Knowledge for Clinical Practice
WWW.DENTALLEARNING.NET
A PEER-REVIEWED PUBLICATION A PEER-REVIEWED PUBLICATION
D
ENTAL
L
EARNING
Failed Integrated Implants Using
Minimally Invasive Techniques
Removal of
Case Series
Stuart J. Froum DDS, Sang-Choon Cho DDS, Kibong Kim DDS
PART 2 IN A SERIES INSIDE Earn 2
CE
Credits
Written for dentists, hygienists and assistantsApproved PACE Program Provider FAGD/MAGD
Dental Learning, LLC is a Dental Board of California CE Provider. The California Provider # is RP5062. All of the information
EDUCATIONAL OBJECTIVES
The overall goal of this article is to provide the reader with information on the frequency of use of the various implant removal techniques at one clinical teaching center. Informa-tion is provided on each of the removal techniques, with emphasis on the indications, effectiveness, limitations and complications of each technique when removing a hopeless but still integrated implant.
On completing this article, the reader will be able to do the following:
1. List the etiologies of failed implants;
2. Describe the counter-ratchet and reverse screw techniques that can be utilized for minimally invasive implant removal; 3. Review the indications and use of piezo tips and
high-speed burs for implant removal;
4. Review the use of trephine burs for implant removal and the technique that should be used; and
5. List and describe the considerations and limitations in selecting an implant removal technique.
SPONSOR/PROVIDER: This is a Dental Learning, LLC continuing education activity. DESIGNATION STATEMENTS: Dental Learning, LLC is an ADA CERP recognized provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Dental Learning LLC designates this activity for 2 CE credits. Dental Learning is also designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from 2/1/2016 - 1/31/2020. Provider ID: # 346890 Dental Learning, LLC is a Dental Board of California CE provider. The California Provider number is RP5062. This course meets the Dental Board of California’s requirements for 2 units of continuing education. EDUCATIONAL METHODS: This course is a self-instructional journal and web activity. Information shared in this course is based on current information and evidence. REGISTRATION: The cost of this CE course is $29.00 for 2 CE credits. ORIGINAL RELEASE DATE: August 2012. REVIEW DATE: July 2015. EXPIRATION DATE: June 2018. REQUIREMENTS FOR SUCCESSFUL COMPLETION: To obtain 2 CE credits for this educational activity, participants must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%. AUTHENTICITY STATEMENT: The images in this course have not been altered. SCIENTIFIC INTEGRITY STATEMENT: Information shared in this continuing education activity is developed from clinical research and represents the most current information available from evidenced-based dentistry. KNOWN BENEFITS AND LIMITATIONS: Information in this continuing education activity is derived from data and information obtained from the reference section. EDUCATIONAL DISCLAIMER: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the field related to the course topic. It is a combination of many educational courses and clini-cal experience that allows the participant to develop skills and expertise. PROVIDER DISCLOSURE: Dental Learning does not have a leadership position or a commercial interest in any products that are mentioned in this article. No manufacturer or third party has had any input into the development of course content. CE PLANNER DISCLOSURE: The planner of this course, Casey Warner, does not have a leadership or commercial interest in any products that are mentioned in this article or any other products or services discussed in this educational activity. She can be reached at [email protected]. TARGET AUDIENCE: This course was written for dentists, dental hygienists, and assistants, from novice to skilled. CANCELLATION/REFUND POLICY: Any participant who is not 100% satisfied with this course can request a full refund by contacting Dental Learning, LLC, in writing. Go Green, Go Online to www.dentallearning.net take your course. Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected]. Go Green, Go Online to www.dentallearning.net take your course. © 2015
Dr. Stuart J. Froum is an international lecturer and has been in private practice for over 35 years. He is on the Research Committee for the Academy of Osseointegra-tion, and is the Vice President of the American Academy of Periodontology where he has previously served as Board Liaison to the Continuing Education Oversight Committee, a member of the Con tinuing Education Committee and as a District Trustee. Dr. Froum has published over 100 articles in peer-reviewed journals, was the editor for the recently-pub lished book titled ‘Dental Implant Complications Etiology, Prevention and Treat ment’, co-author of ‘Compre-hensive Periodontics for the Dental Hygienist’ (2001), and a contributing author for the 11th edition of Carranza’s Clinical Periodontology as well as a co-author of 3 chapters in ‘Sinus Bone Graft’ (2006) and Implant Site Development (2010). He is also a reviewer for the Journal of Periodontology, Inter national Journal of Periodontics and Restorative Dentistry and for Com-pendium. Dr. Froum was awarded the William J. Gies Award for Service to the American Academy of Periodontology in 2006, the American Academy of Periodontology “The Special Citation Award” in 2005, the Hirschfeld Award – NESP in 1999, the Clinical Research Award in both 2004 and 2005, and the J. Coslet – Distinguished Lecturer Award from the University of Pennsylvania Dental School in 2003.
Sang-Choon Cho DDS, MS
Dr. Sang-Choon Cho is a full-time Clinical Assistant Profes-sor and Director of Advanced Program for International Dentists in Implant Dentistry in the Department of Peri-odontology and Implant Dentistry, at New York University College of Dentistry (NYUCD). He is a graduate of both the DDS program and the Advanced Program in Implant Den-tistry for International Dentists at NYUCD and also holds a dental degree and an MS degree from Kyungpook National University in South Korea. In addition to teaching and conducting research at NYUCD, Dr. Cho serves as a liaison to the NYUCD South Korean Alumni Study Club.
Kibong Kim DDS
Dr. Kibong Kim is a Resident of the Advanced Program for International Dentists in Implant Dentistry at New York University College of Dentistry.
Failure of osseointegrated implants can occur due to several etiolo-gies, including implant fracture, implant malpositioning and peri-implantitis. Techniques available for the removal of failed implants include counter-ratchet techniques; reverse screw techniques; and the use of piezo tips, high-speed burs and trephines for bone re-moval around implants. The rere-moval of failed, nonmobile implants requires careful consideration of the least invasive technique that can be used in a given situation as well as the post-removal site.
CE Editor FIONA M. COLLINS Managing Editor BRIAN DONAHUE Creative Director MICHAEL HUBERT Art Director MICHAEL MOLFETTO
Copyright 2015 by Dental Learning, LLC. No part of this publication may be repro-duced or transmitted in any form without prewritten permission from the publisher.
500 Craig Road, First Floor, Manalapan, NJ 07726
Introduction
T
he use of dental implants in the treatment of total or partial edentulism has demonstrated a high de-gree of success, with documented survival rates of 90% to 97%.1,2 Although improvements in implant designand surface microtopography in recent years have resulted in increased success rates of dental implants, between 3% and 10% of implants still fail.3,4 With the
approxi-mately 2 million new implants that are placed worldwide every year, and tens of millions of dental implants cur-rently in function, the estimated number of implants that are failing annually is estimated to be in the range of 200,000–250,000.5 Meanwhile, criteria to determine
suc-cessful integration of dental implants have been proposed.6
Among these, lack of mobility is a primary prerequisite. In cases where an implant demonstrates mobility, all parts of the implant should be immediately removed to prevent progressive destruction of the surrounding tissue. However, even when implants have no mobility, indications for their removal include implant fracture, malposition, infection, pain and advanced peri-implantitis.6
In many cases, failed but nonmobile implants are removed by surgical intervention. Various methods of implant removal are available and include the use of a counter-ratchet technique (CRT), reverse screw technique (RST), piezo tips, high-speed burs, elevators, forceps and trephine burs.7 Generally, these techniques are used alone
or in combination, depending on the clinical situation. However, when removal of an implant is necessary, the least invasive method should be the first option, in order to preserve the site for the possible future treatment and allow for an esthetic replacement, whether an implant restoration or pontic.
Material and Methods
Clinical data in this study was obtained from the Implant Database (ID), which was certified by the Office of Quality Assurance at the New York University Col-lege of Dentistry (NYUCD) Kriser Dental Center. This data was extracted as de-identified information from the routine treatment of patients at the Ashman Department of Periodontology and Implant Dentistry (ADPID) at the NYUCD. This use of the database was in compliance with the Health Insurance Portability and Accountability Act (HIPAA) requirements and approved by the University Committee on Activities Involving Human Subjects.
Advanced peri-implantitis with prolonged pain or signs of continuous infection, fractured implants at either the time of insertion or any time following loading, and malpositioned implants in the esthetic zone with occur-rence of peri-implantitis were included in this study. All of these failed implants showed no mobility, which was assessed on freestanding implants by the application of pressure by two opposing instruments. If a prosthesis was present, this was evaluated for mobility and an assess-ment made to determine whether the prosthesis or the supporting implant (requiring removal of the prosthesis) was mobile. From September 2010 to January 2012, 67 failed, nonmobile dental implants were removed in the ADPID at the NYUCD Kriser Dental Center. At the time of implant removal, a decision tree from a previ-ous article was used to select the least invasive removal technique.7 For cases amenable to removal with the least
invasive method, the implant connection, implant diam-eter, implant geometry, amount of osseointegration re-maining, and patency of the internal or external connec-tion were evaluated. Following this evaluaconnec-tion, when the
Removal of
Failed Integrated Implants Using
Minimally Invasive Techniques
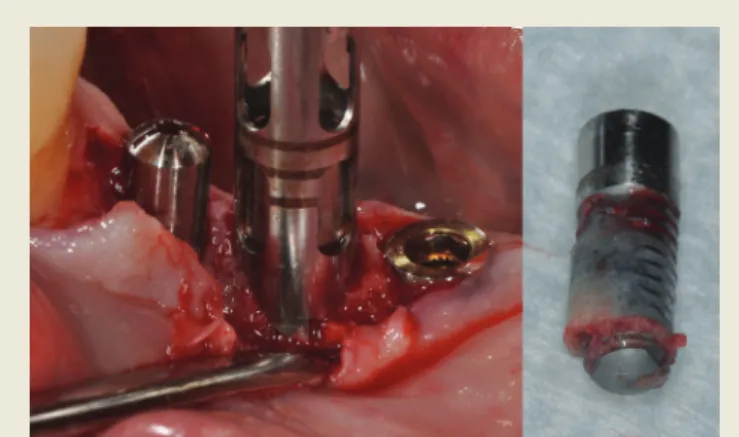
counter-ratchet technique (CRT) was used to remove the implant, the mount and the torque driver of the corre-sponding implant manufacturer were utilized. Whenever the reverse screw technique (RST) was used, the conical explant kit (CEK, EBI Inc., Kyungsan, South Korea) was utilized (Fig. 1). The instrument was inserted manually and turned counterclockwise. Torque was applied with a torque wrench (Sybron, Orange, CA) until the implant was mobilized. Bone removal techniques or combination techniques were used when CRT and RST failed or were not able to be used to retrieve the implants planned for removal.
Results
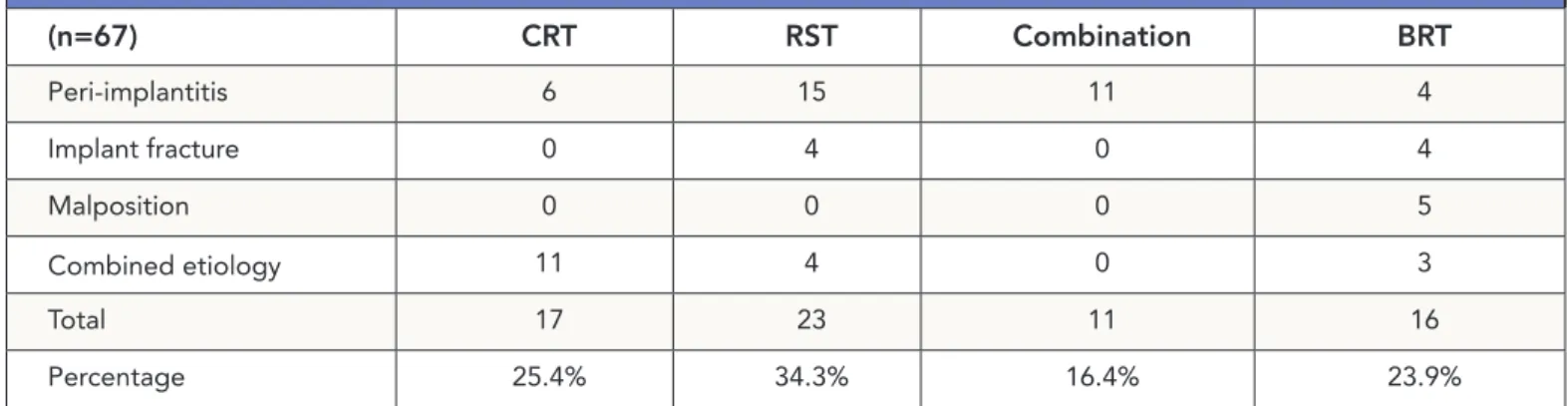
Of the total of 67 nonmobile implants diagnosed as failed and surgically removed, peri-implantitis affected 36 implants, 8 implants were fractured, 5 maxillary anterior implants were malpositioned and the remaining 18 failed implants presented with a combined etiology. The fre-quency of use of CRT, RST, BRT (bone removal technique) and combination technique are summarized in Table 1. The rates of use of each of these techniques were 25.4%, 34.3%, 23.9% and 16.4%, respectively.
Discussion
Approximately 60% of the implants in this case report were removed by minimally invasive techniques (CRT and RST). The RST (CEK) alone was able to remove more than 1⁄3 of the implants in the present study. Thus, the clinician should consider these techniques first if implant removal becomes necessary. Treatment planning for the post-removal site should be considered prior to implant removal. After removing a failed implant, the placement of an immediate replacement implant is often dependent on the amount and distribution of residual bone. Several authors have stated that following implant or tooth removal that guided bone regeneration (GBR) procedures are unnecessary for four-wall socket sites with no fenestrations or dehiscences and a gap distance <2 mm between replacement implant surface and surrounding bone walls.8,9 However, if the implant socket Table 1. Reason for implant failure, and removal technique
(n=67) CRT RST Combination BRT Peri-implantitis 6 15 11 4 Implant fracture 0 4 0 4 Malposition 0 0 0 5 Combined etiology 11 4 0 3 Total 17 23 11 16 Percentage 25.4% 34.3% 16.4% 23.9%
Figure 1. Removal of a stripped screw, ruptured implant and external type implant with the versatile CEK instrument.
Removal of
Failed Integrated Implants
Using Minimally Invasive Techniques
- Case Series
contains fewer than three walls, use of GBR procedures as well as knowledge of the classification of the extraction sock-et type is helpful in treatment planning the augmentation of the socket defect prior to placement of a new implant.10
In the anterior maxillary esthetic zone, an immo-bile failed implant should always be removed whenever possible by using a reverse torque technique in order to preserve soft and hard tissues. Moreover, preservation of the bone during removal of the implant can help avoid or reduce the necessity of future augmentation procedures to allow placement of a new implant. This is essential because the literature suggests that replacement implants have a decreased survival rate.11,12 The following review of the
im-plant removal techniques will vary from the least to most invasive in terms of collateral damage to surrounding soft tissue, bone and teeth.
Removal Instruments, Indications and
Tech-niques: Counter-ratchet and Reverse Screw
Techniques (CRT and RST)
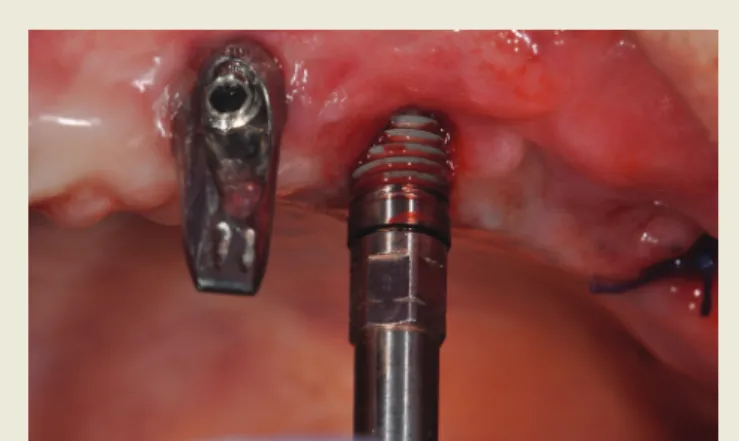
These techniques are the least invasive in removing an implant without damaging surrounding structures. Cases amenable to removal with counter-torque ratchets depend on the implant connection (external hex/internal hex), patency of the internal or external connection, implant diameter, implant geometry, implant location (bone qual-ity), and amount of osseointegration remaining. The use of counter-torque wrenches should be considered the option of choice if the implant is able to be engaged and reverse-torqued until mobile (Fig. 2). RST is the second of the less invasive techniques, indicated in the removal of a fractured implant when the connection is damaged or in the removal of an external connection implant when the counter-torque ratchet cannot be engaged (Fig. 3).
Bone Removal Techniques (BRTs)
Piezo Tips
The use of piezo tips to remove bone surrounding an implant is less invasive than high-speed burs during cut-ting, because they prevent damage to the surrounding soft
tissue.13,14 The bone healing response with piezo surgery
also seems to be more favorable than that with burs.15
However, when deep cuts in bone are necessary, the cutting speed of the piezo tips is decreased and this results in a rise in temperature. Therefore, cooling of the tip by intermit-tent cutting, the use of copious irrigation with cold saline and constant movement of the tip is recommended. High-speed Burs
The use of high-speed burs under copious irrigation is an efficient technique to remove a failed implant. The burs of choice are thin, tapered diamond burs. Chan-nels should be cut on the mesial and distal aspects
Figure 3. Reverse screw technique (RST) Figure 2. Counter-ratchet technique (CRT)
of the implant to avoid damaging buccal and lingual bone. However, air from the high-speed handpiece may be forced into a surgical wound or a laceration in the mouth, causing an air embolism.16 When using high-speed
burs, the residual apical part of the implant should be approached carefully when in proximity to vital struc-tures such as the sinus membrane, inferior alveolar nerve and mental foramen, in order to prevent damage to these. Moreover, pieces of the implant surface may enter the healing wound and should be removed by frequent saline irrigation as part of the procedure. Before using the burs, accurate radiographs to locate anatomical structures are recommended.
Trephine Burs
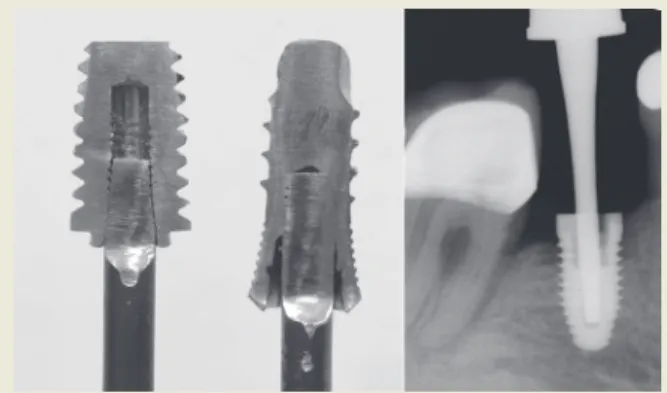
There are several sizes of trephines available correspond-ing to various implant diameters. The smallest effective-size trephine should be selected to avoid collateral damage to the neighboring bone, teeth and/or implants (Fig. 4), and the internal diameter of the trephine should be slightly larger than the implant to avoid engaging the implant body. The preferred speed when using a trephine is 1,200 rpm to 1,500 rpm with copious irrigation. This technique is one of the most invasive options for implant removal. Fatigue fracture of the mandible after the use of a trephine bur has been reported,17 and osteomyelitis is another complication
that may occur following explantation with a trephine bur if bone is overheated.18 Thus, trephine burs are only
indi-cated when absolutely necessary, and the retrieval procedure should be carefully planned and performed under copious irrigation with refrigerator-cooled saline.18 Again,
intermit-tent cutting is recommended, moving the trephine in an apical then coronal direction. For those implants with ex-panded platforms, the implant platform should be trimmed or resected in order to use the smallest diameter of trephine burs possible. Often, only the coronal half of bone around the implant requires removal in order to loosen the im-plant, at which point elevators, forceps and, where possible, torque drivers may be employed as part of a combination technique described below.
Combination Techniques
When an integrated implant cannot be removed with less invasive methods, piezo tips and/or high-speed dia-mond burs should be used to remove sufficient supporting bone around the coronal parts of the implant. The counter-torque ratchets or forceps should then be employed to remove the implant, to reduce the damage to the surround-ing bone (Fig. 5). Whenever burs are used, cuts should be made on the mesial and distal aspects of the implant. Alternating between the counter-torque ratchet and the elevator and occasionally drilling with the tapered dia-mond burs or trephines can then be used in combination to remove the implant.
Figure 5. Combination technique, BRT + RST
Removal of
Failed Integrated Implants
Using Minimally Invasive Techniques
- Case Series
One of the subjects in this study was referred to the Ashman Department of Prosthodontic Dentistry at the NYUCD for removal of failed implants. The subject pre-sented with 10 failing implants affected by peri-implanti-tis. Due to the different degrees of severity and bone loss caused by peri-implantitis, 3 different techniques were required to remove these implants. Four of the mobile implants were removed by forceps. The other 6 implants were removed with RST and trephine burs (Figs. 6-10). This case was interesting, in that indications and limita-tions of the two less invasive techniques and BRT were all apparent within one subject.
Figure 8. Implant removal with BRT (left) and RST (right)
Figure 9. The extracted teeth and implants
Figure 10. The healed maxillary and mandibular ridges following implant removal
Figure 7. Before implant removal
Limitations and Considerations of Less
Invasive Techniques
The choice of implant removal technique should be based on the specific clinical factors such as patency of the internal or external connection, implant site, remaining amount of bone, anatomical conditions at the implant site, and bone quality. However, there are limitations and pos-sible complications that should be considered in treatment planning implant removal.
Counter-ratchet Technique (CRT)
The CRT is a convenient and minimally invasive technique for implant removal. However, to utilize this technique, the connection component should be firm and solid. When used with external hexed implants, with limited height for the connection component, CRT can easily destroy the connection. Therefore, RST should be considered to remove external connection implants. When used with internal connections, at the connection level, the connection should not demonstrate any sign of a crack, rupture or fracture that can result in further fracture of the implant when the CRT is applied (Fig. 11). In such circumstances, RST can be the indica-tion for the implant removal.
Reverse Screw Technique (RST)
The RST was used to remove more than 30% of the implants in the present study. RST devices may require 200 Ncm to 400 Ncm to remove an implant, depending on the type of RST used. The taper and diameter of the device also affects the torque that can be generated. The greatest torque is usually obtained when the device reaches the apex of the screw hole (Fig. 12). In the 41 cases in which the RST was used, there was 1 fracture of the device at the con-nection level (CEK generates up to 250 Ncm according to the EBI). In another case, the RST device was able to break the osseointegration (Fig. 13). However, due to the circu-lar thread design of the implant, it remained rotating but was not able to be removed. A trephine bur was ultimately needed to remove this implant. Therefore, use of RST is Figure 11. Implant fracture at the connection level
Figure 12. Proper binding between the RST device and implants
Figure 13. RST failed due to the circular thread design of the implant
Removal of
Failed Integrated Implants
Using Minimally Invasive Techniques
- Case Series
contraindicated for non-screw-type implants that have undercuts (i.e., Bicon or Paragon micro-vent implants).
Other Less Invasive Techniques in the
Current Literature
A recent case report by Cunliffe et al described the re-moval of a dental implant using electrosurgery.19 An
ultra-high-frequency monopolar electrosurgery unit was applied to the internal surface of the neck of the implant to cause thermonecrosis at the bone-to-implant interface. After one week, with the aid of the CRT technique, the implant was removed. This report demonstrated that heat treatment of failed implants can be used as a minimally invasive tech-nique to remove an implant. However, reliable methods of regulating the heat to implants, the human threshold and possible complications including bone necrosis should be further studied prior to recommending this technique. Moreover, the extent of bone necrosis and repair may com-plicate placement of a new implant in the same site.
Other authors (Pattison et al) have suggested the in-terposition of a foil from a suture pack between the RST device and the implant connection. This can increase the stability of the connection enough to allow for removal.20
However, this technique also requires more research.
Conclusion
Treatment planning of the post-removal site should be performed prior to implant removal. The use of less invasive implant removal techniques can provide more treatment options and better treatment outcomes. The results of the present study demonstrated a 60% retrieval rate using less invasive techniques. Thus, the clinician should consider these less invasive methods first if implant removal becomes necessary. More research on this subject is needed to evalu-ate the effectiveness and applicability of these techniques and verify the findings in the present report.
References
1. Esposito M, Grusovin MG, Coulthard P, Thomsen P, Worthington HV. A 5-year follow-up comparative analysis of the efficacy of various osseointe-grated dental implant systems: a systematic review of randomized controlled
clinical trials. Int J Oral Maxillofac Implants. 2005;20(4):557-68.
2. Romeo E, Lops D, Margutti E, Ghisolfi M, Chiapasco M, Vogel G. Long-term survival and success of oral implants in the treatment of full and partial arches: a 7-year prospective study with the ITI dental implant system. Int J Oral Maxil-lofac Implants. 2004 Mar-Apr;19(2):247-59.
3. Alsaadi G, Quirynen M, Komarek A, Van Steenberghe D. Impact of local and systemic factors on the incidence of oral implant failures, up to abutment con-nection. J Clin Periodontol. 2007;34:610-7.
4. Moy PK, Medina D, Shetty V, Aghaloo T. Dental implant failure rates and as-sociated risk factors. Int J Oral Maxillofac Implants. 2005;20(1):569-77. 5. Machtei EE, Mahler D, Oettinger-Barak O, et al. Dental implants placed in previously failed sites: survival rate and factors affecting the outcome. Clin Oral Implants Res. 2008;19(3):259-64.
6. Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants. 1986;1(1):11-25.
7. Froum S, Yamanaka T, Cho SC, Kelly R, St. James S, Elian N. Techniques to remove a failed integrated implant. Compendium. 2011;32(7):2-24.
8. Covani U, Barone A, Cornelini R, Crespi R. Clinical outcome of implants placed immediately after implant removal. J Periodontol. 2006;77(4):722-7. 9. Paolantonio M, Dolci M, Scarano A, d’Archivio D, di Placido G, Tumini V, Piattelli A. Immediate implantation in fresh extraction sockets: a controlled clinical and histological study in man. J Periodontol. 2001;72(11):1560-71. 10. Elian N, Cho SC, Froum S, Smith RB, Tarnow DP. A simplified socket classifi-cation and repair technique. Prac Periodontics Aesthet Dent. 2007;19(2):99-104. 11. Grossmann Y, Levin L. Success and survival of single dental implants placed in sites of previously failed implants. J Periodontol. 2007;78(9):1670-4. 12. Machtei EE, Horwitz J, Mahler D, Grossmann Y, Levin L. Third attempt to place implants in sites where previous surgeries have failed. J Clin Periodontol. 2011;38:195-8.
13. Vercelloti T. Piezoelectric surgery in implantology: a case report - a new piezoelectric ridge expansion technique. Int J Periodontics Restorative Dent. 2000;20(4):359-65.
14. Wallace SS, Mazor Z, Froum SJ, Cho SC, Tarnow DP. Schneiderian mem-brane perforation rate during sinus elevation using piezosurgery: clinical results of 100 consecutive cases. Int J Perio Restor Dent. 2007;27(5):413-9. 15. Preti G, Martinasso G, Peirone B, Navone R, Manzella C, Muzio G, Russo C, Canuto RA, Schierano G. Cytokines and growth factors involved in the osseointegration of oral titanium implants positioned using piezoelectric bone surgery versus a drill technique: a pilot study in minipigs. J Periodontol. 2007;78(4):716-22.
16. Reznick JB, Ardary WC. Cervicofacial subcutaneous air emphysema after dental extraction. J Am Dent Assoc. 1990;120(4):417-9.
17. Buser D, Maeglin B. Complications with ITI implants. In: Schroeder A, Sut-ter F, Buser D, Krekeler G eds. Oral implantology. Basics, IT1 hollow cylinder system. Stuttgart: Georg Thieine Verlag, 1996:445-76.
18. Esposito M, Hirsch J, Lekholm U, Thomsen P. Differential diagnosis and treatment strategies for biologic complications and failing oral implants: a review of the literature. Int J Oral Maxillofac Implants. 1999;14(4):473-90. 19. Cunliffe J, Barclay C. Removal of a dental implant: an unusual case report. J Dent Implants. 2011;1(1):22-5.
20. Pattison G, Reynold J, Hardy J. Salvaging a stripped drive connection when removing screws. Injury. 1999;30:74-5.
Webliography
American Academy of Periodontology. Position Paper. Dental Implants in Periodontal Therapy. Available at: http://www.perio.org/resources-products/ pdf/31-implants.pdf
Comprehensive Periodontal Therapy: A Statement by the American Academy of Periodontology. Available at: http://www.perio.org/resources-products/ pdf/periodontal-therapy_statement.pdf
1. Documented survival rates for implants range from __________.
a. 80% to 87% b. 85% to 93% c. 90% to 97% d. none of the above
2. Approximately __________ new implants are placed annually worldwide.
a. one million b. two million c. three million d. four million
3. Lack of mobility is __________ for successful osseointegration of dental implants.
a. an initial requirement b. a primary prerequisite c. a secondary requirement d. all of the above
4. __________ is an indication for implant removal.
a. Fracture of the implant b. Pain
c. Infection d. all of the above
5. When removal of an implant is necessary, the __________ method should be the first option.
a. quickest b. least invasive c. most convenient d. none of the above
6. The implant __________ must be evaluated prior to using the least invasive method for implant removal.
a. diameter b. connection c. geometry d. all of the above
7. The mount and the torque driver of the corresponding implant manufacturer are utilized when the __________ technique is used.
a. counter-ratchet b. reverse screw c. piezo
d. all of the above
8. If an implant socket contains fewer than three walls, __________ is helpful in treatment planning.
a. use of guided bone regeneration procedures
b. knowledge of the classification of the extraction socket type c. use of electrophoresis
9. A conical explant kit is used with the __________ technique.
a. counter-ratchet b. reverse screw c. trephine
d. none of the above
10. Treatment planning for the post-removal site should be considered __________ implant removal.
a. prior to b. during c. following d. any of the above
11. Guided bone regeneration procedures have been considered by a number of authors to be unnecessary for four-wall socket sites with __________ and a gap distance __________ between replacement implant surface and surrounding bone wall.
a. fenestrations and dehiscences; < 2 mm b. no dehiscences or fenestrations; < 2 mm c. fenestrations and dehiscences; > 2 mm d. no dehiscences or fenestrations; > 2 mm
12. In the anterior maxillary esthetic zone, an immobile failed implant should always be removed whenever possible by using a __________ in order to preserve soft and hard tissues.
a. counter-ratchet technique b. reverse torque technique c. large trephine
d. a or b
13. The use of counter-torque wrenches should be considered the option of choice if the implant is __________.
a. already well loosened b. able to be engaged c. reverse-torqued until mobile d. b and c
14. The reverse screw technique is indicated in the removal of a fractured implant when the __________ is damaged.
a. connection b. diameter c. restoration d. all the above
15. If a counter-torque ratchet cannot be engaged for the removal of a fractured implant, the __________ technique is indicated. a. counter-ratchet b. reverse-bevel c. reverse screw d. b and c
CE
Quiz
Removal of
Failed Integrated Implants
Using Minimally Invasive Techniques
- Case Series
16. The use of __________ to remove bone surrounding an im-plant is less invasive than __________ during cutting.
a. high-speed burs; piezo tips b. piezo tips; high-speed burs
c. trephine burs; the counter-ratchet technique d. none of the above
17. Cooling of a piezo tip can be obtained by __________.
a. the use of copious irrigation with cold saline b. intermittent cutting
c. first freezing the piezo tips d. a and b
18. If using high-speed burs during removal of a failed implant, the burs of choice are __________ burs.
a. pear-shaped, thin b. tapered, end-cutting c. thin, tapered diamond burs d. all of the above
19. An air embolism can occur if air from the high-speed hand-piece __________.
a. escapes
b. is forced into a surgical wound c. is not immediately suctioned off d. all of the above
20. The smallest effective-size trephine should be selected to avoid collateral damage to __________.
a. neighboring bone b. teeth
c. implants d. all of the above
21. The preferred speed when using a trephine is __________ with copious irrigation.
a. 1,000 rpm to 1,200 rpm b. 1,200 rpm to 1,500 rpm c. 1,500 rpm to 1,800 rpm d. none of the above
22. The use of trephine burs is one of the __________ options for implant removal.
a. safest b. least invasive c. most invasive d. none of the above
23. Osteomyelitis is a complication that may occur following explantation with a trephine bur if bone is __________.
a. over-irrigated b. overheated c. undertreated
24. For those implants with expanded platforms, the implant platform should be __________ in order to use the smallest diameter of trephine burs possible.
a. extended
b. trimmed or resected c. protected
d. none of the above
25. When using high-speed burs, the residual apical part of the implant should be approached carefully when in proximity to __________, in order to prevent damage to these.
a. vital structures b. implants c. bone
d. all of the above
26. Use of the reverse screw technique is contraindicated for __________.
a. screw-type implants b. coated implants
c. non-screw-type implants with undercuts d. all of the above
27. Before ultra-high-frequency monopolar electrosurgery can be recommended for implant removal, __________ is necessary.
a. knowing the human threshold
b. reliable methods of regulating the heat to implants c. study on the possible complications including bone
necrosis d. all of the above
28. When the counter-ratchet technique is used with internal connection implants, at the connection level, the connection should not demonstrate any sign of a __________ that could result in further fracture of the implant.
a. crack b. rupture c. fracture d. all of the above
29. The use of the reverse-screw technique may require the application of _________ to remove an implant.
a. 100 Ncm to 200 Ncm b. 200 Ncm to 400 Ncm c. 300 Ncm to 600 Ncm d. none of the above
30. The results of the study reported in this article demonstrated a __________ retrieval rate using less invasive techniques.
a. 40% b. 50% c. 60%
CE QUIZ
*Address: NPI No.
*City: *State: *Zip: AGD Identification No.
*E-mail:
*Telephone: License Renewal Date:
Please direct all questions pertaining to Dental Learning, LLC or the administration of this course to [email protected]. COURSE EVALUATION and PARTICIPANT FEEDBACK: We encourage participant feedback pertaining to all courses. Please be sure to complete the evaluation included with the course. INSTRUCTIONS: All questions have only one answer. Participants will receive confirmation of passing by receipt of a verification certificate. Verification certificates will be processed within two weeks after submitting a completed examination. EDUCATIONAL DISCLAIMER: The content in this course is derived from current information and research based evidence. Any opinions of efficacy or perceived value of any products mentioned in this course and expressed herein are those of the author(s) of the course and do not necessarily reflect those of Dental Learning. Completing a single continuing education course does not provide enough information to make the participant an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise. COURSE CREDITS/COST: All participants scoring at least 70% on the examination will receive a CE verification certificate. Dental Learning, LLC is an ADA CERP recognized provider. Dental Learning, LLC is also designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing education programs of this program provider are accepted by AGD for Fellowship, Mastership, and membership maintenance credit. Please contact Dental Learning, LLC for current terms of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. Dental Learning, LLC is a California Provider. The California
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
QUIZ ANSWERS
Fill in the circle of the appropriate answer that corresponds to the question on previous pages.
EDUCATIONAL OBJECTIVES
1. List etiologies of failed implants;
2. Describe the counter-ratchet and reverse screw techniques that can be utilized for minimally invasive implant removal;
3. Review the indications and use of piezo tips and high-speed burs for implant removal; 4. Review the use of trephine burs for implant removal and the technique that should be used; and 5. List and describe the considerations and limitations in selecting an implant removal technique.
If you have any questions, please email Dental Learning at [email protected] or call 888-724-5230.
COURSE SUBMISSION:
1. Read the entire course.
2. Complete this entire answer sheet in either pen or pencil.
3. Mark only one answer for each question. 4. Mail answer form or fax to 732-303-0555.
For immediate results:
1. Read the entire course.
2. Go to www.dentallearning.net/MIT-ce. 3. Log in to your account or register to create an
account.
4. Complete course and submit for grading to receive your CE verification certificate.
A score of 70% will earn your credits.
Dental Learning, LLC
500 Craig Road, First Floor Manalapan, NJ 07726
*If paying by credit card, please note: MasterCard | Visa | AmEx | Discover *Account Number
______________________________________________ *Expiration Date
______________________________________________ The charge will appear as Dental Learning, LLC.
If paying by check, make check payable to
Dental Learning, LLC.
ALL FIELDS MARKED WITH AN ASTERISK (*) ARE REQUIRED
AGD Code: 690
Price: $29 CE Credits: 2
Save time and the environment by taking this course online.
COURSE EVALUATION
Please evaluate this course using a scale of 3 to 1, where 3 is excellent and 1 is poor. 1. Clarity of objectives . . . 3 2 1
2. Usefulness of content . . . 3 2 1 3. Benefit to your clinical practice . . . 3 2 1 4. Usefulness of the references . . . 3 2 1 5. Quality of written presentation . . . 3 2 1 6. Quality of illustrations . . . 3 2 1 7. Clarity of quiz questions . . . 3 2 1 8. Relevance of quiz questions . . . 3 2 1 9. Rate your overall satisfaction with this course . . . 3 2 1 10. Did this lesson achieve its educational objectives? Yes No 11. Are there any other topics you would like to see presented
in the future? __________________________________________________________________________ _______________________________________________________________________________________ 1. A B C D 2. A B C D 3. A B C D 4. A B C D 5. A B C D 6. A B C D 7. A B C D 8. A B C D 9. A B C D 10. A B C D 11. A B C D 12. A B C D 13. A B C D 14. A B C D 15. A B C D 16. A B C D 17. A B C D 18. A B C D 19. A B C D 20. A B C D 21. A B C D 22. A B C D 23. A B C D 24. A B C D 25. A B C D 26. A B C D 27. A B C D 28. A B C D 29. A B C D 30. A B C D