Paweł Domosławski
A–D, Tadeusz Łukieńczuk
E, F, Krzysztof Kaliszewski
E, F,
Krzysztof Sutkowski
E, F, Romualda Wojczys
E, F, Beata Wojtczak
E, FSafety and Current Achievements
in Thyroid Surgery with Neuromonitoring
Bezpieczeństwo i najnowsze osiągnięcia w chirurgii tarczycy
z użyciem neuromonitoringu
1st Department and Clinic of General, Gastroenterological and Endocrinological Surgery, Wroclaw Medical University, Poland
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation;
D – writing the article; E – critical revision of the article; F – final approval of article; G – other
Abstract
One of the most important complications during thyroid surgery is injury of the recurrent laryngeal nerve (RLN) which leads to dysfunction and palsy of the vocal folds. Adequate knowledge about the location of the RLN supported by neuromonitoring can help the operating surgeon to prevent this complication. Visualisation of the nerve alone seems to not be enough. Much more important is an estimation of the function of the RLN. One can say that nowadays we are in the passing era (transition period) of only visualisation of the recurrent laryngeal nerve during operation and entering the era of its neuromonitoring. Neuromonitoring gives us information about the location and function of the RLN. Using this equipment, thyroid surgery becomes safer not only for the patients but also for the operating surgeon in the way of the medicolegal consequences of surgical complications (Adv Clin Exp Med 2013, 22, 1, 125–130).
Key words: recurrent laryngeal nerve, neuromonitoring, thyroid surgery.
Streszczenie
Jednym z najpoważniejszych powikłań operacji gruczołu tarczowego są uszkodzenia nerwu krtaniowego wstecz-nego (NKW), prowadzące do porażeń fałdów głosowych. Chirurg, mając odpowiednią wiedzę o położeniu NKW, wspomaganą przez neuromonitoring, może zapobiec temu powikłaniu. Dotychczasowe metody wizualizacji nerwu krtaniowego wstecznego okazały się niewystarczające. Ważnym czynnikiem jest określenie funkcji nerwu podczas zabiegu chirurgicznego. Można więc przyjąć, że obecnie trwa okres przejściowy między erą tylko wizualizacji nerwu krtaniowego wstecznego podczas operacji a nadchodzącą erą jej neuromonitoringu. Neuromonitoring dostarcza informacji o położeniu i funkcji NKW. Chirurgia tarczycy z zastosowaniem sprzętu do neuromonitoringu jest bardziej bezpieczna nie tylko dla pacjenta, ale i dla operującego chirurga, biorąc pod uwagę pozabiegowe prawne następstwa powikłań (Adv Clin Exp Med 2013, 22, 1, 125–130).
Słowa kluczowe: nerw krtaniowy wsteczny, neuromonitoring, chirurgia tarczycy.
Adv Clin Exp Med 2013, 22, 1, 125–130 ISSN 1899–5276
REVIEWS
© Copyright by Wroclaw Medical University
Current standards of thyroid surgery require an extensive knowledge of the recurrent laryngeal nerve (RLN), anatomical course and routine vi-sual identification of the nerve [1]. The recurrent laryngeal nerve is the main motor nerve of all in-trinsic laryngeal muscles except for the cricothy-roid [2].
RLN injury, which was also reported by other au-thors [4–6].
However, the injury of the RLN can occur even in cases with no aberrant anatomy of the laryngeal nerve. This may be caused by thermal injury, com-pression, traction and vacuum pressure. It is also well known that in cases of huge retrosternal goi-ter, thyrotoxicosis, thyroiditis after radiotherapy and in cases of central lymph node clearance, it is difficult to identify this nerve. That was a reason to introduce a new technique apart from nerve visualization, which is called intraoperative neu-romonitoring (IONM).
Touching the nerve with a special electri-cal probe during thyroidectomy, the surgeon can evoke a stimulation of the nerve which affects vo-cal cord movements. Special detecting electrodes placed on the endotracheal tube can detect and convert muscle activity into acoustic and electro-myographical signals [7].
IONM has been suggested as a new method, before visual identification of the recurrent laryn-geal nerve, to prevent nerve palsy. And even in cases of nerve palsy, it is possible to elucidate the mechanism of the nerve injury [8].
Some studies have shown the benefits of IONM. Barczyński et al. showed that, using this method, transient paresis of the recurrent laryn-geal nerve is reduced by 2.9% in high-risk patients and 0.9% in low-risk patients [9]. Other authors say that neuromonitoring significantly decreases the rate of postoperative transient and permanent RLN palsy [10, 11].
Barczynski also suggests that neuromonitoring increases the accuracy of macroscopic identifica-tion in cases of bifurcated RLNs, which prevents neuropraxia of the anterior branch of bifurcated recurrent laryngeal nerve [12].
Higgins et al. [13], based on meta-analysis evaluating 64,699 at-risk nerves, demonstrated no statistically significant difference in the rate of true vocal fold palsy after using IONM versus only identification of the nerve during thyroidectomy. He also suggests that IONM should not be consid-ered as the standard of care and should not sup-plant anatomical identification of the RLN.
Chiang, based on IONM, revealed that the main reason of RLN injury during thyroidectomy is nerve traction, which results in its invisible dam-age [8, 14].
The nerve is prone to injury at the region of Berry’s ligament, so authors even changed the place for initial searching of the RLN, from the region of this ligament to the level of the thyroid artery.
Loss of function of the nerve may be estimated, even when the nerve is visually intact the injury is invisible, so it helps the surgeon in
decision-mak-ing whether to operate or not on the other side, to prevent casual bilateral nerve palsy.
Goretzki suggests that in cases, after one lobe dissection, when the nerve is visible but not func-tioning on one side, further surgery on the other lobe may be postponed in order not to risk bilat-eral vocal cord paralysis [15].
Documentation from neuromonitoring can help to estimate whether the surgeon or another reason caused the palsy of the recurrent nerve, which can be helpful in medicolegal litigation of surgeons.
The International Neural Monitoring Study Group, formed in 2006, has gained widespread ac-ceptance of neuromonitoring as an adjunct to the gold standard of visual nerve identification [2].
Neuromonitoring can locate the point where the loss of signal occurred with an identification of how and when the nerve was injured. These cre-ate an eventual possibility of repairing the nerve or removing the obstacle.
After accidental injury, a damaged nerve can be found using IONM, and a proper anastomosis could be performed by the surgeon.
Only IONM can identify the division of the RLN into the anterior motor branch and the pos-terior sensor branch. The sensor branch could be, depending on the circumstances, treated as a whole nerve, which can cause damage to the anterior mo-tor branch [2].
Standards
of Neuromonitoring
There are certain minimal elements for optimal IONM, which include the necessity of preoperative laryngoscopy (L1) to evaluate the functional status of the vocal cords. The next step is initial dissec-tion and stimuladissec-tion of vagal and laryngeal nerves (V1, R1). These elements allow for verification of the IONM system and subsequent neural mapping of the recurrent nerve before surgery. After dissec-tion of the thyroid gland, the surgeon can test post-operative glottis function, stimulating once again the laryngeal and vagal nerves (R2, V2). Postopera-tive laryngoscopy (L2) is necessary to evaluate the correlation between postoperative stimulation and essential glottic function. All these elements are shortly known as L1- V1- R1- R2- V2- L2.
Preparation for Surgery
consideration changes of the position of the tube during repositioning of the neck for surgery. The depth of insertion of the endotracheal tube has been researched in the Asian population. Women have a slightly smaller depth of insertion, 19.6 ± ± 1 cm, compared to men, 20.6 ± 0.97 cm [16].
The position of the tube could change during the repositioning of the patient. The tube can be displaced up to 21 mm inward and 33 mm out-ward, when the patient is repositioning from the neutral to full neck extension position [17].
The anesthesiologist’s protocol should include initial, short time relaxation agents for intubation, and then anesthesia should be carried out with no muscle relaxation, to achieve good response from the vocal cords.
A xylocaine lubrication agent shouldn’t be used for lubrication of the endotracheal tube as a way to decrease the potential local paralytic agent.
All substances known as neuromuscular block-ing agents should be avoided, because they can re-duce the amplitude of evoked responses.
Equipment
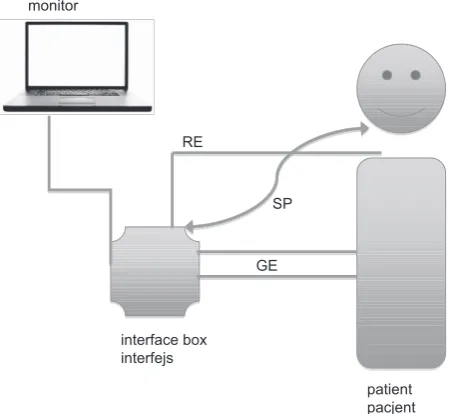
Modern monitoring systems can be divided into audio-only systems and systems which show visual and audio waveform information, includ-ing evoked waveforms. The second system gives us more information about the morphology, am-plitude, latency and threshold, which is very im-portant particularly in estimating and finding the place of injury of the RLN. The general scheme of neuromonitoring equipment is shown in Fig. 1.
Continuous vagal nerve stimulation is a system which uses special probes that stimulate the vagus during the time of thyroidectomy. This system can warn the surgeon before imminent nerve function impairment [18]. Continuous vagal nerve stimula-tion during thyroid surgery has a distinct impact on the autonomous nervous system balance, which can be reliably assessed through analysis of heart rate variability [19].
Recording electrodes are generally needle-based or endotracheal tube-needle-based. Needle- needle-based supports more information, but can provide more injury, like vocal cord laceration, hematoma, in-fection and deflation of the endotracheal balloon. They also record signals only on one side, which requires its repositioning during surgery. Endo-tracheal tube-based electrodes provide EMG data from the vocal cord.
Stainless steel electrodes should be placed on the endotracheal tube on a surface that is exposed at the glottis level. It is important that adhesive pad electrodes should stick firmly to the vocal cords,
so for each patient, the largest size of endotracheal tube should be used. This not only gives better contact with the vocal cords but also improves im-pedance.
Chiang uses 6 mm endotracheal tubes for women and 7 mm for men [8].
Most equipment-related problems are due to malposition of the endotracheal tube recording electrodes.
The position of the endotracheal tube should be checked a second time, when the patient is fully in position. This can be done by direct laryngos-copy or using a fiberoscope applied to the endo-tracheal tube. Another tube-position verification method is a “tap test”. Tapping the midline lar-ynx with a finger at a level of the thyroid cartilage can evoke a nerve-like response, a waveform seen on the monitor. The mechanism of this action is poorly understood [2].
During operation, the surgeon visually iden-tifies the vagus and recurrent laryngeal nerve and its neuromonitoring response. Adequate re-sponses from both of these nerves give informa-tion about good posiinforma-tioning of the endotracheal tube. In case of malposition of the tube, its repo-sitioning during surgery is much more difficult. Lu at al. showed that optimal tube placement was possible at first intubation in 94% of patients [16]. Stimulating electrodes could be bipolar or mo-nopolar and can be configured as a surgical tool. Bipolar is more sensitive, but monopolar is better
Fig. 1. The general scheme of neuromonitoring eqipe-ment; RE – recording electrodes, SP – stimulator probe, GE – ground electrodes
Ryc. 1. Ogólny schemat sprzętu do neuromonitoringu; RE – elektrody odbierające sygnał, SP – sonda stymu-lująca, GE – elektrody uziemiające
patient pacjent monitor
interface box interfejs
GE RE
for searching (mapping) the laryngeal nerve, be-cause can reach a wider area.
Electrocautery units should be placed at some distance far from the monitoring device because they may produce electrical interference. Some newer neu-romonitoring devices are able to monitor while using monopolar electrocautery. Special muting cables, at-tached to the electrocautery can temporarily control signals in other, older equipment. The device is com-patible with Harmonic and Ligasure technologies.
The monitor as a source of visual information should be placed in visual access of sight of the sur-geon.
After positioning the tube in the patient, the monitor parameters should be checked out. The impedance should be less than 5 kΩ, with an imbal-ance between the electrodes of less than 1 kΩ. Lower electrode impedance, less than 5 kΩ per electrode, suggests good contact between the electrodes and vocal cords. High electrode imbalance means that this contact is not sufficient and requires reposition-ing or exchangreposition-ing of the tube [8].
Another parameter of the monitor is the threshold, which should be set at a level of 100 μV, or up to 200 μV in the case of interfering signals of spontaneous respiratory waveforms.
The stimulating probe ought to be set at a value 1 to 2 mA. 2 mA is better for mapping and search-ing for the laryngeal nerve. After findsearch-ing and dis-secting the nerve, it does not evoke greater ampli-tude. 1 mA should be used for stimulation.
The probe’s output is pulsatile, 4 signals per second. It is important to keep the tip of the probe in one place for some time, rather than intermit-tently touching very quickly.
If stimulation of the RLN and vagus shows no EMG activity, excluding equipment problems, this means that loss of signal (LOS) strongly suggests neural injury.
A surgeon after LOS should consider the mechanism of injury of the nerve and the decision whether or not to operate the second lobe ought to be considered.
When the RLN is being stimulated and there is no EMG activity, the first step is assessment of laryngeal twitch by the surgeon with vagal stimu-lation on that side. The laryngeal twitch is the re-sponse to stimulation of the nerves and the surgeon can “feel” this response, by putting his index finger behind the larynx and feeling the delicate contrac-tions of the muscles. The intraoperative estimation of loss of signal scheme is shown in Fig. 2.
A real cut of the nerve is classified as a type 1 RLN injury. Type 2 injuries are after clip place-ment, overheating or suturing the nerve, when the nerve exists as an anatomical structure, but has no conductivity.
Definitions
The neuromonitoring system has special defi-nitions, which have to be described.
The amplitude of the wave, which was evoked by stimulation of the vagal or RLN, is typically a biphasic waveform which represents the sum-mated motor action. The height of this wave is the distance between its vertical top and lowest point (peak to peak). Its amplitude is correlated with the number of muscle fibers participating in this ac-tion. During normal speech, this amplitude ranges from 100 to 800 μV.
During operation, the amplitude may be af-fected by fluid or blood in the place of stimulation, inadequate probe-nerve contact, covering of the nerve by the fascia, the environmental temperature and endotracheal tube electrode surface position.
The threshold is defined as minimal stimu-lating electricity which triggers minimal EMG activity. The vagus and RLN start to be activated at approximately 0.3 to 0.4 mA, when the nerve is dry and well-dissected. Maximum stimulation of all nerve fibers is achieved at 0.8 mA. Beyond this point, increasing stimulation does not give a better response in the EMG, so rational stimulation for most cases is established at 1 mA. The use of 2 mA is suitable in mapping the RLN, because it gives a greater sphere of tissue around the probe tip.
Wu from Taiwan [20] says that current higher than 1 mA is well tolerated by the nerves, but based on his study on piglets, he showed that 1mA should be selected to minimize the potential risk of nerve damage and false results during IONM.
Latency is described as the time of speed of stimulation-induced depolarization. It depends on the distance to the vocal cord, so depends on the level of stimulation. This time is different during stimulation of the vagal nerves. The latency on the left vagal nerve is longer, because the left RLN has a longer way to the vocal cord, wrapping around the aorta.
The latency for the RLN from the level of thy-roid cartilage is 3.5 milliseconds (ms), the left vagal nerve stimulated at the same level is 8.1 ms, and the right one is 5.4 [2].
and help to improve surgical technique and orienta-tion in the operating field [8].
Generally IONM extends the time of the thy-roid operation but provides much more safety not
only for the patient but also for the operating sur-geon in the way of the medicolegal consequences of surgical complications.
Fig. 2. Intraoperative estimation of loss of signal (LOS)
Ryc. 2. Śródoperacyjna ocena utraty sygnału
laryngeal twich present dodatni objaw przeskakiwania krtani
laryngeal twich absent brak objawu przeskakiwania krtani
neural function is assured zapewniona funkcja nerwu
problem: on recording side * Endotracheal
tube malposition * wires connections * salivary pooling
problem po stronie stymulacji:
* złe położenie rurki intubacyjnej
* połączenia kabli * zbyt duża ilość śliny
stimulation contralateral vagus stymulacja przeciwległego nerwu błędnego
means:
– good position of endotracheal tube – possible injury of
contralateral RLN
znaczy:
– dobre ułożenie rurki intubacyjnej – możliwe uszkodzenie
przeciwległego nerwu krtaniowego wstecznego
stimulation side problem – check wires connections – check neuromuscular blockage
problem dotyczący stymulacji – sprawdź połączenia kabli – sprawdź blokadę
-mięśniową possible LOS
możliwa utrata sygnału
+
-References
Dionigi G, Chiang FY, Rausei S, Wu ChW, Boni L, Lee KW, Rovera F, Cantone G, Bacuzzi A:
[1] Surgical anatomy
and neurophysiology of the vagus nerve (VN) for standardised intraoperative neuromonitoring (IONM) of the inferior laryngeal nerve (ILN) – during thyroidectomy. Langenbecks Arch Surg 2010, 395, 893–899.
Randolph G.W, Dralle H et al.:
[2] Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and para-thyroid surgery: International standards guideline statement. Laryngoscope 2011, 121, S1–S16.
Lahey FH, Hoover WB:
[3] Injuries to the recurrent laryngeal nerve in thyroid operations: their management and avoidance. Ann Surg 1938,108 (4), 545–562.
Lahey FH:
[4] Routine dissection and demonstration of recurrent laryngeal nerves in subtotal thyroidectomy. Surg Gynecol Obstet 1938, 66, 775–777.
Riddel VH:
[5] Injury to recurrent laryngeal nerves during thyroidctomy: a comparison between the results of identi-fication and non-identiidenti-fication in 1022 nerves exposed to risk. Lancet 1956, 29, 638–641.
Jatzko GR, Lisborg PH, Muller MG, Wette VM:
[6] Recurrent nerve palsy after thyroid operations – principal nerve identification and a literature review. Surgery 1994, 115, 139–144.
Lorenz K, Sekulla C, Schelle J, Schmeiβ B, Brauckhoff M, Dralle H:
Chiang FY, Lee KW, Chen HC et al.:
[8] Standarization of Intraoperative Neuromonitoring of recurrent Laryngeal Nerve in Thyroid Operation. World J Surg 2010, 34, 223–229.
Barczyński M, Konturek A, Cichon S:
[9] Randomized clinical trial of visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy. Br J Surg 2009, 96(3), 240–246.
Thomusch O, Sekulla C, Walls G, Machens A, Dralle H:
[10] Itraoperative neuromonitoring of surgery for benign goiter. Am J Surg 2002,183 (6), 673–678.
Dralle H, Sekulla C, Haerting J et al.:
[11] Risk factors of paralysis and functional outcome after recurrent laryngeal nerve monitoring in thyroid surgery. Surgery 2004, 136, 1310–1322.
Barczyński M, Konturek A, Stopa M, Hubalewska-Dydejczyk A, Richter P, Nowak W:
[12] Clinical value of
intra-operative neuromonitoring of the recurrent laryngeal nerves in improving outcomes of surgery for well-differen-tiated thyroid cancer. Pol Przegl Chir 2011, 83(4), 196–203.
Higgins TS, Gupta R, Ketcham AS, Sataloff RT, Wadsworth JT, Sinacori JT:
[13] Recurrent laryngeal nerve
moni-toring versus identification alone on post-thyroidectomy true vocal fold palsy: a meta-analysis. Laryngoscope 2011, 121(5), 1009–1017.
Chiang FY, Lu IC, Kuo WR, Lee KW, Chang NC, Wu CW:
[14] The mechanism of recurrent laryngeal nerve injury during thyroid surgery – the application of intraoperative neuromonitoring. Surgery 2008, 143, 743–749.
Goretzki PE, Schwarz K, Brinkmann J, Wirowski D, Lammers BJ:
[15] The impact of intraoperative
neuromoni-toring (IONM) on surgical strategy in bilateral thyroid diseases: is it worth the effort? World J Surg 2010, 34(6), 1274–1284.
Lu IC, Chu KS, Tsai CJ et al.:
[16] Optimal depth of NIM EMG endotracheal tube for IONM of the RLN during thy-roidectomy. World J Surg 2008, 32, 1935–1939.
Yap SJ, Morris RW, Pybus DA:
[17] Alterations in endotracheal tube position during general anesthesia. Anaesth Intensive Care 1994, 22, 586–588.
Jonas J:
[18] Continuous vagal nerve stimulation for recurrent laryngeal nerve protection in thyroid surgery. Eur Surg Res 2010, 44(3–4), 185–189.
Ulmer C, Friedrich C, Kohler A, Rieber F, Basar T, Deuschle M, Thon KP, Lamadé W:
[19] Impact of continuous
intraoperative neuromonitoring on autonomic nervous system during thyroid surgery. Head Neck 2011, 33(7), 976–984.
Wu CW, MD, Lu IC, Randolph GW, Kuo WR, Lee KW, Chen CL, Chiang FY:
[20] Investigation of optimal intensity
and safety of electrical nerve stimulation during intraoperative neuromonitoring of the recurrent laryngeal nerve: a prospective porcine model. Head Neck 2010, 32(10), 1295–1301.
Address for correspondence:
Paweł Domosławski
1st Department and Clinic of General,
Gastroenterological and Endocrinological Surgery Wroclaw Medical University
Skłodowskiej Curie 66 50-369 Wrocław Poland
Tel.: +48 601 572 162
E-mail: [email protected]
Conflict of interest: None declared

![Crystal structure of [tris(4,4′ bipyridine)]diium bis(1,1,3,3 tetracyano 2 ethoxypropenide) trihydrate](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACH5BAEAAAAALAAAAAABAAEAAAICRAEAOw==)