2017
The aim of this study was to compare the accuracy of conventional and digital radiographic
techniques for root canal working length determination. After determining the real working
lengths of 50 permanent maxillary central incisors (gold standard), the conventional (E- and
F-speed films) and digital (CCD, PSP) images were obtained using the parallel technique.
The mean registered working length of each modality was compared with the other and with
the gold standard. No significant difference was found between the recorded working length
values using the conventional and digi-tal radiographic techniques (P=0.828). Within the
limitations of this study, it was concluded that there was no difference between the
measurement accuracy of CCD, PSP and conventional imaging techniques in root canal
working length determination.56
32. (2017) :
The aim of this study was to evaluate the accuracy of working length determination by using
an electronic apex locator, periapical radiography, and cone-beam computed tomographic
(CBCT) imaging obtained at different voxel sizes and field of views (FOVs) in extracted
human teeth. All CBCT images obtained at different FOVs with voxel sizes less than 0.3
mm3 performed similarly and better than intraoral periapical radiography in the
determination of endodontic working length measurement. Apex locator measurements were
better than CBCT and periapical images, and they correlated highly with actual length
29
evaluated in the absence of streak and beam hardening artifacts, motion artifacts, and
anatomic noise from the opposing jaw structures.57
33. Fernanda Gracia et al. (2017)
This in-vivo study was done to assess the accuracy of 2 third-generation electronic apex
locators , Propex II (Dentsply Maillefer) and Root ZX II (J. Morita), and radiographic
technique for locating the major foramen . The measurements obtained using the visual
method exhibited the strongest correlation with Root ZX II (r = 0.94), followed by Propex II
(r = 0.90) and Ingle's technique (r = 0.81; p < 0.001). Descriptive statistics using ANOVA
(Tukey's post hoc test) revealed significant differences between the radiographic
measurements and both EALs measurements (p < 0.05). Both EALs presented similar
accuracy that was higher than that of the radiographic measurements obtained with Ingle's
technique. The results suggest that the use of these EALs for major foramen location is more
accurate than the use of radiographic measurements.58 34. Kaushik Dutta et al (2017):
In this in vitro study they compared the measurement of working length with three different
methods manual tactile sensation, digital radiography and Mutidetector computed
tomography(MDCT). ANOVA and turkeys test showed that there was no significant
difference in the measurements by the three procedures (p>0.05). Working length
measurement with MDCT scan and other two conventional methods does not show
significant difference in measurement. Use of newer 3D imaging technique is useful in root
Review of literature
30
35.Mohamed I. Elshinawy et al (2017):
This in vitro study compared four different working length determination techniques. The
working lengths were repetitively determined in five groups (n = 50 each) using regular tomographic image (group 3), electronic apex locator (group 4) and direct measurement
(group 5, control) by subtracting 0.5 mm from the length of
foramen. The collected data was statistically analyzed using both analysis of variance and
least significant difference (LSD) comparisons at P value less than or equal to 0.05. The difference between the data of study groups (P = 0.011). The LSD comparisons revealed a longer working length (LSD, P
and 2 than groups 3 and 5 (control). On the other hand, no difference (LSD, P > 0.05) was detected between the working length in groups 3 and 4 in comparison with group 5 (control).
radiographs.60
36. Divya Saxena et al, (2017):
This ex vivo study was to comparatively evaluate the accuracy of iRoot, iPex II, and Propex
pixi apex locator using histological sections as the gold standard. Working lengths (WLs) of
teeth were determined using iRoot, iPex II, and Propex pixi. Teeth were then extracted, and
anatomic canal length (ACL) were measured. The apical 4 mm of the roots were
longitudinally shaved away to visualize the canal under a stereomicroscope at ×24
magnification. Digital photographs were evaluated to measure the distance between the major
diameter and minor diameter. Thus, the WL, that is, the minor diameter length (MDL) was
31
acceptable for iRoot, 86.66% for iPex II, and 80% for Propex pixi when compared with mean
MDL as obtained from the histological sections. All apex locators have been shown to
produce acceptable level of accuracy which clearly indicates their reliability in determining
the WL.61
37. Vidhya Bhatt 2017:
The purpose of this study was to evaluate the accuracy of a new-generation electronic apex
locator (iPex) to determine working length in primary teeth with or without root resorption as
compared with the conventional radiographic method. A sample of 30 primary posterior
teeth which are indicated for pulpectomy were selected for the study. Initially, working
length was obtained with iPex (new-generation by Nakanishi International) apex locator
using no.10 K-file, which was then compared with convent
method). In the present study, accuracy of iPex was 70.8% within ±0.5 mm and 90.8% within
±1 mm.There was no statistically significant difference found when using iPex apex locator
for working length determination as compared with that of conventional radiographic
method. Hence Working length determined by iPex apex locator is comparable with that of
conventional radiographic method, hence, can be used as an alternative in determining the
working length of primary teeth.62
38. Cihan Yildrim 2017
The goal of the cone beam computed tomography (CBCT) based investigation was to
compare determination of the WL performance of the electronic apex locator (EAL), CBCT
and digital radiography. 30 single rooted, freshly extracted permanent teeth were included.
Root canal WL measurements were performed using actual length (AL), EAL, digital
Review of literature
32
most accurate method to evaluate the root canal WL, with accuracy of 70%. Accuracy for the
apex locator and periapical radiograph were 40% and 30%, respectively. The CBCT may be
safe to use in determining root canal WL. Because lower radiation dose, a pre-existing CBCT
can be useful to detect the root canal WL more precisely.63
39. Tanikonda Rambabu et al (2018):
The aim of this in-vivo study is to compare and evaluate the preoperative estimated WL with
conventional radiograph and with grid radiograph, with reference to electronic apex locator
The statistical package for the social sciences (SPSS) version
16.0 (SPSS Inc., Chicago, IL, USA) was used to compare the WLs of three groups, and the
statistical significance was considered to be P post hoc test were made to measure the intergroup comparison, and Pearson correlation values were obtained. The
results of the study showed a higher correlation between grid WL and apex locator WL than
conventional WL and apex locator WL. Preoperative metrics with radiographic grid along
with the apex locator is a better measuring tool compared to the conventional radiographic
64
40. Syed Shahbaz 2018
The objective of this study was to compare the working length determination done using
three methods, namely, radiovisiography and conventional radiography, apex locator (Root
ZX mini, MORITA). In this research, to determine the working length, 40 single-rooted teeth
(mandibular first premolars) were selected and each tooth was subjected to all the three
methods of the working length determination. This was compared with the actual working
length measured utilizing ground sections of the individual teeth. The results revealed that all
33
obtained by histological ground sectioning, and among three methods apex locator being the
closest to the actual root canal length.65
41.Razavi 2018
This study aimed at assessing accuracy of digital radiography with different enlargements in
determining working length of root canal and comparing it with standard method. 30
extracted single rooted premolar teeth root canal was prepared. One file with 15 mm size
was placed into canal to the point that its end was observable in canal apex. Firstly, canal
length from reference point was measured based on millimeter and it was measured based on
shortening the length for 0.5 millimeter and it was calculated by 0.1 mm accuracy. The
Radiographic images of indirect digital periapical was provided for all samples by parallel
method after preparing radiography by Scanora software, images were changed into
conventional radiography film size and then they were saved by 2 and 3 times enlargements.
Accuracy of 1x, 2x and 3x enlargements of indirect digital radiography were 95.1%, 96.3%
and 95.9% respectively. Accuracy of enlargements of indirect digital radiography for
estimating root working length were very similar either in general status or in each observers
and there was no significant difference in different enlargements.66
42. Jorge Paredes Vieyra 2018
The aim of this study was to evaluate in vivo the accuracy and predictability of two EALs for determining working length as compared to radiographs: RootZX and CanalPro. One hundred
and sixty teeth (493 canals) with fully formed apices (confirmed by radiographic evaluation
before treatment) and apical periodontitis were used. The Apical Constriction (AC) of each
tooth was located with two electronic apex locators. The measurements obtained by the two
Review of literature
34
For premolar teeth, the Root ZX, CanalPro and radiographs located the minor foramen 79%,
64% and 28% of the time, respectively. Under clinical conditions, the EALs identified the
minor foramen with high degree of accuracy. EAL were more accurate, compared to
radiographs with the potential to greatly reduce the risk of instrumenting and filling beyond
the apical foramen.67
43.Andre Kaled Segato et al 2018:
This study investigates the accuracy of 3D Endo software to determine the working length
when using preoperative cone-beam computed tomographic (CBCT) scans of extracted
teeth, compared with conventional CBCT software and an electronic apex locator (EAL).
CBCT scans of 30 premolars were obtained., the measurement obtained from the coronal
reference to the apical foramen (AF) was recorded as the conventional CBCT length. Then,
using 3D Endo software suggested length SL) and the operator-adjusted length
(3D-OL) were obtained. Teeth were accessed, and the actual length was measured. Finally, the
teeth were measured using the electronic apex locator (EL) using the EAL Root ZX. The
preoperative working length determination using 3D Endo was reliable and similar to
conventional CBCT software. However, the combined use of CBCT with an EAL is
Aim and Objectives
35
AIM
The aim of this study was to determine the accuracy in measuring the working length of root
canal using Tactile Method, Digital Radiographic Method and Electronic Apex Locator, in
Mandibular Premolars in-vivo, comparing the lengths so measured to the actual working
length measured after extraction using CBCT and Magnifying loupeex-vivo.
OBJECTIVES:
1. To compare the accuracy of 3 methods of working length determination in
mandibular Premolars in-vivo : Tactile method, Digital Radiographic Method and
Electronic Apex Locator.
2. To determine the accuracy of the working length measured after extraction ,using
CBCT ex-vivo.
3. To evaluate the level of reliability of four groups TWL, RWL, EWL and CBCTWL
Materials and Methods
36
SAMPLE SELECTION:
Sixty human single-rooted, mandibular premolar teeth with mature apices, scheduled for
orthodontic extraction FIG-6 were selected for the study. Informed written consent was
[image:59.595.154.442.211.354.2]obtained from each patient before treatment.
(
FIG 7 A,B)FIG 6 PRE-OPERATIVE OPG
FIG 7 (A): CONSENT FORM English FIG 7 (B): CONSENT FORM - Tamil
Inclusion criteria
1. Single rooted tooth
2. Presence of single canal
3. Non-carious teeth
37
Exclusion criteria
1. Carious teeth
2. Periodontally compromised teeth
3. Morphologically defective teeth
4. Open apex
5. Young patients with cardiac pacemaker
[image:60.595.73.521.374.679.2]MATERIALS AND INSTRUMENTS USED:
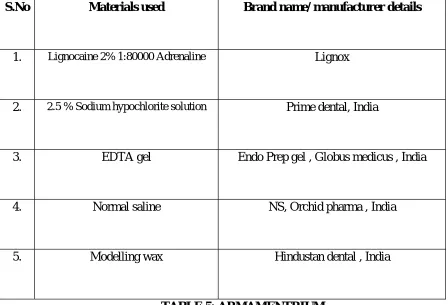
TABLE 5: ARMAMENTRIUM
S.No Materials used Brand name/ manufacturer details
1. Lignocaine 2% 1:80000 Adrenaline Lignox
2. 2.5 % Sodium hypochlorite solution Prime dental, India
3. EDTA gel Endo Prep gel , Globus medicus , India
4. Normal saline NS, Orchid pharma , India
Materials and Methods
38
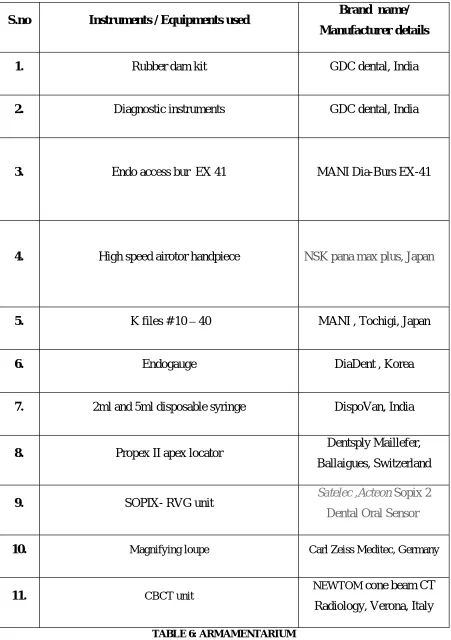
S.no Instruments / Equipments used Brand name/ Manufacturer details
1. Rubber dam kit GDC dental, India
2. Diagnostic instruments GDC dental, India
3. Endo access bur EX 41 MANI Dia-Burs EX-41
4. High speed airotor handpiece NSK pana max plus, Japan
5. K files # 10 40 MANI , Tochigi, Japan
6. Endogauge DiaDent , Korea
7. 2ml and 5ml disposable syringe DispoVan, India
8. Propex II apex locator Dentsply Maillefer, Ballaigues, Switzerland
9. SOPIX- RVG unit Satelec ,Acteon Sopix 2 Dental Oral Sensor
10. Magnifying loupe Carl Zeiss Meditec, Germany
11. CBCT unit NEWTOM cone beam CT
[image:61.595.74.525.78.718.2]Radiology, Verona, Italy
39
METHODOLOGY:
A good quality preoperative radiograph was taken employing the extension cone paralleling
<