The Transformation of Pediatric Education With
a Focus on the Subspecialists
Members of the academic societies, colleagues, and friends: I’m deeply honored to receive the Joseph W. St Geme Jr Leadership Award today on its 25th anniversary in my home town of Boston with the opportunity to share the joy with my family. As I review the names of the previous recipients, I am humbled to be in their company. Although I did not know Dr St Geme personally, I have had the wonderful opportunity to work closely with many of the recent recipients of this award, who have served as mentors, role models, colleagues, and indeed, close friends.
Since I have not been as fortunate as many other recipients in having the opportunity to work directly with Dr St Geme, in preparation for this address I took time to review and reflect on a wonderful series of commentaries that he wrote in the 1980s that were published in Pe-diatrics.1–6I learned a number of things about Dr St Geme. He wrote and spoke with great clarity. He was straightforward in his approach and he cared passionately about education, training, and the quality of care that we provide to our patients. He carried forth a message of optimism, always looking toward the future and anticipating change. I suspect he would be very surprised, and perhaps bothered by, some of the changes under consideration in the realm of pediatric education today. But I hope he would be pleased with the rigor and the thoughtfulness that have been brought to this endeavor. I would like to use this opportunity to address pediatric education and its current transformation with particular focus on the subspecialties.
MORE THAN A DECADE OF CHANGE
Just as societal mandates for quality, accountability, and evidence-based assessment of clinical outcomes are transforming pediatric health care and the way in which we practice pediatrics, a similar transformation is occurring in graduate medical education (GME). There has been more than a decade of extraordinary change. The change began when the 6 general physician competencies were articulated by the Accreditation Council of Graduate Medical Education (ACGME) and the American Board of Medical Specialties.7The educational paradigm was reframed from one of process measurement, that is, the potential to educate, to the measurement of actual accomplishments or outcomes.8The ultimate outcome, of course, is the quality of care provided to our patients. David Leach, who spearheaded the Outcomes Project at ACGME when he served as its chief executive officer, often said“what we measure we tend to improve.”9Implicit in this transformation is the use of formal measurements to assess educational effectiveness and the attainment of competencies.
The focus on outcomes and their measurement was an enormous change that at times has engendered skepticism and concern. A colleague in AUTHOR:Gail A. McGuinness, MD
American Board of Pediatrics, Chapel Hill, North Carolina
KEY WORDS
graduate medical education, residency and fellowship training, subspecialties, competency-based education
ABBREVIATIONS
ABP—American Board of Pediatrics
ACGME—Accreditation Council of Graduate Medical Education FOPE—Future of Pediatric Education
GME—graduate medical education
IIPE—Initiative for Innovation in Pediatric Education MedPAC—Medicare Payment Advisory Commission R3P—Residency Review and Redesign in Pediatrics
Dr McGuinness was the sole author of this special article.
The contents of this work were derived from an invited lecture by the author upon presentation of the 2012 Joseph W. St Geme Jr Leadership Award at the meeting of the Pediatric Academic Societies on April 28, 2012, in Boston, Massachusetts.
www.pediatrics.org/cgi/doi/10.1542/peds.2012-3790
doi:10.1542/peds.2012-3790
Accepted for publication Jan 25, 2013
Address correspondence to Gail A. McGuinness, MD, American Board of Pediatrics, 111 Silver Cedar Court, Chapel Hill, NC 27514. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The author indicated she has no
financial relationships relevant to this article to disclose.
FUNDING:No external funding.
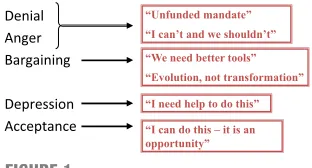
typical grief reaction as shown in Fig 1. As GME undergoes transformation, change has led to initial reactions of denial and anger with progression to increased acceptance of change as an opportunity. The discipline of pediat-rics has seized the opportunity and in many ways has been in the forefront for a number of reasons. There have been collaborative efforts of many of the organizations within pediatrics, including the Association of Pediatric Program Directors, the American Academy of Pediatrics, the American Board of Pediatrics (ABP), and the Federation of Pediatric Organizations as outlined in Table 1. There has been active engagement with the other primary care specialties around resi-dency redesign and faculty devel-opment. The effort in pediatrics began with the Future of Pediatric Education (FOPE) II in 2000 and has continued to the present time as we are beginning to embark on the Milestones Project, a joint effort of the ACGME and the ABP.
FOPE II made 2 recommendations that were very forward looking at the time,11 and relate to a theme you will hear throughout my address. FOPE II em-braced flexibility to accommodate a broad range of individual career goals and recommended that each resident should have an individualized learning plan that incorporates anticipated needs for future practice.
dation, which was called The Residency Review and Redesign in Pediatrics (R3P) Project.12 It started out as an initiative to address the duration and content of general pediatrics training and to make specific recommenda-tions for the future. But it morphed over several years of deliberation in an extraordinary way. It evolved into an ongoing process of innovation leading to goal-directed change, that is, a quality improvement model of GME that was to build on local strengths while fostering educational collaboration. It was in perfect synchrony with the ACGME Outcomes Project. The project is now ongoing and is supported by an entity known as the Initiative for Inno-vation in Pediatric Education (IIPE),13,14 which is serving as the infrastruc-ture to support and foster outcome-directed experimentation in general pediatrics residencies. The IIPE is pro-viding the framework in which in-novation can move forward. The goals of the R3P Project and the IIPE are to create flexibility in training to meet diverse career goals, to develop a con-tinuum of education from medical school through a lifetime of practice, and to address gaps between the cur-rent and the optimal health care out-comes of our patients by educating our residents and fellows in the science and practice of quality improvement.
The next step in the journey is the Pe-diatrics Milestones Project,15,16 which
competency-based learning and as-sessment to the next level, to refine the language of competence in the context of pediatrics and, to make the 6 general physician competencies more mean-ingful as they center around
speci-fic clinical activities that can be observed.17The charge was to develop benchmarks that in the aggregate ad-dress the general competencies, to define the expected performance across the continuum, and to identity or develop tools to be used to measure performance.
EXTERNAL INFLUENCES ON MEDICAL EDUCATION: A CALL FOR REFORM
Medical education across the contin-uum from medical school through GME is under increasing stress due to lim-ited resources, concerns about the adequacy of the workforce, and greater public accountability. There is a major call to redesign the education of our health care workforce that improves access to services and creates high-quality and lower-cost health care. The Medicare Payment Advisory Com-mission (MedPAC) has called for major changes in GME financing,18and GME
financing, as we know it today, is in jeopardy. The MedPAC report has con-cluded that society is not getting an appropriate return on its 9-billion-dollar investment in GME. There is an intent to leverage GME payment poli-cies to accelerate change in resident education and to improve care co-ordination, care in the nonhospital setting, multidisciplinary teamwork, and information technology.
The ACGME has put into place new duty hour regulations19 and is embarking on the Next Accreditation System,20 which will use milestones to assess performance and to evaluate training
FIGURE 1
Changes in GME and the grief reaction. Eric S. Holmboe, MD (Figure provided courtesy of Dr Holmboe with permission, American Board of Internal Medicine, 2010).
TABLE 1 Collaborative Efforts of the Pediatric Organizations to Transform GME
•Future of Pediatric Education (FOPE) II—2000 •Residency Review and Redesign in Pediatrics
(R3P)—2005
•Initiative for Innovation in Pediatric Education (IIPE)—2009
programs. A number of private foun-dations are weighing in including the Macy21and the Carnegie Foundations.22 Congress has just recently called for an Institute of Medicine committee to ana-lyze the governance and financing of GME and to propose specific reforms.
The Macy Foundation made recent recommendations for reforming GME, which are very likely to impact the decisions of the Institute of Medicine. The recommendations have focused on many issues but one I would like to emphasize relates to the length of training. The 2011 Macy report21states that an individual’s readiness for in-dependent practice should not be tied to a fixed duration of training but rather be demonstrated by the fulfi ll-ment of specialty specific standards, ie, the milestones. The defined period of prerequisite general specialty training before subspecialty fellowship should be evaluated and, where possible, shortened. Finally, opportunities to re-duce the duration of subspecialty fel-lowship training should be explored. The clear message is that flexibility should be allowed and encouraged at both the program and the individual trainee’s level.
WHAT ABOUT THE SUBSPECIALISTS?
Whereas the discipline of pediatrics has focused most intently on robust resi-dency redesign, there have also been repetitive calls to reevaluate subspe-cialty training over the last 15 years as outlined in Table 2.11,23–26Beginning in 1999, James Stockman23 addressed this topic when he received the St Geme Award. Most recently, in 2011, Gary Fleisher26touched on the issue in his American Pediatric Society presi-dential address. Although the views of these individuals and various work-groups differ and each proposed somewhat different models as to how subspecialty training could be
redesigned, all emphasized the need forflexibility in the education of sub-specialists with different pathways dependent on the ultimate goal of training.
In 2004, after several years of wide-ranging deliberations by the pediatric subspecialty community, the ABP made changes in the requirements for sub-specialty training and certification.27 But the focus was exclusively on re-quirements for research or scholarly activity. There have been no recom-mendations about clinical training despite the increasing interest in a competency-based approach to expec-tations for clinical performance. All subspecialists are held to the same training model: 3 years of training in-cluding a scholarly component as well as clinical experiences without speci-fying the duration of either.
There continues to be major concern about the availability of subspecialty care for children with perceived shortages in many subdisciplines. The interest in pediatric subspecialty ca-reers is at an all-time high. Based on a survey of residents, at the time of the ABP’s 2011 In-Training Examination, 51% of third year pediatric residents plan to pursue fellowship training. Since 1998 there has been more than a doubling in the number offirst-year fellows, with 1412 entering training in 2011. There has been a change in de-mographics of those interested in sub-specialty training, with an increasing
percentage of fellows who are gradu-ates of US medical schools and who are women. This trend is beginning to more closely approximate the demographics in pediatric residency training pro-grams.
There has been a long-held perception that the private practice rates among subspecialists are low; however, a re-cent publication by Freed et al28calls that assumption into question. The study provided data obtained from a survey of a random-stratified na-tional sample of nearly 1700 sub-specialists in 5 different subspecialties to assess their clinical practice set-tings. Overall, only 65% were working in academic settings. This percentage ranged from a low of 49% in neo-natology to a high of 77% in hematology-oncology.
The Federation of Pediatric Organ-izations has endorsed a policy statement about pediatric fellowship training. The statement wasfirst issued in 1988 and has evolved over the years. The most recent statement in 200429opined that the goal of subspecialty training is to develop future academic pediatricians. But there was a new phrase that appeared in the policy statement for thefirst time:“ie: while recognizing the diverse roles they now play.” This is a clear acknowledgment that within our academic institutions, subspecialists are no longer all engaged in a combi-nation of clinical care, education, and research.
It is time for us to reexamine the current “one size fits all” model of pediatric subspecialty fellowship training and certification and make changes in that model, if they are warranted after careful evaluation and deliberation. We have begun the process with a new Initiative on Subspecialty Clinical Training and Certification convened by the ABP Foundation in 2010.30The on-going discussions have identified a number of common themes that have TABLE 2 Repetitive Calls to Reevaluate
Subspecialty Training
1999: James Stockman (St Geme Award Address) 2000: FOPE II (Pediatric Subspecialists of the Future
Workgroup Report)
2001: Thomas Boat (APS Presidential Address) 2001: FOPO Subspecialty Forum Report 2011: Gary Fleisher (APS Presidential Address)
Each call to reevaluate training emphasizes the need for
flexibility in the education of subspecialists with different pathways dependent on the ultimate goal of training. APS, American Pediatric Society; FOPO, Federation of Pediatric Organizations.
subspecialties requires reevaluation. There is considerable variation be-tween and within subspecialties, both in terms of the design and content of training programs and the career paths of the graduates. Many feel that 3 years of training for all subspecialists may serve no one very well. The phy-sician scientist may need a longer training period with protected time and financial support and clinicians may benefit from altered training that might imbed advanced clinical compe-tencies. There continues to be a strong sentiment that scholarship is a core value and that fellows must learn to analyze, interpret, and apply research evidence at the point of care. There is a continued call forflexibility during fel-lowship recognizing that the flexibility that is already available is not fully used.
There are a number of questions that we need to carefully consider:
What is good about our current train-ing requirements and what should be preserved? How closely should training align with the diversity of professional practice in a subspecialty? If moreflexibility is desirable, whatspecifically is meant by this notion that can’t be achieved in our cur-rent model?
Should training in different sub-specialties vary in length with a shorter minimum, perhaps 2 years? Should formal tracking be explored? Or is the flexibility that already exists sufficient to allow extended research training, clinical educa-tor tracks, and advanced clinical tracks?activities (clinical, scholarly, and procedural) and what should be expected of all fellows upon com-pletion of training?
The last is thorniest question of all. It will require hard work that is ongoing over time. Leaders in each subspecialty will need to come together and develop consensus around these core pro-fessional activities, and develop the curriculum to support these activities. Faculty will be required to engage in rigorous assessment of trainees on the basis of direct observation.
A WORD ABOUT TIME
I would like to end with a word about time. It is obvious from the external influences coming to bear on GME that there is a push to shorten training, to eliminate waste, increase efficiency, and decrease overall cost. A recent editorial commentary in theJournal of the American Medical Association31 was provocative in its premise that the length of undergraduate and graduate medical education could be decreased by 30% without harm. There were 2 statements pertinent to pediatrics: the
first is that the third year is not es-sential.“This year is mainly engaged in supervising and teaching interns, in taking electives, and in some cases, conducting research. While valuable, these activities are hardly essential.” The second comment was that learn-ing the patient care aspects of a sub-specialty could be accomplished in 1 or 2 years.“Time devoted to research is relevant only for that small number of trainees destined to become aca-demic researchers.”Many in pediatrics
value to time. But we need to think carefully about how that time can best be used.
This topic was recently addressed by Hodges32 in an article in Academic
Medicine in which he contrasted a tea-steeping (time-based) or i-Doc (outcomes-based) model of medical education. What is the value of time? It allows for immersion in the discipline and the development of professional identity. Certain elements of compe-tence require time to attain: problem solving, pattern recognition, judgment, capability for self-reflection. If we are going to assess competence in a meaningful and deliberate way, it will require repetitive observations by multiple observers and this will take considerable time. Last, there is the issue of personal development and a “sense of journey” on the way to becoming a pediatrician and a sub-specialist. The pressure for outcomes-based education has been building for a long time. The pure time-based approach is no longer sufficient. Our challenge according to Hodges is “to make sure once the dust settles we have not lost all the elements of time and context that mark the journey of becoming a physician.”
I would like to end with a quote by Dr St Geme that was published inPediatrics
in March 1983.2“Pediatrics is a disci-pline that deals with the future, chil-dren, and we must be prepared to move in that direction with our training and our practice. We must anticipate challenges which bring forth the best in the human spirit.”I believe we now have that challenge.
REFERENCES
1. St Geme JW Jr. Let’s speak up for pediatricians.Pediatrics. 1981;68(5):734– 735
2. St Geme JW Jr. Challenge of pediatric education. Pediatrics. 1983;71(3):442– 443
4. St Geme JW Jr. Treasures in the groves of academe.Pediatrics. 1984;74(2):289–290 5. St Geme JW Jr. In search of wonder and
wisdom: pediatrics in transition. Pediat-rics. 1985;76(2):308–310
6. St Geme JW Jr. Can we rediscover the bedside?Pediatrics. 1987;79(2):287–288 7. Batalden P, Leach D, Swing S, Dreyfus H,
Dreyfus S. General competencies and ac-creditation in graduate medical education. Health Aff. 2002;21(5):103–111
8. Swing SR. The ACGME outcome project: retrospective and prospective.Med Teach. 2007;29(7):648–654
9. Leach DC. Building and assessing compe-tence: the potential for evidence-based graduate medical education. Qual Manag Health Care. 2002;11(1):39–44
10. Holmboe E. Reflections from the IM per-spective. Available at: www.abp.org/abp-website/taskforce/invitconf/Holmboe%20 Presentation.pdf. Accessed February 16, 2013
11. Task Force on the Future of Pediatric Edu-cation. The future of pediatric education II. Organizing pediatric education to meet the needs of infants, children, adolescents, and young adults in the 21st century: a collab-orative project of the pediatric community. Pediatrics. 2000;105(1 pt 2):157–212 12. Jones MD, Leslie LK, McGuinness GA, eds.
Residency review and redesign in pediat-rics: new (and old) questions. Pediatrics. 2009;123(suppl 1):S1–S60
13. Initiative for Innovation in Pediatric Educa-tion (IIPE) Web site. Available at: http:// innovatepedsgme.org. Accessed March 10, 2012
14. Carraccio C, Englander R. Innovation in pediatric education: the path to transforming
pediatric graduate medical education. Pe-diatrics. 2010;125(4):617–618
15. Hicks PJ, Schumacher DJ, Benson BJ, et al. The pediatrics milestones: conceptual frame-work, guiding principles, and approach to development. J Grad Med Educ. 2010;2(3): 410–418
16. American Board of Pediatrics. The Pediatrics Milestones Project. Available at: https://www. abp.org/abpwebsite/publicat/milestones.pdf. Accessed April 8, 2012
17. Carraccio C, Burke AE. Beyond competen-cies and milestones: adding meaning through context.J Grad Med Educ. 2010;2 (3):419–422
18. MedPac. June 2009 report to the Congress: improving incentives in the Medicare pro-gram. Available at: www.medpac.gov/docu-ments.cfm. Accessed March 10, 2012 19. Nasca TJ, Day SH, Amis ES Jr; ACGME
Duty Hour Task Force. The new recom-mendations on duty hours from the ACGME Task Force.N Engl J Med. 2010;363(2):e3 20. Nasca TJ, Philibert I, Brigham T, Flynn TC.
The next GME accreditation system— ra-tionale and benefits.N Engl J Med. 2012;366 (11):1051–1056
21. Johns MME. Ensuring an effective physi-cian workforce for America. Proceedings of a conference sponsored by the Josiah Macy Jr Foundation, held in Atlanta, GA, Oct 24–25, 2010. New York, NY: Josiah Macy Jr Foundation; 2011. Available at: www.macyfoundation.org. Accessed April 3, 2012
22. Cooke M, Irby DM, O’Brien BC.Educating Physicians: A Call for Reform of Medical School and Residency. San Francisco, CA: Jossey-Bass; 2010
23. Stockman JA III. Issues related to sub-specialty education: weasel words in ac-tion.J Pediatr. 1999;135(6):669–674 24. Boat TF. Opportunity and response.Pediatr
Res. 2002;51(6):777–781
25. Jones MD Jr, Boat TF, Stockman JA III, et al. Federation of Pediatric Organizations sub-specialty forum.J Pediatr. 2001;139(4):487– 493
26. Fleisher GR. American Pediatric Society 2011 Presidential Address: earthquakes, tectonic shifts in graduate medical educa-tion, and the role of the APS infinding solid ground.Pediatr Res. 2011;70(6):647–651 27. American Board of Pediatrics. Training
requirements for subspecialty certification, 2004. Available at: https://www.abp.org/ abpwebsite/publicat/trainingrequirements. pdf. Accessed April 3, 2012
28. Freed GL, Dunham KM, Loveland-Cherry C, Martyn KK, Moote MJ; American Board of Pediatrics Research Advisory Committee. Private practice rates among pediatric sub-specialists.Pediatrics. 2011;128(4):673–676 29. Federation of Pediatric Organizations. Policy
statement: pediatric fellowship training. Pe-diatrics. 2004;114(1):295–296
30. American Board of Pediatrics. The Initiative on Subspecialty Clinical Training and Cer-tification 2011. Available at: https://www.abp. org/ABPWebStatic/#murl%3D%2FABPWebStatic %2Ftaskfrc.html%26surl%3D%2Fabpweb-site%2Ftaskforce%2Fisctc.htm. Accessed Jan 3, 2012
31. Emanuel EJ, Fuchs VR. Shortening medical training by 30%.JAMA. 2012;307(11):1143– 1144
32. Hodges BD. A tea-steeping or i-Doc model for medical education?Acad Med. 2010;85 (9 suppl):S34–S44
DOI: 10.1542/peds.2012-3790 originally published online March 25, 2013;
Services
Updated Information &
http://pediatrics.aappublications.org/content/131/4/767 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/131/4/767#BIBL This article cites 24 articles, 11 of which you can access for free at:
Subspecialty Collections
tatistics_sub
http://www.aappublications.org/cgi/collection/research_methods_-_s Research Methods & Statistics
dev_sub
http://www.aappublications.org/cgi/collection/teaching_curriculum_ Teaching/Curriculum Development
ub
http://www.aappublications.org/cgi/collection/career_development_s Career Development
b
http://www.aappublications.org/cgi/collection/medical_education_su Medical Education
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2012-3790 originally published online March 25, 2013;
2013;131;767
Pediatrics
Gail A. McGuinness
The Transformation of Pediatric Education With a Focus on the Subspecialists
http://pediatrics.aappublications.org/content/131/4/767
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.