Changes in insulin sensitivity in response to different
modalities of exercise: a review of the evidence
S. Mann
1*
C. Beedie
2S. Balducci
3S. Zanuso
1J. Allgrove
1F. Bertiato
4A. Jimenez
51UKactive Research Institute,
University of Greenwich, Chatham Maritime, UK 2Department of Sport and
Exercise Sciences, Aberystwyth University, Aberystwyth, UK
3Clinical Science, University of Rome
Sapienza, Monterotondo, Italy 4Faculty of Sport Science,
University of Verona, Verona, Italy 5Institute of Sports,
Exercise and Active Living, ISEAL, Victoria University, Melbourne, Australia
*Correspondence to: S. Mann, School of Science, University of Greenwich, Chatham Maritime, ME4 4TB, UK.
E-mail: [email protected]
Summary
Type 2 diabetes is an increasingly prevalent condition with complications in-cluding blindness and kidney failure. Evidence suggests that type 2 diabetes is associated with a sedentary lifestyle, with physical activity demonstrated to increase glucose uptake and improve glycaemic control. Proposed mechanisms for these effects include the maintenance and improvement of insulin sensitiv-ity via increased glucose transporter type four production. The optimal mode, frequency, intensity and duration of exercise for the improvement of insulin sensitivity are however yet to be identified. We review the evidence from 34 published studies addressing the effects on glycaemic control and insulin sensi-tivity of aerobic exercise, resistance training and both combined. Effect sizes and confidence intervals are reported for each intervention and meta-analysis presented. The quality of the evidence is tentatively graded, and recommenda-tions for best practice proposed. © 2013 The Authors. Diabetes/Metabolism Research and Reviewspublished by John Wiley & Sons, Ltd.
Keywords insulin sensitivity; aerobic exercise; resistance training; combined modalities
Introduction
Diabetes is responsible for over one million amputees worldwide each year, is a major cause of blindness and is the largest cause of kidney failure in the devel-oped world [1]. The prevalence of type 2 diabetes (T2D) is alarming. In 2010, 285 million people worldwide were classified as suffering with the disease, a figure that is expected to rise to 438 million by 2030 [2]. Latest available figures indicate that 8.3% of the US population [3] and 5.1% of the UK popu-lation have the disease [4]. In 2010, the estimated cost of treatment in the UK was £3.5bn per year [5], with US costs estimated at $174bn in 2007 [3].
Type 2 diabetes is characterized by elevated glucose levels in circulating blood, caused by impairment in glucose tolerance following the development of insulin resistance and relative insulin deficiency. Insulin resistance/reduced insulin sensitivity impair the ability of the muscle cells to take up and store glu-cose and triglycerides. This results in higher levels of gluglu-cose and triglycerides circulating in the blood. In a healthy individual, insulin is secreted in response to these rising levels. However, if this does not occur or has little effect, blood glucose levels increase, leading to T2D as recognized by the American Diabetes Associa-tion [22]. This level of impaired glucose control is regarded as a major risk factor of cardiovascular disease [6].
Received: 4 February 2013 Revised: 10 September 2013 Accepted: 8 October 2013
The gold standard measure of insulin sensitivity is ascertained via a hyperinsulinemic euglycaemic clamp – this is however highly invasive and time consuming [7]. As a consequence, other validated methods of data collec-tion are often used to predict or indirectly measure insulin sensitivity; these include glycated haemoglobin (HbA1c) levels in both normoglycaemic [8] and hyperglycaemic pa-tients [9], the oral glucose tolerance test [10], homeostatic model assessment (HOMA) [11] and,finally, a calculation using glycaemic and insulin levels upon fasting [7].
A positive energy balance, indicating more energy be-ing be-ingested than expended, results from low levels of physical activity (PA) and a high calorific diet, resulting in raised levels of glucose and triglycerides in the blood. The muscular contractions associated with PA have the ability to increase glucose uptake via increased glucose transporter type four (GLUT 4) production and increased insulin signalling within skeletal muscle–thus increasing insulin sensitivity [12]. Using PA to maintain or increase insulin sensitivity in individuals at risk of T2D may help to reduce its incidence and lower the economic burden T2D places upon societies.
A sedentary lifestyle has been associated with increased levels of HbA1c[13]. HbA1cindicates average plasma glu-cose concentration over time, with higher levels indicat-ing poor blood glucose control and decreases in insulin sensitivity that are associated with T2D [14] (≥6.5% is ac-cepted as a criterion for diagnosis of T2D [13]). It has been reported that lifestyle modifications inclusive of a PA programme are at least as effective in treating T2D as any single pharmacological agent [15], and increased levels of PA are associated with significantly delaying the onset of T2D. Further, changes in insulin sensitivity occur independently of changes in body weight [16]. This suggests that PA might function to decrease hepatic and muscle insulin resistance and increase glucose disposal through a number of mechanisms not necessarily associ-ated with body weight. Such mechanisms might include increased post-receptor insulin signalling and increased glucose transporter proteins [16]. Although it has previously been shown that there is a positive relationship between T2D and obesity [17], these results suggest that the association is the result of the sedentary behaviour as-sociated with both conditions, as opposed to one being a direct cause of the other. These findings could influence the way in which T2D is managed and prevented; that is, hypothetically basing recommendation on the promo-tion of weight loss alone in the absence of PA might be unproductive.
Chomistek et al. [18] found that men who completed greater levels of vigorous PA (>6 METs)–as detailed in the Health Professionals Follow-up Study (n= 18 225)– exhibited lower levels of HbA1c. Furthermore, those reporting that they completed more than 3 h of
vigorous PA per week had a 22% lower risk of myocar-dial infarction, for which lower HbA1c is a potential mediator. Larsson et al. [19] found an inverse associa-tion (p<0.05) between self-report leisure time PA and insulin resistance (n= 1745– Swedish participants aged 30–74 years), whereas Dwyeret al. [20] reported that by increasing daily step count over a 5-year period, insulin sensitivity, measured via HOMA, could be increased [n= 592–mean age 51.4 (men) 50.3 years (women)]. The authors attribute this improvement to reductions in body mass index (BMI) and waist-to-hip ratio. Further and perhaps most significantly, there was a linear relationship between daily step count and improve-ments in insulin sensitivity. Those sedentary individuals able to alter their behaviour to meet 10 000 steps per day increased insulin sensitivity threefold compared with a similar person who increased to only 3000 steps [20]. These data suggest a dose–response relationship between PA and insulin sensitivity.
The aforementioned evidence suggests that PA can maintain (i.e. prevent decreases in) insulin sensitivity. There may be a dose–response relationship between the volume [20] and energy expenditure [18] of PA and improvements in insulin sensitivity. This would suggest that an increase in volume and intensity of PA might elicit greater improvements in insulin sensitivity. This would es-sentially entail an increase in PA meeting the minimum number of METs per week.
The terms ‘PA’ and ‘exercise’ are often used inter-changeably in the literature. However, it was suggested in the Physical Activity and Health report of the US Surgeon General [21] that the two terms denote two different concepts [21]. PA refers to any bodily movement produced by skeletal muscles that results in an expendi-ture of energy (expressed in kilocalories) and includes a broad range of occupational, leisure and daily activities. Exercise instead refers to planned or structured PA and can be aerobic exercise (AE), resistance training (RT) or combined aerobic and resistance (COM).
In relation to T2D and PA, recent reports by the Ameri-can College of Sports Medicine (ACSM) [22] and the Physical Activity Guidelines Advisory Committee [23] highlight the need to design a programme that will pro-vide appropriate exercise to attain maximal benefit at the lowest level of risk. However, despite a large number of related publications – PubMed searches post-1965 (01/10/2012) for‘insulin sensitivity exercise’and‘insulin sensitivity PA’located 5329 and 4895 articles, respectively (the authors note many articles will appear in both searches)–the optimal modes, intensities and frequencies of exercise in this context are unknown.
recommendations for exercise in the improvement of insu-lin sensitivity are presented.
Selection criteria
A comprehensive PubMed search was conducted for articles published between 1965 and 01/10/2012 (search terms were ‘aerobic exercise’, ‘resistance training’,
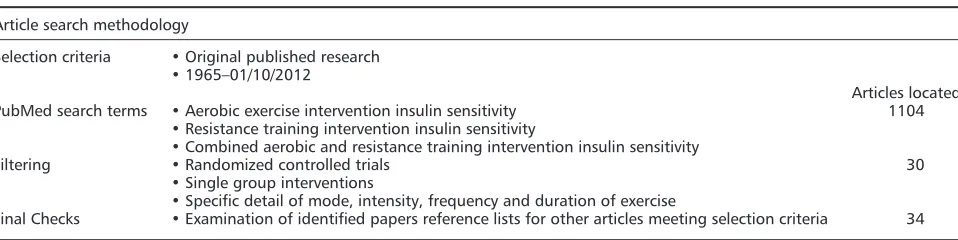
‘combined aerobic and resistance training’ ‘intervention’ and‘insulin sensitivity’). Reference lists of identified articles were also searched, and potentially relevant additional papers identified. Articles were selected if specific to the nature of this review, in that they assessed the impact of at least one of the different modes of exercise on insulin sensitivity in healthy or T2D participants. More specifically, articles were only selected if they contained data regarding the mode, intensity, frequency and duration of exercise un-dertaken (Table 1).
Thefindings of all studies meeting the inclusion criteria are presented in the sections later. These are classified by AE, RT and COM. By including in the present article only those articles providing details of the specific exercise com-pleted, the most effective interventions are identified, and evidence-based exercise recommendations made. In an attempt to ensure the recommendations made are relevant to the general population and specifically those suffering from T2D, investigations in which participants have underly-ing and unrelated conditions for which impaired insulin sen-sitivity is not a risk factor, and chronic diseases such as cancer [24] have been excluded. Studies involving participants with T2D and the metabolic syndrome (MetS) (clustering of multiple, partially or fully expressed metabolic abnormalities such as hypertension, dyslipidemia, obesity and impaired glucose tolerance [25]) have been included [26].
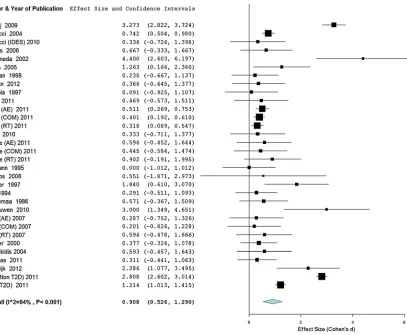
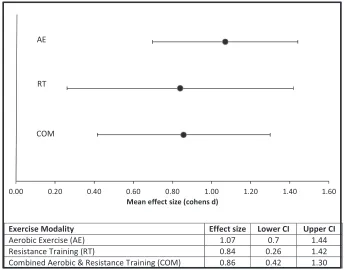
The interventions were evaluated by calculating the Cohen’sd[27] value (Table 2), presented visually in the Forest charts (Figures 1 and 2). All exercise interventions reviewed that present the mean and standard deviation of data pre-intervention and post-intervention have been
included in this analysis. It has not been possible to con-duct a full meta-analysis upon this data set because of the varying methods with which insulin sensitivity has been measured (Table 2).
Aerobic exercise
Lehmanet al. [28] reported that there was absolutely no alteration in HbA1cfollowing a 13-week intervention in-corporating 90-min sessions of AE three times a week at an intensity averaging 50–70% VO2max in participants with well-established (7.8 years) T2D. The exercise inter-vention did however protect against HbA1c increases reported in the control group, suggesting that although significant improvements could not be made, the manage-ment of blood glucose did improve. Similar participants (T2D average 7.1 years) were recruited by Rönnemaaet al. [29] who reported significant reductions in HbA1c follow-ing AE at an intensity of 70% VO2maxfor 45 min six times per week for 8 weeks–indicating that an increased fre-quency of exercise training will reduce HbA1c even in those with long-standing T2D. Mourier et al. [30] also elicited a significant decrease in HbA1cin T2D participants following an intervention lasting 10 weeks. The intensity of AE was set at 75% VO2peak, and participants completed three 55-min sessions a week. Raz et al. [31] replicated thesefindings, that is, a significant reduction in HbA1cin participants without T2D with an intervention also incorporating 55-min AE sessions three times each week, although at a lower intensity of 65% VO2max–the inter-vention did last 2 weeks longer however.
Kohno et al. [32] reported that within hospitalized hypertensive patients, significant reductions in plasma insulin were observed following exercise involving only a 3-min warm-up, a 6-min cycle at 75% VO2max and a 3-min cool down, performed four times daily for 3 weeks. This improvement has added significance as decreases in in-sulin sensitivity lead to a greater retention of magnesium and as a consequence increases in blood pressure [32],
Table 1. Article selection criteria and search methodology
Article search methodology
Selection criteria •Original published research
•1965–01/10/2012
Articles located
PubMed search terms •Aerobic exercise intervention insulin sensitivity 1104
•Resistance training intervention insulin sensitivity
•Combined aerobic and resistance training intervention insulin sensitivity
Filtering •Randomized controlled trials 30
•Single group interventions
•Specific detail of mode, intensity, frequency and duration of exercise
although could only be feasibly replicated in highly con-trolled environments such as hospitals because of the high frequency of exercise training.
Magkos et al. [33] demonstrated that an excess of 1 hour of moderate intensity exercise at 60% VO2max was required to improve whole body basal insulin sensitiv-ity. The same authors identified a curvilinear relationship between energy expenditure and insulin sensitivity in sin-gle bouts of exercise in recreationally active, non-obese men, whereby those expending the most energy saw the greatest benefits, providing further indications that insu-lin sensitivity is related to energy expenditure.
Van Dijket al. [34] investigated whether there was any benefit in exercising daily when compared with every other day if energy expenditure was controlled. No signif-icant between-group differences were observed in reduc-tions in fasting blood glucose (both were significantly improved by the intervention). Participants were asked to cycle for either 60 min every other day at 50% maximal
exertion or 30 min every day; thus, the energy expendi-ture was controlled between the two groups. This sug-gests that although energy expenditure is critical, everyday exercise may not elicit additional benefits over exercise every 2 days, whilst allowing time for recovery and presenting a far more palatable public health message.
High intensity exercise has been presented as an effective and time efficient way of improving insulin sensitivity [35]. Babrajet al. [35] implemented a protocol that consisted of four to six 30-s cycle sprints three times a week. This was shown to increase insulin sensitivity by 23% in young par-ticipants (mean age = 21 ± 2) of normal weight (mean BMI = 23.7 ± 3.1 kg/m2) in just 2 weeks. It must be noted however that this type of exercise may not be appropriate for some populations who may be at risk from such high levels of exertion.
This is a factor considered by Hood et al. [36] who designed a protocol for older, sedentary and overweight Table 2. Interventions effect size (Cohen’sd) and 95% confidence interval (lower and upper)
Author n Mode Measure Effect size Lower CI Upper CI
T2D participants
Lehmannet al. [28] 29 AE HbA1c 0.000 1.012 1.012
Rönnemaaet al. [29] 25 AE HbA1c 0.571 0.367 1.510
Mourieret al. [30] 21 AE HbA1c 1.840 0.610 3.070
Razet al. [31] 40 AE HbA1c 0.291 0.511 1.093
Van Dijket al. [34] 30 AE FBG 2.286 1.077 3.495
Vindet al. [39] (T2D) 26 AE IMGD 1.214 1.013 1.416
Jorgeet al. [43] 48 AE FPG 0.511 0.269 0.753
Jorgeet al. [43] 48 RT FPG 0.401 0.192 0.610
Jorgeet al. [43] 48 COM FPG 0.318 0.089 0.548
Honkolaet al. [44] 38 RT HbA1c 0.091 -o.925 1.107
Dunstanet al. [45] 27 RT FPG 0.235 0.667 1.138
Castanedaet al. [47] 62 RT HbA1c 4.400 2.603 6.197
Cauzaet al. [48] 22 RT HbA1c 1.263 0.166 2.360
Kwonet al. [50] 28 RT HbA1c 0.333 0.711 1.377
Brookset al. [51] 62 RT HbA1c 0.667 0.333 1.666
Tessieret al. [53] 39 COM OGTT 0.377 0.324 1.078
Balducciet al. [54] 120 COM FPG 0.742 0.504 0.980
Tokmakidis et al. [55] 9 COM HbA1c 0.593 0.457 1.642
Sigalet al. [57] 251 AE HbA1c 0.287 0.752 1.326
Sigalet al. [57] 251 RT HbA1c 0.201 0.826 1.227
Sigalet al. [57] 251 COM HbA1c 0.594 0.478 1.666
Laroseet al. [59] 251 AE HbA1c 0.596 0.452 1.643
Laroseet al. [59] 251 RT HbA1c 0.445 0.584 1.474
Laroseet al. [59] 251 COM HbA1c 0.902 0.191 1.996
Balducciet al. [60] 606 COM HbA1c 0.336 0.726 1.398
Mean effect size (T2D participants) 0.780 0.112 1.671
Non-T2D participants
Magkoset al. [33] 30 AE HOMA 0.551 1.871 2.913
Babrajet al. [35] 16 AE CI 3.273 2.822 3.723
Hoodet al. [36] 7 AE FPI 0.469 0.573 1.51
Vindet al. (2011) (non-T2D) 26 AE IMGD 2.808 2.602 3.013
Totsikaset al. [42] 219 AE OGTT 0.311 0.441 1.063
Hansenet al. [49] 18 RT 2HGLT 0.366 0.645 1.376
Schrauwen-Hinderlinget al. [56] 14 COM FBG 3.000 1.349 4.651
Mean effect size (non-T2D participants) 1.540 0.463 2.607
participants (mean age = 45 ± 5, mean BMI = 27 ± 5 kg/m2) that consisted of six sessions of 10 times 1-min cycles at 60% peak power separated by 1-min rest intervals. GLUT 4 protein content increased by 260%, whereas insulin sen-sitivity improved by 35% after 2 weeks of training (three sessions per week). A combination of low intensity cycling and two all-out sprints increasing from 10 to 20 s improved insulin sensitivity by 28% after 6 weeks of training [37]. Metcalfeet al. reported that the average rate of perceived exertion score for each session was 13 and that adherence was 97%, an important consideration when designing public health interventions.
These studies suggest that customizing interval training for differing individuals/populations may present a practi-cal and time-efficient strategy for improving glycaemic control. When all-out exercise is not feasible, that is, in the elderly or new to exercise, the intensity can be lowered to 60% maximal, and duration increased to 1 min and still be effective [36].
Yfantiet al. [38] investigated whether antioxidant sup-plementation in healthy physically active men (n= 21) could enhance the effects of aerobic endurance training upon insulin sensitivity. It was found that following
12 weeks of trainingfive times a week, insulin-stimulated glucose uptake increased by 17.2% in the supplementa-tion group. The placebo group improved by 18.9%. Although these data suggest no beneficial effects of anti-oxidant supplementation upon insulin sensitivity, clear ef-fects of exercise were evident. In all participants, these improvements were augmented by significant increases in GLUT 4, hexokinase II and protein kinase B (Akt), which play key roles in glucose metabolism. Vind et al. [39] propose similar mechanisms for the improvements in insu-lin-mediated glucose disposal observed following an aero-bic training programme consisting of 10 weeks training on a stationary cycle four to five times a week at approxi-mately 65% VO2max. Subjects were obese, the experimen-tal group with T2D (n= 26) and normoglycaemic controls. Significant improvements were observed in both groups (~20%), but the glucose disposal rates of the dia-betic patients remained 38% lower than their non-diadia-betic counterparts. This suggests that although insulin sensitivity was increased, 10 weeks is not long enough to improve glucose disposal to non-T2D levels.
Not all aerobic training programmes are associated with improvements in insulin sensitivity. Mujumdaret al. [40]
implemented a 6-month programme that involved progres-sive marathon running training (6 miles per week increas-ing over time to 55) that did not significantly alter HOMA insulin resistance scores in middle-aged untrained partici-pants. Given thefindings earlier and elsewhere, this is sur-prising and might suggest either a chance outcome or even hint at publication bias in the area (i.e. there may be other unpublished data also suggesting a null effect. This is of course speculative). Either way, thefindings in ques-tion warrant replicaques-tion.
Bacchiet al. [41] compared supervised AE [three times a week over 4 months at 60–65% heart rate (HR) reserve] to RT (three times a week over 4 months at 70–80% 1RM– nine exercises covering all major muscle groups), both sig-nificantly reduced HbA1c. Effects did not differ between groups but were predicted by baseline HbA1c levels, subsequent increases in cardiorespiratory fitness (CRF) and reductions in truncal fat. These findings are at odds with those of Totsikas et al. [42] who reported that im-provements in insulin sensitivity were more likely in those with the highest CRF at baseline – and therefore likely poorer glycaemic control –following a lifestyle interven-tion. The authors provide little detail of the mechanisms that support thisfinding other than that the intervention was only partly supervised and that the participants with the greatest CRF were more compliant to exercise recommendations.
Jorgeet al. [43] found AE to be less effective than RT or COM in a comparative study. However, T2D patients who
completed 60 min of cycling at an intensity relative to lac-tate threshold three times a week for 12 weeks were able to significantly lower fasting plasma glucose.
Based upon the evidence of most published research meeting the selection criteria of this review, it can be con-cluded that AE is effective in improving insulin sensitivity at a variety of intensities and to differing degrees. Signifi -cant improvements can be elicited by interval training (high intensity exercise separated by rest intervals) [35,36] as well as continuous effort [33]. As one study suggests, however, there may be other training interventions that are as effective or even more effective at improving insulin sensitivity, which could include RT and COM.
Resistance training
Honkolaet al. [44] implemented RT within a circuit train-ing session twice a week for 22 weeks–each session last-ing 45 min and incorporatlast-ing two sets of 12–15 repetitions. It was reported that there were no alterations in HbA1clevels. Similar to Lehmanet al. [28], participants had well-established T2D (average 8 years). Once again, there was an increase in HbA1cfound in the control group however – suggesting that glycaemic control was im-proved if not overall HbA1clevels.
Dunstan et al. [45] investigated the effect of circuit weight training at 55% 1RM in 27 adults (mean age
51 years) three times a week for 8 weeks. The training programme elicited significant strength improvements in all exercises (demonstrating training effect) along with improvements in glucose and insulin levels following a 12-h fast when compared with controls [45]. Dunstan et al. [46] followed this work with an investigation incor-porating a higher intensity RT–75–80% 1RM–in older participants with T2D (n= 36 aged between 60 and 80 years) for an increased duration of 26 weeks. Both RT and the control group incorporated a weight loss programme. HbA1cwas reduced to a significantly greater extent following RT at both 13 and 26 weeks. There was no difference between body weight and fat mass reduc-tion between groups. RT increased lean mass however, al-though it was reduced following the weight loss programme alone. This data further strengthen the argu-ment that weight loss interventions to reduce the risk of T2D are flawed unless attempts are made to maintain muscle mass via RT. Eighty per cent 1RM was also the training intensity employed by Castanedaet al. [47] in el-derly T2D subjects (n= 62 mean age 66 years) three times a week over a shorter intervention period of 16 weeks. HbA1c was again significantly reduced with muscular glycogen stores increased, suggesting greater in-sulin action; no such changes were evident in the control group.
Cauzaet al. [48] compared the effects of a 4-month hy-pertrophic strength training programme with endurance training at 60% VO2maxupon measures of insulin sensitivity. Participants had T2D and trained on three non-consecutive days of the week. The RT group reduced HbA1cby 8.3% and significantly reduced blood glucose levels and insulin resis-tance. No such improvements were found in the AE training group.
Maximal RT (five sets, three to four repetitions at 60–85% 1RM) was compared with endurance RT (three sets, 12–15 repetitions at 45–65% 1RM) by Hansenet al. [49]. The intervention lasted 4 months, and all subjects had impaired glucose tolerance at baseline. It was observed that both interventions decreased insulin resistance but by differing mechanisms. Maximal RT increased muscular glu-cose uptake capacity, whereas endurance RT increased the insulin sensitivity of the muscles. Kwonet al. [50] investi-gated the effectiveness of low intensity RT (40–50% 1RM) and were unsuccessful at improving insulin sensitivity tested via the insulin tolerance test in overweight partici-pants with T2D. The training was conducted over a 12-week period, with exercise three times per week, suggesting that the intensity was the determinant factor and that intensities of over 50% are required to generate a significant response unless supplemented with increases in sets and repetitions [49].
Brookset al. [51] investigated the effects of 16 weeks RT– 60–80% 1RM (weeks 1–8) and 70–80% 1RM (weeks 10–14)
compared with conventional care in 62 T2D community-dwelling individuals over the age of 55 years. Insulin sensitivity (measured via HOMA and HbA1c) and mus-cle quality, that is, the strength per unit of musmus-cle mass, were both significantly improved compared with controls.
Possible mechanisms by which insulin action increases with exercise have been attributed to increased expres-sion of GLUT4 and other signalling proteins [26]. Holten et al. [26] investigated the mechanisms behind improve-ments in insulin sensitivity in subjects with T2D by employing an RT intervention (weeks 1 + 2 50% 1RM, weeks 3–6 70–80% 1RM – three sessions per week) in one leg only. Muscle biopsies taken post-intervention showed increases in GLUT4 and various insulin signalling protein activity levels in the trained leg only. This suggests that the improvements in insulin action were a result of local physiological adaptation. That adaptations occurred locally have implications for the use of RT as a method of increasing insulin sensitivity; it implies that large muscle groups should be trained to stimulate the greatest im-provements and, furthermore, that imim-provements will be greater if more muscles are activated.
Further mechanisms and inhibitors to RT upon insulin sensitivity were found when Layne et al. [52] compared RT subjects with and without the MetS. Eight weeks RT elicited improvements in both strength and stamina in all subjects. Insulin sensitivity however was only improved significantly in those without MetS. Layne et al. attribute these differences to changes in GLUT 4 levels, which increased 67% in non-MetS sufferers com-pared with 36% in the MetS group. Further, muscle 5 adenosine monophosphate-activated protein kinase rose 43% in non-MetS and only 8% in MetS. Conversely mus-cle mammalian target of rapamycin was higher in the MetS sufferers than in the non-MetS sufferers, suggesting that the higher activation of mammalian target of rapamycin inhibited the training-related increases in 5 adenosine monophosphate-activated protein kinase in those suffering from MetS, which would have increased GLUT 4 and hexokinase II levels and in turn increased glu-cose uptake by the muscles [52].
The evidence presented earlier suggests that RT is ef-fective in improving insulin sensitivity when the intensity is above 50% 1RM and that adaptations are made locally in the trained muscles.
Combined modalities
COM and their impact upon muscle insulin signalling in T2D patients were investigated [43]. Jorge et al. [43] investigated the effect of a 7-min exercise RT circuit incor-porating large muscle groups completed three times a week over 12 weeks,finding it to improve insulin resistance index scores by 65%. The addition of AE to the RT circuit elicited significantly greater improvements however – a 90% improvement in insulin resistance index scores.
Tessieret al. [53] combined AE at 60–79% HR max and RT (two sets of 20 repetitions) into sessions lasting 60 min, three times a week for 16 weeks. Significant improvements were reported in the oral glucose tolerance test. Balducci et al. [54] investigated 30 min of AE at 40–80% heart rate re-serve and 30 min of RT 40–60% 1RM (reassessed every 3 weeks) when completed three times a week by sedentary individuals. After 1 year, significant reductions in fasting blood glucose were observed, decreasing by 36 mg/dl. This suggests that previously sedentary individuals combining AE and RT, even at low intensities, can have positive outcomes, although the intervention period was particularly long.
A COM intervention lasting only 4 months was employed by Tokmakidis et al. [55] with female T2D post-menopausal subjects. The frequency and intensity of exercise employed were higher than those of the previ-ously cited study–two AE sessions per week beginning at 60–70% heart rate max and increasing to 70–80% after 2 months and two RT sessions a week at 60% 1RM (three sets of 12 repetitions). HbA1clevels decreased by 12.5%, whereas glucose tolerance improved by 38%.
Schrauwenet al. [56] investigated an even shorter 12-week intervention with obese but non T2D subjects (mean BMI = 29.9 ± 0.01 kg/m2). The intervention combined 30-min AE at 55% VO2max and RT at 75% 1RM (two sets × eight repe-titions, following eight repetitions at 55% warm-up) and was completed three times a week. Fasting blood glucose concen-trations were lowered from 6.3 ± 0.2 to 5.7 ± 0.2 mmol/L, and HbA1clevels significantly improved. Thesefindings suggest that positive effects can be observed following relatively short intervention periods (≥12 weeks) when incorporating both aerobic and RT in the same exercise session.
The three modes of exercise training assessed in this re-view were compared by Sigalet al. [57] in a randomized controlled trial involving participants ranging in age from 39 to 70 years. In this investigation, the COM group com-pleted the full AE and RT programmes (AE: 15–20 min 60% HR max progressing to 45 min 75% HR max three times a week RT. Two/three sets at max weight lifted seven to nine times, three times a week), and conse-quently, the training volume was far greater than in the other groups. This was reflected in the results, which showed that although all three training modes were effective in lowering HbA1c, the COM approach was the most effective, supporting the previously established
dose–response relationship between PA volume and insu-lin sensitivity improvements [58].
In a more recent study, Larose et al. [59] correlated HbA1c with increases in CRF. The COM training programme elicited an increase in VO2peakand ventilatory threshold and, consequently, significantly decreased HbA1clevels. AE and RT also elicited positive effects on glucose control independently, although these effects were smaller than the COM training programme. However, as with the previous study, it is not possible to compare the respective effects of each programme inde-pendently because the COM group employed the full AE and RT programmes, which would have increased the overall volume performed. On the basis of the dose– response relationship between exercise volume and insu-lin sensitivity, it can come as little surprise that the effects were greater in conditions in which the overall volume of exercise was greater [20].
The Italian Diabetes and Exercise Study [60] demon-strated the effectiveness of a combined protocol compared with PA alone in 606 sedentary subjects with T2D and MetS. Subjects were randomized into one of the two groups, a control group who received counselling only or an exercise group who completed aerobic and RT in a structured environment twice weekly for 12 months. HbA1c levels were observed to be lower in the exercise group along with several other markers of cardiovascular health. Although the counselling-only group increased their PA to the recommended dosage offive times 30-min PA a week, there was no significant impact upon HbA1c or cardiovascular health profile. This suggests that greater levels of PA are required to improve the health status of individuals with MetS than is currently recommended [61] and that a supervised, structured combined exercise programme will be effective if administered properly.
Evidence grading
To derive the tables of exercise recommendations later, PA was classified (i.e. AE, RT and COM) and graded based upon the level of evidence provided and extent to which insulin sensitivity is improved. This grading is based upon the system implemented by the Ameri-can Diabetes Association and ACSM in their joint posi-tion stand [22] (Table 3 ). The grading is intended to highlight the extent to which different modes of exer-cise have been shown in the literature to improve
insulin sensitivity in multiple populations and through a wide range of interventions (Table 4).
Exercise recommendations
Based upon the exercise detailed in the earlier research and the effect of this exercise on insulin sensitivity, exer-cise recommendations have been formulated (Table 5). Interventions that have demonstrated particular effective-ness, that is, high intensity AE [35] and COM [60], have been incorporated, whereas interventions where particu-lar intensities have been compared the most effective have been recommended. The evidence presented for PA suggests a dose–response relationship between volume of activity and improvements in insulin sensitivity; therefore, the established minimum amounts (30 min of PA five times weekly) recommended by the ACSM [61] are proposed as a minimum. These evidence-based PA/ exercise recommendations should aid in the prescription and delivery of exercise as a measure to prevent and manage T2D.
Table 3. Evidence categories. Modified from American College of Sports Medicine and evidence grading for clinical practice rec-ommendations for the American Diabetes Association [22]
ACSM evidence categories
Evidence category Source of evidence Definition
A Randomized, controlled trials (overwhelming data) Provides a consistent pattern offindings with substantial studies
B Randomized, controlled trials (limited data) Few randomized trials exist, which are small in size.
C Nonrandomized trials, observational studies Outcomes are from uncontrolled, nonrandomized
and/or observational studies.
D Panel consensus judgement Panels expert opinion when the evidence is
insufficient to place it in categories A–C
ACSM, American College of Sports Medicine.
Table 4. Evidence grading for different exercise modalities based upon evidence examined
Current level of evidence–insulin sensitivity
Mode of exercise
Number of papers located in PubMed
search(1104)
Number of papers assessed(34)
Level of evidence
Aerobic exercise 845 16 A
Resistance training 237 10 B
Combined training 22 8 B
Table 5. Evidence-based exercise recommendations for maintaining/improving insulin sensitivity in different demographics
Insulin sensitivity: exercise recommendations
Healthy
(Insulin sensitivity maintenance)
Increase PA to more than 30 min per dayfive times a week [22,58]. Include high intensity aerobic exercise (>75%VO2) [35] three times a week combined with strength training in all major muscle groups [26] at 70% 1RM [48] twice a week separated by more than 24 h [34].
With type 2 diabetes
(Insulin sensitivity improvement)
Increase PA to more than 30 min per dayfive times a week [22,58]. Include long duration (>1 h) moderate intensity (60% VO2max) [33] aerobic training three times a week combined with low intensity and high repetition resistance training (50–60% 1RM) [50] in all major muscle groups [26] twice a week separated by more than 24 h [34].
Those with type 2 diabetes and limited mobility (Disabled, elderly populations, etc.)
Increase PA as much as is feasible [58]. Include low intensity aerobic exercise (40–80% HR reserve)/PA [54] combined with resistance training at low intensity 50–55% 1RM [50] in all major muscle groups [26] three times a
week separated by more than 24 h [34].
Conclusion
This review supports the proposal that PA is beneficial in improving metabolic control in general and in improving insulin sensitivity specifically.
Regular leisure time PA can maintain insulin sensitivity and improve glycaemic control in those with T2D. There may be a dose–response relationship between the inten-sity and duration of PA and improvements in insulin sen-sitivity, in which case the progression to higher levels of systematic PA (i.e. exercise) may elicit greater benefits.
Aerobic exercise appears effective in improving insulin sensitivity even though there is no present evidence to suggest that those benefits transcend those of lifestyle PA unless high intensities are implemented. Interval train-ing has been shown to be particularly effective at both moderate and high intensities, prescribed according to the participant’s ability to meet demands of the exercise.
Evidence suggests that RT is effective, most likely be-cause of an increase in muscle GLUT4 and in various
insulin signalling protein activity levels in the trained muscles. RT seems to be effective at intensities above 50% of 1RM, a fact that is reflected in the recommenda-tions for exercise training in subjects with T2D presented in this review.
It appears that combining AE and RT is the most effi -cient training strategy in improving insulin sensitivity, al-though further research controlling the volume of training is warranted.
This review confirms the effect of different modalities of exercise in improving insulin sensitivity. Having clearly considered the baseline condition of their patients, clini-cians should consider the possibility of prescribing COM training to obtain the optimal benefits in their patients.
Con
fl
ict of interest
None declared.
References
1. National Centre for Chronic Disease Pre-vention and Health Promotion. National Diabetes Fact Sheet. USA 2011. Atlanta, GA: U.S. Department of Health and Hu-man Services, Centers for Disease Con-trol and Prevention, 2011.
2. Hu FB. Globalization of diabetes: the role of diet, lifestyle, and genes.Diabetes Care2011;34: 1249–1257.
3. Centers for Disease Control and Prevention. National Diabetes Fact Sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2011.
4. Diabetes in the UK 2010: Key Statistics on Diabetes. Diabetes UK. 2011. 5. British National Formulary: National
Centre Physical Activity and Health Eco-nomics Factsheet, 2010.
6. Thompson WR, Gordon NF, Pescatello LS. ACSM’s guidelines for exercise test-ing and prescription: Hubsta Ltd; 2009. 7. Muniyappa R, Lee S, Chen H, Quon MJ. Current approaches for assessing insulin sensitivity and resistancein vivo: advan-tages, limitations, and appropriate us-age. Am J Physiol Endocrinol Metab
2008;294: E15–26.
8. Borai A, Livingstone C, Abdelaal F, Bawazeer A, Keti V, Ferns G. The relationship between glycosylated haemoglobin (HbA1c) and measures of insulin resistance across a range of glu-cose tolerance.Scand J Clin Lab Invest
2011;71: 168–172.
9. Patel A, MacMahon S, Chalmers J,et al. Intensive blood glucose control and vas-cular outcomes in patients with type 2 diabetes. N Engl J Med2008;12: 358 (24): 2560–72.
10. Yeckel CW, Weiss R, Dziura J,et al. Vali-dation of insulin sensitivity indices from oral glucose tolerance test parameters in obese children and adolescents. J Clin Endocrinol Metab2004;89: 1096–1101. 11. Inchiostro S. Measurement of insulin sensitivity in type 2 diabetes mellitus: comparison between KITT and HOMA-%S indices and evaluation of their relationship with the components of the insulin resistance syndrome.Diabet Med2005;22: 39–44.
12. Pedersen BK. The diseasome of physical inactivity–and the role of myokines in muscle–fat cross talk.J Physiol2009;
587: 5559–5568.
13. Executive summary: standards of medi-cal care in diabetes–2010.Diabetes Care
2010;33 Suppl 1: S4–10.
14. Healy GN, Matthews CE, Dunstan DW, Winkler EA, Owen N. Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 2003–06.Eur Heart J
2011;32(5): 590–7.
15. Burr JF, Rowan CP, Jamnik VK, Riddell MC. The role of physical activity in type 2 diabetes prevention: physiological and practical perspectives. Phys Sportsmed2010;38: 72–82.
16. Boulé NG, Haddad E, Kenny GP, Wells GA, Sigal RJ. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: a meta-analysis of
controlled clinical trials. JAMA 2001;
286: 1218–1227.
17. Bari MR, Ostgren CJ, Råstam L, Lindblad U. Abdominal obesity and insulin resis-tance in patients with type 2 diabetes in a Swedish community. Skaraborg hyper-tension and diabetes project. Scand J Prim Health Care2006;24: 211–217. 18. Chomistek AK, Chiuve SE, Jensen MK,
Cook NR, Rimm EB. Vigorous physical activity, mediating biomarkers, and risk of myocardial infarction.Med Sci Sports Exerc2011;43(10): 1884–90.
19. Larsson CA, Krøll L, Bennet L, Gullberg B, Råstam L, Lindblad U. Leisure time and occupational physical activity in re-lation to obesity and insulin resistance: a population-based study from the Skaraborg project in Sweden. Metabo-lism2012;61: 590–598.
20. Dwyer T, Ponsonby AL, Ukoumunne OC,et al. Association of change in daily step count overfive years with insulin sensitivity and adiposity: population based cohort study. BMJ 2011; 342: c7249.
21. Physical activity and health a report of the Surgeon General.US Department of Health and Human Services, Public Health Service, CDC, National Center for Chronic Disease Prevention and Health Promotion. Georgia: Atlanta, 1996. 22. Colberg SR, Sigal RJ, Fernhall B,et al.
Exercise and type 2 diabetes: the American College of Sports Medicine and the American Diabetes Association: joint position statement. Diabetes Care
23. Physical Activity Guidelines Advisory Committee report, 2008. To the secre-tary of health and human services. Part A: executive summary.Nutr Rev2009;
67: 114–120.
24. Nuri R, Kordi MR, Moghaddasi M,et al. Effect of combination exercise training on metabolic syndrome parameters in postmenopausal women with breast cancer. J Cancer Res Ther 2012; 8: 238–242.
25. Sirdah MM, Abu Ghali AS, Al Laham NA. The reliability of the National Cholesterol Education Program’s Adult Treatment Panel III (NCEP/ATP III) and the International Diabetes Federa-tion (IDF) definitions in diagnosing met-abolic syndrome (MetS) among Gaza Strip Palestinians.Diabetes Metab Syndr
2012;6: 4–8.
26. Holten MK, Zacho M, Gaster M, Juel C, Wojtaszewski JF, Dela F. Strength train-ing increases insulin-mediated glucose uptake, GLUT4 content, and insulin sig-naling in skeletal muscle in patients with type 2 diabetes. Diabetes 2004;
53: 294–305.
27. Cohen J. A power primer.Psychological bulletin1992;112(1): 155–159. 28. Lehmann R, Vokac A, Niedermann K,
Agosti K, Spinas GA. Loss of abdominal fat and improvement of the cardiovascu-lar risk profile by regular moderate exer-cise training in patients with NIDDM.
Diabetologia1995;38: 1313–1319. 29. Rönnemaa T, Mattila K, Lehtonen A,
Kallio V. A controlled randomized study on the effect of long-term physical exer-cise on the metabolic control in type 2 diabetic patients.Acta Med Scand1986;
220: 219–224.
30. Mourier A, Gautier JF, De Kerviler E,et al. Mobilization of visceral adipose tissue re-lated to the improvement in insulin sensi-tivity in response to physical training in NIDDM. Effects of branched-chain amino acid supplements. Diabetes Care 1997;
20: 385–391.
31. Raz I, Hauser E, Bursztyn M. Moderate ex-ercise improves glucose metabolism in uncontrolled elderly patients with non-insulin-dependent diabetes mellitus.Isr J Med Sci1994;30: 766–770.
32. Kohno K, Matsuoka H, Takenaka K,et al. Depressor effect by exercise training is as-sociated with amelioration of hyperinsulinemia and sympathetic over-activity.Intern Med2000;39: 1013–1019. 33. Magkos F, Tsekouras Y, Kavouras SA, Mittendorfer B, Sidossis LS. Improved insulin sensitivity after a single bout of exercise is curvilinearly related to exer-cise energy expenditure.Clin Sci (Lond)
2008;114: 59–64.
34. van Dijk JW, Tummers K, Stehouwer CD, Hartgens F, van Loon LJ. Exercise ther-apy in type 2 diabetes: is daily exercise required to optimize glycemic control?
Diabetes Care2012;35: 948–954. 35. Babraj JA, Vollaard NB, Keast C, Guppy
FM, Cottrell G, Timmons JA. Extremely short duration high intensity interval
training substantially improves insulin action in young healthy males. BMC Endocr Disord2009;9: 3.
36. Hood MS, Little JP, Tarnopolsky MA, Myslik F, Gibala MJ. Low-volume inter-val training improves muscle oxidative capacity in sedentary adults. Med Sci Sports Exerc2011;43(10): 1849–56. 37. Metcalfe RS, Babraj JA, Fawkner SG,
Vollaard NB. Towards the minimal amount of exercise for improving meta-bolic health: beneficial effects of reduced-exertion high-intensity interval training.Eur J Appl Physiol 2012; 112: 2767–2775.
38. Yfanti C, Nielsen AR, Akerström T,
et al. Effect of antioxidant supplemen-tation on insulin sensitivity in response to endurance exercise training.
Am J Physiol Endocrinol Metab 2011;
300: E761–770.
39. Vind BF, Pehmøller C, Treebak JT,et al. Impaired insulin-induced site-specific phosphorylation of TBC1 domain family, member 4 (TBC1D4) in skeletal muscle of type 2 diabetes patients is restored by endurance exercise-training.
Diabetologia2011;54: 157–167. 40. Mujumdar PP, Duerksen-Hughes PJ,
Firek AF, Hessinger DA. Long-term, pro-gressive, aerobic training increases adiponectin in middle-aged, overweight, untrained males and females. Scand J Clin Lab Invest2011;71: 101–107. 41. Bacchi E, Negri C, Zanolin ME, et al.
Metabolic effects of aerobic training and resistance training in type 2 diabetic subjects a randomized controlled trial (the RAED2 study).Diabetes Care2012;
35: 676–682.
42. Totsikas C, Röhm J, Kantartzis K,et al. Cardiorespiratory fitness determines the reduction in blood pressure and insulin resistance during lifestyle intervention. J Hypertens 2011; 29: 1220–1227.
43. Jorge ML, de Oliveira VN, Resende NM,
et al. The effects of aerobic, resistance, and combined exercise on metabolic control, inflammatory markers, adi-pocytokines, and muscle insulin signal-ing in patients with type 2 diabetes mellitus. Metabolism 2011; 60(9): 1244–52.
44. Honkola A, Forsén T, Eriksson J. Resis-tance training improves the metabolic profile in individuals with type 2 diabe-tes.Acta Diabetol1997;34: 245–248. 45. Dunstan DW, Puddey IB, Beilin LJ,
Burke V, Morton AR, Stanton KG. Effects of a short-term circuit weight training program on glycaemic control in NIDDM. Diabetes Res Clin Pract 1998;
40: 53–61.
46. Dunstan DW, Daly RM, Owen N,et al. High-intensity resistance training im-proves glycemic control in older patients with type 2 diabetes. Diabetes Care
2002;25: 1729–1736.
47. Castaneda C, Layne JE, Munoz-Orians L,
et al. A randomized controlled trial of resistance exercise training to improve
glycemic control in older adults with type 2 diabetes. Diabetes Care 2002;
25: 2335–2341.
48. Cauza E, Hanusch-Enserer U, Strasser B,
et al. The relative benefits of endur-ance and strength training on the metabolic factors and muscle function of people with type 2 diabetes mellitus.
Arch Phys Med Rehabil 2005; 86: 1527–1533.
49. Hansen E, Landstad BJ, Gundersen KT, Torjesen PA, Svebak S. Insulin sensitivity after maximal and endurance resistance training.J Strength Cond Res2012;26: 327–334.
50. Kwon HR, Han KA, Ku YH,et al. The ef-fects of resistance training on muscle and body fat mass and muscle strength in type 2 diabetic women.Korean Diabe-tes J2010;34: 101–110.
51. Brooks N, Layne JE, Gordon PL, Roubenoff R, Nelson ME, Castaneda-Sceppa C. Strength training improves muscle quality and insulin sensitivity in Hispanic older adults with type 2 diabetes. Int J Med Sci 2007;
4: 19–27.
52. Layne AS, Nasrallah S, South MA,et al. Impaired muscle AMPK activation in the metabolic syndrome may attenuate improved insulin action after exercise training.J Clin Endocrinol Metab2011;
96(6): 1815–26.
53. Tessier D, Ménard J, Fülöp T, et al. Effects of aerobic physical exercise in the elderly with type 2 diabetes mellitus. Arch Gerontol Geriatr 2000;
31: 121–132.
54. Balducci S, Leonetti F, Di Mario U, Fallucca F. Is a long-term aerobic plus resistance training program feasible for and effective on metabolic profiles in type 2 diabetic patients?Diabetes Care
2004;27: 841–842.
55. Tokmakidis SP, Zois CE, Volaklis KA, Kotsa K, Touvra AM. The effects of a combined strength and aerobic exer-cise program on glucose control and insulin action in women with type 2 diabetes. Eur J Appl Physiol 2004;
92: 437–442.
56. Schrauwen-Hinderling VB, Hesselink MK, Meex R,et al. Improved ejection frac-tion after exercise training in obesity is accompanied by reduced cardiac lipid content.J Clin Endocrinol Metab2010;
95: 1932–1938.
57. Sigal RJ, Kenny GP, Boulé NG, et al. Effects of aerobic training, resistance training, or both on glycemic control in type 2 diabetes: a randomized trial. Ann Intern Med 2007; 147: 357–369.
58. Koo BK, Han KA, Ahn HJ, Jung JY, Kim HC, Min KW. The effects of total energy expenditure from all levels of physical activity vs. physical activity energy expenditure from moderate-to-vigorous activity on visceral fat and insulin sensitivity in obese type 2 diabetic women. Diabet Med 2010;
59. Larose J, Sigal RJ, Khandwala F, et al. Associations between physical fitness and HbA (c) in type 2 diabetes mellitus.
Diabetologia2011;54: 93–102. 60. Balducci S, Zanuso S, Nicolucci A,et al.
Effect of an intensive exercise interven-tion strategy on modifiable cardiovascular
risk factors in subjects with type 2 diabe-tes mellitus: a randomized controlled trial: the Italian Diabetes and Exercise Study (IDES). Arch Intern Med 2010;
170: 1794–1803.
61. Garber CE, Blissmer B, Deschenes MR,
et al. American College of Sports

![Table 3. Evidence categories. Modified from American College of Sports Medicine and evidence grading for clinical practice rec-ommendations for the American Diabetes Association [22]](https://thumb-us.123doks.com/thumbv2/123dok_us/8019726.1333764/9.594.62.542.565.708/evidence-categories-modied-american-medicine-ommendations-diabetes-association.webp)
