COPYRIGHT © UNIVERSAL MULTIDISCIPLINARY RESEARCH INSTITUTE PVT LTD
THE EFFECTIVENESS OF PSYCHOEDUCATION ON POST
TRAUMATICSTRESS DISORDER (PTSD)
FARJANA SHARMIN* AND JOBEDA KHATUN
Assistant Clinical Psychologist, Department of Clinical Psychology, University of Dhaka,
Dhaka-1000, Bangladesh
*Author for correspondence: [email protected], [email protected]
COPYRIGHT © UNIVERSAL MULTIDISCIPLINARY RESEARCH INSTITUTE PVT LTD
Abstract
The Post traumatic stress disorder reactions and recovery are results of complex interactions among biological, personal, environmental and culturalfactors. “psycho education” followin g trauma in snow increasingly used. The term covers the provision of information, about the nature of stress, symptoms and treatment. Purposive sampling technique had used to select th e sample of the present study. The sample of the study included survivors of the RANA PLAZ A tragedy who met diagnostic criteria of PTSD by psychiatry. Between the samples, there wer e individuals and group sample. Psychoeducation and medicine only had made up as compar ison groups. Three semi-structured psychoeducation sessions conducted for both individually and group session for experimental group. Patient in the “medicine only” group were not pa rticipant in these sessions. Impact of Event Scale (Revised), Depression scale, Anxiety scale h ad used for the measurements. Pre-test, post-test design had used for present study. Paired sa mple t-test had used following the intervention. Subjective rating (0-100) had used for each s ection of psychoeducation. Both individual and group participants had improved after psycho education intervention in compare with medicine only group.
COPYRIGHT © UNIVERSAL MULTIDISCIPLINARY RESEARCH INSTITUTE PVT LTD
INTRODUCTION
Post Traumatic Stress Disorder (PTSD) is known as psychiatric disorder that can occur follo wing the experience or witnessing of a life threatening events such as war, natural disasters, r oad accident, sudden major illness, terrorist incidents, serious incidents, physical or sexual as sault in adult or childhood. Most survivors of trauma return to normal after some time. But, s ome people has develop stress reactions which does not go away or may even get worse over time.
It is common feature of PTSD that, People who are under goesin this disorder often relive the experiences through past incidence, nightmares and flashbacks, have difficulty in sleeping, a nd feel detached or estranged. These symptoms can be severe enough and it can be last long e nough to impair the person’s daily life. PTSD suffers experiencing aspects of the traumatic ev ent is in a very vivid, recurrent and distressing way. This includes flashbacks in which the per son may acts or feels as if the event were happening, nightmares and repetitive and distressin g intrusive images or other sensory impressions from the event.
Both psychological and psychopharmacological approaches have been used to help persons w ith PTSD.Research indicated that these combined therapies are most frequently recommende d and PTSD requires treatment. Usually psychotherapy is recommended first. A combination of psychotherapy and medication may be recommended, if suffer has severe or persistent PTS D. Cognitive behavioral therapy (CBT) is one of the successful and evidence based psychothe rapy.
COPYRIGHT © UNIVERSAL MULTIDISCIPLINARY RESEARCH INSTITUTE PVT LTD odifies and normalized a trauma survivor’s perceptions about the event, of themselves, or of t heir future.
Post-Traumatic Stress Disorder had been developed severe level after the “RANA PLAZA” tr agedy. Effective treatments of PTSD are pharmacological and psychological to reducing distr ess of the individual. Evidence based therapy of the PTSD are prolonged exposure in real life (in vivo) situation or/ and imaginal exposure (in-vetro), progressive muscular relaxation (PM R), breathing relaxation, stress inoculation therapy and cognitive therapy. But, now we have s een that breathing relaxation, PMR doesn’t work effectively for PTSD client who have been s urvivor from RANA PLAZA. They have some physical impairment due to the accident. They could not able to do breathing relaxation, PMR techniques. Imaginal exposure sometime initi ates the flashback of their traumatic event or memory. On the other hand they have no knowl edge about the response or reaction of the PTSD. Psycho education of the PTSD may help the m to reduce their symptoms. Thus the objectives of the present study were: 1) To investigate t he effectiveness of the Psycho-educational intervention in pretest posttest result in reducing s ymptoms of Post- Traumatic Stress Disorder (PTSD). 2) To see the effectiveness of the psych o-educational interventions in reducing depression and anxiety of the participants.3) To see h ow well participants to understand the psychoeducation material of Post- Traumatic Stress Di sorder (PTSD). 4) To see the group and individual subjective responses about the understandi ng of the PTSD. 5) To see the effectiveness psychoeducation material between experiment gr oup and comparison group.
MATARIALS AND METHOD:
The study used pretest to posttest quasi-experiment design with two comparison groups. A qu asi-experimental design often used to gauge the effects of an educational program is the grou p pretest-posttest.
COPYRIGHT © UNIVERSAL MULTIDISCIPLINARY RESEARCH INSTITUTE PVT LTD parison groups for the study as psychoeducation (PE), medication only. Following the eligibil ity assessment and obtaining informed consent, patient had given a follow up appointment. T he protest questionnaires were given 10 days after the last psychoeducation session. The aver age time for completing the questionnaire was 45 minutes. Participants who were in the ‘med ication only’ group had also asked to compare the pretest and posttest questionnaire. The pret est questionnaires were administered during the initial visit to the psychiatric outpatient depar tment while the posttest questionnaires had given 10 days later. Participants were interviewed in private room in the saver central hospital through out the study.
The objective of the preliminary study was to develop a written document of psychoeducat ion about PTSD that is appropriate in the context of Bangladesh. The document of first draft was constructed interviewed PTSD client and understanding their problems. Then through ext ensive review of journal, articles, book on PTSD reviewed. Many expertise, scholar and profe ssor in different countries suggestions and information and documents had taken in developm ent of psycho education. The first draft of psychoeducation had given multidisciplinary team for judge evaluation. They were requested to edit, correct, modify, or rewrite statement if nec essary. The researcher then complied all the feedbacks, revised the material to make it a stand ard form, and prepared for final draft. In short, the design of the development of a written doc ument on PTSD was as follows:
RESULTS AND DISCUSSION:
The participants was included study had physical, psychological, social and legal problems. T hey had burning sensation in whole body, pain, headache, back pain, nightmare, over sensitiv e to sounds, flash back, smell of dead bodies, sleep problems, excessive dizziness, suicidal att empted so on. Some participants also had some legal problems, which made vulnerable their current life.
COPYRIGHT © UNIVERSAL MULTIDISCIPLINARY RESEARCH INSTITUTE PVT LTD
Psychometric tools Pretest Mean Severity leve ls Posttest Mean Severity levels Impact of Event Sca
le
69.73 Severe 36.64 Moderate
Depression Scale 123.96 Severe 89.83 Minimal
Anxiety Scale 99.13 Profound 67.39 Severe
Table 2: Severity level of psychometric tools
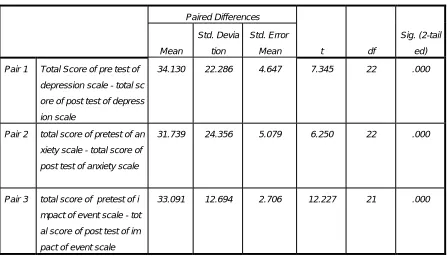
Form the paired samples test table 3 we can see that the pretest posttest t score for depression scale is 7.345, where mean difference 34.130, p≤.0.01. As the same as the pretest posttest t sc ore for anxiety scale is 6.250, where mean difference 31.739, p≤.0.01and the pretest posttest t
score for Impact of Event scale is 12.227, where mean difference 33.091, p≤.0.01.
Paired Samples Test
Paired Differences
t df
Sig. (2-tail ed) Mean Std. Devia tion Std. Error Mean
Pair 1 Total Score of pre test of
depression scale - total sc
ore of post test of depress
ion scale
34.130 22.286 4.647 7.345 22 .000
Pair 2 total score of pretest of an
xiety scale - total score of
post test of anxiety scale
31.739 24.356 5.079 6.250 22 .000
Pair 3 total score of pretest of i
mpact of event scale - tot
al score of post test of im
pact of event scale
COPYRIGHT © UNIVERSAL MULTIDISCIPLINARY RESEARCH INSTITUTE PVT LTD
Individual sessions verbal reports after
PE intervention
After 10 days verbal
Reports
I-01
। এখ
ন
। ।
হয়
।
এখন
I-02 ,
।
,
র ।
।
I-03
।
আর মন
।
I-04
র ।
র
।
হয় ।
I-05
হয়
।
। ।
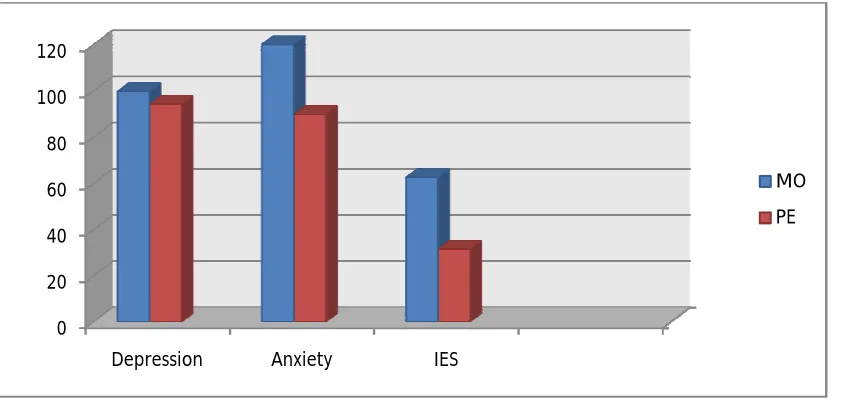
COPYRIGHT © UNIVERSAL MULTIDISCIPLINARY RESEARCH INSTITUTE PVT LTD Figure 5: Graphical presentation of effectiveness of PE
After almost one year psychoeducation intervention had been given to the survivors of Ra na Plaza victims. They had benefited from the psychoeducation intervention in one month ( B ecause of session for psychoeducation and 10 days later posttest). The results of present stud y showed that psychoeducation intervention should be given as early as possible to diagnosed patient.
The paired samples t-test was used to compare the pretests and posttests despite the small s ample size and variances were homogeneous within the groups. Posttest scores of posttrauma tic stress and depression, anxiety and PTSD severity were found significantly lower compare d with the pretests in all intervention groups.
People reported high subjective rating in understanding the psychoeducation intervention. but the model of PTSD rated low than others components. The reason behind that the sample of the present study was low educational background. This model may be applicable to gener al population and higher educational background.
The subjective statement of after PE intervention and posttest had consistency. Participants were positively response after PE intervention and posttest. These results had seen both in in dividual and comparison group.
Psycho-education had some positive effects on participants, but anxiety and hyper-arousal were expected to create obstacles to learning and using adaptive coping strategies. An additio nal supportive and educational approach can therefore be more useful for these patients to get the added benefit of a rapid decrease of anxiety with medication. Despite the decrease in sym
0 20 40 60 80 100 120
Depression Anxiety IES
MO
COPYRIGHT © UNIVERSAL MULTIDISCIPLINARY RESEARCH INSTITUTE PVT LTD ptoms with medication, individuals still need to learn how to deal with new life situations and PTSD symptoms after a traumatic experience. Avoidance as a coping strategy influences the results of the interventions.
References
Akdemir, A. O., Arsel, S., Dag, I., Tu¨ rkc¸apa,r MH. _Is.¸ can, N., & O¨ zbay, H., (1996). Re liability and validity of Hamilton depression rating scale and clinical usage. The Journal of Psychiatry, Psychology and Psychopharmacology 4, 251–259.
Aker, A.T., (2000). Cognitive and behavioral therapies of PTSD. The Journal of Psychiatry, Psychology and Psychopharmacology 8, 38–46.
Aker, T. O., zeren, M., Bas¸ og˘lu, M., Kaptanog,˘lu. C., Erol, A., & Buran, B., (1999). Valid
ity and reliability study of clinician administered posttraumatic stress disorder scale. Turki sh Journal of Psychiatry 10, 286–293).
Armenian, H., Morikawa, M., Melkonian, A.K., Hovanesian, A., Akiskal, K., & Akiskal, H., (2002). Risk factors for depression in the survivors of the 1988 earthquake in Armenia. Jo urnal of Urban Health 79, 373–382.
Bas¸ og˘lu M. S.¸ alcıog,˘lu. E., & Livanou, M., (2002). Traumatic stress responses in earthqu
ake survivors in Turkey. Journal of Traumatic Stress 15, 269–276.
Birol, L., (2000). The Theories Related with Nursing – Hildegard Peplau, in Nursing Process
– A Systematic Approach for Nursing Care, 4th edn. Bozyaka Publishing Company, _Izmi
COPYRIGHT © UNIVERSAL MULTIDISCIPLINARY RESEARCH INSTITUTE PVT LTD Brunello, N., Davidson, J.R., Deahl, M., Kessler, R.C., Mendlewicz, J., Racagni, G., Shalev,
A.Y., & Zohar, J., (2001). Post-traumatic stress disorder: diagnosis and epidemiology, co morbidity and social consequences, biology and treatment. Neuropsychobiology 43, 150–1 62.
Ethnocultural Aspects of Post-traumatic Stress Disorder, 4th edn. American Psychological As sociation, Washington DC.
Foa, E. B., Davidson, J. R. T., & Frances, A., (1999). Treatment of posttraumatic stress disor der. Journal of Clinical Psychiatry 60, 10–19, 71–75.
Kessler, R. C., (2000). Post-traumatic stress disorder: the burden to the individual and to soci ety. Journal of Clinical Psychiatry 61, 4–12.
Livanou, M., Bas¸ og˘lu, M., Marks, I. M., De, S. P., Noshirvani, H., Lovell, K., & Thrasher, S., (2002a). Beliefs, sense of control and treatment outcome in post-traumatic stress diso rder. Psychological Medicine 32, 157–165.
www.hcp.med.harvard.edu/ncs/publications.php