Nursing Procedure: Underwater seal chest drainage in the Highly
Dependent or Critically Ill Infant or Child–
2. The nurses role in ongoing chest drain management
Lead Manager: Ms. Elaine Johnstone, Lead Nurse
Responsible Director: Dr Neil Spenceley, Clinical Director, Critical Care Author(s): Jeanette Grady, Clinical Nurse Educator, Critical Care Approved by: PICU/HDU Clinical Guideline Group
Date approved: September 2013 Date for Review: September 2015 Replaces previous version: June 2011
Chest Drain Ongoing Management Version: 2.0 Page 1 of 10
Authors: Jeanette Grady Authorised by PERG Issue Date: Aug 2013 Revision date: July 2015 Q-Pulse ref: YOR-PICU-030
Chest Drain Ongoing Management Version: 2.0 Page 2 of 10
Authors: Jeanette Grady Authorised by PERG Issue Date: Aug 2013 Revision date: July 2015 Q-Pulse ref: YOR-PICU-030
1. Introduction
Chest drains and chest drainage systems are used frequently in the paediatric intensive care unit. There are many reasons for chest drain insertion but primarily they are used whenever there are specific conditions that interfere with the normal mechanism of lung expansion and altered intrathoracic pressures.
Pleural chest tubes are inserted to evacuate blood, pus, air and fluid, from the thoracic cavity, to re-establish negative pressure in the intra pleural space and thereby expand the lungs following collapse resulting from surgery or trauma.
Mediastinal chest tubes are placed in the mediastinum following open heart surgery, via a medial sternotomy in order to prevent accumulation of blood and clots around the heart, which could cause cardiac tamponade – a life threatening situation.
There are many different types of chest drains available including one-way flutter valve drains such as the Heimlich device or portable drains. However, for the majority of patients in the paediatric intensive care and high dependency units an underwater seal chest drainage system will be used. These systems provide an underwater seal, fluid collection chamber and suction chamber.
In paediatric intensive care and high dependency, it is the bed side nurses’ role to ensure the patient is cared for safely once chest drains have been inserted. Although insertion of a chest drain may be necessary to help restore adequate oxygenation and promote lung re-expansion in the patient, there are potential risks and complications that the nurse must be aware of.
This guideline is intended as a resource for staff involved in caring for childen in the Paediatric Intensive care and High Dependency units that require an underwater seal chest drain in situ. The guideline has been constructed after literature search and review of sourced textbooks, national guidelines (N.I.C.E.), Medline and CINHAL, and external nurse expert peer review and opinion.
Further information on chest drainage in: ‘Tutorial Notes-Chest Drainage’ Maxwell (unpublished 2008, reviewed 2010) and additional chest drain system resource at: www.atriummed.com/
See also recommendations and further information at end of this guideline. 2. Scope
This nursing procedural guideline is intended to be followed by nurses involved in caring for the highly dependent or critically ill infant or child requiring underwater seal chest drainage within the Paediatric Intensive Care and High Dependency Units at R.H.S.C. Yorkhill.
3. Roles and responsibilities
All nursing staff involved in caring for infants or children requiring underwater seal chest
drainage in Paediatric Intensive care and High Dependency should be familiar with this nursing procedural guideline.
4. BODY OF POLICY OR PROCEDURE
Equipment : Available for ongoing management or in case of any untoward event* (*separate guideline)
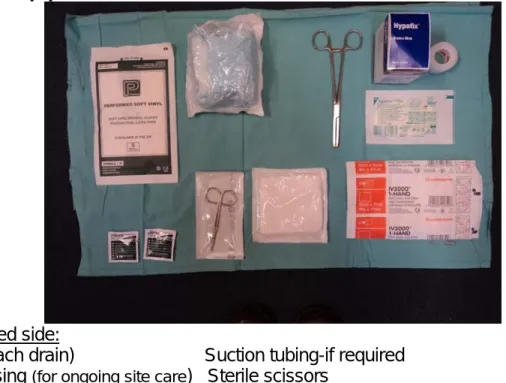
Fig. 1. Bed side equipment
Available at bed side:
Clamps (x1 each drain) Suction tubing-if required Suitable dressing (for ongoing site care) Sterile scissors
Disposable apron Disposable gloves Wall suction gauge-if required (low flow *See Fig. 2)
Occlusive dressing (E.g. sterile swabs)
Tape (to secure occlusive dressing) Sterile gloves Sterile water
Chlorhexidine 2% & 70% alcohol (swab suitable for urgent event) On chest drain trolley:
Chest drain unit
Fig. 2. *Low flow suction unit
Chest Drain Ongoing Management Version: 2.0 Page 3 of 10
Authors: Jeanette Grady Authorised by PERG Issue Date: Aug 2013 Revision date: July 2015 Q-Pulse ref: YOR-PICU-030
Chest Drain Ongoing Management Version: 2.0 Page 4 of 10
Authors: Jeanette Grady Authorised by PERG Issue Date: Aug 2013 Revision date: July 2015 Q-Pulse ref: YOR-PICU-030
PROCEDURE RATIONALE Vital signs & patient observations: The
infant or child with a chest drain(s) in situ must have the following observations monitored frequently & documented:
Respiratory rate, effort & work of breathing
Air entries
Heart rate & pulse
Oxygen saturations (SpO2)
Blood pressure
Temperature
If a suitable invasive monitoring line is in situ then regular arterial or venous blood gases should be done.
Frequent monitoring of vital signs is important in detecting any alterations from previously documented normal values as these may indicate problems such as haemorrhage, unresolved pneumothorax, tension pneumothorax, sepsis, infection and ventilation-perfusion mismatch.
Suggestions for monitoring vital signs ranges from ¼ hourly immediately post drain insertion/admission, to ½ hourly to hourly whilst drain is in situ.
The frequency of monitoring specific vital signs and blood gas analysis will be determined by the child’s clinical status with any deterioration in the child’s vital signs being reported to the nurse-in-charge and medical team immediately. Chest drain site care: the nurse must
ensure the drain site is checked regularly for the following:
Drain is properly anchored with appropriate suture(s) and secured to child’s chest wall
Drain site is dry, clean & covered with dry non-adherent dressing
Drain site dressing should be inspected for signs of leakage or odour
Area around drain site inspected for signs of leakage, inflammation, infection or subcutaneous emphysema
The drain must be well secured after insertion to prevent it becoming dislodged, slipping or falling out.
Large amounts of tape and padding may restrict chest movement and prevent regular inspection of the drain site for complications. A dry non-adherent dressing, non-occlusive is most suitable.
The drain site and dressing should be reviewed daily and the dressing should not need redressed for 2-3 days unless leakage apparent.
Any signs of complications such as infection should be documented and reported and appropriate action taken. E.g. wound swab or medical team review.
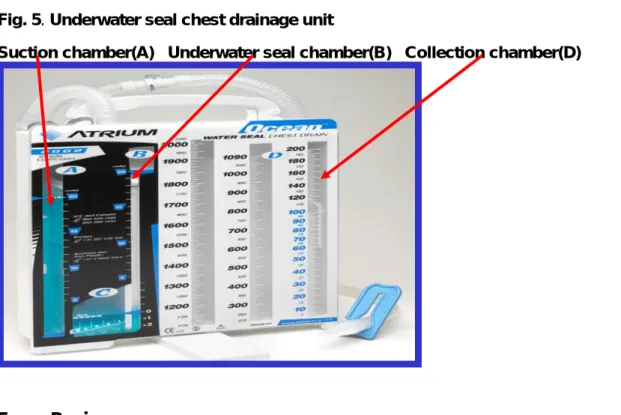
Chest drainage unit (CDU) care: the nurse must check the under water seal chest drainage system frequently to ensure it is working correctly and to avoid potential problems: *see Fig. 5
Chest Drain Ongoing Management Version: 2.0 Page 5 of 10
Authors: Jeanette Grady Authorised by PERG Issue Date: Aug 2013 Revision date: July 2015 Q-Pulse ref: YOR-PICU-030
Keep chest drainage system and tubing below the level of the patients chest
Perform initial inspection of connections & tubing.
Thereafter inspect CDU tubing & drain connections regularly (suggested hourly) and keep tubing free from bed-sides/cot-sides
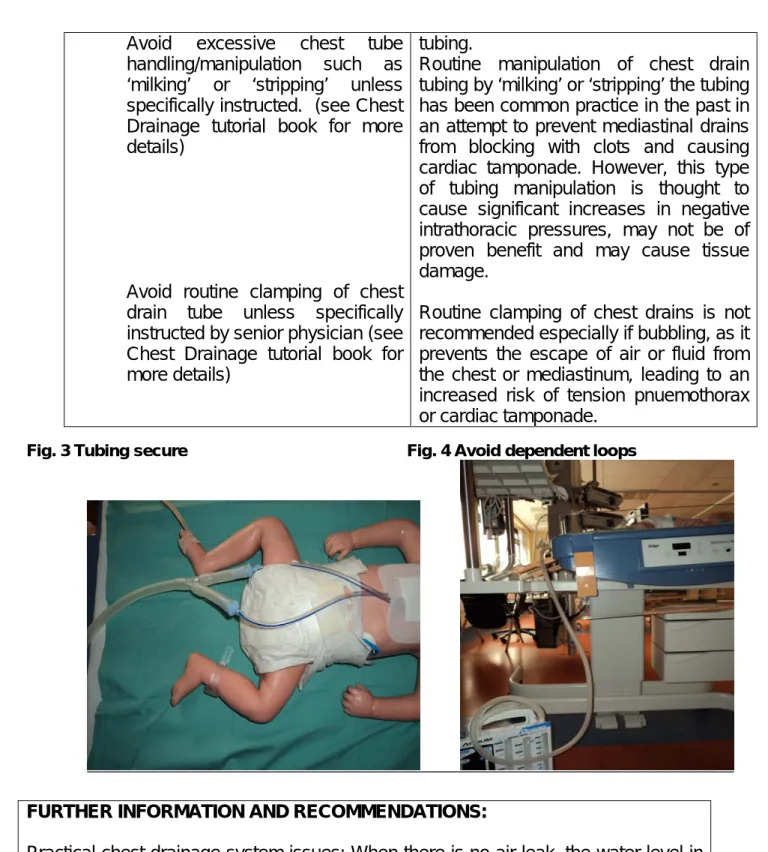
Ensure tubing & drain(s) are secure but not ‘pulling’. Try not to secure tubing to child’s bed, linen or loose clothing (Fig. 3)
Aim to lay tubing horizontally across bed before dropping it vertically into drainage system to facilitate drainage – avoid dependent ‘loops’ or kinking of tubing (Fig. 4)
Ensure chest drainage unit is secured upright on floor beside or at the end of the bed/cot.
Check water seal chamber (B)* maintained at 2cm level
Monitor and record any ‘bubbling’ or ‘swinging’ in the water seal chamber of the CDU. Report any changes to nurse-in-charge.
If chest drain in pleural cavity, observe and record any fluctuations in water seal level of
CDU with respiratory effort/ventilation – ‘tidalling’
Ensure suction chamber (A)* filled to -20cmH2O level in CDU.
The chest drainage system must always be kept below the level of the child’s chest to prevent fluid re-entering the pleural space – syphonage.
Regular inspection of the drain and tubing is vital to ensure that the system is still intact the drain has not slipped, connections have not come loose or tubing has become kinked.
Securing tubing to clothing or bedding is not advised as sudden movements by the child or change of bed-linen could dislodge the drain.
Dependent loops or kinking of tubing can impede drainage, block tubing and cause high pressures at chest tube and drainage tube connections, potentially resulting in clinical complications such as tension pneumothorax.
Securing the drainage system to the floor with tape may be necessary to prevent tipping of system.
Water in the water seal chamber (B)* can evaporate and under water seal will be lost. The level must be checked regularly and ‘topped-up’ as per manufacturers instructions.
Persistent bubbling may suggest visceral pleural air leak, a drain on suction that has one of the drain eyelets open to air or with mediastinal drains patient with ‘open’ chest. ‘Swinging’ of the water seal level with respirations indicates drain patency and confirms drain position in pleural cavity.
If suction is required, a low pressure system must be used as excessive
Chest Drain Ongoing Management Version: 2.0 Page 6 of 10
Authors: Jeanette Grady Authorised by PERG Issue Date: Aug 2013 Revision date: July 2015 Q-Pulse ref: YOR-PICU-030
If suction required - Check suction tubing connected to low flow regulated suction & suction control stopcock at CDU switched on.
Check negative pressure on suction is set low enough to give gentle bubbling in the suction chamber – no excessive bubbling
Ensure suction filter attached – changed when indicated
Check fluid collection chamber (D)* frequently (15 min. intervals to 30min., then hourly) and document volume, type and colour of drainage. E.g. fresh blood, serous, cloudy.
Always label chest drain(s) and drainage units clearly. E.g. Left pleural 1 or Right mediastinal 2.
negative pressures may cause perpetuation of air leaks. If suction is required for more than one chest drain then a separate suction unit is advised for each chest drain.
Turbulent bubbling is unnecessary, will not improve fluid drainage and will result in increased evaporation of water in the chamber.
Frequent assessing and documenting of fluid volume and type drained and from what site is essential, as this may help the nurse determine if the child has any of the following:
Persistent or fresh bleeding
Infection
Chylothorax
Tamponade
Frequency of checking tubing and drainage will range from every 15 minutes initially (for first 6 hours) post admission from cardiac or thoracic surgery, to 30 minutes (6 hours) then hourly once child stabilised. This is provided there is no other evidence or suspicion of bleeding or tamponade present.
Specific nursing care issues:
The nurse should assess the child’s level of pain or discomfort regularly and administer analgesia as prescribed
Reposition the child regularly as tolerated ensuring drain and tubing secure throughout – a two nurse procedure.
Pain from having a chest drain in situ can inhibit the child’s movement and breathing which can slow their recovery. Therefore, regular pain assessment is vital to ensure the child receives adequate analgesia while the drain is in situ.
Repositioning and improving mobility can facilitate drainage, aid breathing and lung expansion and reduce complications associated with immobility.
Repositioning the infant/child with a chest drain in situ should involve at least two nurses in order to prevent accidental disconnection or kinking of drain and/or
Avoid excessive chest tube handling/manipulation such as ‘milking’ or ‘stripping’ unless specifically instructed. (see Chest Drainage tutorial book for more details)
Avoid routine clamping of chest drain tube unless specifically instructed by senior physician (see Chest Drainage tutorial book for more details)
tubing.
Routine manipulation of chest drain tubing by ‘milking’ or ‘stripping’ the tubing has been common practice in the past in an attempt to prevent mediastinal drains from blocking with clots and causing cardiac tamponade. However, this type of tubing manipulation is thought to cause significant increases in negative intrathoracic pressures, may not be of proven benefit and may cause tissue damage.
Routine clamping of chest drains is not recommended especially if bubbling, as it prevents the escape of air or fluid from the chest or mediastinum, leading to an increased risk of tension pnuemothorax or cardiac tamponade.
Fig. 3 Tubing secure Fig. 4 Avoid dependent loops
Chest Drain Ongoing Management Version: 2.0 Page 7 of 10
Authors: Jeanette Grady Authorised by PERG Issue Date: Aug 2013 Revision date: July 2015 Q-Pulse ref: YOR-PICU-030
FURTHER INFORMATION AND RECOMMENDATIONS:
Practical chest drainage system issues: When there is no air leak, the water level in the water seal chamber should rise and fall with the patient's respirations, reflecting normal pressure changes in the pleural cavity during respiration. During spontaneous respirations, the water level should rise during inhalation and fall during exhalation. If the patient is receiving positive pressure ventilation, the oscillation will be just the opposite. Oscillations may be absent if the lung is fully expanded and suction has drawn the lung up against the holes in the chest tubes.
A patient with only mediastinal tubes (and a ‘closed’ chest) should have no bubbling or fluctuations in the water seal chamber, since these tubes are not in contact with the pleural cavity. As one of the risks of accumulation of fluid, blood or clots around the heart is cardiac tamponade, it is particularly important for nurses caring for patients with mediastinal chest tubes to be watchful for signs of cardiac tamponade with special attention paid to the drainage collection chamber.
Fig. 5. Underwater seal chest drainage unit
Suction chamber(A) Underwater seal chamber(B) Collection chamber(D)
. Review 5
his nursing procedural guideline should be reviewed every two years from date of approval. T
. References 6
Allibone, L (2003) Nursing Management of chest drains. Nursing Standard, Vol.12 (17), pp 45-4.
5
Allibone, L (2005) Principles for inserting and managing chest drains. Nursing Times, Vol. 101 42), pp45-48.
(
Atrium (2012) A personal guide to managing chest drainage. Available from:
http://www.atriummed.com/EN/Chest_Drainage/Documents/BlueHandbook342263L.pdf
Chest Drain Ongoing Management Version: 2.0 Page 8 of 10
Authors: Jeanette Grady Authorised by PERG Issue Date: Aug 2013 Revision date: July 2015 Q-Pulse ref: YOR-PICU-030
Chest Drain Ongoing Management Version: 2.0 Page 9 of 10
Authors: Jeanette Grady Authorised by PERG Issue Date: Aug 2013 Revision date: July 2015 Q-Pulse ref: YOR-PICU-030
Balfour-Lynn, IM Abrahamson, E Cohen, G Hartley, J King, S Parikh, D Spencer, D Thomson, AH Urquhart, D (2005) Draft - BTS guidelines for the management of pleural infection in children. Thorax, Vol. 60, Suppl.I, pp. i1-i21.
Bar-El, Y Ross, A Kablawi, A Egenburg, S (2001) Potentially dangerous negative pressures generated by ordinary pleural drainage systems. Chest, Vol. 119 (2), pp 511-514.
Briggs, D (2010) Nursing care and management of patients with intrapleural drains. Nursing
Standard, Vol. 24 (21), pp. 47-55.
Coughlin, AM Parchinsky, C (2006) Go with the flow of chest tube therapy. Nursing, Vol. 36 (3), pp 36-41.
Crawford, D (2011) Care and management of a child with a chest drain. Nursing Children and
Young People, Vol.23 (10), pp.27-33.
Day, TG Perring, RR Gofton, K (2008) Is manipulation of mediastinal chest drains useful or harmful after cardiac surgery? Interactive Cardiovascular and ThoracicSurgery, Vil. 7, pp 888-890.
Duncan, C Erikson R (1982) Pressures associated with chest tube stripping. Heartand Lung,
Vol. 11 (2), pp. 166-171.
Halm. MA (2007) To strip or not to strip? Physiological effects of chest tube manipulation.
American Journal of Critical Care, Vol. 16 (6), pp. 609-612.
Havelock, T Teoh, R Laws, D Gleeson, F (2010) British Thoracic Society Pleural Disease Guideline: Pleural procedures and thoracic ultrasound. Thorax, Vol. 65, (Suppl. 2): ii.61–76. Horrox, F (2002) Chest drain management. In: Manual of Neonatal & Paediatric HeartDisease,
Whurr, London.
Scmelz, JO Johnson, D Norton, JM Andrews, M Gordon, PA (1999) Effects of position of chest drainage tube on volume drained and pressure. American Journal of CriticalCare, Vol. 8 (5), pp. 319-323.
Sullivan, B (2008) Nursing management of patients with a chest drain. British Journalof Nursing, Vol. 17 (6), pp 388-393.
Wallen, M Morrison, A Gillies, D O’Riordan, E Bridge, C Stoddart, F (2002) Mediastinal chest drain clearance for cardiac surgery. Cochrane Database ofSystematic Reviews, Issue 2, CD003042.
Chest Drain Ongoing Management Version: 2.0 Page 10 of 10 Authors: Jeanette Grady Authorised by PERG Issue Date: Aug 2013 Revision date: July 2015 Q-Pulse ref: YOR-PICU-030
A Communication and Implementation Plan R.H.S.C. Nursing Policy Group
PICU/HDU Clinical Guidelines group PICU/HDU Lead Nurse
PICU/HDU ANP’s, Band 7 and Band 6 senior nursing staff and nursing teams PICU/HDU Lead Consultant
PICU/HDU Consultants and junior medical staff B Monitoring
Compliance monitored by Lead nurse, ANP’s and Senior clinical nurses in PICU/HDU. Datix and critical incident reporting of adverse events or incidents
C Impact Assessment
EQIA not relevant to this nursing procedural guideline as there are no discriminatory practices identified in implementing this guideline.