Effectiveness of the Informed Consent Process for a
Pediatric Resuscitation Trial
WHAT’S KNOWN ON THIS SUBJECT: Traditional informed consent is not possible for clinical trials that involve select emergency situations. Federal regulations permit research with an exception from informed consent. Children have been excluded from these studies in part because of their unique informed consent issues.
WHAT THIS STUDY ADDS: We describe an effective method of community consultation and public disclosure for an inpatient pediatric resuscitation trial with an exception from informed consent. These methods could be considered in future trial designs for this population involving emergency research.
abstract
OBJECTIVE:When prospective informed consent is not feasible, clini-cal research that presents more than minimal risk can proceed only with an exception from informed consent. Our objectives were (1) to describe the in-hospital community consultation and public disclosure process for a clinical trial and (2) to evaluate our in-hospital public disclosure process.
METHODS:Community consultation included parents, providers, and administrators in a PICU via focus groups, conferences, and other methods. Public disclosure consisted of a brochure and a poster in all PICU waiting rooms. These materials described risks and benefits of the trial, that no consent would be sought, how to “opt out,” and how to provide feedback. A verbal questionnaire was administered to parents of potential patients during the trial to evaluate the public disclosure process.
RESULTS:Eighty-one percent of 93 parents were aware of the ongoing trial. Seventy-six of 93 remembered seeing the brochure; of these, 26% did not read, 39% read quickly, and 35% read carefully. Thirty-seven of 93 parents remembered seeing the poster; of these, 51% did not read, 32% read quickly, and 17% read carefully. Sixty-seven percent reported that they would want to participate in the study, 9% would not, and 24% were undecided. Of the 7 parents who did not want to participate, 3 had opted out and 4 were unaware that they could opt out.
CONCLUSIONS:Parents endorsed resuscitation research with an ex-ception from informed consent. Public disclosure yielded⬎80% paren-tal awareness. Efforts should be made to ensure awareness of the ability to opt out.Pediatrics2010;125:e866–e875
AUTHORS:Tia Tortoriello Raymond, MD,aTimothy Glenn
Carroll, MD,bGlenda Sales, RN,cand Marilyn Cummings
Morris, MD, MPHd
aDepartment of Pediatrics, Division of Cardiac Critical Care,
Medical City Children’s Hospital, Dallas, Texas;bDepartment of
Pediatrics, Division of Critical Care, andcDivision of Clinical
Research, Children’s Medical Center, University of Texas Southwestern Medical Center, Dallas, Texas; anddChildren’s
Hospital of New York-Presbyterian, New York, New York
KEY WORDS
informed consent, vasopressin, children, pediatric research, cardiopulmonary resuscitation, clinical research/trials
ABBREVIATIONS
CPA— cardiopulmonary arrest EFIC— exception from informed consent FDA—Food and Drug Administration IRB—institutional review board AVP—arginine vasopressin
LAR—legally authorized representative
Reprints will not be ordered.
www.pediatrics.org/cgi/doi/10.1542/peds.2009-2427
doi:10.1542/peds.2009-2427
Accepted for publication Nov 5, 2009
Address correspondence to Tia Tortoriello Raymond, MD, 3501 Southwestern Blvd, Dallas, TX 75225. Email: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2010 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have no financial relationships relevant to this article to disclose.
Because of the emergent nature of car-diopulmonary arrest (CPA), clinical studies must be conducted either with a waiver of informed consent (applica-ble to minimal-risk research only) or with an exception from informed con-sent (EFIC) requirements for emer-gency research (21 CFR 50.24).1 The
Food and Drug Administration (FDA) and the Department of Health and Hu-man Services published guidelines in 1996 allowing resuscitation research to proceed with an EFIC with the follow-ing stipulations: (1) participants are in a life-threatening situation in which available treatments are unproved or unsatisfactory; (2) obtaining informed consent in advance is not feasible; (3) there is potential for direct benefit to the participant; and (4) the research could not be practically conducted without a waiver. In addition, there must be a process of community con-sultation and public disclosure and the subsequent approval of the involved institutional review board (IRB) and the FDA or Department of Health and Human Services (Appendix). No pediat-ric studies conducted with an EFIC have yet been published.
We designed and conducted a pros-pective pilot trial of combination epinephrine-vasopressin for pediatric in-hospital CPA that was refractory to initial epinephrine dosing with an EFIC granted by the FDA. In this report, we (1) describe the in-hospital community consultation and public disclosure process for this trial and (2) evaluate the effectiveness of the in-hospital public disclosure process via a survey of potential patients’ parents in the PICU during the resuscitation trial.
METHODS
Pilot Trial and Randomized, Controlled Trial
In early 2007, a protocol for a prospec-tive pilot trial and subsequent random-ized, controlled pivotal trial by using
arginine vasopressin (AVP) for refrac-tory in-hospital pediatric CPA was de-signed. The pilot trial would be a prospective, nonrandomized, open-labeled study conducted in the PICU at Children’s Medical Center, a tertia-ry care, university-affiliated hospital (University of Texas Southwestern Medical Center). All patients who were admitted to the PICU, were younger than 18 years, and experienced a CPA that required chest compressions and/or defibrillation and at least 2 doses of intravenous or intraosseous vasopressor medications were eligible for inclusion. Pilot group patients would receive epinephrine (0.01 mg/ kg) as the first vasopressor, followed by AVP (0.8 U/kg) as the second vaso-pressor. When required, all subse-quent doses of vasopressor would be epinephrine. The pilot study would en-roll 10 patients; if no problems were encountered, then the pivotal trial would begin. For the subsequent piv-otal trial, patients would be randomly assigned to AVP as already described or standard American Heart Associa-tion pediatric advanced life support with epinephrine only.
Permission to conduct the study under EFIC requirements for emergency re-search and an investigational new drug application were requested from the FDA on May 30, 2007. In July 2007, the investigational new drug applica-tion (#77995) was granted, but the trial was placed on “clinical hold” pending evidence that the trial could not proceed with prospective informed consent. Previous analysis of arrest events in this institution’s PICUs dem-onstrated an overall arrest rate of 3.5% and no prospective indicators that would identify certain patients at higher risk for CPA. To consent pro-spectively enough patients to satisfy the calculated sample size for the study, we would have to consent
⬎4000 patients. Ultimately, the FDA
granted permission to proceed under EFIC requirements for emergency re-search on November 28, 2007. The pro-tocol was submitted to the IRB and ap-proved ⬃5 months after the initial submission.
Community Consultation and Public Disclosure Process
Community consultation was con-ducted during an 18-month period from November 2006 to May 2008; pub-lic disclosure began during that time and continued throughout the pilot trial (Tables 1 and 2). Nine focus groups were conducted, drawn from the community from which partici-pants would be drawn and within which the research would be conduct-ed.1,2These groups consisted of
ents of critically ill children and par-ents of children who were previously admitted to the PICU and their health care providers and hospital adminis-trators. A study team member led all
TABLE 1 Specific Methods Used to Notify and Consult With the Community of Health Care Providers
Six focus groups conducted with health care professionals. (physicians, PICU nurses, PICU pharmacists, administrators)
Letter via mail to attending physicians describing the proposed study with EFIC and clearly indicating the opportunity to provide comments and opt out their patients E-mail sent to all staff attending physicians
describing the proposed investigation with EFIC and clearly indicating the opportunity to provide comments and opt out their patients E-mail sent to all PICU staff describing the
proposed investigation with EFIC and clearly indicating the opportunity to provide comments
Oral presentations of the proposed study with an EFIC to health care professionals with opportunity for discussion and clearly indicating the opportunity to provide comments
Notices posted in areas of the PICU of high health care provider traffic, clearly indicating the opportunity to provide comments
Web site describing the proposed study with EFIC and clearly indicating the opportunity to provide comments
focus groups, and notes were kept and forwarded to the IRB.
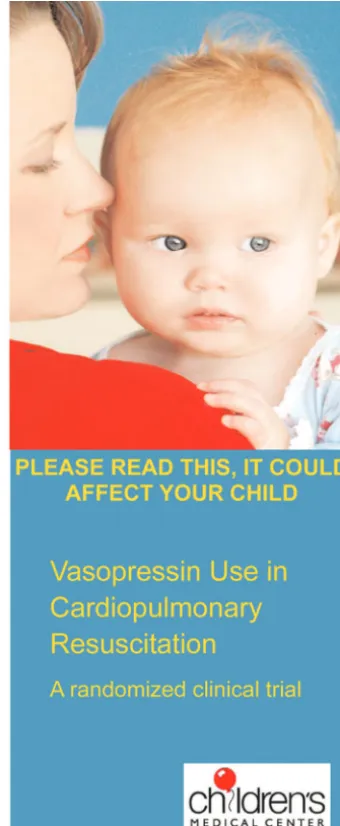
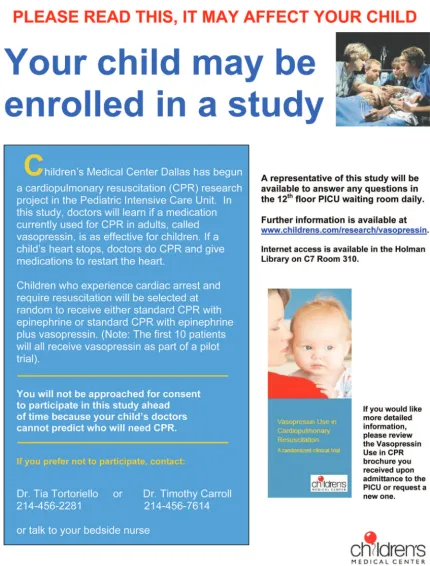
All parents of children who were ad-mitted to the PICU during the study pe-riod received a brochure with informa-tion detailing the study with emphasis on the opportunity to “opt out” (Fig 1). Posters describing the study and the ability to opt out were also placed in the PICU waiting rooms (Fig 2). Study personnel were available 24 hours a day to address questions or concerns and attempted to meet with the par-ents of all new admissions. In addi-tion, a Web site (www.childrens.com/ HealthcareProfessionals/Vasopressin. cfm) with more information about the study was available, and an e-mail ad-dress and a telephone number were provided to allow feedback to the in-vestigators. All information provided was available in English and Spanish. When a parent decided to opt out of the study, a sign was placed on the pa-tient’s bed indicating that the patient was not to be included in the study.
Paper and electronic letters announc-ing the study were sent to all attendannounc-ing physicians on staff before initiation of
the study. The physicians were encour-aged to respond to the investigators with questions, concerns, or com-ments and were provided the opportu-nity to opt out their patients. Providers in the PICU (nurses, physicians, phar-macists, and respiratory therapists) were made aware of the study via e-mail, verbal communication, in-service sessions regarding the study protocol, announcements at staff meetings, posters in staff areas, and verbal communication. One hundred percent of PICU faculty endorsed the study and agreed to have their pa-tients enrolled.
When a patient was enrolled, parents or a legally authorized representative (LAR) was informed of inclusion within 24 hours in person or by telephone or letter if unavailable. Prospective, in-formed consent to continue participa-tion was requested for review of med-ical records and follow-up contact for surviving patients. No parents/LAR of pilot patients declined continued par-ticipation. After completion of the pilot study, public disclosure with a com-prehensive summary of the data was made available to the community via posters in the PICU waiting rooms.
Survey Study
Between November 13, 2008, and March 27, 2009, during active recruit-ment for the AVP pilot trial, a verbal questionnaire was administered to 93 parents of PICU patients to evaluate the public disclosure process. The par-ents were approached by 1 of 2 re-search investigators who visited PICU rooms in numeric order and asked parents whether they were willing to spend 15 minutes discussing an ongo-ing research study in the PICU. When 2 parents were present, 1 parent was asked to be the primary responder, al-though responses from the other par-ent were recorded. The verbal ques-tionnaire was given with the aid of a
translator when the parents were Spanish-speaking. The 20-item survey questionnaire was developed to as-certain respondents’ (1) sociodemo-graphic characteristics, (2) aware-ness of the ongoing resuscitation study being conducted, (3) knowledge and understanding of selected details about the study, (4) primary source(s) of information used, and (5) their awareness of the ability to opt out of participation. A target sample size of 93 parents was based on a population size of 3000 and an accuracy level of⫾10%.
A coding scheme to categorize com-ments according to relevant concepts and themes was developed on the ba-sis of the content analyba-sis of the com-ments and the prospectively designed research questions. Responses were independently categorized by 2 investi-gators (Drs Raymond and Morris), and any discrepancies were resolved to the satisfaction of both investigators. The survey study was considered ex-empt from review by the IRB.
RESULTS
A total of 93 parents completed the survey. Ten were unwilling to partici-pate, for a response rate of 90%. The questionnaire was given in English to 83 (89%) respondents and in Spanish to 10 (11%) respondents. Respondents were primarily mothers, white, and well-educated. Their children were primarily younger than 1 year, and most had been hospitalized for ⬍6 days (Table 3).
Eighty-one percent of parents were aware of the ongoing resuscitation trial, and 46% had been approached by a member of the research team to dis-cuss the study. The majority learned of the ongoing study via the brochure (51%), followed by verbal communica-tion with a PICU staff member or re-search team member (41%), posters (3%), brochure and poster (1%), and TABLE 2 Methods Used to Notify and Consult
With the Community From Which the Patients Will Be Drawn
Three focus groups with the parents of children who were admitted to the hospital and/or PICU
Posters describing the study with an EFIC posted in areas of high PICU parent traffic and clearly indicating the opportunity to provide comments and opt out Brochures describing the study with an EFIC
distributed to the parents of all children who were admitted to the PICU and clearly indicating the opportunity to provide comments and opt out
Web site describing the proposed study with EFIC and clearly indicating the opportunity to provide comments
E-mail address for parents to provide comments to study investigators Study personnel attempted to approach all
not sure (4%). Seventy-six (82%) of 93 parents remembered seeing the bro-chure; of these, 26% did not read it, 39% read it quickly, and 35% read it carefully. Thirty-seven (40%) of 93 par-ents remembered seeing the poster; of these, 51% did not read it, 32% read it quickly, and 17% read it carefully. Par-ents were then asked to rate on a scale of 1 to 5 (1⫽not at all, 5⫽very much) the extent to which the brochure and/or poster made them feel angry or afraid. Three (3%) of 93 parents re-ported that it made them feel more than a little angry (3–5 on the scale),
and 46 (49%) of 93 said that it made them feel more than a little afraid. Sixty (65%) of 93 parents were more than a little glad that the research was occurring. When asked whether they could relay their (general) under-standing of the research study, 64% re-sponded correctly, 30% rere-sponded in-correctly, and 6% were unsure what the study involved. When asked which children could be enrolled in the study, 51% responded correctly, 36% were unaware, and 13% responded incor-rectly. Ninety percent of respondents were aware that parents had a choice
of whether their child could be en-rolled, and 79% knew how to opt out.
Respondents were asked how to make the brochure and poster more notice-able and how to encourage people to read it more carefully. The majority of parents responded that no changes were needed. Those who did suggest changes primarily suggested qualita-tive changes such as color, font size, etc (Figs 3 and 4). Eighty-one percent (76 of 93) of the respondents believed that the use of the brochure and poster was an effective way to commu-FIGURE 1
nicate with parents about the re-search study, and 47% (44 of 93) volun-teered that a face-to-face discussion would improve communication with parents about the research study.
Sixty-seven percent (62 of 93) of par-ents reported that they would want to participate in the study, 9% would not, and 24% were undecided. Reasons given on why these 62 parents would want to participate included direct benefit to the child (53%), advance-ment of science (26%), trust in health care provider (7%), other (12%), and unsure (2%). Of the 7 parents who would decline participation, reasons
included avoiding experimental proce-dures (43%), not wanting focus averted from the primary issues (14%), other (29%), and unsure (14%). Three of the 7 parents had opted out their child, but 4 parents were un-aware that they could opt out.
During the public disclosure and community consultation process and through completion of the pilot trial, the vasopressin Web site was viewed 295 times with an average time on the site of 2 minutes and 22 seconds. No e-mails were received at the e-mail ad-dress provided for feedback. Two nurses in the PICU voiced concerns
during the community consultation process regarding EFIC. One nurse “felt it was wrong that we were taking advantage of people to get our study done,” and another “felt like we didn’t have valid reasons to not consent ev-ery patient.” Both nurses were encour-aged to ensure that parents were aware of the option to decline partici-pation and to assist parents with this process when indicated. Of 2720 chil-dren who were admitted to the PICU dur-ing the pilot trial, 61 (2.2%) were opted out: parents/LAR declined participation in 59 cases, and a consulting neurology staff physician opted out 2 patients. FIGURE 1
DISCUSSION
We found that parents of PICU patients endorse the conduct of inpatient re-suscitation research with an EFIC. Fur-thermore, we found that our model for
community consultation and public disclosure within the PICU community was effective and well-received.
According to FDA Guidance, the 3 pri-mary goals of the community
consulta-tion process are (1) to explain the na-ture of the research, with its attendant risks and benefits; (2) to state that in-formed consent will not be attained from individual patients before study FIGURE 2
participation; and (3) to explain the process by which potential patients can refuse to participate in research studies.3,4The FDA guidance report
de-fines public disclosure as “dissemina-tion of informa“dissemina-tion about the emer-gency research sufficient to allow a reasonable assumption that communi-ties are aware that the study will be conducted, and later, that the
commu-nities and scientific researchers are aware of the study results.”3,4The
reg-ulations do not explicitly state the amount or types of community consul-tation and public disclosure that need to be done to achieve compliance, and each IRB is left to exercise its own dis-cretion in determining appropriate community consultation activities and public disclosure.
There is a unique problem in the defi-nition of what constitutes a community for hospital-based studies, particu-larly those that do not target a group of patients with 1 specific disease. Fami-lies of children who experience an in-patient cardiac arrest come from a
multitude of ethnic, socioeconomic, and religious communities. The larg-est commonality among these families is the experience of having a criti-cally ill child in the hospital setting. Thus, we sought to complete a com-munity consultation and public dis-closure process for inpatient resus-citation research focusing on the hospital/PICU community rather than the geographic community. Previous reports of hypothetical pediatric in-hospital resuscitation studies re-ported unanimous parental support for this approach.5
In previous reports, both parents and health care providers believed FIGURE 3
How could we make the brochure/poster more noticeable?
FIGURE 4
How could we change this brochure/poster to make it more likely that people would read it carefully?
TABLE 3 Demographics of the Study Population (n⫽93)
Demographic n(%)
Respondent
Mother 74 (80)
Father 16 (17)
Other custodial adult 3 (3) Ethnicity
Caucasian/European non-Hispanic 31 (33)
African American 21 (23)
Hispanic 27 (29)
Asian/Indian/Pacific Islander 6 (7)
Other/mixed 5 (5)
Unspecified 3 (3)
Level of education
Elementary/middle school 4 (4)
High school 38 (41)
Associate’s degree or some college 24 (26)
Bachelor’s degree 16 (17)
Graduate or professional degree 11 (12) Religious affiliation
Catholic 21 (24)
Protestant 2 (2)
Jewish 1 (1)
Muslim 3 (3)
Other 42 (45)
None 19 (20)
No response 5 (5)
Elective admission 21 (23)
Child had history of cardiac arrest 19 (20) Child’s age
⬍6 mo 37 (39)
6–11 mo 11 (12)
1–4 y 20 (22)
5–12 y 14 (15)
13–18 y 11 (12)
Duration of child’s PICU stay up to the time of interview
1–6 d 56 (59)
7–14 d 20 (22)
15–28 d 11 (12)
29 d to 6 mo 6 (7)
⬎6 mo 0 (0)
Duration of child’s life spent admitted to a hospital
1–6 d 27 (29)
7–14 d 20 (21)
15–28 d 11 (12)
29 d to 6 mo 26 (28)
strongly that it is inappropriate to en-roll children in these types of trials without parental awareness. In focus groups, parents and health care pro-viders concluded that EFIC may be ac-ceptable if all families of potentially eligible patients are aware of the ongoing study and if parents are given an opportunity to decline participation before study enrollment.5 Of the
par-ents surveyed in this report, 7 stated that they would not want to participate in the study, but only 3 had previously opted out. Four (4%) parents were un-aware of their option to decline partic-ipation. It is important to point out, however, that these misperceptions that parents had are similar to clinical trials in which parents gave informed consent. Previous studies of parental consent for pediatric research vealed significant inadequacies in re-search participants’ level of under-standing about the research to which they had consented. Such inadequacies relate to the nature of the information, who gave the information and sought consent, participant demographics and personal factors, readability of the consent document, and situational stress.6–11Future research that uses an
EFIC should focus on ensuring that fami-lies know that they have the option to de-cline participation.
Our primary methods of public disclo-sure were a brochure given to parents at PICU admission, a poster in all PICU waiting rooms, and attempted verbal communication by a research team member with new PICU admissions. These methods proved to be effective: 81% of surveyed parents were aware of the ongoing resuscitation trial, and 46% had already been approached by a member of the research team before the survey. The majority of parents learned of the ongoing trial via the bro-chure or through verbal communica-tion, rather than via the posters. Of particular importance is the number
of parents who did not read the bro-chure (26%) and/or poster (51%) even though they had access to them. This is consistent with previous reports that parents may be too overwhelmed at the time of PICU admission to focus on a handout.5 Displaying posters may
help inform these parents about an on-going study, because the parents may see the poster themselves, or a visitor may alert them to the information. Other options include displaying the in-formation on patient televisions and putting up more posters, perhaps in restrooms, elevators, or hallways.
Conducting inpatient pediatric resus-citation research may result in sub-stantial fear and anxiety; almost half of the parents who participated said that they would feel more than a little bit afraid after reading the brochure and/or poster. Another feeling men-tioned by parents was the idea of being “singled out” to receive the brochure, feeling that meant that their child was at particular risk. Posters displayed throughout the PICU may decrease this feeling, because the parents would re-alize that the research is for everyone and not just their child. Almost one half of parents volunteered that the most effective way to improve communica-tion would be through a face-to-face method. Availability of researchers to discuss the study may decrease paren-tal fear and anxiety as well as increase participation. Future studies should fo-cus on enhancing verbal communica-tion about the study, with particular emphasis on the parents’ option to de-cline participation in the study at that time.
Current regulations for contact of fam-ily members/LARs state, “IRBs must en-sure there are procedures in place to provide information about the emer-gency research study, at the earliest feasible opportunity, to . . . the sub-ject’s legally authorized representa-tive . . . including notice that the
sub-ject may withdraw or discontinue participation in the study without pen-alty or loss of benefits to which the subject was otherwise entitled.”2 The
authors agree with these require-ments but suggest a modification that would permit the EFIC for emergency research to extend to review of the medical record to the time of hospital discharge to ascertain important out-comes such as survival to discharge and minimize bias. Vulnerable popula-tions, including those who are minori-ties or economically disadvantaged of-ten have poorer outcomes and are more likely to decline continued partic-ipation in the study after being given the study article.12,13 Furthermore,
families of patients with poor out-comes may be less likely to consent than families of patients with good out-comes. Such incomplete assessment of adverse effects in a trial exposes both study patients and society to un-due risk.
CONCLUSIONS
We describe an effective method of community consultation for an inpa-tient pediatric resuscitation trial with an EFIC and confirm that parents and providers endorse resuscitation re-search with an EFIC with a prospective opportunity to opt-out. The public dis-closure process described yielded a
⬎80% awareness of the eligible pa-tient population; however, particular efforts should be made to ensure awareness of the ability to decline participation.
ACKNOWLEDGMENTS
REFERENCES
1. Morris MC, Nadkarni VM, Ward FR, Nelson RM. Exception from informed consent for pediatric resuscitation research: commu-nity consultation for a trial of brain cooling after in-hospital cardiac arrest.Pediatrics.
2004;114(3):776 –781
2. Halperin H, Paradis N, Mosesso V Jr, et al. Recommendations for implementation of community consultation and public disclo-sure under the Food and Drug Administra-tion’s “exception from informed consent re-quirements for emergency research”: a special report from the American Heart As-sociation Emergency Cardiovascular Care Committee and Council on Cardiopulmo-nary, Perioperative and Critical Care— endorsed by the American College of Emer-gency Physicians and the Society for Academic Emergency Medicine.Circulation.
2007;116(16):1855–1863
3. Guidance for institutional review boards, clin-ical investigators, and sponsors: exception from informed consent requirements for emergency research— draft guidance.
Avail-able at: www.fda.gov/OHRMS/DOCKETS/98fr/ 06d-0331-gdl0001.pdf. Accessed November 1, 2006
4. Guidance for institutional review boards, clinical investigators, and sponsors: excep-tion from informed consent requirements for emergency research— draft guidance. Available at: www.fda.gov/oc/ohrt/irbs/ except.html. Accessed December 4, 2006
5. Morris MC, Fischbach RL, Nelson RM, Schleien CL. A paradigm for inpatient resus-citation research with an exception from informed consent.Crit Care Med. 2006; 34(10):2567–2575
6. Harth SC, Thong YH. Parental perceptions and attitudes about informed consent in clinical research involving children.Soc Sci Med.1995;41(12):1647–1651
7. McCollum AT, Schwartz AH. Pediatric re-search hospitalization: its meaning to par-ents.Pediatr Res.1969;3(3):199 –204 8. Mason SA, Allmark PJ. Obtaining informed
consent to neonatal randomised controlled trials: interviews with parents and
clini-cians in the Euricon study.Lancet.2000; 356(9247):2045–2051
9. Simon C, Zyzanski SJ, Eder M, Raiz P, Kodish ED, Siminoff LA. Groups potentially at risk for making poorly informed decisions about entry into clinical trials for childhood cancer.J Clin Oncol.2003;21(11):2173–2178 10. Snowdon C, Garcia J, Elbourne D. Making sense of randomization: responses of par-ents of critically ill babies to random alloca-tion of treatment in a clinical trial.Soc Sci Med.1997;45(9):1337–1355
11. Hazen RA, Drotar D, Kodish E. The role of the consent document in informed consent for pediatric leukemia trials.Contemp Clin Tri-als.2007;28(4):401– 408
12. Clifton GL, Miller ER, Choi SC, et al. Lack of effect of induction of hypothermia after acute brain injury. N Engl J Med.2001; 344(8):556 –563
13. Clifton GL, Knudson P, McDonald M. Waiver of consent in studies of acute brain injury.
APPENDIX Summary of the EFIC Requirements for Emergency Research (21 CFR 50.24)
Justifications
1. The research involves a medical condition or situation in which a. Human subjects are in a life-threatening situation b. Available treatments are unproved or unsatisfactory
c. Evidence is necessary to determine the safety and effectiveness of particular interventions 2. Obtaining informed consent is not feasible because
a. The subject is not able to give consent owing to his or her medical condition
b. The intervention must be administered before it is feasible to obtain consent from a legal representative c. There is no reasonable way to identify eligible subjects prospectively
3. Participation holds the direct benefit to the subjects because a. Subjects face a life-threatening situation that requires intervention
b. Preliminary investigations, including animal studies, and related evidence suggest that this intervention may provide a direct benefit to the individual subject
c. The risks are reasonable
4. The clinical investigation could not practicably be performed without the waiver Obligations of the investigator
5. The proposed study protocol defines the length of the potential therapeutic window, and the investigator
a. Commits to attempt to contact and, if feasible, obtain consent from a legally authorized representative for each subject within that window of time; and b. If a legal representative is not available, commits to attempt to contact within that window some other family member and ask whether that family
member objects to the subject’s inclusion; and
c. Will summarize the efforts made to contact legal representatives and family members and makes this information available to the IRB at the time of continuing review.
6. Consultation with representatives of the communities in which the research will be conducted 7. Public disclosure to the communities where the research is conducted
a. Before initiation of the trial, with regard to study plans, risks, and benefits; b. After completion, disclosure of the results, and subject demographics
8. Perform the study under a separate IND or IDE from the FDA, even if an IND or IDE already exists Obligations of the IRB
9. The IRB has reviewed and approved procedures and documents for a. Use in situations when it is feasible to obtain informed consent
b. Use when it is feasible to provide an opportunity for a family member to object 10. The IRB is responsible for ensuring that procedures are in place to
a. Inform each subject or a legally authorized representative or family member (if the subject is incapacitated) of his or her inclusion in the study and details of the study
b. Inform each subject or representative that he or she may discontinue participation in the trial
c. Inform subjects who become competent after initial notification to representatives of incompetent subjects d. Inform a legally authorized representative or family member of subjects who die before notification about the trial
11. If an IRB determines that it cannot approve a proposed study because it does not meet the criteria for justifying the need for a waiver or for other ethical concerns, the IRB must provide these findings promptly to the investigator and sponsor in writing.
12. The IRB must retain the determinations and documentation required by the above regulations for 3 y after completion of the investigation. Obligation of the sponsor
13. Develop the protocol in collaboration with the appropriate investigators.
14. Establish an independent data monitoring committee to exercise oversight of the clinical investigation.
15. If an IRB denies approval of a protocol per item 11, then the sponsor of the investigation must promptly disclose this information to the FDA, the clinical investigators, and other IRBs that have been or are being asked to review the same or a substantially equivalent trial. The sponsor must track all information disclosed and ensure that disclosed information is placed on the FDA’s public docket.
DOI: 10.1542/peds.2009-2427 originally published online March 15, 2010;
2010;125;e866
Pediatrics
Cummings Morris
Tia Tortoriello Raymond, Timothy Glenn Carroll, Glenda Sales and Marilyn
Effectiveness of the Informed Consent Process for a Pediatric Resuscitation Trial
Services
Updated Information &
http://pediatrics.aappublications.org/content/125/4/e866
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/125/4/e866#BIBL
This article cites 11 articles, 3 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/cardiology_sub
Cardiology
ent_safety:public_education_sub
http://www.aappublications.org/cgi/collection/patient_education:pati
Patient Education/Patient Safety/Public Education
http://www.aappublications.org/cgi/collection/hospital_medicine_sub
Hospital Medicine
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2009-2427 originally published online March 15, 2010;
2010;125;e866
Pediatrics
Cummings Morris
http://pediatrics.aappublications.org/content/125/4/e866
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.