Public Health Theses School of Public Health
8-11-2015
The Role of Health Literacy and Numeracy on
Exercise Self-efficacy and Exercise Behavior in the
PAADRN Bone Health Intervention
Elizabeth A. Fallon
Follow this and additional works at:https://scholarworks.gsu.edu/iph_theses
This Thesis is brought to you for free and open access by the School of Public Health at ScholarWorks @ Georgia State University. It has been accepted for inclusion in Public Health Theses by an authorized administrator of ScholarWorks @ Georgia State University. For more information, please contact [email protected].
Recommended Citation
Fallon, Elizabeth A., "The Role of Health Literacy and Numeracy on Exercise Self-efficacy and Exercise Behavior in the PAADRN Bone Health Intervention." Thesis, Georgia State University, 2015.
ABSTRACT
THE ROLE OF HEALTH LITERACY AND NUMERACY ON EXERCISE SELF-EFFICACY AND EXERCISE BEHAVIOR
IN THE PAADRN BONE HEALTH INTERVENTION
By
ELIZABETH ANNE FALLON
JULY 21, 2015
INTRODUCTION: Osteoporotic bone fracture is a major cause of hospitalization, disability, loss of independent living capacity, and mortality among aging adults. Although physical exercise may sustain bone mineral density and prevent falls and fractures among individuals at risk for low bone mineral density, adherence to exercise recommendations is low. Increasing efficacy and effectiveness of treatment for osteoporosis would benefit from examination of heterogeneity of treatment effects. Previous research indicates that poor health literacy (HL) and health numeracy (HN) may be associated with less exercise behavior and heterogeneity of treatment effects may be evident across high and low level of health literacy and/or health numeracy.
AIM: Examine heterogeneity of treatment effects due to HL/HN on post-intervention exercise self-efficacy and exercise behavior among older adults enrolled in a large, multi-site randomized controlled trial designed to increase exercise as part of osteoporosis guideline concordant care.
EMBARGO
This thesis is postponed from public release for 2 years from the date of degree
THE ROLE OF HEALTH LITERACY AND NUMERACY ON EXERCISE SELF-EFFICACY AND EXERCISE BEHAVIOR IN THE PAADRN BONE HEALTH
INTERVENTION
by
ELIZABETH A. FALLON
B.S., UNIVERSITY OF FLORIDA M.S.E.S.S., UNIVERSITY OF FLORIDA
Ph.D., UNIVERSITY OF FLORIDA
A Thesis Submitted to the Graduate Faculty of Georgia State University in Partial Fulfillment
of the
Requirements for the Degree
MASTER OF PUBLIC HEALTH
APPROVAL PAGE
THE ROLE OF HEALTH LITERACY AND NUMERACY ON EXERCISE SELF-EFFICACY AND EXERCISE BEHAVIOR
IN THE PAADRN BONE HEALTH INTERVENTION
by
ELIZABETH A. FALLON
Approved:
_____________________________________________ Douglas Roblin, Ph.D., Georgia State University
Committee Chair
____________________________________________ Fredric Wolinsky, Ph.D., University of Iowa
Committee Member
DEDICATION
To Brett -
For loving me every day,
ACKNOWLDEGEMENTS
First and foremost, thank you to my committee chair, Dr. Douglas Roblin (Georgia State University), who embodies the noblest ideals of science and academia. His focus on good science through interdisciplinary collaborations has challenged me to broaden my knowledge base, while encouraging me to contribute from my existing areas of
expertise. I could not have imagined a better mentor during this time of professional growth and transition.
Thank you to Dr. Fredric Wolinsky (Thesis Committee Member, University of Iowa), for your brilliant ideas for solving data access problems, and your valuable time in reading this document, and engaging in my thesis defense.
To the entire PAADRN Steering Committee: Dr. Wolinsky, Dr. Roblin, Dr. Peter Cram, Dr. Ken Saag - thank you for your openness to a new collaborator at such a demanding time in the PAADRN trial.
To the members of the PAADRN team (Stephanie Edmonds, Dr. Yiyue Lou, and Thuy Nguyen) who acclimate me to the PAADRN data - Thank you for sharing data
dictionaries, creating simulated data sets, and ultimately, running my SAS code to send the output.
To the GSU biostatistics faculty (Dr. Lai, Dr. Luo, and Dr. Hayat), who put so much time and effort into an evolving and excellent curriculum. I’m already putting my new skills into practice, everyday!
To Tracy Ayers – thank you for being the best SAS teacher, ever.
Thank you to Jessica Pratt, Gina Sample, and Dr. Maggie Tolan who shepherded me (and all my paperwork and petitions) through the MPH process, from admission to graduation. Your passion, work ethic, and thoughtful advice for professional
development have been invaluable.
Finally, to my wonderful family, friends and colleagues: George Fallon, Keith Fallon, Sara Wilcox, Bryan Blissmer, Debra Riebe, Colleen Redding, Ninoska Peterson, Cheryl Der Ananian, Melissa Bopp, Brandonn Harris, Emily Murphy, Kim Fournier, Paige
Author’s Statement Page
In presenting this thesis as a partial fulfillment of the requirements for an advanced degree from Georgia State University, I agree that the Library of the University shall make it available for inspection and circulation in accordance with its regulations governing materials of this type. I agree that permission to quote from, to copy from, or to publish this thesis may be granted by the author or, in his/her absence, by the professor under whose direction it was written, or in his/her absence, by the Associate Dean, School of Public Health. Such quoting, copying, or publishing must be solely for scholarly purposes and will not involve potential financial gain. It is understood that any copying from or publication of this dissertation which involves potential financial gain will not be allowed without written permission of the author.
Author: Elizabeth A. Fallon
TABLE OF CONTENTS
DEDICATION …………...5
ACKNOWLEDGMENTS ...6
LIST OF TABLES………..10
LIST OF FIGURES………...12
1. INTRODUCTION & LITERATURE REVIEW ...13
1.1 National Osteoporosis Foundation Recommendations for Prevention and Treatment of Osteoporosis...………...14
1.2 Role of Physical Exercise for Bone Health ………...15
1.3 Public Health Interventions for Exercise among Individuals at Risk of Osteoporosis………...19
1.4 Mediators and heterogeneity of physical activity intervention effects...…….…...21
1.5 Health Literacy/Numeracy……….……….…...22
1.6 Health Literacy/Numeracy and Health Outcomes.…...24
1.7 Health Literacy/Numeracy and Musculoskeletal Health………...26
1.8 Health Literacy/Numeracy and Exercise Behavior ………...27
2. PURPOSE AND HYPOTHESES………...29
3. METHODS AND PROCEDURES…...36
3.1 Description of the Data……….………..….36
3.2 Protection of human subjects ………....36
3.3 Measures……….…………...37
3.3.1 Demographic Variables ...37
3.3.2 Health Literacy ...38
3.3.3. Health Numeracy ...38
3.3.4. Exercise Behavior ...39
3.3.5. Exercise Self-Efficacy ...40
4. RESULTS...43
4.1 Differences for covariates by treatment group ……...43
4.2 Research Objective 1 ……....…...44
4.3 Research Objective 2...46
4.4 Research Objective 3...47
4.5 Research Objective 4...54
5. DISCUSSION AND CONCLUSION...57
REFERENCES...63
TABLES...79
FIGURES...97
APPENDIX A..………...98
APPENDIX B..………...105
List of Tables
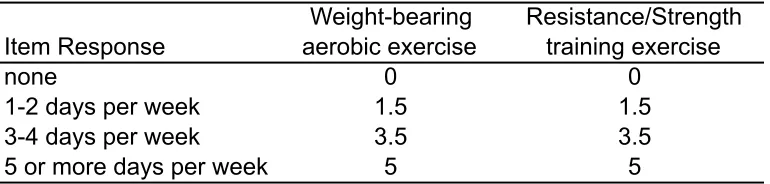
Table 1. Weighted scoring of the exercise measure.
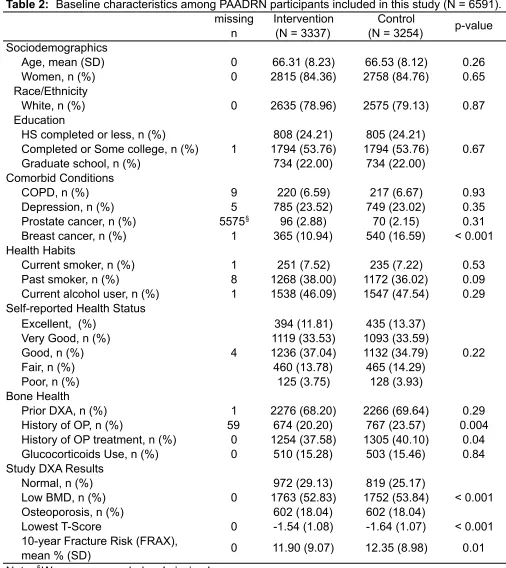
Table 2. Baseline characteristics among PAADRN participants included in this study (N = 6591).
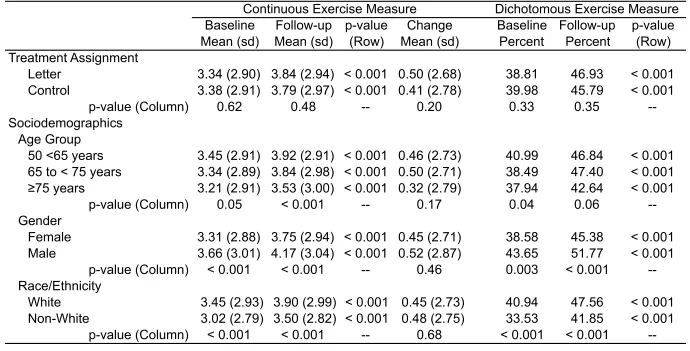
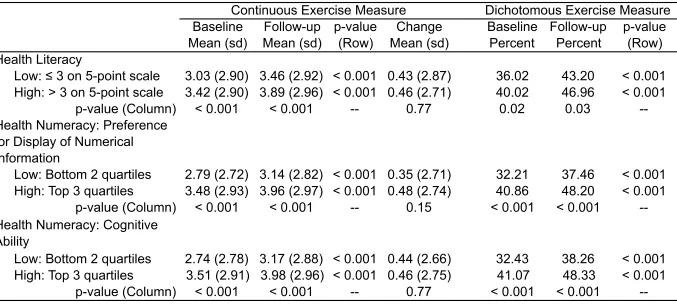
Table 3. Baseline and 12-week follow-up exercise behavior by treatment assignment, covariates, health literacy, and health numeracy (N = 6591).
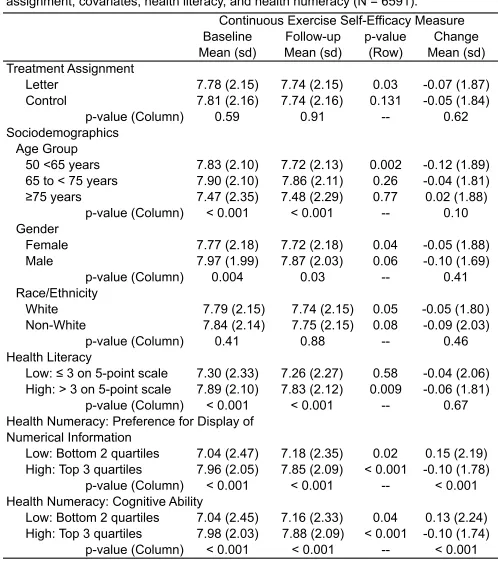
Table 4. Baseline and 12-week follow-up exercise self-efficacy by treatment assignment, covariates, health literacy, and health numeracy (N = 6591). Table 5a. Correlations of 12-week follow-up exercise behavior (continuous, dependent
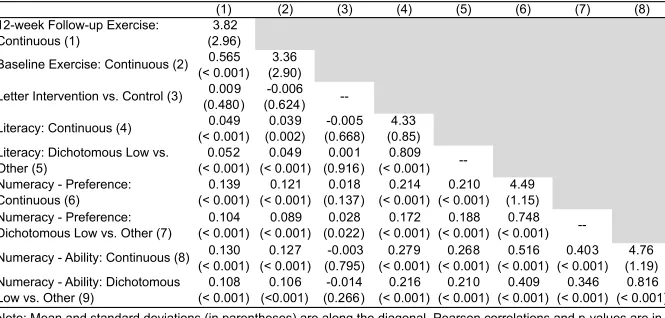
variable) with baseline exercise behavior (continuous), treatment assignment (independent variable), health literacy and health numeracy (moderator variables; N = 6591).
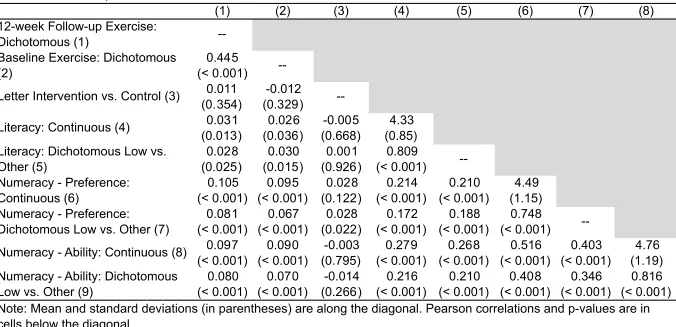
Table 5b. Correlations of 12-week follow-up exercise behavior (dichotomous, dependent variable) with baseline exercise behavior (dichotomous), treatment
assignment (independent variable), health literacy and health numeracy (moderator variables; N = 6591).
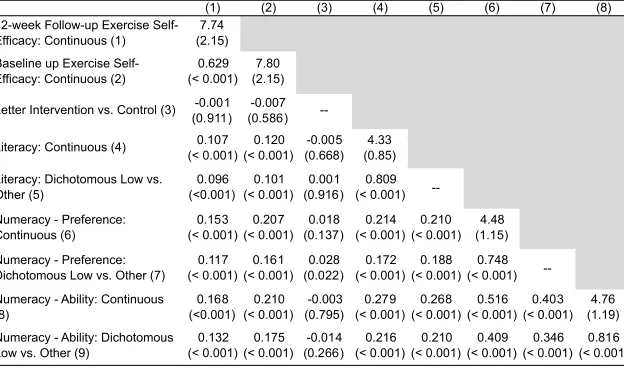
Table 6. Correlations of 12-week follow-up exercise self-efficacy (continuous, dependent variable) with baseline exercise self-efficacy (continuous), treatment assignment (independent variable), health literacy and health numeracy (moderator variables; N = 6591).
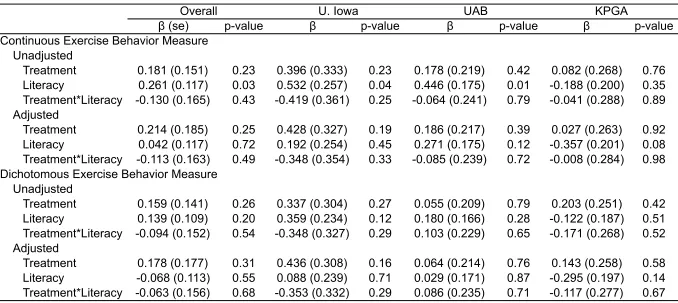
Table 7. Pooled and site-specific regression models (with and without covariates) assessing heterogeneity of treatment effects by literacy level (dichotomous) on 12-week follow-up exercise behavior (N = 6591).
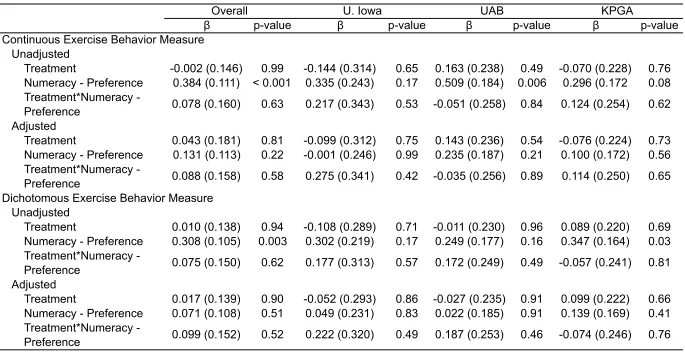
Table 8a. Pooled and site-specific regression models (with and without covariates) assessing heterogeneity of treatment effects by level of preference for
numerical display (dichotomous) on 12-week follow-up exercise behavior (N = 6591).
Table 9. Pooled and site-specific regression models (with and without covariates) assessing heterogeneity of treatment effects by literacy level (dichotomous) on 12-week follow-up exercise self-efficacy (N = 6591).
Table 10. Pooled and site-specific regression models (with and without covariates) assessing heterogeneity of treatment effects by level of numeracy ability (dichotomous) and level of preference for numerical display (dichotomous) on 12-week follow-up exercise self-efficacy (N = 6591).
List of Figures
Introduction
Osteoporosis is characterized by having bone mineral density (BMD) more than
2.5 standard deviations below normal for a healthy 30-year old adult 1,2. Osteopenia is
having a BMD value more than one standard deviation below normal for a healthy
30-year old adult, but less than the 2.5 standard deviations required for osteoporosis
diagnosis. The major deleterious health outcome of osteoporosis is bone fracture,
typically of the hip, vertebrae, and wrist, and is a major cause of hospitalization, loss of
productivity, loss of independent living capacity, and disability among aging adults 3.
Furthermore, among those sustaining hip fractures, mortality rate within one year of
fracture is 20%4.
In the United States, 10.2 million adults have osteoporosis, with osteopenia
affecting an additional 43.4 million5. Currently, annual United States
osteoporotic-related fracture costs are an estimated $US 16.9 billion, with annual costs projected to
rise to $US 25 billion by 2025. Among women 55 years and older, costs associated with
osteoporotic-related bone fracture are more costly than myocardial infarction, stroke, or
breast cancer6.
Internationally, an estimated 49 million individuals over 50 years have
osteoporosis, with higher prevalence among women (9% - 38%), compared to men (1%
- 8%)7. Similar to the United States, costs associated with osteoporotic-related fracture
increase six-fold by 2050 9.
Thus, due to the significant morbidity, mortality, and economic costs of
osteoporotic-fracture and the projected population growth among individuals over 65
years, effective public health interventions designed to improve bone health and
ultimately reduce risk of falls and bone fracture are needed.
LITERATURE REVIEW
National Osteoporosis Foundation Recommendations for Prevention and
Treatment of Osteoporosis. The National Osteoporosis Foundation provides detailed
recommendations for the prevention, risk assessment, diagnosis, and treatment of
osteoporosis in clinical settings10. Briefly, prevention and risk assessment
recommendations state that all men age ≥50 years and postmenopausal women should
be evaluated for osteoporosis risk and universally counseled on prevention actions
(e.g., disease risk, fracture risk, falls prevention, calcium and vitamin D dietary
requirements, necessary weight-bearing, muscle strengthening, flexibility and balance
exercise, smoking cessation, and limiting alcohol consumption). Additionally, height
should be measured annually, using a stadiometer. Approved pharmacologic treatment
(e.g., bisphosphonates, calcitonin, estrogen agonist/antagonist, estrogen or hormone
therapy) should be implemented for:
(a) individuals with BMD ≤ -2.5 standard deviations below normal for a healthy
(b) men aged ≥50 years and postmenopausal women with low bone mineral density
(-1.0 to -2.5 standard deviations below normal for a healthy 30-year old adult)
and a 10-year fracture risk ≥3%, or
(c) a 10-year fracture risk score ≥20%.
Finally, according to National Osteoporosis Foundation recommendations, regular
monitoring (minimum every 1-2 years 10) using BMD testing and biochemical markers
should be conducted to determine the efficacy of individual treatment programs, and
use as basis of treatment initiation and/or modification when indicated 10.
Role of Physical Exercise for Bone Health. The National Osteoporosis
Foundation recommends provider counseling, and subsequent patient self-management
of, and adherence to, physical exercise. Exercise is an important component of
osteoporosis treatment as scientific evidence suggests that exercise interventions
reduce falls 11, sustain and may even modestly increase BMD10 among aging adults
(See Appendix A12-27).
For the purposes of this thesis, systematic literature reviews and meta-analytic
reviews exploring the effect of various exercise modalities on bone mineral density are
summarized in Appendix A12-27. Because osteoporosis prevalence is higher among
women, compared to men, 70.6% (12/17) of reviews have focused on the effect of
exclusively on postmenopausal women. Across the 12 reviews focusing on women,
there is an overall positive effect of exercise on BMD for the:
(a) lumbar spine (total reporting = 9 reviews; positive effect = 8, no effect = 1,
negative effect = 0) and
(b) femur/femoral neck (total reporting = 12 reviews w/13 effect sizes; positive
effect = 7, no effect = 6, negative effect = 0).
The effect of exercise on other skeletal sites (e.g., total hip, vertebral, radius,
whole body) has also been systematically reviewed within the literature, but to a lesser
extent. Despite fewer studies assessing these other skeletal sites, authors generally
note that the findings are similar to that of the lumbar spine and femoral neck,
suggesting that physical exercise likely produces a small, but clinically relevant increase
in BMD among women.
In contrast to the large number of reviews focusing on women, only three
literature reviews have focused exclusively on adult men, all reporting a positive effect
of exercise on the femur/femoral neck. Only one review concluded that exercise
significantly increases BMD for the lumbar spine (no effect = 2).
Regardless of the gender focus of the research, several reviews have noted the
lack of methodological quality among controlled trials examining the effect of exercise
on bone density. Many trials do not have sufficient power to detect change, are
blinding, fail to report compliance/drop-out, and fail to conduct intent-to-treat analysis
and assess/incorporate important confounders (e.g., use of contraception, hormone
replacement therapy). Furthermore, few studies have provided long-term follow-up data.
In light of these methodological limitations within the literature, perhaps the best
approach is to rely on the following conclusions from the most comprehensive and
rigorous systematic literature review of randomized controlled trials examining exercise
on BMD28. These conclusions are that:
a) low intensity resistance training showed no effect on BMD at any skeletal
site,
b) high intensity resistance training showed a significant effect for the spine
and femoral neck, but not total hip,
c) low intensity weight bearing aerobic exercise (e.g., walking, tai chi) had a
significant effect on the spine, while
d) high intensity weight bearing aerobic exercise (e.g., jogging, jumping) had
a significant effect on BMD for total hip and trochanter, but no significant
effect for femoral neck spin, med femur, or tibia 28.
An unfortunate consequence of poor methodological quality within this area of
research is the wide variation in physical activity recommendations adopted across
professional organizations interested in aging adults, exercise, and bone health (See
Appendix B) 10,29-35. While there is agreement that weight-bearing aerobic and anaerobic
needed to assess recent advances in exercise and bone health research and based on
these assessments, create and promote consistent set of recommendations for physical
activity and optimal bone health. Specifically, patients would benefit from health
promotion messages that provide:
(a) minimum exercise duration needed for treatment efficacy and
(b) specific guidance regarding frequency, intensity, time per session, number of
sets/repetitions, mode, or specific exercises most beneficial to improve BMD in
general or at specific body sites.
In conclusion, individuals utilizing physical exercise to improve bone health are
best advised to engage in a combination of moderate to high intensity weight-bearing
aerobic activities (e.g., jogging, jumping, stair climbing) and a whole-body
resistance-training regimen. Regular reassessments of exercise regimen should be conducted to
ensure variety, and continued fitness progression. Furthermore, future clinical trials
examining the effect of exercise on BMD should better adhere to recommendations for
progressive resistance training, cardiovascular health, and older adults 32,36,37 as the
foundational starting point for developing experimental exercise protocols for bone
health. Finally, public health interventions promoting exercise among older adults with
osteoporosis or osteopenia should:
(a) separately promote and measure aerobic weight bearing exercise and
(b) stratify aerobic, strength training, and combined aerobic/strength training
exercise behavior by two (not meeting/meeting recommendations) or three
groups (sedentary/insufficient activity/meets recommendations), and
(c) use both self-report and objective measures of physical activity, where
feasible.
Public Health Interventions for Exercise among Individuals at risk of
Osteoporosis. Because physical exercise can sustain and increase BMD, establishing
efficacious public health interventions to initiate and maintain sufficient levels of physical
activity among aging adults at risk of osteoporosis and osteoporotic fracture becomes
paramount.
The earliest reviews of osteoporosis disease management identified only 2 and 3
randomized control trials using exercise for disease management 38 and prevention of
osteoporotic fractures 39, respectively. Lock et al. 39 concluded from their review that
these interventions resulted in a lower risk of spinal fractures, but this finding was not
statistically significant [total 322 participants; RR = 0.52, 95% CI: 0.17, 1.60]. In 2010,
Lai et al. 40 reviewed a total of 24 randomized control trials of healthcare interventions
for community-dwelling postmenopausal women with osteoporosis and found that 80%
(4/5 studies) showed improvement in calcium intake, while only 25% (1/4 studies)
showed increases in exercise. Most recently, a systematic review of multifaceted
osteoporosis group education interventions summarized a total of seven studies, and
fitness. Of these 75% (3/4) reported significant, positive changes in exercise behavior
and/or fitness.
Fortunately, in the absence of literature specifically focused on lifestyle
interventions to improve bone health among older adults, there is much to be learned
from the plethora of recent systematic and meta-analytic reviews summarize public
health physical activity interventions aimed at aging adults, in general 41-45, and frail
older adults at risk for falls 46,47. Overall, these reviews provide substantial evidence in
support of:
(a) theory-based psychosocial and behavioral interventions 41,44,
(b) the importance of self-efficacy in the behavior change process 41,
(c) the use of “mediated” (non-face-to-face via mailed print materials), “technology
mediated” (telephone, internet) interventions 44 and remote feedback
interventions 42,
(d) the benefit of health care provider and health clinic-based interventions 45,48, and
(e) successful long-term maintenance of physical activity at 12 months follow-up,
but not 24 months follow-up 43.
Thus, behavioral and public health scientists have established a robust foundation from
which scientists and practitioners can learn about efficacious interventions to increase
physical activity and improve health outcomes of older adults.
Public health interventions have some limitations. There is limited information on
and maintenance of resistance training in older adults 49; an exceptional oversight given
the large number of older adults at risk for low BMD and osteoporotic fractures, who
would benefit greatly from moderate- to high-intensity resistance training28. Finally, more
research is needed to better understand mediators of treatment effects and factors
leading to heterogeneity of treatment effects, which may enable increased efficacy of
health communication approaches, individualized tailoring, and potentially improve
cost-effectiveness.
Mediators and heterogeneity of physical activity intervention effects. Due to the
extensive number of physical activity interventions aimed at aging adults, systematic
and meta-analytic reviews have examined heterogeneity of treatment effects and
reported that intervention-induced changes in physical activity behavior were unrelated
to gender 50,51, age 50, race/ethnicity 50, socioeconomic distribution 50, and delivery
method (e.g., home vs. center-based, telephone, mail) 50.
Compared to the examination of factors leading to heterogeneity of treatment
effects, mediation analyses have only recently been widely implemented for physical
activity interventions. Thus, despite heterogeneity of behavioral interventions for
physical activity, only a small number of mediators have been examined. A review of 23
reported studies revealed that insufficient data was available to advocate for one
behavioral theory over another, but did note that self-regulation constructs had the best
Other than socio-economic and demographic characteristics (that are not
mutable), health literacy and health numeracy are two constructs that potentially
influence the efficacy and effectiveness of healthcare and lifestyle interventions for
chronic disease. Self-management regimens required for chronic diseases (e.g., type II
diabetes, heart disease, cancer and osteoporosis) are often complex, and require
patient comprehension of treatment options, health insurance benefits, provider
instructions regarding medication side effects and adherence, and lifestyle changes
(e.g., diet and exercise). As such, lower health literacy has been consistently associated
with greater emergency room admissions and hospitalization, lower use of
evidence-based preventive services (e.g., mammography screenings and flu vaccines), lower
medication adherence, poorer ability to interpret labels and health messages, and
poorer overall health status, and higher mortality rates among aging adults 53.
Health literacy/numeracy. The most widely accepted definition of health literacy is
“the degree to which individuals have the capacity to obtain, process, and understand
basic information and services needed to make appropriate decisions regarding their
health” 54,55. The Institute of Medicine further expands health literacy into four domains
56 considered to be aspects of “health knowledge”:
(1) cultural and conceptual knowledge,
(2) oral literacy, including speaking and listening skills,
(3) print literacy, including writing and reading skills, and
Over time, some researchers have also proposed to expand this rather
“centric” perspective to include the dynamics of provider interactions, and
patient-healthcare system interactions. If the patient-healthcare system is more sensitive to low health
literacy, then health outcomes could be improved by the wide scale adoption of effective
communication strategies to mitigate its deleterious influence 57.
Health numeracy has gained increased attention as an independent,
complementary concept to health literacy because some research has suggested it
influences comprehension of disease risk, food labels, health monitoring tools and tests
(e.g., blood glucose levels), and medication adherence 53. Merging definitions from
different sources, health numeracy is defined as “the degree to which individuals have
the capacity to access, process, interpret, communicate, and act on numerical,
quantitative, graphical, biostatistical, and probabilistic health information needed to
make effective health decisions.” 58 Golbeck and colleagues 58 go on to propose four,
overlapping categories:
(1) basic – skills to identify numbers, and make sense of numerical information
that does not require any manipulation
(2) computational – ability to count, quantify, compute, use simple numerical
manipulations
(3) analytical – the ability to make sense of through inference, estimation,
(4) statistical – the ability to understand probability statements, critically analyze
quantitative health information, and understand concepts such as
“randomization”
According to the National Assessment of Health Literacy 59, 36% of United States
adults have limited health literacy, 22% have only basic health literacy, and 14% have
below basic health literacy. Across 85 empirical studies examining health literacy,
prevalence of low health literacy was 26% [95% CI: 22%, 29%], and prevalence of
marginal health literacy was 20% [95% CI: 16%, 23%] 60. Salient to osteoporosis
research is the finding that age is strongly, negatively associated with health literacy
and numeracy skills 61.
Health literacy/numeracy and health outcomes. A review of health
literacy/numeracy on health outcomes included 98 articles on health literacy, 22 articles
examining health numeracy, and 9 studies measuring both literacy and numeracy 53.
Results revealed that low health literacy was consistently associated with greater
emergency room admissions and hospitalization, lower use of evidence-based
preventive services (e.g., mammography screenings and flu vaccines), lower
medication adherence, poorer ability to interpret labels and health messages, and
poorer overall health status and higher mortality rates among aging adults. Salient to
this study, no attempt was made to isolate the effect of health literacy on exercise
between health literacy and health behaviors in general, was deemed low and/or
insufficient because there were too few studies to confidently calculate an effect 53.
Regarding the relationship between health numeracy and health outcomes, there
were often too few studies to conduct a meta-analytic review, and when analyses were
conducted (e.g., asthma management, healthcare utilization), the results were generally
inconclusive. Furthermore, the authors noted the low or poor quality of many studies,
specifically citing that most studies used cross-sectional designs, often had small
sample sizes, used convenience samples, and many relied unadjusted analyses.
While research examining the relationship between health literacy/numeracy and
health outcomes continues to be important, there is also need to better understand the
mechanism(s) by which health literacy/numeracy effects health outcomes62-64.
Paasche-Orlow & Wolf63 proposed a model by which intrinsic self-care factors of patients (i.e.,
knowledge, skills, self-efficacy, problem-solving, motivation) mediate the relationship
between health literacy and health outcomes. von Wagner and colleagues64 use
aspects of various theories within health psychology (e.g, health belief model, theory of
planned behavior, transtheoretical model) expand to further expand the original model
by separating Paasche-Orolow’s intrinsic self-care factors into two distinct phases:
motivational and volitional. Motivational phase includes the ability of health literacy to
influence knowledge, understanding, beliefs, and attitudes. The volitional phase (also
called action control) focuses on the ability of health literacy to influence implementation
support for the von Wagner et al. model has been demonstrated through a recent
literature review focusing on the association between health literacy and diabetes
self-management behaviors62. Although no similar review was identified specifically for
osteoporosis self-management or physical activity, Fransen et al.62 provide insight into
the value of von Wagner’s model, and provides empirical support for the importance of
examining the relationship between health literacy/numeracy and psychosocial
constructs known to influence health behaviors.
Health literacy/numeracy and musculoskeletal health. Loke et al. 65 reviewed 8
studies examining health literacy and health outcomes among patients with
musculoskeletal disease. Four studies (50%) focused on patients with arthritis, and four
(50%) failed to distinguish patient diagnosis. None explicitly examined patients at risk
for osteopenia/osteoporosis. The authors concluded there was no consistent
relationship between health literacy and disease-specific outcome measures in patients
with chronic musculoskeletal conditions. Similar to the Berkman et al. 53 review,
however, the authors commented on the poor methodological quality of the studies
included in the review. Specifically, the majority of studies were cross-sectional in
design, contained low sample sizes, and several combined patients with various
musculoskeletal diagnoses. Thus, relevant to this study, there is little evidence to
support a relationship between health literacy/numeracy and health outcomes for
Health Literacy/Numeracy and Exercise Behavior. Few studies have examined
the relationship between health literacy/numeracy and exercise behavior. In their
review, Berkman et al. 53 identified only five studies examining health literacy and health
behaviors (e.g., grouping together healthy eating habits, exercise, and seat belt use),
and only one study examining health numeracy and health behaviors.
A systematic literature review conducted for the purposes of this thesis (See
Appendix C) 66-82 identified 17 studies that (a) directly measured health literacy and/or
health numeracy, (b) assessed physical activity/exercise behavior, and (c) presented
statistical analysis examining the relationship between these variables. Of these, 11
were cross-sectional, 2 were longitudinal (without randomization), and 4 were
secondary data analyses from randomized controlled trials intended to change physical
activity behavior. Furthermore, 82.3% (14/17) measured only health literacy, 1/17
measured only health numeracy, 1/17 measured both health literacy and health
numeracy, separately, and 1/17 used a combined measure of health literacy and
numeracy. Thus, while the research examining the relationship between health literacy
and exercise behavior is growing, there is extremely little empirical research for:
(a) the relationship between health numeracy and exercise behavior,
(b) the unique influence of health literacy and health numeracy on exercise
behavior,
(c) the interactive influence of these constructs on exercise behavior.
Among the cross-sectional studies examining health literacy, 55.6% (5/9) found
a statistically significant positive relationship between health literacy and physical
activity, and 11% (1/9) revealed a negative relationship between health literacy and
physical activity. The single cross-sectional study examining health numeracy, showed
no relationship with physical activity behavior.
In three cross-sectional studies 72,73,76, authors examined theoretical frameworks
proposing that knowledge mediates the relationship between health literacy and
self-management behaviors 60,62,83. Of these, two reported that the relationship between
health literacy and physical activity was not mediated by knowledge 73,76.
Both studies utilizing longitudinal (non-randomized designs), found a small but
statistically significant relationship between health literacy and physical activity behavior
77,84. Only one of these studies employed multivariate mediation methods, and found
that the health literacy-physical activity relationship was mediated by self-efficacy 77.
Finally, four randomized controlled trials examined the heterogeneity of treatment
effects due to health literacy on intervention-induced changes to physical activity
behavior. While none of these studies revealed heterogeneity of treatment effects due
to health literacy 79-82, it is important to note that several of these studies varied in
quality, limited by small sample sizes and poor reporting of statistical methodology.
In conclusion, while low health literacy has consistently been associated with
hospitalization, lower use of evidence-based preventive services, lower medication
adherence, poorer ability to interpret labels and health messages, and poorer overall
health status and higher mortality rates among elderly adults), there is insufficient
evidence to support a relationship between health literacy and bone health outcomes or
physical activity behavior, specifically. Furthermore, even less empirical evidence is
available to understand the role of low health numeracy for general health outcomes,
musculoskeletal disease, osteoporosis, or exercise behavior.
PURPOSE AND HYPOTHESES
Due to the complexity of osteoporosis self-management regimens, the
importance of physical activity behavior in sustaining and increasing BMD, and the lack
of research examining the role of health literacy/numeracy in osteoporosis
self-management and specifically for physical activity behavior, the purpose of this study is
to examine the heterogeneity of treatment effects due to of health literacy/numeracy on
post-intervention exercise self-efficacy and exercise behavior among older adults
enrolled in a large, multi-site randomized controlled trial designed to increase
osteoporosis guideline concordant care. Specific research objectives, with
corresponding hypotheses are:
Research Objective 1: To determine whether there is variation in exercise behavior
the dependent variable (exercise behavior) will be assessed using both a continuous
and a categorical measure of exercise behavior.
Hypothesis H1.A.1. Compared to the high health literacy group, the low health
literacy group will have a lower levels of exercise behavior at baseline and at
12-week follow-up time-points.
Hypothesis H1.A.2. Compared to the high health literacy group, the low health
literacy group will have a lower proportion of individuals with exercise behaviors
that are consistent with National Osteoporosis Foundation exercise guidelines at
baseline and at 12-week follow-up time-points.
Hypothesis H1.B.1. Compared to the high numeracy ability group, the low health
numeracy ability group will have a lower levels of exercise behavior at baseline
and at 12-week follow-up time-points.
Hypothesis H1.B.2. Compared to the high numeracy ability group, the low health
numeracy ability group will have a lower proportion of individuals with exercise
behaviors that are consistent with National Osteoporosis Foundation exercise
Hypothesis H1.C.1. Compared to the high preference for numerical display
group, the low preference for numerical display group will have a lower levels of
exercise behavior at baseline and at 12-week follow-up time-points.
Hypothesis H1.C.2. Compared to the high preference for numerical display
group, the low preference for numerical display group will have a lower
proportion of individuals with exercise behaviors that are consistent with National
Osteoporosis Foundation exercise guidelines at baseline and at 12-week
follow-up time-points.
Research Objective 2: To determine whether there is variation in exercise self-efficacy
across high and low levels of health literacy/numeracy. For each of these hypotheses,
the dependent variable (exercise self-efficacy) will be assessed using a continuous
measure.
Hypothesis H2.A. Compared to the high health literacy group, the low health
literacy group will have a lower levels of exercise self-efficacy at baseline and at
12-week follow-up time-points.
Hypothesis H2.B. Compared to the high numeracy ability group, the low
numeracy ability group will have a lower levels of exercise self-efficacy at
Hypothesis H2.C. Compared to the high preference for numeric display group,
the low preference for numeric display group will have a lower levels of exercise
self-efficacy at baseline and at 12-week follow-up time-points.
Research Objective 3: Pending the identification of the hypothesized difference for
exercise behavior across low and high levels of health literacy/numeracy (Research
Objective 1), research objective three is to test whether level of health literacy/numeracy
results in heterogeneity of treatment effects for exercise behavior outcomes. Each
analysis will be conducted for the pooled sample, as well as for each treatment site (i.e.,
University of Iowa, University of Alabama Birmingham, and Kaiser Permanente,
Georgia).
Hypothesis H3.A.1. Heterogeneity of treatment effects will be evident across high
and low levels of health literacy for 12-week exercise behavior. Specifically,
individuals with low health literacy in the control group will have the lowest levels
of exercise behavior, compared to individuals with low health literacy in the
treatment group, and compared to individuals with high health literacy
(regardless of treatment condition).
Hypothesis H3.A.2. Heterogeneity of treatment effects will be evident across high
and low levels of health literacy for meeting exercise recommendations at
12-week follow-up. Specifically, individuals with low health literacy in the control
are consistent with National Osteoporosis Foundation guidelines, compared to
individuals with low health literacy in the treatment group, and compared to
individuals with high health literacy (regardless of treatment condition).
Hypothesis H3.B.1. Heterogeneity of treatment effects will be evident across high
and low levels of numeracy ability for 12-week exercise behavior. Specifically,
individuals with low numeracy ability in the control group will have the lowest
levels of exercise behavior, compared to individuals with low numeracy ability in
the treatment group, and compared to individuals with high numeracy ability
(regardless of treatment condition).
Hypothesis H3.B.2. Heterogeneity of treatment effects will be evident across high
and low levels of numeracy ability for exercise behaviors that are consistent with
exercise recommendations at 12-week follow-up. Specifically, individuals with
low numeracy ability in the control group will have the lowest proportion of
individuals with exercise behaviors that are consistent with National Osteoporosis
Foundation guidelines for exercise behavior, compared to individuals with low
numeracy ability in the treatment group, and compared to individuals with high
numeracy ability (regardless of treatment condition).
Hypothesis H3.C.1. Heterogeneity of treatment effects will be evident across high
and low levels of preference for numerical display for 12-week exercise behavior.
group will have the lowest levels of exercise behavior, compared to individuals
with low preference for numerical display in the treatment group, and compared
to individuals with high preference for numerical display (regardless of treatment
condition).
Hypothesis H3.C.2. Heterogeneity of treatment effects will be evident across high
and low levels of preference for numerical display for exercise behaviors that are
consistent with exercise recommendations at 12-week follow-up. Specifically,
individuals with low preference for numerical display in the control group will have
the lowest proportion of individuals reporting exercise behaviors that are
consistent with National Osteoporosis Foundation guidelines for exercise
behavior, compared to individuals with low preference for numerical display in the
treatment group, and compared to individuals with high preference for numerical
display (regardless of treatment condition).
Research Objective 4: Pending the identification of the hypothesized difference for
exercise self-efficacy across low and high levels of health literacy/numeracy (Research
Objective 2), research objective four is to test whether level of health literacy/numeracy
results in heterogeneity of treatment effects for 12-week self-efficacy outcomes. Each
analysis will be conducted for the pooled sample, as well as for each treatment site (i.e.,
University of Iowa, University of Alabama Birmingham, and Kaiser Permanente,
Hypothesis H4.A. Heterogeneity of treatment effects will be evident across high
and low levels of health literacy for 12-week exercise self-efficacy. Specifically,
individuals in the control group with low health literacy will report the lowest levels
of exercise self-efficacy, compared to individuals in the control group with high
health literacy and compared to individuals in the treatment group (regardless of
health literacy level).
Hypothesis H4.B. Heterogeneity of treatment effects will be evident across high
and low levels of numeracy ability for 12-week exercise self-efficacy. Specifically,
individuals in the control group with low numeracy ability will report the lowest
levels of exercise self-efficacy, compared to individuals in the control group with
high numeracy ability and compared to individuals in the treatment group
(regardless of numeracy ability level).
Hypothesis H4.C. Heterogeneity of treatment effects will be evident across high
and low levels of preference for numerical display for 12-week exercise
self-efficacy. Specifically, individuals in the control group with low preference for
numerical display will report the lowest levels of exercise self-efficacy, compared
to individuals in the control group with high preference for numerical display and
compared to individuals in the treatment group (regardless of preference of
METHODS AND PROCEDURES
Description of the Data. Data for this study was obtained from the Patient
Activation After DXA Notification (PAADRN; ClinicalTrials.gov identifier: NCT01507662)
study 85. PAADRN was designed to be a pragmatic, scalable intervention targeting
adults undergoing DXA screening for osteoporosis within three sites located in Iowa,
Georgia, and Alabama. The primary intervention modality was a printed mailing 86,
designed to better communicate patient-specific:
a) risk status for osteopenia/osteoporosis using DXA,
b) risk status for fracture risk status using FRAX score, and
c) promote actions that reduce risk of fracture and sustain bone health (e.g.,
medication options, physical activity, and dietary change).
Consistent with the goals of pragmatic clinical trials, exclusion criteria for the
original trial were minimal, such that only those with the inability to ready or speak
English, prisoners, and individuals with substantial mental, visual, or auditory
impairments were excluded from participation. Eligible participants were patients at
participating clinical sites, scheduled for bone density scans 85,86.
Protection of human subjects. The primary PAADRN intervention originally
received approval by Institutional Review Boards at University of Iowa (organizing site),
Institutional Review Board at Georgia State University approved this study, a secondary
analysis of the PAADRN data. Informed consent was attained within the original study
protocols, and all data were managed and secured by the PAADRN research staff at
University of Iowa, per the human subjects protocols. Consistent with the PAADRN
steering committee’s processes and procedures, a research proposal containing
detailed research questions, specific variables being requested, analysis protocols, and
hypotheses were submitted for approval before analysis began.
Measures
Covariates. Baseline interviews at the time of the DXA screening were used to
assess the demographic variables gender (male or female), race (white or minority),
age (< 65 years, 65-75 years, and 75 years or older) and education level (≤ high
school/GED, some college/4-year degree, and some graduate school). Health
behaviors that were assessed included drinking any alcohol (yes or no), and being a
former smoker (yes or no) or current smoker (yes or no). The following bone health risk
factors were also assessed: Frax risk score (low risk, moderate risk, and high risk), past
diagnosis of osteopenia (yes or no) or osteoporosis (yes or no), having a prior bone
density scan (yes or no), having a prior hip fracture (yes or no), and currently or formerly
on medication for bone health (yes or no). Finally, having comorbid chronic health
conditions such as chronic obstructive pulmonary disease (yes or no), depression (yes
Health Literacy. The Single Item Literacy Screener 87 was used to assess
perceived health literacy. Using a 5-point Likert-type scale (1-Always, 2-Often,
3-Sometimes, 4-Rarely, and 5-Never), each participant answered the question “How often
do you need to have someone help you when you read instructions, pamphlets, or other
written material from your doctor or pharmacy?” Lower scores are indicative of lower
perceived health literacy. This 1-item tool has been validated 87 using the Short Test of
Functional Health Literacy in Adults 88,89. The recommended cut-off for defining low
health literacy is ≤ 3. For this study, two categories (high and low health literacy) were
created using this method.
Health Numeracy. The Subjective Numeracy Scale 90,91 was used to assess two
facets of health numeracy; numeric ability and preference for display of numeric
information. This instrument has been validated using objective numeracy tests and has
been shown to predict disease risk comprehension 90,91. Four items assessed numeracy
ability on a 6-point Likert-type scale with endpoints “Not at all good” (1) and “Extremely
good” (6). Internal consistency (Cronbach’s alpha) for the numeric ability subscale in
this study was good (α = 0.89). Scores for the four items are averaged with lower scores
indicative of lower numeric ability 92. The mean numeric ability score was used to create
a dichotomous variable (high and low numeracy ability) for the purposes of regression.
Four items assessed preference for display of numeric information on a 6-point
Likert-type scale. After reverse coding the necessary item, the mean preference for
for numerical display 92. Internal consistency (Cronbach’s alpha) for preference for
numerical display in this study was weak (α = 0.62). Consistent with methods for
numeracy ability, the mean score was used to create a dichotomous variable (high and
low preference for numeric display) for the purposes of regression analysis.
Exercise Behavior. Based on the Behavioral Risk Factor Surveillance System 93
weight-bearing aerobic and resistance/strength exercise behaviors were assessed.
Specifically for weight-bearing aerobic exercise, participants were asked “In the past 30
days, how many times per week were you engaged in aerobic activity? (This includes
walking, hiking, jogging, aerobic classes or video, stair climbing, elliptical machine,
dancing, and biking (not on a stationary bike). Please DO NOT include swimming.”
Possible response options included: none, 1-2 times per week, 3-4 times per week, and
5 or more times per week. Using the same response options strength training exercise
was assessed by asking “In the past 30 days, how many times per week were you
engaged in strength training? (This includes lifting weights, using elastic or resistance
bands, lifting your own weight (push-up or crunches), using weight machines, Pilates
and yoga.)”
Responses were then used to create two exercise variables. First, weighted
scores were assigned to each response option (See Table 1), allowing the creation of a
single continuous exercise variable, which combines weight-bearing and resistance
exercise on a scale from 0 (completely sedentary) to 10 (performs aerobic and
dichotomous variable was created (<5: consistent with National Osteoporosis
Foundation recommendations for exercise; ≥5: inconsistent with National Osteoporosis
Foundation recommendations for exercise).
Exercise Self-Efficacy. The Osteoporosis Self-Efficacy Scale 94 contains 10 items
assessing confidence to exercise. Responses were assessed on a 10-point Likert-type
scale, anchored by “not at all confident” (1) to “very confident” (10). Mean scores are
calculated, with higher scores indicative of greater self-efficacy for exercise. Internal
consistency (Cronbach’s alpha) of the scale within this study at baseline (α = 0.97) and
12-week (α = 0.97) follow-up was excellent.
Statistical Analysis
A subset of the PAADRN cohort, containing only individuals with complete data
for treatment, dependent, and moderating variables was created (N = 6591; 85.1% of
original PAADRN sample size). The analytic approach was consistent with the PAADRN
primary outcomes papers85,86. Statistical analysis began by examining whether there
were differences between treatment and control groups for baseline demographics and
relevant covariates. Normality of continuous variables was assessed using the
Kolmogorov-Smirnov statistic. For normally distributed continuous variables,
independent sample t-tests were conducted, using pooled or Satterthwaite statistics, as
indicated by the equality of variances test. For non-normally distributed continuous
variables, chi-square analyses were conducted. For ordinal categorical variables with
more than two categories, the Mantel-Haenszel chi-square was computed.
Second, the following three sets of unadjusted pairwise comparisons were
conducted to better understand the role of treatment group, sociodemographic
variables, and proposed moderators on exercise self-efficacy and behavior:
(1) differences in baseline and 12-week exercise behavior and exercise
self-efficacy by each study covariate,
(2) differences in baseline and 12-week exercise behavior and exercise
self-efficacy were examined within each covariate sub-category, and
(3) differences in exercise self-efficacy and behavior change by each study
covariate.
For continuous outcome variables, this analysis used independent samples and paired
t-tests, as appropriate. For the dichotomous exercise outcome variable (meets/does not
meet recommendations), chi-square analyses were conducted, and generalized linear
models with Tukey’s post hoc tests were used when covariates had more than two
categories.
Third, Pearson correlations were conducted among the study’s independent,
dependent and proposed moderating variables. Finally, generalized linear mixed
models were used to conduct unadjusted and adjusted examinations of the moderating
categories: low vs. high numeracy ability; 2 categories: low vs. high preference for
numerical display) on post-intervention exercise self-efficacy and exercise behavior.
Conceptually, the moderation analysis was guided by the Baron and Kenny95
model (See Figure 1). When the effect of the intervention arm on exercise behavior
(path a) is statistically significant, and the effect of health literacy (or health numeracy)
on exercise behavior (path b) is statistically significant, moderation exists when the
interaction of intervention arm and health literacy (or numeracy; path c) are entered into
the model and found to be statistically significant. Thus, there is a moderating effect
when the interaction of the treatment arm and health literacy (or numeracy) significantly
changes the strength or direction of the intervention effect on exercise
behavior/self-efficacy (path a’).
Analytically, two linear mixed models using PROC GLIMMIX in SAS (version 9.4)
were conducted to test for moderation, according to the Baron and Kenny method. The
reduced model included the 12-week exercise behavior variable served as the
dependent variable, and treatment group (2 categories: treatment vs. control), literacy
(or numeracy) variable (2 categories: high vs. low), and the treatment by moderating
variable interaction (See Figure 1) were included in the model, while controlling for
baseline exercise behavior/self-efficacy. The full model included the independent and
dependent variables as described above for the reduced model but also included the
following covariates: age (3 groups), gender, race, education, COPD, depression,
self-reported health status (5 categories), receiving prior DXA, history of osteoporosis,
history of osteoporosis treatment, glucocorticoids use, bone density risk (3 categories:
normal, low, osteoporosis), study site, lowest t-score, and 10-year FRAX score. This
analytical method was also conducted using 12-week exercise self-efficacy as the
dependent variable, controlling for baseline exercise self-efficacy. Furthermore,
consistent with the PAADRN primary outcomes papers, full and reduced regression
models were used to assess the pooled effect (including all three study sites), as well as
the site-specific effect.
Results
Due to missing data for key covariates, participant numbers included in the
analysis for reduced and full models will vary. When examining differences for
covariates by treatment group (See Table 2), results showed that the control group had
significantly greater numbers of individuals reporting breast cancer diagnosis (χ2 =
45.60, df = 2, p < 0.001), more individuals reporting past diagnosis of osteoporosis (χ2 =
10.99, df = 2, p = 0.004), and treatment for osteoporosis (χ2 = 4.43, df = 1, p = 0.04).
Based on DXA results, there were fewer individuals in the control group diagnosed as
‘normal’ bone health (χ2 = 17.06, df = 1, p < 0.001). Individuals in the control group had
significantly lower t-scores for bone mineral density (z = -4.27, p < 0.001), and
Research Objective 1. Results of all pairwise comparisons, conducted for the first
two research objectives are displayed in Tables 3 and 4. There is sufficient evidence to
reject the null hypothesis that high and low health literacy groups have equal levels of
exercise at baseline and 12-week time-points (Hypothesis H1.A.1, See Table 3).
Therefore, compared to individuals in the high health literacy group, individuals in the
low health literacy group have lower levels of exercise at baseline (t = -4.01, df = 6589,
p < 0.001) and 12-week follow-up (t = -4.22, df = 6589, p < 0.001). There was no
difference between high and low health literacy groups for change in exercise behavior
(t = -0.30, p = 0.77; Cohen’s d = 0.011).
Similarly, there is sufficient evidence to reject the null hypothesis that high and
low health literacy groups have equal proportions of individuals exercising consistent
with National Osteoporosis recommendation (Hypothesis H1.A.2, See Table 3).
Compared to those with high health literacy, there are a lower proportion of individuals
with low health literacy exercising at a level consistent with National Osteoporosis
Foundation recommendations at baseline (χ2 = 5.91, df = 1, p = 0.02) and at 12-week
follow-up (χ2 = 5.00, df = 1, p = 0.03).
For numeracy ability, there is sufficient evidence to reject the null hypothesis that
compared to those with high numeric ability, individuals with low numeric ability have
lower levels of exercise at baseline and 12-week follow-up (Hypothesis H1.B.1, See
Table 3). Compared to individuals with high numeric ability, individuals with low numeric
and 12-week follow-up (t = -8.79, df = 6589, p < 0.001). There was no difference
between high and low numeric ability groups for change in exercise behavior (t = -0.29,
df = 6589, p = 0.77; Cohen’s d = -0.048).
Similarly, there is sufficient statistical evidence to reject the null hypothesis that
high and low numeric ability groups have equal proportions of individuals exercising
consistent with National Osteoporosis recommendation (Hypothesis H1.B.2, See Table
3). Compared to the high numeric ability group, the low numeric ability group had a
lower proportion of individuals exercising at a level consistent with National
Osteoporosis Foundation recommendations at baseline (χ2 = 32.43, df = 1, p < 0.001)
and at 12-week follow-up (χ2 = 42.24, df = 1, p < 0.001).
Finally, for preference for numerical display, there is sufficient evidence to reject
the null hypothesis that compared to those with high preference for numeric display,
individuals with low preference for numeric display have lower levels of exercise at
baseline and 12-week follow-up (Hypothesis H1.C.1, See Table 3). Results revealed
that individuals with low preference for numerical display have lower levels of exercise
behaviors at baseline (t = 7.28, df = 1699.6, p < 0.001) and 12week followup (t =
-8.79, df = 1676.5, p < 0.001). There was no difference between high and low preference
for numeric display groups for change in exercise behavior (t = -1.43, p = 0.15; Cohen’s
Additionally, there is sufficient statistical evidence to reject the null hypothesis
that high and low preference for numeric display groups have equal proportions of
individuals exercising consistent with National Osteoporosis recommendation
(Hypothesis H1.C.2, See Table 3). Compared to those with high preference for
numerical display, a lower proportion of individuals with low preference for numerical
display are exercising at a level consistent with National Osteoporosis Foundation
recommendations at baseline (χ2 = 29.27, df = 1, p < 0.001) and at 12-week follow-up
(χ2 = 43.27, df = 1, p < 0.001).
Research Objective 2. Regarding self-efficacy for exercise, there is sufficient
statistical evidence to reject the null hypothesis that compared to those with high health
literacy, individuals with low health literacy have lower levels of exercise self-efficacy at
baseline and 12-week follow-up (Hypothesis H2.A, See Table 4). Compared to
individuals with high health literacy, individuals with low health literacy had lower levels
of exercise self-efficacy at baseline (t = -7.71, df = 1380.6, p < 0.001) and 12-week
follow-up (t = -7.50, df = 1406.2, p < 0.001). There was no difference between high and
low health literacy groups for change in exercise behavior (t = 0.42, df = 1364.3, p =
0.67; Cohen’s d = 0.010).
There is sufficient statistical evidence to reject the null hypothesis that compared to
those with high numeric ability, individuals with low numeric ability have lower levels of
exercise self-efficacy at baseline and 12-week follow-up (Hypothesis H2.B, See Table
baseline (t = -12.85, df = 1738.4, p < 0.001) and 12-week follow-up (t = -10.08, df =
1815.1, p < 0.001). A statistically significant difference between high and low numeric
ability groups for change in exercise self-efficacy was revealed (t = 3.45, df = 1680.1, p
< 0.001; Cohen’s d = 0.125). Individuals with high numeric ability decreased in
self-reported exercise self-efficacy (mean change = -0.10, sd = 1.74; p < 0.001) while
individuals with low numeric ability increased in self-reported exercise self-efficacy
(mean change = 0.13, sd = 2.24; p = 0.04).
There is sufficient statistical evidence to reject the null hypothesis that compared to
those with high preference for numeric display, individuals with low preference for
numeric display have lower levels of exercise self-efficacy at baseline and 12-week
follow-up (Hypothesis H2.C, See Table 4). Those with low preference for numerical
display had lower levels of exercise self-efficacy at baseline (t = -11.71, df = 1456.2, p <
0.001) and 12-week follow-up (t = -8.84, df = 1510.5, 1406.2, p < 0.001). There was,
however, a statistically significant difference between high and low preference for
numerical display groups for change in self-reported self-efficacy (t = 3.63, df = 1443.8,
p < 0.001; Cohen’s d = 0.125). Individuals with high preference for numeric display
decreased in self-reported self-efficacy (mean change = -0.10, sd = 1.78; p < 0.001)
while individuals with low preference for numeric display increased in self-efficacy
(mean change = 0.15, sd = 2.19; p = 0.02).
Research Objective 3. Reduced linear mixed models (without covariates)
exercise behavior for the entire sample (See Table 7; n = 6591, t = 2.23, p = 0.03), as
well as University of Iowa (n = 1532, t = 2.07, p = 0.04), and the University of Alabama,
Birmingham (n = 2714, t = 2.56, p = 0.01) samples. This effect did not remain
statistically significant, however, in the full models containing covariates (pooled: n =
6542, t = 0.39, p = 0.70; University of Iowa: n = 1516, t = 0.76, p = 0.45; University of
Alabama, Birmingham: n = 2698, t = 1.55, p = 0.12). Furthermore, there is insufficient
evidence to reject the null hypothesis that there is no evidence for heterogeneity of
treatment effects across high and low levels of health literacy for 12-week exercise
behavior (Hypothesis H3.A.1, See Table 7). Full models (including covariates) revealed
no heterogeneity of treatment effects of health literacy on 12-week exercise behavior
(full model, pooled effect: n = 6591, t = -0.73, p = 0.47; full model, University of
Alabama, Birmingham only: n = 2698, t = -0.35, p = 0.72; full model, Kaiser
Permanente, Georgia only: n = 2328, t = -0.03, p = 0.98; full model, University of Iowa
only: n = 1516, t = -0.98, p = 0.33). Covariates that were significantly associated with
12-week follow-up exercise behavior in pooled analyses (n = 6542) included:
self-reported health status (t = -8.13, p < 0.001), depression (t = -3.64, p < 0.001), being a
current smoker (t = -2.46, p = 0.01), using alcohol (t = 2.71, p = 0.006), having some
graduate school (t = 4.73, p < 0.001), and being male (t = 4.16, p < 0.001).
Furthermore, there is insufficient statistical evidence to reject the null hypothesis
that there is no evidence for heterogeneity of treatment effects across high and low
levels of health literacy for exercising at a level consistent with National Osteoporosis
was no association between health literacy and exercising at levels consistent with
National Osteoporosis Foundation recommendations for exercise behavior in the
reduced model (pooled: n = 6591, t = 1.28, p = 0.20; University of Iowa: n = 1532, t =
1.54, p = 0.12; University of Alabama, Birmingham: n = 2714, t = 1.08, p = 0.28; Kaiser
Permanente, Georgia: n = 2345, t = -0.65, p = 0.51), or the full model with covariates
(pooled: n = 6542, t = -0.57, p = 0.57; University of Iowa: n = 1516, t = 0.37, p = 0.71;
University of Alabama, Birmingham: n = 2698, t = 0.17, p = 0.87; Kaiser Permanente,
Georgia: n = 2328, t = -1.45, p = 0.14). Covariates that were significantly associated
with exercising at levels consistent with National Osteoporosis Foundation
recommendations at 12-week follow-up in pooled analyses (n = 6542) included:
self-reported health status (t = -9.20, p < 0.001), depression (t = -2.78, p =0.01), being a
current smoker (t = -2.21, p = 0.03), using alcohol (t = 3.60, p < 0.001), having some
graduate school (t = 4.06, p < 0.001), and being male (t = 3.82, p < 0.001), being on
osteoporosis medications in the past (t = 2.34, p = 0.02), and being above 75 years (t =
-3.35, p < 0.001).
While reduced mixed models (without covariates) revealed a significant positive
relationship between preference for numerical display and 12-week continuous exercise
behavior for the total sample (See Table 8a; reduced model, pooled effect: n = 6591, t =
3.46, p < 0.001), as well as site-specific effects for University of Alabama, Birmingham
(n = 2714, t = 2.77, p = 0.006) and Kaiser Permanente, Georgia (n = 2345, t = 1.72, p =
0.08). These associations were no longer significant, in the full models with covariates
University of Alabama, Birmingham only: n = 2698, t = 1.25, p = 0.21; full model, Kaiser
Permanente, Georgia only: n = 2328, t = 0.58, p = 0.56). Additionally, there is
insufficient statistical evidence to reject the null hypothesis that there is no evidence for
heterogeneity of treatment effects across high and low levels of preference for
numerical display for 12-week exercise behavior (Hypothesis H3.C.1, See Table 8a).
Full models (including covariates) revealed no heterogeneity of treatment effects of
preference for numerical display on 12-week exercise behavior (full model, pooled
effect: n = 6542, t = 0.61, p = 0.55; full model, University of Alabama, Birmingham only:
n = 2698, t = -0.14, p = 0.89; full model, Kaiser Permanente, Georgia only: n = 2328, t =
0.46, p = 0.65). Covariates that were significantly associated with exercise behavior at
12-week follow-up in pooled analyses (n = 6542) included: self-reported health status (t
= -8.01, p < 0.001), depression (t = -3.59, p < 0.001), being a current smoker (t = -2.49,
p = 0.01), using alcohol (t = 2.58, p = 0.01), having some graduate school (t = 4.53, p <
0.001), and being male (t = 4.03, p < 0.001), and being above 75 years (t = -3.15, p =
0.002).
Similar to the results for 12-week exercise behavior, the reduced model (without
covariates) revealed a significant, positive association between preference for numerical
display and exercising at levels consistent with the National Osteoporosis Foundation
recommendations for exercise at 12-week follow-up (See Table 8a; pooled: n = 6591, t
= 2.94, p = 0.003, University of Iowa: n = 1532, t = 1.38, p = 0.17; University of
Alabama, Birmingham: n = 2714, t = 1.40, p = 0.16, Kaiser Permanente, Georgia: n =