Trends
in
advanced
breast
cancer
incidence
rates
after
implementation
of
a
mammography
screening
program
in
a
German
population
Alexandra
Simbrich
a,
Ina
Wellmann
a,
Jan
Heidrich
b,
Oliver
Heidinger
b,
Hans-Werner
Hense
a,b,*
aInstituteofEpidemiologyandSocialMedicine,UniversityofMünster,Germany b
EpidemiologicalCancerRegistryNorthRhine-Westphalia,Münster,Germany
ARTICLE INFO Articlehistory: Received5May2016
Receivedinrevisedform4July2016 Accepted14July2016
Availableonline25July2016
ABSTRACT
Background:Mammographyscreeningprograms(MSPs)aimtodetectearly-stagebreastcancersinorder todecreasetheincidenceofadvanced-stagebreastcancersandtoreducebreastcancermortality.We analyzedthetimetrendsofadvanced-stagebreastcancerincidenceratesinthetargetpopulationbefore andafterimplementationoftheMSPinaregionofnorthwesternGermany.
Methods:TheMSPintheMünsterdistrictstartedinOctober2005.Atotalof13,874womenwithan incidentinvasivebreastcancer(BC)wasidentifiedbythepopulation-basedepidemiologicalcancer registrybetween2000and2013inthetargetgroup50–69years.Multipleimputationmethodswere usedtoreplacemissingdataontumorstages(10.4%).Theincidenceratesforearly-stage(UICCI)and advanced-stage(UICCII+)BCweredetermined,andPoissonregressionanalyseswereperformedto assesstrendsovertime.
Results:TheincidenceratesforUICCIbreastcancersincreasedduringthestep-upintroductionofthe MSPandremainedelevatedthereafter.Bycontrast,afterincreasingfrom2006to2008,theincidence rates of UICC II+ breast cancersdecreased to levelsbelow the pre-screening period. Significantly decreasingUICCII+incidencerateswerelimitedtotheagegroup55–69yearsandreachedlevelsthat weresignificantlylowerthanincidenceratesinthepre-screeningperiod.
Discussion:Theincidence ratesofadvanced-stagebreastcancersdecreasedintheagegroups from 55yearstotheupperagelimitforscreeningeligibility,butnotintheadjacentagegroups.Thefindings areconsistentwithMSPleadtimeeffectsandseemtoindicatethattheMSPlowersadvanced-stage breastcancerratesinthetargetpopulation.
ã2016TheAuthors.PublishedbyElsevierLtd.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1.Introduction
Invasivebreastcancer(ICD10:C50)isthemostcommoncancer amongwomen in Germany,withover 70,000newly diagnosed casesandover17,000deathsin2010[1].Stageofbreastcancerat diagnosisisassociatedwithcancersurvival,aspatientswith early-stagebreastcancersclearlyshowhighersurvivalratesthanthose withadvanced-stage breast cancers[2,3].Therefore, systematic mammographyscreeningprograms(MSP)havebeenintroduced intoroutinemedicalcareinmanycountries[4]withtheaimof detectingbreastcancerinitsearlystageswhichmaybetreated more successfully. As a result, a decrease in the incidence of advanced-stagebreastcancersisassumedtoheraldasubsequent
reductioninbreastcancermortalityinthegroupofwomeneligible forscreening[5].
However, recent studies have produced very controversial resultswithregardtotheincidenceratesofadvancedstagesof breast cancer following the implementation of mammography screening programs; indications of declining late-stage breast cancersreportedbysomeauthors[6–10]werenotconfirmedby others[11–14].InGermany,theMSPstartedin2005andtargets the population of all resident women aged between 50 and 69yearswithbiennialinvitations.Theprogramisorganizedinline with the European Guidelines for Quality Assurance in Breast CancerScreeningandDiagnosis[15].
The aim of this study was to estimate the changes in the incidenceofadvanced-stagebreastcancersinthetarget popula-tionbeforeandafterthestartoftheMSPinanorthwesternregion ofGermany(theMünsterdistrict).
*Corresponding author at: Institute of Epidemiology and Social Medicine, UniversityofMünster,Germany.
E-mailaddress:[email protected](H.-W.Hense). http://dx.doi.org/10.1016/j.canep.2016.07.006
1877-7821/ã2016TheAuthors.PublishedbyElsevierLtd.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/). ContentslistsavailableatScienceDirect
Cancer
Epidemiology
The
International
Journal
of
Cancer
Epidemiology,
Detection,
and
Prevention
j o u r n a l h o m e p a g e : w w w . c a n c e r e p i d e m i o l o g y. n e t2.Materialandmethods
2.1.Datasource
The German MSP adheres to the European Guidelines for QualityAssuranceinBreastCancerScreeningandDiagnosis[15]. Accordingly, the target population includes women aged 50– 69yearswhoareinvitedbiannually.Inallstudycenters,two-view mammogramswereobtainedusingfull-fielddigital mammogra-phy systems. All mammograms were double-read by certified readers,andabnormalfindingsdetectedbyoneorbothreaders resultedin amandatoryconsensusmeetingwitharbitrationfor recallinvitations.
Bytheendof2005,thefirstscreeningunitsinGermanystarted mammographyscreeningservicesintheMünsterdistrictwitha populationof2.6millioninhabitants.Theprogramwasintroduced byopeningregionalscreeningunitsinastep-upmanner;theMSP was fully implemented in thedistrict by theend of 2008 and continuedwithaparticipationrateofaround55%untiltheendof thestudyperiodin 2013.Weobtainedinformationonincident femalebreastcancercasesintheyearsfrom2000to2013fromthe Epidemiological Cancer Registry of the Münster District, a subregistryofthestate-wideEpidemiologicalCancerRegistryof NorthRhine–Westphalia;theregistryhasbeencollectingdataon cancerincidencewithacompletenessofmorethan90%[1].This database,coveringalongregistrationperiod,wasusedtoassess changes in breast cancer incidence rates in response to the implementationoftheMSPinNRW.
2.2.Studypopulation
ThestudypopulationconsistedofallwomenintheMünster districtwhowerediagnosedwithincidentbreastcancerandwho wereintheagerangeeligibleformammographyscreening,thatis, aged50–69years.Toaccountfordelayedeffectsofscreeningon breast cancer incidence due to lead time, we expanded the populationtoalsoincludewomenwhowereaged70–79years.We further included women aged 45–49 years to address secular incidencechangesthatoccurredpriortotheirenteringthetarget agegroup.Thecancerregistryprovidedtumor-specific informa-tiononallnewlydiagnosedinvasivebreastcancers(ICD-10:C50) notifiedintheyears2000–2013.In-situcases(ICD-10:D05)and deathcertificateonly(DCO)caseswereexcluded.Thepopulation numberspercalendaryearwereobtainedfromtheStateStatistical Bureau(ITNRW).
Theinformationontumorsizeandlymph-nodeinvolvement(T and N stage) of each breast cancercase was used to define a dichotomized stage according to the UICC classification (early stage:UICCIandadvancedstage:UICCII+).UICCIwasassignedto tumors with a T-stage T1 (diameter 20mm)and withno or minimal lymph-node involvement (N stage=N0 or N1mic). T stages T2,T3or T4or any numberof affectedlymphnodes (N stage=N+excludingT1N1mic)werecodedasUICCII+.
2.3.Statisticalmethods 2.3.1.Imputationmethods
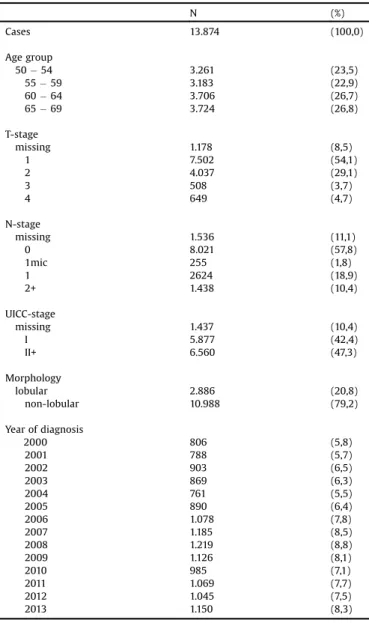
InformationonTand/orNstagewasmissingin2627(11.6%)of allbreastcancercasesaged45–79years;therewere1437(10.4%) missingcasesintheMSPtargetgroupaged50–69years(Table1). As informative data for other variables were still available for patientswithamissing UICCclassification,multipleimputation methodswereusedtofillinthemissingdata.Thevariableswith completeinformationthatcouldbeusedformultipleimputation wereageatdiagnosis,yearofdiagnosis,breastcancerdetection mode(screen-detectedor not),cancermorphology (lobular/not
lobular) and survival; grading data were also available but incomplete. A fullyconditional specification (FCS) methodwas applied,assumingtheexistenceofajointdistributionforthese variables.Themissingvaluesforthevariablesgrading,Tstage,and Nstagewerefilledinusingadiscriminantfunctionmethod[16].In theFCSmethod,themissingvaluesforallvariablesarefilledin sequentiallyoverthevariablestakenoneatatime.Inoursetting, grading was imputed first conditional on the set of complete variables,followedbyTstageandthenNstage.Themissingvalues were imputedin five runs. To assessthe efficiencyof multiple imputation,asimulationstudywascarriedout[17].In100samples
drawn from among all women with complete UICC stage
(n=12,437),each encompassinga samplingfraction of20%,the informationonTandNstagewasomittedandthenfilledupusing FCS multipleimputations.To decidewhethertheimputeddata delivered a good representation of the original data, we used Box plots and testsof equivalence. The true rates of advanced breastcancersagreedcloselywiththoseafterimputation.
Age-andstage-specificbreastcancerrates,includingimputed values,werecomputedforeachcalendaryearfrom2000to2013. Overallandstage-specificincidencerateswereage-standardized usingthenewEuropeanstandardpopulation[18].
Table1 Baselinecharacteristics. N (%) Cases 13.874 (100,0) Agegroup 50 54 55 59 60 64 65 69 3.261 3.183 3.706 3.724 (23,5) (22,9) (26,7) (26,8) T-stage missing 1 2 3 4 1.178 7.502 4.037 508 649 (8,5) (54,1) (29,1) (3,7) (4,7) N-stage missing 0 1mic 1 2+ 1.536 8.021 255 2624 1.438 (11,1) (57,8) (1,8) (18,9) (10,4) UICC-stage missing I II+ 1.437 5.877 6.560 (10,4) (42,4) (47,3) Morphology lobular non-lobular 2.886 10.988 (20,8) (79,2) Yearofdiagnosis 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 806 788 903 869 761 890 1.078 1.185 1.219 1.126 985 1.069 1.045 1.150 (5,8) (5,7) (6,5) (6,3) (5,5) (6,4) (7,8) (8,5) (8,8) (8,1) (7,1) (7,7) (7,5) (8,3)
2.3.2.Poissonregressionmodeling
In ordertomodelthetimetrendsweemployedaloglinear Poissonmodelforbreastcancerrates[19],stratifiedforstage(low and advanced) and 5-year age group. The study intervals comprisedthepre-screeningperiod(2000–2005),the implemen-tation phase (2006–2008), and the subsequent period (2009– 2013)withafullyimplementedscreeningprogram.Therefore,we modeled the logarithmic annual rates with three continuous piecewiselinear functions of time according tothe aforemen-tionedtimeintervals.Theprocedurewasappliedforeachofthe five imputation runs. The results were summarized using SAS PROCMIANALYZE.Theresultinglinearsplines[20]arepresented inFig.3.Theslopeparametersandtheratedifferencesbetween thebeginningandendofthestudyperiod(200/2013)aredisplayed inTable2.
Statistical analyses were performed with SAS for Windows Version9.4(SASInc.,Cary,NC,USA).
3.Results
3.1.Baselinedescription
From 2000 to 2013, overall 13,874 cases of invasive breast cancersweredetectedinthetargetpopulationofwomenaged50– 69years intheMünsterdistrict.Thebaseline characteristicsof thesewomenarelistedinTable1.Completeinformationonearly (UICC I) and advanced (UICC II+) cancers were available for 12,437patients(89.6%).
3.2.Temporaltrendsofage-standardizedbreastcancerincidencerates Theage-standardizedincidencerateofinvasivebreastcancer increased markedly after the implementation of the MSP in 2005andpeakedintheyear2008(Fig.1).Fig.1alsodisplaysthe proportionsofmissingUICCvaluespercalendaryear.
Fig.2showstheage-standardizedincidencerates–separately forearly- andadvanced-stagebreastcancer–intheMSPtarget population.Clearly,theincidenceratesofcancersinstageUICCI
increasedafterintroductionof theMSPin 2005andleveledoff after2008,remainingelevateduntil2013ascomparedtothe pre-screenperiod.Bycontrast,ariseinincidenceratesof advanced-stagecancers (UICC II+)during thestep-up introductionof the program was followed by a rather consistent decline in the incidenceratesafter2008,reachinglevelsin2012/13thatwere lowerthaninthe5yearsofthepre-screeningperiod.
3.3.Temporaltrendsofage-specificbreastcancerincidencerates Age-stratifiedanalysesin5-yearagegroups,involvingalsothe agesadjacenttotherangeofscreeningeligibility(i.e.,45–49,70– 74and75–79years),showedthattheincidenceratesof early-stage cancers (UICC I) increased almost instantly after the introductionof theMSP intheregion (Fig. 3).Table2Ashows thatthisrisewasparticularlymarkedinthescreeningofeligible agegroupsasindicatedbystatisticallysignificantpositiveslopes. Afterfullimplementationof thescreeningprogram,theslopes declinedagainbutremainedelevatedabovethepre-screenlevels. This patternwasobservedin all eligibleage groups,from age groups50–54 yearsupto65–69years.Onlyaminorriseupto 2008 and a subsequent drop in incidence rates were seen in women aged 70–74 years, and none were observed among women of older ages. The UICC I rates for women aged 45– 49yearsshowedaweakerbutsignificantriseinparallelwiththe MSPintroduction.Bycontrast,theincidenceratesof advanced-stagebreastcancers(UICCII+)remainedunchangedinthisandin the youngest eligible age group (50–54 years). However, in womenaged54–69years, theimplementationof theMSPwas accompaniedbyshort-termincreasesinUICCII+incidencewhich was followed by marked declines which were statistically significant(Fig.3andTable2B).Ofnote:theincidenceratesof UICCII+cancersinwomenaged55–69yearsdecreasedtolevels thatwere significantly lower than in the pre-screening period (seedifference 2000–2013in Table 2B). Decliningtrends were also observed between 2006 and 2013 in women aged 70– 74 years (Table 2B), although these did not reach statistical significance.Inaddition,theincidencelevelin2013wasnotlower Table2
(A)Timetrendsfor(logarithmic)incidenceratesofstageIbreastcancer(BC)byperiodsbefore(2000–2005),duringthestep-upintroduction(2006–2008)andwiththefully implemented(2009–2013)mammographyscreeningprogram(MSP).Parameterestimatesand95%confidenceintervalspresentedarefromPoissonregressionmodels,per 5yearsagegroup.
Stage Age Slope2000– 2005 [95%CI] Slope2006– 2008 [95%CI] Slope2009– 2013 [95%CI] Difference 2000–2013 [95%CI] I 45–49 0.003989 [ 0.05711;0.04913] 0.07532 [0.00219;0.14844] 0.03547 [ 0.08141;0.01046] 0.02864 [ 0.20266;0.25993] I 50–54 0.066774 [0.01026;0.12329] 0.11618 [0.04841;0.18395] 0.01356 [ 0.02459;0.05170] 0.75020 [0.52521;0.97519] I 55–59 0.029229 [ 0.02568;0.08414] 0.18346 [0.11640;0.25052] 0.04523 [ 0.08279; 0.00768] 0.47036 [0.25426;0.68646] I 60–64 0.045263 [ 0.00023;0.09076] 0.15557 [0.09472;0.21643] 0.00198 [ 0.03376;0.03772] 0.70295 [0.51459;0.89132] I 65–69 0.076466 [0.02804;0.12489] 0.16569 [0.10814;0.22324] 0.02042 [ 0.05661;0.01576] 0.77728 [0.56346;0.99109] I 70–74 0.070497 [0.01632;0.12467] 0.04712 [ 0.02828;0.12252] 0.05501 [ 0.10425; 0.00577] 0.21878 [ 0.03169;0.46926] I 75–79 0.036094 [ 0.03704;0.10923] 0.00896 [ 0.10436;0.08644] 0.03120 [ 0.02543;0.08782] 0.30957 [0.01945;0.59969] (B)Timetrendsfor(logarithmic)incidenceratesofstageII+breastcancer(BC)byperiodsbefore(2000–2005),duringthestep-upintroduction(2006–2008)andwiththe fullyimplemented(2009–2013)mammographyscreeningprogram(MSP).Parameterestimatesand95%confidenceintervalspresentedarefromPoissonregression models,per5yearsagegroup.
Stage Age Slope 2000–2005 [95%CI] Slope 2006–2008 [95%CI] Slope20 09–2013 [95%CI] Difference 2000–2013 [95%CI] II+ 45–49 0.002042 [ 0.04219;0.04627] 0.01508 [ 0.04717;0.07734] 0.00526 [ 0.04503;0.03452] 0.02916 [ 0.16532;0.22363] II+ 50–54 0.018466 [ 0.06333;0.02640] 0.00319 [ 0.06013;0.06651] 0.01610 [ 0.02385;0.05606] 0.00223 [ 0.19149;0.18702] II+ 55–59 0.014404 [ 0.05627;0.02747] 0.00082 [ 0.06137;0.05972] 0.05435 [ 0.09499;-0.01370] 0.34623 [ 0.53288;-0.15957] II+ 60–64 0.001920 [ 0.03803;0.03419] 0.05806 [0.00281;0.11332] 0.08881 [ 0.12770;-0.04992] 0.27946 [ 0.45371;-0.10521] II+ 65–69 0.011773 [ 0.02554;0.04908] 0.06199 [0.00981;0.11416] 0.11307 [ 0.15319;-0.07294] 0.32051 [ 0.51523;-0.12580] II+ 70–74 0.035916 [ 0.00141;0.07324] 0.00418 [ 0.05858;0.05022] 0.02428 [ 0.06019;0.01163] 0.04562 [ 0.12509;0.21633] II+ 75–79 0.009083 [ 0.04929;0.03113] 0.00505 [ 0.05265;0.06275] 0.03946 [0.00401;0.07491] 0.16706 [ 0.00044;0.33455]
than at the beginning of the pre-screen period. No declining trendswereobservedaboveage75years.
4.Discussion
Thecurrentstudyinvestigatedwhethertheimplementationof theMSPsince2005affectedtheincidenceratesofadvanced-stage breastcancers(UICCII+)in50–69-year-oldwomenoftheMünster district.Thetimingofthisanalysiscorrespondstothepre-defined evaluationphasesoftheGermanMSP[21].
4.1.Temporaltrendsofearlyandadvancedbreastcancerincidence rates
Age-standardizedand age-specific analyses showed that the incidenceratesofadvanced-stagebreastcancer,afteraninitialrise following the introduction of the MSP, started to decline after 2008andreachedlevelsbelowthepre-screeningperiodin2013. Concomitantly,theincidenceofearly-stage(UICCI)breastcancers increased from 2005 and have remained elevated since. This suggests that the implementation of the MSP in the Münster districtresultedinaconsistentstageshiftforbreastcancerinthe targetpopulation.
Esserman et al. have described a hypothetical screening scenariowheretheincidenceratesofearly-stagecancersincrease aftertheintroductionofascreeningprogram,whiletheincidence rates of advanced cancers decrease after a while and remain
persistentlylowered[22].Infact,weobservedashortriseinthe ratesofadvancedbreastcancersaftertheintroductionoftheMSP; we suggest that this was attributable mainly to the increased detectionofclinicallyasymptomaticN+tumorsintheprevalence roundofthescreening.Thesubsequentdeclineofadvancedbreast cancerincidenceratesisconsideredoneofthebestindicatorsofan effectiveMSP[23–25].Declinesfollowingtheintroductionofan MSPhavebeenconsistentlyreportedinthoserandomizedclinical trialsthat achievedmarkedmortalityreductions;this ledTabar et al.tosuggest thatbreast cancermortalityreductionscanbe expectedonlyinsettingsthatareeffectiveinreducing advanced-stagebreastcancers[25].
4.2.Declinesinadvancedbreastcancerincidenceratesand mammographyscreening
Ourstudyrevealedmarkedandstatisticallysignificantdeclines in advanced breast cancer rates, mainly in women aged 55– 69 years. By contrast, many countries with long-standing mammographyscreeningprogramshavenotseencleardeclines inincidenceratesofadvancedbreastcancer.Asystematicreview by Autier et al. concluded that in many populationstudies in Europe,NorthAmericaandAustralia,onlysmalldeclines,ifanyat all,wereobserved[11,23].Interestingly,whileamuch-citedrecent study from the US reported only marginally reduced rates of advanced-stage cancers [12], another study, adjusting for the temporal trends before screening program initiation, found a Fig.1.Age-standardizedincidenceratesofinvasivebreastcancer(per100.000)from2000to2013,womenaged50–69yearsresidingintheMünsterDistrict.Thenumbers indicatetheproportionofmissingtumorstageinformationpercalendaryear.ThetwoverticalreferencelinesindicatethestartofimplementationoftheMSPin2005,andfull implementationoftheMSPin2008.
substantialreductioninadvanced-stagebreastcancersintheUS population[9].IntheNetherlands,astudybyateamofradiologists observedthat ratesof advanced breastcancers inwomen with screen-detectedandintervalcancersremainedconstantovertime [14].Likewise,reviewingtheNorwegianMSP,Lousdaletal.found nodeclineintheincidenceoflate-stagecancersinthescreening target group of 50–69-year-old women compared to an un-screenedgroupof20–49-year-oldwomen[13].Ontheotherhand, several studies observed declining incidence rates of advanced breastcancersaftertheintroductionoforganizedmammography screening.Forexample,decliningratesofadvanced-stagebreast cancerswerefoundearlyintheDutchMSP[7],andsignificantly lowerincidenceratesforstageIIIandIVcancerswerealsoreported fromtwostudiesinNorway[13,26].Arecentstudydescribedthat theincidence of advanced breast cancerwould havebeen 29% higherwithoutmammographyscreeningwhenemployinganage– period–cohortmodelbasedonUSSEER(Surveillance, Epidemiol-ogy,andEndResultsProgram)data[8].InItaly,asignificantdecline inadvanced(pT2topT4)breastcancercasesoccurredfromyear 3 onwards after the implementation of the MSP in over 700municipalitiesofsixadministrativeregions[6].
4.3.Validityaspectsofthestudyfindings
Thesecontroversialstudyfindingsareoftenrelatedto differ-encesinthemethodologyused,asdescribedpreviously[23,27].In particular,thereisnoconcurrentcontrolgroupwhenanorganized
screeningprogramisofferedtotheentirepopulation,aswasthe case in Germany. Therefore, the present results must first be viewed as a mere descriptionof the trend of advanced breast cancer incidence after the implementation of the MSP in the Münsterdistrict,thatis,asanecologicalstudy.Theevidencelevel of this type of epidemiological observational study is low and cannotfirmlyestablishcausalrelations. However,argumentsof consistencyandplausibilityofthefindingsmayhelptoenforcethe credibilityofacausalinterpretation.First,changesforbothearly andadvancedbreastcancerincidenceoccurredstrictlyafterthe introduction of the MSP, plausibly corroborating a temporal sequence. Second, these changes were mostly confined to the agegroupsthatwerealsoeligibleforMSP;theywerenotseenin youngerorolderagegroups.Third,whilerisesinearly-stagebreast cancerincidence rates after 2005 wereseen in all eligible age groups(50–69years),decrementofadvancedbreastcancerswas observed in those aged 55–69 years; this was indeed to be expectedbecauseleadtimeresultsinadvancementofearly-stage breastcancerdetectiontoyoungeragegroupswhilecausingatthe sametime the incidenceofadvanced stages todecreasein the olderagegroups.Infact,eventheweakerdeclinesintheagegroup 70–74yearsmaybepotentiallyattributabletoa‘spill-overeffect’ ofdecreasingadvanced-stageincidenceratesduetothisdetection advancement.Ofnote,itisunderstoodthatapotentialconcurrent declineinthe‘natural’incidenceofadvanced-stagebreastcancers withoutascreeningprogramcannotbecompletelyruledoutby thesearguments;however,inourview,thefindingsinthisstudy Fig.2.Age-standardizedincidencerates(per100.000)ofearly(stageI)andadvanced(stageII+)invasivebreastcancerfrom2000to2013,womenaged50–69yearsresiding intheMünsterDistrict.Caseswithmissingdataontumorstagingwereimputed.ThetwoverticalreferencelinesindicatethestartofimplementationoftheMSPin2005,and fullimplementationoftheMSPin2008.
appearhighlyconsistentwithand plausiblyindicativeofa true impact of the MSP on the incidence of advanced-stage breast cancer in the target population. On the other hand, the participation rate per screening round was only about 55% between2006 and 2012 in this MSP, and this may appear too lowtocreatesuchamarkedpopulationimpact.However,inthe population perspective, the cumulative proportion of ‘ever screened’ women, that is, of womenwho have participated in theMSPatleastonceintheentireperiod,washigherandrangedat about70%duetowomenwhorespondedtotheinvitationonlyin thesecond or third screening rounds.We also consideredthat opportunistic mammography screening was widespread before theintroductionoftheorganizedMSP[28]andthatthismayhave contributedtotheobserveddeclines.However,dataprovidedby
thestatutoryhealthinsurancesinNRWrevealthatopportunistic screeningdropped substantiallyandpersistentlyinthewake of MSP implementation. Hence, previous opportunistic screening does not seemto beable toplausibly explainwhy declines in advancedstagesofincidentbreastcancersoccurredafteraninitial increasefromaround2005andadeclinemostlyafter2008.Finally, theinitialincreaseinadvanced-stagecancersafterthestartofthe MSP maybe inpartattributable tostagemigration due tothe increased use of sentinel lymph-node biopsies (SNBs). The Association of German Tumor Centers reported an increase in SNBsfromabout30%in2005to80%in2011[29],whichmayhave resultedinsomeupstagingofbreastcancers.However,thelarge majorityoflymph-nodeinvolvementsdetectedbySNBaredueto micrometastases[30,31]whichwillnothaveaccruedasadvanced Figure3. Incidenceratesforearly(stageI)andadvanced(stageII+)breastcanceramongwomenaged45–79yearsintheMünsterDistrict,between2000and2013,by5years agegroup(datapoints).TheblacklinesrepresentperiodspecificestimatesoftrendsinincidenceratesasobtainedfromPoissonregressionmodels;theblueshadedareas representtherespective95%confidencebands.Thetwoverticaldottedlinesdemarcatethetransitionfromthepre-screenperiod(2000–2005)tothestep-upintroduction phaseofthemammographyscreeningprogram(2006–2008),andbetweenthestep-upintroductionandthesubsequentphaseoffullimplementation(2009–2013).(For interpretationofthereferencestocolourinthisfigurelegend,thereaderisreferredtothewebversionofthisarticle.)
stages (UICC II+) but as UICC IB. Moreover, the permanent upstaging of breast cancers cannot explain the decline in UICC II+ cancers after 2008 because stage-shift should have mitigatedratherthanamplifiedtheobserveddecline.
4.4.Strengthsandlimitations
A key strength of this study is the longstanding, large and population-basedstudysampleofwomenwithbreastcancerthat wasassembledwithahighlevelofcompleteness(>90%)ina well-definedstudyarea.Thisenabledthethoroughinvestigationofthe temporal trends of breast cancer incidence rates in the target populationbeforeandafterthestart theMSP.Ofnote,acertain degreeofincompletecancerregistrationwasobservedintheyear 2004,resultingfromarestructuringoftheregistrationprocessand thetransformationtoasystemofstatewidecancerregistrationin 2005.WeemployedPoissonregressionmodelingtoattenuatethe variabilitybetweencalendaryearssuchthattherelative‘reporting gap’in2004presumablyhadonlyaminorinfluenceonourresults. Furthermore, decreased use of postmenopausal hormone therapy (PMH) has been shown in the past to influence total breastcancerincidencerates[32,33].Unfortunately,todatethere arenostudiesshowingadifferentialimpactofthefallingPMHuse onearly-andlate-stagebreastcancerincidence;thus,apotential roleofdifferentpatternsofPMHtherapyintheobservedincidence trendscannotbecompletelyruledout.
Finally,thestudypopulationisnotnecessarilyrepresentative foralleligiblewomeninGermany,andthefindingsapplystrictly onlytotheMünsterdistrict;ontheotherhand,thesystematic screeningprocedures,includingstandardizedindicatorsofprocess quality,arebyandlargecomparableforallGermanregions.Thus, wesuggestthatourfindings maybeassumedtoalsopossessa relevantlevelofexternalvalidity.
5.Conclusions
Weprovideadescriptionoftrendsinadvancedbreastcancer incidence rates in the female population before and after the implementationoftheMSPintheMünsterdistrict.Ourdatashow that the fully implemented program was associated with a decreaseintheincidenceratesofadvancedbreastcancersafter a step-up introduction period. By contrast, early-stage breast cancer incidence rates increased almost instantaneously after starting the program. Age-specific analyses suggest that the declinein unfavorablebreast cancerstagesin olderagegroups isduetoadvancingearly-stagebreastcancerdetectioninyounger agegroups.
Conflictsofinterest
Allauthorsdeclarethattherearenoconflictsofinterest. Authors’contributions
AS:Dataanalyses,firstdraftandinterpretationofdata. IW:Dataanalyses,datainterpretation.
HWH:Studydesign,datainterpretation,revisionofintellectual content.
JH, OH: Data acquisition, data interpretation, revision of intellectualcontents.
Allauthorshavefinallyapprovedthesubmittedversion.
Acknowledgment
WethankDr.VanessaKääb-Sanyalfrom Kooperationsgemein-schaftMammographieforthoughtfulcommentsonanearlierdraft ofthemanuscript.
References
[1]Robert Koch-Institut (Hrsg) und die Gesellschaft der epidemiologischen KrebsregisterinDeutschlande.V.(Hrsg),KrebsinDeutschland2009/2010, RobertKoch-Institut(Hrsg)unddieGesellschaftderepidemiologischen KrebsregisterinDeutschlandeV(Hrsg),2013(9.Ausgabe).
[2]M. Sant, C. Allemani, R. Capocaccia,et al., Stage at diagnosis is a key explanationofdifferencesinbreastcancersurvivalacrossEurope,Int.J.Cancer 106(3)(2003)416–422.
[3]S.Walters,C.Maringe,J.Butler,etal.,Breastcancersurvivalandstageat diagnosisinAustralia,Canada,Denmark,Norway,SwedenandtheUK,2000– 2007:apopulation-basedstudy,Br.J.Cancer108(5)(2013)1195–1208. [4]L.Giordano,K.L.von,M.Tomatis,etal.,Mammographicscreeningprogrammes
inEurope:organization,coverageandparticipation,J.Med.Screen.19(Suppl. 1)(2012)72–82.
[5]IARCHandbooksofCancerPrevention,Volume7:BreastCancerScreening, IARCPress,Lyon,France,2002.
[6]F.Foca,S.Mancini,L.Bucchi,etal.,Decreasingincidenceoflate-stagebreast canceraftertheintroductionoforganizedmammographyscreeninginItaly, Cancer119(11)(2013)2022–2028.
[7]J.Fracheboud,S.J.Otto,J.A. vanDijck,M.J.Broeders,A.L.Verbeek,H.J.de Koning,Decreasedratesofadvancedbreastcancerduetomammography screeninginTheNetherlands,Br.J.Cancer91(5)(2004)861–867. [8]R.E. Gangnon, B.L. Sprague, N.K. Stout, et al., The contribution of
mammographyscreeningtobreastcancerincidencetrendsintheUnited States:anupdatedage-period-cohortmodel,CancerEpidemiol.Biomarkers Prev.24(6)(2015)905–912.
[9]M.A.Helvie,J.T.Chang,R.E.Hendrick,M.Banerjee,Reductioninlate-stage breastcancerincidenceinthemammographyera:implicationsfor overdiagnosisofinvasivecancer,Cancer120(17)(2014)2649–2656. [10]S.Hofvind,C.I.Lee,J.G.Elmore,Stage-specificbreastcancerincidencerates
amongparticipantsandnon-participantsofapopulation-based
mammographicscreeningprogram,BreastCancerRes.Treat.135(1)(2012) 291–299.
[11]P.Autier,M.Boniol,R.Middleton,etal.,Advancedbreastcancerincidence followingpopulation-basedmammographicscreening,Ann.Oncol.22(8) (2011)1726–1735.
[12]A.Bleyer,H.G.Welch,Effectofthreedecadesofscreeningmammographyon breast-cancerincidence,N.Engl.J.Med.367(21)(2012)1998–2005. [13]M.L.Lousdal,I.S.Kristiansen,B.Moller,H.Stovring,Trendsinbreastcancer
stagedistributionbefore,duringandafterintroductionofascreening programmeinNorway,Eur.J.PublicHealth24(6)(2014)1017–1022. [14]J. Nederend, L.E. Duijm, A.C. Voogd,J.H. Groenewoud, F.H.Jansen, M.W.
Louwman,Trendsinincidenceanddetectionofadvancedbreastcancerat biennialscreeningmammographyinTheNetherlands:apopulationbased study,BreastCancerRes.14(1)(2012)R10.
[15]N.Perry, M.Broeders,C.deWolf,S.Tornberg,R. Holland,L.vonKarsa, EuropeanGuidelinesforQualityAssuranceinBreastCancerScreeningand Diagnosis,fourthedition,OfficeforOfficialPublicationsoftheEuropean Communities,Luxembourg,2006.
[16]S.vanBuuren,Multipleimputationofdiscreteandcontinuousdatabyfully conditionalspecification,Stat.MethodsMed.Res.16(3)(2007)219–242. [17]N.Eisemann,A.Waldmann,A.Katalinic,Imputation ofmissing valuesof
tumourstageinpopulation-basedcancerregistration,BMCMed.Res. Methodol.11(2011)129.
[18]European Commission, EUROSTAT: Methodologies and Working Papers. RevisionoftheEuropeanStandardPopulation,ReportofEurostat'stask force(2013).
[19]N.E.Breslow,N.E.Day,TheDesignandAnalysisofCohortStudies.Statistical MethodsinCancerResearch.VolumeII,IARCScientificPublicationsNo.82, Lyon,1987.
[20]S.Greenland,Dose-responseandtrendanalysisinepidemiology:alternatives tocategoricalanalysis,Epidemiology6(4)(1995)356–365.
[21]Stellungnahme des Wissenschaftlichen Gremiums des Beirates der KooperationsgemeinschaftMammographie,VerfahrenzurBewertungder WirksamkeitdesDeutschenMammographie-Screening-Programmsaufdie SenkungderSterblichkeitdurchBrustkrebs,2011,Stellungnahmedes WissenschaftlichenGremiumsdesBeiratsderKooperationsgemeinschaft Mammographievom17.10.2011.
[22]L.Esserman,Y.Shieh,I.Thompson,Rethinkingscreeningforbreastcancerand prostatecancer,JAMA302(15)(2009)1685–1692.
[23]P.Autier,M.Boniol,Breastcancerscreening:evidenceofbenefitdependson themethodused,BMCMed.10(2012)163.
[24]N.E.Day,D.R.Williams,K.T.Khaw,Breastcancerscreeningprogrammes:the developmentofamonitoringandevaluationsystem,Br.J.Cancer59(6)(1989) 954–958.
[25]L.Tabar,A.M.Yen,W.Y.Wu,etal.,Insightsfromthebreastcancerscreening trials:howscreeningaffectsthenaturalhistoryofbreastcancerand
implicationsforevaluatingservicescreeningprograms,BreastJ.21(1)(2015) 13–20.
[26]M.L.Lousdal, I.S. Kristiansen, B. Moller, H.Stovring, Effect of organised mammographyscreeningonstage-specificincidenceinNorway:population study,Br.J.Cancer114(5)(2016)590–596.
[27] R.S.Falk,S.Hofvind,P.Skaane,T.Haldorsen,Overdiagnosisamongwomen attendingapopulation-basedmammographyscreeningprogram,Int.J.Cancer 133(3)(2013)705–712.
[28]G.Schott,M.Reichel,H.Junkermann,N.Becker,Retrospectivequantificationof backgroundincidenceandstagedistributionofbreastcancerforthe mammographyscreeningpilotprojectinWiesbaden,Germany,J.CancerRes. Clin.Oncol.134(1)(2008)29–35.
[29]www.tumorzentren.de/tl_files/dokumente/Qualitaetskonferenzen/5.% 20Bundesweite%20Onkologische%20Qualitaetskonferenz%202014/ Fachvortraege%20auf%20dem%20DKK%202014/
DKK2014_Mamma_20140217_AGO.pdf(2016).
[30]A.J.Maaskant,L.V.vandePoll-Franse,A.C.Voogd,J.W.Coebergh,M.C.Tutein Nolthenius-Puylaert,G.A.Nieuwenhuijzen,Stagemigrationdueto introductionofthesentinelnodeprocedure:apopulation-basedstudy,Breast CancerRes.Treat.113(1)(2009)173–179.
[31]T.F.Tvedskov,M.B.Jensen,E.Balslev,B.Ejlertsen,N.Kroman,Stagemigration afterintroductionofsentinellymphnodedissectioninbreastcancer treatmentinDenmark:anationwidestudy,Eur.J.Cancer47(6)(2011)872– 878.
[32]A. Katalinic,A.Lemmer, A.Zawinell, R. Rawal,A. Waldmann,Trends in hormonetherapyandbreastcancerincidence—resultsfromtheGerman NetworkofCancerRegistries,Pathobiology76(2)(2009)90–97.
[33]A.Stang,Decline inhormonereplacementprescriptionandfall inbreast cancerincidence:anepidemiologicaldiscourse,Dtsch.Arztebl.Int.105(16) (2008)303–309.