1
Comprehensive comparison of the performance of six prognostic signatures
1
for estrogen receptor positive breast cancer
2
3
Ivana Sestak PhD1, Richard Buus PhD2,3, Jack Cuzick PhD1, Peter Dubsky MD4,5,
4
Ralf Kronenwett MD6, Carsten Denkert MD7, Sean Ferree PhD8, Dennis Sgroi MD9,
5
Catherine Schnabel PhD10, Frederick L. Baehner MD11, Elizabeth Mallon PhD12,
6
Mitch Dowsett PhD2,3
7
8
1. Centre for Cancer Prevention, Queen Mary University of London, London, UK
9
2. Ralph Lauren Centre for Breast Cancer Research, Royal Marsden, London,
10
UK
11
3. Breast Cancer Now Research Centre at The Institute of Cancer Research,
12
London, UK
13
4. Medical University of Vienna, Austria
14
5. Klinik St. Anna, Luzern, Switzerland
15
6. Sividon Diagnostics GmbH, Köln, Germany
16
7. Charité Universitätsmedizin and German Cancer Consortium (DKTK), Berlin,
17
Germany
18
8. NanoString Technologies, Seattle, USA
19
9. Massachusetts General Hospital, Boston, USA
20
10. Biotheranostics, San Diego, USA
21
11. GenomicHealth, Redwood City, USA
22
12. University of Glasgow, Glasgow, UK
23 24
25
Correspondence to:
26
Ms Ivana Sestak
27
Centre for Cancer Prevention
28
Wolfson Institute of Preventive Medicine
29
Queen Mary University London
30
Charterhouse Square
31
London, EC1M 6BQ
32
United Kingdom
33
Tel.: +442078823522
34
Email: [email protected]
35 36
Word count: 3023
37
Date of revision: 01/12/2017
2
Key points
39
Question: What is the comparative performance of prognostic multigene signatures
40
for prediction and risk stratification of overall and late distant recurrence in ER
41
positive/HER2 negative breast cancer?
42
Findings: In this retrospective biomarker analysis, we found that a combination of
43
multigene expression test with clinical information improved the prognostic value for
44
the prediction of distant recurrences and risk stratification, specifically in women with
45
node-positive disease. Clear differences for the prediction of late distant recurrence
46
were observed where these tests may be valuable for decision-making with regards
47
to extended endocrine treatment.
48
Meaning: The combination of clinical and molecular information enhanced the
49
prognostic value for the prediction of distant recurrence and risk stratification for
ER-50
positive, HER2-negative breast cancer, particularly for women with node positive
51
disease.
3
Abstract
53
Importance:Multiple molecular signatures are available for managing estrogen
54
receptor positive (ER+) breast cancer patients but little direct comparative
55
information to guide their choice.
56
Objective: To conduct a within-patient comparison of the prognostic value of
57
Oncotype Dx (RS), ProSigna (ROR), EndoPredict (EPclin), Breast Cancer Index
58
(BCI), and IHC4 in women with early ER+ breast cancer treated with 5 years’
59
endocrine therapy.
60
Design: Retrospective biomarker analysis.
61
Setting: Randomized clinical trial of 5 years’ of anastrozole versus tamoxifen
62
(ATAC) with 10-year follow-up.
63
Participants: 774 postmenopausal women with ER+ /HER2-negative breast cancer
64
with results for all tests.
65
Main Outcomes: The primary objective was to compare the added prognostic value
66
of these signatures on top of the Clinical Treatment Score (nodal status, tumor size,
67
grade, age, endocrine treatment) for distant recurrence (i) for years 0-10, and (ii) for
68
years 5-10 after diagnosis. Likelihood ratio statistics (LR-χ2
) were used to assess the
69
prognostic value of each signature.
70
Results: In women with node-negative disease (N=591), the signatures providing
71
the most prognostic information were ROR, followed by BCI, and EPclin. Each
72
provided significantly more information than CTS, RS, and IHC4. Substantially less
73
information was provided by all of the molecular tests for patients with 1-3
node-74
positive disease (N=183), but BCI and EPclin provided more additional prognostic
75
information than the other signatures.
4
Conclusions and Relevance: For women with node-negative disease, ROR, BCI,
77
and EPclin were significantly more prognostic for overall and late distant recurrence.
78
For women with 1-3 positive nodes limited independent information was available
79
from any test. These data will help oncologists and patients to choose the most
80
appropriate test to aid considerations of chemotherapy use and/or extended
81
endocrine therapy.
82
5
Introduction
84
Almost all women with estrogen receptor (ER) positive primary breast cancer are
85
offered adjuvant endocrine therapy and a highly relevant clinical question is who
86
remains at high risk for distant recurrence despite completion of primary adjuvant
87
therapy. Multigene expression profiles have significantly increased our ability to
88
predict distant recurrence in ER-positive breast cancer following surgery and
89
endocrine treatment [1]. These signatures are used in combination with different
90
clinical characteristics to aid the selection of patients for whom chemotherapy may
91
be appropriate based on prognosis. Several of these signatures such as the
92
Oncotype Dx Recurrence Score (RS) (Genomic Health), PAM50-based Prosigna
93
Risk of Recurrence Score (ROR) (NanoString), Breast Cancer Index (BCI)
94
(Biotheranostics), EndoPredict (EPclin) (Myriad Genetics), and the NKI 70-gene
95
signature (Mammaprint) (Agendia) are commercially available, endorsed by several
96
guidelines [2-5] and routinely used by clinicians.
97
98
The TransATAC cohort was previously used to develop two prognostic algorithms,
99
the Clinical Treatment Score (CTS), which includes clinicopathological information,
100
and the immunohistochemical score (IHC4), which combines prognostic information
101
of four widely used IHC markers [6]. We have furthermore evaluated four gene
102
expression based signatures in the TransATAC cohort: RS [6], ROR [7], BCI [8], and
103
EPclin [9]. RS and BCI include only molecular information in their signatures, while
104
ROR (tumour size) and EPclin (tumour size and number of positive nodes) integrate
105
clinical information. All of these signatures significantly predicted the risk of distant
106
recurrence, particularly in women with node-negative disease, but with varying
107
amount of prognostic information for late distant recurrence (5-10 years). An
6
important area of research remains to accurately predict the risk of late distant
109
recurrence in women with ER positive disease, as over 50% of recurrences occur
110
after five years of endocrine treatment. Gene expression based signatures should
111
show an improvement in prediction when compared to standard clinical parameters
112
[8, 10, 11].
113
114
There has not been a direct and comprehensive comparison of multigene signatures
115
in the same patient population with long-term follow-up data. Here, we compare the
116
prognostic performance of six signatures for distant recurrence in (i) the 10 years
117
period following diagnosis to assess the potential value of the addition of
118
chemotherapy versus endocrine therapy alone, and (ii) for late distant recurrence in
119
years 5-10 to investigate the potential value of extended adjuvant endocrine therapy.
120
Furthermore, the comparison was performed separately for women with
node-121
negative and 1-3 node-positive disease, since the most significant prognostic clinical
122
indicator for early stage breast cancer is the presence or absence of lymph node
123
involvement.
124
125
126
7
Methods
128
129
Study design and patients 130
In this comparative analysis, tumour blocks from the TransATAC study were used
131
from patients with hormone receptor positive early stage breast cancer treated with
132
five years of tamoxifen or anastrozole in the ATAC randomized clinical trial [12].
133
Micro-dissection of the tumours and RNA extraction was done by Genomic Health
134
Inc. and residual RNA was provided to collaborators for RNA expression profiling.
135
Women were excluded from the analysis if they received chemotherapy, did not
136
have ER-positive disease, received the combination treatment (i.e. anastrozole plus
137
tamoxifen), or had 4 or more positive lymph nodes. All women consented for their
138
tissue to be used in translational research. This study was approved by the
South-139
East London Research Ethics Committee.
140
141
Procedures 142
The CTS and IHC4 were developed in TransATAC and have been described in
143
detail previously [6]. In brief, the CTS contains information on nodal status, grade,
144
tumour size, age, and treatment (tamoxifen versus anastrozole). The IHC4 combines
145
four commonly used IHC markers: estrogen receptor (ER), progesterone receptor
146
(PgR), Ki67, and HER2. The commercial signatures are all based on RNA
147
expression profiling and were performed according to specifications by the individual
148
commercial collaborators, who were all blinded to clinical outcome data. The
149
Oncotype Dx RS [13] is a 21-gene signature that was developed in ER-positive,
150
negative breast cancer patients. RS risk groups were determined in
8
negative patients as previously described [13], using predefined cut-offs of 18 and 31
152
to determine low, intermediate, and high risk groups, respectively. The
RS-153
Pathology-Clinical (RSPC) score was calculated using the website tool for
node-154
negative patients [14, 15]. BCI [16, 17] combines the HOXB13/IL17BR ratio with the
155
molecular grade index (MGI; five proliferation genes) in a linear model and was
156
developed in postmenopausal breast cancer patients with ER-positive, lymph-node
157
negative disease [8]. Cut-off points for BCI were determined in a node-negative
158
population (low risk < 5.0825, high risk >6.5025) [18]. The Prosigna ROR score [7]
159
incorporates 46 genes and was developed in pre- and postmenopausal women
160
treated without any adjuvant systemic therapy, and includes information on tumour
161
size. The TransATAC cohort was used to determine the cut-off points for Prosigna
162
ROR for risk stratification in node-negative and node-positive patients separately.
163
They correspond approximately to a point estimate of up to 10% distant recurrence
164
rate for low risk, and more than 20% rate for high risk after ten years of follow-up
165
[19]. EPclin was developed in pre- and postmenopausal tamoxifen-treated patients
166
with ER-positive, HER2-negative breast cancer. It incorporates the expression of 12
167
genes plus information on tumour size and nodal status [20]. A pre-defined cut-off
168
point (EPclin=3.3, based on [20]) was used for risk stratification, which corresponds
169
to a 10% distant recurrence risk at 10 years.
170
171
Statistical analysis 172
The primary endpoint was time to distant recurrence. Distant recurrence was defined 173
as metastatic disease, excluding contralateral disease, and locoregional and 174
9 event. We defined two primary analysis populations: firstly patients with ER-positive, 176
HER2-negative, node-negative breast cancer, and secondly patients with ER-177
positive, HER2-negative breast cancer with 1 to 3 positive lymph nodes. The primary 178
objective was the comparison of prognostic signatures in negative and node-179
positive patients separately, for two specific follow-up periods: overall (0-10 years) 180
and late (5-10 years). 181
182
We assessed overall distant recurrence in the first 10 years after diagnosis (N=774)
183
and late distant recurrence within the subset of patients who remained distant
184
recurrence free for the first five years after diagnosis (N=689). Partial likelihood ratio
185
tests based on Cox regression models were used to test the prognostic information
186
of all signatures. The amount of prognostic information provided by each signature
187
alone was assessed by C-indices. Furthermore, partial likelihood ratio χ² value
(LR-188
χ²), with a two-side 5% significance level (LR-χ²=3.84) are also presented. The
189
improvement in distant recurrence prediction of each signature over clinical and
190
pathological variables (CTS) was quantified by the increase of the likelihood ratio χ²
191
value (ΔLR-χ²; two-sided 5% significance level). Pre-defined cut-off points were used
192
to determine risk stratification for the four commercially available signatures. Kaplan–
193
Meier curves were used to estimate the average risk of distant recurrence after 10
194
years of follow up in pre-defined risk groups. To compare the prognostic
195
performance of all signatures, continuous scores were normalised to have unit
196
variance and the hazard ratios and associated 95% confidence interval (CI) were
197
estimated from Cox models. All statistical analyses were two-sided, and a P-value of
198
less than .05 was regarded as significant. All analyses were performed with STATA
199
version 13.1 (College Station, Texas, USA).
11
Results
202
A total of 774 postmenopausal women with ER-positive, HER2-negative disease for
203
whom we had all signatures available were included in this analysis (eFigure 1). 591
204
women had node-negative disease, with a mean age of 63.4 years (standard
205
deviation (SD) 7.9) and a mean tumour size of 17.6mm (SD 8.5). A total of 58 distant
206
recurrences (9.8%) were recorded for this population, with approximately half of
207
distant recurrences (N=34) occurring in the late follow-up period (eTable 1). In
208
contrast, women with 1-3 node-positive disease (N=183) were significantly older
209
(mean age 66.4 (SD 8.3)) and had significantly larger tumours (mean size 24.2mm
210
(SD 12.2)) than node-negative women (eTable 1). 40 distant recurrences were
211
recorded over 10 years of follow-up, with 21 of them occurring 5 years post
212
diagnosis. Results of the prognostic performance of all six signatures for the overall
213
population (node-negative and node-positive combined) and C-indices are shown in
214
eTable 2.
215
216
Years 0-10
217
Node-negative population 218
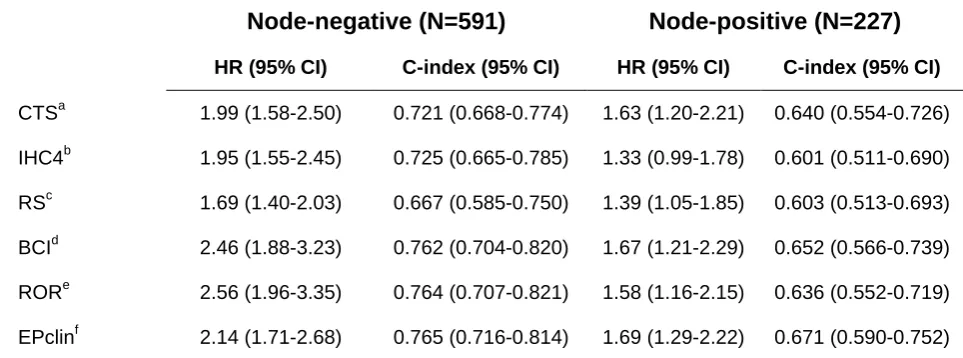
All six signatures provided statistically significant prognostic value for distant
219
recurrence in years 0-10 and all HRs and C-indices are shown in Table 1.ROR
220
(HR=2.56 (95% CI 1.96-3.35)), BCI (HR=2.46 (95% CI 1.88-3.23)), and EPclin
221
(HR=2.14 (95% CI 1.71-2.68)) provided statistically more prognostic than the other
222
signatures in this patient population. The CTS (HR=1.99 (95% CI 1.58-2.50)) and
223
IHC4 (HR=1.95 (95% CI 1.55-2.45)) provided similar amounts of prognostic
224
information in this time period (Table 1, eFigure 2). All signatures provided
12
independent prognostic information beyond the CTS for women with node-negative
226
disease, in particular BCI and ROR provided the most prognostic value (eFigure 2).
227
228
We determined 10-year DR risks for the four commercially available multigene
229
signatures using pre-defined cut-off points (Figure 1). All four signatures identified a
230
large proportion of women who were at low risk of developing a distant recurrence
231
(<10%) after 10 years of follow-up. EPclin only has two risk groups, and categorised
232
429 (73%) of women into the low risk group of which 27 (10-year DR=6.6%)
233
developed a distant recurrence (Figure 1). Only 10% of patients were categorised
234
into the high risk group by RS, and they had a 10-year DR risk of 27%. EPclin, BCI,
235
and ROR identified larger proportions of women as high risk, who had a 10-year DR
236
risk of 22%, 27%, and 32%, respectively (Figure 1). For 507 women we also had
237
information for the RSPC and the incorporation of clinical parameters into the RS
238
substantially improved the prognostic performance for the prediction of distant
239
recurrence compared to the molecular RS alone (data not shown).
240
241
1-3 node-positive population 242
CTS (HR=1.63 (95 CI 1.20-2.21)), BCI (HR=1.67 (95% CI 1.21-2.29)), ROR
243
(HR=1.58 (95% CI 1.16-2.15)), and EPclin (HR=1.69 (95% CI 1.29-2.22)) provided
244
significant prognostic information in this patient population (Table 1). The prognostic
245
performance of all signatures, while significant, was much weaker than for
node-246
negative disease as evidenced by the smaller HRs and C-indices in this patient
247
group. IHC4 did not provide any prognostic value for the prediction of distant
248
recurrence. Apart from the IHC4, all signatures provided independent prognostic
13
information, with BCI and EPclin showing largest improvements beyond the CTS
250
(eFigure 2).
251
252
Risk group stratification is shown in Figure 1. ROR identified a small group of women
253
(N=15) as low risk of whom none developed a distant recurrence at 10 years (Figure
254
1). EPclin categorised 43 women (23.5%) into the low risk group of whom 5.6% had
255
a distant recurrence at ten years. Both signatures identified most women as high risk
256
with an average ten year distant recurrence risk of more than 30%. In contrast, BCI
257
and RS categorised a high proportion of women into the low risk group with a high
258
risk of distant recurrence at 10 years (Figure 1).
259
260
261
Years 5-10
262
Node-negative population 263
To assess the prognostic power of each signature for late distant recurrence, 535
264
women who were alive and without distant recurrence after five years of follow-up
265
were included. HRs and C-indices are shown in Table 2. ROR (HR=2.77 (95% CI
266
1.93-3.96), BCI (HR=2.30 (95% CI 1.61-3.30)), and EPclin (HR=2.19 (95% CI
1.62-267
2.97)) provided significant prognostic value for late distant recurrence (Table 2,
268
eFigure 3), and substantially more than the CTS alone (HR=1.95 (95% CI
1.43-269
2.65)). IHC4 and RS were not significant predictors for late distant recurrence when
270
added to CTS (eFigure 3). BCI, EPclin, and in particular ROR, provided significant
271
independent prognostic information for late distant recurrence beyond the CTS
14
(eFigure 3). RSPC provided twice as much prognostic information for late distant
273
recurrence compared to the RS alone in the univariate analysis, but no additional
274
prognostic value for late distant recurrence above CTS (data not shown).
275
276
All four signatures categorised the majority of women into the low risk group, who on
277
average had a very low distant recurrence risk in years 5-10 of less than 5% (Figure
278
2). EPclin categorised 26.5% of patients into the high risk group, which had the
279
lowest 10-year distant recurrence risk of 14.6%. In contrast the ROR identified over
280
14% of women as high risk, and they had the highest 10-year DR risk of any test
281
(23%) (Figure 2).
282
283
1-3 node-positive population 284
154 women who were alive and did not recur within the first five years of follow-up
285
were included (Table 2, eFigure 3). EPclin provided the most prognostic value for the
286
prediction of late distant recurrence on its own, followed by ROR, and BCI (Table 2).
287
IHC4 and RS did not provide any prognostic information for late distant recurrence
288
univariately or in addition to the CTS (eFigure 3). EPclin and BCI added significant
289
but limited independent prognostic information to CTS (eFigure 3).
290
291
Good risk stratification in this patient group was observed for BCI, ROR, and EPclin
292
(Figure 2). ROR categorised 9.7% of women into the low risk group of whom none
293
developed a late distant recurrence. EPclin identified a larger proportion of women
15
as low risk (26%), of which only one patient developed a distant recurrence by year
295
10. No clear risk stratification was observed for the RS (Figure 2).
296
16
Discussion
298
Multigene signatures have become increasingly important for the prognostic
299
evaluation of ER-positive, HER2-negative breast cancer [6, 21, 22]. Here we
300
compared six prognostic signatures for the prediction of distant recurrence in the
301
TransATAC cohort. In years 0-10, all signatures provided significant prognostic
302
information in women with node-negative disease in addition to clinical variables. For
303
women with 1-3 node-positive disease, the independent prognostic strength of the
304
investigated signatures was much weaker. It should be noted that even though there
305
were fewer patients with node-positive than node-negative disease, the number of
306
distant recurrences was similar and hence provided similar power. For the prediction
307
of late distant recurrence, BCI, ROR, and EPclin provided independent prognostic
308
information among women with node-negative and 1-3 node-positive disease.
309
310
We have previously published the results of the individual evaluations of the four
311
commercial signatures and have shown that all provide significant and similar
312
prognostic information in the first 5 years after diagnosis [6-9]. In this study we have
313
shown that the difference in prognostic performance between signatures over ten
314
years of follow-up is largely due to their differential ability to predict distant
315
recurrence between 5 and 10 years. Thus BCI [8, 23], ROR [24] and, EPclin [9, 10]
316
clearly have molecular components in their signatures that specifically predict late
317
recurrence better than IHC4 or RS. An important finding is that combined genomic
318
and clinical models showed enhanced prognostic performance, particularly for
319
patients with 1-3 positive lymph nodes, and are thus the preferred approach for the
320
decision making process for this patient group. This was furthermore underlined by
17
the finding that the RSPC provided significantly more prognostic value for distant
322
recurrence in node-negative patients than the molecular RS alone.
323
324
In the adjuvant setting, the need for chemotherapy or extended endocrine therapy
325
(for late recurrence) are important clinical questions. We used pre-defined cut-off
326
points to determine the 10-year distant recurrence risk for the commercial scores in
327
years 0-10 (chemotherapy) and years 5-10 (extended endocrine therapy). For
node-328
negative disease, the majority of women were categorised into the low risk group by
329
all four signatures and women had a low average risk<7% where chemotherapy
330
might not be indicated. The two signatures that contain clinical variables in their
331
scores (ROR and EPclin) identified a sizeable group of women with 1-3
node-332
positive disease who had a very low risk of distant recurrence at ten years (average
333
risk<6%), suggesting that chemotherapy would be of very limited benefit in these
334
women.
335
336
None of the signatures were specifically developed to predict late distant
337
recurrences. However, BCI, ROR, and EPclin demonstrated accurate prediction of
338
these late events in our analysis. Wolmark and colleagues reported that the RS was
339
significantly prognostic for the prediction of late distant recurrence, but only in
340
patients with high ESR1 levels [25]. However, we did not observe any relationship
341
between high ESR1 levels and prediction of late distant recurrence with RS in our
342
dataset. A few studies have investigated a series of extended endocrine therapy
343
(EET) with aromatase inhibitors to address the question what the ideal length of
344
extended treatment is. The MA17.R trial [26] showed that ten years of letrozole
18
resulted in significantly higher rates of disease-free survival compared to placebo. In
346
the NSABP-B42 [27], DATA [28], and IDEAL [29] trials no significant improvement in
347
disease-free or overall survival with EET was observed. These data raise the
348
question whether patients need to be specifically selected for EET (i.e. based on
349
high risk for late distant recurrence or high likelihood of benefit from extended
350
therapy).
351
352
Strengths of our study include the mature clinical data with clinical outcome and
353
long-term follow-up, well characterised tissue samples, and data on six prognostic
354
signatures for breast cancer. For all RNA analyses the same extraction of RNA used.
355
For all commercial signatures standardised quantitative methods and analyses were
356
used, and all collaborators were blinded to clinical outcome. Limitations include that
357
our results are only applicable for chemotherapy-free and postmenopausal women.
358
An unintended selection bias might have occurred as sample analyses might have
359
only been possible where sufficient amounts of RNA were available, but all assays
360
yielded reportable results. IHC4, CTS and partially RSPC were trained in the
361
TransATAC cohort thus slightly overestimating their performance in this analysis.
362
The risk group cut-off points of the ROR score were defined in the TransATAC
363
cohort for node-negative and node-positive women separately, therefore optimising
364
the cut-offs to identify a low-risk group with less than 10% risk and high risk group
365
with greater than 20% risk. Finally, our current analysis wasn’t able to assess the
366
ability of these signatures to predict the benefit from chemotherapy or extended
367
endocrine therapy.
19
In summary, the prognostic signatures evaluated provided significant information to
369
help determine appropriate candidates for whom chemotherapy and extended
370
endocrine therapy might not be indicated in patients with ER-positive,
HER2-371
negative breast cancer. In patients with node negative disease, all multigene
372
signatures provided significant and clinically meaningful prognostic information
373
beyond clinical factors. The combination of clinical and molecular information
374
enhanced prognostic performance, particularly for women with node positive
375
disease. All signatures performed similarly in the first 5 years of follow-up, but clear
376
differences in years 5-10 were seen, where these tests may be valuable for
decision-377
making with regards to extended endocrine treatment.
378
379
20
Acknowledgements
381
This work was supported by the Royal Marsden, National Institute of Health
382
Biomedical Research Centre, Breast Cancer Now [CTR-Q4-Y1], and Cancer
383
Research UK [C569/A16891]. The funders had no role in design and conduct of the
384
study; collection, management, analysis and interpretation of the data; preparation,
385
review, or approval of the manuscript; and decision to submit the manuscript for
386
publication.
387
IS had full access to all the data in the study and takes the responsibility for the
388
integrity of the data and the accuracy of the data analysis.
389
IS declares speaker’s fee from Myriad Genetics. PD declares grant support from
390
Agendia, Sividon, Myriad Genetics, Nanostring, and advisory role for Amgen, and
391
speaker’s fee from Myriad Genetics, Sividon, and Amgen. RK is an inventor on the
392
Endopredict patent, employee and previous shareholder of Sividon. SF declares
393
employment and shareholder of Nanostring Technologies. CS declares employment
394
and shareholder of Biotheranostics. FLB declares employment and shareholder of
395
Genomic Health. DM declares fees for advisory board from Genoptix and for lectures
396
from Myriad. All remaining authors have declared no conflict of interest.
397
398
399
400
401
21
References
403
1. Massague, J., Sorting out breast-cancer gene signatures. N Engl J Med, 2007. 356(3): p.
404
294-7.
405
2. Harris, L.N., N. Ismaila, L.M. McShane, et al., Use of Biomarkers to Guide Decisions on 406
Adjuvant Systemic Therapy for Women With Early-Stage Invasive Breast Cancer: American 407
Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol, 2016. 34(10): p.
1134-408
50.
409
3. Duffy, M.J., N. Harbeck, M. Nap, et al., Clinical use of biomarkers in breast cancer: Updated 410
guidelines from the European Group on Tumor Markers (EGTM). Eur J Cancer, 2017. 75: p.
411
284-298.
412
4. Coates, A.S., E.P. Winer, A. Goldhirsch, et al., Tailoring therapies--improving the 413
management of early breast cancer: St Gallen International Expert Consensus on the Primary 414
Therapy of Early Breast Cancer 2015. Ann Oncol, 2015. 26(8): p. 1533-46.
415
5. Senkus, E., S. Kyriakides, S. Ohno, et al., Primary breast cancer: ESMO Clinical Practice 416
Guidelines for diagnosis, treatment and follow-up. Ann Oncol, 2015. 26 Suppl 5: p. v8-30.
417
6. Cuzick, J., M. Dowsett, S. Pineda, et al., Prognostic value of a combined estrogen receptor, 418
progesterone receptor, Ki-67, and human epidermal growth factor receptor 2 419
immunohistochemical score and comparison with the Genomic Health recurrence score in 420
early breast cancer. J Clin Oncol, 2011. 29(32): p. 4273-8.
421
7. Dowsett, M., I. Sestak, E. Lopez-Knowles, et al., Comparison of PAM50 risk of recurrence 422
score with oncotype DX and IHC4 for predicting risk of distant recurrence after endocrine 423
therapy. J Clin Oncol, 2013. 31(22): p. 2783-90.
424
8. Sgroi, D.C., I. Sestak, J. Cuzick, et al., Prediction of late distant recurrence in patients with 425
oestrogen-receptor-positive breast cancer: a prospective comparison of the breast-cancer 426
index (BCI) assay, 21-gene recurrence score, and IHC4 in the TransATAC study population. 427
Lancet Oncol, 2013. 14(11): p. 1067-76.
428
9. Buus, R., I. Sestak, R. Kronenwett, et al., Comparison of EndoPredict and EPclin With 429
Oncotype DX Recurrence Score for Prediction of Risk of Distant Recurrence After Endocrine 430
Therapy. J Natl Cancer Inst, 2016. 108(11).
431
10. Dubsky, P., J.C. Brase, R. Jakesz, et al., The EndoPredict score provides prognostic 432
information on late distant metastases in ER+/HER2- breast cancer patients. Br J Cancer,
433
2013. 109(12): p. 2959-64.
434
11. Filipits, M., T.O. Nielsen, M. Rudas, et al., The PAM50 risk-of-recurrence score predicts risk 435
for late distant recurrence after endocrine therapy in postmenopausal women with endocrine-436
responsive early breast cancer. Clin Cancer Res, 2014. 20(5): p. 1298-305.
437
12. Cuzick, J., I. Sestak, M. Baum, et al., Effect of anastrozole and tamoxifen as adjuvant 438
treatment for early-stage breast cancer: 10-year analysis of the ATAC trial. Lancet Oncol,
439
2010. 11(12): p. 1135-41.
440
13. Paik, S., S. Shak, G. Tang, et al., A multigene assay to predict recurrence of tamoxifen-441
treated, node-negative breast cancer. N Engl J Med, 2004. 351(27): p. 2817-26.
442
14. Tang, G., J. Cuzick, J.P. Costantino, et al., Risk of recurrence and chemotherapy benefit for 443
patients with node-negative, estrogen receptor-positive breast cancer: recurrence score alone 444
and integrated with pathologic and clinical factors. J Clin Oncol, 2011. 29(33): p. 4365-72.
445
15. Health, G.
https://breast-cancer.oncotypedx.com/en-US/Professional-446
Invasive/Resources/ODX-Tools-RSPC.aspx. [cited 2017 January]. 447
16. Jerevall, P.L., X.J. Ma, H. Li, et al., Prognostic utility of HOXB13:IL17BR and molecular grade 448
index in early-stage breast cancer patients from the Stockholm trial. Br J Cancer, 2011.
449
104(11): p. 1762-9.
450
17. Ma, X.J., R. Salunga, S. Dahiya, et al., A five-gene molecular grade index and 451
HOXB13:IL17BR are complementary prognostic factors in early stage breast cancer. Clin
452
Cancer Res, 2008. 14(9): p. 2601-8.
453
18. Zhang, Y., C.A. Schnabel, B.E. Schroeder, et al., Breast cancer index identifies early-stage 454
estrogen receptor-positive breast cancer patients at risk for early- and late-distant recurrence. 455
Clin Cancer Res, 2013. 19(15): p. 4196-205.
22 19. Sestak, I., J. Cuzick, M. Dowsett, et al., Prediction of late distant recurrence after 5 years of 457
endocrine treatment: a combined analysis of patients from the Austrian breast and colorectal 458
cancer study group 8 and arimidex, tamoxifen alone or in combination randomized trials using 459
the PAM50 risk of recurrence score. J Clin Oncol, 2015. 33(8): p. 916-22.
460
20. Filipits, M., M. Rudas, R. Jakesz, et al., A new molecular predictor of distant recurrence in 461
ER-positive, HER2-negative breast cancer adds independent information to conventional 462
clinical risk factors. Clin Cancer Res, 2011. 17(18): p. 6012-20.
463
21. Wirapati, P., C. Sotiriou, S. Kunkel, et al., Meta-analysis of gene expression profiles in breast 464
cancer: toward a unified understanding of breast cancer subtyping and prognosis signatures. 465
Breast Cancer Res, 2008. 10(4): p. R65.
466
22. Sotiriou, C. and L. Pusztai, Gene-expression signatures in breast cancer. N Engl J Med,
467
2009. 360(8): p. 790-800.
468
23. Sgroi, D.C., E. Carney, E. Zarrella, et al., Prediction of late disease recurrence and extended 469
adjuvant letrozole benefit by the HOXB13/IL17BR biomarker. J Natl Cancer Inst, 2013.
470
105(14): p. 1036-42.
471
24. Gnant, M., M. Filipits, B. Mlineritsch, et al.Clinical validation of the PAM50 risk of recurrence
472
(ROR) score for predicting residual risk of distant-recurrence (DR) after endocrine therapy in
473
postmenopausal women with ER+ early breast cancer (EBC): An ABCSG study. in SABCS. 474
2012. San Antonio: Cancer Research. 475
25. Wolmark, N., E.P. Mamounas, F.L. Baehner, et al., Prognostic Impact of the Combination of 476
Recurrence Score and Quantitative Estrogen Receptor Expression (ESR1) on Predicting Late 477
Distant Recurrence Risk in Estrogen Receptor-Positive Breast Cancer After 5 Years of 478
Tamoxifen: Results From NRG Oncology/National Surgical Adjuvant Breast and Bowel 479
Project B-28 and B-14. J Clin Oncol, 2016. 34(20): p. 2350-8.
480
26. Goss, P.E., J.N. Ingle, K.I. Pritchard, et al., Extending Aromatase-Inhibitor Adjuvant Therapy 481
to 10 Years. N Engl J Med, 2016. 375(3): p. 209-19.
482
27. Mamounas, E., H. Bandos, B.C. Lembersky, et al., Abstract S1-05: A randomized, double-483
blinded, placebo-controlled clinical trial of extended adjuvant endocrine therapy (tx) with 484
letrozole (L) in postmenopausal women with hormone-receptor (+) breast cancer (BC) who 485
have completed previous adjuvant tx with an aromatase inhibitor (AI): Results from NRG 486
Oncology/NSABP B-42. Cancer Res, 2017. 77(4).
487
28. Blok, E.J., C. Van de Velde, E.M. Meershoek-Klein Kranenbarg, et al., Abstract S1-04: 488
Optimal duration of extended letrozole treatment after 5 years of adjuvant endocrine therapy; 489
results of the randomized phase III IDEAL trial (BOOG 2006-05). Cancer Res, 2016. 77(4).
490
29. Tjan-Heijnen, V.C., I.E. Van Hellemond, P.G. Peer, et al., Abstract S1-03: First results from 491
the multicenter phase III DATA study comparing 3 versus 6 years of anastrozole after 2-3 492
years of tamoxifen in postmenopausal women with hormone receptor-positive early breast 493
cancer. Cancer Res, 2017. 77(4).
494
495
23
Figure legends
497
Figure 1: Kaplan-Meier curves and 10-year distant recurrence risks according to
498
signature and nodal status for years 0-10.
499
Figure 2: Kaplan-Meier curves and 5-10 year distant recurrence risks according to
500
signature and nodal status for years 5-10.
501
24
Table 1: Univariate Hazard Ratios (95% CI) and C-indices for all prognostic
503
signatures according to nodal status in years 0-10. All HRs are for a change in one
504
Standard Deviation.
505
Node-negative (N=591) Node-positive (N=227)
HR (95% CI) C-index (95% CI) HR (95% CI) C-index (95% CI)
CTSa 1.99 (1.58-2.50) 0.721 (0.668-0.774) 1.63 (1.20-2.21) 0.640 (0.554-0.726)
IHC4b 1.95 (1.55-2.45) 0.725 (0.665-0.785) 1.33 (0.99-1.78) 0.601 (0.511-0.690)
RSc 1.69 (1.40-2.03) 0.667 (0.585-0.750) 1.39 (1.05-1.85) 0.603 (0.513-0.693)
BCId 2.46 (1.88-3.23) 0.762 (0.704-0.820) 1.67 (1.21-2.29) 0.652 (0.566-0.739)
RORe 2.56 (1.96-3.35) 0.764 (0.707-0.821) 1.58 (1.16-2.15) 0.636 (0.552-0.719)
EPclinf 2.14 (1.71-2.68) 0.765 (0.716-0.814) 1.69 (1.29-2.22) 0.671 (0.590-0.752)
HR=Hazard Ratio, CI=Confidence Interval, a) CTS=Clinical Treatment Score, b) IHC4=Immunohistochemical Score, c) 506
RS=Recurrence Score, d) BCI=Breast Cancer Index, e) ROR=Risk of Recurrence Score, f) EPclin=EndoPredict clinical 507
508
25
Table 2: Univariate Hazard Ratios (95% CI) and C-indices for all prognostic
510
signatures according to nodal status in years 5-10. All HRs are for a change in one
511
Standard Deviation.
512
Node-negative (N=535) Node-positive (N=154)
HR (95% CI) C-index (95% CI) HR (95% CI) C-index (95% CI)
CTSa 1.95 (1.43-2.65) 0.721 (0.654-0.788) 1.61 (1.05-2.47) 0.644 (0.534-0.753)
IHC4b 1.59 (1.16-2.16) 0.660 (0.576-0.745) 1.20 (0.79-1.81) 0.579 (0.460-0.697)
RSc 1.46 (1.09-1.96) 0.585 (0.467-0.702) 1.24 (0.81-1.90) 0.555 (0.418-0.693)
BCId 2.30 (1.61-3.30) 0.749 (0.668-0.830) 1.60 (1.04-2.47) 0.633 (0.514-0.751)
RORe 2.77 (1.93-3.96) 0.789 (0.724-0.854) 1.65 (1.08-2.51) 0.643 (0.528-0.758)
EPclinf 2.19 (1.62-2.97) 0.768 (0.701-0.835) 1.87 (1.27-2.76) 0.697 (0.594-0.799)
HR=Hazard Ratio, CI=Confidence Interval, a) CTS=Clinical Treatment Score, b) IHC4=Immunohistochemical Score, c) 513
RS=Recurrence Score, d) BCI=Breast Cancer Index, e) ROR=Risk of Recurrence Score, f) EPclin=EndoPredict clinical 514
D is ta nt re cu rr en ce fr ee (% ) Node-negative patients
Follow-up time [years]
365 (61.8%) Number of women 156 (26.4%) 143 (24.2%) 318 (53.8%) 178 (30.1%) 95 (16.1%) 429 (72.6%) 162 (27.4%) 374 (63.3%) 83 (14.0%) 61 (10.3%) 3.9% (2.3-6.7) 19.3% (13.3-27.6) 27.3% (18.7-38.8) 10-year DR risk (%) 5.9% (3.8-9.1) 16.7% (11.5-24.0) 27.2% (17.3-41.2) 3.0% (1.6-5.8) 14.1% (9.4-20.8) 32.4% (23.4-43.8) 6.6% (4.5-9.7) 22.1% (16.2-29.8) Node-positive patients
Low Intermediate High
Number of women 15 (8.2%) 58 (31.7%) 110 (60.1%) 43 (23.5%) 140 (76.5%) 10-year DR risk (%) 0% 20.7% (12.0-34.4) 30.7% (22.2-41.3) 5.6% (1.4-20.9) 30.3% (23.0-39.3) 10 0 80 60 BCI 10 0 80 60 RS 10 0 80 60 ROR
Followup time [years]
-10
0
80
60
0 2 4 6 8 10
EPclin 58 (31.7%) 105 (57.4%) 20 (10.9%) 19.4% (12.5-29.5) 29.1% (18.9-43.1) 38.0 % (20.0-64.1) 95 (51.9%) 60 (32.8%) 28 (15.3%) 15.5% (9.3-25.3) 32.0% (21.1-46.6) 41.4% (24.3-64.1)
0 2 4 6 8 10
EPclin 10 0 80 60 10 0 80 60 ROR 10 0 80 60 RS 10 0 80 60 BCI
D is ta nt r ec ur re nc e fr ee ( % )
Follow-up time [years] EPclin
5 6 7 8 9 10
80 90 10 0 80 90 10 0 BCI 80 90 10 0 ROR 80 90 10 0 RS Node-negative patients
Low Intermediate High
340 (63.6%) Number of women 134 (25.1%) 126 (23.6%) 292 (54.6%) 165 (30.8%) 78 (14.6%) 393 (73.5%) 142 (26.5%) 351 (65.6%) 69 (12.8%) 50 (9.3%) 2.6% (1.3-5.0) 14.4% (9.0-22.6) 15.9% (8.9-27.6) 10-year DR risk (%) 4.8% (2.9-7.9) 9.6% (5.6-16.3) 16.1% (8.0-30.8) 1.4% (0.5-3.8) 10.0% (6.0-16.5) 23.2% (14.9-35.2) 4.3% (2.6-7.1) 14.6% (9.6-22.0) 80 90 10 0 BCI 80 90 10 0 RS 80 90 10 0 ROR 80 90 10 0
5 6 7 8 9 10
EPclin
Follow-up time [years]
84 (54.6%) Number of women 45 (29.2%) 50 (32.5%) 15 (9.7%) 51 (33.1%) 88 (57.1%) 40 (26.0%) 114 (74.0%) 94 (61.0%) 20 (13.0%) 15 (9.7%) 9.5% (8.3-23.9) 14.3% (8.3-23.9) 36.5% (20.4-59.6) 10-year DR risk (%) 17.9% (11.5-27.3) 19.5% (10.9-33.5) 27.5% (11.2-57.9) 0% 13.0% (6.1-26.7) 25.0% (17.5-35.0) 3.3% (0.5-21.4) 23.6% (17.0-32.1) Node-positive patients