Vancomycin MICs for
Staphylococcus aureus
Isolates Recovered from
Pediatric Patients
Lucia Rose,aShannon Chan,bJobayer Hossain,c,dM. Cecilia Di Pentimae
Department of Pharmacy Practice, Western New England University College of Pharmacy, Springfield, Massachusetts, USAa
; Department of Pediatrics, Alfred I. DuPont Hospital for Children, Wilmington, Delaware, USAb
; Nemours Biomedical Research, Wilmington, Delaware, USAc
; University of Delaware, Newark, Delaware, USAd ; Infectious Diseases Division, Department of Pediatrics, Vanderbilt University, Nashville, Tennessee, USAe
We evaluated the evolution of vancomycin MICs for
Staphylococcus aureus
and their relationship with vancomycin use among
hospitalized children.
S. aureus
isolates recovered from sterile sites were prospectively tested for vancomycin susceptibility
us-ing the Etest between 1 April 2000 and 31 March 2008. Vancomycin MICs were grouped into three categories:
<
1, 1.5, and 2
g/
ml. The association between vancomycin MICs and aggregate vancomycin use and individual patient vancomycin exposure 6
months prior to the documented infection was assessed. The geometric mean values for vancomycin MICs for
S. aureus
fluctu-ated over time without a significant trend (
P
ⴝ
0.146). Of the 436 patients included in the study, 363 (83%) had
methicillin-sus-ceptible
S. aureus
(MSSA) and 73 (17%) had methicillin-resistant
S
.
aureus
(MRSA) infections. The rate of isolates with a
vanco-mycin MIC of 2
g/ml increased from 4% (2 of 46) in 2000 to 2001 to 24% (11 of 46) in 2007 to 2008, despite a decrease in
vancomycin use (
r
ⴝ ⴚ
0.11;
P
ⴝ
0.825). The percentage of isolates with a vancomycin MIC of 2
g/ml was higher for MRSA
(15%; 11 of 73) than for MSSA strains (5.2%; 19 of 363) (
2ⴝ
9.2;
P
ⴝ
0.01). Individual patient vancomycin exposure was not
associated with a higher vancomycin MIC. In the unadjusted model, in which we compared patients with
S. aureus
infections
with MICs of
<
1
g/ml, the odds ratios of exposure rates for patients with isolates with MICs of 1.5
g/ml and 2
g/ml were
1.02 (
P
ⴝ
0.929) and 1.13 (
P
ⴝ
0.767), respectively. In our experience, the geometric means of vancomycin MICs from
S. aureus
isolates recovered from hospitalized children oscillated over time and were not associated with previous individual patient
van-comycin exposure or aggregate vanvan-comycin use.
O
ver the past two decades, methicillin-resistant
Staphylococcus
aureus
(MRSA) has become a major etiology of both
com-munity-acquired and health care associated infections in children
(
1
–
4
). Since its introduction to the market in 1958, vancomycin
has remained the first-line agent for management of hospitalized
pediatric patients with these severe infections. Vancomycin MICs
creeping above 1.5
g/ml for MRSA strains and associated
re-duced vancomycin efficacy reported in adults have challenged
cli-nicians’ choices of effective antibiotic therapies in critically ill
pa-tients (
5
–
14
). Moreover, pharmacokinetic-pharmacodynamic
(PK-PD) simulation studies in children promote the use of more
aggressive vancomycin dosing despite limited available data
re-garding safety in this patient population (
15
,
16
).
We evaluated the trend in vancomycin MICs for
S. aureus
over
an 8-year period, its correlation with aggregate and
individual-patient vancomycin exposure, and clinical outcomes associated
with infections when the MIC of the isolate was 2
g/ml.
(This study was presented in part as an abstract and a poster at
the 47th Annual Meeting of the Infectious Diseases Society of
America, Philadelphia, PA, October 2009 [
17
].)
MATERIALS AND METHODS
Settings.The study was conducted at the Alfred I. DuPont Hospital for Children, a 180-bed tertiary-care academic pediatric hospital affiliated with Thomas Jefferson University (Philadelphia, PA). Overall, the inpa-tient units averaged 9,000 admissions per year, with 78 pediatric/medicine residents and 31 pediatric fellows providing rotating care (18).
Definition of antimicrobial susceptibility.The Clinical and Labora-tory Standards Institute (CLSI) definesS. aureusisolates with oxacillin MICs ofⱕ2g/ml andⱖ4g/ml as methicillin-susceptibleS. aureus
(MSSA) and methicillin-resistantS. aureus(MRSA) strains, respectively (19). Vancomycin-susceptibleS. aureus(VSSA) isolates are considered susceptible if the MIC for vancomycin isⱕ2g/ml. Vancomycin-inter-mediateS. aureus(VISA) strains require concentrations between 4 and 8
g/ml for growth inhibition, and isolates requiringⱖ16g/ml are con-sidered resistant (19).
S. aureusclinical isolates.S. aureusisolates recovered from sterile sites from pediatric patients admitted to the Alfred I. DuPont Hospital for Children from 1 April 2000 to 31 March 2008 were included in the study. Only oneS. aureusisolate per patient per year was included in the analysis. Sterile sites included bloodstream (peripheral and catheter related), mus-culoskeletal (bone, joint, and muscle), cerebrospinal fluid, and pleural fluid.S. aureusisolates were identified according to standard procedures (e.g., growth conditions, morphological criteria, Gram staining, catalase test, Staphaurex test [Remel, Lenexa, KS], or tube coagulase test) and by Vitek (bioMérieux, Durham, NC) at the Alfred I. DuPont Hospital mi-crobiology laboratory. The percentages of susceptibility for oxacillin and vancomycin were calculated according to the 2006 CLSI recommenda-tions (20).
MIC determination.Clinical isolates were tested prospectively for vancomycin susceptibility using an Etest (AB Biodisk, bioMérieux, S.A.,
Received21 March 2013Returned for modification19 April 2013 Accepted8 June 2013
Published ahead of print19 June 2013
Address correspondence to M. Cecilia Di Pentima, [email protected].
Copyright © 2013, American Society for Microbiology. All Rights Reserved.
doi:10.1128/JCM.00768-13
on May 16, 2020 by guest
http://jcm.asm.org/
Marcy l’Etoile, France) at the Alfred I. DuPont Hospital microbiology laboratory according to the manufacturer’s instructions. Etest suscepti-bilities were read at the point of care by a single observer. Vancomycin MICs were grouped into three categories, MICsⱕ1g/ml, 1.5g/ml, and 2g/ml. Oxacillin susceptibility analyses were routinely performed using a Vitek (bioMérieux, Durham, NC).
Data collection and definitions.Patient demographic information was retrieved from medical records and recorded into the database. Clinical and outcome data of patients with MICs of 2 g/ml were recorded into a separate database. Clinical data collected included underlying medical condition and diagnosis at admission as well as presence of a central venous catheter (CVC). Empirical antibiotic ther-apy refers to the antibiotic agents given pending culture reports. De-finitive antibiotic therapy refers to antibiotics given based on isolate identification and susceptibility data. Outcome data collected in-cluded duration of bacteremia, the presence of sepsis, and death dur-ing hospitalization. Duration of bacteremia refers to the number of days from the first positive blood culture to the first negative blood culture. Attributable mortality was defined as death during bacteremia or sepsis in the absence of another cause.
Measures of vancomycin use. Medication administration record (MAR) data were stored in the Cerner database and in the Nemours data warehouse. Tables containing selected critical data elements were down-loaded daily from CareNet and PharmNet to the Nemours data ware-house by using an Oracle database (Oracle Corporation, Redwood Shores, CA) established to integrate business, operational risk, and clinical data with patient encounters (18). Numbers of vancomycin doses adminis-tered were retrieved by querying the Cerner medication administration record tables linked to vancomycin in the data warehouse (21). Data from 1 April 2000 to 31 March 2008 were captured by the number of doses administered to each unique patient. Doses administered were normal-ized per 1,000 patient-days to control for differences in the annual hospi-tal census (18,21).
Individual-patient vancomycin exposure.Vancomycin therapy, ex-pressed as doses administered and days of therapy, was recorded for each individual patient during the 6 months preceding theS. aureusinfection.
The Nemours Institutional Review Board approved this study. Statistics.A chi-square test was used to determine the statistical sig-nificance between patient characteristics and groups ofS. aureusMICs. Continuous variables were compared by use of the Studentttest. Geomet-ric means of vancomycin MICs were calculated and a simple linear regres-sion of the log(MIC) of time was performed to determine the trend of the natural logarithm-transformed MIC over time. Temporal trends of
aggre-gate vancomycin use per 1,000 patient-days were analyzed using a2test trend for proportions (21). Spearman’s correlation coefficient was used to evaluate the association between aggregate vancomycin use and rates ofS. aureusinfection with higher MICs. A multivariable logistic regression analysis was used to determine the association between individual-patient vancomycin exposure and the vancomycin MIC forS. aureus, while con-trolling for methicillin resistance. All tests were two tailed, with aPvalue of 0.05 as the set level of significance. Analyses were performed using IBM SPSS software version 20 (IBM Corp.) and statistical software R version 2.10.2.
RESULTS
During the study period,
S. aureus
geometric means of
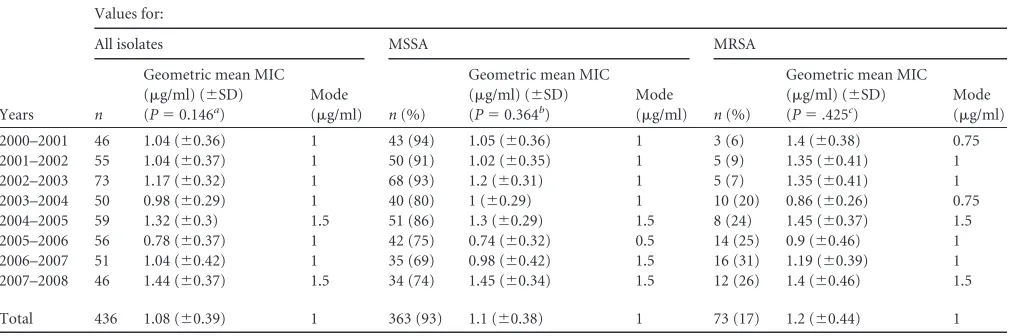
vancomy-cin MIC values fluctuated as depicted in
Table 1
. Over time, we did
not find a statistically significant trend in the geometric mean
change in the log(MIC) (slope [SE], 2.012 [0.008];
P
⫽
0.146). A
total of 436 children, with a median age of 4 years (range 0 to 20
years), developed invasive
S. aureus
infection. All documented
infections were susceptible to vancomycin. Males represented
60% of individuals with infections. Of these, 363 (83%) developed
infections with MSSA strains and 73 (17%) developed infections
with MRSA. The geometric means of vancomycin MICs for MSSA
and MRSA isolates were 1.1
g/ml and 1.2
g/ml, respectively
(
Table 1
). Trends for the vancomycin MIC geometric means for
MSSA and MRSA isolates were not statistically significant when
evaluated separately (
Table 1
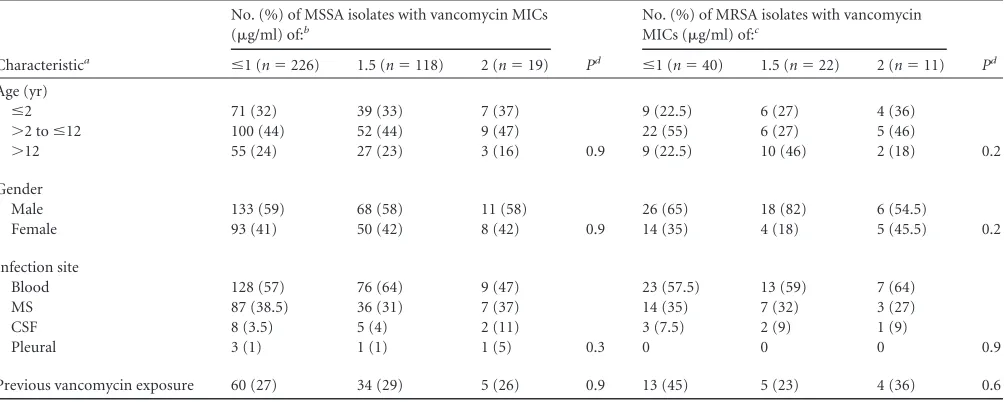
). Patient characteristics and rates of
invasive staphylococcal infections based on
S. aureus
susceptibility
to methicillin and vancomycin MICs are shown in
Table 2
. The
rates of
S. aureus
isolates with vancomycin MICs of 2
g/ml
in-creased from 4% (2 of 46) during the first year of the study to 24%
in 2007 to 2008 (11 of 46). From 2000 to 2001 to 2007 to 2008, a
higher percentage of MRSA (15%; 11 of 73) isolates expressed a
vancomycin MIC of 2
g/ml than MSSA isolates (5.2%; 19 of 363)
(
2⫽
9.2;
P
⫽
0.01). Rates of MSSA isolates with MICs of 2
g/ml
fluctuated between 2% (1 of 50) and 6% (2 of 35) in 2001 to 2002
and 2006 to 2007, respectively, and sharply increased to 21% (7 of
34) during the last year of the study. MRSA strains with MICs of 2
g/ml were not recovered until 2001 to 2002 (20%; 1 of 5), and
peaked in 2007 to 2008 at 33% (4 of 12).
[image:2.585.41.546.78.246.2]Of the 30 patients who developed
S. aureus
infections with
TABLE 1Vancomycin MICs forStaphylococcus aureusby Etest at Alfred I. DuPont Hospital for Children, 1 April 2000 to 31 March 2008
Years
Values for:
All isolates MSSA MRSA
n
Geometric mean MIC (g/ml) (⫾SD) (P⫽0.146a)
Mode
(g/ml) n(%)
Geometric mean MIC (g/ml) (⫾SD) (P⫽0.364b)
Mode
(g/ml) n(%)
Geometric mean MIC (g/ml) (⫾SD) (P⫽.425c)
Mode (g/ml)
2000–2001 46 1.04 (⫾0.36) 1 43 (94) 1.05 (⫾0.36) 1 3 (6) 1.4 (⫾0.38) 0.75
2001–2002 55 1.04 (⫾0.37) 1 50 (91) 1.02 (⫾0.35) 1 5 (9) 1.35 (⫾0.41) 1
2002–2003 73 1.17 (⫾0.32) 1 68 (93) 1.2 (⫾0.31) 1 5 (7) 1.35 (⫾0.41) 1
2003–2004 50 0.98 (⫾0.29) 1 40 (80) 1 (⫾0.29) 1 10 (20) 0.86 (⫾0.26) 0.75
2004–2005 59 1.32 (⫾0.3) 1.5 51 (86) 1.3 (⫾0.29) 1.5 8 (24) 1.45 (⫾0.37) 1.5
2005–2006 56 0.78 (⫾0.37) 1 42 (75) 0.74 (⫾0.32) 0.5 14 (25) 0.9 (⫾0.46) 1
2006–2007 51 1.04 (⫾0.42) 1 35 (69) 0.98 (⫾0.42) 1.5 16 (31) 1.19 (⫾0.39) 1
2007–2008 46 1.44 (⫾0.37) 1.5 34 (74) 1.45 (⫾0.34) 1.5 12 (26) 1.4 (⫾0.46) 1.5
Total 436 1.08 (⫾0.39) 1 363 (93) 1.1 (⫾0.38) 1 73 (17) 1.2 (⫾0.44) 1
a
Slope (SE)⫽2.012 (0.008). bSlope (SE)⫽2.008 (0.009). c
Slope (SE)⫽2.018 (0.022).
on May 16, 2020 by guest
http://jcm.asm.org/
strains expressing MICs of 2
g/ml, 16 (53%) developed
bacter-emia, more commonly associated with MSSA isolates. Over time,
the rates of bacteremia caused by isolates with an MIC of 2
g/ml
increased (
2trend
⫽
13;
P
⫽
0.0003) (
Fig. 1
). No significant
dif-ferences were noted between age groups and
S. aureus
infections
(Pearson’s
2⫽
0.907;
P
⫽
0.9) and/or bacteremia (Pearson’s
2⫽
4.9;
P
⫽
0.3) caused by isolates with vancomycin MICs of 2
g/ml. Demographic and clinical characteristics of children with
S. aureus
bloodstream infections (BSI) and non-BSI due to strains
with vancomycin MICs of 2
g/ml are shown in
Table 3
and
Table 4
, respectively. Among these 30 patients, 9 (30%) had a
preceding exposure to vancomycin within the previous 6
months. Patients treated with vancomycin received daily
dos-ages ranging from 20 to 40 mg/kg of body weight per day. In
this cohort, one death (3.3%) was attributed to MSSA BSI in a
12-month-old infant while on hospice care for intractable
bi-lineal leukemia.
We noted a sharp decline in the rates of
S. aureus
isolates with
vancomycin MICs of
ⱕ
1
g/ml between 2006 to 2007 and 2007 to
2008 (
P
⬍
0.001). No intermediate or
vancomycin-resistant strains were recovered.
[image:3.585.43.545.87.288.2]We previously reported the trends of vancomycin use 3
years before and after implementation of our antimicrobial
stewardship program (
21
). Prior to the implementation of the
antimicrobial stewardship program, vancomycin use increased
from 112 doses administered/1,000 patient-days during the
TABLE 2Selected characteristics of children with invasive staphylococcal infections at Alfred I. DuPont Hospital for Children, 1 April 2000 to 32
March 2008
Characteristica
No. (%) of MSSA isolates with vancomycin MICs (g/ml) of:b
Pd
No. (%) of MRSA isolates with vancomycin MICs (g/ml) of:c
Pd
ⱕ1 (n⫽226) 1.5 (n⫽118) 2 (n⫽19) ⱕ1 (n⫽40) 1.5 (n⫽22) 2 (n⫽11) Age (yr)
ⱕ2 71 (32) 39 (33) 7 (37) 9 (22.5) 6 (27) 4 (36)
⬎2 toⱕ12 100 (44) 52 (44) 9 (47) 22 (55) 6 (27) 5 (46)
⬎12 55 (24) 27 (23) 3 (16) 0.9 9 (22.5) 10 (46) 2 (18) 0.2
Gender
Male 133 (59) 68 (58) 11 (58) 26 (65) 18 (82) 6 (54.5)
Female 93 (41) 50 (42) 8 (42) 0.9 14 (35) 4 (18) 5 (45.5) 0.2
Infection site
Blood 128 (57) 76 (64) 9 (47) 23 (57.5) 13 (59) 7 (64)
MS 87 (38.5) 36 (31) 7 (37) 14 (35) 7 (32) 3 (27)
CSF 8 (3.5) 5 (4) 2 (11) 3 (7.5) 2 (9) 1 (9)
Pleural 3 (1) 1 (1) 1 (5) 0.3 0 0 0 0.9
Previous vancomycin exposure 60 (27) 34 (29) 5 (26) 0.9 13 (45) 5 (23) 4 (36) 0.6
a
MS, musculoskeletal; CSF, cerebrospinal fluid. bTotaln⫽363.
c
Totaln⫽73. dPearson’s chi-square.
FIG 1Vancomycin use and percentage of patients at the Alfred I. DuPont Hospital for Children withS. aureusinfections with vancomycin MICs of 2g/ml.
Vancomycin use is expressed as number of doses administered per 1,000 patient-days (shown with bars on the left axis) and percentage of hospitalized children withS.aureus(SA) infections with MICs of 2g/ml (represented as dotted and solid lines on the right axis).
on May 16, 2020 by guest
http://jcm.asm.org/
[image:3.585.135.451.512.694.2]first year of the study to 378 doses administered/1,000
patient-days in 2003 to 2004 (
2trend
⫽
218.14;
P
⬍
0.001). After the
implementation of the program, the use of vancomycin
de-creased to 255 doses administered/1,000 patient-days in 2007
to 2008 (
2trend
⫽
41.16;
P
⬍
0.001).
Figure 1
depicts trends
of aggregate vancomycin use and percentages of
S. aureus
in-fections associated with isolates expressing vancomycin MICs
of 2
g/ml (
r
⫽ ⫺
0.11;
P
⫽
0.825). Of the 436 patients included
in the study, 121 (27.8%) received vancomycin within 6
months of the documented infection. In these children,
indi-vidual-patient vancomycin exposure was not associated with a
higher vancomycin MIC. In the unadjusted model, in which we
compared patients with
S. aureus
infections with MICs of
ⱕ
1
g/ml, the odds ratios of exposure rates for patients whose
isolates had MICs of 1.5
g/ml and 2
g/ml were 1.02 (
P
⫽
0.929) and 1.13 (
P
⫽
0.767), respectively. After we controlled for
isolate susceptibility to methicillin, these odds ratios were 1.02 (
P
⫽
0.932) and 1.10 (
P
⫽
0.821), respectively, showing no differences
between groups.
DISCUSSION
[image:4.585.41.283.97.419.2]During the 8 years of the study,
S. aureus
infections in children at
our institution were mainly associated with MSSA isolates. Over
time, we did not find a statistically significant trend for the
geo-metric mean of vancomycin MIC or an association between
ag-gregate and individual-patient vancomycin exposure and
vanco-mycin MICs among the
S. aureus
isolates recovered. The most
striking finding was the higher proportion of
S. aureus
infections
associated with higher MICs (2
g/ml) noted during the last year
of the study, despite the steadily declining use of vancomycin after
the implementation of antimicrobial stewardship strategies. Of
these patients, only 30% had a prior exposure to vancomycin. In
our cohort, patients with MRSA bloodstream infections due to
isolates with higher MICs were treated with vancomycin doses
ranging between 20 and 40 mg/kg/day, and these patients cleared
their bacteremia within 72 h. None of these patients died.
Further-more, we found no differences between days of positive blood
TABLE 3Selected characteristics of children withStaphylococcus aureus
bloodstream infection and vancomycin MICs of 2g/ml, Alfred I. DuPont Hospital for Children, 1 April 2000 to 31 March 2008
Characteristica MSSA (n⫽9) MRSA (n⫽7) Pvalue
Age, median (range) 8 mo (0–11 yr) 3 mo (0–12 yr) 0.4
Male sex (n[%]) 5 (56) 4 (57) 0.5
Underlying condition (n)
Prematurity 4
Endocarditis 1
Osteomyelitis 2 2
Leukemia, HLH 4
TPN dependent 2
Tracheostomy 1
Previous vancomycin exposure (n[%])b 3 (33) 3 (43)
Sepsis (n) 2 2
Central venous access (n) 8 7
Empirical antibiotic therapyc(n)
Vancomycin 2
Vancomycin⫹ -lactamd
5 1
Vancomycin⫹aminoglycoside 2
Vancomycin⫹clindamycin 1
Vancomycin⫹rifampin 1
-Lactam⫹clindamycin 1
Clindamycin 1
-Lactam 2
Days of bacteremia, mean (range) 2.67 (1–6) 2.29 (1–3) 0.4
Definitive antibiotic therapye (n)
Vancomycin alone 1 5
Vancomycin⫹ -lactam 1
Vancomycin⫹rifampin 1
-Lactam 5
--Lactam⫹rifampin 1
-Lactam⫹aminoglycoside 1
Linezolid 1
Duration of therapy (mean [range]) (days)
26 (1–42) 17 (4–42) 0.3
Mortalityf
(n) 1g
0 0.5
aHLH, hemophagocytic lymphohistiocytosis; TPN, total parenteral nutrition.n,
number of children with characteristic.
bPatients with previous vancomycin exposure, measured as doses of vancomycin
administered, 6 months prior to the documentedS. aureusinfection. cAntibiotic agents given pending culture reports.
d
-Lactam antibiotics included oxacillin, nafcillin, cefazolin, cefepime, cefotaxime, ceftriaxone, and piperacillin-tazobactam.
e
Antibiotic therapy given based on identification and susceptibility report. fAttributable mortality.
g
[image:4.585.297.543.97.394.2]Patient on hospice care admitted with sepsis and orders to not resuscitate.
TABLE 4Selected characteristics of children withStaphylococcus aureus
nonbloodstream infection and vancomycin MICs of 2g/ml, Alfred I. DuPont Hospital for Children, 1 April 2000 to 31 March 2008
Characteristic MSSA (n⫽10) MRSA (n⫽4) Pvalue
Age, median (range) (yr) 8 (0–16) 15 (3–19) 0.12
Male sex (n[%]) 5 (50) 2 (50)
Underlying condition (n)
Osteomyelitis 3 1
Malignancya 2
Hydrocephalus 1
Congenital heart diseaseb
1
Spine malformationc 2 2
Previous vancomycin exposure (n[%])d
2 (20) 1 (25)
Sepsis (n) 1 1
Central venous access (n) 7 2 0.5
Site of infection (n)
Skin and soft tissue 1 1
Surgical site infection 5 2
Bone 3 1
Lung 1
Empirical antibiotic therapye (n)
Vancomycin 1
Vancomycin⫹ -Lactamf 3 1
Vancomycin⫹clindamycin 1 1
Vancomycin⫹rifampin 1 1
-Lactam 5
Definitive antibiotic therapyg (n)
Vancomycin alone 1 2
Vancomycin⫹rifampin 1
-Lactam 10
Linezolid 1 1
Duration of therapy (mean [range]) (days)
33 (7–42) 36 (30–42) 0.45
Mortalityh
(n) 0 0
aLeukemia, brain tumor.
b
Congenital heart disease, tetralogy of Fallot.
cSpine malformations, neuromuscular and idiopathic scoliosis, spina bifida.
d
Patients with previous vancomycin exposure, measured as doses of vancomycin administered, 6 months prior to the documentedS. aureusinfection.
e
Antibiotic agents given pending culture reports.
f-Lactam antibiotics included oxacillin, nafcillin, cefazolin, cefepime, cefotaxime, ceftriaxone, and piperacillin-tazobactam.
gAntibiotic therapy given based on identification and susceptibility report.
h
All-cause and attributable mortality.
on May 16, 2020 by guest
http://jcm.asm.org/
cultures among patients with MSSA and MRSA treated with
ap-propriate

-lactam antibiotics or vancomycin. Among these, four
children with osteomyelitis did not have a history of previous
vancomycin exposure. Susceptibility testing by Etest has been
shown to yield higher vancomycin MICs than automated testing
methods (
8
,
22
,
23
). This could explain the favorable clinical
out-come seen in patients with MRSA bacteremia treated with
vanco-mycin despite the high vancovanco-mycin MICs noted
in vitro
.
Never-theless, several studies have demonstrated poor clinical outcomes
in adults with MRSA bacteremia and vancomycin MICs of
⬎
1.5
g/ml measured by Etest (
10
,
24
–
27
). Different confounding
fac-tors in this patient population, including comorbidities and
phar-macokinetics, could be responsible for the differences in clinical
outcomes. Diversity in bacterial genotype and expression of
het-eroresistance could play a role in the inferior outcomes reported
in these patients (
28
).
Our findings are consistent with those reported by Mason and
colleagues (
8
). Among their cohort of pediatric patients with
MRSA bacteremia treated with vancomycin, these authors did not
find a correlation between MIC and duration of positive blood
cultures (
8
). Additional outcome studies in pediatric patients with
invasive MRSA infections with higher vancomycin MICs have not
been published. In a multicenter prospective study of adult
pa-tients with MSSA and MRSA bacteremia, those with higher MICs
had poorer outcomes. However, the antibiotic choice, specifically
the use of vancomycin, was not a contributing factor for mortality
(
24
). More data correlating MICs, mortality, and antibiotic choice
are necessary in the pediatric population.
In the absence of randomized studies assessing clinical
out-comes associated with vancomycin MICs and vancomycin dosing,
these retrospective reports support the Infectious Diseases Society
of America (IDSA) recommendations for antibiotic management
of children infected with MRSA isolates expressing MICs of 2
g/ml (
29
). Clinical practice guidelines indicate that therapy
should be guided by the clinical response independent of the MIC
(IDSA-U.S. Public Health Service grading system: A-III) and
chal-lenge PK-PD studies suggesting the need to use higher doses or an
alternative agent in the presence of MICs of
⬎
1
g/ml to
⬍
2
g/ml and 2
g/ml (
15
,
29
,
30
). The optimal vancomycin PK-PD
parameter was evaluated in a single human study of 108 adult
patients with MRSA pneumonia. For vancomycin, a value of
ⱖ
400 for the area under the concentration-time curve for 24 h
(AUC
24) divided by the MIC (AUC
24/MIC) was shown to be
as-sociated with optimal clinical outcomes (
31
). Applying this
prin-ciple in a PK-PD simulation study, Frymoyer et al. (
15
) reported
that current vancomycin dosing of 40 mg/kg/day in children with
invasive infections due to MRSA strains with an MIC of 1
g/ml
would not achieve an AUC
24/MIC of
ⱖ
400 and more aggressive
doses (60 mg/kg/day) should be used in these patients. For MRSA
strains with an MIC of 2
g/ml, the optimal AUC
24/MIC cannot
be achieved safely, and an alternative agent should be strongly
considered (
15
,
32
). Differences in tissue penetration and
phar-macokinetics in children argue against the assumption that an
AUC/MIC target ratio of
⬎
400 should apply to infections other
than pneumonia (
16
). Moreover, vancomycin is among the most
commonly used antibiotics in children, and higher dosing
regi-mens in the absence of clinical efficacy and safety data could
pro-mote increased rates of toxicity.
One limitation of our study was that isolates were not available
for subsequent testing, including automated susceptibility and
as-sessment of
S. aureus
heterogeneous vancomycin-intermediate
rates over time. The higher rate of vancomycin MICs noted during
the last year of the study could have been related to nosocomial
transmission of these organisms. The majority of patients (19 of
32, 59%) with isolates expressing higher MICs had underlying
conditions requiring multiple hospitalizations. In addition,
dis-continuation of Etest and MIC reporting by the microbiology
lab-oratory limited our ability to follow vancomycin MIC trends
be-yond the study period. Nevertheless, in the two subsequent years,
the microbiology laboratory did not recover
S. aureus
isolates
ex-pressing vancomycin MICs of
⬎
2
g/ml.
Most studies demonstrating a vancomycin MIC creep were
limited to short time intervals (
6
–
9
,
33
). Similar to our study,
studies for which longer time spans have been reported had
van-comycin MICs that fluctuated over time without showing a
statis-tically significant trend (
26
,
34
). Emergence of resistance is
mul-tifactorial and an expected adaptation to antibiotic selective
pressure. Long-term studies are needed to determine the impact
of vancomycin dosing and the use of trends of vancomycin MICs
to modify these regimens. Most importantly, in an era of
person-alized medicine, further pediatric studies are warranted to
evalu-ate the use of applied pharmacodynamic principles to target
ther-apy to individual patient-pathogen interactions to improve
clinical outcomes and avoid toxicity and the emergence of
resis-tance.
ACKNOWLEDGMENT
The authors report no conflicts of interest relevant to this article.
REFERENCES
1.Kaplan SL, Hulten KG, Gonzalez BE, Hammerman WA, Lamberth L,
Versalovic J, Mason EO, Jr.2005. Three-year surveillance of
community-acquiredStaphylococcus aureusinfections in children. Clin. Infect. Dis.
40:1785–1791.
2.Purcell K, Fergie J.2005. Epidemic of community-acquired
methicillin-resistantStaphylococcus aureusinfections: a 14-year study at Driscoll Chil-dren’s Hospital. Arch. Pediatr. Adolesc. Med.159:980 –985.
3.Richards MJ, Edwards JR, Culver DH, Gaynes RP.1999. Nosocomial
infections in pediatric intensive care units in the United States. National Nosocomial Infections Surveillance System. Pediatrics103:e39.
4.Gerber JS, Coffin SE, Smathers SA, Zaoutis TE.2009. Trends in the
incidence of methicillin-resistantStaphylococcus aureusinfection in chil-dren’s hospitals in the United States. Clin. Infect. Dis.49:65–71.
5.Sievert DM, Rudrik JT, Patel JB, McDonald LC, Wilkins MJ, Hageman
JC. 2008. Vancomycin-resistantStaphylococcus aureus in the United States, 2002-2006. Clin. Infect. Dis.46:668 – 674.
6.Steinkraus G, White R, Friedrich L.2007. Vancomycin MIC creep in
non-vancomycin-intermediateStaphylococcus aureus(VISA), vancomy-cin-susceptible clinical methicillin-resistantS.aureus(MRSA) blood iso-lates from 2001-05. J. Antimicrob. Chemother.60:788 –794.
7.Wang G, Hindler JF, Ward KW, Bruckner DA.2006. Increased
vanco-mycin MICs forStaphylococcus aureusclinical isolates from a university hospital during a 5-year period. J. Clin. Microbiol.44:3883–3886.
8.Mason EO, Lamberth LB, Hammerman WA, Hulten KG, Versalovic J,
Kaplan SL.2009. Vancomycin MICs forStaphylococcus aureusvary by
detection method and have subtly increased in a pediatric population since 2005. J. Clin. Microbiol.47:1628 –1630.
9.Jimenez-Truque N, Thomsen I, Saye E, Creech CB.2010. Should higher
vancomycin trough levels be targeted for invasive community-acquired methicillin-resistantStaphylococcus aureusinfections in children? Pediatr. Infect. Dis. J.29:368 –370.
10. Soriano A, Marco F, Martinez JA, Pisos E, Almela M, Dimova VP,
Alamo D, Ortega M, Lopez J, Mensa J.2008. Influence of vancomycin
minimum inhibitory concentration on the treatment of methicillin-resistantStaphylococcus aureusbacteremia. Clin. Infect. Dis.46:193–200.
11. Sakoulas G, Moise-Broder PA, Schentag J, Forrest A, Moellering RC,
on May 16, 2020 by guest
http://jcm.asm.org/
Jr., Eliopoulos GM.2004. Relationship of MIC and bactericidal activity to efficacy of vancomycin for treatment of methicillin-resistant Staphylococ-cus aureusbacteremia. J. Clin. Microbiol.42:2398 –2402.
12. Moise PA, Sakoulas G, Forrest A, Schentag JJ.2007. Vancomycin in
vitro bactericidal activity and its relationship to efficacy in clearance of methicillin-resistant Staphylococcus aureusbacteremia. Antimicrob. Agents Chemother.51:2582–2586.
13. Ward PB, Johnson PD, Grabsch EA, Mayall BC, Grayson ML.2001.
Treatment failure due to methicillin-resistantStaphylococcus aureus
(MRSA) with reduced susceptibility to vancomycin. Med. J. Aust.175:
480 – 483.
14. Stevens DL.2006. The role of vancomycin in the treatment paradigm.
Clin. Infect. Dis.42(Suppl 1):S51–S57.
15. Frymoyer A, Hersh AL, Benet LZ, Guglielmo BJ.2009. Current
recom-mended dosing of vancomycin for children with invasive methicillin-resistantStaphylococcus aureusinfections is inadequate. Pediatr. Infect. Dis. J.28:398 – 402.
16. Giuliano C, Haase KK, Hall R.2010. Use of vancomycin
pharmacoki-netic-pharmacodynamic properties in the treatment of MRSA infections. Expert Rev. Anti Infect. Ther.8:95–106.
17. Chan S, Di Pentima MC.2009. Pediatric experience with Staphylococcus
aureus MIC’s and vancomycin use: antimicrobial exposure and evolution, abstr 586, poster 1122. 47th Annu. Meet. Infect. Dis. Soc. Am., Philadel-phia, PA, October 2009.https://idsa.confex.com/idsa/2009/webprogram /Paper28697.html.
18. Di Pentima MC, Chan S, Hossain J.2011. Benefits of a pediatric
anti-microbial stewardship program at a children’s hospital. Pediatrics128:
1062–1070.
19. Clinical and Laboratory Standards Institute.2009. Performance
stan-dards for antimicrobial susceptibility testing; 19th informational supple-ment. CLSI M100-S19. Clinical and Laboratory Standards Institute, Wayne, PA.
20. Clinical and Laboratory Standards Institute.2006. Analysis and
presen-tation of cumulative antimicrobial susceptibility test data. CLSI M39-A2. Clinical and Laboratory Standards Institute, Wayne, PA.
21. Di Pentima MC, Chan S.2010. Impact of antimicrobial stewardship
program on vancomycin use in a pediatric teaching hospital. Pediatr. In-fect. Dis. J.29:707–711.
22. Bland CM, Porr WH, Davis KA, Mansell KB.2010. Vancomycin MIC
susceptibility testing of methicillin-susceptible and methicillin-resistant
Staphylococcus aureusisolates: a comparison between Etest® and an auto-mated testing method. South. Med. J.103:1124 –1128.
23. Kruzel MC, Lewis CT, Welsh KJ, Lewis EM, Dundas NE, Mohr JF,
Armitige LY, Wanger A.2011. Determination of vancomycin and
dap-tomycin MICs by different testing methods for methicillin-resistant
Staphylococcus aureus. J. Clin. Microbiol.49:2272–2273.
24. Holmes NE, Turnidge JD, Munckhof WJ, Robinson JO, Korman
TM, O’Sullivan MV, Anderson TL, Roberts SA, Gao W, Christiansen
KJ, Coombs GW, Johnson PD, Howden BP.2011. Antibiotic choice
may not explain poorer outcomes in patients withStaphylococcus au-reusbacteremia and high vancomycin minimum inhibitory concentra-tions. J. Infect. Dis.204:340 –347.
25. Hidayat LK, Hsu DI, Quist R, Shriner KA, Wong-Beringer A.2006.
High-dose vancomycin therapy for methicillin-resistantStaphylococcus aureusinfections: efficacy and toxicity. Arch. Intern. Med.166:2138 – 2144.
26. Musta AC, Riederer K, Shemes S, Chase P, Jose J, Johnson LB, Khatib
R.2009. Vancomycin MIC plus heteroresistance and outcome of methi-cillin-resistantStaphylococcus aureusbacteremia: trends over 11 years. J. Clin. Microbiol.47:1640 –1644.
27. Lodise TP, Graves J, Evans A, Graffunder E, Helmecke M, Lomaestro
BM, Stellrecht K.2008. Relationship between vancomycin MIC and
fail-ure among patients with methicillin-resistantStaphylococcus aureus bac-teremia treated with vancomycin. Antimicrob. Agents Chemother.52:
3315–3320.
28. Holmes NE, Johnson PD, Howden BP. 2012. Relationship between
vancomycin-resistantStaphylococcus aureus, vancomycin-intermediateS.
aureus, high vancomycin MIC, and outcome in seriousS.aureus infec-tions. J. Clin. Microbiol.50:2548 –2552.
29. Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan
SL, Karchmer AW, Levine DP, Murray BE, Rybak MJ, Talan DA,
Chambers HF.2011. Clinical practice guidelines by the Infectious
Dis-eases Society of America for the treatment of methicillin-resistant Staph-ylococcus aureusinfections in adults and children: executive summary. Clin. Infect. Dis.52:285–292.
30. Kish MA.2001. Guide to development of practice guidelines. Clin. Infect.
Dis.32:851– 854.
31. Moise-Broder PA, Forrest A, Birmingham MC, Schentag JJ. 2004.
Pharmacodynamics of vancomycin and other antimicrobials in patients withStaphylococcus aureuslower respiratory tract infections. Clin. Phar-macokinet.43:925–942.
32. Fry Moyer A, Guglielmo BJ, Hersh AL.6 May 2013. Desired vancomycin
trough serum concentration for treating invasive methicillin-resistant staphylococcal infections. Pediatr. Infect. Dis. J. [Epub ahead of print.] doi:10.1097/INF.0b013e318299f75c.
33. Alos JI, Garcia-Canas A, Garcia-Hierro P, Rodriguez-Salvanes F.2008.
Vancomycin MICs did not creep inStaphylococcus aureusisolates from 2002 to 2006 in a setting with low vancomycin usage. J. Antimicrob. Che-mother.62:773–775.
34. Pitz AM, Yu F, Hermsen ED, Rupp ME, Fey PD, Olsen KM.2011.
Vancomycin susceptibility trends and prevalence of heterogeneous van-comycin-intermediateStaphylococcus aureus in clinical methicillin-resistantS.aureusisolates. J. Clin. Microbiol.49:269 –274.