THE CENTRE FOR MARKET AND PUBLIC ORGANISATION
Centre for Market and Public Organisation Bristol Institute of Public Affairs
University of Bristol 2 Priory Road Bristol BS8 1TX http://www.bristol.ac.uk/cmpo/ Tel: (0117) 33 10752 Fax: (0117) 33 10705 E‐mail: cmpo‐[email protected]
The Centre for Market and Public Organisation (CMPO) is a leading research centre, combining expertise in economics, geography and law. Our objective is to study the intersection between the public and private sectors of the economy, and in particular to understand the right way to organise and deliver public services. The Centre aims to develop research, contribute to the public debate and inform policy‐making.
CMPO, now an ESRC Research Centre was established in 1998 with two large grants from The Leverhulme Trust. In 2004 we were awarded ESRC Research Centre status. CMPO is now wholly funded by the ESRC.
ISSN 1473‐625X
Poverty and survival
Sonia BhalotraDecember 2010
Working Paper No. 10/253
CMPO Working Paper Series No. 10/253
Poverty
and
survival
Sonia Bhalotra1 1 CMPO and Department of Economics, University of Bristol December 2010 Abstract
A recent literature highlights the uncertainty concerning whether economic growth has any causal
protective effect on health and survival. But equal rates of growth often deliver unequal rates of
poverty reduction and absolute deprivation is more clearly relevant. Using state‐level panel data for
India, we contribute the first estimates of the impact of changes in poverty on infant survival. We
identify a significant within‐state relationship which persists conditional upon state income,
indicating the size of survival gains from redistribution in favour of households below the poverty
line. The poverty elasticity declines over time after 1981. It is invariant to controlling for income
inequality but diminished upon controlling for education, fertility and state health expenditure, and
eliminated once we introduce controls for omitted trends.
Keywords poverty, income, inequality, infant mortality, India, economic reform, state health
expenditure, panel data.
JEL Classification O15, I12
Electronic version www.bristol.ac.uk/cmpo/publications/papers/2010/wp253.pdf Address for correspondence
CMPO, Bristol Institute of Public Affairs
University of Bristol 2 Priory Road Bristol BS8 1TX [email protected] www.bristol.ac.uk/cmpo/ Acknowledgements
I would like to thank Andrew Newell for encouraging me to write this paper.
Poverty and Survival
Sonia Bhalotra
1. Introduction
There is considerable uncertainty concerning whether income has a protective effect on health and survival (Cutler et al. 2006). There appears to be no causal relationship between absolute changes in life expectancy and economic growth in cross-country data over 10, 20, or 40 year periods between 1960 and 2000, rather, the correlation between the two is probably driven by a third factor such as education or public health provision (Deaton 2007a). Higher frequency (annual) changes in many OECD member countries reveal a negative relationship between income and survival which appears to arise from substitution or selection effects dominating income effects (Ruhm 2000, 2005, Dehejia and Lleras-Muney 2004). Although the income-survival relationship is positive in India and on average across developing countries (Ferreira and Schady 2009, Bhalotra 2010a), it is sometimes negative in the richer set of countries in Latin America (Palloni and Hill 1997, Ortega and Reher 1997, Abdala et al. 2000, Miller and Urdinola 2010). Overall, the evidence is consistent with the stylized fact that health is concave in income, most likely because low levels of (aggregate) income are associated with absolute deprivation, including lack of food and clean water (Preston 1975, Cutler et al. 2006). It follows that improvements in income are more likely to improve health and survival when they are distributed in favour of the poor. This is evident in country comparisons that showcase, for example, Cuba, Sri Lanka and the Indian state of Kerala, regions with progressive states that have conducted redistribution. Health improvements in these cases have often proceeded independently of economic growth (Dreze and Sen 1995). However the political institutions that effected poverty reduction in these regions also motivated investments in public health and women’s education. It is therefore unclear that the reduction of income poverty was essential to their health achievements. In the analysis to follow, we control for long-standing institutional differences between state governments and attempt to isolate the role of income poverty.
Previous studies of the income-health relationship have tended to relate indicators of population health to average national income (GDP), neglecting to consider the importance of redistribution and absolute deprivation (e.g. Dehejia and Lleras-Muney 2004, Ferreira and Schady 2009, Bhalotra 2010a). In fact the responsiveness of health to changes in average income growth will depend upon the growth elasticity of poverty, and this varies with initial conditions and the institutional setting in which policy and individual investment decisions are made (Datt and Ravallion 2002, Besley and Burgess 2003). If equal growth rates result in unequal changes in poverty then it is relevant to directly estimate the impact of poverty change on health. Even if the incomes of the poor grow proportionately with average income (as argued in Dollar and Kray 2002), concavity of the health-income relationship suggests that poverty reduction will generate health improvements conditional upon average income. This paper provides what would appear to be the first systematic investigation of the importance of poverty reduction efforts in improving child survival which, in developing countries, is the driver of changes in life expectancy. This is clearly relevant to evaluating the payoff from worldwide poverty reduction efforts spurred by one of the Millenium Development Goals being a halving of poverty incidence by 2015 relative to its level in 1990. In an early related study, Anand and Ravallion (1993) showed, using a single cross-section of 22 developing countries that the correlation of income and life expectancy was driven to zero by conditioning upon poverty and public health spending. However, their estimates are likely to be contaminated by the considerable unobserved heterogeneity at the country level. We control for this and find contrasting results.
India is an appropriate setting for the analysis. The period analysed, 1970-1998, was one of momentous change. Starting in the early 1980s and accelerating a decade later, India has seen unprecedented economic growth. Poverty incidence has declined, albeit not as quickly as it might have. India accounts for 15% of the world’s population, 33% of the world’s poor (Besley et al. 2006) and 25% of all infant deaths, which is about 2.5 million (Black et al. 2003). Most of these deaths are preventable, arising from an interaction of infectious disease and under-nutrition (Jones et al. 2003). Under-nutrition increases vulnerability to infectious disease and, in turn, infectious disease inhibits assimilation of nutrition (Scrimshaw, Taylor and Gordon
1968). Children under the age of five are most vulnerable because their immune systems are not fully developed. Indeed, 30% of all deaths in developing countries occur amongst children, compared with less than 1% in richer countries (Cutler et al. 2006). This is clearly because richer countries have largely eliminated death from infectious diseases. What is less clear is what the role of reducing absolute income deprivation is in this relative to, for example, the role of improvements in public health (Cutler et al. 2006).
India has a federal political structure in which state governments have considerable autonomy with respect to poverty and health although their efforts are supplemented by nationwide interventions in both domains. We use state level panel data to obtain difference-in-difference estimates allowing for differential underlying state trends in mortality. The average unconditional rural within-state poverty elasticity of mortality is unity. This implies that a one standard deviation change in poverty within states is associated with a 3.4% point decline in the mortality rate which is a third of the mean (9.36%) and more than two thirds of the standard deviation of mortality in the sample. This estimate implies that the observed decline in poverty in India in the twenty year period between 1970-75 and 1990-95 can explain 57% of the actual mortality decline in the same period. Controlling for average income per capita substantially lowers the poverty elasticity to 0.37 and delivers a within-state income elasticity conditional on poverty of -0.67. This specification implies that redistribution towards the poor can, income constant, explain 21% of the observed mortality decline while income growth, conditional upon poverty incidence, can explain 60%. Introducing state health expenditure lowers both coefficients, most strikingly the income coefficient, indicating that more than half of the impact of income on survival conditional upon poverty may work through its raising state health expenditure. In this specification, the poverty and income elasticities of survival are equal but the stronger trend in income as compared with poverty in the sample period implies that poverty can now explain 10% of the actual mortality decline, while income can explain 24%. Conditional on state income and poverty, state health expenditure explains 53% of the actual decline. We identify significant and sizeable effects of parents’ education, mother’s age at birth and birth order (fertility) on infant survival and controlling for these lowers the poverty
elasticity. The poverty and health expenditure coefficients are rendered small and insignificant upon controlling for unobserved trends but the income elasticity remains significant, at -0.34.
To complement our estimates of the mortality-reducing impacts of poverty reduction and income growth, each conditional upon the other, we present estimates of the income elasticity of poverty. The within groups estimate, at -0.6, is similar to that in a recent literature that uses the same specification (Besley and Burgess 2003). However, it is driven down to -0.2 once we control for omitted trends. This suggests that previous work may have over-estimated this elasticity; though see section 7.1. In view of public policy debates regarding the impact of the wave of economic liberalisation from 1991 onwards on poverty, we estimated the elasticity pre and post 1991. It fell slightly if significantly from -0.706 to -0.694 but this difference is eliminated upon controlling for omitted trends, consistent with the evidence in Deaton and Dreze (1991).
The baseline model, absent trends, is subject to a range of robustness checks and extensions. Adding (rural) inequality to the specification does not alter the poverty or income coefficients. This confirms that poverty is not simply proxying inequality and makes it more likely that it captures absolute deprivation. The poverty coefficient is also robust to including the square of income, suggesting that poverty is not just capturing concavity of survival in income. The income quadratic is significant, confirming concavity. Neonatal mortality is less sensitive to poverty and income than infant mortality and under-5 mortality is more sensitive. This is consistent with the influence on survival of the external socioeconomic environment relative to birth endowments increasing with age of exposure of the child. Replacing the headcount rate with alternative poverty measures, in particular the squared poverty gap and rural mean consumption produces significant effects and the elasticities estimated from levels-levels and log-log specifications are similar to the elasticities from the baseline semi-log model. The coefficient on the lagged headcount rate is similar to that on the current rate. State specific estimates are obtained and are compared with state fixed effects estimated from the pooled model.
Economic liberalisation in India accelerated sharply in 1991 and there has been some discussion of the welfare (poverty) impact of reform but there is limited
evidence of impacts on health (Deaton and Dreze 2002). We find significantly smaller income and poverty elasticities after 1991. The marginal impact of poverty on mortality fell by almost a half, from 0.043 to 0.024. The marginal impact of income also fell but only by about a sixth, from -0.062 to -0.052. However, we show that both elasticities were declining through the sample period, consistent with the progression of reforms from 1981 onwards (Virmani 2004).
Recent research suggests that lowering poverty and improving health in early life bring persistent benefits for survivors and their offspring (Deaton 2007b, van den Berg et al. 2006, 2008, Almond and Currie 2010, Bhalotra and Venkataramani 2010, Bhalotra 2010b). This suggests multiplier effects that our estimates do not take account of. In particular, the gain in life expectancy induced by lowering poverty will tend to exceed the gain in childhood survival that we estimate. The rest of this paper unfolds as follows. Section 2 introduces the data sources and section 3 describes trends and regional variation in the key variables along with nonparametric estimates of the unconditional relationships of interest. The estimators are discussed in section 4 and the results in section 5. Section 6 presents a range of robustness checks and extensions and section 7 places the findings in a wider context. Conclusions are in section 8.
2. Data
The data are a 29 year panel running from 1970-98 for the 15 major states of India, in which about 95% of the population resides. Poverty rates are calculated using inflation-adjusted Government of India poverty lines for rural and urban areas applied to household-level consumption data from National Sample Survey data gathered at intervals of between 0.9 and 5.5 years (Ozler et al. 1996). Data on state net domestic product (henceforth income) at constant prices are also sourced from Ozler et al., updated by Besley and Burgess (2004). Rainfall time series by state are acquired from www.indiastat.com and transformed into positive and negative-valued z-scores to denote rainfall shocks. The infant mortality and fertility data are derived from the second Indian National Family Health Survey (NFHS), as are education, caste and religion of the parents. Infant mortality is an indicator for death between birth and the age of twelve months. Fertility is indicated by mother’s age at first birth and birth order. State averages of these variables are constructed using sample weights provided
in the microdata; see IIPS and ORC Macro (2000) for details of the sampling strategy. Consistent with the individual risk of mortality varying non-linearly with the level of the independent variables, we include the percentage distribution of the relevant characteristics in the state population, for example, the percentage of mothers and fathers with different levels of educational attainment.
The sample analysed is restricted to rural households which supply 77% of all births. Poverty and mortality are concentrated in rural areas. In line with the wider literature, we measure the incidence and severity of poverty rather than the incomes of the poor. The main analysis uses the headcount rate, as this is the measure that governments and international organisations target and monitor. We investigate alternative indices that are sensitive to the depth of poverty, and average rural expenditure. The main analysis is for infant mortality as this is the widely used measure of population health in poorer countries (e.g. Reidpath and Allotey 2003), but we also investigate neonatal and under-5 mortality.
A reason that there is relatively limited quantitative analysis of trends in health, mortality and fertility in developing countries is that time series data on these variables are not readily available. Although they have not been used very much for this purpose the NFHS surveys and their counterpart Demographic and Health Surveys (DHS) for other developing countries contain retrospective fertility histories from which monthly (or annual) time series of mortality rates comparable across the states can be constructed (see Bhalotra 2008a, 2010a). In contrast international infant mortality statistics are quinquennial and unreliable (Pritchett and Summers 1996, Ross 2006). The state level panel for India is an unusually good resource. An analogous cross-country analysis would be restricted to more widely spaced data that are not necessarily comparable across countries. International poverty and inequality data are not available through the period analysed (e.g. Besley and Burgess 2003). Annual GDP data are available but there are issues of comparability across countries (Johnson et al. 2009). A sub-national analysis has the further advantage that federal (national) institutions are constant and (unobservable) differences in medical technology across states are likely to be small.
This section describes state and all-India trends and variation in the infant mortality rate, the headcount poverty rate and log real per capita income during 1970-98. Figure 1 plots the density of mortality and poverty, from which a considerable spread is apparent. The mean [standard deviation] of infant mortality and poverty in percentages are 9.36 [4.6] and 46.6 [14]. The relationship between poverty and mortality in the analysis to follow is identified from within state time variation. Estimated on the within-state variation, the standard deviations are still large, at 3.8 and 9 respectively. Volatility of poverty rates is consistent with the macroeconomic volatility that characterises poor countries (Pritchett 2000, Koren and Tenreyro 2007).
All-India trends are in Figure 2. Across the three decades, the poverty rate declined from almost 60% to about 35%, the infant mortality rate fell from almost 15% to about 6% and real per capita income grew by about 70%, the annual linear rate of increase averaged over the period being 3% p.a. Poverty started to decline in 1974 and income started to rise in 1976. Income growth increased through the period but poverty decline slowed in the 1980s, picking up again in the 1990s. Variability in both poverty and mortality appears to have increased in the 1990s, the post-reform decade in which the economy grew most rapidly. The lower panel of Figure 2 superimposes smoothed trends of poverty and mortality in levels and logs. These pictures suggest that, in levels, both rates of decline slowed after the mid-80s. The rate of poverty decline also slowed in proportional terms, indeed, if 1983 is chosen as the break point, it halved, from 2.2% p.a. to 1.1% p.a. However the proportional rate of mortality decline was more or less the same before and after 1983. The slowing of mortality reduction in India would appear to correspond to a more general slowdown across countries in the 1990s compared with the 1980s (Ahmad, Lopez, and Inoue 2000). We are not aware of any previous analysis of long term trends in mortality in India but the slowing of poverty decline concurrent with a quickening of income growth in India has been widely debated and analysed (e.g. Deaton and Dreze 2002, Deaton and Kozel 2005).
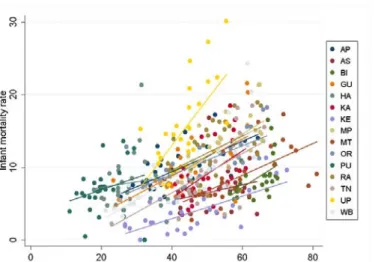
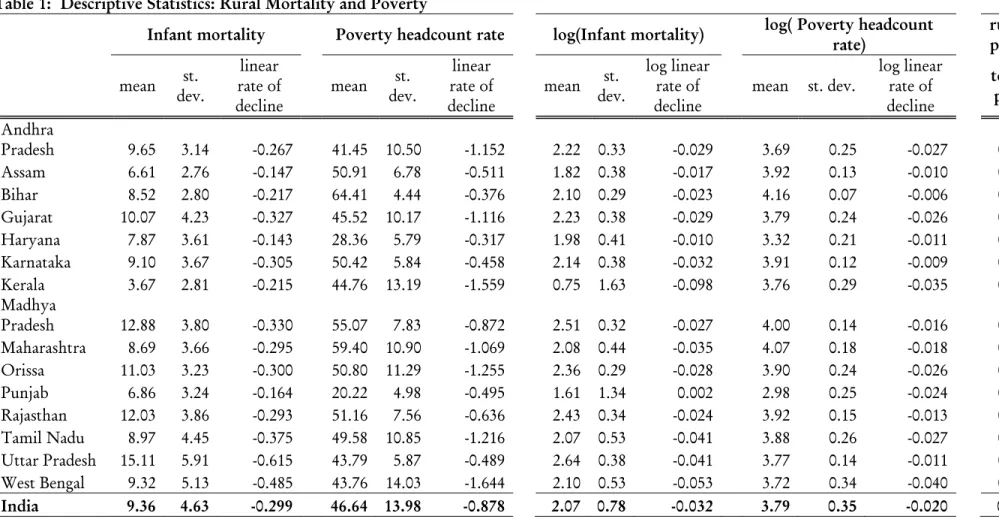
State-specific trends are in Figure 3. There is considerable variation across states in levels, trend and fluctuations around trend. Table 1 presents the mean and s.d. of mortality and poverty and the annual linear [absolute] and log-linear
[proportional] rate of decline of each for every state and all-India. On average, mortality declined by 3.2% p.a. and poverty by 2% p.a. Kerala stands out for showing the sharpest rate of decline in both variables, at 9.8% and 3.5% p.a. respectively. On the other hand, Uttar Pradesh exhibits an above-average rate of decline in morality (in absolute and proportional terms) even though its rate of poverty decline was well below the average. The mean mortality rate ranges from 15.1% in Uttar Pradesh to 3.7% in Kerala (with the rate in Bihar being 8.5%). The poverty rate ranges from 64.4% in Bihar to 20.2% in Punjab, with the rate in Uttar Pradesh being below average at 43.8% and that in Kerala being close to the average at 44.8%. Overall, there is huge cross-state variation and state averages indicate a weak relationship between mortality and poverty rates. Figure 3 suggests that the levels of income and poverty are no less dispersed across states at the end of the period than at the beginning. The level of mortality, in contrast, shows some tendency towards convergence. This is consistent with nationwide public health campaigns such as the Universal Immunization Programme of the Government of India, which started in 1985/6 and had extended across the nation by 1990.
Nonparametric Estimates
The unconditional relationship of mortality with poverty and income is depicted using the non-parametric lowess estimator. Figure 4 presents the cross-state relationships estimated by averaging the data for each state across the 29 years in the sample. There is considerable dispersion around both fitted curves. The slope of a linear fit of the between-state mortality-poverty relationship is -0.026 (t=2.4), which implies an elasticity of 0.28. The linear fit of the mortality-income relationship has a similar slope but this is insignificantly different from zero. So, in the raw data, average state income is uncorrelated with the state mortality rate but state level poverty incidence is positively correlated with the state mortality rate. The scatter points for Uttar Pradesh and Kerala deviate in opposite directions from the lowess fit; we discuss these cases further below. In contrast to Uttar Pradesh, Bihar lies (almost) on the fitted curve.
Figure 5 shows closer fits estimated on the all-India time series. The mortality-poverty relationship is again better determined than the mortality-income relationship. Deviations from the (lowess) fit are more pronounced at higher levels of
poverty and at lower levels of income. Up until poverty levels just above the median (47.3%), the relationship is almost linear in levels, after which it grows steeper (if less well determined). Since poverty incidence has not crossed 50% since 1980, this amounts to saying that the relationship was stronger in the 1970s; regression estimates by decade are discussed in section 6.1. The relationship was plotted again using the semi-log form, mortality against the logarithm of the poverty rate, and its shape was similar (not shown).
State-specific time series scatters on which a linear fit is superimposed are shown in Figure 5. A positive relationship of morality and poverty is apparent in every state. A striking feature of this picture is that the level of infant mortality associated with a given level of poverty varies dramatically across states. Given poverty, mortality is highest in Uttar Pradesh and lowest in Kerala; this was also evident in Figure 4 (left panel).1 Slopes for states other than UP are fairly similar, which suggests that the pooled estimates are likely to provide a fair description of the underlying within-state relationships.
4. Methodology
We initially estimate the raw (unconditional) correlation in the pooled data from a simple log-linear regression of the level of mortality (M) on the log of poverty (p)-
Mst = 0pst + e0st (1)
where s and t indicate state and year respectively. We also estimate equation (1) with the mortality rate replaced by its logarithm. We retain the specification with the level of mortality for the reason that this is the variable of policy interest if concern is with the numbers of children dying. Modelling proportional changes involves the mean, creating the possibility that the estimated parameter captures long run cross-state associations that are not causal (see the discussion in Deaton 2007a). Consistent with this, once we condition upon state fixed effects (below), we find that the elasticity is not sensitive to whether or not mortality is logged. We estimate a specification that conditions upon the log of real p.c. state income (y) -
1 This ranking was apparent unconditional on poverty. Conditioning on a variable does have
the potential to reverse a ranking but in this case, as it happens, it does not to do this. In the pooled regressions, these levels differences are captured by state fixed effects.
Mst = 1pst +
0yst +e1st (1a)The parameters 0 and 1 are the unconditional and conditional correlations
respectively.
Historical differences in the natural environment and in political and community institutions across the states have tended to create persistent differences in living standards. As it can be difficult to draw out causal relationships from the long standing processes that underlie cross-sectional differences, we modify the correlations in (1) and (1a) by purging them of all state-level time-invariant variables. Denoting state fixed effects s or vs we estimate
Mst = 2pst + s + e2st (2)
Mst = 3pst +
1yst +vs + e3st (2a)This is the within groups specification that is commonly estimated in the predominantly cross-country literature on poverty and growth. Since mortality and poverty are both trended, a weakness of equations (2) and (2a) is that omitted trends or state-time varying shocks that are correlated with poverty will tend to load onto the poverty coefficient creating a bias. We therefore extend the model to include observed state-time varying variables, xst, namely education, religion and caste
composition of the state population, rainfall shocks and indicators of fertility. There may remain unobserved trends or shocks, for example, advances in health technology and delivery or changes in policy, governance and political economy. We exploit the panel structure of the data to control for these, including year dummies (
t) andstate-specific trends (
s.f(t)).Mst = 4pst + xst +
s.f(t) +
t + s + e4st(3)
Mst = 5pst +
2yst + 1xst +
1s.f(t) +
t + s + e5stWe initially specify f(t) as linear, although we also investigate cubic state trends. We consistently report estimates of the poverty elasticity of mortality, , with and without average income held constant. We use the linear probability estimator having confirmed that probit estimates are similar. Standard errors are adjusted for heteroskedasticity and clustered at the state level to allow for autocorrelation within the states.
5. Results
The poverty elasticity of infant mortality
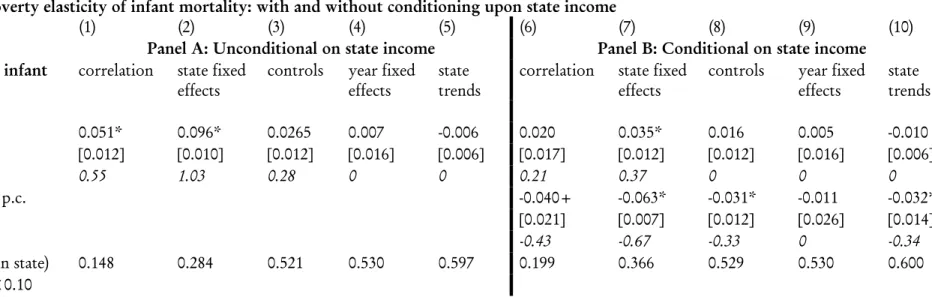
Refer Table 2a. The unconditional correlation of the mortality rate and the logarithm of the poverty rate in the pooled data (equation 1 above, column 1, Table 2a) implies an elasticity of 0.55. Controlling for state fixed effects almost doubles the elasticity,
an indication that the within-state relationship is stronger than the between-state relationship (column 2). A one standard deviation (s.d.) change in log poverty (0.354) reduces infant mortality by 3.4% points which is 36% of the sample mean.2
We investigated controlling for state-time varying covariates. Including religion and caste composition and rainfall shocks leaves the poverty coefficient unaltered. Controls for the educational level of mothers and fathers and for indicators of fertility lower it. Education drives the poverty elasticity down from 1.03 to 0.7 and fertility drives it down further to 0.28 (column 3). Conditional on these covariates, a one s.d. change in log poverty lowers infant mortality by 0.93% points or just about 10% of the mean. These changes are consistent with poverty being correlated with parental education and fertility. A correlation with education at the state level could, in a democratic setting, operate through education increasing voice or turnout amongst the poor or generating more progressive attitudes amongst the rich. A correlation of poverty with fertility is well-established (Lanjouw and Ravallion 1995).
Since migration and religious conversion are limited, religion and caste composition are plausibly exogenous. However, fertility is potentially endogenous (e.g. Bhalotra and van Soest 2008). While parental education is predetermined at the individual level it is not exogenous if parents who acquire low education have
2 If we conduct this simulation using a one s.d. change estimated on the within-state variation
in log poverty (which is 0.21) then the predicted decline in mortality is 2% points. This is a fifth of the mean and 43% of the s.d. of mortality in the sample.
unobserved traits that are correlated with their health-creating behaviours. There is the further issue that parents may endogenously select into birth and this selection may be on traits such as their religion, caste or education. In this case, the sample composition of births exposed to the risk of infant mortality will vary endogenously with (cyclical) variation in poverty. For example, educated women may time their fertility in response to a poverty shock differently than uneducated women. Recall that because the data sample is constructed from fertility histories, the share of women with, let us say, primary education in any year is in fact the share of women with primary education who gave birth in that year, and similarly for religion and caste. We have previously identified heterogeneous fertility timing in response to income shocks on this sample. In recessions (during which poverty rates rise), uneducated and scheduled caste women in rural India defer birth (Bhalotra 2010a). This suggests a pathway through which changes in poverty can generate changes in (composition by) education. However, since the covariates are potentially endogenous, they are not retained in the subsequent specifications.
Year dummies and state-specific trends are added to the specification in col. 2 to control for unobserved time-varying variables. The poverty coefficient is now close to zero and insignificant (columns 4-5); adding cubic state trends does not change this. This suggests that state-level poverty is correlated with omitted trends, for example, the quality of public health provision and that with this held constant, within-state variation in poverty has no causal impact on infant mortality.
The poverty elasticity of infant mortality conditional upon income
Panel B of Table 2a reports the same sequence of specifications designed to estimate the impact of poverty conditional upon state income. The relationship between poverty and mortality is less than half as strong conditional upon state income. The within state poverty elasticity of mortality (conditional on income) is 0.37 (column 7). This means that a one s.d. decline in poverty (0.354 in logs), average income constant, results in a 1.23% point decline in mortality, which is 13.1% of mean mortality in the sample. This is an estimate of the impact on infant survival of poverty reduction with a given pot of state income.
Conditional upon the poverty rate, the income elasticity of mortality is 0.67 (column 7). A one s.d. increase in state income (0.388 in logs), poverty rate constant, results in a 2.4% point decline in mortality, 26% of the mean rate. If infant mortality occurs predominantly amongst households below the poverty line then, as this is conditional upon the poverty rate, it is an estimate of the impact of state income when it works not through raising private incomes but through other channels such as improving public services. This result cautions against the naïve view that the impact of income growth on mortality works primarily through raising the incomes of the poor; see Anand and Ravallion (1993). Conditional upon demographics, rain shocks and fertility, the income elasticity falls to 0.33, about half its size (column 8). Adding year dummies diminishes it to close to zero but including state trends pushes it back up to 0.34.
Conditioning upon state health expenditure
We re-estimated equation (2a) to include the log of real p.c. health expenditure. The elasticity of infant mortality with respect to health expenditure is a significant -0.35. The poverty elasticity falls by a third and the income elasticity falls by two-thirds; both elasticities are now -0.27. The relatively large drop in the income elasticity is consistent with previous findings that a mechanism by which state income influences survival in India is through its influence on state health expenditure (Bhalotra 2010a); the income elasticity of health expenditure in India at the state level is estimated as -0.41 (Bhalotra 2007a).3 The share of state income dedicated to state health expenditure (or, alternatively, health expenditure conditional on state income) is positively correlated with the share of development spending, which includes expenditures on poverty programmes. This may explain why the poverty coefficient falls when state health expenditure is included.
The contributions of poverty reduction and income growth to mortality decline
We now use the estimated coefficients (
) together with the actual changes in mortality, income and poverty rates (M, y, p) over two decades to simulate the contributions of poverty and income change to mortality decline. Using five year averages at each end to reduce measurement error, the change in log poverty between3 In that paper I regressed state health expenditure on state income, a lagged dependent
variable (instrumented with two further lags), year and state dummies and state-specific trends.
1970-75 and 1990-95 was -0.36 which is, coincidentally, close to a one standard deviation change. The change in log income in the same two decades was 0.58 (larger than a one s.d. change) and the observed change in infant mortality was 6.07% points. The baseline model that includes only state fixed effects (column 2) implies that poverty decline accounts for 57% of the mortality decline in this period. Conditional upon average state income (column 7) we estimate a contribution of poverty to mortality decline of 21%. Income growth in this period, holding constant the poverty rate, can explain 60% of the observed mortality decline (column 7). The greater importance of income growth reflects not only its larger elasticity but also its stronger trend. Adding controls for education, fertility and demographic composition lowers the contribution of poverty, unconditional on income, to 15.7% (column 3). Conditional on income and covariates, the poverty elasticity is close to zero (column 8), as it is conditional on unobserved trends (columns 4-5). However, even after controlling for education, demographics, fertility and unobservable trends, income can explain 31% of the observed mortality decline (column 10).4
The income elasticity of poverty
We have observed that improvements in average income growth have a stronger impact on mortality than reductions in poverty incidence and, further, that the income coefficient is robust to controlling for unobserved trends while the poverty coefficient is not. However, our estimates of the impact of income condition upon the poverty rate. In fact income growth lowers poverty (e.g. Besley and Burgess 2003). Dropping poverty from the equation raises the within state estimate of the income coefficient by 25% suggesting that poverty is a channel by which income influences infant mortality. Table 3 shows estimates of the income elasticity of poverty for the alternative specifications employed in Table 2a. The within state elasticity is -0.6. Conditioning upon time-varying covariates or unobserved trends brings this down to the region of -0.2. In view of public policy debates regarding the impact of the wave of economic liberalisation from 1991 onwards on poverty, we estimated the elasticity pre and post 1991. It fell slightly but significantly from -0.706 to -0.694 but this difference is eliminated upon controlling for omitted trends.
4 In an alternative exercise conducted on these data, we estimate the rate of income growth
The effects of other covariates on infant mortality
Consider the size of the effects of rainfall, education and fertility (column 3, Table 2a). Since the religious and caste composition of the states is relatively stable, it does not contribute to explaining trends. We find significant beneficial effects on survival of positive rain shocks. The mortality-raising effects of negative rain shocks are slightly smaller and only significant at the 14% level. Both effects are small, a one s.d. change in rainfall being associated with a 0.34% point change in mortality. There is, naturally, no trend in rainfall, which suggests that rain shocks cannot explain any of the observed mortality decline. The data indicate a reduction in rain volatility over the sample period, which means that, assuming constant coefficients, rain explains a decreasing share of the variation in mortality around a trend.
Mortality is significantly lower if mothers have completed primary education as compared with their having no education or less than primary. A one s.d. increase in the proportion of women with primary education results in a decline in mortality of 0.56% points which is 6% of the mean. The percentage of rural mothers that have primary education increased from 5.6% to 7% on average. There was more movement at the bottom and top of the distribution5 but there are no significant gains in this specification from higher education. There is no evidence of mortality falling in the education of men.
Fertility is proxied mother’s age at first birth and birth order categories. Both have significant (non-linear) effects on mortality. Infant mortality is higher when a relatively high proportion of women have their first birth before they are 15 and lower when more women are 22-24 years old at first birth (relative to the omitted case, the modal age at first birth, of 19-21). Conditional upon age at first birth, mortality is higher when the proportion of second and higher order births is high relative to the proportion of first-born children (ie when fertility is high). To simulate its impact, we estimated the linear effect of age at first birth, using age in years. Between 1970-75 and 1990-98, mean age at first birth increased from 17.1 to
5 Amongst babies born in 1970-75, the percentage with uneducated mothers and fathers was
75 and 45 respectively and the percentage with mothers and fathers with secondary or higher education was 1.3 and 11.7. By 1990-98, the percentage of uneducated parents had fallen to 60 and 35 and the percentage with higher education had risen to 8.6 and 20. The overall sample mean of rural mother’s years of education 1.93, the overall standard deviation (s.d.) is 1.46 and the within-state s.d. is 0.69.
18.6. The coefficient on this variable implies that this alone can explain 33% of the mortality decline, other things equal. This is striking as popular and academic debates concerning the impact of growth or poverty on health or survival have tended to neglect the role of fertility.
6. Robustness Checks and Extensions
Results are in Table 4. Robustness checks are benchmarked on the specification in column 7 of Table 2. The poverty elasticity of mortality in this model is 0.37.
6.1. Robustness checks
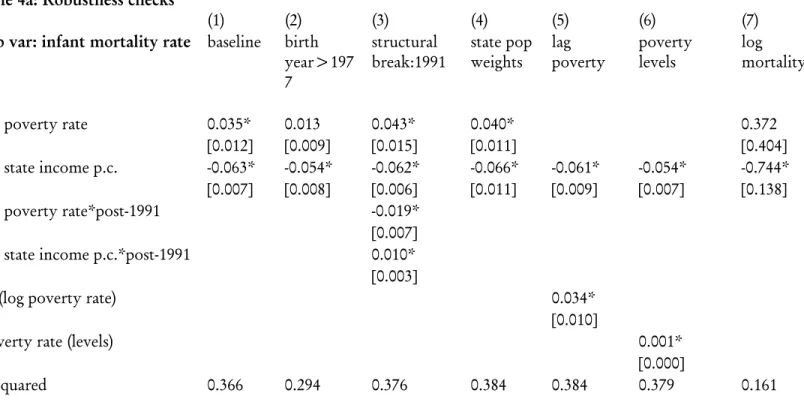
Refer Table 4a. The mortality data are drawn from retrospective fertility histories that include births that occur as many as 40 years before the survey date. We have so far used data left truncated at 28 years before the survey date, that is, we dropped births that occurred before 1970. Our own analysis of the NFHS data and previous work by demographers suggest that a retrospective window of more than 20 years may be associated with recall error. We therefore now restrict the sample to births that occur after 1978. The poverty coefficient falls to just more than a third of its baseline size (column 2), and we cannot reject the hypothesis that the poverty elasticity identified in the full sample rests upon the births in the 1970s. This may signal data issues but it is unclear why data issues would push in this direction. An alternative explanation of the results is that the relationship was strong in the 1970s and weak after. To investigate this, we estimated the model allowing heterogeneity in the poverty and income coefficients by decade. There is a significant decline in both coefficients from one decade to the next when the 1970s births are in the sample but no significant change between the 1980s and 1990s when the 1970s births are excluded from the sample.6
In view of public policy interest in the impact of economic reforms in India on welfare, we created a dummy for post-1991 and interacted this with both poverty and income. We find significantly smaller income and poverty elasticities after 1991, the year in which economic reform in India accelerated sharply. The marginal impact of poverty on mortality fell by almost a half, from 0.043 to 0.024. The marginal
6 The baseline specification is that in column 2 of Table 2a. Including the 1970s births, the
1970s poverty coefficient is 0.036. It is 0.022 in the 1980s and 0.019 in the 1990s. The income coefficients by decade are -0.047, -0.042, -0.041. These decade differences are all statistically significant. Dropping the 1970s births, the poverty and income coefficients for 1980 and 1990
impact of income also fell but only by about a sixth, from -0.062 to -0.052 (column 3). As economic reforms were phased in through the 1980s and 1990s, albeit with a sharp change in 1991, we investigated alternative break points. Consistent with the onset and diffusion of economic reforms in India (Virmani 2004), the first break point in the sample is in 1982 and pre/post differences in elasticities are significant from then on.
The Indian states have vastly different populations (see Table 1). We weighted the regressions using the square root of the mean rural population of each state to account for heteroskedasticity (e.g. Ruhm 2000, and footnote 20 therein). The resulting changes in the coefficients of interest are insignificantly small (column 4). To mitigate concerns regarding possible feedback from infant mortality to poverty, we re-estimated the model using the first lag of the poverty rate. Lagged poverty may alternatively be interpreted as picking up the influence of poverty in the foetal year on infant mortality. In any case, this creates no significant change (column 5). We discussed our choice of a semi-log functional form in section 4. We now consider alternative forms. A model relating the level of mortality to the level of poverty produces a poverty elasticity of 0.5 (column 6). A log-log model produces a poverty elasticity of 0.37, virtually identical to the baseline case (column 7). Note that we identify a relationship of income and poverty with both absolute and proportional changes in mortality.
We investigated alternative measures of poverty and mortality (Table 4b). The sensitivity of mortality risk to the socio-economic environment will tend to increase with distance from birth. Consistent with this, neonatal mortality is less sensitive to both poverty and income than infant mortality (column 1) while under-5 mortality is more so (column 2). The headcount poverty index is attractive because it is easy to collect and easy to interpret. It has the weakness that it does not say anything about the severity of poverty, that is, the distance of the poor from the poverty line. This is indicated by the poverty gap and the squared poverty gap (columns 3, 4). The relationship of mortality with the poverty gap is poorly determined but it exhibits a significant positive relationship with the squared poverty gap. The poverty headcount and gap measures are defined with respect to a threshold level of real consumption (a poverty line) using consumption data at the household level (see the
Data section). We investigated the importance of raising average rural consumption per capita in the state as opposed to lowering the proportion of people who live below a consumption-poverty line. The elasticity of rural mortality with respect to rural consumption is 0.48, conditional upon average state income (column 5). We replaced the poverty rate with the Gini coefficient for inequality in household consumption in rural areas. This has a positive if weakly determined association with mortality, income constant (column 6).
We estimated a model that includes inequality in the baseline model alongside average income and poverty. We have argued that for a given level of average income, the poverty coefficient reflects the sensitivity of mortality to absolute deprivation. But poverty may be proxying for an alternative distributional measure, inequality, with which it is positively correlated. It is striking that the poverty and income coefficients are insignificantly different when inequality is introduced as a control. The coefficient on inequality is now smaller and statistically insignificant (column 7). This establishes that poverty is indeed picking up deprivation rather than inequality. It also shows that for a given level of income and poverty incidence, redistribution has no impact on infant mortality. We included the square of income in the baseline specification. The poverty coefficient is robust. The quadratic income term is significant and shows diminishing returns to raising state income (column 8).
6.2. State-specific estimates
The Indian states exhibit dramatically different initial levels and trends of both poverty and mortality (section 3). A way of allowing for the impact of initial conditions on the efficacy of poverty reduction in lowering infant mortality is to estimate a specification that interacts state dummies with poverty. This approach has been taken in estimation of the growth-poverty relationship in India (Datt and Ravallion 2002). In their cross-country paper on growth and poverty Besley and Burgess (2003) make the related argument that institutional differences mean that a given level of growth can yield vastly different degrees of poverty decline in different regions or at different times. These arguments are related as long as we believe that initial conditions determine institutions (Acemoglu et al. 2001). Rather than employ interactions, we estimate individual time series equations by state as this is more
general. The following specification is estimated for the 15 states in the sample (T=28)-
Mt = pt + + et (4)
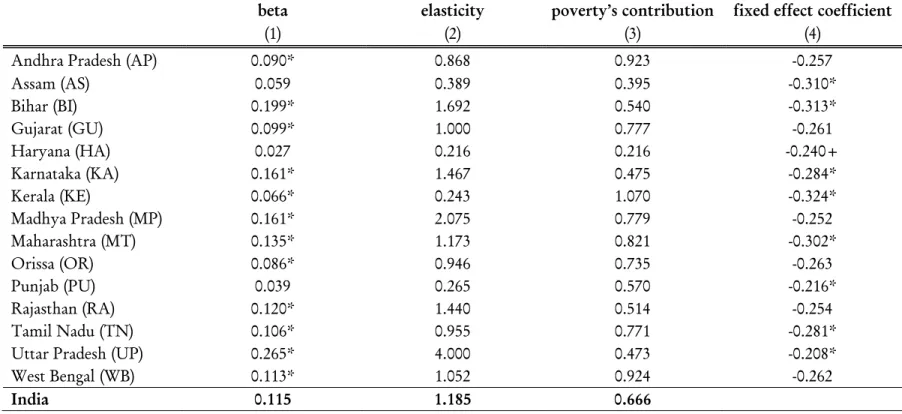
where M and p denote the infant mortality rate and the log poverty rate respectively and the constant is effectively a state fixed effect. Estimates are in Table 5.
The poverty elasticity of mortality is significant in all states other than Punjab, Haryana and Assam. It is striking that it is relatively large in Uttar Pradesh and Bihar (where poverty and mortality rates are high) and relatively small in Kerala (where both rates are low). The finding of a stronger elasticity in regions with higher mortality is consistent with diminishing returns to poverty reduction. Looking at proportional declines, Kerala stands out in having exhibited the steepest decline in mortality and it was second only to West Bengal in achieving poverty decline, despite having started with relatively low initial levels of both, especially mortality (Table 1). The finding that Kerala has a relatively small mortality elasticity of poverty suggests that while a strong poverty trend contributed, mortality-reducing factors other than poverty were important in explaining Kerala’s success in lowering mortality. This is indicated by the relatively large (negative) fixed effect for Kerala reported in Table 5. In contrast, the more shallow trend in mortality in UP and Bihar is clearly a function of a high sensitivity of mortality to poverty in an environment in which poverty declined quite slowly. Interestingly, the fixed effect is relatively large in UP but relatively small in Bihar, or UP has lower poverty than Bihar but higher mortality. We have put down only indicative comments here but perusal of Tables 1 and 5 together offers a wealth of further insight.
7. Discussion
7.1. The role of omitted trends
We find that the poverty elasticity of mortality is not robust to controls for omitted trends. There are no similar studies of the impact of poverty on mortality to compare with. However related studies that estimate the impact of growth on poverty using cross-country panel data or cross-state data for India tend to control only for country or state fixed effects (e.g. Besley and Burgess 2003, Besley et al. 2006) and, in some
cases, linear state trends but not year dummies (Datt and Ravallion 2002). Our estimates suggest that these studies may over-estimate the impact of growth on poverty. This is demonstrated in Table 3. Indeed our estimate of an income elasticity of poverty of -0.6 matches the estimate that Besley and Burgess report for South Asia and it is close to their estimate of -0.73 for all developing countries in their sample. We have shown that controlling for omitted trends brings this down to -0.2. However, if controls for unobserved trends are picking up mechanisms by which poverty reduction lowers infant mortality (Table 2) or by which increases in aggregate income lead to lower poverty (Table 3), then by including these controls we may be throwing the baby out with the bathwater. For example, state income growth may lead to increases in state development spending on targeted poverty programmes and we would expect this to be counted as part of the effect of income on poverty but would risk it being absorbed by controls for omitted trends. On the other hand, if trends in development spending are driven by political rather than economic progress then failing to control for them would lead us to incorrectly attribute to income a benefit that in fact flows from an improved political economy. Since we do not know what the year dummies and state trends are picking up, it is difficult to argue that estimates that condition upon them are more accurate.7 It also means that we cannot be sure to what extent China’s record rates of poverty reduction since the 1980s and Africa’s failure to lower poverty in that same time predict differences in the health of their populations without more information on concurrent trends.
7.2. Long run effects
Reducing poverty and improving early life health both create persistent benefits for survivors and their offspring (van den Berg et al. 2006, 2008, Bhalotra and Venkataramani 2010, Bhalotra 2010b, Almond and Currie 2010). The payoff to poverty reduction is therefore a multiplier of the estimates we present. Using pre-industrial data from the Netherlands and Denmark respectively, van den Berg et al. (2006) and van den Berg et al. (2008) show that recessions experienced in early life have a causal effect on later life morbidity and life expectancy. This is relevant insofar as poverty incidence increases in recessions and it suggests that poverty reduction not
only improves survival rates but also the future health of survivors. Early childhood mortality rates lower adult stature (Deaton 2007b, Bhalotra 2007b) which is an indicator of health and life expectancy (Fogel 2004, Waaler 1984). For women, stature predicts the health of offspring (Bhalotra and Rawlings forthcoming).
8. Conclusions
The unconditional within-groups estimate of the poverty elasticity of infant mortality is 1. Conditional upon state income it is 0.37. Changes in poverty and income are estimated to have made significant independent contributions, explaining as much as 21% and 60% respectively of the mortality decline observed in India between the early 1970s and the early 1990s. The poverty and income elasticities of mortality are both declining over time since the initiation of economic liberalization in India in 1981. Both elasticities are invariant to controlling for income inequality, suggesting that poverty is picking up deprivation rather than inequality. The estimates suggest that for a given level of income and poverty incidence, redistribution has no impact on infant mortality. Conditioning upon state health expenditure brings the poverty and income elasticities into line (they are identical) although the stronger trend in income in the period means that it contributed more to the observed trend in mortality. In a model with flexible controls for omitted trends at the national and state levels, poverty ceases to make a significant contribution and the contribution of income falls to 31%. Trends in poverty in the Indian states are correlated with trends in education and fertility, each of which is estimated to have made significant contributions to mortality decline.
References
Acemoglu D, S Johnson, J Robinson (2001). The colonial origins of comparative
development: An empirical investigation. The American Economic Review, Vol. 91, No. 5
Dec., pp. 1369-1401
Abdala F, R Geldstein and S Mychaszula (2000), Economic reestructuring and mortality
changes in Argentina: Is there any connection? In G. Cornia and R. Paniccià (eds), The
Mortality Crisis in Transitional Economies, New York: Oxford University Press, pp. 328–50. Ahmad, OB, AD Lopez and M Inoue (2000). The decline in child mortality: A reappraisal. Bulletin of the World Health Organization, 78:10, pp. 1175-91.
Almond, D., Currie, J., 2010. Human capital development before age five. NBER Working Paper No. 15827.
Anand, S. and M Ravallion (1993). Human Development in Poor Countries: On the Role of Private Incomes and Public Services. The Journal of Economic Perspectives, Vol. 7, No. 1, Winter, pp. 133-150
Besley T and R Burgess (2003). Halving global poverty. Journal of Economic Perspectives, vol. 17, issue 3, pages 3-22.
Besley T and R Burgess (2004). Can labor regulation hinder economic performance? evidence
from India. Quarterly Journal of Economics, 119:1, 91-134.
Besley T, R Burgess and B Esteve-Volart (2006). The policy origins of poverty and growth in
India. Chapter 3 in Delivering on the Promise of Pro-Poor Growth, ed. by Tim Besley and
Louise Cord, Palgrave Macmillan and The World Bank.
Bhalotra S. 2007a. Spending to save? State health expenditure and infant mortality in India. Health Economics, 16(9), September 2007.
Bhalotra S. 2007b. Wuthering heights: birth shocks and adult stature in India. Mimeograph. University of Bristol.
Bhalotra S. 2008a. Sibling-Linked Data in the Demographic and Health Surveys. Economic
and Political Weekly, Nov 29- Dec 5, 2008, Vol. XLIII(48), 39-44.
Bhalotra S. 2008b. Childhood mortality and economic growth in India. Chapter 6, M.
McGillivray (ed.), Achieving the Millennium Development Goals, Palgrave-McMillan & the
United Nations University-WIDER.
Bhalotra S and A van Soest 2008. Birth-spacing, fertility and neonatal mortality in India:
dynamics, frailty and fecundity. Journal ofEconometrics, Vol. 143 (2), April, 274-290.
Bhalotra S. and A. Venkataramani. 2010. Long-Run and intergenerational impacts of disease and medical technology: evidence from the sulfa drug innovation. Mimeograph, presented at the AEA meetings in Denver. University of Bristol and University of Washington St Louis.
Bhalotra, S. 2010a. Fatal fluctuations: Cyclicality in infant mortality in India. Journal of
Development Economics. Volume 93, Issue 1, September 2010, Pages 7-19
Bhalotra S. 2010b. The intergenerational spillover of early life conditions. Mimeograph, University of Bristol.
Bhalotra, S and S. Rawlings. Intergenerational persistence in health in developing countries:
The penalty of gender inequality? , Journal of Public Economics, forthcoming
Black, R., S. Morris and J. Bryce 2003. Where and why are 10 million children dying every year? Lancet, 361, pp. 2226-34.
Cutler, D., A. Deaton and A. Lleras-Muney 2006. The determinants of mortality, Journal of
Economic Perspectives, 20(3), Summer.
Datt G and M Ravallion 2002. Is India’s economic growth leaving the poor behind? Journal of
Economic Perspectives, 16(3), 89-108.
Deaton A and V Kozel 2005. Data and dogma: the great Indian poverty debate, World Bank
Research Observer, Fall, 20 (2): 177-199.
Deaton A and J Dreze 2002. Poverty and Inequality in India: A Re-Examination. Economic
and Political Weekly, Vol. 37, No. 36, Sep. 7-13, pp. 3729-3748.
Deaton A 2007a. Global patterns of income and health: facts, interpretations, and policies, WIDER Annual Lecture, Helsinki, September.
Deaton 2007b, ‘Height, health and development’ Proceedings of the National Academy of
Sciences of the United States of America, Vol. 104, No. 33, pp. 13232-13237.
Dehejia, R. and A. Lleras-Muney 2004, Booms, busts, and babies' health, Quarterly Journal of
Economics, MIT Press, Vol. 119(3), pp. 1091-1130.
Dollar D and A Kraay (2002). Growth is good for the poor. Journal of Economic Growth,
Dreze J and A Sen (1995). India, Economic Development and Social Opportunity, Oxford University Press.
Ferreira F and N Schady 2009. Aggregate economic shocks, child schooling, and child health. The World Bank Research Observer.
Fogel, R. W., 2004. Health, nutrition, and economic growth. Economic Development and
Cultural Change 52 (3), 643-658.
IIPS and ORC Macro (2000), National Family Health Survey (NFHS-2) 1998-9: India. Mumbai:
International Institute for Population Sciences (IIPS).
Johnson, S., Larson, W., Papageorgiou, C. and Subramanian, A. (2009). Is newer better? The Penn world table revisions and the cross-country growth literature, NBER Working Paper 15455.
Jones, R. et al. (2003), How many child deaths can we prevent this year?, The Lancet, 362, 5:
65-71.
Koren M and S Tenreyro (2007). Volatility and development. The Quarterly Journal of
Economics, 122:243–287.
Lanjouw, P and M Ravallion (1995), Poverty and household size. Economic Journal. 105
(November) 1415-1434
Miller, G. and P. Urdinola (2007), Time vs. money in child health production: the case of
coffee price fluctuations and child survival in Colombia, Quarterly Journal of Economics,
forthcoming.
Ortega O and D Reher (1997), Short-term economic fluctuations and demographic behaviour: Some examples from 20th-century South America, in G. Tapinos, A. Mason and
J. Bravo (eds.), Demographic Responses to Economic Adjustment in Latin America, Oxford:
Clarendon Press, pp. 129–55.
Ozler B, G Datt and M Ravallion (1996). A database on poverty and growth in India, Development Research Group, Washington DC: The World Bank.
Palloni A and K Hill (1997). The effects of economic changes on mortality by age and cause:
Latin America, 1950-1990, in G. Tapinos, A. Mason and J. Bravo (eds.), Demographic
Responses to Economic Adjustment in Latin America, Oxford: Clarendon Press, pp. 75-128. Preston, SH (1975), The changing relation between mortality and level of economic
development”, Population Studies, 29(2), July, 231-248.
Pritchett, L (2000). Understanding patterns of economic growth: searching for hills among
plateaus, mountains, and plains. The World Bank Economic Review 14(2), 221-250.
Pritchett L and LH Summers (1996). Wealthier is healthier. Journal of Human Resources,
31(4), pp.841-68.
Reidpath D and Allotey P (2003). Infant mortality rate as an indicator of population health. Journal of Epidemiology and Community Health 57 (5), 344-346.
Ross, M. (2006), Is democracy good for the poor? Mimeograph, UCLA Department of
Political Science, Forthcoming, American Journal of Political Science.
Ruhm CJ (2000). Are recessions good for your health? Quarterly Journal of Economics, 115(2),
pp. 617-50.
Ruhm CJ (2005), Mortality increases during economic upturns, International Journal of
Epidemiology, Vol. 34, No. 6, December, 1206-1211.
Scrimshaw N, C Taylor and J Gordon 1968, Interactions of nutrition and infection. World Health Organisation monograph series No. 57.
Virmani A (2004), 'India's Economic Growth: From Socialist Rate of Growth to Bharatiya Rate of Growth'. Working Paper No. 122, New Delhi: Indian Council for Research on Internatioinal Relations (ICRIER)
Van den Berg, G.J., M. Lindeboom and F. Portrait (2006), Economic conditions early in life and individual mortality, American Economic Review 96, 290-302.
Van den Berg, G.J., G. Doblhammer and K. Christensen. 2008. Being born under adverse economic conditions leads to a higher cardiovascular mortality rate later in life - evidence based on individuals born at different stages of the business cycle. Bonn: IZA Discussion Paper 3635.
Waaler, HT (1984), ‘Height, Weight, and Mortality: The Norwegian Experience’ Acta Medica
Scandinava, Vol. 77, pp. 279-303.
Yamano, T, H Alderman and L Christiaensen. (2005). Child growth, shocks, and food aid in
Figure 1: Density of infant mortality and poverty rates
Figure 2: All-India trends in infant mortality, poverty and log state income
Notes: The top panel shows trends in mortality and poverty rates on the left and in the mortality rate and average income on the right. The bottom panel presents the trends in mortality and poverty smoothed using lowess, with levels on the left and logarithms on the right. There is a dip in infant mortality in 1973 for which there is no evident explanation. This is apparent in every state. It will therefore be absorbed by year dummies in the specification that includes them. I have
confirmed that excluding this year from the sample does not change the poverty elasticity of mortality.
Figure 3: State-specific trends in infant mortality, poverty and log state income
Notes: The state acronyms are matched to state names in Table 5. It is difficult to identify the state labels when the Figure is presented without colour but for a more systematic account of levels and trends, refer to Table 1. Figures with colour are in a pdf of the paper at
Figure 4: The relationship of mortality with poverty and income between states, time-averages, lowess fit
Figure 6: The mortality-poverty relationship by state- linear fits on time variation
Figure 7: The mortality-income relationship by state- linear fits on time variation
Table 1: Descriptive Statistics: Rural Mortality and Poverty
Infant mortality Poverty headcount rate log(Infant mortality) log( Poverty headcount rate) rural pop/ pop/ state
mean dev. st. rate of linear
decline mean st. dev. linear rate of decline mean st. dev. log linear rate of
decline mean st. dev.
log linear rate of decline
total
pop total pop
Andhra Pradesh 9.65 3.14 -0.267 41.45 10.50 -1.152 2.22 0.33 -0.029 3.69 0.25 -0.027 0.76 8.14 Assam 6.61 2.76 -0.147 50.91 6.78 -0.511 1.82 0.38 -0.017 3.92 0.13 -0.010 0.90 2.75 Bihar 8.52 2.80 -0.217 64.41 4.44 -0.376 2.10 0.29 -0.023 4.16 0.07 -0.006 0.88 10.70 Gujarat 10.07 4.23 -0.327 45.52 10.17 -1.116 2.23 0.38 -0.029 3.79 0.24 -0.026 0.68 5.12 Haryana 7.87 3.61 -0.143 28.36 5.79 -0.317 1.98 0.41 -0.010 3.32 0.21 -0.011 0.78 1.99 Karnataka 9.10 3.67 -0.305 50.42 5.84 -0.458 2.14 0.38 -0.032 3.91 0.12 -0.009 0.71 5.56 Kerala 3.67 2.81 -0.215 44.76 13.19 -1.559 0.75 1.63 -0.098 3.76 0.29 -0.035 0.79 3.75 Madhya Pradesh 12.88 3.80 -0.330 55.07 7.83 -0.872 2.51 0.32 -0.027 4.00 0.14 -0.016 0.79 8.03 Maharashtra 8.69 3.66 -0.295 59.40 10.90 -1.069 2.08 0.44 -0.035 4.07 0.18 -0.018 0.64 9.63 Orissa 11.03 3.23 -0.300 50.80 11.29 -1.255 2.36 0.29 -0.028 3.90 0.24 -0.026 0.88 3.98 Punjab 6.86 3.24 -0.164 20.22 4.98 -0.495 1.61 1.34 0.002 2.98 0.25 -0.024 0.72 2.53 Rajasthan 12.03 3.86 -0.293 51.16 7.56 -0.636 2.43 0.34 -0.024 3.92 0.15 -0.013 0.79 5.25 Tamil Nadu 8.97 4.45 -0.375 49.58 10.85 -1.216 2.07 0.53 -0.041 3.88 0.26 -0.027 0.66 7.20 Uttar Pradesh 15.11 5.91 -0.615 43.79 5.87 -0.489 2.64 0.38 -0.041 3.77 0.14 -0.011 0.82 17.01 West Bengal 9.32 5.13 -0.485 43.76 14.03 -1.644 2.10 0.53 -0.053 3.72 0.34 -0.040 0.73 8.34 India 9.36 4.63 -0.299 46.64 13.98 -0.878 2.07 0.78 -0.032 3.79 0.35 -0.020 0.77 100
Notes: The infant mortality and poverty rates are in percentages in the first two panels and in logarithms of the percentages in the next two. Rates of decline are estimated by regressing the level or log on a linear trend. st dev is standard deviation, pop is population.
Table 2a: The poverty elasticity of infant mortality: with and without conditioning upon state income
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10)
Panel A: Unconditional on state income Panel B: Conditional on state income
Dependent var: infant
mortality rate correlation state effects fixed controls year effects fixed trends state correlation state effects fixed controls year effects fixed state trends
log poverty rate 0.051* 0.096* 0.0265 0.007 -0.006 0.020 0.035* 0.016 0.005 -0.010
[0.012] [0.010] [0.012] [0.016] [0.006] [0.017] [0.012] [0.012] [0.016] [0.006]
poverty elasticity 0.55 1.03 0.28 0 0 0.21 0.37 0 0 0
log state income p.c. -0.040+ -0.063* -0.031* -0.011 -0.032*
[0.021] [0.007] [0.012] [0.026] [0.014]
income elasticity -0.43 -0.67 -0.33 0 -0.34
R-squared (within state) 0.148 0.284 0.521 0.530 0.597 0.199 0.366 0.529 0.530 0.600
* p<0.05, + p<0.10
Notes: The number of observations is 420, 15 states and 28 years. Since the dependent variable, infant mortality, is in levels, poverty and income elasticities are calculated as the estimated coefficients divided by the sample mean of infant mortality (0.0936). A zero indicates an insignificantly small elasticity. Infant mortality and poverty rates are state averages for rural households while income is the overall state net domestic product per capita deflated by the consumer price index. Columns 3 and 8 include the following covariates, each expressed as a percentage of mothers (or fathers) in the state-year with the named characteristic: religion, caste, educational level, age of mother at birth, birth order. They also include the z-score of rainfall split as positive and negative shocks. Estimates in columns 4 and 5 and in columns 9 and 10 are without these covariates.
Table 2b: The poverty and income elasticity of infant mortality conditional upon state health expenditure
(1) (2) (3) (4)
Dep var: infant mortality rate Panel A: Unconditional on
income Panel B: Conditional on income
log poverty rate 0.096* 0.034* 0.035* 0.025
[0.010] [0.015] [0.012] [0.014]
poverty elasticity 1.03 0.37 0.37 0.27
log state income p.c. -0.063* -0.025*
[0.007] [0.011]
income elasticity -0.67 -0.27
log state health expend p.c. -0.043* -0.033*
[0.008] [0.012]
health expenditure elasticity -0.46 -0.33
R-squared 0.284 0.390 0.366 0.396
Notes: see Notes to Table 2a. State health expenditure per capita is deflated by the consumer price index. It is added to the specifications in columns 2 and 7 in Table 2a which are repeated in columns 1 and 3 in this Table for convenience.
Table 3: The Income elasticity of poverty
(1) (2) (3) (4) (5) (6)
Dependent variable: log poverty rate correlation state FE year FE state trends controls drop trends
log state income p.c. -0.669* -0.604* -0.313* -0.188* -0.218* -0.372*
[0.160] [0.068] [0.119] [0.085] [0.094] [0.065]
R-squared 0.513 0.580 0.671 0.802 0.823 0.677
Notes: The changes to the specification described in the column heads are cumulative. In column 6, year fixed effects and state trends are dropped. Since both income and poverty are in logarithms, the coefficients are the elasticities. FE is fixed effects. Also see notes to Table 2a.
Table 4a: Robustness checks
(1) (2) (3) (4) (5) (6) (7)
dep var: infant mortality rate baseline birth year>197 7
structural
break:1991 state pop weights lag poverty poverty levels log mortality
log poverty rate 0.035* 0.013 0.043* 0.040* 0.372
[0.012] [0.009] [0.015] [0.011] [0.404]
log state income p.c. -0.063* -0.054* -0.062* -0.066* -0.061* -0.054* -0.744*
[0.007] [0.008] [0.006] [0.011] [0.009] [0.007] [0.138]
log poverty rate*post-1991 -0.019*
[0.007]
log state income p.c.*post-1991 0.010*
[0.003]
lag(log poverty rate) 0.034*
[0.010]
poverty rate (levels) 0.001*
[0.000]
R-squared 0.366 0.294 0.376 0.384 0.384 0.379 0.161
Notes: The baseline specification is column 7 of Table 2. Column 2 truncates births that occur more than 20 years before the survey date to limit potential problems with long retrospective windows. Column 3 investigates heterogeneity in the coefficients as a function of economic reforms which intensified in 1991. Column 4 weights by the square root of the average state population. Column 5 replaces current log poverty with its lag. Column 6 replaces current log poverty with its level (i.e. removing the logarithm). Column 7 replaces the mortality rate in levels with its log to yield a log-log specification. In column 7, the coefficient is the elasticity. In column 6, the elasticity is the coefficient multiplied by mean poverty and divided by mean mortality; sample means are in Table 1. In other columns, elasticities are calculated as in Table 2a. Also see Notes to Table 2a.
Table 4b: Robustness checks: Alternative measures of mortality, poverty and income
(1) (2) (3) (4) (5) (6) (7) (8)
neonatal under5 poverty squared poverty mean inequality headcount & square of
mortality mortality gap gap consumption inequality income
log poverty rate 0.023* 0.046* 0.034* 0.036*
[0.009] [0.018] [0.012] [0.012]
log state income p.c. -0.038* -0.095* -0.074* -0.067* -0.071* -0.081* -0.062* -0.386*
[0.006] [0.011] [0.008] [0.007] [0.007] [0.008] [0.007] [0.139]
log poverty gap 0.009+
[0.005]
log squared poverty gap 0.012*
[0.004]
log mean consumption p.c. -0.047*
[0.018]
log inequality (gini) 0.019+ 0.013
[0.011] [0.010]
square of log state income pc 0.023*
[0.009]
R-squared 0.258 0.447 0.349 0.354 0.361 0.353 0.367 0.374
Notes: The dependent variable is changed from infant mortality to neonatal and under-5 mortality respectively in columns 1 and 2. In columns 3-6, the poverty headcount rate is replaced by alternative measures of poverty. In column 7, inequality is entered alongside the poverty headcount rate and in column 8, the linear is replaced with a quadratic function of log state income. Also see Notes to Table 2a.