PICU Nurses’ Self-Perceived Competency in End-of-Life Care
By
Kirstin MacLeod
Senior Honors Thesis School of Nursing
The University of North Carolina at Chapel Hill April 11, 2020
Approved:
Megan P. Williams, EdD, MSN, RN, FNP, Thesis Advisor Abstract
The majority of pediatric inpatient deaths occur in pediatric intensive care units (PICUs), where registered nurses (RNs) caring for children and their families at the end of life face unique challenges such as differing developmental stages, increased caregiver involvement, and
Keywords: end-of-life care, palliative care, pediatric intensive care unit, education, competency, experience, nursing role
PICU Nurses’ Self-Perceived Competency in End-of-Life Care
In the United States, approximately 40,000 children die each year from traumatic injuries, malignant neoplasms, congenital conditions, complications of prematurity, respiratory
conditions, illness, and other etiologies (AAP, 2000; CDC, n.d.; Stayer, 2012). Most of these children die in hospital settings, and pediatric intensive care units (PICUs) are the most common place of inpatient deaths (Mu et al., 2019).Children hospitalized in PICUs for treatment of life-limiting conditions, as well as their families, can benefit significantly from the resources and support offered by palliative care services (Short & Thienprayoon, 2018).Palliative care is “an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by … treatment of pain and other problems, physical, psychosocial, and spiritual” (WHO, n.d.). Ideally, palliative care should be initiated at the time of diagnosis and continued throughout the course of illness, regardless of the outcome (AAP, 2000). End-of-life (EOL) care is a component of palliative care that addresses patient and family needs when a condition cannot be cured with, or is not responding to, existing medical treatments (Short & Thienprayoon, 2018).
holistic patient care, can use their knowledge of patient and family values to support families across these domains. Providing psychological support, advocating for the family’s preferences, contributing patient-specific information, and answering questions are identified throughout the literature as vital nursing contributions to EOL discussions (Brien, Duffy, & Shea, 2010; Zaal-Schuller, Willems, Ewals, van Goudoever, & de Vos, 2018).
Pediatric nurses face unique challenges in providing EOL care. One major challenge is the consideration of the child’s developmental stage (Baker et al., 2015). Nurses caring for children at the end of life must be able to adjust their communication style and symptom management strategies based on the age of the child. Due to the increased involvement of
caregivers in decision making and other treatment components, pediatric nurses must also utilize strong communication skills to support parents and engage them in care (Baker et al., 2015). Further difficulty in supporting families through the EOL period stems from the uncertain prognostication of life-limiting pediatric conditions (Price et al., 2017). Recognizing the
particular challenges of providing EOL care to pediatric populations, the American Academy of Pediatrics (AAP) released a statement in 2000 recommending the development and
implementation of pediatric-specific palliative care services to address the distinct needs of pediatric populations. While it is widely recognized that there are unique educational needs for nurses caring for pediatric patients at the end of life, it remains unclear if these demands are being met.
unit orientations, national programs, professional associations) and in a variety of formats (i.e. lectures, simulations, self-study), they may not adequately prepare nurses to meet the demands of providing EOL care (Montagnini, Smith, & Balistrieri, 2012; Price et al., 2017; Smith et al., 2018). Montagnini et al. (2012) found that even nurses who have participated in formal training report self-perceived deficiencies, particularly in communication skills and participation in the decision-making process. Similarly, a study of medical providers found that competency in providing EOL care is often achieved through life experiences and on-the-job learning, rather than through formal training (Dickens, 2009).
Nurse-specific perspectives are underrepresented in literature related to healthcare provider EOL education and competency. Despite the unique demands of caring for pediatric patients at the end of life, few studies have investigated the experiences of this subset of nurses. It is necessary to evaluate current educational practices and competency in EOL care in PICU settings so that potential gaps can be identified and addressed.
Purpose
This study aims to determine current levels of self-perceived competency in providing EOL care among PICU nurses. Additional goals include assessing the effect of previous
palliative care education on nurses’ self-perceived competency in providing care and the need for implementation of pediatric-specific palliative care education, specifically surrounding nurse involvement in seven domains: patient- and family-centered decision making, communication within the team and with patients and families, continuity of care, emotional and practical support for patients and families, symptom management and comfort care, spiritual support for patients and families, and emotional and organizational support for ICU clinicians.
Study Design and Participants
This study took place in the pediatric intensive care unit (PICU) at the North Carolina Children’s Hospital. All PICU registered nurses (RNs) employed at the time of the survey were eligible to participate in the study. Participation was voluntary, and RNs were informed of their ability to withdraw from the study at any time.
In the study, participants answered questions in a two-part online survey (see Appendix A). The survey contained 18 questions and was designed to be completed in less than 10 minutes. Participants were first asked to provide demographic information including type of nursing education, years of experience, previous EOL education (yes or no), location of education (unit orientation, continuing education, certification course, undergraduate program, graduate program, and other), instructional method (lecture, reading, role play, simulation, and other), and frequency of providing EOL care. In part two of the survey, RNs participated in the Scale of End-Of-Life Care in the ICU (EOLC-ICU) developed and validated by Montagnini et al. (2012). The EOLC-ICU was designed to assess self-perceived competencies in seven domains of EOL care – patient and family decision making, communication within the team and with patients and families, continuity of care, emotional and practical support for patients and families, symptoms management and comfort care, spiritual support for patients and families, and emotional and organizational support for staff (Clarke et al., 2003). Permission to use the EOLC-ICU in this study was obtained prior to survey distribution.
Data Collection
survey link to PICU RNs via email. The nurse manager also sent a follow-up email five days before the data collection period ended to remind RNs of the opportunity to participate. 85 RNs were employed in the PICU during the three-week data collection period, and 27 responses were received (32%).
Data Analysis
In this cross-sectional descriptive study, EOLC-ICU items were scored with a 5-point Likert scale: 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, and 5 = strongly agree. Questions answered as not applicable were coded as 0. Scores were calculated by summing both total responses and responses specific to the individual seven domains, with higher scores indicating greater self-perceived competency in providing EOL care. Frequencies were calculated to determine the distribution of previous education and experience. Analysis of variance (ANOVA) procedures were used to compare EOLC-ICU total and individual domain scores between groups. Potential differences in EOLC-ICU scores between groups were calculated for factors such as years of experience, number of educational sources, number of educational methods, and frequency of providing EOL care.
Results
Description of Participants
five (20.8%) had 3-4 years of experience, eight (33.3%) had 5-10 years of experience, and two (8.3%) had 21-25 years of experience. Further, 19 participants (79.2%) had been employed at this particular PICU for 0-5 years, three participants (12.5%) had been employed for 6-10 years, and two participants (8.3%) had been employed for 11-15 years. Twenty respondents (83.3%) received their nursing education from a bachelor’s degree program, three respondents (12.5%) received their education from an associate’s degree program, and one respondent (4.2%) was educated through a diploma program.
Table 1
Participant Characteristics (N=24)
Characteristic n (%)
Age
18-24 5 (20.8)
25-34 12 (50)
35-44 4 (16.7)
45-54 3 (12.5)
Gender
Female 23 (95.8)
Male 1 (4.2)
Nursing Program
Diploma 1 (4.2)
Associate Degree 3 (12.5)
Bachelor’s Degree 20 (83.3)
Years of RN Experience
1-2 9 (37.5)
3-4 5 (20.8)
5-10 8 (33.3)
21-25 2 (8.5)
Years of Employment at Current Workplace
0-5 19 (79.2)
6-10 3 (12.5)
11-15 2 (8.3)
Previous EOL Education
Yes 19 (79.2)
No 5 (20.8)
Experience Providing EOL Care at Current Workplace
No 2 (8.3)
EOL Education
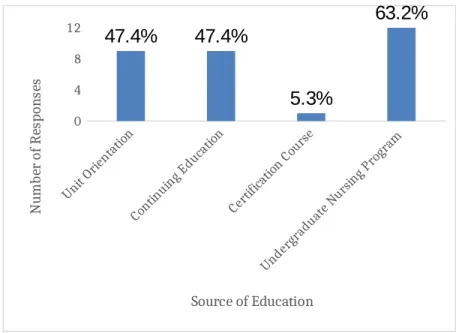
When asked about receiving previous EOL education, 19 respondents (79.2%) reported that they had previous EOL education. The most common place of previous EOL education was in an undergraduate nursing program, with 12 participants (63.2%) reporting education from this source (Figure 1). Unit orientation and continuing education courses were also common sources of EOL education – nine respondents (47.4%) disclosed previous EOL education from each of these locations. Only one respondent (5.3%) reported receiving EOL education through a certification course. When given the option to further describe the places of previous EOL education, participants noted “a different hospital”, “past work experience”, and “required computer-based learning modules” as additional sources. Several participants reported previous EOL education from multiple sources. Six participants (31.6%) reported two sources, three participants (12.5%) reported three sources, and one participant (5.3%) reported four sources.
0 4 8
12 47.4% 47.4%
5.3%
63.2%
Source of Education
N
um
be
r
of
R
es
po
ns
es
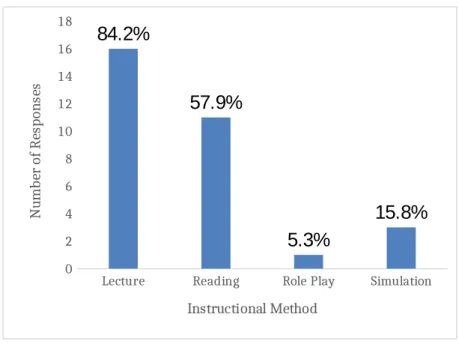
Lectures and reading material were common mediums for EOL care instruction – 16 participants (84.2%) reported lectures as the instructional method used in their EOL education and 11 participants (57.9%) reported learning from readings (Figure 2). Simulations and roleplay were utilized less frequently, with three participants (15.8%) reporting education through use of simulations and one participant (5.3%) reporting use of role play. Several participants noted gaining skills through experiential learning. Two respondents noted “clinical” and “on the job experience” as sources of EOL education. One participant wrote “Literally on the job. My first patient passed and the charge nurse helped a little as it happened. I would have loved to have had some knowledge before the event.” The majority of participants reported having two or more instructional methods during their EOL education. Seven respondents (36.8%) reported two instructional methods and four respondents (21.1%) reported three instructional methods. Eight respondents (42.1%) reported only one instructional method.
Lecture Reading Role Play Simulation
0 2 4 6 8 10 12 14 16 18 84.2% 57.9% 5.3% 15.8% Instructional Method N um be r of R es po ns es
Figure 2. Instructional Method of Participant EOL Education
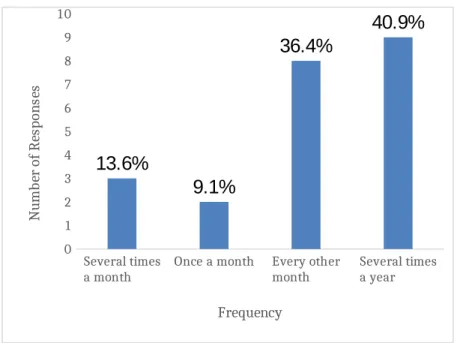
Participants were asked if they have provided EOL care in the PICU setting, and 22 respondents (91.7%) reported that they have provided EOL care in the PICU. The frequency of providing EOL care varied between participants (Figure 3). Three (13.6%) typically provide EOL care several times a month, two (9.1%) provide EOL care once a month, eight (36.4%) provide EOL care every other month, and nine (40.9%) provide EOL care several times a year.
Several times
a month Once a month Every other month Several times a year
0 1 2 3 4 5 6 7 8 9 10 13.6% 9.1% 36.4% 40.9% Frequency N um be r of R es po ns es
Figure 3. Participant Frequency of Providing EOL Care in the PICU
Self-Perceived Competency Ratings
Table 2 outlines mean self-perceived competency ratings based on total EOLC-ICU scores and individual domain scores. Symptom management had the greatest self-perceived competency score (4.10), while continuity of care had the lowest self-perceived competency score (3.19). Participants also rated their competency in emotional support for patients and families (4.06) and spiritual support (3.83) highly in comparison to other domains. Decision making (3.25) and communication (3.20) were domains with lower competency scores. Table 2
Category of Perceived Competency Mean (SD)
Total 3.59 (0.66)
EOL Care Domain
Decision Making 3.25 (0.94)
Communication 3.20 (0.97)
Continuity of Care 3.19 (1.10)
Emotional Support for Patients and Families 4.06 (0.83)
Symptom Management 4.10 (0.58)
Spiritual Support 3.83 (0.96)
Emotional Support for Staff 3.60 (0.90)
Analysis
Self-perceived competency in EOL care tended to increase with participant age, years of RN experience, and years of PICU experience (Table 3). Mean differences between groups were calculated using one-way ANOVAs. A significant difference was found between self-perceived competency scores of 18-24-year-olds and 45-54-year-olds (p=0.021). However, differences in scores between other age groups were not found to be significant. When comparing EOLC-ICU scores of groups with varying years of RN experience, a significant finding was that individuals with more experience had higher competency scores (p=0.029). While EOLC-ICU scores tended to increase with years of employment in this particular PICU, differences in total scores were not significant. However, participants with 11-15 years of PICU experience reported significantly higher confidence in decision making than participants with 0-5 years of experience (p=0.021). Table 3
Mean Self-Perceived Competency Rating Across Groups
Participant Characteristic Mean EOLC-ICU Score
Age
18-24 3.06
25-34 3.77
35-44 3.52
45-54 3.84
1-2 3.30
3-4 3.75
5-10 3.64
21-25 4.29
Years of Employment at Current Workplace
0-5 3.51
6-10 3.65
11-15 4.29
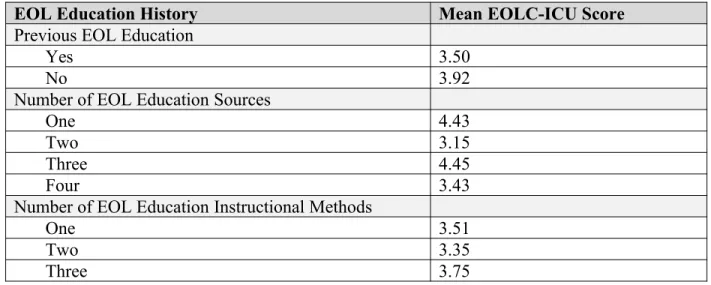
Previous EOL education was not associated with higher self-perceived competency scores (Table 4). Participants who denied previous EOL education had higher average EOLC-ICU scores than those who did have previous education. However, the difference between the two groups was not statistically significant (p>0.05). There did not appear to be a relationship between the number of EOL education sources and instructional methods with self-perceived competency in EOL care.
Table 4
EOLC-ICU Scores Across EOL Education Backgrounds
EOL Education History Mean EOLC-ICU Score
Previous EOL Education
Yes 3.50
No 3.92
Number of EOL Education Sources
One 4.43
Two 3.15
Three 4.45
Four 3.43
Number of EOL Education Instructional Methods
One 3.51
Two 3.35
Three 3.75
Table 5 depicts mean self-perceived competency for groups with various levels of
was not significant (p>0.05). Further, there was no significant difference in EOLC-ICU scores between groups who provided EOL care with various frequency.
Table 5
EOLC-ICU Scores Across Clinical Backgrounds
EOL Clinical Background Mean EOLC-ICU Score
Experience Providing EOL Care at Current Workplace
Yes 3.62
No 3.27
Frequency of Providing EOL Care
Several times a month 3.11
Once a month 3.37
Every other month 3.75
Several times a year 3.73
Discussion and Implications for Clinical Practice
The results of this study provided insight into current levels of self-perceived
competency, education, and frequency providing EOL care among PICU nurses. While previous EOL education was common among PICU nurses, it was not necessarily effective in increasing competency in providing EOL care. PICU RNs who reported previous EOL education had lower mean EOLC-ICU scores than those who denied previous education. However, it is important to note that the difference in scores was not statistically significant. The number of EOL education sources and methods used also did not have significant effects on EOLC-ICU scores.
also increased with years of RN experience and years of employment in this setting. However, there were not significant differences in EOLC-ICU scores between groups.
Given that nurses who participated in EOL education did not have significantly higher EOLC-ICU scores than those who did not, and learning through on-the-job experiences was associated with higher scores, introducing new interactive instructional methods may be useful in improving EOL education. Simulations have been shown to improve communication skills during EOL situations and have been received positively by participants (Smith et al., 2018). In this study, previous EOL education through simulations and role play were reported at low rates compared to lectures and reading. The integration of these methods into existing EOL
educational programs may be helpful in improving effectiveness. Further research should be conducted to determine the feasibility and efficacy of using these methods.
PICU nurses reported lower self-perceived competency in areas related to continuity of care, patient- and family-centered decision making, and communication with patients, families, and team members. These results are generally consistent with findings by Montagnini et al. (2012), who identified that ICU clinicians perceive continuity of care and communication as particularly challenging components of care. A heavy focus on the ambiguity of nurses’ role in EOL decision making in the existing literature, especially in pediatric settings, also supports these findings. Further EOL education with an increased focus on content related to these domains would be beneficial to improving nurse competency in these challenging areas.
A major limitation of this study was the small sample size. The low statistical power and lack of significant differences in mean scores between groups limit the reliability and
with larger sample sizes are needed to assess for significant differences in self-perceived competency between groups.
References
American Academy of Pediatrics. Committee on Bioethics and Committee on Hospital Care. Palliative care for children. (2000). Pediatrics, 106(2 Pt 1), 351–357.
Baker, J. N., Levine, D. R., Hinds, P. S., Weaver, M. S., Cunningham, M. J., Johnson, L., … Kane, J. R. (2015). Research priorities in pediatric palliative care. The Journal of Pediatrics, 167(2), 467–70.e3. https://doi.org/10.1016/j.jpeds.2015.05.002
Bennett, R. A., & LeBaron, V. T. (2019). Parental perspectives on roles in end-of-life decision making in the pediatric intensive care unit: An integrative review. Journal of Pediatric Nursing, 46, 18–25. https://doi.org/10.1016/j.pedn.2019.02.029
Brien, I. O., Duffy, A., & Shea, E. O. (2010). Medical futility in children’s nursing: Making end-of-life decisions. British Journal of Nursing, 19(6), 352–356.
https://doi.org/10.12968/bjon.2010.19.6.47234
Centers for Disease Control and Prevention, National Center for Health Statistics. 2018. Underlying cause of death 1999-2017. CDC WONDER Online Database.
Clarke, E. B., Curtis, J. R., Luce, J. M., Levy, M., Danis, M., Nelson, J., … Robert Wood Johnson Foundation Critical Care End-Of-Life Peer Workgroup Members. (2003). Quality indicators for end-of-life care in the intensive care unit. Critical Care Medicine, 31(9), 2255–2262. https://doi.org/10.1097/01.CCM.0000084849.96385.85
Dickens, D. S. (2009). Building competence in pediatric end-of-life care. Journal of Palliative Medicine, 12(7), 617–622. https://doi.org/10.1089/jpm.2009.0032
family communication during end-of-life care of pediatric patients. Journal of Palliative Medicine, 21(6), 862–878. https://doi.org/10.1089/jpm.2017.0307
Mitchell, S., Spry, J. L., Hill, E., Coad, J., Dale, J., & Plunkett, A. (2019). Parental experiences of end of life care decision-making for children with life-limiting conditions in the paediatric intensive care unit: A qualitative interview study. BMJ Open, 9(5), e028548. https://doi.org/10.1136/bmjopen-2018-028548
Montagnini, M., Smith, H., & Balistrieri, T. (2012). Assessment of self-perceived end-of-life care competencies of intensive care unit providers. Journal of Palliative Medicine, 15(1), 29–36. https://doi.org/10.1089/jpm.2011.0265
Mu, P.-F., Tseng, Y.-M., Wang, C.-C., Chen, Y.-J., Huang, S.-H., Hsu, T.-F., & Florczak, K. L. (2019). Nurses’ experiences in end-of-life care in the PICU: A qualitative systematic review. Nursing Sciene Quarterly, 32(1), 12–22.
Pirie, A. (2012). Pediatric palliative care communication: Resources for the clinical nurse specialist. Clinical Nurse Specialist CNS, 26(4), 212–215.
https://doi.org/10.1097/NUR.0b013e31825aeb97
Price, D. M., Strodtman, L., Montagnini, M., Smith, H. M., Miller, J., Zybert, J., … Ghosh, B. (2017). Palliative and end-of-life care education needs of nurses across inpatient care settings. Journal of Continuing Education in Nursing, 48(7), 329–336.
https://doi.org/10.3928/00220124-20170616-10
Smith, M. B., Macieira, T. G. R., Bumbach, M. D., Garbutt, S. J., Citty, S. W., Stephen, A., … Keenan, G. (2018). The use of simulation to teach nursing students and clinicians palliative care and end-of-life communication: A systematic review. The American Journal of Hospice & Palliative Care, 35(8), 1140–1154.
https://doi.org/10.1177/1049909118761386
Stayer, D. (2012). Pediatric palliative care: A conceptual analysis for pediatric nursing practice. Journal of Pediatric Nursing, 27(4), 350–356. https://doi.org/10.1016/j.pedn.2011.04.031
World Health Organization. (n.d.). WHO definition of palliative care. Retrieved February 26, 2020, from https://www-who-int.libproxy.lib.unc.edu/cancer/palliative/definition/en/ Zaal-Schuller, I. H., Willems, D. I., Ewals, F., van Goudoever, J. B., & de Vos, M. A. (2018).
Appendix A
EOL Pediatric Nurses Survey
In the following survey, you will be asked to answer questions about your nursing education and experience. You will also be asked to rank your confidence in performing several components of end-of-life care. This survey is anonymous and participation is voluntary. Do you consent to participate?
o
Yeso
NoThank you for participating in this survey. Before we begin, please answer the following demographic questions.
What is your age?
o
18-24o
25-34o
35-44o
45-54o
55-64What is your gender?
o
Maleo
Femaleo
OtherWhere did you receive your Nursing degree?
o
Diploma Programo
Associate Degree (ADN) Programo
Bachelor's Degree (BSN) Programo
Other (please specify) ________________________________________________How many years have you worked as an RN?
o
Less than 1o
1-2o
3-4o
5-10o
11-15o
16-20o
21-25o
26-30o
31-35How many years have you been employed at your current workplace?
o
0-5o
6-10o
11-15o
16-20o
21-25o
26-30o
31-35o
35+Which of the following best describes your current employment status?
o
Full-timeo
Part-timeo
Per diemPlease answer the following questions about your education and experience related to end-of-life care.
Have you received any end-of-life education?
o
YesWhere did you receive your end-of-life education?
▢
Unit Orientation▢
Continuing Education▢
Certification Course▢
Undergraduate Nursing Program▢
Graduate Nursing Program▢
Other (please describe) ________________________________________________Which instructional methods were utilized during your end-of-life education?
▢
Lecture▢
Reading▢
Role Play▢
Simulation▢
Other (please describe) ________________________________________________Have you provided end-of-life care at your current workplace?
o
YesOn average, how often do you provide end-of-life care?
o
Several times a weeko
Once a weeko
Several times a montho
Once a montho
Every other montho
Several times a yearo
Once a yearo
Other (Please specify) ________________________________________________I am well prepared
to: DisagreeStrongly Disagree Neutral Agree StronglyAgree ApplicableNot
Treat pain in the dying patient with
pharmacological measures (e.g.,
opioids, anticonvulsants, antidepressants).
o
o
o
o
o
o
Treat pain in the dying patient with nonpharmacological
measures (e.g. heat, cold, massage,
relaxation techniques)
o
o
o
o
o
o
Treat respiratory symptoms in the dying patient (e.g.,
dyspnea and cough).
o
o
o
o
o
o
Treat gastrointestinal symptoms in the dying patient (e.g.,
nausea, vomiting, constipation, and bowel obstruction).
o
o
o
o
o
o
Treat neuro/psychiatric
symptoms in the dying patient (e.g. delirium seizures,
anxiety, and restlessness).
o
o
o
o
o
o
Discuss advance care planning with
patients and their
Discuss code status with patients and
families.
o
o
o
o
o
o
Withdraw life support in the dying
patient.
o
o
o
o
o
o
Identify the emotional needs of
dying patient and
their families.
o
o
o
o
o
o
Identify the cultural needs of dying patients and their
families.
o
o
o
o
o
o
Provide grief and bereavement support to patients and families at the
end of life.
o
o
o
o
o
o
Identify the spiritual needs of dying patients and their
I feel:
Strongly
Disagree Disagree Neutral Agree StronglyAgree ApplicableNot Comfortable
discussing advance care planning with
families and patients.
o
o
o
o
o
o
Comfortable discussing code
status with patients and
families.
o
o
o
o
o
o
Comfortable withdrawing life support in
the dying patient.
o
o
o
o
o
o
It is important for physicians, nurses, and other ICU team
members to collaborate in
end-of-life decision making.
o
o
o
o
o
o
ICU staff would benefit by commemorating
the death of patients in the
ICU.
In the ICU: Strongly
Disagree Disagree Neutral Agree
Strongly Agree Not Applicable I initiate advance care planning with patients/families
when they are admitted with
no documentation of advance care
plans.
o
o
o
o
o
o
I use the patient's advance directive when
developing goals for
end-of-life care.
o
o
o
o
o
o
Code status is discussed with patients/families
in a timely fashion when
the patient's clinical status
deteriorates.
o
o
o
o
o
o
Withdrawal of life support is discussed with patients/families
in a timely fashion when
the patient's clinical status
deteriorates.
o
o
o
o
o
o
Clear and consistent information is provided by team members to patients/families
making decisions regarding end-of-life care. Conflicts among team members are addressed before meeting with the patient and/or family.
o
o
o
o
o
o
Team members meet with the patient and/or family on a regular basis to
review the patient's status
and to answer questions.
o
o
o
o
o
o
Palliative care experts are consulted in a timely manner for end-of-life
issues.
o
o
o
o
o
o
We prepare patients and families for changes of clinicians (attending physicians, residents, medical students, nurses, etc.).
o
o
o
o
o
o
Continuity of care for the patient/family at
end of life is observed when
nursing
assignments are made. There is sufficient support for staff
to handle the personal distress that may arise when
caring for patients at end
of life.