STUDY
C
URRENTO
PINION‘No touch’ technologies for environmental
decontamination: focus on ultraviolet devices
and hydrogen peroxide systems
David J. Weber
a,b, Hajime Kanamori
a, and William A. Rutala
a,bPurpose of review
This article reviews ‘no touch’ methods for disinfection of the contaminated surface environment of hospitalized patients’ rooms. The focus is on studies that assessed the effectiveness of ultraviolet (UV) light devices, hydrogen peroxide systems, and self-disinfecting surfaces to reduce healthcare-associated infections (HAIs).
Recent findings
The contaminated surface environment in hospitals plays an important role in the transmission of several key nosocomial pathogens including methicillin-resistantStaphylococcus aureus, vancomycin-resistant
Enterococcusspp.,Clostridium difficile,Acinetobacterspp., and norovirus. Multiple clinical trials have now demonstrated the effectiveness of UV light devices and hydrogen peroxide systems to reduce HAIs. A limited number of studies have suggested that ‘self-disinfecting’ surfaces may also decrease HAIs.
Summary
Many studies have demonstrated that terminal cleaning and disinfection with germicides is often inadequate and leaves environmental surfaces contaminated with important nosocomial pathogens. ‘No touch’ methods of room decontamination (i.e., UV devices and hydrogen peroxide systems) have been demonstrated to reduce key nosocomial pathogens on inoculated test surfaces and on environmental surfaces in actual patient rooms. Further UV devices and hydrogen peroxide systems have been demonstrated to reduce HAI. A validated ‘no touch’ device or system should be used for terminal room disinfection following discharge of patients on contact precautions. The use of a ‘self-disinfecting’ surface to reduce HAI has not been convincingly demonstrated.
Keywords
healthcare-associated infections, hydrogen peroxide systems, room decontamination, surface environment, UV devices
INTRODUCTION
Healthcare-associated infections (HAIs) remain an important source of patient morbidity and mortality. Based on a large sample of U.S. acute care
hospitals, 4% of patients on any given day has
at least one HAI [1]. Based on this study, it was estimated that 722 000 HAIs occurred in 2011 in U.S. acute care hospitals which resulted in75 000 deaths. The total annual costs for the five major HAIs have been estimated to be $9.8 billion (2012 US dollars) [2]. Dr Weinstein estimated that the source of pathogens causing an HAI in the intensive care unit was the patients’ endogenous flora, 40–60%; cross-infection via the hands of healthcare personnel (HCP), 20–40%; antibiotic-driven changes in flora, 20–25%; and other (includ-ing contamination of the environment), 20% [3].
Further, contamination of the hands of HCP could result directly from patient contact or indirectly from touching contaminated environmental surfa-ces [4]. It has been shown that the gloves or hands of HCP are just as likely to become contaminated from touching a patient as touching an environmental surface in a patient’s room [5,6].
aDepartment of Hospital Epidemiology, University of North Carolina
Health Care and bDivision of Infectious Diseases, UNC School of
Medicine, Chapel Hill, North Carolina, USA
Correspondence to Dr David J. Weber, MD, MPH, 2163 Bioinformatics, CB #7030, Chapel Hill, NC 27599-7030, USA. Tel: +1 919 966 2536; fax: +1 919 966 1451; e-mail: [email protected]
This article will briefly review the following: first, data demonstrating that the contaminated surface environment in a hospitalized patent’s room plays an important role in the transmission of sev-eral key healthcare-associated pathogens; second, the rationale for the development and use of ‘no-touch’ methods of room decontamination; and third, the evidence supporting the effectiveness from room decontamination of ultraviolet (UV) light devices and hydrogen peroxide systems. This review will focus on the recent studies demonstrat-ing the effectiveness of ‘no-touch’ methods to decrease HAIs, and update and expand a recent paper that reviewed the ability of UV devices and hydrogen peroxide systems to decrease HAI [7&
].
ROLE OF THE CONTAMINATED SURFACE
ENVIRONMENT IN TRANSMISSIN OF
HEALTHCARE-ASSOCIATED PATHOGENS
Over the past decade, substantial scientific evidence has accumulated that contamination of environ-mental surfaces in hospital rooms plays an
important role in the transmission of several key healthcare-associated pathogens, including methi-cillin-resistantStaphylococcus aureus(MRSA), vanco-mycin-resistantEnterococcusspp. (VRE),Clostridium difficile,Acinetobacterspp., and norovirus [8–11,12&
]. In general, all these pathogens share the following characteristics: ability to survive for prolonged periods of time on environmental surfaces, ability to remain virulent after environmental exposure, frequent contamination of the hospital environ-ment, ability to colonize patients, ability to transi-ently colonize the hands of HCP, and transmission via the contaminated hands of HCP [8]. Norovirus andC. difficilealso are noted for a small inoculating dose, and relative resistance to antiseptics and dis-infectants used on environmental surfaces. Evi-dence supporting the role of the contaminated surface environment in the transmission of several key healthcare-associated pathogens is summarized as follows:
(1) The surface environment in rooms of colon-ized or infected patients is frequently contami-nated with the pathogen.
(2) The pathogen is capable of surviving on hos-pital room surfaces and medical equipment for a prolonged period of time.
(3) Contact with hospital room surfaces or medical equipment by HCP frequently leads to contamination of hands and/or gloves. (4) The frequency with which room surfaces are
contaminated correlates with the frequency of hand and/or glove contamination of HCP. (5) Daily use of a disinfectant instead of a
deter-gent reduces HAI rates.
(6) The patient admitted to a room previously occupied by a patient colonized or infected with a pathogen (e.g., MRSA, VRE,C. difficile,
Acinetobacter) has an increased likelihood of developing colonization or infection with that pathogen.
(7) Daily disinfection of room surfaces (versus clean only if soiled) reduces acquisition of pathogens on hands of HCP after contact with surfaces or patients.
(8) Improved terminal cleaning of rooms leads to a decreased rate of individual patient coloniza-tion and/or infeccoloniza-tions.
(9) Improved terminal cleaning of rooms leads to a decreased facility-wide rate of colonization and/or infection.
(10) Improved terminal disinfection with a ‘no-touch’ method leads to a decreased rate of infection in patients subsequently admitted to a room in which the prior occupant was colonized or infected.
KEY POINTS
The contaminated surface environment in patient rooms has been linked to transmission of several important nosocomial pathogens including MRSA, VRE,C. difficile,Acinetobacterspp., and norovirus.
Multiple studies have demonstrated that a substantial number of room surfaces are not adequately cleaned following patient discharge. Admittance to a room previously occupied by a patient colonized or infected with a multidrug-resistant pathogen (e.g., MRSA, VRE,
Acinetobacter) results in the newly admitted patient having an increased risk of acquiring that pathogen by 39–353%.
Because room surfaces are frequently not clean/ disinfected during terminal cleaning, multiple ‘no touch’ methodologies have been invented for terminal room disinfection. The most studied technologies are UV devices and hydrogen peroxide systems.
UV devices and hydrogen peroxide systems have been shown to eliminate clinically relevant numbers of important nosocomial pathogens from inoculated test objects and from actual room surfaces.
Multiple clinical trials have now demonstrated that UV devices and hydrogen peroxide systems decrease HAIs due to multidrug-resistant pathogens. Although many of the studies are of low quality, the consistency of the studies and the few well designed studies lead one to conclude that ‘no touch’ technologies are an effective method for enhancing terminal room disinfection and reducing the incidence of HAIs.
(11) Improved terminal disinfection with a ‘no-touch’ method leads to a decreased rate of facility-wide colonization and/or infection.
Importantly, admission to a room wherein the previous occupant was colonized or infected with a multidrug-resistant pathogen (e.g., MRSA, VRE, Aci-netobacterspp.) has been shown to increase the risk of acquiring that pathogen by 39–353% [9,13&&
]. Recent studies have extended the findings on the role of the environment in the transmission of noso-comial pathogens. A variety of medically important viruses have been found to be able to survive for an epidemiologically important duration as
well as contaminate environmental surfaces
including influenza viruses, severe acute respiratory disease-coronavirus and Middle East respiratory syndrome-coronavirus [14&
,15]. Carbapenem-resist-antEnterobacteriaceae(CRE) have been demonstrated to contaminate the environmental surfaces near colonized patients [16]. However, CRE strains do not survive for prolonged periods on environmental surfaces decreasing the risk that subsequent patients would acquire the pathogen [17]. As noted above the surface environment in rooms of colonized or infected patients is frequently contaminated. Recently, environmental contamination has been demonstrated in the rooms of C. difficileexcretors without diarrhea or active infection [18–20]. Several recent papers have demonstrated the presence of medically important nosocomial pathogens (e.g., MRSA, VRE,C. difficile) on the surfaces in rooms of patients not colonized or infected with the pathogen thus emphasizing the need for appropriate terminal disinfection of all hospital rooms [21,22].
RATIONALE FOR USING A ‘NO-TOUCH’
METHOD FOR TERMINAL ROOM
DISINFECTION
Multiple studies have demonstrated that surfaces in hospital rooms are poorly cleaned during terminal cleaning. Although methods of assessing the adequacy of cleaning varied (i.e., visibly clean, ATP bioluminescence, fluorescent dye, aerobic plate counts), several studies have demonstrated that less than 50% of room surfaces were properly cleaned [23,24]. Improved cleaning has been demonstrated to lead to reductions in HAIs [25]. However, it has been reported that there is a paucity of high-quality studies demonstrating that improved cleaning/ disinfection reduces HAIs [26]. Importantly, the studies that have assessed interventions to improve cleaning have reported that following the
interven-tion, 5 to 30% of surfaces remain potentially
contaminated [24].
‘NO TOUCH’ METHODS FOR
DECONTAMINATING HOSPITAL ROOM
SURFACES
As noted above, multiple studies have demonstrated that environmental surfaces and objects in rooms are frequently improperly cleaned/disinfected and these surfaces may be important in transmission of healthcare-associated pathogens. Further, although interventions aimed at improving cleaning thor-oughness have demonstrated effectiveness, many surfaces remain inadequately cleaned and therefore, potentially contaminated. For this reason, multiple new methodologies have been developed to decon-taminate environmental surfaces (i.e., ‘no touch’ methods) (Table 1) [7&
,27,28,29&&
,30&&
,31&
]. In addition, new technologies have been developed to inhibit the growth of microbes on environmental surfaces (i.e., ‘self-disinfecting surfaces’) (Table 1) [32,33,34&&
].
There are now substantial data demonstrating the effectiveness of ‘no touch’ methodologies for terminal room disinfection. These methodologies fall into two broad classes; devices that use UV light and systems that generate hydrogen peroxide
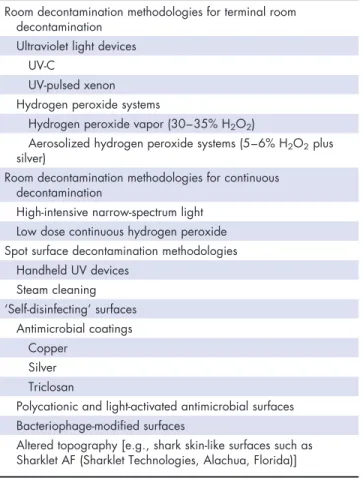
Table 1. ‘No touch’ methodologies for decontamination of hospital room surfaces
Room decontamination methodologies for terminal room decontamination
Ultraviolet light devices UV-C
UV-pulsed xenon Hydrogen peroxide systems
Hydrogen peroxide vapor (30–35% H2O2)
Aerosolized hydrogen peroxide systems (5–6% H2O2plus silver)
Room decontamination methodologies for continuous decontamination
High-intensive narrow-spectrum light Low dose continuous hydrogen peroxide Spot surface decontamination methodologies
Handheld UV devices Steam cleaning ‘Self-disinfecting’ surfaces
Antimicrobial coatings Copper
Silver Triclosan
Polycationic and light-activated antimicrobial surfaces Bacteriophage-modified surfaces
[7&
,27,28,29&&
,30&&
,31&
]. Ultraviolet light – C (UV-C) devices use specifically designated wavelengths (254 nm range) and deliver targeted doses for vege-tative bacteria (e.g., 12 000mW s/cm2) or for spores
(22 000–36,000mW s/cm2) on surfaces, while the
UV pulsed xenon devices emit broad spectrum UV in short pulses [28]. There are currently two major hydrogen peroxide systems [27]. First, H2O2 vapor
systems that deliver a heat-generated vapor of 30–
35% (w/w) aqueous H2O2 through a high-velocity
air stream to achieve homogeneous distribution throughout an enclosed area. Second, aerosolized H2O2 systems deliver a pressure-generated aerosol
[27]. The systems employed most frequently in
healthcare use a solution containing 5–6% H2O2
and less than 50 ppm silver. Aerosolized droplets
are introduced into an enclosure via a
unidirectional nozzle.
Ultraviolet light devices
Multiple studies have assessed the effectiveness of UV devices to inactivate microbes inoculated onto various test surfaces which are then placed in a typical hospital room [7&
,29&&
,30&&
]. In general, the inoculating doses were more than 4-log10in order to
fully assess the level of inactivation. The most com-monly tested organisms were epidemiologically important healthcare-associated pathogens and included MRSA, VRE,C. difficile, and Acinetobacter
spp. From these studies one can conclude that more than 3-log10vegetative organisms can be killed in
5–25 min by UV, but it requires greater time and
energy to kill a spore-forming organism such asC.
difficile. All studies have reported reduced killing via indirect versus direct line of sight from the UV device. The time needed to inactivate pathogens has been demonstrated to be shortened by use of UV reflective wall paint for multiple different UV-C devices [35,36]. In addition, multiple studies have assessed the effectiveness of UV devices to decon-taminate actual hospital rooms following discharge of a patient colonized or infected with a multidrug-resistant pathogen [7&
,29&&
,30&&
]. Pathogens
eval-uated included MRSA, VRE, Acinetobacter, and C.
difficile. Cycle times for vegetative bacteria ranged
from 10 to 25 min and for C. difficile from 10 to
45 min. In all cases the frequency of positive surface sites post-treatment was less than 11% and in many
cases was less than 1%. The reported log10
reductions were always greater than 2. It is import-ant to understand that the bioburden on contami-nated surfaces in hospital rooms is relatively low and therefore the reduction in frequency of positive surface sites is a better measure of UV effectiveness than the log10reduction.
Hydrogen peroxide systems
The effectiveness of H2O2 vapor systems has been
well studied [7&
,27,37]. Multiple studies have dem-onstrated the ability of H2O2vapor systems to
inac-tivate viruses and bacteria inoculated onto test surfaces. H2O2 vapor systems are capable of
inacti-vating nonenveloped viruses, mycobacteria, and even high numbers of bacterial spores. Further, multiple studies have demonstrated the ability of hydrogen peroxide systems to reduce multi-drug-resistant organisms (MDROs) contaminating surfaces in hospital rooms [7&
,27,29&&
,30&&
]. In the majority of studies, the number of contaminated surfaces was reduced to 0% and in all cases to less than 5%. Of note, none of the studies described
the log10 reduction in pathogens. It is important
to realize that there are key differences in the man-ner in which the various H2O2-based room
disinfec-tion systems generate and deliver their active agent. H2O2vapor systems use heat to generate hydrogen
peroxide vapor (HPV) from 30 to 35% H2O2, while
aerosolized H2O2systems use pressure or ultrasonic
nebulization to generate H2O2from 5 to 6%. These
systems have fundamental differences which result in the H2O2vapor systems having an increased level
of efficacy, homogeneous distribution, and shorter cycle times [27,37,38].
Recent studies assessing the use parameters
and effectiveness of ultraviolet devices and
hydrogen peroxide systems
Hydrogen peroxide vapor has been demonstrated to inactivate key pathogens (i.e., MRSA, VRE, Acineto-bacter) on both porous and nonporous surfaces [39]. Several recent studies have assessed the effect of use parameters on the effectiveness of UV devices. Boyceet al.[40] studied the impact of distance and
orientation using inoculated (MRSA, VRE, C.
diffi-cile) test objects on the effectiveness of a single UV-C device. They concluded that UV-C irradiance, dosage, and antimicrobial effect received from a mobile UV-C device varied substantially based on location in a room relative to the UV-C device.
Cadnum et al. [41] compared UV-C devices and
concluded that variations in test methods can sig-nificantly impact measured reductions in pathogens by UV-C devices during experimental testing. Specifically, they reported that the following factors affected pathogen killing: spreading the inoculum over a larger surface area enhanced killing, orien-tation of the carriers in parallel rather than perpen-dicular enhanced killing, and different types of organic load affecting killing. However, type of carrier, variation in carrier height, and interrupted cycles had no effect on killing.
Few studies have directly compared the effec-tiveness of different ‘no touch’ methods. Nerandzic
et al.[42] compared a UV-C device with a UV light – pulsed xenon (UV-PX) device at manufacturer recommended exposure times and demonstrated that the UV-C device had superior killing of MRSA, VRE, and C. difficile. Increasing distance from the UV-PX device dramatically reduce killing efficacy whereas pathogen concentration, organic load, and
shading did not. Wong et al. [43] compared two
different UV-C devices. Both were effective in killing
MRSA and VRE up to concentrations of 106CFU/ml
when suspended in a isotonic saline. However, one device was approximately seven times more effec-tive in killing MRSA and VRE when they were sus-pended in a protein solution.
CLINICAL TRIALS USING ‘NO TOUCH’
ROOM DECONTAMINATION METHODS
Multiple clinical trials have assessed the efficacy of a UV device or hydrogen peroxide system for terminal room decontamination to reduce HAIs from multi-drug-resistant pathogens (Table 2). Thirteen studies have now demonstrated that the use of a ‘no touch’ device or system reduces the incidence or prevalence of selected MDROs. However, overall the quality of these studies, in general, is poor for the following three reasons: first, most of the studies used a before–after design which is more likely subject to bias than cross-over studies or randomized clinical
trials (however, the use of controls as was done in some studies can reduce the possibility of bias); second, almost all of the studies did not provide a prespecified statistically valid measure of success with a prestudy sample size calculation; and third, most of the studies did not assess potential con-founding that could explain the decrease in multi-drug-resistant pathogens such as hand hygiene compliance and compliance with appropriate sur-face cleaning prior to decontamination. Another limitation to assessing the relative effectiveness of different ‘no touch’ methods is that no study com-pared two different methods. However, the multi-tude of positive studies suggests that ‘no touch’ technologies do indeed decrease HAIs. Further, some studies described below were well designed and assessed potential confounders. Along with the studies listed in Table 2, one before–after study used a UV-PX device nightly in the operating rooms and reported a decrease in surgical site infections for class 1 procedures [57]. The mechanism for this reduction is unclear because the surface environ-ment is not felt to have a substantial impact on the likelihood of surgical site infections.
Several studies warrant detailed discussion, including the studies by Passaretti et al. [53], by Pegueset al.[47], and by Andersonet al.[46]. Passar-etti et al. [53] performed a 30-month prospective cohort (before–after study that was strengthened by the use of concurrent controls) intervention using a HPV device on six high-risk units in a 994-bed
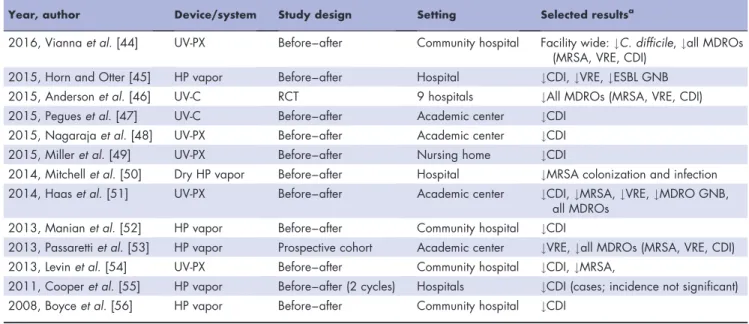
Table 2. Clinical trials of ‘no touch’ methods: UV devices and hydrogen peroxide systems
Year, author Device/system Study design Setting Selected resultsa
2016, Viannaet al.[44] UV-PX Before–after Community hospital Facility wide:#C. difficile,#all MDROs (MRSA, VRE, CDI)
2015, Horn and Otter [45] HP vapor Before–after Hospital #CDI,#VRE,#ESBL GNB 2015, Andersonet al.[46] UV-C RCT 9 hospitals #All MDROs (MRSA, VRE, CDI) 2015, Pegueset al.[47] UV-C Before–after Academic center #CDI
2015, Nagarajaet al.[48] UV-PX Before–after Academic center #CDI 2015, Milleret al.[49] UV-PX Before–after Nursing home #CDI
2014, Mitchellet al.[50] Dry HP vapor Before–after Hospital #MRSA colonization and infection 2014, Haaset al.[51] UV-PX Before–after Academic center #CDI,#MRSA,#VRE,#MDRO GNB,
all MDROs 2013, Manianet al.[52] HP vapor Before–after Community hospital #CDI
2013, Passarettiet al.[53] HP vapor Prospective cohort Academic center #VRE,#all MDROs (MRSA, VRE, CDI) 2013, Levinet al.[54] UV-PX Before–after Community hospital #CDI,#MRSA,
2011, Cooperet al.[55] HP vapor Before–after (2 cycles) Hospitals #CDI (cases; incidence not significant) 2008, Boyceet al.[56] HP vapor Before–after Community hospital #CDI
CDI,Clostridium difficileinfection; ESBL, extended spectrum beta-lactamase producers; GNB, Gram negative bacteria; HP, hydrogen peroxide; MDRO, multidrug-resistant organism; MRSA, methicillin-multidrug-resistantStaphylococcus aureus; UV-C, ultraviolet light – C; UV-PX, ultraviolet light – pulsed xenon; VRE, vancomycin-resistantEnterococcus.
tertiary care hospital. Patients admitted to rooms decontaminated using HPV were 64% less likely to acquire any multidrug-resistant pathogen [inci-dence rate ratio (IRR), 0.36;P<0.001] and 80% less likely to acquire VRE (IRR, 0.20; P<0.001). The risk of acquiringC. difficile, MRSA, and multidrug-resistant Gram-negative bacilli was reduced, but not significantly. The proportion of rooms environ-mentally contaminated with MDROs was reduced significantly on the HPV units (relative risk, 0.65;
P¼0.03).
Pegues et al. [47] performed a prospective
cohort (before–after study) in three haematol-ogy–oncology units to assess the efficacy of
a UV-C device to reduce C. difficile infections
(CDIs). Importantly, rooms were disinfected with bleach prior to use of the UV-C device. A significant association between UV-C use and a decline in CDI incidence was noted on study units (IRR,
0.49; 95% CI, 0.26–0.94;P¼0.03) but not on the
nonstudy units (IRR, 0.63; 95% CI, 0.38–1.06;
P¼0.08). Importantly, hand hygiene compliance,
which was monitored by observation, and room cleaning compliance, which was monitored using ATP bioluminescence, were similar in the baseline and intervention periods (D. Pegues, personal communication).
The study by Anderson et al. [46] is the first
randomized clinical trial to assess a ‘no touch’ method (UV-C, Tru-D) for terminal room disinfec-tion. Specifically this was a prospective, multicenter, cluster-randomized, crossover trial in nine hospitals which evaluated three strategies for enhanced ter-minal room disinfection: standard quaternary ammonium compound plus UV-C, bleach alone, and bleach plus UV-C. Patients colonized or infected with MRSA or VRE, or with CDI were considered ‘seed rooms’ with ‘exposed’ patients being patients subsequently admitted to a ‘seed room.’ Exposed patients were followed for the development of an HAI due to a target pathogen. Compliance with hand hygiene and terminal room cleaning were measured and there were no differences in these potential confounders among the baseline group (quaternary ammonium compound alone) and the three intervention arms. The study showed that enhanced room decontamination strategies (i.e., bleach and/or UV-C decontamination) decreased the clinical incidence of acquisition of target
MDROs (i.e., MRSA, VRE, C. difficile) by �10 to
30% (P¼0.036).
‘No-touch’ room disinfection devices have been used as a component to control healthcare-associ-ated outbreaks [7&
]. The outbreaks involved S. aur-eus, multidrug-resistant Gram-negative bacilli, C. difficile, and Acinetobacter baumannii plus MRSA.
The device used in the great majority of cases was a HPV system.
CHOOSING A ‘NO TOUCH’ DEVICE OR
SYSTEM
Hospitals should use a ‘no touch’ device or system for terminal room decontamination after dis-charge of patients on contact precautions. How-ever, the multitude of commercially available devices and systems makes choosing a specific device or system difficult. UV devices may vary because of differences in UV wavelength, bulb size, energy output, ability to measure energy delivery, and cost. Similarly, hydrogen peroxide systems differ with regard to concentration, use of other microbicides, and method of injecting hydrogen peroxide into a room or space, and cost. For these reasons, infection control professionals should review the peer-reviewed literature and choose for purchase only devices with demonstrated bactericidal capability as assessed by the carrier test method and/or ability to disinfect actual patient rooms. Ultimately, one should choose only devices that have demonstrated the ability to reduce HAIs [7&
].
Further, infection control professionals should be aware of the advantages and disadvantages of both UV and hydrogen peroxide systems (Table 3). Because UV devices and hydrogen peroxide systems will not physically clean a room (e.g., remove dust or stains), room cleaning must precede disinfection. ‘No touch’ systems should be seen as adjunctive methods of room decontamination. A recent modeling study revealed the importance of hand hygiene to reduce HAIs and reported that a 2 : 1 improvement in terminal cleaning compared with hand hygiene was required to match an equal
reduction in acquisition rates [58]. Another
study implemented a three sequential tiered set of interventions: first, fluorescent markers to provide monitoring and feedback on thoroughness of clean-ing; second, addition of a UV-C device for adjunc-tive decontamination of rooms that housed a patient with CDI; and third, enhanced standard disinfection ofC. difficilerooms. During the baseline
period 67% of the C. difficile rooms had positive
cultures after disinfection, whereas with interven-tions 1, 2, and 3, the percentages of rooms with positive cultures after disinfection was reduced to 57, 35, and 7%, respectively [59].
CONCLUSIONS
‘No touch’ technologies have been demonstrated to kill nosocomial pathogens on inoculated test
surfaces, and on actual environmental surfaces and equipment in hospital rooms. Further, more than a dozen clinical trials have now demonstrated that use of one of these technologies can reduce HAIs. Additional well-designed studies (e.g., randomized clinical trials) should be undertaken to assess the degree to which these technologies can reduce HAIs. Studies directly comparing different technologies would be extremely useful. Finally, cost–benefit analyses should be conducted.
Because there are substantial differences
between UV devices and hydrogen peroxide systems and within each technology there are multiple com-mercial choices, healthcare providers should rely on the peer-reviewed literature to validate specific devi-ces and systems prior to purchase.
Acknowledgements
None.
Financial support and sponsorship
This work was supported by the Division of Adult Infec-tious Diseases, University of North Carolina at Chapel Hill, NC and UNC Hospitals, Chapel Hill, North Car-olina.
Conflicts of interest
W.A.R. is a consultant for Clorox and has received honoraria from 3M. D.J.W. is a consultant for Clorox and Germitec. H.K. has no conflicts of interest.
REFERENCES AND RECOMMENDED
READING
Papers of particular interest, published within the annual period of review, have been highlighted as:
& of special interest && of outstanding interest
1. Magill SS, Edwards JR, Bamberg W,et al.Multistate point-prevalence survey of healthcare-associated infections. N Engl J Med 2014; 370:1198–1208.
2. Zimlichman E, Henderson D, Tamir O,et al.Healthcare-associated infections: a meta-analysis of costs and financial impact on the US healthcare system. AMA Intern Med 2013; 173:2039–2046.
3. Weinstein RA. Epidemiology and control of nosocomial infections in adult intensive care units. Am J Med 1991; 91 (Suppl 3B):179S–184S.
4. Otter JA, Yezli S, French GL. The role played by contaminated surfaces in the transmission of nosocomial pathogens. Infect Control Hosp Epidemiol 2011; 32:687–699.
5. Steifel U, Cadnum JL, Eckstein BC,et al.Contamination of hands with methicillin-resistantStaphylococcus aureusafter contact with environmental surfaces and after contact with the skin of colonized patients. Infect Control Hosp Epidemiol 2011; 32:185–187.
6. Morgan DJ, Rogawski E, Thom KA,et al. Transfer of multidrug-resistant bacteria to healthcare workers’ gloves and gowns after patient contact increases with environmental contamination. Crit Care Med 2012; 40:1045–1051.
7.
&
Weber DJ, Rutala WA, Anderson DJ, et al. Effectiveness of UV devices and hydrogen peroxide systems for terminal room decontamina-tion: focus on clinical trials. Am J Infect Control 2016; 44 (5 Suppl):e77– e84.
This paper provided a detailed review of all clinical trials of UV devices and hydrogen peroxide systems that used HAIs as an outcome.
8. Weber DJ, Rutala WA, Miller MM,et al.Role of hospital surfaces in the transmission of emerging health care-associated pathogens: norovirus, Clos-tridium difficile, and Acinetobacter species. Am J Infect Control 2010; 38:S25–S33.
9. Otter JA, Yezli S, Salkeld JAG, French GL. Evidence that contaminated surfaces contribute to the transmission of hospital pathogens and an overview of strategies to address contaminated surfaces in hospital settings. Am J Infect Control 2013; 41:S6–S11.
10. Weber DJ, Anderson DJ, Sexton DJ, Rutala WA. Role of the environment in the transmission ofClostridium difficilein healthcare facilities. Am J Infect Control 2013; 41:S105–S110.
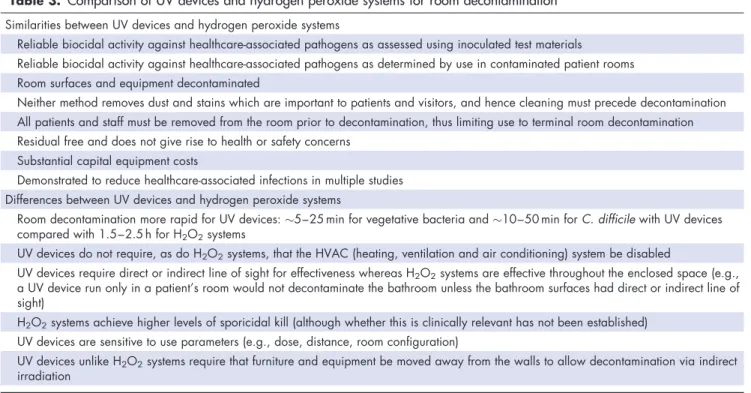
11. Weber DJ, Anderson D, Rutala WA. The role of the surface environment in healthcare-associated infections. Curr Opin Infect Dis 2013; 26:338–344. Table 3. Comparison of UV devices and hydrogen peroxide systems for room decontamination
Similarities between UV devices and hydrogen peroxide systems
Reliable biocidal activity against healthcare-associated pathogens as assessed using inoculated test materials
Reliable biocidal activity against healthcare-associated pathogens as determined by use in contaminated patient rooms Room surfaces and equipment decontaminated
Neither method removes dust and stains which are important to patients and visitors, and hence cleaning must precede decontamination All patients and staff must be removed from the room prior to decontamination, thus limiting use to terminal room decontamination Residual free and does not give rise to health or safety concerns
Substantial capital equipment costs
Demonstrated to reduce healthcare-associated infections in multiple studies Differences between UV devices and hydrogen peroxide systems
Room decontamination more rapid for UV devices:5–25 min for vegetative bacteria and10–50 min forC. difficilewith UV devices compared with 1.5–2.5 h for H2O2systems
UV devices do not require, as do H2O2systems, that the HVAC (heating, ventilation and air conditioning) system be disabled
UV devices require direct or indirect line of sight for effectiveness whereas H2O2systems are effective throughout the enclosed space (e.g., a UV device run only in a patient’s room would not decontaminate the bathroom unless the bathroom surfaces had direct or indirect line of sight)
H2O2systems achieve higher levels of sporicidal kill (although whether this is clinically relevant has not been established) UV devices are sensitive to use parameters (e.g., dose, distance, room configuration)
12.
&
Siani H, Maillard J-Y. Best practice in healthcare environmental decontamina-tion. Eur J Clin Microbiol Infect Dis 2015; 34:1–11.
An excellent review of best practices currently used in healthcare to reduce environmental contamination.
13.
&&
Mitchell BG, Dancer SJ, Anderson M, Dehn E. Risk of organism acquisition from prior room occupants: a systematic review and meta-analysis. J Hosp Infect 2015; 91:211–217.
A comprehensive review of all studies that assessed the risk of being admitted to a room wherein the previous occupant was colonized or infected with a specified multidrug-resistant pathogen. Provides a quantitative assessment of the risk.
14.
&
Otter JA, Donskey C, Yezli S,et al.Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect 2016; 92:235–250. A comprehensive review that describes the frequency and duration of environ-mental contamination by viral pathogens.
15. Bin SY, Heo JY, Song MS,et al.Environmental contamination and viral shedding in MERS patients during MERS-CoV outbreak in South Korea. Clin Infect Dis 2016; 62:755–756.
16. Lerner A, Adler A, Abu-Hanna J, et al. Environmental contamination by carbapenem-resistantEnterobacteriaceae. J Clin Microbiol 2013; 51:177– 181.
17. Weber DJ, Rutala WA, Kanamori H,et al.Carbapenem-resistant Enterobac-teriaceae: frequency of hospital room contamination and survival on various inoculated surfaces. Infect Control Hosp Epidemiol 2015; 36:590–593.
18. Biswas JS, Patel A, Otter JA,et al.Contamination of the hospital environment from potentialClostridium difficileexcretors without active infection. Infect Control Hosp Epidemiol 2015; 36:975–977.
19. Kundrapu S, Sunkesula V, Tomas M, Donskey CJ. Skin and environmental contamination in patients diagnosed withClostridium difficileinfection but not meeting clinical criteria for testing. Infect Control Hosp Epidemiol 2015; 36:1348–1350.
20. Faden HS, Dryja D. Importance of asymptomatic shedding ofClostridium difficilein environmental contamination of a neonatal intensive care unit. Am J Infect Control 2015; 43:887–888.
21. Villamaria FC, Berlanga G, Liao IC,et al.Comparison of environmental MRSA levels on high-touch surfaces in contact isolation and noncontact isolation patient rooms. Infect Control Hosp Epidemiol 2015; 36:1472–1475.
22. Rutala WA, Gergen MF, Sickbert-Bennett EE,et al.Effectiveness of improved hydrogen peroxide in decontaminating privacy curtains contaminated with multidrug-resistant pathogens. Am J Infect Control 2014; 42:426–428.
23. Carling PC, Parry MM, Rupp ME,et al.Improving cleaning of the environment surrounding patients in 36 acute care hospitals. Infect Control Hosp Epide-miol 2008; 29:1035–1041.
24. Carling PC, Parry MF, Bruno-Murtha LA, Dick B. Improving environmental hygiene in 27 intensive care units to decrease multidrug-resistant bacterial transmission. Crit Care Med 2010; 38:1054–1059.
25. Donskey CJ. Does improving surface cleaning and disinfection reduce healthcare-associated infections? Am J Infect Control 2013; 41:S12–S19.
26. Han J, Sullivan N, Leas BF,et al.Cleaning hospital rooms to prevent health care-associated infections: a technical brief. Ann Intern Med 2015; 163:598–607.
27. Otter JA, Yezli S, Perl TM,et al.The role of ‘no-touch’ automated room disinfection systems in infection prevention and control. J Hosp Infect 2013; 83:1–13.
28. Canadian Agency for Drugs and Technologies in Health, Ottawa (ON). Non-manual techniques for room disinfection in healthcare facilities: a review of clinical effectiveness and guidelines [Internet]; 2014 April.
29.
&&
Barbut F. How to eradicateClostridium difficilefrom the environment. J Hosp Infect 2015; 89:287–295.
A comprehensive review of the methods to reduceC. difficilecontamination of the environment. Includes a discussion of the effectiveness of ‘no touch’ methods.
30.
&&
Doll M, Morgan DJ, Anderson D, Bearman G. Touchless technologies for decontamination in the hospital: a review of hydrogen peroxide and UV devices. Curr Infect Dis Rep 2015; 17:498.
A comprehensive review of touchless technologies for decontamination. Includes excellent tables describing the studies that support the use of touchless technol-ogies.
31.
&
Rutala WA, Weber DJ. Disinfection and sterilization in health-care facilities: an overview and current issues. Infect Dis Clinic N Am 2016. [in press] A comprehensive review of disinfection and sterilization in healthcare which includes a detailed discussion of the advantages and disadvantages of UV device and hydrogen peroxide systems.
32. Weber DJ, Rutala WA. Self-disinfecting surfaces: review of current meth-odologies and future prospects. Am J Infect Control 2013; 41 (Suppl):S31– S35.
33. Humphreys H. Self-disinfecting and microbiocide-impregnated surfaces and fabrics: what potential in interrupting the spread of healthcare-associated infection? Clin Infect Dis 2014; 58:848–853.
34.
&&
Muller MP, MacDougall C, Lim M,et al.Antimicrobial surfaces to prevent healthcare-associated infections: a systematic review. J Hosp Infect 2016; 92:7–13.
An up-to-date review of ‘self-disinfecting’ surfaces. Only very limited clinical trial data are available to assess the utility of this technology.
35. Rutala WA, Gergen MF, Tande BM, Weber DJ. Rapid hospital room decon-tamination using ultraviolet (UV) light with a nanostructured UV-reflective wall coating. Infect Control Hosp Epidemiol 2013; 34:527–529.
36. Rutala WA, Gergen MF, Tande BM, Weber DJ. Room decontamination using an ultraviolet-C device with short ultraviolet exposure time. Infect Control Hosp Epidemiol 2014; 35:1070–1072.
37. Fu TY, Gent P, Kumar V. Efficacy, efficiency and safety aspects of hydrogen peroxide vapour and aerosolized hydrogen peroxide room disinfection sys-tems. J Hosp Infect 2012; 80:199–205.
38. Barbut F, Yezli S, Otter JA. Hydrogen peroxide room disinfection: there is no elephant in the room but there’s plenty of evidence in the trunk. J Hosp Infect 2013; 83:353–356.
39. Lemmen S, Scheithauer S, Ha¨fner H,et al.Evaluation of hydrogen peroxide vapor for the inactivation of nosocomial pathogens on porous and nonporous surfaces. Am J Infect Control 2015; 43:82–85.
40. Boyce JM, Farrel PA, Towle D,et al. Impact of room location on UV-C irradiance and UV-C dosage and antimicrobial effect delivered by a mobile UV-C light device. Infect Control Hosp Epidemiol 2016. [Epub ahead of print]
41. Cadnum JL, Tomas ME, Sankar T,et al.Effect of variation in test methods on performance of ultraviolet-C radiation room decontamination. Infect Control Hosp Epidemiol 2016; 37:555–560.
42. Nerandzic MM, Thota P, Sankar CT,et al.Evaluation of a pulsed xenon ultraviolet disinfection system for reduction of healthcare-associated patho-gens in hospital rooms. Infect Control Hosp Epidemiol 2015; 36:192–197.
43. Wong T, Woznow T, Petrie M,et al.Postdischarge decontamination of MRSA, VRE, andClostridium difficileisolation rooms using 2 commercially available automated ultraviolet-C-emitting devices. Am J Infect Control 2016; 44:416– 420.
44. Vianna PG, Dale CR Jr, Simmons S,et al.Impact of pulsed xenon ultraviolet light on hospital-acquired infection rates in a community hospital. Am J Infect Control 2016; 44:299–330.
45. Horn K, Otter JA. Hydrogen peroxide vapor room disinfection and hand hygiene improvements reduceClostridium difficileinfection, methicillin-re-sistantStaphylococcus aureus, vancomycin-resistant enterococci, and ex-tended-spectrumb-lactamase. Am J Infect Control 2015; 43:1354–1356.
46. Anderson DJ, Chen LF, Weber DJ,et al.The BETR-disinfection study. San Diego, CA: IDweek; 2015. [Abstract]
47. Pegues D, Gilmar C, Denno M, Gaynes S. ReducingClostridium difficile
infection among hematology-oncology patients using ultraviolet irradiation for terminal disinfection. In: IDweek; San Diego, CA; 2015[Abstract 1715]
48. Nagaraja A, Visintainer P, Haas JP,et al. Clostridium difficileinfections before and during use of ultraviolet disinfection. Am J Infect Control 2015; 43:940– 945.
49. Miller R, Simmons S, Dale C,et al.Utilization and impact of a pulsed-xenon ultraviolet room disinfection system and multidisciplinary care team on Clos-tridium difficilein a long-term acute care facility. Am J Infect Control 2015; 43:1350–1353.
50. Mitchell BG, Digney W, Locket P, Dancer SJ. Controlling methicillin-resistant
Staphylococcus aureus (MRSA) in a hospital and the role of hydrogen peroxide decontamination: an interrupted time series analysis. BMJ Open 2014; 4:e004522.
51. Haas JP, Menz J, Dusza S, Montecalvo MA. Implementation and impact of ultraviolet environment disinfection in an acute care setting. Am J Infect Control 2014; 42:586–590.
52. Manian FA, Griesnauer S, Bryant A. Implementation of hospital-wide en-hanced terminal cleaning of targeted patient rooms and its impact on endemic
Clostridium difficileinfection rates. Am J Infect Control 2013; 41:537–541.
53. Passaretti CL, Otter JA, Reich NG,et al.An evaluation of environmental decontamination with hydrogen peroxide vapor for reducing the risk of patient acquisition of multidrug-resistant organisms. Clin Infect Dis 2013; 56:27–35.
54. Levin J, Riley LS, Parrish C,et al.The effect of portable pulsed xenon ultraviolet light after terminal cleaning on hospital-associatedClostridium difficile in-fection in a community hospital. Am J Infect Control 2013; 41:746–748.
55. Cooper T, O’Leary M, Yezli S, Otter JA. Impact of environmental decontami-nation using hydrogen peroxide vapour on the incidence of Clostridium difficileinfection in one hospital trust. J Hosp Infect 2011; 78:238–245.
56. Boyce JM, Havill NL, Otter JA,et al.Impact of hydrogen peroxide vapor room decontamination onClostridium difficileenvironmental contamination and transmission in a healthcare setting. Infect Control Hosp Epidemiol 2008; 29:723–729.
57. Catalanotti A, Abbe D, Simmons S, Stibich M. Influence of pulsed-xenon ultraviolet light-based environmental disinfection on surgical site infections. Am J Infect Control 2016. [Epub ahead of print]
58. Barnes SL, Morgan DJ, Harris AD,et al. Preventing the transmission of multidrug-resistant organisms: modeling the relative importance of hand hygiene and environmental cleaning interventions. Infect Control Hosp Epi-demiol 2014; 35:1156–1162.
59. Sitzlar B, Deshpande A, Fertelli D, et al.An environmental disinfection odyssey: evaluation of sequential interventions to improve disinfection of
Clostridium difficileisolation rooms. Infect Control Hosp Epidemiol 2013; 34:459–466.