International Journal of Applied Exercise Physiology 2322-3537 www.ijaep.com
Vol.7 No.4
Received: April 2018 , Accepted: October 2108 , Available online: December 2018
DOI: 10. 30472 /ijaep.v7i4.283
The effect of a balance training program with and without mirror on postural control of lower limb amputees
Mahya Mohamadtaghi1*, Parisa Hejazidinan2, Parvane Shamsipourdehkordi2, Esmaeel Saemi3
1Department of Motor Behavior, Shahid Beheshti University, Tehran, Iran; 2Department of Motor Behavior, Alzahra
University, Tehran, Iran; 3.Department of Sport Psychology, Shahid Chamran University of Ahvaz, Iran
ABSTRACT:
Objectives. The aim of the present study was to compare the effect of a selected balance program with and without using mirror on balance of individual with amputee. Methods. Twenty-one lower limb amputees (with age range between 25 to 60 years) participated in this study and randomly were recruited into three groups: control, balance program, and mirror balance program. The participants took part in pretest after one month. Experimental groups performed their balancing program for 1 month (4 weeks, 5 sessions per week, 30 minutes each session). To asses postural control, Computerized Dynamic Posturography was used Using sensory organization test, balance was measured in six conditions (first: existence of sight, hearing and proprioception; second: elimination of sight; third: manipulation of vestibular system; fourth: manipulation of proprioception; fifth: elimination of sight and manipulation of proprioception and sixth: manipulation of vestibular system and proprioception). Results. The results indicated that the stability score in both balance and mirror balance groups have improved compare to the control group. Furthermore, in the first and second conditions, both experimental groups have obtained a higher stability score and a less displacement in the center of gravity compare to the control. In the sixth condition, the stability score was lower and displacement score was higher. Also, the amputee in the balance exercise using mirror group had a better balance in all the six conditions. Conclusion .Finally, we can conclude that undergoing a series of balance exercises with and without mirror improves balance and postural stability in lower limb amputee.
INTRODUCTION
One of the most common problems after leg amputation is balance disorder and the weakening of physical performance [1]. Most likely, people with lower limb amputation cannot participate steadily in daily and social activities [2] as they are not willing to risk falling. However, maintaining balance and controlling posture in different protection levels doing daily life activities is necessary for the amputee [3]. Mancini and Horak, (2010) have stated in their research that assessing clinical balance can contribute to evaluate the risk of falling and the main reasons for balance disorders [4]. Previous research has shown that falling is one of the factors in decreasing the level of personal and public health, noticing the fact that each year about 12 million people are prone to fall [5]. Miller et al. (2002) in a study done on 435 people with unilateral transtibial or transfemoral (above and below knee) disabilities, have found out that %52.4 of the participants reported the risk of falling, and % 49.2 have not reported the fear of falling [6]. They concluded that falling and the fear of falling is widespread among people with disabilities [6, 7].
Research findings show that exercise may function as an intervening therapy to improve balance control and posture among the amputee and thus could be considered as a therapeutic tool by experts and occupational therapists. In this regard, Damayanti-Sethy et al. (2009) have investigated the effect of balance exercises on controlling balance among people with unilateral lower limb amputation [8]. In doing so, thirty people with lower limbs amputation (above knee and below knee) were selected and put into two groups of 15. The control group received routine daily activities and the experiment group engaged in balance exercise program while doing their routine daily activities. The program last four weeks and five days a week, 30 minutes each day. The results
showed that the intervention of balance exercises was effective in promoting balance ability in people with unilateral lower limb amputation [8]. In another study, Barnett et al. (2013) have studied the adaptive responses in postural control among transtibial amputee after discharge from rehabilitation program. In this research, dynamic balance was manipulated in disturbed and non-disturbed conditions. Seven transtibial unilateral amputees underwent Sensory Organization Test (SOT) and Limits of Stability (LOS) test with NueroCom Equitest apparatus, following one, three, or six months after discharge from a rehabilitation center. In general, balance had been significantly improved after discharge using somatosensory perception and limiting hip strategy. There wasn’t any significant change in the reaction time and speed of movement at any direction in LOS test. However, the movement of COG decreased significantly [9].
Occupational therapists and researchers use the exercise therapy protocols in rehabilitating people with lower limb amputation. Furthermore, researchers agree that among the sensory data which is effective on balance and falling, the sense of sight has a more important role in maintaining balance by creating changes in the head’s position and its movements in relation to the surrounding environment [10].
52 participated in this project after four days of
therapy; feeling of pain using VAS and UPS before and after intervention was compared. The findings showed that mirror therapy interventions and electrical intradermal stimulation are effective procedures in decreasing pain temporally. However, there was no difference between two groups in feeling pain in the long run [15].
The aim of rehabilitating individuals with lower limb amputation is to re-enable them to walk, gain independency in movements, save energy in walking, maintain balance and control posture. Given the possible effect of exercise interventions on postural control among individuals with lower limb amputations, one of the requirements of the present research is to design balance exercise protocols using mirror feedback and to investigate the influence of these exercise protocols on the degree of balance among this population under conditions of sight, vestibular, and proprioception data manipulation. The effect of exercise interventions where all three sensory data – sight, hearing, and proprioception – are available for the patient with amputation has already been studied. The present research intends to investigate whether designing balance training protocols using mirror has a different effect on controlling posture among individuals with lower limb amputation under manipulation of sight, vestibular, and proprioception data in six different conditions. Researchers have noted that
assessment depending on self-reporting of balance and multi-dimension movements in individuals with leg amputation is common procedures in previous studies. Researchers and therapist have rarely used clinical assessments of balance abilities using more developed and reliable tools [16]. Balance and postural control of individuals with lower limb amputation has mostly been studied by various clinical tools such as Berg balance test, Burpee balance test, Star test, and using questionnaire and some field tests [17, 18, 19].
Among rehab physicians, the most commonly used test based on the ability to maintain balance has been Berg’s Balance Scale [20]. Though these practical tools have proven their efficiency with regard to assessing the balance performance of people with limb amputation [18]. the potentiality of these questionnaires and field studies in identifying the nature of balance disorders in the amputee is limited, hence necessitating the need for using balance control tests and exact posture tests. Also, until now, there aren’t any studies which examine the additive effect of balance training with mirror training together on the balance control in amputee individuals. Therefore, the purpose of the present study was to examine the effect of balance and mirror training on balance control under six different sensory conditions during exercise interventions in amputee individuals.
METHODS
Participants. The present research is quasi-empirical with a pre-test, post-test design and a control group. Twenty-one people with transtibial amputations (7 people in control group, 7 in mirror balance group, and 7 in balance group) were recruited. These people participated in the project by an announcement made by Tehran’s Red Cross Research Center. The sample was chosen by entrance and exit criteria.
Entrance criteria were unilateral transtibial amputation, age 25-60, no skeletal
muscle disorder or movement disabilities to stand and walk, the amputation was due to disease or accident, and the amputee can walk a flat distance of 45 meters with or without assistance. In case one of these criteria did not exist, or the participants were not willing to continue intervention exercises, they were dropped out of the study. This study was in accordance with the ethical standards of the 1964 Helsinki declaration.
To asses postural control and balance of the examinee, posturography, one of the most developed systems in analyzing and manipulating effective sensory systems in postural control was used [21]. Sensory Organization Test (SOT) was done in the research to assess six sensory conditions. In three conditions, the power platform is stable, and in the other three conditions, the platform moves along and against the walking person. In the first condition, the amputee is placed on the posturography where all the involved sensory data in controlling posture (sight, hearing, and proprioception) are accessible. In the second condition, the examinee is blindfolded (elimination of sight information). In the third condition, the eyes are open, but the sight environment is dynamic in such a way as to produce false sight perception. In the fourth condition, the power plates are moving; therefore, proprioception data is eliminated. In the fifth condition, the examinee is blindfolded and the moving power plate eliminates proprioception. In this condition, the effect of vestibular system in postural control is tested. Similarly, in the sixth condition, the data of vestibular system in postural control is assessed where the proprioception data has been eliminated, and visual figures are presented to the examinees. Each test lasts 20 seconds, and each condition is repeated three times [21].
Procedure. At first, an ethical agreement was prepared by the committee of ethics in Tehran’s Red Cross Organization and the examinee were asked to fill in the form if they were willing to cooperate. The objectives and stages of the research were fully explained to the amputee. They were assured that confidentiality will be observed in data saving and the data has only research values and will not be used otherwise.
After the announcement, the volunteers with the needed requirements were chosen and then randomly divided into three groups of balance, mirror balance, and control. First, to determine alignment scores and displacement of the center of gravity in six sensory conditions,
the examinee underwent a test by Computerized Dynamic Posturography in the pre-test stage.
The distance between the two legs to be placed on the power plate was measured based on the width of the hip and was considered equal to 50 percent of hip to hip distance (Anterior-Superior Iliac Spine). The obtained distance for each person in all six sensory conditions and in both pre and post-test stage was considered as a criterion for positioning the legs. All the stages of the test were conducted in the Rehabilitation Center of Red Cross in Iran. The environment for conducting the test had enough light and ventilation with suitable temperature. Also, during the test there was complete silence and equal conditions for everyone during the pre and post-test was prepared. Before carrying out the pre-test all the points in the research guide were presented to the groups.
In the pre-test stage, the examinee had to stand on the power plate of the posturography while barefooted and with their hands on their sides [22]. Furthermore, to prevent disturbance and disorder in the vestibular system, they were asked to look straight ahead and do not move their heads [23]. In all the stages of Sensory Organization Test (SOT), the variables of alignment and displacement of center of gravity were measured. This test assesses the role of proprioception, vestibular, and sight information in controlling posture, which has six conditions for manipulating sensory data. Each test condition lasts 20 seconds with 10 seconds interval between the tests. In the break time, the next stage in SOT was explained to the examinee. During all stages of the test, no feedback was given. Each sensory condition was repeated for three times and the mean for kinetic variables in the three tests were considered [21].
54 The mirror balance group had the same
schedule, except for the fact that they performed their exercises in front of a mirror. The control group just attended the pre-test session, and did not have intervention exercises, and only
continued their routine daily activates. In Table 1 the most important movements in the exercise protocol are presented.
Table 1: Selected exercises used in training protocols
The exercise sessions were held between 9-12 a.m. each day at the Red Cross gym center. At first, the position and size of the mirror for
the mirror balance intervention exercise group was proved. The correct way of doing the exercises was explained to the examinee and all necessary elaboration was given to them in written format too. To control the exercises each
Warm up (10 minutes) Stretching exercises of knee and hip,
lying on back or abdomen and pressing down the buttocks, putting a pillow or a ball between the thighs and hips and pressing above the knee, lying on back and pressing the stump to the bed, sideling on the intact thigh with knee slightly bent for support and elevating the stump up to the ceiling with straight hip , lying down on back and raising the stump as much as possible, raising the pelvic when lying on back and bridging up, sitting on a chair with intact knee bent and straightening the stump as much as possible
Specialized balance training for two groups
15 minutes for the first session
The exercise time were increased 5 minutes each week
Partial weight bearing (without support): Shift the body weight
from the sound leg to the prosthetic leg.
Sound-leg step through (without support): Step forward and backward with the sound leg, holding the prosthesis slightly in adduction.
Side Stepping
Balancing a stick: Stand a stick upright on your hand.
Rising from a chair: Place the sound leg under the chair and flex the trunk.
Side-to-Side Balance
Cross over
Sitting down and getting up from the floor (method 1: forward) (method 2: backward)
Braiding
Walking between the parallel bars (without support)
day necessary points regarding the whole process was explained to the participants. After finishing the balance exercise protocols, in the post-test the variables of alignment and displacement of center of gravity in all the six sensory conditions for three groups were reassessed by the Computerized Dynamic Posturography, similar to the pre-test conditions.
Data analysis. Descriptive statistics mean and standard deviation was used to draw the figures.
A 3 (control group, balance exercise, and balance exercise using mirror) × 2 (pre-test and post-test measurement) × 6 (conditions of sensory data manipulation) mixed ANOVA with repeated measurements on the last two factors and also Bonferroni post-hoc test were used to analyze the data. The data were analyzed in SPSS (version 19) with a significance level of (P≤0.05).
RESULTS
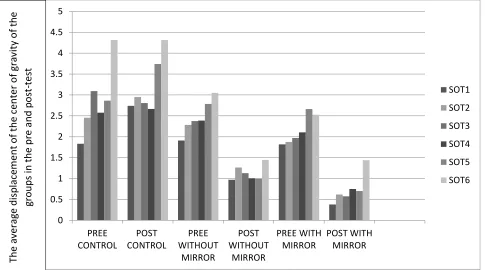
The results of the 3(groups) × 2(time) × 6(SOT) mixed ANOVA with repeated measurements on the last two factors for balance showed that the main effect of the group was significant (P≤0.05). according of the Bonferroni post-hoc test, the mean displacement of center of gravity in mirror balance group (Mean=1.45) was significantly less than the mean displacement of center of gravity in control group (Mean=3.02) and balance group (Mean=1.80). Hence people with lower limp amputation in mirror balance group had less fluctuation and better balance in comparison to the control group.
The interactive effect of conditions (six manipulation conditions; SOT) and the groups (control, balance exercise, and balance exercise using mirror) was also significant (P=0.03). Comparing the mean index of displacement of the center in different conditions and groups shows that the mean index in all six conditions, especially in the sixth condition (manipulation of vestibular and proprioception), for the balance group (Mean=1.24) and for the mirror group (Mean=1.98) are less than the six conditions in control group, which indicates a decrease in fluctuation and a better balance in the balance and mirror balance groups. Furthermore, comparing the means shows that the examinee in the first condition (existence of sight, vestibular, and proprioception) in the balance and mirror balance groups had a lower mean displacement of center of gravity and a better balance.
The interactive effect of assessment time (pre-test and post-test) was significant in the groups (control, balance exercise, and balance exercise using mirror) (P=0.002). Comparing the means of displacement of center of gravity in the groups showed that the mean index in post-test for the balance group (Mean=1.13) and mirror balance (Mean=0.74) were lower than control group (Mean=3.20), which indicates the decrease of fluctuation and a better balance in balance and mirror balance groups.
The interactive effect of condition (six manipulation conditions) during the assessment (pre-test and post-test) was not significant (P=0.18). Comparing the means index of the displacement of center of gravity showed that the mean displacement of center of gravity in the post-test stage is better than the mean displacement of center of gravity in control group in all the six conditions, and the examinee in the balance and balance exercise using mirror groups in the post-test of first condition (existence of sight, hearing, and proprioception) and of the second condition (elimination of sight) had better balance in comparison to other stages (P≤0.05).
56 The difference of mean displacement of
center of gravity between three groups was significant (P=0.001). Comparing the means shows that the displacement of center of gravity
of the examinee in the balance and balance exercise using mirror groups is lower than control group (Figure 1).
Figure 1: Average yield shift of the center of gravity in three groups at the pre and post-test
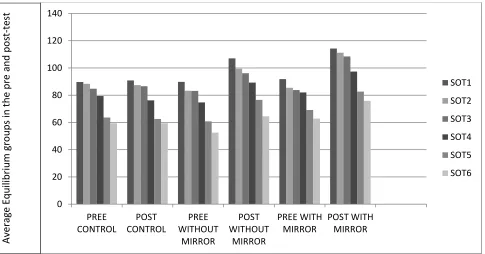
The results of the 3(groups) × 2(time) × 6(SOT) mixed ANOVA with repeated measurements on the last two factors for stability variable showed that the main effect of the group was significant (P=0/001). Bonferroni post-hoc test in comparing the groups showed that the mean of stability score in the mirror balance group (Mean=88.74) is higher than control (Mean=77.33) and balance (Mean=81.40) groups, and so the lower limb amputee had a better balance in mirror balance group. However, there was not any significant difference in the mean of stability score between the balance and control groups.
The interactive effect of condition (six manipulation conditions) was not significant in the groups (control, balance exercise, and balance exercise using mirror) (P=0.79).
The interactive effect of assessment time (pre-test and post-test) was significant in the groups (control, balance exercise, and balance exercise using mirror) (P=0.001). Comparing the mean of stability index in the groups showed that the index of mean in post-test for the balance group (Mean=88.78) and mirror balance group (Mean=98.31) were higher than control group (Mean=77.14), which indicates balance 0
0.5 1 1.5 2 2.5 3 3.5 4 4.5 5
PREE CONTROL
POST CONTROL
PREE WITHOUT
MIRROR
POST WITHOUT
MIRROR
PREE WITH MIRROR
POST WITH MIRROR
SOT1
SOT2
SOT3
SOT4
SOT5
SOT6
The
av
erag
e disp
lace
m
ent
o
f t
h
e c
ent
er
o
f gr
av
ity
o
f t
h
e
gro
u
p
s in the pr
e
an
d
p
o
st
-te
improvement in balance and mirror balance groups.
The interactive effect of condition (six manipulation conditions) and time of assessment (pre-test and post-test) was not significant for the stability variable (P=0.09). The interactive effect of condition (six manipulation conditions) during assessment (pre-test and post-test) in the groups (control, balance exercise, and balance exercise using mirror) was not significant (P=0.31). However, comparing the means of the
stability index in conditions over time showed that the mean of stability index of post-test assessment was better in all the six conditions than the mean of stability index in control group in pre-test and post-test assessment. The examinee in the balance and balance exercise using mirror groups had better performance in the post-test of the first (existence of sight, vestibular, and proprioception), and the second condition (elimination of sight and existence of vestibular and proprioception) (Figure 2).
Figure 2: Average yield stability of three groups in the pre and post-test
DISCUSSION
The purpose of the present research was to compare the effect of a selected balance and balance exercise using mirrors program on postural control among lower limb amputee under the conditions of afferent sensory data manipulation by using the Computerized Dynamic Posturography. Analyzing the degree of displacement of center of gravity and stability in control, balance exercise, and balance
exercise using mirror groups under the conditions of sensory data manipulation showed that the balance scores of the amputee in balance and balance exercise using mirror groups improved in the post-test, and this improvement is more in balance exercise using mirror groups. The results were consistent with some previous findings [13, 14, 15]. It seems that beginning therapy before prosthesis, enhances the balance 0
20 40 60 80 100 120 140
PREE CONTROL
POST CONTROL
PREE WITHOUT
MIRROR
POST WITHOUT
MIRROR
PREE WITH MIRROR
POST WITH MIRROR
SOT1
SOT2
SOT3
SOT4
SOT5
SOT6
Ave
rag
e E
q
u
ilib
riu
m
gr
o
u
p
s in the pr
e
an
d
po
st
-te
58 and walking ability, and hence helps the
amputee to be sooner independent in doing activities of daily living [24].
Notarnicola, et al. (2014) have investigated the effect of ballad learning with and without mirror on young female students’ balance. Their finding showed that using a mirror in the class, for 6 months could improve the movement skills and balance of the ballerinas [14]. Mohan, et al. (2013) have investigated the effectiveness of therapy with mirror in improving lower limb movements, balance, and movement in patients after acute brain stroke, concluding that mirror therapy after brain stroke has improved the patients’ movement [13]. Tilak, et al. (2015) have researched the effect of mirror therapy and electric intradermal neurological stimulation for controlling phantom limb in the amputee. After 4 days of therapy, the pain was measured again by the therapist. The findings showed that both forms of intervention, mirror therapy and electric intradermal neurological stimulation were effective in reducing pain temporally. However, no difference between the two groups was observed [15]. Mc Cormick et al. (2014) and Rothgangel, et al. (2011) have stated that one promising suggestion for the unilateral amputee, is exercise in front of mirror, which allows the patient to see his/her phantom limb as a reflection of his/her intact limb [25, 26]. Research on the mechanisms of mirror therapy in brain’s functions and its plasticity has been exponentially increasing. Most studies have used neuropsychological measurement tools, such as fMRI, Lateral Readiness Potential: LRP and Motor Evoked Potential: MEP, during mirror intervention therapy. In various theories, researchers have discussed the role of mirror cells systems and the primary motor cortex when exercising in front of mirror in increasing the performance of the amputee [27, 28, 29]. It seems that one of the reasons for the stronger effect of balance exercises in front of mirror, is that the patient has a pleasant feeling when he/she sees his/her healthy limb moving, and simultaneously looking at the mirror, feeling to
be able to move the amputated limb. Even if it is not the reality, but the mirror boosts motivation, confidence, and self-sufficiency in doing tasks among people with lower limb amputation.
While most researchers have accepted the therapy as a routine treatment for the amputee, the findings of the present study aren’t consistent with the initial findings of Mohan, et al. (2013), in that study, using mirror intervention therapy after brain stroke in comparison to conventional rehabilitation methods, lower limb movement or balance weren’t improved [13]. Of the reasons for this inconstancy could be the population involved, because in Mohan et al. (2013)’s research the participants suffering a brain stroke while in the present study the participants had a lower limb amputation.
biofeedback coherent by using the reflected image of their body on the mirror to improve their upright stance [32]. Of the reasons for this latter inconsistency could be different method of introducing visual data and different assessment tools by Hlavackova, et al. (2009) and Damayanti-Sethy et al. (2009) have investigated the effect of sight and hearing exercises for controlling balance, and have pointed out that sight and hearing feedback can improve the balance in the amputee [8, 32]. This is inconsistent with the findings of the present study. One of the reasons for this inconsistency might be the fact that Nicholas et al. have used different tools for assessing balance. The examinee of the balance and mirror balance groups in post-test of sixth condition (manipulation of vestibular and proprioception), had lower performance and balance than other stages. Peterka, (2002) has stated that healthy people rely %70 on proprioception, %20 on vestibular and %10 on sight, to control posture. They have shown that the coherence of the data received by these three senses plays a pivotal role in postural control [33]. Given these studies and the findings in the present study, the manipulation of two or three senses at the same time causes imbalance in the amputee.
In summary, the results of the present study have shown that a period of balance and balance exercise using mirror can improve balance and
stabilize posture in individuals with a lower limb amputation. It has also been found that in comparison to the control group, the stability mean score and the displacement of center of gravity improved in both balance and balance exercise using mirror groups and in all of the six sensory conditions. The balance improvement in exercise groups in the first (existence of three senses) and second condition (elimination of sight) has been higher than other conditions. Moreover, the findings show that the mean score of stability and displacement of center of gravity in balance exercise using mirror groups are better than other groups (control and balance). Postural stability is very important in standing still, moving, and any activity which requires a high degree of balance [11]. An impairment in balance control and postural stability may be due to the adaptation in the functional tissue, neuro– muscular response, or continuing an unnatural form of gait and movement. These changes can lead to spinal instability, bone movement beyond the physiological limits and pain [34]. According to Geurts and Mulder, (1992) relearning balance and postural control is necessarily required in everyone’s recovery program [35]. The implementation of rehabilitation interventions and exercises program would be more useful when it could meet all the needs for balance and postural control, and improve the controlling variables involving balance and posture.
CONCLUSIONS
Based on the finding in the present study, it is recommended that occupational therapists, physiotherapists, and rehabilitation experts design and use balance and balance exercise using mirrors to improve postural control in lower limb amputee especially in difficult conditions where two or three senses of afferent data do not exist. Since the samples of the present study were above amputee, it is recommended that further research be done on the other sight amputation.
CONflICT OF INTEREST STATEMENT. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
60
REFERENCES
1. Van Velzen, JM., van Bennekom, CA., Polomski, W., Slootman, JR., van der Woude, LH., Houdijk, H. Physical
capacity and walking ability after lower limb amputation: a systematic review. Clinical Rehabilitation, 2006. 20: 999-1016.
2. Miller, WC., Speechley, M., Deathe, AB. Balance confidence among people with lower-limb amputations. Physical
Therapy, 2002. 82: 856–865.
3. Wu, G., Chiang, JH. The effects of surface compliance on foot pressure in stance. Gait and Posture, 1996.
4:122-129.
4. Mancini, M., Horak, FB. The relevance of clinical balance assessment tools to differentiate balance deficits. European Journal of Physical Rehabilitation Medicine, 2010. 46:239-248.
5. Stevens, JA., Corso, PS., Finkelstein, EA., Miller, TR. The costs of fatal and non-fatal falls among older adults. Injury Prevention, 2006.12:290-295.
6. Miller, WC., Deathe, AB., Speechley, M., Koval, J. The influence of falling, fear of falling, and balance confidence on prosthetic mobility and social activity among individuals with a lower extremity amputation. Archives of Physical Medicine and Rehabilitation, 2001.82:1238-1244.
7. Miller, WC., Deathe, AB. A prospective study examining balance confidence among individuals with lower limb
amputation. Disability and Rehabiltation, 2004.26:875-881.
8. Damayanti Sethy, MO., Kujur, ES., Sau, K. Effect of balance exercise on balance control in unilateral lower limb
amputees. Indian Journal of Occupational Therapy, 2009.41:63-68.
9. Barnett, CT., Vanicek, N., Polman, RC. Postural responses during volitional and perturbed dynamic balance tasks
in new lower limb amputees: A longitudinal study. Gait and Posture, 2013.37:319-325.
10. Bottini, G., Karnath, HO., Vallar, G., Sterzi, R., Frith, CD., Frackowiak, RS., Paulesu, E. Cerebral representations for egocentric space. Brain, 2001.124:1182-1196.
11. Ramachandran, VS., Rogers-Ramachandran, D. Synaesthesia in phantom limbs induced with mirrors. Proceedings
of the Royal Society of London, 1996.263:377-386.
12. Sütbeyaz, S., Yavuzer, G., Sezer, N., Koseoglu, BF. Mirror therapy enhances lower-extremity motor recovery and
motor functioning after stroke: a randomized controlled trial. Archives of Physical Medicine and Rehabilitation, 2007.88:555-559.
13. Mohan, U. Effectiveness of mirror therapy on lower extremity motor recovery, balance and mobility in patients with acute stroke: a randomized sham-controlled pilot trial. Annals of Indian Academy of Neurology, 2013.16:634-639. 14. Notarnicola, A., Maccagnano, G., Pesce, V., Di Pierro, S., Tafuri, S., Moretti, B. Effect of teaching with or without
mirror on balance in young female ballet students. BMC Research Notes, 2014.7:426-433.
15. Tilak, M., Isaac, SA., Fletcher, J., Vasanthan, LT., Subbaiah, RS., Babu, A., Bhide, R., Tharion, G. Mirror Therapy and Transcutaneous Electrical Nerve Stimulation for Management of Phantom Limb Pain in Amputees—A Single Blinded Randomized Controlled Trial. Physiotherapy research international: the journal for researchers and clinicians in physical therapy, 2015. Apr 1. Doi: 10.1002/pri.1626.
16. Wong, CK., Chen, CC., Welsh, J. Preliminary assessment of balance with the Berg Balance Scale in adults who
have a leg amputation and dwell in the community: Rasch rating scale analysis. Physical Therapy, 2013. 93:1520-1529.
17. Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the" get-up and go" test. Archives of Physical Medicine and Rehabilitation 1986;67:387-389.
18. Condie, E., Scott, H., Treweek, S. Lower limb prosthetic outcome measures: a review of the literature 1995 to 2005. JPO Journal of Prosthetics and Orthotics, 2006.18:13-45.
19. Shumway-Cook, A., Woollacott, MH. Motor control: translating research into clinical practice. Lippincott Williams & Wilkins, 2007.
20. Tyson, SF.,Connell, LA. How to measure balance in clinical practice. A systematic review of the psychometrics and clinical utility of measures of balance activity for neurological conditions. Clinical Rehabilitation, 2009.23:824-840. 21. Ferber-Viart, C., Ionescu, E., Morlet, T., Froehlich, P., Dubreuil, C. Balance in healthy individuals assessed with Equitest: maturation and normative data for children and young adults. International Journal of Pediatric Otorhinolaryngology, 2007.71:1041-1046.
22. Rinaldi, NM., Polastri, PF., Barela, JA. Age-related changes in postural control sensory reweighting. Neuroscience Letters, 2009.467:225-229.
23. Arnold, BL., Schmitz, RJ. Examination of balance measures produced by the Biodex Stability System. Journal of
24. Dorta, HS. Physical Therapy in the pre and post the transtibial amputation. International Journal of Archives of Physical Medicine and Rehabilitation, 2015.3:276. doi:10.4172/2329-9096.1000276
25. McCormick, Z., Chang‐Chien, G., Marshall, B., Huang, M., Harden, RN. Phantom Limb Pain: A Systematic
Neuroanatomical‐Based Review of Pharmacologic Treatment. Pain Medicine, 2014.15:292-305.
26. Rothgangel, AS., Braun, SM., Beurskens, AJ., Seitz, RJ., Wade, DT. The clinical aspects of mirror therapy in rehabilitation: a systematic review of the literature. International Journal of Rehabilitation Research, 2011.34:1-13. 27. Fukumura, K., Sugawara, K., Tanabe, S., Ushiba, J., Tomita, Y. Influence of mirror therapy on human motor cortex.
International Journal of Neuroscience, 2007.117:1039-1048.
28. Touzalin-Chretien, P., Dufour, A. Motor cortex activation induced by a mirror: evidence from lateralized readiness potentials. Journal of neurophysiology 2008;100:19-23.
29. Matthys K, Smits M, Van der Geest JN, Van der Lugt A, Seurinck R, Stam HJ, Selles RW. Mirror-induced visual
illusion of hand movements: a functional magnetic resonance imaging study. Archives of Physical Medicine and Rehabilitation, 2009.90:675-681.
30. Vrieling, AH., Van Keeken, HG., Schoppen, T., Otten, E., Hof, AL., Halbertsma, JP., Postema, K. Balance control
on a moving platform in unilateral lower limb amputees. Gait & Posture, 2008.28:222-228.
31. Duclos, C., Roll, R., Kavounoudias, A., Mongeau, JP., Roll, JP., Forget, R. Postural changes after sustained neck
muscle contraction in persons with a lower leg amputation. Journal of Electromyography and Kinesiology,
2009.19:214-222.
32. Hlavackova, P., Fristios, J., Cuisinier, R., Pinsault, N., Janura, M., Vuillerme, N. Effects of mirror feedback on upright stance control in elderly transfemoral amputees. Archives of Physical Medicine and Rehabilitation, 2009.90:1960-1963.
33. Peterka, RJ. Sensorimotor integration in human postural control. Journal of Neurophysiology, 2002.88:1097-1118.
34. Hendershot, BD., Nussbaum, MA. Persons with lower-limb amputation have impaired trunk postural control while
maintaining seated balance. Gait & Posture, 2013.38:438-442.