Our reference: JBUR 5807
P-authorquery-v9
AUTHOR QUERY FORM
Journal:
JBUR
Please e-mail your responses and any corrections to:
Article Number:
5807
E-mail:
Dear Author,
Please check your proof carefully and mark all corrections at the appropriate place in the proof (e.g., by using on-screen
annotation in the PDF file) or compile them in a separate list. Note: if you opt to annotate the file with software other than
Adobe Reader then please also highlight the appropriate place in the PDF file. To ensure fast publication of your paper please
return your corrections within 48 hours.
For correction or revision of any artwork, please consult
http://www.elsevier.com/artworkinstructions
.
Any queries or remarks that have arisen during the processing of your manuscript are listed below and highlighted by flags in
the proof. Click on the ‘
Q
’ link to go to the location in the proof.
Location in
Query / Remark:
click on the Q link to go
article
Please insert your reply or correction at the corresponding line in the proof
Q1
Please check the presentation of all the tables, and correct if necessary.
Q2
Please provide the significance of bold values in Table 3.
Q3
Your article is registered as a regular item and is being processed for inclusion in a regular issue of
the journal. If this is NOT correct and your article belongs to a Special Issue/Collection please contact
[email protected] immediately prior to returning your corrections.
Q4
Please confirm that the provided email is the correct address for official communication, else provide
an alternate e-mail address to replace the existing one, because private e-mail addresses should not be
used in articles as the address for communication.
Q5
The author names have been tagged as given names and surnames (surnames are highlighted in teal
color). Please confirm if they have been identified correctly.
Q6
Highlights must be provided as 3-5 bullet points, each bullet point having a maximum of 125 characters.
Please rephrase the following highlights or provide new highlights.
Q7
Please check the hierarchy of section headings, and correct if necessary.
Q8
Please provide the volume, issue or page range for Ref. [11].
Please check this box or indicate your approval if
you have no corrections to make to the PDF file
1
Highlights
Burnsxxx(2019)xxx–xxx
Patterns
and
predictors
of
burn
scar
outcome
in
the
first
12
months
post-burn:
The
patient
’
s
perspective
Z.M.Rashaan*,K.A.A. Kwa,M.B.A.vanderWal,W.E.Tuinebreijer,P.P.M.vanZuijlen, R.S.Breederveld
ThePOSASpatienttotalandindividualitemscoresshowedastatisticallysignificantimprovementofthescarqualityinthefirst
12monthspost-burn,exceptforrelief.
Q6
Sex,age,depthofthewound,percentageofTBSAandflameburnswerepredictorsofvariousPOSASpatientitemsat3,6and
12monthspost-burn.
TheeffectofthepredictorswasnotthesameontheindividualPOSASpatientitems.
burns xxx (2019) xxx–xxx
Available
online
at
www.sciencedirect.com
ScienceDirect
1Q3
Patterns
and
predictors
of
burn
scar
outcome
in
the
2
first
12
months
post-burn:
The
patient
’
s
perspective
3Q4Q5
Z.M.
Rashaan
a,b,*
,
K.A.A.
Kwa
a,b,
M.B.A.
van
der
Wal
e,
4
W.E.
Tuinebreijer
b,
P.P.M.
van
Zuijlen
c,d,
R.S.
Breederveld
a,b5 aDepartmentofSurgery,LeidenUniversityMedicalCentre,Albinusdreef2,2333ZALeiden,Leiden,TheNetherlands
6 b
BurnCentreandDepartmentofSurgery,RedCrossHospital,Vondellaan13,1942LE,Beverwijk,TheNetherlands 7 cBurnCentreandDepartmentofPlasticandReconstructiveSurgery,RedCrossHospital,Vondellaan13,1942LE,
8 Beverwijk,TheNetherlands
9 dDepartmentofPlasticandReconstructiveSurgeryandMOVEResearchInstitute,VUUniversityofAmsterdam,Van
10 derBoechorststraat7,1081BT,Amsterdam,TheNetherlands
11 e
AssociationofDutchBurnCentres,Zeestraat27-29,1941AJ,Beverwijk,TheNetherlands
a
b
s
t
r
a
c
t
Objective:Thisstudyaimedtoprovideinsightintothepatternsandfactorsthatpredictburn scaroutcomesat3,6and12monthspost-burn.
Methods:ThePatientandObserverScarAssessmentScale(POSAS)wasusedtoassessthescar formationofeachpatient.Structuralequationmodellingwasused.Thepredictorvariablesused inthisstudyweresex,threeagecategories,TBSA,depthofthewoundandcauseoftheburn.
Results:ThePOSASpatienttotalandindividualitemscoresdemonstrateda statistically significantdecreaseinthefirst12monthspost-burn,exceptforthereliefitem.Malepatients hadalowertotalanditemsscores(betterscarquality)forpainandprurituscomparedwith femalepatients.Fullthicknessburnshadahigherscoresforpruritus,pliability,thickness andreliefcomparedtothepartial-thicknessburns.Agesyoungerthan5years,higherTBSA valuesandflameburnswerepredictorsofvariousPOSASitemsat3and6monthspost-burn.
Conclusion:ThePOSASpatienttotalandindividualitemscoresdemonstratedastatistically significantimprovementinthescarqualityinthefirst12monthspost-burn,exceptforthe relief.Sex,age,depthofthewound,thepercentageofTBSAandflameburnswerepredictors ofvariousPOSASpatientitemsat3,6and12monthspost-burn.
©2019ElsevierLtdandISBI.Allrightsreserved.
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Accepted26March2019 Availableonlinexxx
12 Keywords: 13 Burnwounds
14 Burnscars
15 POSAS
16 Scarquality
17 Predictorsandpatterns
18
1.
Introduction
19 Burnscarshaveextensiveimpactsonburnpatientsintermsof 20 quality of life, functional impairment and physiological
21
problems[1–3].Thus,theoptimalmanagementofburnscars
22
requires more insight into the factors that influence the
23
severityofburnscars.
24
Todate,sex,age,skintype,location,bacterialcolonisation,
25
time to wound healing, type of graft, multiple surgical
Abbreviations:CFI,comparativefitindex;POSAS,thePatientandObserverScarAssessmentScale;SEM,structuralequationmodelling; LGM,latentgrowthcurvemodel;RMSEA,therootmeansquareerrorofapproximation.
* Correspondingauthor.
E-mailaddresses:[email protected](Z.M. Rashaan),[email protected](K.A.A. Kwa),[email protected](M.B.A. vanderWal),
[email protected](W.E. Tuinebreijer),[email protected](P.P.M. vanZuijlen),[email protected](R.S. Breederveld).
https://doi.org/10.1016/j.burns.2019.03.025
0305-4179/©2019ElsevierLtdandISBI.Allrightsreserved.
burns xxx (2019) xxx–xxx JBUR58071–8
Pleasecitethisarticleinpressas:Z.M.Rashaan,K.A.A.Kwa,M.B.A.vanderWaletal.Patternsandpredictorsofburnscaroutcomein thefirst12monthspost-burn:Thepatient’sperspective.Burns(2019),https://doi.org/10.1016/j.burns.2019.03.025
Available
online
at
www.sciencedirect.com
ScienceDirect
26 procedures, burn severity and the skin being subjected to 27 stretchinghavebeenfoundtoberiskfactorsforhypertrophic 28 scarring[4–8].Theimpactsofburnscarsnotonlyentailthe 29 appearanceofthescarbutalsoinvolveofitsaccompanying 30 symptoms. Up to 47% of patients experience pain that is 31 associatedwiththeirburnscars[9].Inaddition,prurituswas 32 foundtostillbepresentin67%oftheburnpatientsattwoyears 33 post-burn [10]. It should be noted that different burnscar 34 assessmentstrategieswereusedinthesestudies,andthese 35 studieswereoftenlimitedbythelackofanappropriatetoolfor 36 evaluatingscaroutcomes.
37 Currently,thePatientandObserverScarAssessmentScale 38 (POSAS)iswidelyusedtoassessscarquality[11].ThePOSAS 39 consistsofobserverandpatientcomponentsandhasbeen 40 foundtobeareliableandvalidinstrumentfortheassessment 41 ofburnscars[12,13].ThePOSASpatientscalebyDraaijersetal. 42 (version1.0)incorporatesscoresforthefollowingsixitemsby 43 using a 10-point rating scale: pain, itch, color, pliability, 44 thicknessandrelief[12,14].Ahighscoreindicatesaworsescar 45 quality. There is a paucity of research investigating the 46 changesinthePOSAS scoresafterburns[15].Van derWal 47 et al. described that full thickness wounds and a higher 48 percentageofTBSA were significantpredictorsofahigher 49 POSASscore,whereastheaetiologyandageofthepatienthad 50 no influence on the scar quality [16]. In addition, POSAS 51 assessmentathreemonthspost-burnfoundtobepredictiveof 52 finalscarqualityattwelvemonthspost-burn[17].
53 The purpose of the present study was to describe the 54 influenceofpredictorsonchangesinPOSASpatientscoresat 55 3,6and12monthspost-burn.
56
2.
Materials
and
m
ethods
57 2.1. Recruitmentandstudypopulation
58 Thisretrospectivestudywas performedattheburncentre 59 outpatientclinicattheRedCrossHospital,Beverwijkinthe 60 Netherlands between June 2004 and December 2009. This 61 studywasconductedinaccordancewiththeethicalstandards 62 oftheinstitutionaland/ornationalresearchcommitteeand 63 withthe1964Helsinkideclarationanditslateramendmentsor 64 comparableethicalstandards.ThePOSASquestionnaireisa 65 standardpartofeachroutinefollow-upvisitofeachoftheburn 66 patientsintheoutpatientclinicat3,6and12monthsatour 67 specializedburncentre.Thedataofthe patientswho were 68 admittedtotheburncentreandwhoweresubsequentlyseen 69 attheoutpatientclinicat3,6and12monthspost-burnwere 70 included in the analysis. In this consecutive sample, the 71 patientswhoparticipatedinclinicaltrialsforwoundorscar 72 treatments were excluded from the study. The parentsor 73 caregiverswereaskedtofillinthePOSASpatientcomponent 74 for patients who were under the age of5 years. Baseline 75 characteristics such as sex, age at the time of burn, the 76 percentage of total body surface area (TBSA), burn depth 77 (partialorfullthickness)andthe causeoftheburnwound 78 (flameorscald)werecollected.Atourinstitution,patientswith 79 full-thickness burns were operated (skin grafting). Mixed 80 burns(partialandfull-thickness)wereconservativelytreated 81 forapproximately10–14 days.Burn woundsof>3cm2that
82
were not yet healed, were considered for skin grafting
83
procedures.Partial-thicknessburnsweretreatedwithtopical
84
antisepticsorhydrofibredressings.Thistreatmentalgorithm
85
waschosenbecausewoundhealingthattakesmorethanthree
86
weeks to complete, is considered to be a risk factor for
87
hypertrophic scarformation[18].Patients werecategorized
88
intothefollowingthreeage-groups:<5years,5–18yearsand
89
>18years.Thecut-offvalueof5yearswaschosenbecauseof
90
tworeasons.First,theepidemiologyofburnwoundstendsto
91
bedifferentbetweenchildren<5yearsandolderchildren.In
92
general,scaldburnsweremorecommoninchildrenwhowere
93
youngerthan 5yearscomparedwitholderchildren[19,20].
94
Second,thePOSASpatientscoresofthisagecategorywere
95
completed by the caregivers, which may influence the
96
outcomescomparedwitholderchildrenwhocompletedthe
97
POSASpatientscoresontheirown.Thestudylocationatthree
98
monthspost-burnwasdefinedasthemostapparentpartof
99
the scar according to the patient. Standard treatment
100
consisted ofsilicones or pressure garments depending on
101
the location and scar activity. If there was a significant
102
functional impairment during ADL, then there was an
103
indicationofreconstructionsurgeryduringthefirst12months
104
post-burn. After 12 months post-burn, an operation was
105
indicated for both functional impairment and esthetical
106
reasons.
107
2.2. ThePOSAS
108
Tothebestofourknowledge,thereisconflictingdatainthe
109
literatureconcerningtheanalysisofthePOSASpatientscores.
110
VanderWaletal.foundthatthePOSASpatientquestionnaire
111
wasunidimensional.Therefore,theindividualandsumofthe
112
itemsofthePOSASpatientscorescouldbeusedforstatistical
113
analysis[21].Conversely,deJongetal.foundthatthePOSAS
114
patientquestionnairewasmultidimensional.Therefore,the
115
only individual POSAS patients scores could be used for
116
statistical analysis [13]. In this study, we used both the
117
individualandsumofthePOSASpatientscoresforstatistical
118
analysis. Ifthepatientwasunabletoanswerthe
question-119
naire,e.g.inthecaseofchildren<5yearsorinthecaseof
120
mentallyimpairedpatients,thenthecaretakerwasaskedto
121
scoretheitems.
122
2.3. Studymodelandstatisticalanalyses
123
Structuralequationmodelling(SEM)wasperformedusingthe
124
IBMSPSS statisticalpackage AMOSTL24 [22].We applieda
125
latent growth curve model (LGM), which was a special
126
applicationoftheSEMwithseveraladvantages.Latentgrowth
127
curvemodellinginAMOSwasabletoaccommodateirregularly
128
spaced measurements at the three time points (3, 6 and
129
12monthspost-burn)inourdata[23].Inaddition,theuseof
130
LGMmadeitpossibletoassessthefitofthemodeltothedata
131
andtoeffectivelycomputethemaximumlikelihoodestimates
132
inourdataset,whichwasnotcompletedatallthreeofthetime
133
points(AppendixB).TheInter-individualdifferencesinthe
134
changesovertimewereassessed,andgroup-levelstatistics
135
such asthe mean change rates and mean interceptswere
136
provided. TheLGM accountsfortheofchange(slopecurve
137
analysis)attheindividuallevel(patient)andatthegrouplevel
138 (forinstance,thedepthoftheburnwound,sex,etc.).Thefitof 139 theLGMwastested.Theabsoluteandcomparativefitindices 140 werecalculated.
141 The following predictor variables were entered into the 142 models:sex,age<5years,age5–18yearsandage>18years,the 143 percentageofTBSA,depthofthewoundandcauseoftheburn. 144 OurmodelwasbasedonourearlierstudythatusedthePOSAS 145 patientscaletostudytheinfluenceoftime-invariantpredictors 146 (suchassex,thepercentageofTBSA,wounddepthandage 147 categories)onthePOSASscaleinthesamegroupofpatients 148 [16].Thethreedifferentinterceptestimatesrepresentedthe 149 patients’totalscoresat3,6or12months.Thetimemomentof 150 theintercept wasdependenton how thetime values were coded 151 (0,1,3; 1,0,2or 3, 2,0).Theslopeestimatesrepresentedthe 152 patients’ratesofchangebetween3,6and12monthspost-burn. 153 PositiveinterceptsindicatedhigherPOSASscoresat3,6and 154 12monthspost-burn,whichthusindicatedaworsescarquality 155 comparedtothatofthereferencegroup.Significantnegative 156 slopesinthePOSASscoresindicatedaslowerrateofchangein 157 the presented predictor category compared to that in the 158 referencecategory(forexample,flameburnscomparedtothe 159 referencecategoryscaldburns).
160 Thecorrelationsbetweentheinterceptsandslopeswere 161 calculated.Apositivevalueindicatedahighinitialscoreat 162 3monthspost-burnwithagreaterrateofchange,whereasa 163 negativecorrelationindicatedahighinitialscoreat3months 164 post-burnwithalowerrateofchange.
165 TheLGMwasinvestigatedinamodelforthetotalscoreand 166 wasindividuallyinvestigatedinamodelforthesixitemsthat 167 wereincorporatedin thePOSASpatientscale,bothwithand 168 withoutpredictors.Theinterceptestimatecanbeinterpretedas 169 theinfluenceofthepredictorsonthePOSASpatientscoresat3, 170 6and 12 months post-burn. The positiveintercepts implied 171 higherPOSASscorescomparedtothereferencecategory.The 172 slope estimate can be interpreted as the influence of the 173 predictorsonthechangesinthePOSASscoresovertime.Positive 174 slopesindicatehigherdegreeofchangeovertimecomparedto 175 thereference category. An detaileddescription of the study 176 modelandstatisticalanalysescanbefoundinAppendixD.
177
3.
Results
178 3.1. Baselinecharacteristics
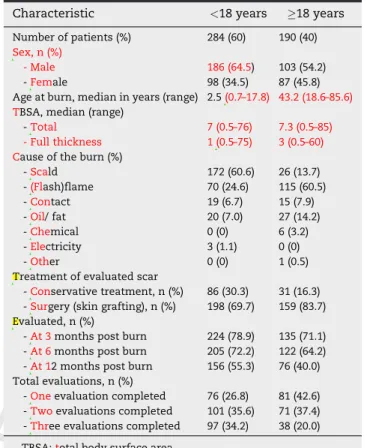
179 Atotalof284childrenand190adultpatientswereincludedinthis 180 study.Thepatients’characteristicsareshowninTable1.There 181 wereno statisticallysignificantdifferences in the totalTBSA 182 (p=0.99,independentt-test),full-thicknessburns(p=0.30, inde-183 pendentt-test),orsurgeriesontheevaluatedscars(p=0.53, chi-184 squaretest)thatwereobservedbetweenthegroupsofpatients 185 whocompletedallthreeevaluations(n=157)andthepatients 186 whocompletedoneortwooftheevaluationsmoments(n=317).
187 3.2. Thefitindicesforthedifferentmodels
188 The fit indices for the different models are presented in 189 AppendixB.Thefitindicesforthemodelwiththetotalscore 190 and the sixpredictors (Appendix A)revealed the following 191 results: The minimum discrepancy (CMIN) was 6.751 with
192
7degrees of freedom (df)and ap-valueof 0.455. Thecomparative
193
fit index (CFI) was 1.00. The root mean square error of
194
approximation(RMSEA)was0.0001withaconfidenceinterval
195
of0.0001–0.055.Thesevaluesofthefitindicesagreewitha
good-196
to-perfect fitwiththetotal scoreandthe sixpredictors.Allofthe
197
modelsthatevaluatedthesixindividualitemshadaperfectfit.
198
Themodelwiththetotalscorewithoutthesixpredictorshada
199
moderatefit,andthemodelswiththeitemsofthicknessor
200
reliefandwithoutthesixpredictorshadapoorfit.
201
3.3. PatternsofchangeinthePOSASpatientscores
202
Theparameterestimatesfortheinterceptandslopesofthe
203
modelthatevaluatedtheseparatetotalPOSASpatientscale
204
scoresandtheseparate6itemswithoutthe6predictorsare
205
showninTable2.TheparameterestimatesforthetotalPOSAS
206
scoresobtainedfromthepredictormodelsarepresentedin
207
Table2andAppendixA.Painhadthelowestseparateintercept
208
score,whichimpliedthatpainhadthelowestitemscoreoutof
209
thesixitemsinthePOSASat3monthspost-burn.Thetotal
210
score and all of the items (except relief) had significant
211
negativeslopes,whichimpliedthattheratesofchangeinthe
212
scoresshowedadecreasingtrend.Thecovariancesbetween
213
thepredictorvariablesofthetotalPOSASpatientscalescors
214
areshowninAppendixC.
215
3.4. Sex
216
MalepatientshadlowertotalPOSASpatientscoresat3,6and
217
12monthspost-burn,withnosignificantdifferenceintherate
Table1–Patientcharacteristics. Q1
Characteristic <18years 18years
Numberofpatients(%) 284(60) 190(40) Sex,n(%)
-Male 186(64.5) 103(54.2)
-Female 98(34.5) 87(45.8)
Ageatburn,medianinyears(range) 2.5(0.7–17.8) 43.2(18.6–85.6) TBSA,median(range)
-Total 7(0.5–76) 7.3(0.5–85) -Fullthickness 1(0.5–75) 3(0.5–60) Causeoftheburn(%)
-Scald 172(60.6) 26(13.7)
-(Flash)flame 70(24.6) 115(60.5)
-Contact 19(6.7) 15(7.9)
-Oil/ fat 20(7.0) 27(14.2)
-Chemical 0(0) 6(3.2)
-Electricity 3(1.1) 0(0)
-Other 0(0) 1(0.5)
Treatmentofevaluatedscar
-Conservativetreatment,n(%) 86(30.3) 31(16.3) -Surgery(skingrafting),n(%) 198(69.7) 159(83.7) Evaluated,n(%)
-At3monthspostburn 224(78.9) 135(71.1) -At6monthspostburn 205(72.2) 122(64.2) -At12monthspostburn 156(55.3) 76(40.0) Totalevaluations,n(%)
-Oneevaluationcompleted 76(26.8) 81(42.6) -Twoevaluationscompleted 101(35.6) 71(37.4) -Threeevaluationscompleted 97(34.2) 38(20.0)
TBSA:totalbodysurfacearea.
burns xxx (2019) xxx–xxx
3
JBUR58071–8
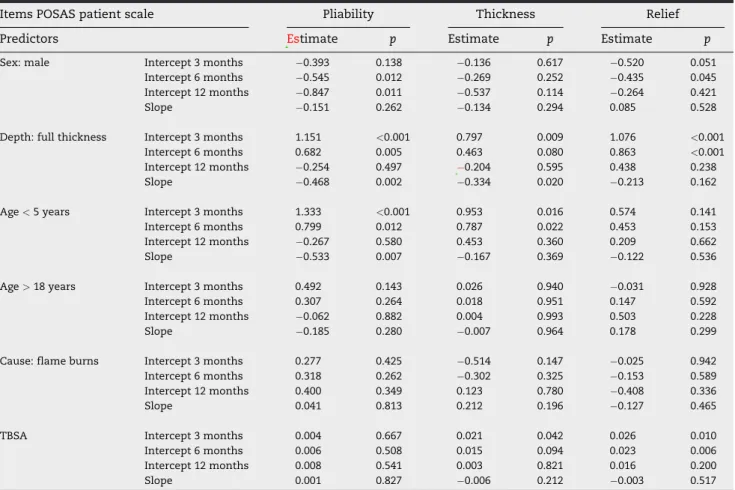
218 ofchange whencomparedtofemale patients.(Table3)The 219 malepatientshadlowerpainscoresat3and6months post-220 burn,withanequalrateofchangecomparedtofemales.Men 221 tendedtohaveloweritchscoresat3and6monthspost-burn. 222 Nevertheless, the changes in the scores over time were 223 comparable.(Table4A)MalepatientshadhigherPOSASscores 224 forreliefat3and6monthspost-burn,withlowerpliability 225 scoresat6and12monthspost-burn.However,thechangesin 226 the scores were comparable to those observed in female 227 patients(Table4B).
228 3.5. Wounddepth
229 PatientswithfullthicknessburnshadhigherPOSASpatient 230 totalscoresat3monthspost-burnandalowerrateofchange 231 duringthefirst12monthspost-burncomparedtopatientswith 232 partial thickness burns. The total POSAS scores for full 233 thicknessand partialthicknessburnsshowednodifference 234 at12monthspost-burn(Table3).Pruritusscoresat3months 235 weresignificantlyhigherinpatientswithfullthicknessburns 236 thanthoseinpatientswithpartialthicknessburns.Therateof 237 changeinthepruritusscoreswassignificantlylowerinpatients 238 withfullthicknessburns(Table4A).Finally,patientswithfull 239 thickness burns had significantly higher POSAS scores for 240 pliability,thicknessand reliefat3and 6monthspost-burn 241 comparedwithpatientswithpartialthicknessburns(Table4B).
242 3.6. Age
243 TherewasnosignificantdifferenceinthetotalPOSASscores 244 betweenyoungerpatients orpatients who wereolderthan
245
5years.However,patientswhowereyoungerthan5yearshad
246
significantlylowerpruritusscoresat12monthspost-burnand
247
lowerratesofchangecomparedtoolderpatients.(Table4A)
248
Patientsagedbelow5yearshadhigherscarcolor,pliabilityand
249
thicknessscoresat3and6monthspost-burn,whilepatients
250
olderthan18yearshadahigherscarcolorscoresat12months
251
post-burn anda greaterchangeinscoresthanthe younger
252
patients(Table4B).Patientsolderthan18yearshadhigherpain
253
scoresat3,6and12monthspost-burnthanyoungerpatients,
254
butgroupsofpatientshadequalratesofchange.(Table4A)
255
3.7. AetiologyandpercentageofTBSA
256
The covariancesbetweenthe predictor variablesof thetotal Q7
257
POSASpatientscoreareshowninAppendixAandAppendixC.
258
NoeffectsofthepercentageofTBSAorcauseofburnwerefound
259
onthetotalPOSASpatientscale.(Table3)Patientswithflame
260
burnsgenerallyhadsignificantlyhighercolorscoresat3and
261
6monthspost-burn.(Table4A)Patientswithahigherpercentage
262
ofTBSAhadhigherPOSASscoreforreliefat3and6months
post-263
burn.(Table 4B) Pruritus scores at 6 and 12 months post-burn were
264
higherinpatientswithahigherpercentageofTBSAvalues.
265
4.
Discussion
266
Thechange inthe POSASpatient scalescores wasstudied
267
between 3 and 6 months post-burn and between 6 and
268
12monthspost-burn.ThePOSASpatienttotalscoreandallof
269
the itemscoresshowedastatisticallysignificantdeclinein
270
thesetwotimeperiods,exceptforthereliefitem.Thegreatest
Table2–Estimatesoftheintercepts,slopesandcovariancesbetweeninterceptsandslopesofthetotalscoresanditemspain,
pruritus,color,pliability,thicknessandreliefwithoutpredictors.
POSASpatientscale Intercept Slope Covariances
Estimate SE CR P Estimate SE CR p Estimate SE CR p
Totalscore 3months 29.18 0.55 53.25 <0.001 2.02 0.25 8.25 <0.001 2.86 4.56 0.63 0.531
6months 27.16 0.47 57.75 <0.001 1.13 2.94 0.38 0.701
12months 23.12 0.65 35.60 <0.001 2.34 8.83 0.26 0.791
Items:
Pain 3months 2.38 0.10 22.45 <0.001 0.17 0.04 4.26 <0.001 0.07 0.14 0.47 0.637
6months 2.21 0.09 25.01 <0.001 0.01 0.09 0.07 0.942
12months 1.87 0.11 16.75 <0.001 0.15 0.27 0.55 0.581
Pruritus 3months 4.54 0.13 33.81 <0.001 0.49 0.06 8.09 <0.001 0.67 0.26 2.55 0.011
6months 4.05 0.11 36.05 <0.001 0.10 0.18 0.54 0.592
12months 3.07 0.15 19.92 <0.001 1.05 0.51 2.06 0.039
Color 3months 6.94 0.11 64.43 <0.001 0.54 0.06 9.56 <0.001 0.52 0.21 2.52 0.012
6months 6.40 0.09 74.02 <0.001 0.17 0.14 1.27 0.204
12months 5.32 0.14 39.26 <0.001 0.52 0.39 1.32 0.187
Pliability 3months 5.79 0.13 44.66 <0.001 0.47 0.07 7.07 <0.001 0.40 0.30 1.37 0.172
6months 5.33 0.11 50.73 <0.001 0.10 0.19 0.52 0.600
12months 4.40 0.16 27.59 <0.001 0.50 0.58 0.87 0.383
Thickness 3months 5.26 0.13 39.84 <0.001 0.31 0.06 5.06 <0.001 0.08 0.28 0.29 0.770
6months 4.96 0.11 43.61 <0.001 0.10 0.18 0.52 0.601
12months 4.34 0.16 26.80 <0.001 0.12 0.57 0.21 0.832
Relief 3months 5.08 0.13 39.10 <0.001 0.09 0.06 1.34 0.179 0.35 0.29 1.19 0.236
6months 5.00 0.11 47.33 <0.001 0.07 0.19 0.37 0.715
12months 4.82 0.16 30.83 <0.001 0.48 0.57 0.85 0.397
SE,standarderror;CR,criticalratio.
271 declinewasobservedduringthelongertimeperiodbetween 272 6and12monthspost-burn.Thepainitemscalepresentedthe 273 lowestdeclinescore,andthecoloritemexhibitedthehighest 274 declinescore. Therefore,the painand color itemshad the 275 lowest and highest influences on the total POSAS score, 276 respectively. The low pain scores could be the result of 277 effectivemedicationforpainand/ortheresultofreallowpain 278 valuesinpatientsafter3monthspost-burn.Thehighcolor 279 values represent the importance of color for the patient 280 assessmentofhisorherscars.Patientswiththehighesttotal 281 anditemscorespresentedthelowestchangesduringthe3and 282 6monthspost-burn,thusleadingtothelowestdeclineinthe 283 totalscore.
284 Inourstudy,astrongeffectofsexwasobservedonthetotal 285 POSASpatientscore.Malepatientshadabetterscarquality, 286 whichwascausedbylowerscoreofpruritusandpain,aswell 287 asabetterscoreforpliabilityandreliefcomparedtothescar 288 qualityinfemalepatients.Variousstudieshavedemonstrated 289 higherpain-relatedsymptomsinwomencomparedwithmen 290 [26–28].Sexrolebeliefs,paincopingstrategies,pain-related 291 expectationsandevenhormonalfactorsmaypossiblyexplain 292 thedifferenceinpainexperiencebetweenmalesandfemales 293 [29].Inlinewithourstudy,twostudiesobservedhigheritch 294 intensityscoresinwomencomparedtomen,althoughthis 295 phenomenonisnotwellunderstood[10,30].Higherpliability
296
and relief scores in the female group in our study could
297
possibly be explained by the differences in body images
298
betweenmalesandfemales.Ingeneral,womenhaveamore
299
negative body imagecompared to men[31–33].Dyer et al.
300
observedthatwomenwithscarsthatresultedfromaccidents
301
orsurgeriesreportedamorenegativebodyimage[33].
302
PatientswithfullthicknessburnshadhighertotalPOSAS
303
scores,whichwerecausedbyhigherscoresforthepruritus,
304
pliability,thicknessandreliefitems.Otherstudieshavealso
305
described higheritchingscoresforfullthicknessburnsand
306
graftedwounds[10,30,34].Anincreaseinbothmediatorsand
307
neuronal damage are thought to contribute to pruritus
308
symptomsinfullthicknessburns[35].Inourstudy,pruritus
309
diminishedafter3monthspost-burn;afindingthathasbeen
310
previously describedinother studies[10,16]. HigherPOSAS
311
scoresforpliability,thicknessandreliefareexplainedbythe
312
lossofepidermalanddermalstructures.
313
Previousstudieshavefoundthattheageofthepatientdoes
314
notinfluencescarbehavior[6,16,36].Ourresultsareconsistent
315
withthesereportswhenconsideringthetotalPOSASscore.
316
However, thisisnotthecasewhenlookingattheseparate
317
items.Patientswhowereagedbelow5yearshadsignificantly
318
higher scores for color, pliability and thickness at 3 and
319
6monthspost-burn,andthesepatientsalsohadsignificantly
320
lesspruritusat12monthspost-burn.Thefactthatcaretakers
Table3–Regressionweightsandp-valuesofthePOSASpatientscoresandthepredictorsTBSA,burndepth,agecategory, Q2
sexandcauseofburn.
POSASpatientscaletotalscore Estimate SE CR p
Predictors
Sex:male Interceptat3months 3.327 1.138 2.922 0.003
Interceptat6months 3.204 0.973 3.292 <0.001
Interceptat12months 2.959 1.332 2.222 0.026
Slope 0.122 0.504 0.243 0.808
Depth:fullthickness Interceptat3months 3.543 1.283 2.762 0.006
Interceptat6months 1.997 1.097 1.820 0.069
Interceptat12months 1.095 1.501 0.730 0.466
Slope 1.546 0.568 2.722 0.006
Age<5years Interceptat3months 3.130 1.664 1.881 0.060
Interceptat6months 1.673 1.423 1.176 0.240
Interceptat12months 1.242 1.942 0.640 0.522
Slope 1.458 0.735 1.984 0.047
Age>18years Interceptat3months 0.649 1.443 0.450 0.653
Interceptat6months 1.229 1.234 0.996 0.319
Interceptat12months 2.388 1.689 1.414 0.157
Slope 0.580 0.639 0.907 0.364
Cause:flameburns Interceptat3months 1.006 1.490 0.675 0.499
Interceptat6months 0.840 1.272 0.661 0.509
Interceptat12months 0.509 1.719 0.296 0.767
Slope 0.166 0.651 0.255 0.799
TBSA Interceptat3months 0.024 0.044 0.552 0.581
Interceptat6months 0.041 0.037 1.107 0.268
Interceptat12months 0.076 0.051 1.486 0.137
Slope 0.017 0.019 0.893 0.372
SE,standarderror;CR,criticalratio.Referencecategorieswerefemalesex,partialthicknessburns,age5–18years,scaldburns.TBSAwasa continuousvariableinthemodel.
burns xxx (2019) xxx–xxx
5
JBUR58071–8
321 completedthequestionnairesforthepatientsunder5years 322 oldmayhavecontributedtothedifferencesintheoutcomes 323 between theage groups. We did notfindany studiesthat 324 reportedtheinfluenceofageoncolorchangeinburnscars. 325 Furthermore,itshouldbenotedthatdifferentstudieshave 326 describedanegativeassociationbetweenageand hypertro-327 phic scar formation [37]. This finding is supported by the 328 decreased proliferation, reepithelization and inflammatory 329 responsesthatareobservedduringwoundhealing,aswellas 330 theslowerepidermalturnoverandthedifferentremodeling 331 phasethatareobservedinagedindividuals[7,37,38].However, 332 the present study did not investigate hypertrophic scar 333 formation. Finally, patients who were above 18 years had 334 higherpainscoresat3,6and12monthspost-burncompared 335 topatientswhowerebelow18years.
336 ThepercentageofTBSAwasapredictorforthepruritus, 337 thicknessandreliefitemscores.Theeffectofthepercentage 338 of TBSA on pruritus has been well described in various 339 studies.However,thereareconflictingdataontheeffectof 340 thepercentageofTBSAonthedurationofpruritus.VanLoey 341 etal.describedahigherTBSAtobeariskfactorforpruritusat 342 3 months post-burn[10]. The scar tissue modulation and 343 nerve densitywhicharethought tobehighestin thefirst 344 6monthspost-burncould explainthiseffect.However, in 345 linewithotherstudies,wefoundtheeffectofthepercentage
346
ofTBSAtobesignificantevenat12monthspost-burn[30,39].
347
Furthermore, the effect of full thickness burns and the
348
percentageofTBSAonitchingisdifferentthantheeffectof
349
fullthicknessburnsonpain.Painscoreswereobservedtobe
350
thelowestofallthescoreditemsonthePOSASpatientscale.
351
Thiscouldbecausedbyadifferentmechanismorbyabetter
352
treatmentforpain.
353
Scaldinjuriesaremoreoftenobservedinpatientswhoare
354
under5years,whereasfire/flameburnsareobservedmore
355
ofteninolderpatients.Additionally,moremalesthanfemales
356
areadmittedtoburncentres.Fullthicknessburnsandburns
357
withahigherpercentageofTBSAtendtooccurmoreoftenin
358
patientswhoareolderthan18years.Flameburnsaremore
359
oftendeepdermalorfull-thicknessburns.Overall,ourdataare
360
corroborated by the findings of various epidemiological
361
studies[19,40].
362
Our studyhad several limitations.First, the age-related
363
findings ofthepatients whowereunder5yearsshouldbe
364
interpretedwithcaution,giventhatthecaregiverscompleted
365
the questionnaires.Second,nosamplesizecalculationwas
366
performed,giventhelargenumberofincludedpatientsand
367
giventhatthedatawereretrospectivelycollected.However,a
368
samplesizecalculationcouldstillberelevant,basedonthe
369
amountofmissingdata.Third,theextentoftheinfluenceof
370
theexcludedpatientsontheresultsofthecurrentstudyis
Table4A–Regressionweightsandp-valuesoftheitemspain,pruritusandcolorofthePOSASpatientscalefromthe
predictorsTBSA,burndepth,agecategory,sexandcauseofburn.
ItemsPOSASpatientscale Pain Pruritus Color
Predictors Estimate p Estimate p Estimate p
Sex:male Intercept3months 0.730 <0.001 0.676 0.015 0.181 0.419
Intercept6months 0.598 <0.001 0.614 0.009 0.039 0.830
Intercept12months 0.335 0.124 0.489 0.118 0.246 0.375
Slope 0.132 0.117 0.062 0.611 0.143 0.217
Depth:fullthickness Intercept3months 0.125 0.572 0.756 0.016 0.249 0.324
Intercept6months 0.090 0.631 0.374 0.156 0.100 0.624
Intercept12months 0.019 0.939 0.392 0.266 0.200 0.524
Slope 0.035 0.708 0.383 0.005 0.150 0.250
Age<5years Intercept3months 0.070 0.807 0.069 0.866 1.031 0.002
Intercept6months 0.071 0.771 0.316 0.355 0.660 0.012
Intercept12months 0.072 0.822 1.084 0.017 0.082 0.839
Slope 0.000 0.997 0.384 0.031 0.371 0.027
Age>18years Intercept3months 1.282 <0.001 0.480 0.175 0.008 0.978
Intercept6months 1.330 <0.001 0.311 0.294 0.360 0.115
Intercept12months 1.427 <0.001 0.009 0.983 1.065 0.003
Slope 0.049 0.648 0.169 0.275 0.352 0.016
Cause:flameburns Intercept3months 0.303 0.240 0.065 0.858 0.951 0.001
Intercept6months 0.313 0.150 0.027 0.929 0.527 0.025
Intercept12months 0.333 0.236 0.049 0.903 0.320 0.371
Slope 0.010 0.926 0.038 0.810 0.424 0.004
TBSA Intercept3months 0.001 0.854 0.020 0.067 0.001 0.900
Intercept6months 0.002 0.801 0.023 0.011 0.005 0.491
Intercept12months 0.002 0.808 0.029 0.016 0.012 0.254
Slope 0.000 0.948 0.003 0.506 0.004 0.405
Referencecategorieswerefemalesex,partialthicknessburns,age5–18years,scaldburns.TBSAwasacontinuousvariableinthemodel.
371 unknown, because no data ofthe excluded patients were 372 recorded.Fourth,thereareconflictingdataonwhetherthe 373 POSASscoreisaunidimensionalinstrument.Therefore,the 374 scoresoftheindividualitemscouldbesummedintoatotal 375 score[13,21]. Intheory,the POSASpatientquestionnaireis 376 basedonaformativemodelinwhichtheindividualitemsof 377 the POSAS patient score are causal indicators of the scar 378 quality.Aformativequestionnairecouldconsistofmorethan 379 onedimension.Thustheindividualitemscouldbesummedto 380 afinalscore,forexampleasisdonefortheApgarscore.Finally, 381 theincludedstudypredictorswereobtainedfromtheavailable 382 literature,whereasnosystematicsearchwasperformed.Asa 383 result,theremaybepredictorsthatarenotincludedinthe 384 currentstudy,whichmayberelevantinthecontextofchanges 385 inthePOSASscoresat3,6and12monthspost-burn.
386
5.
Conclusion
387 This retrospective study, the POSAS patient total and 388 individualitemscoresdemonstratedastatisticallysignificant 389 improvementinthefirst12monthspost-burn,exceptforthe 390 relief item. Furthermore, sex, age, depth of the wound, 391 percentage of TBSA and flame burns were predictors of
392
variousPOSASpatientitemsat3,6and12monthspost-burn.
393
However,theeffectofthesepredictorswasnotthesamefor
394
theindividualPOSASpatientitems.
395
Source
of
funding
396
Thisworkwasconductedwithoutexternalfinancialsupport.
397
Conflict
of
interest
398
Noneoftheauthorshaveanypotentialconflictsofinterestto
399
disclose.
400
Uncited
re
ferences
401
[24,25].
402
Acknowledgements
403
None.
Table4B–Regressionweightsandp-valuesoftheitemspliability,thicknessandreliefofthePOSASpatientscalefromthe
predictorsTBSA,burndepth,agecategory,sexandcauseofburn.
ItemsPOSASpatientscale Pliability Thickness Relief
Predictors Estimate p Estimate p Estimate p
Sex:male Intercept3months 0.393 0.138 0.136 0.617 0.520 0.051
Intercept6months 0.545 0.012 0.269 0.252 0.435 0.045
Intercept12months 0.847 0.011 0.537 0.114 0.264 0.421
Slope 0.151 0.262 0.134 0.294 0.085 0.528
Depth:fullthickness Intercept3months 1.151 <0.001 0.797 0.009 1.076 <0.001
Intercept6months 0.682 0.005 0.463 0.080 0.863 <0.001
Intercept12months 0.254 0.497 0.204 0.595 0.438 0.238
Slope 0.468 0.002 0.334 0.020 0.213 0.162
Age<5years Intercept3months 1.333 <0.001 0.953 0.016 0.574 0.141
Intercept6months 0.799 0.012 0.787 0.022 0.453 0.153
Intercept12months 0.267 0.580 0.453 0.360 0.209 0.662
Slope 0.533 0.007 0.167 0.369 0.122 0.536
Age>18years Intercept3months 0.492 0.143 0.026 0.940 0.031 0.928
Intercept6months 0.307 0.264 0.018 0.951 0.147 0.592
Intercept12months 0.062 0.882 0.004 0.993 0.503 0.228
Slope 0.185 0.280 0.007 0.964 0.178 0.299
Cause:flameburns Intercept3months 0.277 0.425 0.514 0.147 0.025 0.942
Intercept6months 0.318 0.262 0.302 0.325 0.153 0.589
Intercept12months 0.400 0.349 0.123 0.780 0.408 0.336
Slope 0.041 0.813 0.212 0.196 0.127 0.465
TBSA Intercept3months 0.004 0.667 0.021 0.042 0.026 0.010
Intercept6months 0.006 0.508 0.015 0.094 0.023 0.006
Intercept12months 0.008 0.541 0.003 0.821 0.016 0.200
Slope 0.001 0.827 0.006 0.212 0.003 0.517
Referencecategorieswerefemalesex,partialthicknessburns,age5–18years,scaldburns.TBSAwasacontinuousvariableinthemodel.
burns xxx (2019) xxx–xxx
7
JBUR58071–8
404
Appendix
A.
Supplementary
data
405 Supplementary material related to this article can be 406 found,intheonlineversion,atdoi:https://doi.org/10.1016/j.
407 burns.2019.03.025.
408
REFERENCES
[1]
409 Stavrou,WeissmanO,TessoneA,ZilinskyI,HollowayS,Boyd
J,etal.Healthrelatedqualityoflifeinburnpatients—areview
410 oftheliterature.Burns2014;40(5):788–96.
[2]
411 Falder,BrowneA,EdgarD,StaplesE,FongJ,ReaS,etal.Core 412 outcomesforadultburnsurvivors:aclinicaloverview.Burns
2009;35(5):618–41. [3]
413 vanBaarE,Essink-BotML,OenIM,DokterJ,BoxmaH,van 414 BeeckEF.Functionaloutcomeafterburns:areview.Burns
2006;32(1):1–9. [4]
415 GangemiN,GregoriD,BerchiallaP,ZingarelliE,CairoM, 416 BolleroD,etal.Epidemiologyandriskfactorsforpathologic 417 scarringafterburnwounds.ArchFacialPlastSurg2008;10 418 (2):93–102.
[5]
419 BombaroM,EngravLH,CarrougherGJ,WiechmanSA,Faucher
L,CostaBA,etal.Whatistheprevalenceofhypertrophic
420 scarringfollowingburns?Burns2003;29(4):299–302.
[6]
421 DeitchA,WheelahanTM,RoseMP,ClothierJ,CotterJ. 422 Hypertrophicburnscars:analysisofvariables.JTrauma
1983;23(10):895–8. [7]
423 Butzelaar , UlrichMM, MinkvanderMolen AB, NiessenB, Beelen
RH. Currently known riskfactors for hypertrophic skin scarring: 424 areview.JPlastReconstrAesthetSurg2016;69(2):163–9.
[8]
425 LawrenceW,MasonST,SchomerK,KleinMB.Epidemiology 426 andimpactofscarringafterburninjury:asystematicreviewof 427 theliterature.JBurnCareRes2012;33(1):136–46.
[9]
428 Li-TsangW,LauJC,ChanCC.Prevalenceofhypertrophicscar 429 formationanditscharacteristicsamongtheChinese 430 population.Burns2005;31(5):610–6.
[10]
431 VanLoeyE,BremerM,FaberAW,MiddelkoopE,Nieuwenhuis
MK.Itchingfollowingburns:epidemiologyandpredictors.BrJ
432 Dermatol2008;158(1):95–100. [11]
433 MundyR,MillerHC,KlassenAF,CanoSJ,PusicAL.
Patient-434 reportedoutcomeinstrumentsforsurgicalandtraumatic 435 scars:asystematicreviewoftheirdevelopment,content,and 436Q8 psychometricvalidation.AestheticPlastSurg2016.
[12]
437 DraaijersJ,TempelmanFR,BotmanYA,TuinebreijerWE, 438 MiddelkoopE,KreisRW,etal.Thepatientandobserverscar 439 assessmentscale:areliableandfeasibletoolforscarevaluation. 440 PlastReconstrSurg2004;113(7)1960–5discussion6–7.
[13]
441 DeJongM,PhillipsM,EdgarDW,WoodFM.Patientopinionof 442 scarringismultidimensional:aninvestigationofthePOSAS 443 withconfirmatoryfactoranalysis.Burns2017;43(1):58–68.
[14]
444 Thepatientandobserverscarassessmentscale(POSAS)..
[15]
445 Tyack,WasiakJ,SpinksA,KimbleR,SimonsM.Aguideto 446 choosingaburnscarratingscaleforclinicalorresearchuse. 447 Burns2013;39(7):1341–50.
[16]
448 vanderWalB,VloemansJF,TuinebreijerWE,vandeVenP,van 449 UnenE,vanZuijlenPP,etal.Outcomeafterburns:an 450 observationalstudyonburnscarmaturationandpredictors 451 forseverescarring.WoundRepairRegen2012;20(5):676–87.
[17]
452 Goei,vanderVliesCH,TuinebreijerWE,vanZuijlenPPM, 453 MiddelkoopE,vanBaarME.Predictivevalidityofshortterm 454 scarqualityonfinalburnscaroutcomeusingthePatientand 455 ObserverScarAssessmentScaleinpatientswithminorto 456 moderateburnseverity.Burns2017;43(4):715–23.
457 CubisonC,PapeSA,ParkhouseN.Evidenceforthelink 458 betweenhealingtimeandthedevelopmentofhypertrophic
[18]scars(HTS)inpaediatricburnsduetoscaldinjury.Burns 459 2006;32(8):992–9.
[19]Dokter,VloemansAF,BeerthuizenGI,vanderVliesCH, 460
461
BoxmaH,BreederveldR,etal.Epidemiologyandtrendsin
462
severeburnsintheNetherlands.Burns2014;40(7):1406–14.
[20]VloemansF,DokterJ,vanBaarME,NijhuisI,BeerthuizenGI, 463
464
NieuwenhuisMK,etal.Epidemiologyofchildrenadmittedto
465
theDutchburncentres.Changesinreferralinfluence
466
admittanceratesinburncentres.Burns2011;37(7):1161–7.
[21]vanderWalB,TuinebreijerWE,BloemenMC,VerhaegenPD, 467
468
MiddelkoopE,vanZuijlenPP.RaschanalysisofthePatientand
469
ObserverScarAssessmentScale(POSAS)inburnscars.Qual
470
LifeRes2012;21(1):13–23.
[22]Arbuckle.AMOSTM22user’sguide.IBM;2013. 471 [23]ByrneM.StructuralequationmodelingwithAMOS.Basic 472
473
concepts,applications,andprogramming.Thirded.NewYork &London:Taylor&FrancisGroup;2016.
[24]DiLallaF.Astructuralequationmodelingoverviewformedical 474
475
researchers.JDevBehavPediatr2008;29(1):51–4.
[25]ByrneM,LamWW,FieldingR.Measuringpatternsofchangein 476
477
personalityassessments:anannotatedapplicationoflatent
478
growthcurvemodeling.JPersAssess2008;90(6):536–46.
[26]AnderssonI,EjlertssonG,LedenI,RosenbergC.Chronicpain 479
480
inageographicallydefinedgeneralpopulation:studiesof
481
differencesinage,gender,socialclass,andpainlocalization.
482
ClinJPain1993;9(3):174–82.
[27]ForgaysG,RzewnickiR,OberAJ,ForgaysDK.Headachein 483
484
collegestudents:acomparisonoffourpopulations.Headache 1993;33(4):182–90.
[28]SternbachA.Painand’hassles’intheUnitedStates:findings 485
486
oftheNuprinpainreport.Pain1986;27(1):69–80.
[29]FillingimB.Sex,gender,andpain:womenandmenreallyare 487
488
different.CurrRevPain2000;4(1):24–30.
[30]CarrougherJ,MartinezEM,McMullenKS,FauerbachJA, 489
490
HolavanahalliRK,HerndonDN,etal.Pruritusinadultburn
491
survivors:postburnprevalenceandriskfactorsassociated
492
withincreasedintensity.JBurnCareRes2013;34(1):94–101.
[31]CashF,MorrowJA,HraboskyJI,PerryAA.Howhasbodyimage 493
494
changed?Across-sectionalinvestigationofcollegewomenand
495
menfrom1983to2001.JConsultClinPsychol2004;72(6):1081–9. [32]SmithE,ThompsonJK,RaczynskiJM,HilnerJE.Bodyimage 496
497
amongmenandwomeninabiracialcohort:theCARDIA
498
Study.IntJEatDisord1999;25(1):71–82.
[33]Dyer,Mayer-EckhardL,WhiteAJ,AlpersGW.Theroleofscar 499
500
origininshapingmen’sbodyimage.AmJMensHealth2015;9
501
(2):115–23.
[34]KuipersC,BremerM,BraemL,GoemanneAS,MiddelkoopE, 502
503
vanLoeyNE.Itchinburnareasafterskintransplantation:
504
patientcharacteristics,influencingfactorsandtherapy.Acta
505
DermVenereol2015;95(4):451–6.
[35]Goutos,DziewulskiP,RichardsonPM.Pruritusinburns: 506
507
reviewarticle.JBurnCareRes2009;30(2):221–8.
[36]SchwanholtA,RidgwayCL,GreenhalghDG,StaleyMJ, 508
509
GabouryTJ,MorressCS,etal.Aprospectivestudyofburnscar
510
maturationinpediatrics:doesagematter?JBurnCareRehabil 1994;15(5):416–20.
[37]MahdavianDelavary,vanderVeerM,FerreiraJA,NiessenFB. 511
512
Formationofhypertrophicscars:evolutionandsusceptibility.
513
JPlastSurgHandSurg2012;46(2):95–101.
[38]Stevenson,ThorntonJ.Effectofestrogensonskinaging 514
515
andthepotentialroleofSERMs.ClinIntervAging2007;2
516
(3):283–97.
[39]Willebrand,LowA,Dyster-AasJ,KildalM,AnderssonG, 517
518
EkseliusL,etal.Pruritus,personalitytraitsandcopingin
long-519
termfollow-upofburn-injuredpatients.ActaDermVenereol 2004;84(5):375–80.
[40]Smolle,Cambiaso-DanielJ,ForbesA,WurzerP,Hundeshagen 520 G,BranskiLK,etal.Recenttrendsinburnepidemiology
521
worldwide:asystematicreview.Burns2016.