_____________________________________________________________________________________________________
*Corresponding author: E-mail: [email protected];
(Past name: British Journal of Medicine and Medical Research, Past ISSN: 2231-0614, NLM ID: 101570965)
Hemodynamic Responses and the Sustainability of
Force during Submaximal Isometric Handgrip
Exercise: Are There Sex Differences?
Konstantina Dipla
1*1
Exercise Physiology and Biochemistry Laboratory, TEFAA at Serres, Aristotle University of Thessaloniki, Agios Ioannis, Serres 62110, Greece.
Author’s contribution
The sole author designed, analyzed and interpreted and prepared the manuscript.
Article Information
DOI: 10.9734/JAMMR/2017/35357 Editor(s): (1)Teodoro Cordova Fraga, University in Guanajuato, Mexico. Reviewers: (1) Naro Ohashi, Hamamatsu University School of Medicine, Japan. (2)Vagner Raso, University of Sao Paulo, Brazil. (3)Ayfer Pazarbasi, Çukurova University, Turkey. Complete Peer review History:http://www.sciencedomain.org/review-history/20702
Received 9th July 2017 Accepted 24th August 2017 Published 28th August 2017
ABSTRACT
Background: Sex related differences in the control of blood pressure at resting conditions have been previously reported. Studies in rodents have also shown that during exercise, female animals have an enhanced capacity to inhibit sympathetic vasoconstriction than male animals.
Aims: To examine whether sex differences exist in (i) systolic/diastolic blood pressure (SBP/DBP) and systemic vascular resistance (SVR) responses during handgrip exercise, (ii) the ability to sustain a predetermined target force during isometric handgrip, in young, healthy, lean adults. Study Design / Methodology: Fourty-six adults (19 men and 27 women), aged 20-27 years, underwent a protocol that included a seated rest (baseline), a 3-min handgrip at 30% of maximal voluntary contraction (MVC), and recovery. Continuous, beat-to-beat SBP/DBP and heart rate were recorded (Finapres). Handgrip force was monitored (Biopac).
Results: Men had higher MVC than women (P < 0.001), however, both sexes exhibited similar handgrip steadiness. Men rated the exercise session as fatiguing as their female counterparts. During baseline, no differences were found between groups in SBP, DBP, and heart rate; however, during exercise and recovery, men exhibited a higher DBP response than females (P < 0.05). SVR
Dipla; JAMMR, 23(7): 1-11, 2017; Article no.JAMMR.35357
remained relatively stable during handgrip in men, whereas, a decline in SVR during exercise and recovery was observed in women (P < 0.05).
Conclusion: Differential hemodynamic responses during isometric exercise and recovery were revealed between young, healthy, and lean men and women. However, the steadiness and ability to sustain force during isometric exercise were not significantly different between men and women.
Keywords: Gender differences; isometric exercise; blood pressure; hemodynamics; total peripheral resistance; females; force; stability.
1. INTRODUCTION
Sex related differences in the control of blood pressure at resting conditions have been previously reported [1-3]. For most of human life (i.e. up to the fifth decade of life), women have lower resting blood pressure and experience orthostatic hypotension more often than men of similar age [2,4]. In addition, young women show a lower incidence of hypertension than young men [3,5]. Previous studies have also reported that at resting conditions young females exhibit a blunted forearm vasoconstrictor response to adrenergic stimulation, induced by norepinephrine (NE) injection [6,7]. Moreover, estrogen has been shown to increase nitric oxide (NO) synthase expression and NO bioavailability, inducing vasodilatory effects at resting conditions [8-11]. Since women have a greater relative abundance of estrogen compared to men, it seems plausible to suggest that females may have an enhanced potential to inhibit vasoconstriction not only at rest, but also during exercise. In accordance with this view, recent studies in rodents have shown that during exercise, female animals have an enhanced capacity to inhibit sympathetic vasoconstriction (i.e. they exhibit a greater functional sympatholysis) [12].
Exercise training has been widely recommended in the prevention of high blood pressure (BP). Although aerobic exercise has been the traditionally used mode of exercise for hypertension, recent studies suggested that isometric resistance training can also be effectively used to lower resting BP [13-16]. A limited number of studies have investigated whether there are sex-related differences in the hemodynamic control of blood pressure during resistance exercise, and even fewer during isometric handgrip exercise [17]. Furthermore, during isometric handgrip exercise, the contracting muscles exert a sustained mechanical compression on the blood vessels. This causes a transient restriction of inflow in the exercising muscles, and possibly contributes to
the marked increases in blood pressure (BP) observed during this mode of exercise. As men exhibit a greater handgrip force in absolute terms than women, and possibly a greater mechanical compression of their vessels during sustained contractions, it was hypothesized that men will exert a greater restriction of blood flow during exercise. In turn, this inflow restriction could induce not only greater hemodynamic responses, but could also a limit the ability to maintain steady force, resulting in earlier signs of fatigue during a submaximal handgrip test compared to women. Therefore, the purpose of this study was to examine if sex differences exist in (i) the systolic/diastolic BP and the systemic vascular resistance (SVR) responses during handgrip exercise, (ii) the ability to sustain a predetermined target force during isometric handgrip in young, healthy, and lean adults. It has been hypothesized that women will possibly exert a differential hemodynamic control during exercise, exhibiting a blunted change in SVR than men. It has also been hypothesized that women will be able to sustain a greater percentage of their target force, with greater stability than men. For these purposes, beat-by-beat hemodynamic responses at rest, during handgrip exercise, and recovery were assessed in young men and women. Force was continuously recorded during a sustained 3-min handgrip exercise. Examination of sex related differences in cardiovascular responses, stability, and perceived exertion during isometric handgrip exercise could allow for more optimized sex-based isometric exercise prescription, and thereby maximize the effectiveness of the isometric exercise training.
2. MATERIALS AND METHODS
2.1 Participants
index <25 kg/m2, and were recreationally active. The study was conducted in accordance with the Declaration of Helsinki and approved by department’s review board committee. Before the study, all participants were informed about the aims and study procedures and gave their written informed consent. Participants were non-smokers, because acute and chronic smoking can alter exercise hemodynamics [18]. Participants were also instructed to avoid intense physical activity the previous day before testing. Participants were instructed not to consume coffee, tea and alcohol for 12 hours before testing. Women were tested in different phases of their menstrual cycle (so that an equal number of women were in the follicular and in the luteal phase), but not during menstruation.
2.2 Testing Procedures and
Instrumentation
Participants arrived in the laboratory in the morning hours. After obtaining a personal and family history, anthropometrical characteristics were assessed. The participant was then connected to the experimental apparatus for assessment of hemodynamics. More specifically, the participant was connected to the finger photoplethysmography apparatus (Finometer, Finapres Medical Systems, Amsterdam, The Netherlands) for continuous, beat-to-beat assessment of systolic and diastolic arterial pressure (SAP/DAP) and heart rate. The finger cuff of the Finapres apparatus was placed on the middle finger and the inflatable cuff was placed at the heart level on the non-dominant arm.
Following calibration (for approximately 12 min) and baseline (for 5 min) measurements with the participant in the seated position, the handgrip exercise protocol started. Initially, the participant’s maximal handgrip strength was assessed using a Biopac dynamometer (MP150, CA, USA). Each participant performed three maximal voluntary contractions (MVC) with the dominant hand, with the elbow flexed at 90°, and a 60-s rest between trials. The highest reading of the three trials was considered as the MVC. After that, a 3-min isometric handgrip exercise was performed, during which the participant was required to maintain his/her 30% MVC. Visual feedback on a monitor was provided to the participant and specific instructions were given, in order to maintain force as steady as possible. The participant was constantly instructed to avoid the Valsalva maneuver and keep non-participating muscles relaxed. A 5-min recovery followed. The participant’s rate of perceived
exertion was evaluated using the Borg scale (6-20).
Finapres and biopac data were stored on computers for offline analysis. Stroke volume was calculated non-invasively using the Modelflow method, an arterial pressure wave analysis which has been shown to be a reliable alternative to invasive thermodilution techniques [19,20]. Systemic vascular resistance was calculated as mean BP / cardiac output using the BeatScope software, version 1.a. The magnitude of change from baseline (delta) in systolic and diastolic blood pressure, during handgrip exercise, and recovery was also calculated (i.e. delta SAP handgrip: SAPexercise – SAPbaseline;
delta DAP: DAPexercise – DAPbaseline; delta SAP
recovery: SAPrecovery – SAPbaseline; delta DAP:
DAPrecovery – DAPbaseline. SVR data were
normalized for body surface area (BSA) and reported as systemic vascular resistance index (SVRI). Average force maintained and the standard deviation of force (i.e. stability) during handgrip was calculated by AcqKnowledge 3.9.1 software.
2.3 Statistical Analysis
Dipla; JAMMR, 23(7): 1-11, 2017; Article no.JAMMR.35357
hemodynamic variables and force (MVC, force maintained). A P < 0.05 was considered as statistically significant.
3. RESULTS AND DISCUSSION
3.1 Participants’ Characteristics
Nineteen normotensive young men, aged 21.8 ± 1.5 years and twenty seven young women 21.14 ± 1.99 years participated in the study. Men had higher body weight and body mass index (BMI) than females (body weight: 77.2±9.8 vs. 59.6±8.3 kg; BMI: 24.0±2.1 vs. 22.0 ± 2.6 kg/m2; P < 0.01).
3.2 Isometric Handgrip Strength and Stability
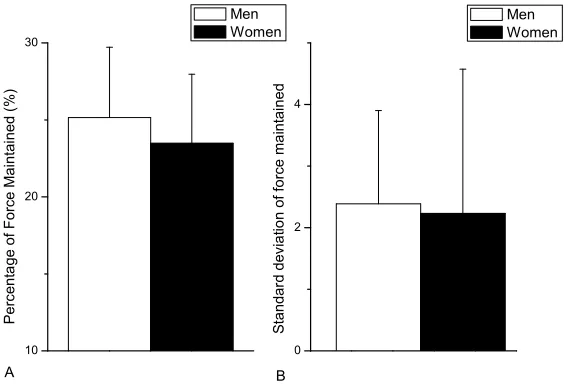
Men had higher MVC than women (54.9 ± 9.7 vs. 34.6 ± 7.5 kg, respectively; P < 0.001). The statistically significant difference in MVC between men and women persisted when MVC data were normalized for BMI (i.e. handgrip kg/body weight kg/m2; 2.3 ± 0.5 vs. 1.6 ± 0.3, P < 0.001). During the 3-min exercise, men maintained a higher absolute force than women (13.8 ± 3.1 vs. 8.2 ±2.6 kg, respectively; P < 0.001). However, men and women did not differ in the percentage of their MVC maintained during the 3-min handgrip (25.2 ± 4.6 and 23.5 ± 4.5%, in men and women, respectively; P = 0.21; Fig. 1A). Men and women exhibited a similar steadiness in their grip, in absolute terms (2.4 ±1.5 and 2.2 ± 2.3 kg, respectively; P = 0.9; Fig. 1B) and in relative
terms (i.e. normalized for MVC: 0.04 ± 0.02 and 0.06 ± 0.06, respectively; P = 0.13). Men rated the exercise session as fatiguing as their female counterparts (15.9 ± 2.0 and 15.3 ± 0.8, respectively; P = 0.42).
3.3 Hemodynamic Responses
3.3.1 Blood pressure and heart rate responses
Average data for SAP, DAP, and heart rate per testing period in the two groups, are presented in Fig. 2. During baseline, there were no significant differences between groups in SAP, DAP, and heart rate (SAP: 127.2 ±10.7 vs. 122.9 ± 9.3 mmHg; DAP: 79.0 ± 7.1 vs. 74.8 ± 5.8 mmHg; heart rate: 67.8 ±9.2 vs. 74.9 ± 10.2 bpm, respectively).
During isometric exercise, SAP and DAP significantly (P < 0.001) increased within each group (SAP: 161.5 ± 16.4 and 154.2 ± 12.3 mmHg, DAP: 102.3 ± 12.5 and 95.3 ± 6.7 mmHg, in men and women, respectively). Although during exercise there were no statistically significant differences between groups in SAP (P = 0.29), men exhibited significantly higher DAP values than women (P = 0.03). Heart rate significantly increased during exercise compared to baseline in both groups (96.9 ±17.9 vs. 103.4 ±14.5 bpm, males and females, respectively, P <0.001), without statistically significant differences between groups (P = 0.4).
Fig. 1. (A) Percentage of maximal voluntary contraction maintained during the 3-min handgrip and (B) Stability of force during the 3-min handgrip exercise (standard deviation of force
maintained) 10
20 30
B Men Women
Perc
ent
a
ge
of Force
Mai
ntai
ned
(%)
Men Women
A
0 2 4
S
tandar
d
dev
ia
tio
n of
force ma
intai
Fig. 2. Absolute values in (A) systolic blood pressure, (B) diastolic blood pressure, and (C) heart rate responses during rest, handgrip exercise, and recovery in men and women
*P < 0.05 vs. baseline, † P < 0.05 vs. men in the respective period
During recovery, SAP declined compared to the HG values (141.2 ± 11.7 and 131.3 ± 10.43 mmHg, in men and women respectively), but remained higher than baseline in both groups. SAP during this period has slightly higher in men than women; however, this difference was not statistically significant (P = 0.07). DAP also declined during recovery, in both groups, however, it remained higher than baseline in men. In contrast, DAP returned to baseline in women, with men exhibiting greater values than women (83.8±7.7 vs. 76.5±5.4 mmHg, respectively; P < 0.024) during this period. Heart rate was not different between men and women during recovery (69.1 ± 11.00 and 75.0 ± 9.7 beats per min).
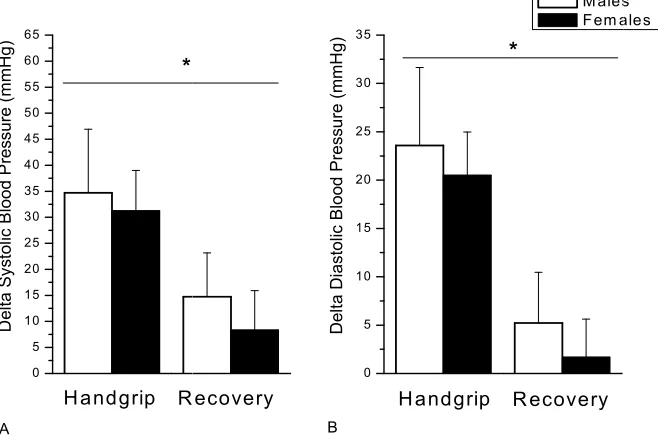
Next, the magnitude of increase in BP from baseline (delta-SAP and delta-DAP) during exercise and recovery, was calculated. A significant main effect of gender was been revealed in the magnitude of responses during exercise in BP (that is, main effect of gender in
delta-SAP p=0.039, partial η2 =0.09, medium effect size; main effect of gender in delta-DAP p=0.017, partial η2 =0.12, medium-large effect size) responses (Fig. 3).
3.3.2 Systemic vascular resistance responses
0.013). More specifically, in males, SVRI remained stable during the protocol (
0.132, 0.532 ± 0.186, and 0.535 ±
during baseline, exercise, and recovery, respectively; P = 0.98); however, in females SVRI decreased during exercise compared with baseline levels (P <0.001) and remained lower (P <0.01) than exercise during recovery (
Fig. 3. Magnitude of change from baseline (delta) in (A) systolic and (B) diastolic blood pressure, during handgrip exercise, and recovery in men and women
*P < 0.05 significant main effect of gender (i.e.
Fig. 4. Correlation of the magnitude of change from baseline (delta) in (A) systolic and (B) diastolic blood pressure during handgrip exercise with maximal voluntary contraction in men
and women (R = 0.13 and R = 0.16,
0 5 10 15 20 25 30 35 40 45 50 55 60 65
D
elta Sy
s
tol
ic B
lood P
res
sure
(
m
mHg)
*
H a nd grip R ecovery
A
Dipla; JAMMR, 23(7): 1-11, 2017; Article no.
0.013). More specifically, in males, SVRI remained stable during the protocol (0.545 ± ± 0.134 MU/m2, during baseline, exercise, and recovery, respectively; P = 0.98); however, in females SVRI decreased during exercise compared with baseline levels (P <0.001) and remained lower (P <0.01) than exercise during recovery (0.719 ±
0.229, vs. 0.628 ± 0.193, 0.651 MU/kg/m2, during baseline, exer
recovery, respectively). Furthermore, the magnitude of change from baseline in SVRI during exercise was significantly greater in men than women (0.014 ± 0.10 vs. 0.091 ± 0.10 MU/kg/m2; main effect of gender in delta p=0.05, partial η2 = 0.09, medium effect size).
Fig. 3. Magnitude of change from baseline (delta) in (A) systolic and (B) diastolic blood pressure, during handgrip exercise, and recovery in men and women
*P < 0.05 significant main effect of gender (i.e. men vs. women)
A
Fig. 4. Correlation of the magnitude of change from baseline (delta) in (A) systolic and (B) diastolic blood pressure during handgrip exercise with maximal voluntary contraction in men
and women (R = 0.13 and R = 0.16, respectively; P > 0.05) R ecovery
0 5 10 15 20 25 30 35
M ales F em ales
Delt
a Di
astolic
B
loo
d
Pre
s
s
u
re (mmH
g)
H a nd grip R ecovery
*
B
; Article no.JAMMR.35357
0.229, vs. 0.628 ± 0.193, 0.651 ± 0.186 during baseline, exercise, and recovery, respectively). Furthermore, the magnitude of change from baseline in SVRI during exercise was significantly greater in men than women (0.014 ± 0.10 vs. 0.091 ± 0.10 ; main effect of gender in delta-SVRI: 9, medium effect size).
Fig. 3. Magnitude of change from baseline (delta) in (A) systolic and (B) diastolic blood pressure, during handgrip exercise, and recovery in men and women
B
Fig. 4. Correlation of the magnitude of change from baseline (delta) in (A) systolic and (B) diastolic blood pressure during handgrip exercise with maximal voluntary contraction in men
No significant correlation was observed between the magnitude of increase in BP during exercise (delta-SAP and delta-DAP) with MVC or with the force maintained during handgrip (delta-SAP with MVC: R = 0.13, P = 0.39 and delta-DAP with MVC: R = 0.16, P = 0.29; delta-SAP with force
maintained: R = 0.09, P = 0.53 and R = 0.15, P = 0.30; Fig. 4). In addition, the magnitude of
change in SVRI during exercise, was not significantly correlated with MVC (R = 0.052, P = 0.74) and with the force maintained during handgrip (R = 0.06, P = 0.7).
3.4 Discussion
The results of this study showed that women exhibited lower DAP response during isometric exercise at 30% MVC and a faster recovery to baseline levels compared with men. In addition, a differential response in SVR between sexes was observed, with women exhibiting a reduction in SVR during exercise and recovery, whereas, SVR remained unaltered in men throughout the protocol. Although during handgrip exercise men exerted a greater force in their forearm muscles in absolute terms than women, no differences in the steadiness of handgrip and in the rate of perceived exertion were found between groups.
In this study, all participants were normotensive and no baseline differences in BP and heart rate were observed between groups. The slightly higher, non-statistically significant differences in SVR observed in women, are in accordance with previous studies [2]. Only lean individuals were recruited for this study, as obesity can alter the hemodynamic/neural responses to exercise, even in young individuals [21-23]. Testing in women was performed in different phases in their menstrual cycle with an equal number of women being in follicular and in luteal phase, so that the results of the study apply in women in both phases of the menstrual cycle. Women were not tested during the menstrual phase, so that hemodynamic responses are not influenced by differences in fluid loss or dehydration among the participants.
The isometric handgrip exercise used in this study, is a physiological excitatory stimulus of the sympathetic nervous system. During handgrip, the control of circulation depends on the interaction of neural stimuli i.e. signals from higher brain centers (originating in the brain’s
motor cortex, termed as central command) and peripheral afferents (baroreceptors,
mechanoreceptors, and metaboreceptors), as
well as, local vasodilatory factors released during exercise (such as NO and ATP) [24-32]. The interplay of these stimuli regulates cardiac output and peripheral resistance and results in an effective elevation of blood pressure, in an attempt to supply the working muscles with the required oxygen [33]. The selection of the exercise intensity in this study, was based on previous results, showing that exercise at 30% MVC activates both the mechanoreflex and the metaboreflex components of the exercise pressor reflex and allows force to be maintained for about 3 min [18,34-36]. This exercise intensity (30% MVC) has also been used in studies using isometric handgrip as the mode of chronic training [37]. All participants in the present study were able to complete the 3-min protocol, with no differences in the rating of perceived exertion observed between groups.
Dipla; JAMMR, 23(7): 1-11, 2017; Article no.JAMMR.35357
showed a greater reduction in resting DAP than men [41].
The differential response in SVR during isometric exercise between men and women possibly suggests a greater functional sympatholysis in women. Functional sympatholysis, defined as the diminished vasoconstriction to increased sympathetic activity that occurs in the working muscles during exercise, has been previously attributed to at least two possible mechanisms [31,42]. The first proposed mechanism is that NO synthase is activated in the contracting muscle and releases NO, which in turn acts on vascular smooth muscle or endothelial cells to oppose the activation of α1- and α2-adrenergic receptors by NE, attenuating vasoconstriction; while the second mechanism involves ATP, released from both muscle and deoxygenated hemoglobin that activates the purinergic receptors, acting again on vascular smooth muscle or endothelial cells and attenuates vasoconstriction [32,43-45]. In a recent study in rats, an enhanced functional sympatholysis was observed in female compared to male rats mediated by an NO dependent mechanism. However, the exact mechanism in humans requires further research.
In line with the present findings showing that a differential response of blood vessels (i.e. a reduction in SVR) during isometric exercise in females and not in males, a previous study by Collier showed that following chronic resistance training, women did not experience the increase in arterial stiffness (assessed using pulse wave velocity) that was observed in men [41]. Thus, our findings point to different integrated physiological mechanisms to maintain a normal BP during exercise between healthy, young, lean men and women. A limitation of this study is that individual blood estrogens and progesterone levels were not measured; thus, it can only be speculated that estrogen-mediated effects on the vasculature play a role in the present findings. Future studies should be conducted to examine the association of estrogen levels to the SVR responses during exercise. Another limitation of this study is that SVR responses were calculated from the beat-by-beat Finapres recordings and not directly measured with a catheter. The Finapres photophlethysmographic technique however, has the merit of being non-invasive, and has been proven to be valid both at rest and during exercise [46,47]. Finally, men exhibited greater force during handgrip than women. Thus, the greater force maintained could be partially
contributed to the greater increase in exercise DAP. However, the magnitude of increase in BP and in SVR in this study, were not significantly correlated with MVC nor with the force maintained during handgrip. In addition, differences in force exerted between men than women, were evident even when differences in body size are taken into account (i.e. when force was normalized for body size). Therefore, this greater force is an intrinsic characteristic of men. Choosing men and women with similar force to investigate gender differences in force stability could have assisted to isolate a gender effect, however, the selection of the participants in the two groups would not have been representative of the two populations.
In contrast to our hypothesis that men will show a greater variability in their force production (due to their greater, in absolute terms, compressive mechanical forces, limiting muscle hyperemia in the exercising forearm) compared to women, no differences in force stability were observed between groups. It has been previously shown in vitro studies and in healthy men that the mechanical stress to erythrocytes and endothelial cells may stimulate ATP release [48]. Whether blood and/or endothelial cells or enhanced local deoxygenation in men increase more intravascular ATP release during exercise, permitting local blood perfusion to the same level as in women, requires further investigation [49]. Furthermore, other mechanisms such as motor cortex activation, cerebral oxygenation, and central command that are involved in the ability to sustain handgrip force also require further study. In addition, since in this study participants were young, healthy, and lean adults, future studies should examine whether these findings apply to individuals with hypertension and other chronic disease.
4. CONCLUSION
CONSENT
A written informed consent was obtained from each participant.
ETHICAL APPROVAL
All experiments have been examined and approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
COMPETING INTERESTS
Author has declared that no competing interests exist.
REFERENCES
1. Joyner MJ, Wallin BG, Charkoudian N. Sex differences and blood pressure regulation in humans. Experimental Physiology. 2016;101:349-55.
2. Hart EC, Charkoudian N, Wallin BG, Curry TB, Eisenach JH, Joyner MJ. Sex differences in sympathetic neural-hemodynamic balance: Implications for human blood pressure regulation. Hypertension (Dallas, Tex: 1979). 2009;53:571-6.
3. Hart EC, Charkoudian N, Wallin BG, Curry TB, Eisenach J, Joyner MJ. Sex and ageing differences in resting arterial pressure regulation: The role of the beta-adrenergic receptors. The Journal of Physiology. 2011;589:5285-97.
4. Fu Q, Arbab-Zadeh A, Perhonen MA, Zhang R, Zuckerman JH, Levine BD. Hemodynamics of orthostatic intolerance: Implications for gender differences. American Journal of Physiology Heart and Circulatory Physiology. 2004;286:H449-57. 5. Wiinberg N, Hoegholm A, Christensen HR, Bang LE, Mikkelsen KL, Nielsen PE, et al. 24-h ambulatory blood pressure in 352 normal Danish subjects, related to age and gender. American Journal of Hypertension. 1995;8:978-86.
6. Kneale BJ, Chowienczyk PJ, Brett SE, Coltart DJ, Ritter JM. Gender differences in sensitivity to adrenergic agonists of forearm resistance vasculature. Journal of the American College of Cardiology. 2000;36:1233-8.
7. Bowyer L, Brown MA, Jones M. Vascular reactivity in men and women of reproductive age. American Journal of Obstetrics and Gynecology. 2001;185:88-96.
8. Muller-Delp JM, Lubahn DB, Nichol KE, Philips BJ, Price EM, Curran EM, et al. Regulation of nitric oxide-dependent vasodilation in coronary arteries of estrogen receptor-alpha-deficient mice. American Journal of Physiology Heart and Circulatory Physiology. 2003;285:H2150-7. 9. Fredette NC, Meyer MR, Prossnitz ER. Role of GPER in estrogen-dependent nitric oxide formation and vasodilation. The Journal of Steroid Biochemistry and Molecular Biology; 2017.
10. Nevzati E, Shafighi M, Bakhtian KD, Treiber H, Fandino J, Fathi AR. Estrogen induces nitric oxide production via nitric oxide synthase activation in endothelial cells. Acta Neurochirurgica Supplement. 2015;120:141-5.
11. Sobrino A, Vallejo S, Novella S, Lazaro-Franco M, Mompeon A, Bueno-Beti C, et al. Mas receptor is involved in the estrogen-receptor induced nitric oxide-dependent vasorelaxation. Biochemical Pharmacology. 2017;129:67-72.
12. Just TP, DeLorey DS. Sex differences in sympathetic vasoconstrictor responsive-ness and sympatholysis. Journal of Applied Physiology (Bethesda, Md: 1985). 2017;00139.
13. Cornelissen VA, Buys R, Smart NA. Endurance exercise beneficially affects ambulatory blood pressure: A systematic review and meta-analysis. Journal of Hypertension. 2013;31:639-48.
14. Cornelissen VA, Smart NA. Exercise training for blood pressure: A systematic review and meta-analysis. Journal of the American Heart Association. 2013;2: e004473.
15. Carlson DJ, Dieberg G, Hess NC, Millar PJ, Smart NA. Isometric exercise training for blood pressure management: A systematic review and meta-analysis. Mayo Clinic Proceedings. 2014;89:327-34. 16. Jin YZ, Yan S, Yuan WX. Effect of
isometric handgrip training on resting blood pressure in adults: A meta-analysis of randomized controlled trials. The Journal of Sports Medicine and Physical Fitness. 2017;57:154-60.
Dipla; JAMMR, 23(7): 1-11, 2017; Article no.JAMMR.35357
Sex differences in the modulation of vasomotor sympathetic outflow during static handgrip exercise in healthy young humans. American Journal of Physiology Regulatory, Integrative and Comparative Physiology. 2011;301:R193-200.
18. Anyfanti P, Triantafyllidou E, Papadopoulos S, Triantafyllou A, Nikolaidis MG, Kyparos A, et al. Smoking before isometric exercise amplifies myocardial stress and dysregulates baroreceptor sensitivity and cerebral oxygenation. Journal of the American Society of Hypertension: JASH. 2017;11:376-84. 19. Guelen I, Westerhof BE, Van Der Sar GL,
Van Montfrans GA, Kiemeneij F, Wesseling KH, et al. Finometer, finger pressure measurements with the possibility to reconstruct brachial pressure. Blood Pressure Monitoring. 2003;8:27-30. 20. Parati G, Casadei R, Groppelli A, Di
Rienzo M, Mancia G. Comparison of finger and intra-arterial blood pressure monitoring at rest and during laboratory testing. Hypertension (Dallas, Tex: 1979). 1989;13:647-55.
21. Dipla K, Zafeiridis A, Koidou I, Geladas N, Vrabas IS. Altered hemodynamic regulation and reflex control during exercise and recovery in obese boys. American Journal of Physiology Heart and Circulatory Physiology. 2010;299:H2090-6. 22. Milia R, Velluzzi F, Roberto S, Palazzolo G, Sanna I, Sainas G, et al. Differences in hemodynamic response to metaboreflex activation between obese patients with metabolic syndrome and healthy subjects with obese phenotype. American Journal of Physiology Heart and Circulatory Physiology. 2015;309:H779-89.
23. Negrao CE, Trombetta IC, Batalha LT, Ribeiro MM, Rondon MU, Tinucci T, et al. Muscle metaboreflex control is diminished in normotensive obese women. American Journal of Physiology Heart and Circulatory Physiology. 2001;281:H469-75. 24. Mitchell JH, Kaufman MP, Iwamoto GA. The exercise pressor reflex: Its cardio-vascular effects, afferent mechanisms, and central pathways. Annual Review of Physiology. 1983;45:229-42.
25. Fisher JP, Ogoh S, Young CN, Keller DM, Fadel PJ. Exercise intensity influences cardiac baroreflex function at the onset of isometric exercise in humans. Journal of Applied Physiology (Bethesda, Md: 1985). 2007;103:941-7.
26. Rowell LB, O'Leary DS. Reflex control of the circulation during exercise: Chemoreflexes and mechanoreflexes. Journal of Applied Physiology (Bethesda, Md: 1985). 1990;69:407-18.
27. Crisafulli A, Marongiu E, Ogoh S. Cardiovascular reflexes activity and their interaction during exercise. BioMed Research International. 2015;394183. 28. Jendzjowsky NG, Delorey DS. Short-term
exercise training enhances functional sympatholysis through a nitric oxide-dependent mechanism. The Journal of Physiology. 2013;591:1535-49.
29. Saltin B, Mortensen SP. Inefficient functional sympatholysis is an overlooked cause of malperfusion in contracting skeletal muscle. The Journal of Physiology. 2012;590:6269-75.
30. Thomas GD. Functional sympatholysis in hypertension. Autonomic Neuroscience: Basic & Clinical. 2015;188:64-8.
31. Mitchell JH. Abnormal cardiovascular response to exercise in hypertension: contribution of neural factors. American Journal of Physiology Regulatory, Integrative and Comparative Physiology. 2017;312:R851-R63.
32. Mortensen SP, Saltin B. Regulation of the skeletal muscle blood flow in humans. Experimental Physiology. 2014;99:1552-8. 33. Williamson JW, Fadel PJ, Mitchell JH. New
insights into central cardiovascular control during exercise in humans: A central command update. Experimental Physiology. 2006;91:51-8.
34. Dipla K, Papadopoulos S, Zafeiridis A, Kyparos A, Nikolaidis MG, Vrabas IS. Determinants of muscle metaboreflex and involvement of baroreflex in boys and young men. European Journal of Applied Physiology. 2013;113:827-38.
35. Dipla K, Triantafyllou A, Grigoriadou I, Kintiraki E, Triantafyllou GA, Poulios P, et al. Impairments in microvascular function and skeletal muscle oxygenation in women with gestational diabetes mellitus: Links to cardiovascular disease risk factors. Diabetologia. 2017;60:192-201.
36. Seals DR, Chase PB, Taylor JA. Autonomic mediation of the pressor responses to isometric exercise in humans. Journal of Applied Physiology (Bethesda, Md: 1985). 1988;64:2190-6. 37. Badrov MB, Freeman SR, Zokvic MA,
training lowers resting blood pressure and improves local brachial artery flow-mediated dilation equally in men and women. European Journal of Applied Physiology. 2016;116:1289-96.
38. Maruf FA, Ogochukwu UN, Dim PA, Alada AR. Absence of sex differences in systolic blood pressure and heart rate responses to exercise in healthy young adults. Nigerian Journal of Physiological Sciences: Official Publication of the Physiological Society of Nigeria. 2012;27:95-100.
39. Duchateau J, Hainaut K. Isometric or dynamic training: Differential effects on mechanical properties of a human muscle. Journal of Applied Physiology: Respiratory, Environmental and Exercise Physiology. 1984;56:296-301.
40. Crisafulli A, Marongiu E, Ogoh S. Cardiovascular reflexes activity and their interaction during exercise. BioMed Research International. 2015;1-10. ID: 394183
41. Collier SR. Sex differences in the effects of aerobic and anaerobic exercise on blood pressure and arterial stiffness. Gender Medicine. 2008;5:115-23.
42. Buckwalter JB, Taylor JC, Hamann JJ, Clifford PS. Role of nitric oxide in exercise sympatholysis. Journal of Applied Physiology (Bethesda, Md: 1985). 2004;97:417-23. Discussion 6.
43. Rosenmeier JB, Hansen J, Gonzalez-Alonso J. Circulating ATP-induced vasodilatation overrides sympathetic
vasoconstrictor activity in human skeletal muscle. The Journal of Physiology. 2004;558:351-65.
44. Mizuno M, Iwamoto GA, Vongpatanasin W, Mitchell JH, Smith SA. Exercise training improves functional sympatholysis in
spontaneously hypertensive rats through a nitric oxide-dependent mechanism.
American Journal of Physiology Heart and Circulatory Physiology. 2014;307:H242-51. 45. Buckwalter JB, Hamann JJ, Clifford PS. Vasoconstriction in active skeletal muscles: a potential role for P2X purinergic receptors? Journal of Applied Physiology (Bethesda, Md: 1985). 2003;95:953-9. 46. Wesseling KH. Finger arterial pressure
measurement with Finapres. Zeitschrift fur Kardiologie. 1996;85(Suppl 3):38-44. 47. Imholz BP, Wieling W, van Montfrans GA,
Wesseling KH. Fifteen years experience with finger arterial pressure monitoring: Assessment of the technology. Cardiovascular Research. 1998;38:605-16. 48. Crecelius AR, Kirby BS, Richards JC, Dinenno FA. Mechanical effects of muscle contraction increase intravascular ATP draining quiescent and active skeletal muscle in humans. Journal of Applied Physiology (Bethesda, Md: 1985). 2013;114:1085-93.
49. Kirby BS, Crecelius AR, Richards JC, Dinenno FA. Sources of intravascular ATP during exercise in humans: Critical role for skeletal muscle perfusion. Experimental Physiology. 2013;98:988-98.
_________________________________________________________________________________ © 2017 Dipla; This is an Open Access article distributed under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Peer-review history: