Implementation of Universal Influenza Immunization Recommendations
for Healthy Young Children: Results of a Randomized, Controlled Trial
With Registry-Based Recall
Allison Kempe, MD, MPH*‡; Matthew F. Daley, MD*‡; Jennifer Barrow, MSPH‡; Norma Allred, PhD§; Nellie Hester, BA‡; Brenda L. Beaty, MSPH‡; Lori A. Crane, PhD, MPH‡㛳; Kellyn Pearson, MSN‡; and
Stephen Berman, MD*‡
ABSTRACT. Background. An Advisory Committee on Immunization Practices policy of encouraging influenza vaccination for healthy 6- to 23-month-old children was in effect during the 2003–2004 influenza season, which was unusually severe in Colorado. We collaborated with 5 pediatric practices to attempt universal influenza im-munization in this age group.
Objectives. The objectives were (1) to assess the
max-imal influenza immunization rates that could be achieved for healthy young children in private practice settings, (2) to evaluate the efficacy of registry-based reminder/recall for influenza vaccination, and (3) to de-scribe methods used by private practices to implement the recommendations.
Methods. The study was conducted in 5 private
pedi-atric practices in Denver, Colorado, with a common billing system and immunization registry. Although rec-ommendations by the Advisory Committee on Immuni-zation Practices included children who were 6 to 23 months of age at any point during the influenza season, our practices chose not to recall children 22 to 23 months of age, because they would have become>24 months of age during the study period. Therefore, our study popu-lation consisted of all healthy children 6 to 21 months of age from the 5 practices (Nⴝ5193), who were random-ized to intervention groups (nⴝ2595) that received up to 3 reminder/recall letters or to control groups (nⴝ 2598) that received usual care. The primary outcome was re-ceipt of >1 influenza immunization, as noted either in the immunization registry or in billing data.
Results. Immunization rates for>1 dose of influenza
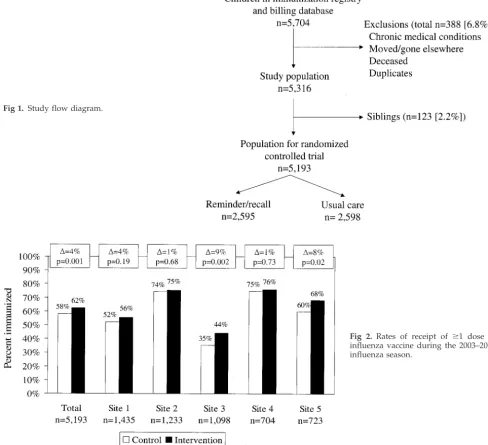
vaccine for the intervention groups in the 5 practices were 75.9%, 75.4%, 68.1%, 55.6%, and 44.3% at the end of the season. Overall, 62.4% of children in the intervention groups and 58.0% of children in the control groups were immunized (4.4% absolute difference), with absolute dif-ferences, compared with control values, ranging from
1.0% to 9.1% according to practice. However, before in-tensive media coverage of the influenza outbreak began (November 15, 2003), absolute differences, compared with control values, ranged from 5.1% to 15.3% and were 9.6% overall. Before November 15, significant effects of recall were seen for children in the intervention groups, in both the 12- to 21-month age category (10.4% increase over control) and the 6- to 11-month category (8.1% in-crease over control); at the end of the season, however, significant effects of recall were seen only for the older age group (6.2% increase over control). The rates of re-ceipt of 2 vaccine doses >1 month apart for eligible children ranged from 21% to 48% among the practices. Four of the 5 practices held influenza immunization clin-ics during office hours, evenings, or weekends, and these clinics achieved higher coverage rates.
Conclusions. These results demonstrated that, in an
epidemic influenza year, private practices were able to immunize the majority of 6- to 21-month-old children in a timely manner. Although media coverage regarding the epidemic blunted the effect of registry-based recall, re-call was effective in increasing rates early in the epi-demic, especially for children between 1 and 2 years of age. The practices that achieved the highest immuniza-tion rates were proactive in planning influenza clinics to handle the extra volume of immunizations required.
Pe-diatrics 2005;115:146–154; influenza, immunizations,
re-minder/recall, immunization registry.
ABBREVIATION. ACIP, Advisory Committee on Immunization Practices.
I
nfluenza causes an average of 36 000 cardiac and respiratory deaths1and 114 000 hospitalizations2 each year in the United States, with⬃90% of the deaths from influenza occurring among personsⱖ65 years of age.1,3In addition to its toll on the elderly, influenza disease causes substantial morbidity among children. Children play a pivotal role in ini-tiating and maintaining influenza epidemics. Popu-lation-based surveillance data have shown that pre-school-aged and pre-school-aged children have the highest attack rates during influenza epidemics, with rates exceeding 40% among preschool-aged children and 30% among school-aged children.4–9 Having a child in the household is the most important deter-minant of the occurrence of influenza within a fam-ily,7,10 and children are also an important factor in the transmission of infection to adults at high risk.11,12Influenza among children is associated withFrom the Departments of *Pediatrics and㛳Preventive Medicine and Biomet-rics, University of Colorado Health Sciences Center, Denver, Colorado; ‡Children’s Outcomes Research Program, Children’s Hospital, Denver, Col-orado; and §National Immunization Program, Centers for Disease Control and Prevention, Atlanta, Georgia.
Accepted for publication Oct 4, 2004. doi:10.1542/peds.2004-1804
Portions of this work were presented at the 38th National Immunization Conference; May 11–14, 2004; Nashville, TN; and the Pediatric Academic Societies Annual Meeting; May 1– 4, 2004; San Francisco, CA.
No conflict of interest declared.
Address correspondence to Allison Kempe, MD, MPH, Children’s Hospital, 1056 E 19th Ave, B032, Denver, CO 80218. E-mail: kempe.allison@ tchden.org
complications such as acute otitis media resulting in antibiotic use, pneumonia, febrile seizures, and, less commonly, encephalopathy, myositis, myocarditis, and pericarditis.13–19 Infection can also exacerbate chronic illnesses, such as asthma, among infected children.20Influenza infection among children is re-sponsible for increasing medical costs, both directly through the care of sick children21–24 and indirectly through increased work absenteeism among adults caring for infected children.25
In recent years, there has been increasing recogni-tion of the morbidity of influenza disease among children⬍2 years of age. Although high hospitaliza-tion rates for respiratory illnesses in this age group have been documented for decades,26–28 only re-cently have studies attempted to differentiate the relative contributions of respiratory syncytial virus and influenza to the burden of hospitalization among young children.1,14,29,30 Estimates vary, but recent studies suggested that influenza-related hos-pitalization rates among children 0 to 2 years of age without high-risk conditions are in the range of 144 to 1038 cases per 100 000 persons per year, compa-rable to rates among personsⱖ65 years of age.29,30
Since the 1960s, efforts in the United States to reduce the burden of influenza have been directed toward annual vaccination of targeted groups thought to be at higher risk of morbidity or death resulting from influenza.31,32 Until 2000, these tar-geted groups included persons ⱖ6 months of age with chronic pulmonary, cardiovascular, or other medical conditions, all personsⱖ65 years of age, and close contacts of these groups.33 In 2000, universal recommendations were extended to include people
ⱖ50 years, because of their increased risk of chronic illnesses.34Because of the recent data demonstrating the morbidity of influenza disease among young children, in 2002 and 2003 the Advisory Committee on Immunization Practices (ACIP) encouraged vac-cination for healthy children 6 to 23 months of age “when feasible,”35,36and in 2004 both ACIP and the American Academy of Pediatrics recommended uni-versal vaccination for this age group and their close contacts for the 2004 –2005 influenza season.37,38
Because these recommendations have not yet been implemented, there is little information available re-garding their feasibility for practicing pediatricians. Practical concerns for practitioners facing the 2004 – 2005 influenza season include potentially dramatic increases in the need for visits within a fairly short time period, especially because most young children require 2 doses;37,38problems estimating the amount of vaccine needed and concerns about ordering too much or with having inadequate supplies; problems identifying and recalling children in the targeted age range; and concerns about reimbursement for fami-lies who are underinsured. In addition, practitioners must address families’ concerns regarding the num-ber of vaccinations already required, the safety and side effects of the influenza vaccine, and whether influenza disease is sufficiently serious to warrant vaccination.
Because the ACIP was already encouraging uni-versal influenza immunization among children 6 to
23 months of age and a full recommendation ap-peared imminent, we collaborated with providers in 5 pediatric practices in Denver, Colorado, to attempt universal immunization of 6- to 21-month-old chil-dren against influenza during the 2003–2004 season. The primary objectives of the study were (1) to assess the maximal influenza immunization rate that could be achieved among healthy children 6 to 21 months of age during the first year of implementation of the new guidelines in private practice settings, (2) to examine the efficacy of registry-based reminder/re-call in increasing influenza immunization rates in this age group, and (3) to identify and describe the methods used by private practices to implement the recommendations.
METHODS Study Setting and Population
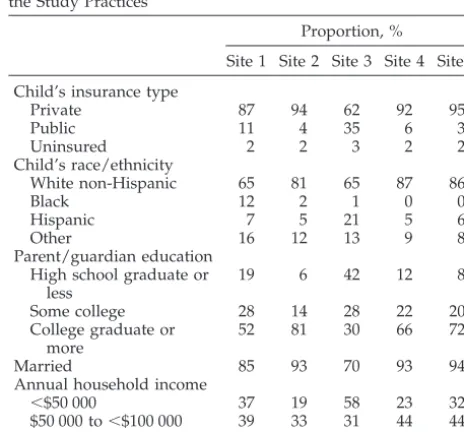
The study protocol was reviewed and approved by the Colo-rado Multiple Institutional Review Board. The study was con-ducted in 5 pediatric practices in metropolitan Denver, Colorado, from September 1, 2003, through February 29, 2004. Providers in the practices had agreed to encourage influenza immunization for healthy young children 6 to 23 months of age during the 2003– 2004 influenza season. All of the practices participate in a regional immunization registry and share a common computerized billing system. The practices are in urban or suburban locations and range from a low of 7 to a high of 16 total providers per practice, with 6 to 9 pediatricians per practice. The characteristics of the patient populations at the practices are shown in Table 1.
The study population included all children 6 to 21 months of age who had visited 1 of the offices in the previous 18 months and had a record in the immunization registry. Although the ACIP recommendations would have included children who were 6 to 23 months of age at any point during the influenza season, our practices chose not to recall children 22 to 23 months of age; the practices were concerned that insurers would not reimburse for vaccination of children who became older than 23 months during the influenza season, because the ACIP encouragement for uni-versal vaccination of these children was not yet a full recommen-dation. Children were excluded if they had a chronic medical condition (identified with International Classification of Diseases, Ninth Revision, codes from office billing data), they had died, or
TABLE 1. Patient and Parent/Guardian Characteristics for the Study Practices
Proportion, %
Site 1 Site 2 Site 3 Site 4 Site 5 Child’s insurance type
Private 87 94 62 92 95
Public 11 4 35 6 3
Uninsured 2 2 3 2 2
Child’s race/ethnicity
White non-Hispanic 65 81 65 87 86
Black 12 2 1 0 0
Hispanic 7 5 21 5 6
Other 16 12 13 9 8
Parent/guardian education High school graduate or
less
19 6 42 12 8
Some college 28 14 28 22 20
College graduate or more
52 81 30 66 72
Married 85 93 70 93 94
Annual household income
⬍$50 000 37 19 58 23 32
$50 000 to⬍$100 000 39 33 31 44 44
ⱖ$100 000 25 48 11 33 24
there was documentation that the family had moved to a different office that was not participating in the study. If there was⬎1 child per family in the specified age group, then 1 child per family was randomly selected for participation and the others were excluded.
Data Sources
Administrative Data
The practices share a common administrative and billing data-base that contains demographic data and is updated at the time of each visit. A bill is generated for each encounter, including im-munizations recorded with Current Procedural Terminology codes.39In this study, both administrative data and registry data
were used to assess whether an influenza vaccination had been administered.
Immunization Registry Data
As previously described,40immunization records for all
chil-dren⬍72 months of age in the participating practices were entered into an existing regional immunization registry 15 to 24 months before the present study, with immunization data from medical records and billing data. The registry is Internet-based and cur-rently contains records for 47% of children 0 to 6 years of age in Colorado. The registry operates in accordance with national stan-dards for immunization registries.41Staff members at the
partici-pating practices are instructed to enter all immunizations within 24 hours after administration. Quality assessment data for the 5 practices, comparing medical record data and registry data for May to July 2003 (samples of 30 charts per practice), demonstrated an overall completeness rate of 97.4% (children in the practice who were in the registry) and an error rate of 7.2% (immunization not in the registry or incorrect date).
Survey Data
For the purpose of describing the characteristics of the study practice populations, we used data collected in telephone surveys during August to October 2003. The overall objective of the tele-phone surveys was to assess parents’ attitudes and intentions for influenza vaccination, and surveyed parents were not given infor-mation about influenza vaccination or encouraged to vaccinate their children. The survey included a brief verbal consent but no formal written consent, because all surveys were deidentified after data collection. Survey respondents represented a random sample of parents of children 6 to 21 months of age at the 5 study sites, sampled proportionately for the sizes of the practices. Families were considered ineligible if they did not speak English, the age of the parent was⬍18 years, or the child’s age was not within the prescribed age range. Of an eligible sample of 828 families, 472 surveys were successfully completed, for a response rate of 57%. Sources of nonresponse included families that could not be con-tacted after 20 attempts and those that refused to participate in the survey.
Randomization
This study was a randomized, controlled trial to evaluate the effectiveness of immunization registry-based reminder/recall for influenza vaccination among 6- to 21-month-old children. We used random allocation of subjects stratified according to practice site, to ensure equal numbers in the intervention and control groups for each practice.
Study Interventions
Patient Reminder/Recall Intervention
The intervention group received up to 3 reminder/recall letters, generated by the immunization registry. The reminder/recall let-ters stated that the providers at the practices were recommending yearly influenza vaccination for all children 6 to 23 months of age and that the practice recommended immunization of the family’s child. The letters provided information about how to schedule an appointment and, in some practices, about times of influenza clinics and whether patients were allowed to “walk in” for immu-nizations. Families in the control group did not receive a remind-er/recall letter, although providers were committed to immuniz-ing such children if they were examined. Each of the practices followed ACIP recommendations to provide 2 immunizations, a
minimum of 1 month apart, to previously unvaccinated chil-dren.36
The first reminder letter was sent in October 2003 to all inter-vention subjects, and a second recall letter was sent in November to those not yet vaccinated at the time of the mailing. Two of the practices (sites 1 and 5) sent a third recall letter in December to those not yet vaccinated, whereas the other 3 practices chose not to send an additional recall letter because they were experiencing shortages of influenza vaccine in their offices.
Practice Interventions
Although the major focus of this study was to evaluate the effectiveness of reminder/recall, the study team, in the course of preparing for the trial, offered general assistance to the practices in preparing for the increased volume of patients expected. On the basis of administrative and registry data, our study manager provided the office managers with projected numbers of expected influenza immunizations, for estimation of the number of doses to be ordered. The study team also organized a preseason meeting with practice office managers, to discuss options for planning for the increased volume of immunizations during a short period of time. At this meeting, the practices were not given specific sug-gestions by the study team but discussed possible options of their own choosing. The practices made individual decisions regarding their methods of handling the extra volumes (Table 2).
Outcome Measures
The primary outcome measure of the trial was receipt ofⱖ1 influenza immunization, recorded in either the immunization reg-istry or billing data, between September 1, 2003, and February 29, 2004. Other outcomes included (1) immunization rates before and after November 15, 2003, when media reports of the influenza epidemic increased and influenza-related deaths began to be re-ported; (2) immunization rates for children 6 to 11 months of age or 12 to 21 months of age; and (3) rates of receipt of 2 doses of influenza vaccine for eligible children. The strategies used to implement the guidelines were assessed qualitatively through weekly consultations with the office managers during the study. With the use of Current Procedural Terminology codes from bill-ing data, all visits at which influenza vaccine was administered were divided into 3 mutually exclusive categories, ie, (1) “shot-only” visits, defined as encounters with either no associated Eval-uation and Management code or EvalEval-uation and Management codes 99201 or 99211; (2) well-child care visits, with codes 99381, 99382, 99391, or 99392; and (3) non–well-child care visits, with codes 99202 to 99205 or 99212 to 99215.39Codes 99201 and 99211
were designated as indicating shot-only visits because use of these codes does not require the presence of a physician.39Because the
influenza epidemic itself resulted in excess visits by anxious par-ents for treatment of illness, we could not determine to what extent excess visits, compared with the previous year, were related to guideline implementation. The percentages of children 6 to 21 months of age who were vaccinated during the studied season (2003–2004), compared with those vaccinated during the previous season (2002–2003), when the practices were not attempting uni-versal immunization, were assessed to demonstrate the change in immunization volume achieved in each practice.
Data Analysis
Intention-to-treat analysis was used for all analyses.2tests of
immunization frequency, overall and in different strata, were used. In assessment of the rates of receipt of a second influenza vaccine dose, children who had received an influenza vaccine injection in the previous year (according to administrative data) were excluded from the eligible pool, because they would not have required a second dose if they had been immunized during the previous season. The SAS System for Windows, version 8 (SAS Institute, Cary, NC),42was used in the randomization process and
for data analysis.
The 2003–2004 Influenza Season in Colorado
Media Coverage
and peaked early and was more severe than the 3 previous influ-enza seasons.43In addition, 152 deaths of children⬍18 years of
age were reported.43Because pediatric influenza-associated death
was not a nationally notifiable condition in the past, no compara-ble data on pediatric deaths in previous influenza seasons were available. In Colorado, influenza activity began in October 2003, with widespread activity, including several pediatric deaths, be-ing reported in November 2003.44–47During November and
De-cember 2003, there was extensive media coverage of the epidemic. Because of the obvious potential effect of the media coverage on our trial, we tracked the content and timing of news stories re-garding the outbreak in the 2 major local newspapers and 1 major local television station. The volume of news stories increased dramatically in mid-November, and daily stories appeared after that time; therefore, the timing of major media coverage, for purposes of examination of the effects on our trial, was designated as November 15.
Influenza Vaccine Shortages
Local influenza vaccine shortages were first reported by the Colorado Department of Public Health and Environment on De-cember 5, 2003.48Four of the 5 study practices experienced vaccine
shortages for the remainder of the influenza season.
RESULTS Adequacy of Randomization
As shown in Fig 1, 5704 children 6 to 21 months of age represented the target population. A total of 9.0% were excluded for the reasons specified in Fig 1, and the remaining 5193 were randomized to the remind-er/recall intervention groups (n ⫽ 2595, 50.0%) or the control groups (n ⫽ 2598, 50.0%). The interven-tion and control groups were similar with respect to gender (female: 49.8% in the intervention group and 49.5% in the control group; P ⫽ .75), age (6 –11 months: 32.7% in the intervention group and 33.2% in the control group;P⫽.75), and insurance (private: 80.3% in the intervention group and 82.1% in the control group; public: 16.0% in the intervention group and 14.8% in the control group; uninsured: 3.4% in the intervention group and 3.0% in the con-trol group;P⫽.32). Because of the stratified random-ization, there were no significant differences in the proportions randomized to the control and interven-tion groups at any of the sites (data not shown).
Comparisons of Rates of Receipt of>1 Influenza Vaccine Dose, Overall and According to Practice
As demonstrated in Fig 2, differences between in-tervention and control groups in the percentages of eligible children who received ⱖ1 influenza shot ranged among the practices from a low of 1.0% to a high of 9.1%. The overall difference when all prac-tices were combined was 4.4% (P ⫽ .001). For the intervention groups, 2 practices achieved immuniza-tion rates ofⱖ75%, with only 1 practice achieving a rate of⬍50%.
Comparisons of Immunization Rates Stratified According to Timing of Immunization and Age
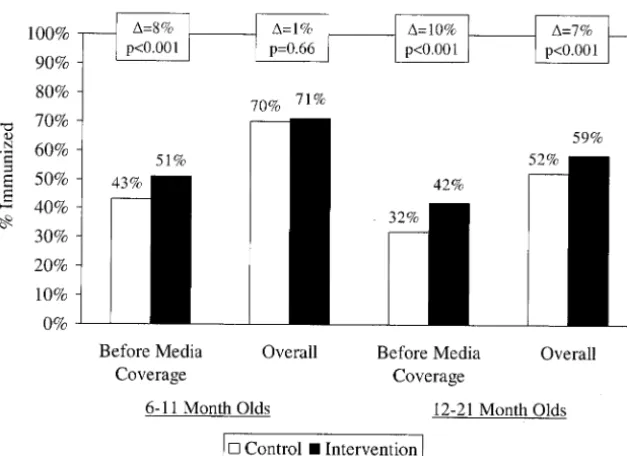
When the immunization data were stratified ac-cording to whether immunizations occurred before or after intensive media coverage began, the absolute difference in immunization rates between the inter-vention and control groups before the outbreak was 9.6% (P ⬍ .001, data not shown). In contrast, after media coverage began, children in the control group
were more likely to receive an influenza immuniza-tion, with an absolute difference of 5.2% (P ⬍ .001, data not shown). As demonstrated in Fig 3, in which the data are stratified according to age, significant effects of the reminder/recall were seen both before intensive media coverage began and overall for chil-dren 12 to 21 months of age, whereas significant effects were seen only in the period before media coverage for the 6- to 11-month age group.
Rates of Receipt of 2 Influenza Vaccine Doses by Eligible Children, According to Practice
Of the total study population (N⫽5193), 16% (n⫽ 810) were documented to have received an influenza vaccination during the previous year, which left 4383 subjects who appeared to require 2 influenza vaccine doses. Among these 4383, rates of receipt of a second vaccine dose ⱖ1 month after the first vaccine dose were 27% (site 1), 33% (site 2), 21% (site 3), 48% (site 4), and 46% (site 5). Among the subset of children who received ⱖ1 vaccine dose during the studied
influenza season (n ⫽ 2495 at the 5 sites), the per-centages who received the second dose were 54%, 46%, 55%, 65%, and 76% for sites 1 to 5, respectively.
Practice Implementation Strategies and Implementation Burden
The numbers of eligible children according to practice, a summary of the implementation strategies at each practice, the percentages of shots adminis-tered at well-child visits, illness visits, and shot-only visits, and the rates of influenza immunization for 6-to 21-month-old children during 2003–2004, com-pared with 2002–2003, are reported in Table 2. Four of the 5 practices added influenza clinics, either dur-ing or after office hours or on weekends, to absorb the extra volume. The sites varied substantially in the proportions of influenza shots that were given in association with well-child visits, from a low of 17% to a high of 42%. The proportion of influenza shots given at well-child visits was greater for children 6 to 11 months of age, compared with those 12 to 21 Fig 1. Study flow diagram.
months of age (40.0% and 21.1%, respectively, for all practices combined) (data not shown).
DISCUSSION
This study is the first to provide data regarding the feasibility of universal influenza immunization for 6-to 23-month-old children in private pediatric prac-tices. Our data demonstrated that, during an epi-demic, private practices were able to immunize the majority of 6- to 21-month-old children in a timely manner. Two practices achieved levels of⬎75%, and only 1 practice failed to vaccinate ⬎50% of the tar-geted children. Registry-based reminder/recall was an effective intervention in this effort, particularly in shifting the immunization to earlier times during an unexpectedly early influenza epidemic, in compari-son with nonrecalled children, especially among 1- to 2-year-old children. The effects of recall for the entire season, however, were underestimated in this study, because extensive publicity regarding the epidemic appeared to increase rates in the control groups, blunting the apparent effect of recall.
Because the formal recommendation for universal vaccination of all 6- to 23-month-old children will not be in effect until the 2004 –2005 influenza season,37 little has been published regarding the feasibility of implementation of this recommendation in pediatric practices. We were unable to find any published studies of attempts at universal immunization of young children with which to compare the rates achieved by our participating practices. The rates documented in our study were substantially higher than immunization rates previously achieved for other high-risk pediatric groups,40,49,50for which rec-ommendations have been in effect for many years.36,51,52 There are several reasons why the new recommendations for universal immunization of young children may be more easily implemented than those for children with chronic illnesses. Iden-tification of children with chronic illnesses requires either a prospective tracking system or retrospective
review of administrative databases with subsequent reminder/recall,40whereas age criteria pose substan-tially lower barriers to ready identification and re-call. In addition, most children with identified chronic illnesses are ⬎2 years of age and therefore visit much less frequently for routine care, compared with children⬍2 years of age. As demonstrated in a recent study, children in the 6- to 12-month age group represent a subgroup that is especially likely to be examined for reasons other than influenza im-munization during the time period in which influ-enza vaccinations must be administered.53Therefore, the new recommendations targeting the very chil-dren who are likely to be seen for care during the preseason period may be much more successful than previous recommendations targeting older children with chronic illnesses. Even if children with chronic illnesses are identified and recalled, immunization may not occur because parents may not recognize the child’s condition as chronic and therefore may not respond to recall. Finally, unless it is the subject of a visit, a child’s chronic condition may not be obvious to a provider, whereas the child’s age is evident and relevant to any visit. The success of these practices in the first year of attempted universal im-munization of young children suggests the potential benefit of targeting immunization according to age category rather than condition, thus decreasing ef-forts required for targeted recall and missed oppor-tunities when patients present for care.
Our data demonstrated that many children who were eligible to receive 2 doses of influenza vaccine received only 1 dose. This is an important outcome to monitor in this age group, because data on immuno-genicity suggest much lower rates of protection with 1 versus 2 influenza vaccine doses.54–57Recent data on the clinical efficacy of 1 versus 2 doses of influ-enza vaccine among 6- to 23-month-old children sug-gest that children in this age group who receive 1 dose have minimal protection, compared with those who receive 2 doses.58Despite the decrease in rates Fig 3. Influenza immunization rates before
in our study, 2 of the practices did manage to deliver 2 doses to one half of their eligible young patients. In 4 of the 5 practices, more than one half of children who received the first influenza vaccine dose re-ceived the second dose. Earlier recall might have helped the practices achieve 2 immunizations within the appropriate time period, but our practices were reluctant to recall any patients before they had vac-cine available and most did not receive supplies before the beginning of October. Although there is certainly room for improvement, these rates for full immunization are more impressive when it is con-sidered that this was the first year in which the practices attempted universal immunization and that significant vaccine shortages developed later in the season, which the practices reported clearly affected the delivery of second vaccine doses.
There were no previously published reports detail-ing the manner in which practicdetail-ing pediatricians might handle the burden of implementing the new recommendations. Szilagyi et al53examined the the-oretical burden by assessing the number of addi-tional visits, compared with baseline values, that might be required to vaccinate children not usually treated during the influenza season, varying the time period during which vaccinations would be offered and the type of visits at which vaccinations would be administered. Their data suggested that, if a 4-month vaccination period was used, 54% of children would require 1 or 2 additional visits if only routine visits were used for vaccination and 29% would requireⱖ1 additional visit if all visits were used. These data were based on the assumption that practitioners would incorporate the extra volume into their usual schedule of visits. In the present study, although all of the practices administered influenza immuniza-tions at all types of visits during office hours, with substantial variation in the proportions of shots given at visits billed as well-child visits, the majority of the practices chose to absorb a substantial part of the excess demand by adding high-volume influenza immunization clinics. The practices varied with spect to whether they pulled medical records or re-quired appointments for these clinics, but in 3 of the 5 practices the influenza clinics operated substan-tially outside the usual office visit structure. This is consistent with data for adult populations that dem-onstrated higher influenza immunization rates in practices that conducted clinics geared to vaccinating large numbers of patients.59
The number of extra clinics required to achieve the reported rates gives some indication of the impact of implementation of the new guidelines. Our data were consistent with the theory that immunization of 6- to 11-month-old children would require fewer additional visits for influenza vaccine because those children are examined more frequently.53 Immuni-zation rates were higher for children 6 to 11 months of age, the recall intervention was more effective among children 12 to 21 months of age, and more children in the 6- to 11-month age group were im-munized in association with well-child visits, which suggests that more children in the younger subgroup were treated without being recalled. Our data also
demonstrated that relatively few children were im-munized during illness visits, which suggests that there might have been many missed opportunities. Comparisons of immunization rates for the target populations during the 2002–2003 and 2003–2004 seasons provide some insight into the burden of guideline implementation, although such compari-sons must be made with caution. Other factors, such as differences in the severity of the influenza out-breaks and variations in vaccine supplies between the 2 seasons, confound such between-year compar-isons. However, our data do illustrate that these practices were able to increase their capacities signif-icantly, in order to deliver influenza vaccine to many more children.
The maximal immunization rates achieved varied considerably among our practices. Although the number of practices involved in our study was too small for quantitative examination of the reasons for these differences, some of the strategies adopted by the 2 practices that achieved the highest rates are noteworthy. One practice chose to have high-vol-ume, after-hours and weekend shot clinics for which appointments were not required and no medical records were pulled. The other practice had more frequent shot clinics, scheduled during office hours 7 half-days per week. The least successful sites either did not have any shot clinics, attempting to incorpo-rate all increased volume into appointment slots, or had low-volume, after-hours clinics for which ap-pointments were required and medical records were pulled. Practices were most successful when access was easy and the administrative burden was light. Interestingly, 4 of the 5 practices immunized the adults who accompanied the young children, with obvious beneficial collateral effects. In addition to the differences in the ways the practices dealt with the practical issues specifically related to influenza im-munization, the observed differences may reflect fundamental structural or organizational differences among the practices. These observed responses to the extra burden of universal immunization of young children are likely to be correlated strongly with characteristics of the practice environment. Factors such as organizational policies, organizational cul-ture, motivations of key stakeholders, compensation practices, and market pressures from managed care organizations were found to be related to the deliv-ery of preventive care services in other studies.60–64 Additional analyses are underway to examine qual-itatively the contributions of structural and organi-zational factors to variations in rates among our practices.
effica-cious. The intensive media coverage of the influenza outbreak probably also increased the rates of immu-nization that were achieved in these practices. Con-versely, shortages of vaccine might have limited the maximal rates that could have been achieved. The epidemic did provide a natural experiment, allowing us to assess strategies used by the practices to im-munize large numbers of patients when demand was very high. There are also important issues regarding the generalizability of our data. The participating practices are part of a regional immunization regis-try, have participated in previous recall efforts, and are generally committed to increasing influenza im-munization rates. Although several of the practices treat Medicaid patients and have more economically heterogeneous patient populations, the patient pop-ulations in these practices are generally well edu-cated and middle class. Therefore, our data may present an optimistic view of the results that can be expected in other practice settings.
Our study provides the first data on the feasibility of universal influenza vaccination of young children in private pediatric practices. Overall, the results are very encouraging. Practices stood up well to the challenges of providing vaccine to large numbers of young children in a short period of time, despite an extensive outbreak of influenza that increased the overall number of visits and produced shortages of influenza vaccine. Reminder/recall was important to the success of the practices, especially in shifting the timing of vaccination to the period before the early epidemic developed. The highest immunization rates were achieved in practices that did not simply try to incorporate the extra volume into their usual schedules but were proactive in meeting the extra demand, primarily in designated influenza clinics. The outcome of this trial offers encouraging results and practical suggestions for private pediatricians facing the 2004 –2005 influenza season. Success is likely to be contingent on preseason education of practice providers and staff members, as well as parents of young children; a proactive and practice-wide strategy for managing the excess demand, pref-erably involving influenza clinics that maximize vol-ume and minimize the administrative burden; careful planning by practice office managers regard-ing anticipated doses of vaccine that will be needed and timing of influenza clinics to maximize delivery of second doses of vaccine; influenza reminder/re-call, if possible, especially for children 1 to 2 years of age, who are less likely to present for care for other reasons during the relevant time period than are children ⬍1 year of age; and maximization of all opportunities to immunize young children who present before or during the season for any type of visit. With advance preparation and, it is hoped, adequate influenza vaccine supplies, our data sug-gest that private pediatric practitioners should be optimistic about their ability to implement the new guidelines for universal immunization of healthy young children.
ACKNOWLEDGMENTS
This project was supported under a cooperative agreement with the Centers for Disease Control and Prevention through the Association of American Medical Colleges (grant MM-0752-04/ 04). M.F.D. was also supported by a Research Scholar Award from the Children’s Hospital Research Institute (Denver, CO). Addi-tional technical support was provided by the Colorado Immuni-zation Information System.
The contents of this report are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Association of American Medical Colleges.
REFERENCES
1. Thompson WW, Shay DK, Weintraub E, et al. Mortality associated with influenza and respiratory syncytial virus in the United States.JAMA.
2003;289:179 –186
2. Simonsen L, Fukuda K, Schonberger LB, Cox NJ. The impact of influ-enza epidemics on hospitalizations.J Infect Dis.2000;181:831– 837 3. Simonsen L, Clarke MJ, Schonberger LB, Arden NH, Cox NJ, Fukuda K.
Pandemic versus epidemic influenza mortality: a pattern of changing age distribution.J Infect Dis.1998;178:53– 60
4. Glezen WP, Keitel WA, Taber LH, Piedra PA, Clover RD, Couch RB. Age distribution of patients with medically-attended illnesses caused by sequential variants of influenza A/H1N1: comparison to age-specific infection rates, 1978 –1989.Am J Epidemiol.1991;133:296 –304
5. Longini IM Jr, Koopman JS, Monto AS, Fox JP. Estimating household and community transmission parameters for influenza.Am J Epidemiol.
1982;115:736 –751
6. Wright PF, Ross KB, Thompson J, Karzon DT. Influenza A infections in young children: primary natural infection and protective efficacy of live-vaccine-induced or naturally acquired immunity.N Engl J Med.
1977;296:829 – 834
7. Fox JP, Hall CE, Cooney MK, Foy HM. Influenzavirus infections in Seattle families, 1975–1979. I. Study design, methods and the occurrence of infections by time and age.Am J Epidemiol.1982;116:212–227 8. Monto AS, Sullivan KM. Acute respiratory illness in the community:
frequency of illness and the agents involved.Epidemiol Infect.1993;110: 145–160
9. Glezen WP, Couch RB. Interpandemic influenza in the Houston area, 1974 –76.N Engl J Med.1978;298:587–592
10. Foy HM, Cooney MK, Allan I. Longitudinal studies of types A and B influenza among Seattle schoolchildren and families, 1968 –74.J Infect Dis.1976;134:362–369
11. Frank AL, Taber LH, Wells CR, Wells JM, Glezen WP, Paredes A. Patterns of shedding of myxoviruses and paramyxoviruses in children.
J Infect Dis.1981;144:433– 441
12. Hurwitz ES, Haber M, Chang A, et al. Effectiveness of influenza vacci-nation of day care children in reducing influenza-related morbidity among household contacts.JAMA.2000;284:1677–1682
13. Glezen WP. Prevention of acute otitis media by prophylaxis and treat-ment of influenza virus infections.Vaccine.2000;19(suppl 1):S56 —S58 14. Neuzil KM, Zhu Y, Griffin MR, et al. Burden of interpandemic influenza
in children younger than 5 years: a 25-year prospective study.J Infect Dis.2002;185:147–152
15. Peltola V, Ziegler T, Ruuskanen O. Influenza A and B virus infections in children.Clin Infect Dis.2003;36:299 –305
16. Chiu SS, Tse CY, Lau YL, Peiris M. Influenza A infection is an important cause of febrile seizures. Pediatrics. 2001;108(4). Available at: www.pediatrics.org/cgi/content/full/108/4/e63
17. Douglas RG Jr. Influenza in man. In: Kilbourne E, ed.Influenza Viruses
and Influenza.New York, NY: Academic Press; 1975
18. McCullers JA, Facchini S, Chesney PJ, Webster RG. Influenza B virus encephalitis.Clin Infect Dis.1999;28:898 –900
19. Morishima T, Togashi T, Yokota S, et al. Encephalitis and encephalop-athy associated with an influenza epidemic in Japan.Clin Infect Dis.
2002;35:512–517
20. Glezen WP, Greenberg SB, Atmar RL, Piedra PA, Couch RB. Impact of respiratory virus infections on persons with chronic underlying condi-tions.JAMA.2000;283:499 –505
21. O’Brien MA, Uyeki TM, Shay DK, et al. Incidence of outpatient visits and hospitalizations related to influenza in infants and young children.
Pediatrics.2004;113:585–593
23. Iwane MK, Schwartz B. Pediatric influenza immunization: should healthy children be vaccinated?Pediatr Ann.2001;30:354 –357 24. Menec VH, Black C, MacWilliam L, Aoki FY. The impact of
influenza-associated respiratory illnesses on hospitalizations, physician visits, emergency room visits, and mortality.Can J Public Health.2003;94:59 – 63 25. Neuzil KM, Hohlbein C, Zhu Y. Illness among schoolchildren during influenza season: effect on school absenteeism, parental absenteeism from work, and secondary illness in families.Arch Pediatr Adolesc Med.
2002;156:986 –991
26. Glezen WP. Serious morbidity and mortality associated with influenza epidemics.Epidemiol Rev.1982;4:25– 44
27. Glezen WP, Decker M, Joseph SW, Mercready RG Jr. Acute respiratory disease associated with influenza epidemics in Houston, 1981–1983.
J Infect Dis.1987;155:1119 –1126
28. Mullooly JP, Barker WH. Impact of type A influenza on children: a retrospective study.Am J Public Health.1982;72:1008 –1016
29. Neuzil KM, Mellen BG, Wright PF, Mitchel EF Jr, Griffin MR. The effect of influenza on hospitalizations, outpatient visits, and courses of anti-biotics in children.N Engl J Med.2000;342:225–231
30. Izurieta HS, Thompson WW, Kramarz P, et al. Influenza and the rates of hospitalization for respiratory disease among infants and young children.N Engl J Med.2000;342:232–239
31. Surgeon General. Surgeon General’s Advisory Committee on Influenza Research Report of February, 1960.Public Health Rep.1960;75:944 32. Terebuh P, Uyeki T, Fukuda K. Impact of influenza on young children
and the shaping of United States influenza vaccine policy.Pediatr Infect
Dis J.2003;22(suppl):S231—S235
33. Centers for Disease Control and Prevention. Prevention and control of influenza: recommendations of the Advisory Committee on Immuniza-tion Practices (ACIP).MMWR Recomm Rep.1999;48(RR-4):1–28 34. Centers for Disease Control and Prevention. Surveillance for influenza:
United States, 1994 –95, 1995–96, and 1996 –97 seasons.MMWR CDC
Surveill Summ.2000;49(SS-3):13–28
35. Centers for Disease Control and Prevention. Prevention and control of influenza: recommendations of the Advisory Committee on Immuniza-tion Practices (ACIP).MMWR Recomm Rep.2002;51(RR-3):1–31 36. Centers for Disease Control and Prevention. Prevention and control of
influenza: recommendations of the Advisory Committee on Immuniza-tion Practices (ACIP).MMWR Recomm Rep.2003;52(RR-8):1–34 37. Centers for Disease Control and Prevention. Prevention and control of
influenza: recommendations of the Advisory Committee on Immuniza-tion Practices (ACIP).MMWR Recomm Rep.2004;53(RR-6):1– 40 38. American Academy of Pediatrics, Committee on Infectious Diseases.
Recommendations for influenza immunization of children.Pediatrics.
2004;113:1441–1447
39. American Medical Association. Current Procedural Terminology: CPT 2003. Chicago, IL: American Medical Association; 2002
40. Daley MF, Barrow J, Pearson K, et al. Identification and recall of children with chronic medical conditions for influenza vaccination.
Pediatrics.2004;113(1). Available at: www.pediatrics.org/cgi/content/
full/113/1/e26
41. National Immunization Program. 2001 minimum functional standards for immunization registries. Available at: www.cdc.gov/nip/registry/ min-funct-stds2001.htm. Accessed July 26, 2004
42. SAS Institute.SAS for Windows, Version 8.1. Cary, NC: SAS Institute; 1999 –2000
43. Centers for Disease Control and Prevention. Update: influenza activity: United States and worldwide, 2003– 04 season, and composition of the 2004 – 05 influenza vaccine.MMWR Morb Mortal Wkly Rep. 2004;53: 547–552
44. Centers for Disease Control and Prevention. Weekly report: influenza summary update: week ending October 11, 2003-week 41. Available at: www.cdc.gov/flu/weekly/weeklyarchives2003-2004/weekly41.htm. Accessed August 3, 2004
45. Centers for Disease Control and Prevention. Weekly report: influenza summary update: week ending November 29, 2003-week 48. Available
at: www.cdc.gov/flu/weekly/weeklyarchives2003-2004/weekly48.htm. Accessed August 3, 2004
46. Colorado Department of Public Health and Environment. News release, Tuesday, November 4, 2003: flu hits Colorado early: Coloradans re-minded of importance of receiving flu shots. Available at: www.cdphe. state.co.us/release/2003/110403.html. Accessed August 3, 2004 47. Colorado Department of Public Health and Environment. News release,
Wednesday, November 26, 2003: state health department reports 3,957 confirmed flu cases. Available at: www.cdphe.state.co.us/release/ 2003/112603.html. Accessed August 3, 2004
48. Colorado Department of Public Health and Environment. News release, Friday, December 5, 2003: state health officials recommend targeting of remaining flu vaccine. Available at: www.cdphe.state.co.us/release/ 2003/120503.html. Accessed August 3, 2004
49. Szilagyi PG, Rodewald LE, Savageau J, Yoos L, Doane C. Improving influenza vaccination rates in children with asthma: a test of a comput-erized reminder system and an analysis of factors predicting vaccina-tion compliance.Pediatrics.1992;90:871– 875
50. Gaglani M, Riggs M, Kamenicky C, Glezen WP. A computerized re-minder strategy is effective for annual influenza immunization of chil-dren with asthma or reactive airway disease.Pediatr Infect Dis J.2001; 20:1155–1160
51. American Academy of Pediatrics, Committee on Infectious Diseases. Reduction of the influenza burden in children. Pediatrics.2002;110: 1246 –1252
52. Zimmerman RK. Recommended childhood and adolescent immuniza-tion schedule, United States, 2003, and update on childhood immuni-zations.Am Fam Physician.2003;67:188, 190, 195–196
53. Szilagyi PG, Iwane MK, Schaffer S, et al. Potential burden of universal influenza vaccination of young children on visits to primary care prac-tices.Pediatrics.2003;112:821– 828
54. Phillips CF, Phillips CA, Hodgkin WE, Forsyth BR, Rubin BA, Geraghty ME. Killed subunit influenza vaccine in children.Pediatrics.1973;52: 416 – 419
55. Wright PF, Thompson J, Vaughn WK, Folland DS, Sell SH, Karzon DT. Trials of influenza A/New Jersey/76 virus vaccine in normal children: an overview of age-related antigenicity and reactogenicity.J Infect Dis.
1977;136(suppl):S731—S741
56. Gruber WC, Taber LH, Glezen WP, et al. Live attenuated and inacti-vated influenza vaccine in school-age children.Am J Dis Child.1990;144: 595– 600
57. Neuzil KM, Dupont WD, Wright PF, Edwards KM. Efficacy of inacti-vated and cold-adapted vaccines against influenza A infection, 1985 to 1990: the pediatric experience.Pediatr Infect Dis J.2001;20:733–740 58. Centers for Disease Control and Prevention. Assessment of the
effec-tiveness of the 2003– 04 influenza vaccine among children and adults: Colorado, 2003.MMWR Morb Mortal Wkly Rep.2004;53:707–710 59. Zimmerman RK, Nowalk MP, Bardella IJ, et al. Physician and practice
factors related to influenza vaccination among the elderly.Am J Prev Med.2004;26:1–10
60. Cohen D, McDaniel RR Jr, Crabtree BF, et al. A practice change model for quality improvement in primary care practice.J Healthc Manag.
2004;49:155–168
61. Vaughn TE, Ward MM, Doebbeling BN, Uden-Holman T, Clarke WT, Woolson RF. Organizational and provider characteristics fostering smoking cessation practice guideline adherence: an empirical look.
J Ambul Care Manage.2002;25:17–31
62. Landon BE, Wilson IB, Cleary PD. A conceptual model of the effects of health care organizations on the quality of medical care.JAMA.1998; 279:1377–1382
63. Shortell SM, Jones RH, Rademaker AW, et al. Assessing the impact of total quality management and organizational culture on multiple out-comes of care for coronary artery bypass graft surgery patients.Med
Care.2000;38:207–217
DOI: 10.1542/peds.2004-1804
2005;115;146
Pediatrics
Brenda L. Beaty, Lori A. Crane, Kellyn Pearson and Stephen Berman
Allison Kempe, Matthew F. Daley, Jennifer Barrow, Norma Allred, Nellie Hester,
Registry-Based Recall
Healthy Young Children: Results of a Randomized, Controlled Trial With
Implementation of Universal Influenza Immunization Recommendations for
Services
Updated Information &
http://pediatrics.aappublications.org/content/115/1/146
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/115/1/146#BIBL
This article cites 52 articles, 6 of which you can access for free at:
Subspecialty Collections
b
http://www.aappublications.org/cgi/collection/infectious_diseases_su
Infectious Disease following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2004-1804
2005;115;146
Pediatrics
Brenda L. Beaty, Lori A. Crane, Kellyn Pearson and Stephen Berman
Allison Kempe, Matthew F. Daley, Jennifer Barrow, Norma Allred, Nellie Hester,
Registry-Based Recall
Healthy Young Children: Results of a Randomized, Controlled Trial With
Implementation of Universal Influenza Immunization Recommendations for
http://pediatrics.aappublications.org/content/115/1/146
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.