P
EDIATRICS
May 1999VOL. 103 NO. 5
zzz
zzz
zzz
zzz
zz
In Which Journals Will Pediatricians Find the Best Evidence for
Clinical Practice?
Catherine S. Birken, MD*, and Patricia C. Parkin, MD, FRCPC*‡
ABSTRACT. Objective. The objective of this study was to identify the journals that contain the best evi-dence relating to clinical pediatric practice, thus enabling general pediatricians and pediatric trainees to identify the best quality evidence more efficiently and to select journals for general reading more judiciously.
Methods. In the first of three strategies, journal cita-tions from completed systematic reviews using topic headings of pediatric(s), child, infant(s), newborn, neo-nate(s), neonatology, and adolescent(s) in the Cochrane Database of Systematic Reviews (CDSR) in the 1997, Issue 4, Cochrane Library were collected. In the second strategy, journal citations from American Academy of Pediatrics’ (AAP) policy statements from 1994 to 1996 found in the AAP policy reference guide were collected. In the third strategy, journal citations from the Canadian Paediatric Society (CPS) statements from 1990 to 1997 found inPediatrics and Child Healthwere collected. Top-ics related to tertiary neonatology, nonphysician health care professionals, public health policy, ethics, and non-journal citation sources were excluded. All statements with no references were excluded. Journal citations in CDSR with no pediatric subjects and citation of AAP policy statements cited in AAP policy statements were excluded. The number of citations from the journal cited most frequently, from journals that represented;10% of all citations and from the 10 journals cited most fre-quently were expressed as a percent of total citations and a 95% CI was calculated.
Results. Using all three strategies (CDSR, AAP, and CPS), the journal cited most frequently wasPediatrics. Using the CDSR strategy (n5234), citations from Pedi-atricsrepresented 6.0% of the total (95% CI: 3.0%, 9.0%), using the AAP strategy (n5930), citations from
Pediat-ricsrepresented 11.4% of the total (95% CI: 9.4%, 13.4%), and using the CPS strategy (n 5 873), citations from
Pediatrics represented 11.9% of the total (95% CI: 9.8, 14.1). Using the CDSR strategy, citations from the 10 journals cited most frequently made up 38.9% of the total citations (95% CI: 32.7%, 45.1%), using the AAP strategy, citations from the 10 journals cited most frequently made up 42.3% of the total citations (95% CI: 39.3%, 45.3%), and using the CPS strategy, citations from the 10 journals cited most frequently made up 60.6% of the total citations (95% CI: 57.4, 63.8). In the CPS strategy, citations from the
Journal of Pediatricsrepresented 10.2% of the total cita-tions (95% CI: 8.2, 12.2) and citacita-tions fromNew England Journal of Medicinerepresented 9.5% of the total citations (95% CI: 7.6, 11.5). A total of 7 journals were found to be among the 10 cited most frequently using all three strat-egies (in alphabetical order): Archives of Diseases in Childhood,British Medical Journal,Journal of the Amer-ican Medical Association, Journal of Pediatrics, Lancet,
New England Journal of Medicine, andPediatrics.
Conclusions. This study provides the general pedia-trician and pediatric trainee with a strategy to identify efficiently a significant proportion of the best evidence on pediatric practice by restricting searches and reading to a limited number of journals. It also highlights the fact that the best quality evidence on pediatric practice is found in a large number of medical journals.Pediatrics
1999;103:941–947;evidence-based medicine, medical educa-tion, clinical pediatrics, information services, biblio-metrics.
ABBREVIATIONS. CDSR, Cochrane Database of Systematic Re-views; AAP, American Academy of Pediatrics; CPS, Canadian Paediatric Society, HIV, human immunodeficiency virus.
T
he daily care of patients, the continuing
edu-cation of practicing physicians, and the
educa-tion of physicians-in-training is dependent on
the ability of the clinician to access, critically
ap-praise, and incorporate medical evidence into clinical
practice. Evidence-based medicine is a process of
lifelong, self-directed learning that begins with the
conversion of clinical and health care information
From the *Department of Pediatrics, University of Toronto Faculty of Medicine; and the ‡Division of Pediatric Medicine, the Hospital for Sick Children, and the Hospital for Sick Children Research Institute, Toronto, Ontario, Canada.
Received for publication; accepted Oct 2, 1998.
needs into answerable questions and the efficient
identification of the best available evidence with
which to answer them.
1The series of articles entitled
Users’ Guide to the Medical Literature
2teaches
physi-cians to translate the results of medical research into
clinical practice using critical appraisal. However,
strategies on the efficient identification of evidence
worthy of appraisal are limited.
As the body of medical research continues to
grow, it is becoming increasingly difficult to assess
all available literature on a given topic efficiently.
One approach to the proficient identification of
po-tentially sound medical evidence worthy of critical
appraisal is the delineation of the journals that are
most likely to publish manuscripts of high quality.
The objective of this study was to identify the
jour-nals that contain the best evidence relating to clinical
pediatric practice.
METHODS
A method to identify journal articles containing the best evi-dence for clinical pediatrics was developed. We hypothesized that a source of systematic reviews of the medical literature would provide a database containing the highest quality journal articles. We hypothesized further that a source of statements developed by consensus and endorsed by a national professional organization would provide a database containing high quality journal articles. To ensure validity of these hypotheses and to provide adequate citation sample size, several data sources were sought.
Three data sources that contain citations of high quality journal articles were identified: the Cochrane Database of Systematic Re-views (CDSR), the American Academy of Pediatrics (AAP) policy statements, and the Canadian Paediatric Society (CPS) statements. We hypothesized that the journal citations found in these sources represented the best medical evidence available, and therefore a ranking of journals based on citation frequency closely repre-sented a ranking of journals containing the best available evidence on clinical pediatric practice.
The Cochrane Collaboration is an international network of individuals helping to prepare, maintain, and disseminate system-atic reviews on the effects of health care.3Systematic reviews are reviews of international literature on a specific topic that are undertaken by designated collaboration review groups who use stringent and explicitly defined standards of critical appraisal. Although the review citations consist primarily of randomized, controlled trials, specific methods for literature review and refer-ence inclusion are discussed in each systematic review. The re-views are found in the CDSR, an electronic database that is up-dated quarterly.
The AAP policy statements found in thePolicy Reference Guide of the American Academy of Pediatrics4 are issued by the AAP, reviewed every 3 years by the authoring body, and revised or reaffirmed by the board of directors.
The CPS statements, found in the CPS statement book5and published currently inPediatrics & Child Health, the Journal of the
Canadian Paediatric Society, are prepared by 17 ad hoc CPS com-mittees and are approved by the board of directors.
This study used a survey design to identify the total number of journal citations found in systematic reviews on pediatric topics in the CDSR, AAP, and CPS. To obtain the required number of citations (noted below), it was necessary to include citations from the AAP policy statements for the 3-year period of 1994 through 1996 and from the CPS statements for the 8-year period 1990 to 1997.
In the CDSR strategy, a search in 1997 CDSR, Issue 4, was performed using topic headings pediatric(s), child, infant(s), new-born, neonate(s), neonatology, adolescent(s), and adolescence. The total number of journal citations, delineated as they were in-cluded, were tabulated manually and sorted by journal title.
In the AAP strategy, journal citations from the AAP policy statements from 1994 to 1996 found in theAAP Policy Reference Guidewere tabulated manually and sorted by journal title, and in the CPS strategy, journal citations from the CPS statements from 1990 to 1997 were tabulated manually and sorted by journal title. The purpose of this study was to identify the journals that contain the best evidence relating to clinical pediatric practice. This required exclusion of many topics, including topics related to tertiary neonatology, nonphysician health care professionals, pub-lic health popub-licy, and ethics. Nonjournal citation sources also were excluded. Journal articles in CDSR without pediatric subjects and citations of AAP policy statements cited in AAP policy statements were excluded. CPS statements with no references were excluded. Exclusions were identified independently by the two investigators (C.S.B. and P.C.P.) and discrepancies were resolved jointly. Non-English language journal citations were tabulated separately and excluded from the primary analysis.
A sample size calculation was performed. With no evidence on which to base a sample size estimate, a post hoc power calculation was undertaken after completion of the CDSR strategy (n5234). Power was,80%, and a sample size requirement was reestimated. To ensure that the journal cited most frequently contributed 10% 6 2% of the total citation, with 95% CI, a strategy that included 864 citations was required. Citations from the AAP and CPS datasets were added to the original CDSR citations to ensure that.864 citations were available for analysis.
Descriptive statistics were used to analyze the data. The num-ber of citations from the journal cited most frequently, from jour-nals that represented 10% of all citations, and from the 10 jourjour-nals cited most frequently were expressed as a percent of total citations and a 95% CI was calculated.
RESULTS
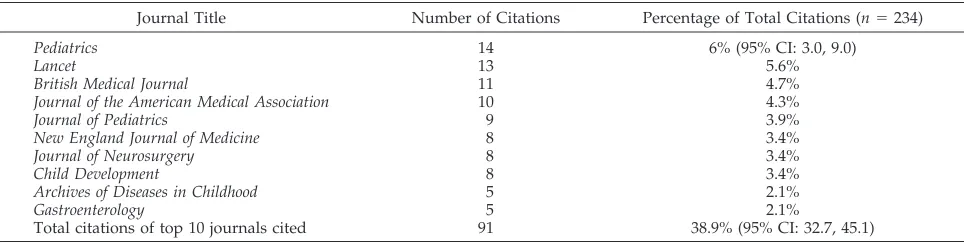
In the CDSR strategy, 31 systematic reviews were
included (“Appendix”) and 96 were excluded
(“Ap-pendix”). A total of 234 citations were recruited from
the included systematic reviews. Citations from the
10 journals cited most frequently made up 38.9%
(95% CI: 32.7%, 45.1%) of the total citations (Table 1).
A total of 6% of all CDSR citations were from
non-English language journals.
In the AAP strategy, 58 AAP policy statements
were included (“Appendix”) and 71 were excluded
TABLE 1. Top 10 Journals Cited: CDSR Strategy
Journal Title Number of Citations Percentage of Total Citations (n5234)
Pediatrics 14 6% (95% CI: 3.0, 9.0)
Lancet 13 5.6%
British Medical Journal 11 4.7%
Journal of the American Medical Association 10 4.3%
Journal of Pediatrics 9 3.9%
New England Journal of Medicine 8 3.4%
Journal of Neurosurgery 8 3.4%
Child Development 8 3.4%
Archives of Diseases in Childhood 5 2.1%
Gastroenterology 5 2.1%
(“Appendix”). A total of 960 citations were recruited
from the included policy statements. Citations from
the 10 journals cited most frequently made up 42.3%
(95% CI: 39.3%, 45.3%) of the total citations (Table 2).
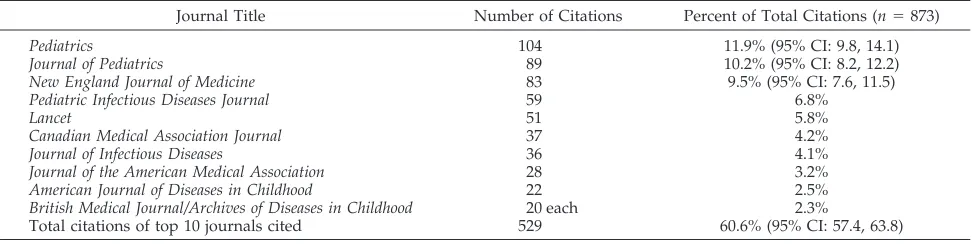
In the CPS strategy, 46 CPS statements were
in-cluded (“Appendix”) and 16 were exin-cluded
(“Ap-pendix”). A total of 873 citations were recruited from
the included CPS statements. Citations from the 10
journals cited most frequently made up 60.6% (95%
CI: 57.4, 63.8) of the total citations (Table 3).
Using all three strategies (CDSR, AAP, and CPS),
the journal cited most frequently was
Pediatrics
(10.8% of all citations). Using the CDSR strategy,
citations from
Pediatrics
represented 6.0% of the total
(95% CI: 3.0%, 9.0%) (Table 1); using the AAP
strat-egy, citations from
Pediatrics
represented 11.4% of the
total (95% CI: 9.4%, 13.4%) (Table 2); and using the
CPS strategy, citations from
Pediatrics
represented
11.9% of the total (95% CI: 9.8, 14.1) (Table 3).
In the CPS strategy, citations from the
Journal of
Pediatrics
represented 10.2% of the total citations
(95% CI: 8.2, 12.2), and citations from
New England
Journal of Medicine
represented 9.5% of the total
cita-tions (95% CI: 7.6, 11.5) (Table 3). In the CPS strategy,
British Medical Journal
and
Archives of Diseases in
Childhood
each contributed 20 citations, making a
total of 11 journals cited most frequently. Only 20
citations were used in the data analysis.
Seven journals were found to be among the 10
journals cited most frequently using all three
strate-gies (in alphabetical order):
Archives of Diseases in
Childhood, British Medical Journal, Journal of the
Amer-ican Medical Association, Journal of Pediatrics, Lancet,
New England Journal of Medicine,
and
Pediatrics.
A total of three additional journals were found to
be among the 10 cited most frequently using two of
the strategies (in alphabetical order):
American
Jour-nal of Diseases of Childhood
,
Journal of Infectious
Dis-eases
, and
Pediatric Infectious Diseases Journal
.
DISCUSSION
The results of this study demonstrate that a large
proportion (
;
40% to 60%) of the best medical
evi-dence for clinical pediatric practice can be found in a
small number of medical journals. These findings
have future ramifications for practicing pediatricians
and pediatric trainees. Users of Medline and other
electronic databases may choose to restrict their
searches to the top journals cited in the CDSR, AAP,
and CPS strategies, thus aiding in the efficient
iden-tification of high quality evidence worthy of critical
appraisal. This potential implication is even more
poignant as of 1998, because Medline users no longer
have the option to limit searches to the
Abridged Index
Medicus
. Additionally, the results of this study may
help guide pediatricians-in-training to judiciously
se-lect journals for general reading.
This study also highlights the fact that the best
quality medical evidence in pediatric practice is
found in a large number of diverse journals, proving
that no one journal has a monopoly on sound
med-ical evidence. Other issues highlighted in this study
include the poor use of international medical
evi-dence in North American clinical medicine. For
ex-ample, 6% of all citations in CDSR were in languages
other than English. No non-English language studies
were cited in the AAP policy statements or the CPS
statements reviewed.
We hypothesized that using a data source of
sys-tematic reviews (such as the CDSR) and statements
developed by consensus (such as the AAP and CPS
policy statements) would provide a database
con-TABLE 3. Top 10 Journals Cited: CPS Strategy
Journal Title Number of Citations Percent of Total Citations (n5873)
Pediatrics 104 11.9% (95% CI: 9.8, 14.1)
Journal of Pediatrics 89 10.2% (95% CI: 8.2, 12.2)
New England Journal of Medicine 83 9.5% (95% CI: 7.6, 11.5)
Pediatric Infectious Diseases Journal 59 6.8%
Lancet 51 5.8%
Canadian Medical Association Journal 37 4.2%
Journal of Infectious Diseases 36 4.1%
Journal of the American Medical Association 28 3.2%
American Journal of Diseases in Childhood 22 2.5%
British Medical Journal/Archives of Diseases in Childhood 20 each 2.3%
Total citations of top 10 journals cited 529 60.6% (95% CI: 57.4, 63.8) TABLE 2. Top 10 Journals Cited: AAP Strategy
Journal Title Number of Citations Percent of Total Citations (n5960)
Pediatrics 106 11.4% (95% CI: 9.4, 13.4)
Journal of Pediatrics 63 6.8%
New England Journal of Medicine 45 4.8%
Journal of the American Medical Association 42 4.5%
Journal of Infectious Diseases 35 3.8%
American Journal of Diseases in Childhood 30 3.2%
Pediatric Infectious Diseases Journal 21 2.3%
Lancet 20 2.3%
British Medical Journal 18 1.9%
Archives of Diseases in Childhood 13 1.4%
taining the highest quality journal articles. Other
data sources, such as review articles or journals,
could be used in this method. However, we
hypoth-esized that such sources may contain journal articles
that had undergone less rigorous critical appraisal by
single authors.
The unique methodologic approach used in this
study to the identification of high quality medical
journals represents an alternate method to evaluate
journals, compared with the use of impact factors.
The impact factor, developed by the Institute for
Scientific Information and published in the
Journal
Citations Reports
, is a measure of the frequency with
which the average article in a journal has been cited
in a particular period.
6The applications of journal
impact factors include market research for
publish-ers, management of library journal collections, and
controversial application of academic evaluation.
7One of the implications of impact factors is the
infer-ence that journals with high impact factors publish
the best studies. Journal impact factors should not be
used to evaluate the quality of articles published in a
particular journal, because they are dependant on the
research field of the journal. They are not
represen-tative statistically of individual journal articles,
8and
even the method of calculating impact factors may be
misleading.
9There are some limitations in the study. The
sources of journal citations, namely the CDSR, AAP,
and CPS statements may not always cite the best
available medical evidence. The Cochrane
Collabo-ration that seems to be a gold standard of sources of
journal citations has set guidelines outlining
inclu-sion criteria of articles for review, but how closely
these are adhered to is unknown. The AAP policy
statements and CPS statements have no explicit
guidelines for article inclusion and are not
peer-reviewed. Although it is evident that the CDSR is
more likely to cite evidence of high quality, there are
a limited number of reviews on pediatric topics. In
addition, there is no apparent strategy by the
Co-chrane Collaboration, the AAP, or the CPS for
select-ing pediatric topics for review. This may explain the
inclusion of certain subspecialty journals because of
the overrepresentation of certain review topics.
Ad-ditionally, any research strategy using citation
fre-quency may have methodologic problems such as
reference accuracy
10and publication biases.
11How-ever, there was little variation in the results of the
three strategies, suggesting that the use of the CDSR,
AAP policy statements, and CPS statements may be
valid. Finally, the purpose of this study was to
iden-tify the journals that contain the best evidence
relat-ing to clinical pediatric practice. This required
exclu-sion of many topics as discussed in “Methods”. The
exclusion of these topics probably biased the results
away from some journals and toward others.
Inves-tigators may choose to replicate the methods used in
this article modifying the topics included in the
search. This may be used to identify the journals that
contain the best evidence relating to other medical
specialties such as subspecialty pediatrics or public
health policy.
Despite these limitations, strategies to allow
med-ical practitioners to identify quality medmed-ical evidence
efficiently and judiciously are necessary in the
cur-rent medical environment in which the body of
sci-entific literature is growing rapidly and the use of
evidence-based medicine in medical decision making
is fundamental.
APPENDIX
CDSR Strategy: Included Systematic Reviews
• Adherence with medications
• Amodiaquine for the treatment of malaria • Antiepileptics after brain injury
• Antibiotics for acute bronchitis • Antibiotics for sore throat • Barbiturates in severe brain injury • Breastfeeding technique
• Breastfeeding and discharge times • Breastfeeding and early contact • Chambers/nebulizers, acute asthma • Clozapine for schizophrenics
• Combined inhaled anticholinerics andbagonists • Crohns: induction remission, AZA, or 6-MP • Crohns: maintenance azathioprine
• EMLA to reduce circumcision pain • Family therapy for childhood asthma • Feeding schedule for neonates in hospital • Health and welfare effects of preschool day care • Home-based maternal support
• Infants’ sleep patterns and feeding • Maternal antigen avoidance as treatment • Maternal antigen avoidance in pregnancy • Oral steroids in cystic fibrosis
• Physician advice for smoking cessation
• Ribavirin for respiratory syncytial virus lowers respiratory tract infection
• Steroids and asthma relapse
• Steroids in acute traumatic brain injury • Treating scabies
• Treatments for acute otitis media
• Ulcerative colitis: induction remission, 5-ASA • Ursodeoxycholic acid in cystic fibrosis
CDSR Strategy: Excluded Systematic Reviews
• Absorbable staples for caesarian section • Alternative versus conventional delivery settings • Amnioinfusion for cord compression
• Amnioinfusion for meconium liquor in labor
• Antenatal thyrotropin-releasing hormone before preterm delivery
• Anti-D administration in pregnancy • Anti-Rh-D prophylaxis postpartum
• Antibiotic prophylaxis in the intensive care unit • Anticonvulsants for pre-eclampsia
• Antipsychotics, learning disabilities, schizophrenia • Balanced protein/energy supplementation • Betamimetics for impaired growth • Biophysical profile
• Blood transfusion in sickle cell anemia
• Cerebrospinal fluid tapping after intraventricular hemorrhage • Cesarean delivery for the second twin
• Caffeine to prevent postoperative apnea in preterm • Calcium channel blockers for impaired fetal growth • Chemotherapy of schistosomiasis
• Chest physio for babies being extubated • Chorion villus sampling versus amniocentesis • Continuity of care during pregnancy and childbirth • Continuous electronic fetal monitoring
• Corticosteroids before preterm delivery • Dexamethasone in neonates being extubated • Dietary regulation for gestational diabetes • Doxapram treatment for apnea in preterm labor
• Energy/protein restriction in pregnancy • Episiotomy policies in vaginal births • Expanding outpatient pharmacists’ role • Gonorrhea in pregnancy
• Human immunodeficiency virus (HIV) infection in pregnancy • High frequency oscillatory ventilation for respiratory distress
syndrome
• High protein supplementation in pregnancy • Hormonal placental function tests
• Hormone therapy for impaired fetal growth • Hospitalization for bed rest in multiple pregnancy • Hyperventilation in acute traumatic brain injury • Immersion in water during pregnancy and childbirth • Immunotherapy for recent miscarriage
• Inosital in preterm infants
• Intercessory prayer for alleviation of ill health • Intrapartum antibiotics for Group B streptococcus
• Intrapartum fetal electrocardiogram plus heart rate recordings • Intraventricular streptokinase after intraventricular
hemor-rhage
• Intubation for meconium
• Iron supplementation in pregnancy • Isocaloric balanced protein supplementation • Kinesthetic stimulation in preterm infants • Lateral tilt during caesarean section
• Light reduction to prevent retinopathy of prematurity • Magnesium sulfate versus diazepam for eclampsia • Magnesium sulfate versus phenytoin for eclampsia • Malaria vaccines
• Maternal iodine supplements in areas of deficiency • Maternal oxygen for fetal distress
• Maternal oxygen therapy in impaired fetal growth • Methylxanthines for apnea of prematurity • Minimal enteral nutrition
• Multiple versus single dose surfactant
• Nasal continuous positive airway pressure after extubation in preterm infants
• Natural versus synthetic surfactant • Nitric oxide in neonatal respiratory failure • Nutritional advice in pregnancy
• Oxytocin and lactation
• Oxytocin for premature rupture of membranes at or near term • Pelviectomy for cephalic presentations
• Phenobarbital before preterm birth • Pregnancy and malaria prevention
• Preventing/optimizing outcome post-term pregnancy • Prophylactic indomethacin
• Prophylactic intravenous preloading • Prophylactic natural surfactant • Prostaglandins for PROM at/near term • Pyridoxine in pregnancy
• Regular aerobic exercise in pregnancy • Routine folate supplementation in pregnancy • Short versus long hospitalizations
• Somatostatin/octeotride in acute bleeding varicees • Support during at risk pregnancy
• Support during childbirth
• Surfactant materials for perineal repair • Treatment of giardiasis
• Treatment of trichomoniasis
• Trichomonas treatment during pregnancy • Umbilical artery catheters: catheter position • Umbilical artery catheters: catheter design • Umbilical artery catheters: heparin usage • Vacuum extraction versus forceps delivery • Vaginal candidiasis in pregnancy
• Vitamin D supplementation in pregnancy • Vitamin K previous preterm birth • Zinc supplementation in pregnancy
AAP Strategy: Included Policy Statements
• Administration of the third dose of oral poliomyelitis vaccine at 6 to 18 months of age
• Adolescent assault victim needs: a review of issues and model protocol
• Alcohol use and abuse: a pediatric concern • Aluminum toxicity in infants and children
• Assessing physical activity and fitness in the office setting • Atlantoaxial instability in Down’s syndrome: subject review • Behavioral and cognitive effects of anticonvulsant therapy • Camphor revisited: focus of toxicity
• Cardiac dysrythmias and sports
• Death of a child in the emergency department
• Distinguishing sudden death syndrome from child abuse fatal-ities
• Evaluation and preparation of pediatric patients undergoing anesthesia
• Eye examination and vision screening in infants, children, and young adults
• Guidelines of forgoing life sustaining medical treatment • Health care for children of farm workers
• Health care needs of children in foster care • Health needs of homeless children and families • Health supervision for children with achondroplasia • Health supervision for children with Down’s syndrome • Health supervision for children with fragile X syndrome • Health supervision for children with Marfan’s syndrome • Health supervision for children with neurofibromatosis • Health supervision for children with sickle cell disease and their
families
• Health supervision for children with Turner’s syndrome • Human milk, breastfeeding, and transmission of HIV in the
United States
• Infant feeding practices and their possible relationship to the etiology of diabetes mellitus
• Management of acute gastroenteritis in young children • Management of hyperbilirubinemia in the healthy newborn • Managing otitis media with effusions in young children • Medication for children with attention disorders
• Meningococcal disease prevention and control strategies for practice-based physicians
• Metered dose inhalers for young athletes with exercise-induced asthma
• Mitral valve prolapse and athletic participation in children and adolescents
• Neurodiagnostic evaluation of the child with a first simple febrile seizure
• Office management of acute exacerbation of asthma in children • Pediatricians’ role in family support programs
• Pediatricians’ role in helping children and families deal with separation and divorce
• Physicians’ role in coordinating care of hospitalized children • Positioning and sudden infant death syndrome: update
prena-tal genetic diagnosis for pediatricians • The prenatal visit
• Prevention of hepatitis A infections: guidelines for the use of hepatitis A vaccine and immune globulin
• Promotion of healthy weight control practices in young athletes • Reassessment of the indications for ribavirin therapy in
respi-ratory syncytial virus infections
• Recommendations for the use of live-attenuated viruses and globulin preparations
• The relationship between pertussis vaccine and central nervous system sequelae: continuing assessment
• Screening infants and young children for developmental dis-abilities
• Screening for tuberculosis in infants and children • Selection of substance abuse treatment programs • Sexual assault and the adolescent
• Sexually transmitted diseases
• Treatment guidelines for lead exposure in children
• Update on timing of hepatitis B vaccination for premature infants and children with lapsed immunizations
• Update on tuberculosis skin testing of children • Use and abuse of the Apgar score
• Use of chloral hydrate for sedation in children
• Use of codeine and dextromethorphan containing cough syrups in pediatrics
• Use of fruit juice in the diets of young children • Use of whole cow milk in infancy
AAP Strategy: Excluded Policy Statements
• The application of health and safety guidelines to out-of-home child care programs
• Bicycle helmets
• Children, adolescents, and advertising • Children, adolescents, and television • Condom availability and youth • Drug-exposed infants
• Efforts to reduce the toll of injuries in childhood require ex-panded research
• Ethics and the care of critically ill infants and children • Financing of substance abuse treatment for children and
ado-lescents
• Graduate medical education and pediatric work force issues and principles
• Guidelines for ethical conduct of studies to evaluate drugs in pediatric populations
• Guidelines for expert witness testimony in medical liability cases
• Guidelines for home care of infants, children, and adolescents with chronic disease
• Guidelines for pediatric emergency care facilities
• Guiding principles for managed care arrangements for health care of infants, adolescents, and young adults
• The hazards of child labor
• Hospital stay for healthy term newborns
• Impact of music lyrics and music videos on children and youth • Implementation of the immunization policy
• The inappropriate use of school readiness tests
• Informed consent, parental permission, and assent in pediatric practice
• Inhalant abuse
• The initiation or withdrawal of treatment for high risk new-borns
• Injuries associated with infant walkers • Integrated school health services
• Issues of confidentiality in adoption: the role of the pediatrician • Joint committee on infant hearing 1994 position statement • Media violence
• Medicaid policy statement
• Medical conditions affecting sports participation
• Policy update: medical staff appointment and delineation of pediatric privileges in hospitals
• Medication of dispensing in pediatric office practice • Newborn screening fact sheets
• Office-based counseling for injury prevention
• Parental leave for residents and pediatric training programs • Polychlorinated biphenyls in breast milk
• The pediatrician’s role in advocating life-support courses for parents
• The pediatrician’s role in promoting the health of patients in early childhood education and or child care programs. • Perinatal care at the threshold of viability
• Perinatal HIV testing
• Policy on the development of immunization tracking systems • Committee report: population to pediatrician ratio estimate, a
subject review
• Prenatal genetic diagnosis for pediatricians • Prevention of sexual harassment in the workplace • Protective eyewear for young athletes
• Repraisal of lytic cocktail demerol, phenergean, and thorazine (dipropyltryptamine) for the sedation of children
• Reducing the risk of HIV infection associated with illicit drug use
• Reimbursement for medical foods for inborn errors of metabo-lism
• Risk of injury from baseball and softball in children 5 to 14 years of age
• The role of the pediatrician in implementing the American with Disabilities Act: subject review
• The role of the pediatrician in prescribing therapy services for children with motor disabilities
• The roles of the primary care pediatrician in a management of high risk newborn infants
• The role of schools in combating substance abuse
• Safe transportation of premature and low birth weight infants • Safeguards needed in transfer of patient data
• School bus transportation of children with special needs • School transportation safety
• Selecting and using the most appropriate car safety seats for growing children
• Sexuality, contraception, and the media
• Sexuality: education of children adolescents with developmen-tal disabilities
• Staffing patterns for patient care and support personnel in a general pediatric unit
• Summary of major changes in the 1994Red Book
• The teenage driver
• Testing for drugs of abuse in children and adolescents • Tobacco free environment: an imperative for the health of
chil-dren and adolescents
• Transition of care provided for adolescents with special health care needs
• Triathlon participation by children and adolescents • Unapproved uses of approved drugs
• Universal access to good quality education and care of children from birth to 5 years
• Why supplemental security income is important for children and adolescents
CPS Strategy: Included Policy Statements
• Adolescent pregnancy
• Alcohol and substance abuse by adolescents • Blood tests for allergy
• Breastfeeding: 15 years of progress? • Care of the chronically ill adolescent
• Cat scratch disease: diagnosis and management
• Ceftriaxone in the treatment of meningitis and gonococcal in-fection
• Childhood tuberculosis: current concepts in diagnosis • Chickenpox: prevention and treatment
• Cytomegalovius infection in day care centers
• Coagulase negative staphylococcus as pathogen: believe it or not
• Dexamethasone in bacterial meningitis in an era of decreased invasiveHaemophilus influenzaedisease
• Dexamethasone therapy for bacterial meningitis • Effective discipline for children
• Enuresis
• Head lice infections: a persistent itchy pest
• Hepatitis A vaccine: how should we use it in children • Initial therapy for meningitis
• IVIG use in children
• Management of children with head trauma
• Management of the febrile 1 to 36 months of age child with no focus of infection
• Management of the pediatric patient with generalized convul-sive status epilepticus in the emergency department
• Meeting the iron needs of infants and very young children • Megavitamin and megamineral therapy in children
• Meningococcal disease prevention and control strategies for practice-based pediatricians
• Mupirocin in the treatment of impetigo • Neonatal surfactant replacement therapy • Office practice guidelines
• Oral rehydration therapy and early refeeding in the manage-ment of childhood gastroenteritis
• Pediatricians role in childhood sexual abuse
• Periconceptual use of folic acid for reduction of the risk of neural tube defects
• Perinatal HIV testing • Prevention of firearm deaths
• Reducing the risk of sudden infant death syndrome
• Report of the joint CPS/NHW working group on dietary fat and children
• Routine administration of vitamin K to newborns • Sexual abuse: chronic
• Sexuality education
• Tetracycline use in children: updated
• Toward the rational management of herpes infection in preg-nancy in women and their newborn infants
• Treatment of chronic asthma • Use of acyclovir in children
• Use of fluoride in infants and children
• Use of ribavirin treatment of infections caused by respiratory syncytial virus
• Vertical transmission of hepatitis C virus: current knowledge and issues
CPS Strategy: Excluded Policy Statements
• Acute childhood encephalitis and meningoencephalitis • Age limits and adolescents
• Antimicrobial resistance: implications for therapy of infections with common childhood pathogens
• Assessment of childhood refugees and immigrants: role of screening for parasites
• Diabetes and the first nations
• Evaluation of care in neonatal-perinatal medicine • Facilitating discharge home after a normal term delivery • Family friendly adolescent health care
• Health care standards for youth in custodial facilities • Human milk drinking and storage
• Minimal equipment guidelines for pediatric prehospital care • National consensus statement on prevention of early onset
group B streptococcal infections in the newborn • Scabies management
• Nutrition for healthy term infants
• Ribavirin: is there a risk to hospital personnel? • Should there be routine testing for HIV in pregnancy?
REFERENCES
1. Sackett DL, Rosenberg WMC. The need for evidence-based medicine.
J R Soc Med. 1995;88:620 – 624
2. Oxman AD, Sackett DL, Guyatt GH. Users’ guide to the medical liter-ature. How to get started.JAMA.1993;270:2093–2095
3. Bero L, Rennie D. The cochrane collaboration: preparing, maintaining, and disseminating systematic reviews on the effects of health care.
JAMA. 1995;274:1935–1938
4. American Academy of Pediatrics.Policy Reference Guide of the American Academy of Pediatrics:A Comprehensive Guide to the AAP Policies Issued Through December 1996.10th ed. Elk Grove Village, IL: American Acad-emy of Pediatrics; 1997
5. Canadian Paediatric Society.Statement Book. Ottawa, Canada: Canadian Paediatric Society; 1975–1997
6. Garfield E. The impact factor.Curr Contents. 1994;25:3–7
7. Garfield E. How can impact factors be improved?BMJ. 1996;313: 411– 413
8. Seglen PO. Why impact factors of journals should not be used for evaluating research.BMJ. 1997;314:498 –502
9. Moed HF, Van Leeuwen. Impact factors can mislead.Nature. 1996;381: 186
10. Evans JT, Nadjari HI, Burchell SA. Quotational and reference accuracy in surgical journals, a continuing peer review problem.JAMA. 1990;263: 1353–1354
11. Wenneras C, Agnes W. Nepotism and sexism in peer review.Nature. 1997;22:341–343
HONESTY ABOUT SCREENING
We should be more honest in reporting measurements to individuals,
research-ers, the media, and practicing clinicians all tend to portray medical advances in a
positive light. For example, I could tell one of my patients, ‘‘Yearly mammograms
will decrease your risk of fatal breast cancer by 33%.’’ Or I could say, ‘‘Seven
thousand people like you would need to have yearly mammograms to prevent one
premature cancer death.’’ Both statements are fairly accurate. Which statement is
more likely to encourage my patient to comply with my recommendation of yearly
mammograms?
Murphy DJ. Guideline glitches. Measurement, money and malpractice. In: Boyle PJ, ed.Getting Doctors to Listen. Washington, DC: Georgetown University Press; 1998