Pharmaceutical Society of South Africa
PSSA Conference 2018
Part 1
Highlights from the conference –
our erudite speakers introduce some of the topics discussed
NHI: The pharmacist’s
role – Stéphan Möller
Delegates were given an overview of the progress made towards an historic collaboration involving pharmacists working in all sectors of the profession, as well as the professional organisations that represent their interests.All stakeholders in the pharmacy profession recognise the importance of identifying the role that they can play in the delivery
of pharmaceutical services to the nation when National Health Insurance (NHI) is introduced as a funder for universal health care. The NHI Pharmacy Stakeholders Forum is an inclusive forum that gives a voice to pharmacists in all practice areas.
Members of the NHI Pharmacy Stakeholders Forum include representatives of local and multinational manufacturers, pharmaceutical wholesalers and distributors, community pharmacies (including courier, corporate and independent community pharmacies), private institutional pharmacies, information technology, academia and several pharmacists’ associations. Naturally, the National Department of Health and the statutory bodies are integral to the discussions.
While the primary objective of the Forum is to promote the inclusion of appropriate pharmaceutical services within the NHI framework, there are a few secondary objectives. These are: • To use all available pharmaceutical healthcare professionals
and resources
• To achieve positive clinical outcomes at the best possible price • To improve on availability of essential medicines and
pharmaceutical care
• To enhance efficacy and equity
Stéphan Mõller focuses on capturing the essence of the presentations
• To propose an implementable plan
• To link available information to performance
• To develop the capacity for organisational change in pharmacies
The next step is that the Forum intends to appoint an independent contractor to shape a submission document that unites pharmacy across all disciplines.
Session – Practice innovations – targeting
special interests
1. Opportunities for pharmacists in delivering value in healthcare – Praneet Valodia
Three areas in which pharmacists may make their presence felt were identified – task shifting, harm reduction and health outcomes measurement.
Task shifting involves moving specific tasks that were traditionally performed by specific healthcare professionals to others with shorter training and fewer qualifications. Where appropriate, certain tasks can be
allocated to midlevel workers, such as pharmacist’s assistants and pharmacy technicians. This not only saves on costs but permits the pharmacist to spend more time on patient-centred activities. It is a more efficient use of existing human resources that has been recognised globally.
Harm reduction refers to policies and interventions to reduce the harmful consequences of alcohol, tobacco, marijuana and other psychoactive substance use. The intention is to reduce the risk of a harmful activity by using safer alternatives, e.g. the use of nicotine patches in smoking cessation. In some case, harm reduction may minimise the negative health impact of a risky activity without stopping it entirely.
Health outcome measurement is perhaps the single most powerful tool available to enable health care system reform. Valodia stressed that it is important that pharmacists should measure the value of their interventions in an objective and scientific way. He cited a method that was developed to measure the value of a clinical pharmacokinetic service in managing epileptic patients in public hospitals. When implemented, a study showed that seizure frequency was reduced by 65% and adverse events were reduced from 20,5% to 3,2% of patients. A similar approach could be followed for other interventions performed by hospital and community pharmacists and would demonstrate their value in their practices.
2. Peculiarities of radiopharmaceuticals – Judith Wagener
Judith Wagener is a scientist in the field of radiochemistry at the South African Nuclear Energy Corporation.
Radiopharmaceuticals are highly regulated, both as medicinal products and as radioactive substances intended as either diagnostic or therapeutic agents. It is not surprising therefore that application of two sources of control, i.e. Good Manufacturing
Practice (GMP) requirements and radiation safety regulations, may lead to conflicting situations. This can deter their development and clinical use. It must also be noted that GMP requirements were developed for large-scale and centralised manufacturing of medicinal products.
Because radiopharmaceuticals are fundamentally different, the GMP requirements are not always suitable for their production. Specific skills, such as radiation safety, and specialised knowledge of radionuclides and related organ targeting are required.
They are produced in small batch sizes and have a short shelf life after constituted. The short shelf life necessitates fast transportation and application to the patient. A direct implication is the pre-release before the completion of a sterility test. A better understanding and knowledge of the workable requirements in the production, the application and regulatory activities will benefit all parties and ultimately the end user.
Nuclear medicine teams are eager to have pharmacists as part of the group. They realise that the specialised handling of radiopharmaceuticals for advanced therapy and research can only be achieved using pharmacists as part of the team. Progress in nuclear medicine in South Africa, and postgraduate Radiopharmacy training will benefit Africa as a whole. Radiopharmacy is as challenging and varied as other specialist pharmacy disciplines. The qualified person responsible for releasing the radiopharmaceutical forms an integral part of the production and needs to be more clearly defined in the South African environment.
Although most guidelines make the disclaimer that all applicable regulations should be adhered to, a gap exists where no or very limited guidance is provided in the control of the manufacture of radiopharmaceuticals. Guidelines can be vague and do not specify the need for concessions that may be required to comply with all conflicting regulations governing this industry. Therefore, industry norms and concessions are required to ensure that radiopharmaceuticals are manufactured to the standards required and that the industry is regulated adequately and consistently.
Praneet Valodia
3. Dr Google – pharmacist’s friend or foe? – Nadine Butler
Patients are increasingly using the Internet to access health information. Yet pharmacists do not know whether to encourage or discourage this reliance on “Dr Google”.
Nadine and her students assessed the knowledge, attitudes and practices of community pharmacists towards patients using the Internet. While they acknowledged these patient
behaviours to be common, there was negativity and concern expressed about the wisdom of supporting their patients in this regard.
Ten common terms covering health issues and medicine use were identified. Each term was used in professional as well as layman’s language in English, Afrikaans and isiXhosa. Each was entered into 3 search engines (Google, Yahoo and Bing). The first 10 sites for each separate search (610 sites after duplicates removed) were assessed for credibility, accuracy, objectivity, design and readability.
Results showed that retrieved information in English and Afrikaans was generally valid in terms of the assessment criteria; the isiXhosa search terms did not return useable results. No significant differences in information retrieved were found when comparing the lay versus professional search terms. The different search engines did not provide significantly different results.
This study did not support the expressed fear that the Internet is rife with incorrect or misleading information. “Dr Google” can therefore be considered as a complementary source of health information for English and Afrikaans speaking patients. Pharmacists are encouraged to actively engage with patients thereby maximising the probability that their Internet search behaviours would be beneficial.
Session – Antimicrobial stewardship
1. Understanding South Africa’s antimicrobial consumption – Ruth Lancaster
South Africa (SA) is committed to combating antimicrobial resistance (AMR) including antibiotic resistance, and in 2014 published the AMR National Strategic Framework 2014-2024. A key objective of the strategy is enhancing surveillance of antimicrobial use (AMUse) in humans and animals in order to optimise policy decisions. As AMUse is a key driver of AMR, the creation of a consolidated,
representative view of AMR and AMUse in South Africa will assist in monitoring trends to evaluate the impact of the AMR Strategy Framework.
Four sources for antimicrobial use data in South Africa were reviewed, namely South African Revenue Services import data, South African Animal Health Association, Quintiles IMS data and the RSA Pharma database.
The extent of SAs consumption was compared to international levels, and the comparison of human versus animal consumption in the country was estimated. AMUse in the public sector was analysed using defined daily doses.
SA’s AMUse was found to be significantly higher than other countries, but similar to BRICS countries, which are increasing access to health services in their countries.
In 2014, 23% of imported antimicrobials were used for animal health, the remaining 77% in human health. This is in contrast to values reported in the United States of America, but similar to other low-middle-income countries. Out of the total antimicrobial consumption, humans consume 98% of all penicillins and streptomycins imported in the country.
Despite imitations in the data, an overview of AMUse in the country can be determined. The majority of AMuse is in humans, and methods to reduce this will impact on AMR. More analysis is needed to determine use in community versus hospital care, and if the standard treatment guidelines are being adhered to.
Sustainable and consistent sources of data for AMuse are critical to allow trend analysis and a view of the impact that any AMR interventions will have on antimicrobial use and AMR in the future.
2. Antimicrobial stewardship activities in a private hospital group – Shirley Leadbeater
The beginning of the end? Not on our watch! This is the message given by Shirley Leadbeater and her pharmacy team at the Life Healthcare group of private hospitals.
Nadine Butler
Ruth Lancaster
The group has four key focus areas – upskilling pharmacists, building a multidisciplinary team, system tools and reporting.
Pharmacists form the backbone of the AMS programme. Clinical or ward-based pharmacists practise AMS at the patient’s bedside, while dispensary-based pharmacists also play a critical role and can assess the ‘low-hanging fruit’ of AMS.
Successes of the programme include:
• An increase in antibiotic load during the study period was prevented, despite increased drug resistance
• 29% of clinical pharmacists’ interventions prevented or reduced the possibility of potentially severe adverse reactions, including potential organ damage or system failure
• 59% of interventions resulted in improved quality of patient care
• 12% of interventions improved convenience or compliance Cost impact of clinical pharmacist interventions:
• 70% of interventions led to a decrease in drug therapy costs (with a saving of 43%)
• 23% of interventions led to an initial increase in drug therapy costs but improved patient outcomes
• The balance related to a cost decrease due to generic or therapeutic substitution
• The intervention rate has shown a 57% improvement year on year
3. Antimicrobial stewardship activities in public health care facilities in Gauteng Province – Charlotte Maxeke Academic Hospital (CMAH) – Lungile Mabuza
Antimicrobial resistance is a major public health, clinical and economic issue facing our generation. A call has been made to
set up antimicrobial stewardship (AMS) teams at an institutional level to further this initiative. A study was undertaken to determine the extent of irrational use of antibiotics within the Charlotte Maxeke Johannesburg Academic Hospital, with 1068 beds and serving 4000 admitted patients and 95 000 outpatients per month. Objectives of the study included determining the
extent of AMS activities within the hospital and facilitating the establishment of an AMS committee for the hospital.
An audit of AMS activities relating to injectable antimicrobials was conducted, followed by cost analysis of the data. The study focused on intravenous antimicrobials prescribed for in-patients admitted to CMJAH. An audit was also conducted on motivational forms on restricted anti-microbial medications.
In particular, the audit motivations identified the need for education of staff. Of the 316 motivations examined, 78 forms (25%) had incomplete patient information. Five forms (1.5%) omitted the name of the anti-microbial requested. Fifty-two forms (16.5%) were submitted for antimicrobials that did not require any motivation, e.g. amoxicillin with clavulanic acid. Eight forms (2.5%) were either incorrect or outdated versions of the necessary form.
The actions taken after the audit will help to have more effective AMS. The AMS committee was formalised and endorsed by the hospital leadership. This committee will address issues relating to antimicrobial use, including prescribing and restricting use of certain antimicrobials. In addition, the committee will assist in evaluation and selection of antimicrobials for the CMAH formulary and will monitor resistance patterns. A more user friendly anti-microbial chart has now been developed by the committee, which will assist in motivation for restricted antimicrobials.
4. The ethics of antibiotic use in animal farming – Precious Ncayiyana
The unnecessary use of antimicrobials poses a global threat to human health by contributing to the Antimicrobial Resistance (AMR) development. Scientific evidence suggests that non-therapeutic use of antibiotics in animal farming is one of the main contributors to AMR in humans. Non-therapeutic in this context means that antibiotics are
routinely added to animal feed or drinking water to help animals gain weight faster and protect them from infectious diseases.
Ncayiyana performed a study to evaluate the ethical and scientific implications of non-therapeutic use of antibiotics in animal farming. The report also critiques O’Neill’s (2016) report on tackling drug-resistant infections globally. This report reflected the evidence found in analysis of 280 published papers that addressed AMR in agriculture.
The study found that the non-therapeutic use of antibiotics in animal farming contributes to AMR development and that it is not ethically justifiable for farmers to carry on farming with antibiotics non-therapeutically. The study also argues that intensive factory farming poses the greatest risk in the preservation of all classes of antibiotics because it is customary to use antibiotics where many animals are kept in close proximity for example, in pig and poultry farming.
The O’Neill report found a direct link between use of antibiotics routinely in animal farming and AMR development in humans. The report suggests ways to reduce the demand for antimicrobials in order to respond to the rapidly growing demand for antimicrobials because the frequency and quantities have a direct impact on resistance development. By restricting the use, the rate at which resistance occurs can be reduced.
Recommendations:
• An immediate ban use in animal farming of antibiotics deemed medically important for humans, e.g.
colistin, is necessary in order to prevent the spread of antibiotic resistance. • This however, must go hand in hand with
preparation for abandonment of intensive farming systems for a ban to be successful. • The study also recommends the adoption of O’Neill’s (2016) recommendations on tackling AMR. These include:
▫ Promotion of the development of new antibiotics, and making better use of existing ones
▫ Support for the innovation and uptake of rapid point-of-care diagnostics
▫ Improvement of global surveillance of drug resistance and antimicrobial consumption in humans and animals • A national public awareness campaign is justified by the threat
posed by AMR. Governments and other relevant stakeholders involved should formulate policies or frameworks to deal with the problem with the urgency it requires.
Session – Pharmaceutical health care delivery
under Universal Health Coverage
1. Distinguishing between different disease profiles in different communities in South Africa – Candy Day
Candy started her presentation with the chilling facts – we are all going to die, and the differences in how people live, fall ill and die can sometimes be hard to see from our perspective on the ground.
Measures of disease burden include:
• Disability-adjusted life years (DALYs)
• Years of life lost (YLLs), which
will indicate the leading causes of premature death • Mortality rates, including age-standardised mortality rates • Prevalence of disease in a population at a particular time The following data, and most of the tables, were obtained from the 2015/16 and 2016/17 issues of the District Health Barometer, which is produced by Health Systems Trust, and is currently funded by the National Department of Health.
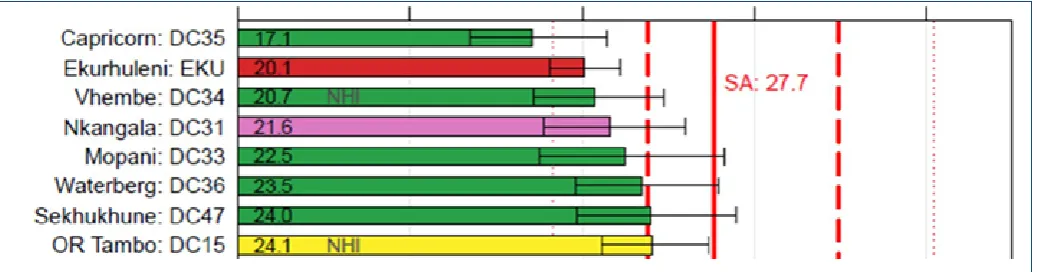
The leading single cause of death varies from district to district:
• HIV is the leading cause in most districts, but is ranked 3rd in
Namakwa and Overberg • TB is in 2nd place overall
• Cerebrovascular disease in individual districts varies from 3rd
to 9th place
Candy Day
• Diarrhoeal diseases are the 6th leading cause overall
• Malaria only shows up for Vhembe, in 20th place
• Cancers are less visible since each type is listed as a single cause
The National Income Dynamics Study (NiDS) is the only South African survey that enables estimation of disease prevalence at the district level. Based on measurements of blood pressure and self-reported use of antihypertensive medication in adults, hypertension has been identified as a major risk factor.
Opportunities to improve health services:
• Hypertension – strengthening the cascade of care ▫ Testing and diagnosis
▫ Treatment
▫ Effective treatment (control) • HIV testing coverage
• Deliveries to women under 18 years – contraceptive services, which will have an impact on maternal and perinatal conditions • Immunisation coverage
2. Vitality – A model of shared value – Deepak N Patel
Dr Patel is the Principal Clinical Specialist at Discovery Vitality. His presentation dealt with the health landscape, determinants of health behaviour, the role of behavioural economics in health, the Vitality programme and Vitality Research. South Africa has a quadruple burden of disease – diseases of poverty (such as gastroenteritis, pneumonia and malnutrition), accidents and violence (often related to alcohol and substance
abuse), HIV and AIDS, chronic diseases often related to lifestyle behaviour (e.g. hypertension, hyperlipidaemia, diabetes, lung diseases and cancer).
There is a high prevalence in the population of poor lifestyle factors which are associated with chronic diseases. The four main risk factors, which are poor nutrition, a sedentary lifestyle, smoking and alcohol, can lead to the four main non-communicable diseases, i.e.
diabetes, respiratory disease, cancer and cardiovascular disease. These four diseases account for 60% of all deaths worldwide. According to Dr Patel, humans are intended to be endurance athletes, but have evolved into beings with physical inactivity and sedentary behaviour. The development of labour-saving devices, such as electrical and electronic devices and the use of motorised transport, have resulted in the use of external energy at the expense of internal (physical) energy, which is one reason why lifestyle modification can benefit one’s health. Food choices that are now available may lead the person to choose the most convenient food rather than the healthiest.
He compared the underlying premises of decision making in a standard economics model and in a behavioural economic model.
Standard economics model Behavioural economics model
Humans make perfectly rational decisions if given sufficient information and if the price or incentives are right
Humans have bounded rationality
Decisions are intended to maximise their utility (satisfaction)
People may exhibit poor self-control
Time-consistent preferences Time inconsistent preferences Humans exercise maximum self-control People are prone to biases
Fig. 2 – comparison of underlying premises of decision making
Similarly, the architecture of two systems of cognition, i.e. intuition vs reasoning, were compared.
Intuition – Want Reasoning –Should
Fast Slow
Automatic Controlled
Effortless
Emotional Deliberative
Governed by habit Value-based
Fig. 3 – The architecture of two systems of cognition
Some of the stimuli that encourage people to make unhealthy choices are:
• Time preferences– people tend to delay the implementation of decisions that are in their long-term interests for decisions that provide immediate gratification.
Deepak Patel
• Other people’s behaviour – people do many things by observing others and copying them; people are encouraged to continue to do things when they feel other people approve of their behaviour. Individuals are more likely to model behaviour observed in people with whom they can identify, such as peer groups.
• The power of the media and advertising unhealthy choices must not be underestimated.
• Habits are comfortable and familiar.
• People tend to be overconfident and overestimate their abilities and health status – “I can stop smoking/drinking any time I like.”
• Over-weighing of small probabilities, such as aeroplane crashes, and under-weighing of high probabilities, such as the consequences of smoking, alcohol, poor nutrition and lack of exercise.
• Individuals tend to maintain a current state even when the adoption of alternate options is likely to lead to better outcomes.
The bottom line is that people often know what is in their long-term interest but have difficulty in implementing decisions in the present to enhance those interests.
The Vitality Wellness Programme uses behavioural economic principles to drive change in key areas of health risk, such as physical inactivity, poor nutrition and smoking. It does not infringe on the right of individuals to make unhealthy choices.
Vitality provides access to partners that lowers the barriers to healthy choices and incentivises ongoing engagement. This includes a physical activity platform, rewards for making healthy food choices and easy access to preventive health screening.
Research into the outcomes attained by members who make use of the opportunities shows results are positive. It has been shown that, depending on the degree of engagement with the programme, the number of hospital admissions, the duration of
the stay in hospital and the cost per patient can all be significantly reduced.
The Vitality programme demonstrates that medical scheme members can be incentivised to make beneficial choices.
3. Possible health promotion ideas for own practices
Three possibilities were presented to delegates. a. National Asthma Education Programme (NAEP)
– Riaz Khan
The NAEP is a non-profit organisation that aims to disseminate impartial information about asthma diagnosis and treatment to health professionals and the South African public. It is part of an international drive which subscribes to management guidelines set out by GINA (Global Initiative for Asthma), SATS (South African Thoracic Society) and ALLSA (Allergy Society of Asthma). Objectives of NAEP
i. To raise awareness among patients, health professionals and the public that asthma is a serious chronic disease ii. To ensure that symptoms of asthma are recognised by
patients, families, and the public, and that appropriate diagnosis is made by health professionals
iii. To ensure effective control of asthma by encouraging a partnership among patients, physicians and other health professionals, using appropriate, modern treatment and education programmes
The SA Certificate in Asthma Care is a six-month learning course which runs from March each year. The course is widely applicable to a variety of personnel but is particularly useful for primary healthcare professionals, such as community pharmacists and nurses, who come into frequent contact with asthma patients. Candidates are accepted from both the public and private health sectors.
b. Five-day advanced course in diabetes – Michael Brown Michael Brown, Head: Education /
Media and Publishing, at the Centre for Diabetes and Endocrinology, quoted Congressman Earl L “Buddy” Carter, who said “Today, as before, many pharmacists provide patient-centred services like medication coordination, medication management, patient education, and more. We are the front line of the health care team and often see patients more than any other provider. Pharmacists
Vitality – a model of shared value
Riaz Khan
have become the most over-trained and under-utilised professionals in America.”
The five-day course offered by the CDE offers a unique approach to diabetes focussed on principles, insights and understanding. It is a journeyof discovery starting with the practitioner.
• Reflection • Self-awareness • Insight • Mindfulness • Chronicity
• Clarification of attitudes, values, beliefs & personality traits The topics covered begin with basic physiology of food metabolism and hormone action and progress through diagnosis, classification and pathophysiology of diabetes. Topics of interest to all healthcare professionals include prevention and management of diabetes, including acute complications, but of interest are other topics that pharmacists may not initially consider to be important to themselves. These include the patient’s psychological adjustment to diabetes and the importance not only of nutrition but also of exercise. The importance of integrated care by an appropriate multidisciplinary team is emphasised. This includes endocrinologists, biokineticists, podiatrists, psychologists and dieticians. Pharmacists may play an important role in this team, particularly when it comes to pharmacotherapy.
c. Higher Certificate in Vaccinology Qualification – Hannelie Meyer
The South African Vaccination and Immunisation Centre is a public-private-academic alliance between the National Department of Health (NDoH), the vaccine industry, academic institutions and other stakeholders, with its activities undertaken in close collaboration with the NDoH, the Network for Education and Support in Immunisation (NESI), the World Health Organisation and its partners. It is hosted by
the School of Pharmacy at Sefako Makgatho Health Sciences University.
The Higher Certificate in Vaccinology has been accredited by the South African Qualifications Authority and is endorsed by the Health Professions Council of South Africa. It is a basic introductory programme for in-service healthcare workers to equip them with the theoretical knowledge and practical expertise necessary for running an up-to-date EPI-SA (Expanded Programme on Immunisation) clinic.
While there is currently no officially required accreditation for administration of vaccines by pharmacists, it must be remembered that the so-called Ethical Rule 22 requires pharmacists to provide only professional acts for which he/she is adequately trained and
sufficiently experienced. This course, which is delivered mainly on-line but with contact session workshops for practical assignments, meets those requirements. Remember that the pharmacist’s role in immunisation does not stop with supplying and administering the vaccination.
Access to appropriate pain relief in palliative care – developing a suitable indicator – Andy Gray
Palliative care is the holistic multi-disciplinary care of a patient and family affected by a life limiting or life threatening illness and is applicable from the time of diagnosis for all adults and children across the life span and includes bereavement care for the family.
Following the World Health Assembly’s resolution in 2014 to strengthen palliative care as a component of comprehensive
care throughout the life course, it was important for South Africa to develop a strategy to achieve this. South Africa’s National Policy Framework and Strategy on Palliative Care 2017 – 2022 was published in late 2017. Among other actions, it calls for the development of a national morphine monitoring system. The vision of the policy is that “all adults and children, including their families, facing the problems associated with life threatening or life limiting illness will receive palliative care to maintain quality of life, dignity and comfort as well as manage painthroughout the course of the illness.”
One of the indicators suggested for this monitoring system is the total number of mg of morphine issued per 100 combined primary healthcare and out-patient head count, per district, reported quarterly or annually. The feasibility of the proposed indicator was assessed using data from the KwaZulu-Natal Provincial Medicines Procurement Unit (PMPU), combined with denominator data from the District Health Information System (DHIS). The DHIS uses data from hospitals, community health clinics and primary healthcare
Hannelie Meyer
clinics and provides workload statistics and population estimates. The KwaZulu-Natal PMPU provided opioid issue data, i.e. total number of mg of morphine issued per quarter, combining all oral solid dosage forms, pack sizes and strengths and oral morphine powder, for 2016 for 10 districts. This data showed marked variability, from 2.8mg per 100 ambulatory care presenters per year in Umzinyathi to 156.2 in uMgungundlovu.
Disaggregating these data by age groups, and other “vulnerable” groups (e.g. gender, income quintiles, urban/rural and specific diagnoses), remains challenging. Other challenges include expanding to district-level as soon as possible, tracking access per facility and incorporating private sector and non-governmental organisation (hospice) data.
This study showed that existing public sector utilisation and denominator data can be efficiently combined to portray a measure of access to an important analgesic in palliative care, and can be the stimulus for interventions to improve such access.
Pharmacists can use appropriate pharmacoepidemiological tools to document access to medicines over time, and between important sub-populations. Under NHI, it will be important to ensure that all service provision with health districts is captured, so that the implementation of critical national policies and initiatives can be tracked.
The remainder of the presentations will be included in the next issue of the SAPJ.
The PSSA/Alpha Pharm distance learning
programme 2018
The PSSA/Alpha Pharm Distance Learning Programme continues to offer pharmacists useful, practical, up-to-date information that enables them to provide optimal pharmaceutical care to their patients.
Module 4/2018 – Anxiety disorders
Everyone occasionally experiences fear and anxiety. Fear is an emotional, physical and behavioural response to an immediately recognisable external threat, while anxiety is a distressing, unpleasant emotional state of nervousness and uneasiness and its causes are less clear. There is also a difference between anxiety and stress. While most people can cope with a certain amount of stress, anxiety is a disorder that requires management.
Anxiety occurs in a wide range of physical and mental disorders,
but it is the predominant symptom in an anxiety disorder. Anxiety disorders (e.g. panic disorder, social anxiety disorder and generalised anxiety disorder) are the most prevalent psychiatric disorders and are associated with a high burden of illness. They can affect nearly 30% of adults at some point in their lives. Anxiety disorders are often under-recognised and under-treated in primary care.
This module discusses the more frequently occurring anxiety disorders, including panic disorder, social anxiety disorder and generalised anxiety disorder and their management.
For more information about this programme contact Gill or Glynis at Insight Medicine Information on 011 706 6939 or email: [email protected].
The PSSA/Alpha Pharm clinical education
programme 2018 for pharmacy staff
The PSSA/Alpha Pharm Pharmacy Staff Clinical Education Programme continues to offer front-shop assistants or pharmacist’s assistants up-to-date information that enables them to provide optimal pharmaceutical care to their patients. All pharmacy staff need to be familiar with the use of unscheduled medicines and should be reminded of when it is necessary to refer the patient to the pharmacist.
Module 4/2018 – Common hair and scalp
conditions
Our skin and hair are important parts of our body image. For many people, loss of hair or other visible scalp conditions can cause
immense distress, and sensitivity is required when dealing with these problems.
This module discusses common scalp and hair problems that may present in the pharmacy and the ways in which to manage these conditions. Common types of hair loss in men and women as well as how to deal with head lice, cradle cap and dandruff are discussed.
Reflections on the duties of the President
Sarel MalanImmediate Past President of the PSAA
This was indeed the pinnacle of my career in service of pharmacy. It was also the greatest honour to have this opportunity and to work alongside people with a passion for the profession. I always tried to serve with the patience, wisdom and dignity this position requires – where I have failed, I sincerely apologise.
When I started in this position, I stated
that my goal in life is to have made a difference and that I believed that this could be done by doing the right thing, in the right way, at the right time and for the right reason. As Natie Finkelstein pointed out to me many years ago, ‘it is not enough to do things right, you also have to do the right things’.
I have always believed, and still do, that there is only one way to change our profession and the PSSA and that is from the inside. The egg that breaks from the inside brings new life – if it is broken from the outside, it is the end of life.
This goes hand in hand with the fact that I have never seen myself as a revolutionary. For me, the answer would always be evolution – no need to throw everything out and start anew, rather review and enhance what works, or what is necessary, and build on that. Using our knowledge wisely, taking the appropriate actions and capitalising on our unique skills set is how the pharmacists can and will make a living and a life.
We must admit that one of our biggest problems currently lies in the way that the profession and pharmacists are perceived. We are reminded of the Marcus Aurelius quotation, “Everything we hear is an opinion, not a fact. Everything we see is a perspective, not the truth” and the Talmudic words, “We do not see things as they are. We see things as we are”. This is relevant not only to the public but also in the role that Department of Health sees for the pharmacist. For pharmacy to succeed, we will need to change perceptions. That is only possible by showing what pharmacists can contribute and then not only publishing it, but also promoting it. If it is not published, it never happened and will never be acknowledged. In this we must accept that science informs practice, but that it is just as important that practice informs science – this will determine the future scientific and educational development, and thus practice.
In addition to changes and developments, our patients or clients have evolved, or maybe regressed, into health consumers, ever expecting more, wanting it all in terms of expertise and
dispensing and clinical services, whilst demanding convenience and accessibility. The pharmacist of the future will thus need to be some kind of accessible wizard – a combination of a scientific professional and tech guru or IT specialist – able to take a specific place in society, knowing or having access to his/her patients’ medical histories, providing basic care for minor ailments using appropriate medicines, deciphering or interpreting data from health technology and wearables, and providing advice on lifestyle and medication based on this data. In addition, all of these will have to be done with the emphasis on wellness and preventing disease or illness.
With this said, the strength of pharmacy has always been its strong scientific basis and this has been enhanced by the more recent patient focussed education. In the words of two past FIP presidents (Mitsura Hashida and Kamal Midha): The pharmacist is (and has) to remain the scientist in the community’ and “A molecule becomes a medicine (only) when it passes through the hands of a pharmacist”.
It is time for innovation, and maybe even disruptive innovation, in our profession. We must deliver products and services that are not only better and less expensive, but more creative, useful, with a wider impact and ultimately scalable to enable service where it was not possible previously. It is thus not only about meeting current needs, but also anticipating unstated or future needs. This is only possible when you clearly know what your purpose and core business really are.
It might be time to overturn the apple cart, but on our own terms – for too long the best apples, the most important and best things we as pharmacists can do, have been hidden at the bottom of our carts, never seeing the light of day, never being recognised. We know what we have, we know what we are capable of and how we can make a difference – now we just have to find our strength, which is and will depend on unity. To quote Kipling – “… the strength of the pack is the wolf, and the strength of the wolf is the pack”.
In South Africa we are doubly blessed for not only can we count on “Strength in Unity”, but we also have “Unity in Diversity’” as depicted in our National Coat of Arms. To take it even further, we just have to add purpose and that we have in the base scroll of the PSSA, “Pro Salute et Valetudine Populi” which translated to English is “For the health and well-being of the people”.