Received: October, 2015 Accepted: February, 2016 ,Available online: March, 2016
Does long term sport rock climbing training affect on echocardiography and heart
rate variability in sedentary adults? A randomized, and controlled study.
Dicle Aras*1, Cengiz Akalan2, Mitat Koz3, Mehmet Ileri4
1Ph.D., Research Assistant - Ankara University Faculty of Sport Sciences - Department of Coaching Education. E-mail address:
2Ph.D., Associate Professor - Ankara University Faculty of Sport Sciences - Department of Coaching Education. E-mail address:
3MD., Professor - Ankara University Faculty of Sport Sciences - Department of Coaching Education. E-mail address:
4MD., Associate Professor - Ankara Numune Education and Research Hospital - Department of Cardiology. E-mail address:
*Mailing address: Ankara University Faculty of Sport Sciences, Department of Coaching Education, 06830, Golbasi/Ankara/Turkey. E-mail: [email protected] Tel: +90 532 306 0415 Fax: +90 312 212 2986
ABSTRACT: Regular physical activity can cause some long term effects on human body. The
purpose of this research was to examine the effect of sport rock climbing (SRC) training at 70 % HRmax level on echocardiography (ECHO) and heart rate variability (HRV) for one hour a day and three days a week in an eight-week period. A total of 19 adults participated in this study voluntarily. The subjects were randomly divided into two groups as experimental (EG) and control (CG). While the EG went and did climbing training by using the top-rope method for 60 minutes a day, three days a week for 8 weeks and didn’t join any other physical activity programs, CG didn’t train and take part in any physical activity during the course of the study. Same measurements were repeated at the end of eight weeks. According to the findings, no significant change was observed in any of the ECHO and HRV parameters. However, an improvement was seen in some HRV parameters [average heart rate (HRave), standard deviation of all NN intervals (SDNN), standard deviation of the averages of NN intervals in all five-minute segments of the entire recording (SDANN), percent of difference between adjacent NN intervals that are greater than 50 ms (PNN50), square root of the mean of the sum of the squares of differences between adjacent NN interval (RMSSD)] in EG. An exercise program based on SRC should be made more than eight weeks in order to have statistically significant changes with the purpose of observing an improvement in heart structure and functions.
INTRODUCTION
Rock climbing has been defined as a physical activity in which the arms are used when the legs do not have the capacity to move the climber over the rock face [1]. In recent years, it has become a very popular activity in both competitive and recreational terms [2, 3]. Every day, almost 3000 people attempt rock climbing for the first time, and sport climbing has been announced as a candidate for the 2020 Olympic Games. The increase in interest in rock climbing for recreational purposes and as a competitive sport [3, 4, 5] can be attributed to its being both a psychological and a physical challenge [6], and also to the appeal of being able to pursue it both in natural surroundings and indoors [7]. Despite the fact that there are many sub-branches and varying difficulty levels for each climbing wall, most recreational climbers prefer sport rock climbing (SRC) in which fixed anchors are placed at set intervals on the climbing wall [8]. Due to the existence of these fixed anchors, SRC is considered to be a safe climbing method which allows recreational climbers to meet almost all of their physiological and psychological requirements.
Echocardiography (ECHO) is a non-invasive imaging technique used to analyze the anatomy and physiology of the heart [9], and is the most commonly used technique in examining heart structure [10]. In exercise and the sports sciences, it is used to examine the acute effect of physical activity and the chronic effects of exercise on the heart [11]. Heart rate variability (HRV) is also widely used in the sports sciences as it shows the magnitude and time between consecutive heart beats [12] and is another non-invasive method to evaluate autonomous heart functions [13].
In recent years, there have been several scientific research studies into SRC. In many of these, energy consumption, heart rate and anxiety levels were determined and acute SRC effects were examined. The purpose of this research is to determine whether an eight-week SRC training period at 70 % of HRmax for one hour a day, three days a week causes a chronic change in heart structure and function. This will allow a better understanding of how SRC affects heart health.
METHODS
Participants and study design
19 students from the Ankara University Faculty of Sport Sciences voluntarily participated in this study. They were divided into two groups. 10 were placed in the control group (4 males and 6 females, age 21.90 ±1.66 years, height 168.50 ±4.40 cm, weight 61.18 ±7.08 kg) and 9 were placed in the experimental group (5 males and 4 females, age 21.11 ±2.31 years, height 167.33 ± 6.44
cm, weight 59.31 ±8.39 kg). The
experimental group consisted of people who were not acrophobic, had not participated in any regular physical training for at least six months, and who would not participate in any regular physical training other than the climbing exercises for the eight-week study period. The control group was composed of volunteers who had not participated in any regular physical activity for at least six months, and who would not participate in any exercise programs during the study period. The research was approved by the Ankara
University Medical Faculty Clinical
Research Ethics Committee (13-434-12), and Informed Consent Forms were completed by all participants in both groups.
indoor artificial climbing wall. All the climbing exercises utilized the top-rope technique, with the provision of a safety line. Heart rates were determined by using the HRreserve method [Target HR = (percentage of load) x (HRmax - HRrest) + HRrest] during the training period for each subject [14]. HRrest was taken before the HRmax test, after having the subjects lie down for 5 minutes [15]. HRmax values were taken from the Bruce treadmill test protocol, and were used to determine 70 % intensity of HRmax for each subject during the climbing exercise. Each subject had their own monitor (Polar Team 2 Polar, Finland) adjusted to within ±5 of the HRtarget range in order to achieve the desired exercise intensity, and the subjects were asked to change their pace of climbing accordingly. The subjects exercised 3 days a week for 8 weeks, with 60 minutes for each session [14, 16, 17]. Prior to the study, the subjects were trained in basic holding and stepping skills, as well as the safe usage of climbing materials and rope techniques. All subjects received pre- and post-test measurements of body composition, aerobic power, echocardiography, and heart rate variability for the 4 days prior to the start of the climbing exercises and immediately after the end of the 8-week test period.
Measurements
Body Composition: Body weights were
measured with an Avis 333 plus (Korea) analyzer and a Holtain branded stadiometer with 1mm accuracy was used to measure height (Holtain, U.K.).
Aerobic power: VO2max (ml.kg-1.m-1) and
HRmax (pulse/min) were measured using the Bruce treadmill test protocol. VO2max oxygen consumption was measured
(Viasys-Oxycon branded MasterScreen-CPX
spirometre Hoechberg, Germany) during a treadmill run (RAM branded 770 M treadmill Camin, Italy). Failure of the subject to
continue at the required pace was taken as a criteria to end the test.
Echocardiography: Echocardiographic examinations were made and interpreted by using the transthrocacic method and a Vingmed branded CFM 725 device (GE Vingmed Ultrasound AS, Horten, Norway), which is used by cardiology specialists to conduct 2D colored Doppler analyses. A transducer was set at 2.5 MHz during the measurements. The examination was made
by using suitable echocardiographic
windows (left parasternal area, apical area 2nd, 3rd and 4th spaces, subcostal area, and the parasternal long axis and short axis) while the participant was lying on his/her left side. M-mode and colored Doppler evaluations
were applied respectively to the
measurements according to the criteria recommended by the American Society of Echocardiography.
The ECHO measurements allowed the interpretation of each participant’s left atrial diameter (LAD), left ventricular end-diastolic diameter (LVEDD), left ventricular
end-systolic diameter (LVESD), left
ventricular ejection fraction (LVEF), interventricular septal thickness (IVST), left ventricular posterior wall thickness (LVPWT) and aortic root diameter (ARD) .
Heart Rate Variability: HRV results were
By using the measurements made with the device; total HR (HRtot), average HR (HRave), minimum HR (HRmin), maximum HR (HRmax) and some additional HRV parameters (SDNN, SDANN, PNN50, RMSSD, TRIA) could be obtained.
Statistical analysis
An SPSS 20 (SPSS Inc., Chicago, IL, USA) was used for the statistical data analyses of the research. The distribution of data was tested for parametric or nonparametric tests. The normality distribution was tested using a
Shapiro Wilk test, the normal distribution parametric was subjected to a Paired Sample t-Test, and the nonparametric distribution was given a Wilcoxon test. An alpha value of 0.05 was accepted for all of the statistical analyses.
STATISTICAL RESULTS
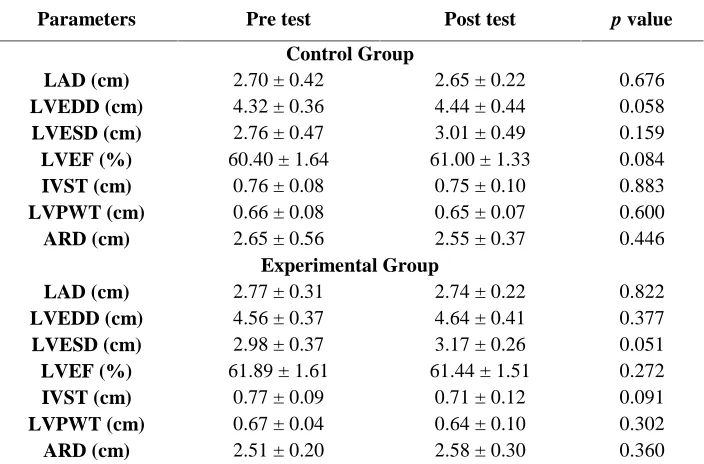
The results of ECHO values obtained from participants and average comparisons are shown in Table 1 for both the control and the experimental groups.
Table 1. Echocardiography values and their mean differences obtained from pre- and post-tests.
Parameters Pre test Post test p value
Control Group
LAD (cm) 2.70 ± 0.42 2.65 ± 0.22 0.676
LVEDD (cm) 4.32 ± 0.36 4.44 ± 0.44 0.058
LVESD (cm) 2.76 ± 0.47 3.01 ± 0.49 0.159
LVEF (%) 60.40 ± 1.64 61.00 ± 1.33 0.084
IVST (cm) 0.76 ± 0.08 0.75 ± 0.10 0.883
LVPWT (cm) 0.66 ± 0.08 0.65 ± 0.07 0.600
ARD (cm) 2.65 ± 0.56 2.55 ± 0.37 0.446
Experimental Group
LAD (cm) 2.77 ± 0.31 2.74 ± 0.22 0.822
LVEDD (cm) 4.56 ± 0.37 4.64 ± 0.41 0.377
LVESD (cm) 2.98 ± 0.37 3.17 ± 0.26 0.051
LVEF (%) 61.89 ± 1.61 61.44 ± 1.51 0.272
IVST (cm) 0.77 ± 0.09 0.71 ± 0.12 0.091
LVPWT (cm) 0.67 ± 0.04 0.64 ± 0.10 0.302
ARD (cm) 2.51 ± 0.20 2.58 ± 0.30 0.360
LAD: Left atrial diameter; LVEDD: Left ventricular end-diastolic diameter; LVESD: Left ventricular end-systolic
diameter; LVEF: Left ventricular ejection fraction; IVST: Interventricular septal thickness; LVPWT; Left ventricular
posterior wall thickness; ARD: Aortic root diameter.
At the end of the examination, no significant differences between the pre- and post-tests were found in any of the ECHO parameters.
HRV results obtained from LT-HRV recording and average comparisons are shown in Table 2.
Parameters Pre test Post test p value
Control Group
HRtot 99499.60 ± 15094.74 100296.30 ± 16528.32 0.859
HRmax 167.70 ± 41.12 177.70 ± 34.95 0.114
HRave 75.10 ± 8.22 75.30 ± 8.24 0.719
HRmin 43.90 ± 6.15 44.80 ± 6.17 0.475
SDNN 180.50 ± 28.62 189.30 ± 35.05 0.439
SDANN 91.90 ± 29.30 79.40 ± 16.52 0.415
PNN50 27.70 ± 8.74 24.10 ± 8.35 0.106
RMSSD 66.70 ± 25.28 64.00 ± 17.23 0.721
TRIA 792.80 ± 151.42 794.50 ± 165.03 0.976
Experimental Group
HRtot 91173.56 ± 13519.90 94301.89 ± 14166.33 0.449
HRmax 156.56 ± 23.70 159.11 ± 19.14 0.788
HRave 70.11 ± 9.64 67.00 ± 10.76 0.369
HRmin 42.33 ± 6.65 41.67 ± 6.96 0.833
SDNN 203.77 ± 37.44 215.00 ± 51.71 0.607
SDANN 94.11 ± 30.33 104.56 ± 34.81 0.411
PNN50 29.67 ± 12.65 34.89 ± 15.25 0.406
RMSSD 73.00 ± 26.04 78.22 ± 34.26 0.638
TRIA 899.00 ± 237.17 841.67 ± 234.98 0.542
HRtot: Total heart rate; HRmax: Maximum heart rate; HRave: Average heart rate; HRmin: Minimum heart rate;
SDNN: standard deviation of all NN intervals; SDANN5: standard deviation of the averages of NN intervals in all
five-minute segments of the entire recording; PNN50: percent of difference between adjacent NN intervals that are
greater than 50 ms; RMSSD: square root of the mean of the sum of the squares of differences between adjacent NN
interval; TRIA: Triangular index.
According to the results, no significant differences were found in the HRV parameters’ pre- and post-tests average. However, in some HRV parameters for the experimental group, improvements showing a decrease in sympathetic effect and an increase in parasympathetic activity were observed. The decrease of HRave and the increase of time-domain (SDNN, SDANN, PNN50, and RMSSD) parameters show the increase of parasympathetic activity.
DISCUSSION
As expected, no significant differences were observed in any of the ECHO and HRV results in the control group. This is a positive result in terms of this study’s consistency, and shows that the control group members did not participate in any physical activity programs.
[18]. Ostariz et al. (2013) reported an LVEF of 67 % in 91 male bicycle riders in a study where they examined ECHO findings [19]. In the current study, the value for LVEF was found to be 61.44 %. Nagashima et al. (2003) examined the ECHO values of 297 ultra-marathon (100 km) runners aged between 20 and 73 [20]. At the end of their research, the average LVEDD was 6.18 cm and the LVEDD of 33 runners was over 7.0 cm [20], which is above the values reported by other studies. An LVEDD of 7.0 cm in bicycle riders has also been reported in some previous research studies [21]. The result we obtained from the present study is 4.64 cm. Nagashima et al. (2003) also observed an LAD of 4.02 cm in the same research [20]. In other research studies [20, 21] a LAD of 4.5 cm and an ARW of 3.9 cm was observed in rowers. In the present research, we obtained measurements of 2.74 cm for LAD and 2.58 cm for ARD. That being the case, it is clear that morphologic changes are more likely to occur after long periods of training. In another research, the ECHO findings of people from different sports branches were examined. The IVST values were 0.94 cm, 1.04 cm, 1.26 cm, 1.08 cm and 1.05 cm for football players, sprinters, long distance runners, weight lifters and body builders respectively; this value is 0.77 cm in the present study. The same study recorded LVPWT rates of 1.05 cm, 0.96 cm, 1.10 cm, 1.03 cm and 0.97 cm with the same order, and an LVPWT of 0.64 cm was recorded in the current research. In addition, the LVEDD was 5.14 cm, 5.18 cm, 5.38 cm, 5.03 cm and 4.98 cm whereas it was found to be 4.64 cm in ours. Finally, the study’s LVESD values of 3.74 cm, 3.86 cm, 3.73 cm, 3.57 cm and 3.50 cm, were recorded as 3.17 cm in the present research.
Heart enlargement in athletes is an adaptation that occurs due to training instead of its occurrence due to cardiovascular disease in other people [22]. It is thought that changes such as cardiac hypertrophy, left ventricle diameter widening, left ventricle wall thickening as well as increase in left ventricle diastolic and systolic diameters in the hearts of athletes occur only after extended periods [23]. When compared with the above-mentioned studies, the high values in LAD, LVEDD, LVESD, LVEF, IVST, LVPWT and ARD as recorded by the ECHO findings in the current research support this information.
Insignificant improvements were seen in some HRV data in the experimental group. In HRave results dropped from 70.11 to 67.00. Insignificant improvements were also observed in SDNN, SDANN, PNN50, RMSSD, which were obtained within the time-domain parameters of HRV. In the literature, there is no other study that has examined the long-term effect of sports rock climbing exercises according to HRV time-domain or frequency-time-domain parameters. However, the effects of different physical activities with similar frequency, duration and intensity have been examined.
on HRV of a 14-week aerobic exercise program with variable intensity (VO2max varying from 45 % to 70 %) undertaken by 11 untrained male subjects with an average age of 36.8 and could not find any significant difference in HRV parameters [26]. A similar study was conducted by Perini et al., and no significant effect on HRV parameters resulted from an eight-week aerobic training conducted with bicycle ergometers for three days a week and 60 minutes per day (with an intensity of 40-60 %) undertaken by a sedentary group of participants with an average age of 73.9 [27]. Another study was made with a sedentary group with an average age of 62. In this study, it was reported that a one-year exercise program consisting of aerobic and power training (with low and moderate intensity) was had no effect on HRV parameters [28]. The results of these studies, which were conducted over longer periods than present research, and in which no changes in HRV were observed, show similarities with the results obtained in the present study.
However, there are also studies that prove the positive effects of exercise on HRV. In one study, 3328 healthy adults aged between 45 and 68 were examined, it was reported that people whose physical activity level is moderate (≤3- <5 MET) and high (≥5 MET) have longer HRV ranges and lower HRrest [29]. Another study examined the effects of a twelve-week cardiovascular and muscle strength training with a moderate-high intensity on the HRV values of 183 healthy adults in different positions (lying, standing up, standing for 180-360 seconds and for 360-540 seconds) was examined. It was discovered that regular physical activity leads to significant improvements in many HRV parameters in all body positions. The HR, RR, SDNN, RMSSD, PNN50, SD, LF, HF, LFnu, HFnu (p< 0.01) and LF/HF (p< 0.05) parameters significantly changed when the
subjects were lying down. In the other three positions, significant improvements were observed only in LF/HF, LFnu and HFnu [30]. Cornelissen et al. (2010) examined the HRV effects caused by 10 weeks of low-intensity (33 % of HRreserve) and high-intensity (66 % of HRreserve) aerobic exercises done by a group of sedentary participants with an average age of 55. They stated that running, bicycle riding and step activities for 50 minutes a day, three days a week lead to a significant difference only on TP (p< 0.001) at both intensities [31]. In another study made with 12 healthy female adults, it was seen that eight-weeks of Hatha-Yoga exercises done for 60 minutes a week caused a significant change in the night measurements of PNN50, whereas only insignificant improvements were observed in the other HRV parameters [32].
Even though it is believed that physically active individuals have higher HRV values than their sedentary peers [12], and that the parasympathetic effect is dominant while resting, it can be seen that the effects of regular physical activities on OSS is open to
discussion when the above-mentioned
studies are examined. The currently available research results are not enough to clearly explain the relationship between exercises and HRV. New studies made with different groups, different exercise duration and intensity with many participants will bring additional clarity to this subject. However, when the positive effects observed in some research studies are taken into account, it can be considered normal to see similar changes (although they are insignificant) after eight weeks of sports rock climbing training.
According to the results obtained from this study, exercise experts should plan programs which are longer than eight weeks in order to see significant changes if they intend to use sport rock climbing as the main activity in exercise programs that target structural and functional changes in the heart. The same research can be carried out by creating a second experimental group undergoing an aerobic exercise program which will be accepted as a standard in following studies. Thus, chronic adaptations that occur as a result of rock climbing can be compared with other types of activities in a more accurate and simultaneous manner. Another limitation of the study was the uncontrolled diet of the participants. They continued with their own diets, and this may also have been effective
on their levels of cardiovascular adaptation. Apart from this, researchers could use this type of exercise in other populations such as the elderly and children for further studies to achieve a better understanding.
As a result; it was observed that an eight-week sports rock climbing training period did not make any significant changes in ECHO. On the other hand, it was understood that it caused insignificant improvement in HRave obtained from the heart rate variability measurements and most of the time-domain parameters (SDNN, SDANN, PNN50, and RMSSD). However, the exercise should be longer than eight weeks in order to produce significant positive changes in HRV.
REFERENCES
1. Sturm G, Zintl F. Felsklettern, Alpin-Lehrplan 2, Deutscher Alpenverein. München: BlV Verlagsgesellschaft; 1979:1-13.
2. Backe S, Erıcson L, Janson S, Timpka T. Rock climbing injury rates and associated risk factors in a general climbing population. Scand J Med Sci Sports 2009;19:850-856.
3. Sibella F, Frosio I, Schena, F, Borghese NA. 3D Analysis of the body center of mass in rock climbing. Hum Mov Sci 2007;26(6):841-852.
4. Draper N, Jones GA, Fryer S, Hodgson CI, Blackwell G. Physiological and psychological responses to lead and top-rope climbing for intermediate level rock climbers. Eur J Sport Sci 2010;10(1):13-20.
5. Shell AV. Physiology of sport rock climbing. Br J Sports Med 2004;38(3):355-359.
6. Hodgson CI, Draper N, Mcmorris T, Jones G, Fryer S, Coleman I. Perceived anxiety and plasma cortisol concentrations following rock climbing with differing safety rope protocols. Br J Sports Med 2008;43(7):531-535.
7. Fanchini M, Violette F, Impellizzeri FM, Maffiuletti NA. Differences in climbing-specific strength between boulder and lead rock climbers. J Strength Cond Res 2013;27(2):310-314.
9. Solomon SD, Bulwer BE. Essential Echocardiography. Totowa, NJ: Humana Press; 2007:3.
10. Nanda NC, Hsiung MC, Miller AP, Hage FG. Live/Real Time Echocardiography. Hoboken, NJ: Wiley-Blackwell Publication; 2012:13.
11. Hnidawei MA, Mjall M, Zayed Z. The upper limit of physiological cardiac hypertrophy in elite male athletes. Am J Appl Sci 2010;7(10):1327-1333.
12. Borresan J, Lambert MI. Autonomic control of heart rate during and after exercise. Sports Med 2008;38(8):633-646.
13. Myllymaki T, Rusko H, Syvaoja H, Juuti T, Kinnunen ML, Kyrolainen H. Efects of exercise intensity and duration on nocturnal heart rate variability and sleep quality. Eur J Appl Physiol 2012;112:801-809.
14. Ehrman JK. Exercise prescription. In: Swain DP, Ehrman JK, ed. ACSM’S resource manual for guidelines for exercise testing and prescription. 6th ed. Philadelphia: Wolters Kluver Lippincott Williams & Wilkins; 2010:448-455.
15. Donath L, Faude O, Roth R, Zahner L. Effects of stair-climbing on balance, gait, strength, resting heart rate, and submaximal endurance in healthy seniors. Scand J Med Sci Sports 2014;24:93-101.
16. Thompson WR, Bushman BA, Desh J, et al. ACSM’S Resources for the Personal Trainer. Philadelphia: Wolters Kluver Lippincott Williams & Wilkins; 2010:367.
17. Heyward VH. Advanced Fitness Assessment and Exercise Prescription. Champaign, IL: Human Kinetics; 2010:98.
18. Sundstedt M, Jonason T, Ahren T, Damm S, Wesslen L, Henriksen L. Left ventricular volume changes during supine exercise in young endurance athletes. Acta Physiol Scand 2003;177(4):467-472.
19. Ostariz ES, Ramon ML, Arroyos DC, et al. Post-exercise left ventricular dysfunction measured after a long-duration cycling event. BMC Research Notes 2013;6(211):1-5.
20. Nagashima J, Musha H, Takada H, Murayama M. New upper limit of physiologic hypertrophy in japanese participants in the 100-km ultramarathon. J Am Coll Cardiol 2003;42(9):1617-1623.
21. Pellicia A, Maron BJ, Spataro A, Proschan MA, Spirito P. The upper limit of physiologic cardiac hypertrophy in in highly trained elite athletes. N Engl J Med 1991;324(5):295-301.
22. Macfarlane N, Northbridge DB, Wright AR, Grant S, Dargie HJ. A comparative study of left ventricular structure and function in elite athletes. Br J Sports Med 1991;25(1):45-48.
24. Jakubec A, Stejskal P, Kovacova L, et al.Changes in heart rate variabılity after a six month long aerobic dance or step-dance programme in women 40–65 years old: the influence of different degrees of adherence, intensity and initial levels. Acta Gymnica 2008;38(2):35-44.
25. Lu WA, Kuo CD. Effect of 3 month tai chi chuan on heart rate variability, blood lipid and cytokine profiles in middle-aged and elderly individuals. Int J Gerontol 2012;6(4):267-272.
26. Martinmaki K, Hakkinen K, Mikkola J, Rusko H. Effect of low-dose endurance training on heart rate variability at rest and during an incremental maximal exercise test. Eur J Appl Physiol 2008;104(3):541-548.
27. Perini R, Fisher N, Veicsteinas A, Pendergast DR. Aerobic training and cardiovascular responses at rest and during exercise in older men and women. Med Sci Sports Exerc 2002;34(4):700-708.
28. Verheyden V, Eijnde BO, Beckers F, Vanhees L, Aubert AE. Low-dose exercise training does not influence cardiac autonomic control in healthy sedentary men aged 55-75 years. J Sports Sci 2006;24(11):1137-1147.
29. Rennie KL, Hemingway H, Kumari M, Brunner E, Malik M, Marmot M. Effects of moderate and vigorous physical activity on heart rate variability in a british study of civil servants. Am J Epidemiol 2003;158(2):135-143.
30. Grant CC, Viljoen M, Rensburg DCJ, Wood PS. Heart rate variability assessment of the effect of physical trainig on autonomic cardiac control. Ann Noninvasive Electrocardiol 2012;17(3):219-229.
31. Cornelissen VA, Verheyden B, Aubert AB, Fagard RH. Effects of aerobic training intensity on resting, exercise and post-exercise blood pressure, heart rate and heart-rate variability. J Hum Hypertens 2010;24(3):175-182.