Breakpoints and Revision of Tetracycline Breakpoints for
Streptococcus
pneumoniae
Steven D. Dallas,a,bLesley McGee,cBrandi Limbago,dJean B. Patel,eM. Leticia McElmeel,bLetitia C. Fulcher,bDavid R. Lonsway,d James H. Jorgensenb
Department of Clinical Laboratory Sciences, University of Texas Health Science Center, San Antonio, Texas, USAa; Department of Pathology, University of Texas Health Science Center, San Antonio, Texas, USAb; Respiratory Diseases Branch, Centers for Disease Control and Prevention, Atlanta, Georgia, USAc; Division of Healthcare Quality Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia, USAd; Office of the Director, Centers for Disease Control and Prevention, Atlanta, Georgia, USAe
A study was performed to derive susceptibility testing interpretive breakpoints for doxycycline with
Streptococcus
pneu-moniae
and to reassess breakpoints for tetracycline using the requirements defined in Clinical and Laboratory Standards
Institute (CLSI) document M23-A3. Tetracycline and doxycycline MICs and disk diffusion zone sizes were determined on
189 isolates selected from the 2009-2010 CDC Active Bacterial Core surveillance strain collection according to the testing
methods described in CLSI documents M07-A8 and M02-A10. Tetracycline and doxycycline MICs and zones were
com-pared to each other directly, and the reproducibility of MICs and zone diameters for both drugs was determined.
Scatter-grams of tetracycline MICs versus corresponding zone diameters and doxycycline MICs versus zones were prepared, and
analysis indicated that the present CLSI tetracycline MIC and disk breakpoints did not fit the susceptibility data for
doxy-cycline. Doxycycline was 1 to 3 dilutions more potent than tetracycline, especially in strains harboring the
tetM
resistance
determinant.
tetM
was detected in
>
90% of isolates having tetracycline MICs of
>
4
g/ml and in
>
90% with doxycycline
MICs of
>
1. Limited pharmacokinetic/pharmacodynamic (PK/PD) data coupled with application of the error-rate
bounded method of analysis suggested doxycycline-susceptible breakpoints of either
<
0.25
g/ml or
<
0.5
g/ml, with
intermediate and resistant breakpoints 1 and 2 dilutions higher, respectively. The disk diffusion zone diameter correlates
were susceptible at
>
28 mm, intermediate at 25 to 27 mm, and resistant at
<
24 mm. Revised lower tetracycline MIC
break-points were suggested as susceptible at
<
1
g/ml, intermediate at 2
g/ml, and resistant at
>
4
g/ml. Suggested
tetracy-cline disk diffusion zones were identical to those of doxycytetracy-cline.
S
treptococcus pneumoniae
is a leading cause of
community-acquired pneumonia (CAP), causing up to 70% of cases (
1
).
It is also a major cause of sepsis, meningitis, and otitis media
(
1
). The emergence of penicillin-resistant
S. pneumoniae
iso-lates has led to the increased use of extended-spectrum
cepha-losporins, macrolides, fluoroquinolones, and even
vancomy-cin. The need for alternate treatment options has enhanced the
importance of accurate susceptibility testing. Doxycycline is
recommended by the Infectious Diseases Society of America as
an alternative antimicrobial agent for the treatment of
commu-nity-acquired pneumonia caused by
Streptococcus pneumoniae
in ambulatory patients and also in those with penicillin
aller-gies (
1
); however, the CLSI document M100-S22 (
2
), which is
used to suggest and interpret susceptibility tests, includes MIC
and disk testing interpretive criteria only for tetracycline. For
this reason, a footnote in the CLSI document states that
“or-ganisms that are susceptible to tetracycline are also considered
susceptible to doxycycline and minocycline.” However, using
tetracycline susceptibility data as a surrogate to predict
doxy-cycline is problematic because it may underestimate the
activ-ity of doxycycline against pneumococci, in which doxycycline
is usually 1 or 2 doubling dilutions more active than
tetracy-cline (
3
). The principal resistance mechanism of
S. pneumoniae
to tetracycline and doxycycline is the ribosomal protection
protein resistance mechanism mediated by the
tetM
gene (
4
).
This gene product affects doxycycline to a lesser degree than it
does tetracycline; thus, using tetracycline as a surrogate may
underestimate the activity of doxycycline against some strains
of
S. pneumoniae
(
5
). In addition, reporting tetracycline as a
surrogate for doxycycline or minocycline requires
susceptibil-ity footnotes on laboratory reports to alleviate potential
mis-understanding by clinicians. The purposes of this study were to
compare
S. pneumoniae
tetracycline and doxycycline
suscepti-bilities, to propose specific MIC and disk diffusion interpretive
breakpoints for doxycycline, and to reassess the MIC and disk
diffusion breakpoints for tetracycline in the context of the
presence of modern pharmacokinetic (PK) and
pharmacody-namic (PD) concepts and the impact of the
tetM
determinant.
MATERIALS AND METHODS
Isolates.One hundred oneS. pneumoniaestrains previously character-ized for tetracycline susceptibility were selected and initially tested in one laboratory (University of Texas Health Science Center, San Anto-nio [UTHSCSA]). The strains were from the 2009-2010 CDC Active Bacterial Core Surveillance (ABCs) study from eight of 10 sites, in-cluding California, Connecticut, Colorado, Maryland, New Mexico,
Received17 January 2013 Returned for modification9 February 2013 Accepted27 March 2013
Published ahead of print3 April 2013
Address correspondence to Steven D. Dallas, [email protected].
Copyright © 2013, American Society for Microbiology. All Rights Reserved.
doi:10.1128/JCM.00125-13
on May 16, 2020 by guest
http://jcm.asm.org/
New York, and Tennessee. The selected strains represented 30 differ-ent serotypes as depicted inTable 1. Fifty-seven strains were initially tetracycline resistant (MIC,ⱖ8), four were tetracycline intermediate (MIC, 4), and 40 were tetracycline susceptible (MIC,ⱕ2). Based upon initially encouraging results and on the recommendations of the staphylococcal and streptococcal working group of the CLSI Antimi-crobial Susceptibility Testing Subcommittee that reviewed the initial data, the same 101 strains and an additional 88 strains from all 10 of the CDC ABCs surveillance program sites were tested at the CDC in the Streptococcal Laboratory and in the Division of Healthcare Quality Promotion (DHQP) laboratory. The additional strains included those from the states mentioned above and from Georgia and Minnesota. Overall, strains were selected to represent approximately 50% tetracy-cline resistance based upon previous testing results.
Reproducibility testing.To determine the reproducibility of MIC and zone diameter determinations, nine selected isolates that exhibited resis-tant tetracycline MICs (8, 16, orⱖ16g/ml) but lower doxycycline MICs (1, 2, 4, or 8g/ml) were repeat tested three times on three separate days. Ten selected isolates with small tetracycline zone diameters (11 to 16 mm) were repeat tested on four different days and measured by four different researchers.
Broth microdilution MIC testing. Tetracycline and doxycycline MICs were determined for each of the 101 strains tested at UTHSCSA using frozen in-lab-prepared microdilution panels containing Mueller-Hinton broth (Difco) with 3% lysed horse blood. These same strains and the 88 additional isolates were tested at the CDC Respiratory Diseases Branch using Mueller-Hinton lysed horse blood panels prepared at CDC
using a different brand (BBL) of Mueller-Hinton dehydrate than that used at the UTHSCSA lab. Retesting of some discrepant MICs was performed at the CDC DHQP laboratory using frozen CDC-prepared panels utiliz-ing Mueller-Hinton broth (BBL) with 5% lysed horse blood. All panels were prepared and inoculated according to CLSI document M07-A8 (6). Panels were incubated at 35°C in ambient air for 20 to 24 h before MIC interpretations.
Disk diffusion testing.Tetracycline and doxycycline disk (BBL, 30
g) diffusion tests were performed with commercially prepared (BD) Mueller-Hinton 5% sheep blood agar plates at the UTHSCSA lab. The same brand (BD) and a second brand (Remel) of commercially prepared Mueller-Hinton sheep blood agar plates were used for disk testing at the CDC labs. The plates were incubated at 35°C in 5% CO2for 20 to 24 h as described in CLSI document M02-A10 (7).
QC.S. pneumoniaeATCC 49619 was used as the control organism for MIC and disk testing. Quality control (QC) was performed with each batch of tests at each laboratory.
tetMPCR.A convenience sample of 118 isolates was analyzed at UTHSCSA and the CDC for the presence of thetetMgene. A 740-bp fragment of thetetMgene was amplified using the primer sequences TETM2 (5=GAACTCGAACAAGAGGAAAGC3=) and TETM3 (5=ATGA AGCCCAGAAAGGAT3=), using the parameters described by Olsvik et al. (4).
[image:2.585.300.544.87.360.2]Data analysis.Tetracycline and doxycycline MICs and zone diam-eters were compared to each other using pivot tables. Scattergrams of isolate MICs versus zone diameters were plotted for tetracycline and doxycycline with the original assumption that doxycycline MIC break-points should be the same as those of tetracycline. For the purpose of creating merged scattergrams, the means of the repeat disk diffusion zones determined at the CDC using Remel agar were plotted along with the BD agar zones from UTHSCSA. Doxycycline disk breakpoints were analyzed by the error-rate bounded method of Metzler and De-Haan (8,9).
TABLE 1Streptococcus pneumoniaeserotype distribution for the 189 isolates tested
Serotype No. of isolates
[image:2.585.43.288.89.426.2]1 6 3 15 6A 2 6B 8 6C 7 7C 3 7F 12 8 3 9N 6 9V 1 10A 3 11A 2 12F 6 13 1 14 2 15A 15 15B 2 16F 2 18C 2 19A 53 19F 3 20 1 22F 8 23A 11 23B 4 31 2 33F 5 35B 2 35F 1 37 1 Total 189
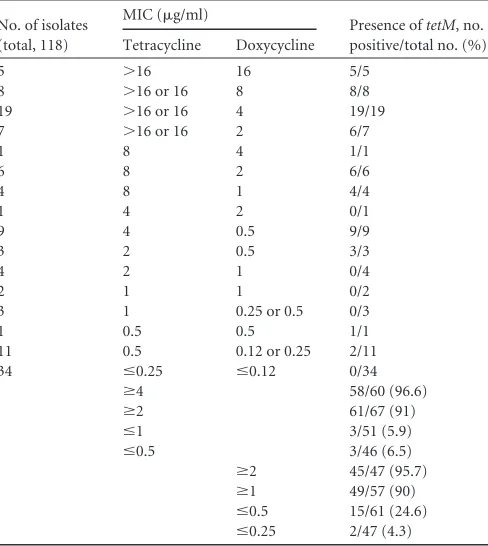
TABLE 2Comparison of tetracycline and doxycycline MICs with the presence of thetetMresistance determinant
No. of isolates (total, 118)
MIC (g/ml)
Presence oftetM, no. positive/total no. (%) Tetracycline Doxycycline
5 ⬎16 16 5/5
8 ⬎16 or 16 8 8/8
19 ⬎16 or 16 4 19/19
7 ⬎16 or 16 2 6/7
1 8 4 1/1
6 8 2 6/6
4 8 1 4/4
1 4 2 0/1
9 4 0.5 9/9
3 2 0.5 3/3
4 2 1 0/4
2 1 1 0/2
3 1 0.25 or 0.5 0/3
1 0.5 0.5 1/1
11 0.5 0.12 or 0.25 2/11
34 ⱕ0.25 ⱕ0.12 0/34
ⱖ4 58/60 (96.6)
ⱖ2 61/67 (91)
ⱕ1 3/51 (5.9)
ⱕ0.5 3/46 (6.5)
ⱖ2 45/47 (95.7)
ⱖ1 49/57 (90)
ⱕ0.5 15/61 (24.6)
ⱕ0.25 2/47 (4.3)
New Doxycycline and Tetracycline Breakpoints
on May 16, 2020 by guest
http://jcm.asm.org/
Discrepancy analysis.Nonconcordant MIC/zone diameter results were investigated using CLSI document M23-A3, section 8.2.3.2, page 25 (10). Essentially, if no obvious technical or transcriptional errors were found, the tests were repeated twice using separate inocula. If at least two of the three results were identical, the original data point was replaced with this new data point in the scattergram. If all results (original and the repeat results) were different, the original result was retained. The detailed results of all discordant pair results were re-corded in a separate table.
RESULTS
Reproducibility testing.
Both tetracycline and doxycycline
MICs and zone diameters were found to be highly
reproduc-ible, with MICs varying by 1 dilution or less (data not shown).
Disk diffusion zone sizes varied by 2 mm or less (data not
shown).
MIC testing.
Doxycycline was consistently more potent (lower
MICs) than tetracycline, especially against the
tetracycline-resis-tant isolates harboring
tetM
(
Table 2
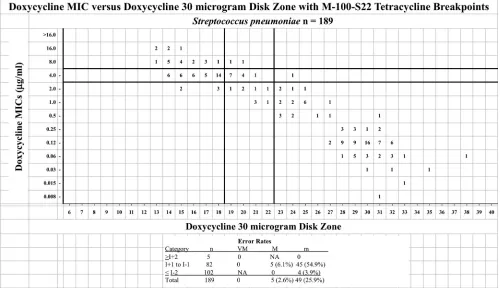
). Review of the doxycycline
scattergrams indicated that the present CLSI tetracycline MIC and
disk breakpoints did not fit the distribution of susceptibility data
for doxycycline (
Fig. 1
).
[image:3.585.43.543.69.357.2]tetM
PCR.
The presence of the
tetM
resistance determinant
was examined in 30 of the initial 101 isolates and all 88 additional
isolates (118 total isolates) and was detected primarily in isolates
TABLE 3Comparison of tetracycline and doxycycline MICs among the initial 101 isolates
Tetracycline MIC (g/ml)
No. of isolates with doxycycline MIC (g/ml):
0.03 0.06 0.12 0.25 0.5 1 2 4 8 16 Total
⬎16 5 29 8 3 45
16 1 6 1 8
8 3 1 4
4 1 3 4
0.5 1 2 3
0.25 12 12
0.12 12 9 21
0.06 2 2 4
Total 2 14 22 3 3 3 7 35 9 3 101
FIG 1Scattergram comparing the results of doxycycline broth microdilution MICs (micrograms/ml) to the inhibition zone diameters (mm) around a 30-g doxycycline disk for 189 isolates ofStreptococcus pneumoniaetested in three laboratories using historic tetracycline breakpoints per CLSI document M100-S22. The table at the bottom depicts the number of isolates tested (n) and very major (VM), major (M), and minor (m) error rates for each category: greater than or equal to the intermediate category breakpoint plus 2 dilutions (ⱖI⫹2), intermediate category breakpoint plus or minus 1 dilution (I⫹1 to I⫺1), and less than or equal to the intermediate category breakpoint minus 2 dilutions (ⱕI⫺2) (10). NA, not applicable.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:3.585.42.548.590.723.2]having tetracycline MICs of
ⱖ4
g/ml and with doxycycline MICs
of
ⱖ
1
g/ml (
Table 3
). These microbiological data coupled with
limited pharmacokinetic and pharmacodynamic (PK/PD) data
suggested that the doxycycline susceptible breakpoint should
probably be 0.25 or 0.5
g/ml (
Table 4
).
DISCUSSION
Historically, surrogate reporting of antimicrobial agents has
been an accepted and efficient mechanism of testing a
repre-sentative class agent and trusting that the antimicrobial
suscep-tibility or resistance data generated would apply to other agents
in the class. The combined results of this study generated in
three different laboratories from 189
S. pneumoniae
strains
in-dicate that specific testing criteria for doxycycline could be
employed rather than relying on the less potent agent
tetracy-cline as a surrogate for doxycytetracy-cline with
Streptococcus
[image:4.585.39.286.89.157.2]pneu-moniae.
In performing this exercise and reviewing limited
PK/PD data for tetracycline (
3
,
5
), it became apparent that a
revision of the tetracycline breakpoints was also in order.
Doxycycline is more potent than tetracycline against
S.
pneu-moniae, based on lower doxycycline MICs (usually by 1 to 3
2-fold dilutions), especially with strains containing the
tetM
determinant. Limited PK/PD data (
3
,
5
) coupled with
applica-tion of the error-rate bounded method of analysis suggested
doxycycline-susceptible breakpoints of either
ⱕ
0.25
g/ml or
0.5
g/ml, with intermediate at 0.5 or 1
g/ml and resistant at
ⱖ1 or 2
g/ml, and disk diffusion susceptible zones of
ⱖ28
mm, intermediate zones of 25 to 27 mm, and resistant zones of
ⱕ
24 mm with either set of MIC breakpoints (
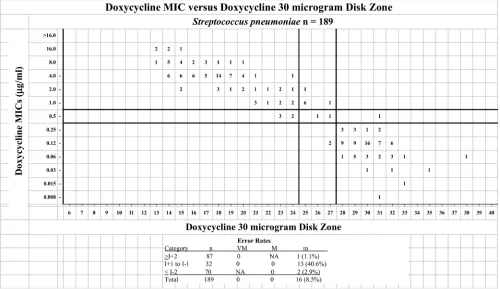
Fig. 2
). Revised
tetracycline MIC breakpoints are suggested as susceptible at
ⱕ
1
g/ml, intermediate at 2
g/ml, and resistant at
ⱖ
4
g/ml.
Suggested tetracycline disk diffusion zones are identical to
those of doxycycline (
Fig. 3
). Testing of doxycycline specifically
might better represent the activity of that agent against
pneu-mococci and would make laboratory reporting simpler than
having to indicate that a surrogate marker was used in testing.
These data and tentative recommendations were reviewed by
the Antimicrobial Susceptibility Testing Subcommittee of the
CLSI and serve as the basis of recommendations published in
the newest edition of CLSI document M100, M100-S23 (
11
).
The CLSI subcommittee chose the lower set of doxycycline
breakpoints due to concerns about declaring some strains with
TABLE 4New and previous doxycycline and tetracycline MIC (g/ml) and disk diffusion (mm) breakpoints forS. pneumoniae
Antimicrobial agent
Breakpoint (g/ml), S, I, R, by CLSI standard
MIC Zone diam
New (M100-S23)
Previous
(M100-S22) New (M100-S23) Previous (M100-S22) Doxycycline ⱕ0.25, 0.5,ⱖ1 NAa ⱖ28, 25–27,ⱕ24 NA
Tetracycline ⱕ1, 2,ⱖ4 ⱕ2, 4,ⱖ8 ⱖ28, 25–27,ⱕ24 ⱖ23, 19–22,ⱕ18 aNA, not applicable.
FIG 2Scattergram comparing the results of doxycycline broth microdilution MICs (micrograms/ml) to the inhibition zone diameters (mm) around a 30-g doxycycline disk for 189 isolates ofStreptococcus pneumoniaetested in three laboratories. The solid lines represent the proposed interpretive criteria. The table at the bottom depicts the number of isolates tested (n) and very major (VM), major (M), and minor (m) error rates for each category: greater than or equal to the intermediate category breakpoint plus 2 dilutions (ⱖI⫹2), intermediate category breakpoint plus or minus 1 dilution (I⫹1 to I⫺1), and less than or equal to the intermediate category breakpoint minus 2 dilutions (ⱕI⫺2) (10). NA, not applicable.
New Doxycycline and Tetracycline Breakpoints
on May 16, 2020 by guest
http://jcm.asm.org/
[image:4.585.43.543.386.675.2]the
tetM
determinant to be susceptible or intermediate to
doxycycline (
12
).
ACKNOWLEDGMENTS
S.D.D. has received research support from Meridian Biosciences Inc. J.H.J. has consulted for Accelerate Diagnostics and Merck and received research support from bioMerieux and Merck. For all other authors, there are no conflicts to report. No outside funding was received to support this study.
We thank the CDC ABCs sites for collection of the pneumococcal strains used in this study.
REFERENCES
1.Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM, Jr, Musher DM, Niederman MS, Torres A, Whitney CG.2007. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis.44(Suppl 2):S27–S72. doi:10 .1086/511159.
2.Clinical and Laboratory Standards Institute.2012. Performance stan-dards for antimicrobial susceptibility testing. Twenty-second informa-tional supplement, M100-S22. Clinical and Laboratory Standards Insti-tute, Wayne, PA.
3.Christianson J, Andes D, Craig WA.2001. Characterization of the phar-macodynamics of doxycycline againstStreptococcus pneumoniaein a mu-rine thigh-infection model, abstr A-1103. Abstr. 41st Intersci. Conf. An-timicrob. Agents Chemother.
4.Olsvik B, Olsen I, Tenover FC.1995. Detection oftet(M) andtet(O) using polymerase chain reaction in bacteria isolated from patients with periodontal disease. Oral Microbiol. Immunol.10:87–92.
5.Christianson J, Andes D, Craig WA. 2001. Magnitude of the 24-H AUC/MIC required for efficacy of doxycycline (DOXY) against Strepto-coccus pneumoniae(SP) in a murine thigh-infection model, abstr 475. Abstr. 39th Annu. Meet. Infect. Dis. Soc. Am.
6.Clinical and Laboratory Standards Institute.2009. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically. Ap-proved standard, 8th ed, M07-A8. Clinical and Laboratory Standards In-stitute, Wayne, PA.
7. Clinical and Laboratory Standards Institute. 2009. Performance standards for antimicrobial disk susceptibility tests; approved stan-dard—10th ed, M02-A10. Clinical and Laboratory Standards Institute, Wayne, PA.
8.Brunden MN, Zurenko GE, Kapik B.1992. Modification of the error-bounded classification scheme for use with two MIC breakpoints. Diagn. Microbiol. Infect. Dis.15:135–140.
9.Metzler DM, DeHaan RM.1974. Susceptibility tests of anaerobic bacte-ria: statistical and clinical considerations. J. Infect. Dis.130:588 –594. 10. Clinical and Laboratory Standards Institute.2008. Development of in
vitro susceptibility testing interpretive criteria and quality control param-eters. Approved guideline, 3rd ed, M23-A3. Clinical and Laboratory Stan-dards Institute, Wayne, PA.
11. Clinical and Laboratory Standards Institute.2013. Performance stan-dards for antimicrobial susceptibility testing. Twenty-third informational supplement, M100-S23. Clinical and Laboratory Standards Institute, Wayne, PA.
12. Dudley MN, Ambrose PG, Bhavnani SM, Craig WA, Ferraro MJ, Jones RN.18 January 2013. Background and rationale for revised Clinical and Laboratory Standards Institute (CLSI) interpretive criteria (breakpoints) forEnterobacteriaceaeandPseudomonas aeruginosa: I. Cephalosporins and aztreonam. Clin. Infect. Dis. [Epub ahead of print.] doi:10.1093/cid /cit017.
FIG 3Scattergram comparing the results of tetracycline broth microdilution MICs (micrograms/ml) to the inhibition zone diameters (mm) around a 30-g tetracycline disk for 189 isolates ofStreptococcus pneumoniaetested in three laboratories. The dotted lines represent current interpretive criteria. The solid lines represent the proposed interpretive criteria. The table at the bottom depicts the number of isolates tested (n) and very major (VM), major (M), and minor (m) error rates for each category: greater than or equal to the intermediate category breakpoint plus 2 dilutions (ⱖI⫹2), intermediate category breakpoint plus or minus 1 dilution (I⫹1 to I⫺1), and less than or equal to the intermediate category breakpoint minus 2 dilutions (ⱕI⫺2) (10). NA, not applicable.