DIAGNOSIS
AND
TREATMENT
BACTERIAL MENINGITIS
A Symposium
David H. Smith, M.D., David 1. Ingram, M.D., Arnold 1. Smith, M.D., Floyd Gilles, M.D., and M. J. Bresnan, M.D.
Children's Hospital Medical Center and Hamard Medical School, Boston, Massachwdkr 02115
INTRODUCTION
David H. Smith, M. D.
Prior to the introduction of specific anti- bacterial therapy, bacterial meningitis was a disease with a universally fatal or disas- trous outcome. The introduction of type- specific antiserum, and then of the an- tibacterial drugs, improved this situation dramatically.
Improvements in the general medical care of acutely ill children, and the intro- duction of a series of more potent antibi- otics against its bacterial causes helped to generate an attitude that bacterial men- ingitis was, or soon would be, a disease of the past. The experience of the past two
decades belies this thesis. Today, interest in many facets of this disease has been re- newed by many physicians concerned
with
the health of children: the epidemiology, pathophysiology, diagnosis, and treatment. This symposium attempts to summarize for the practitioner the highlights of currentknowledge in this area, and to outline cer- tain areas in which recent advances can be anticipated, or will be studied.
Tuberculous meningitis will be omitted for the sake of brevity, as will the special problems of meningitis in the newborn infant.
I.
THE EPIDEMIOLOGY
OF
MENINGITIS IN CHILDREN
David 1. Ingram, M.D.
There has been a resurgence of interest in developing vaccines to prevent Hemo-
philw injluenzae
b, pneurnococcal, and meningococcal Group A,B,
and C men- ingitis. These organisms cause almost all the bacterial meningitis after the first two months of life. If, as now seems possible, vaccines against most or all of these or- ganisms will soon become available, those children having the greatest risk must bedefined to determine who, and at what age should have priority in receiving the vaccine(s).
A. THE CURRENT MAGNITUDE OF THE PROBLEM
The Center for Disease Control estimates that, in the United States, there are 29,000
cases of H.
injluenzae
b, 4,800 cases of pneumococcal meningitis, and 4,600 casesPresented by members of the staff of the Children's Hospital Medical Center to the New England Pediatric Society, October 4, 1972.
ADDRESS FOR REPRINTS: (A.L.S.) Children's Hospital Medical Center, Boston, Massachusetts 02115.
BACTERIAL MENINGITIS
I
MENINGITIS DUE-
TOH. influenzae type b
I , 8 ,
40- , ,
I ,
I , I t
I I I , I #
# ,
I I
I I 30- j j
V)
W
V)
a
0 C . H . PITTSBURGH
TOTAL ADMISSION 1945 5000 1950 5500 1960 6000 1970 8500
0 1 I I 1 I I
1945 1950 1955 1960 1965 1970
YEAR
FIG. 1. Yearly admission for iduenzal, pneumococcal, and meningococcal meningitis as compared to total admissions, as calculated from Michaels'.
of meningococcal meningitis per year.' The risk of a child developing H. influenzae meningitis in the first five years of life varies between one chance in 400 and one in 2,000. In Pittsburgh, a tenfold increase in the number of admissions to the Chil- dren's Hospital for H. influenzae meningitis has occurred since 1945, while the total number of admissions increased less than twofold. During this same period, the in- cidence of pneumococcal meningitis has remained unchanged, and the incidence of meningococcal meningitis has declined
(Fig.
The age of greatest risk for bacterial meningitis is 6 to 12 months, with 90% of cases occurring between 1 month to
5
years of age.3pi At the Children's Hospital Medi- cal Center in Boston, and in Mecklenburg County, North C a r ~ l i n a , ~ the age distribu- tion of meningitis had not changed during the past 40 years, suggesting no change in the development of immunity to H. influ- enzue bS or carriage rate of meningitis organisms.Current estimates of the mortality rate in children with H. influenzae b meningitis were
4.7%
in Mecklenburg County, NorthCarolina between 1966 and 1970. The mor- tality rate between 1961 and 1971 in Charles- ton County, South Carolina was 14% for H. influenzae; 7% for meningococcal, and 36%
for pneumococcal meningiti~.~
B. LONG-TERM SEQUELAE OF H. INFLUENZAE MENINGITIS
In 1971, 86 Tennessee children who had meningitis between 1950 and 1964 and were adequately treated by cuqent stan- dards, were evaluated by Sell et
aL5;
11 had died, eight during therapy. Of the re- maining 75, 35% had significant central nervous system damage; 16% had possible CNS damage, and only 4% fell into the normal range on extensive psychological t e ~ t i n g . ~ If these and other data6 are extra- polated to the 29,000 cases of H. inflwnzue meningitis occurring annually in the U.S.,lDIAGNOSIS AND TREATMENT 588
Up to 80% of children will carry nonen- capsulated H. influenzae at some time or other; however, only a small percent will carry the virulent encapsulated organism. In an English investigation7 of serial throat cultures in families, 3.2% of children less than 5 years old, 0.8% of older children and 0.4% of adults carried H. influenzae type b at any one time. In a nursery of 0 to 1-year-olds in British West Indies, 45% car- ried H. influenzae type b for a few months, without any clinical d i s e a ~ e , ~ while in a Connecticut study of three families, four out of five siblings of a child with meningitis carried
H.
influenzae b, while the organism was not isolated from any of the parents.% Thus, carriage of the virulent b organism is predominantly in the susceptible age group, and higher in those in contact with children with H. influenzae b disease.In Charleston County, South Carolina, the incidence of H. influenme meningitis was three and one-half-fold greater in blacks than in whites, but appeared to be related to poverty, more than to race. In whites, the incidence was greater in rural areas than in urban areas, but there was no increased incidence in overcrowded households. It was postulated that the increased incidence of meningitis in blacks and rural whites was probably related to lack of access to early medical care to prevent complications of H. influenzae b otitis medias4 Only 4% of otitis media is caused by type b organism^,^ but of patients with such otitis, 14% develop
H.
influenzae meningitis.C. MENINGOCOCCAL MENINGITIS Groups B and C are the common causes of meningococcal meningitis in the U.S., with a carriage rate of 1% to 10% of the gen- eral population. Unlike the situation with H. influenzae b, meningococcal carriers tend to be over 21 years of age, harbor the organism for many months, and display slow spread among family members. In an outbreak of group B meningococcal men-
ingitis in three first cousins during a 6- month period, Greenfield and Feldmanlo found a carriage rate of the same organism in 44% of the extended family; 50% in family members in contact with the patients; 29% in friends and neighbors, and 3% in noncon- tact community controls. The estimated likelihood of severe meningococcal disease in family contacts usually occumng almost simultaneously with the first case," is about 1%. As with H , influenzae b, no correlation has been found between meningococcal meningitis and crowding within house- holds, but the disease occurred only in ur- ban areas of Charleston County, South Carolina. Thus, meningococcal meningitis in the civilian population currently is a disease of young children exposed to chronic adult carriers, usually in the same family.
D. PNEUMOCOCCAL MENINGITIS Of the 89 sero-types of pneumococci, types 1, 6, 14, 18, 19, and 23 are the most common causes of sepsis and otitis media, and probably meningitis and pneumonia in children.'* The risk of pnuemococcal meningitis is 5.5-fold in blacks as compared to whites, and is independent of income, population density and ~ r o w d i n g . ~ Eleven percent of blacks with pneumococcal men- ingitis had sickle cell disease; if generally true, this indicates that one in every 27 children with sickle cell disease may de- velop pneurnococcal meningitis by the age of 4 years4; an incidence 36-fold greater than in normal blacks, and 314-fold greater than in white children.
SUMMARY
ARTICLES
II. DIAGNOSIS OF BACTERIAL MENINGITIS
Arnold 1. Smith, M.D.
A. GENERAL CONSIDERATIONS LEADING TO SPECIFIC DIAGNOSIS
The approach to the diagnosis of bac- terial meningitis is based on the detection of microorganisms in the subarachnoid space, or the observation of the host response to the infection. Fever and lassi- tude, the nonspecific host responses char- acteristic of the young infant, should bring to mind the diagnosis of bacterial menin- gitis. Table I depicts a compilation of signs and symptoms in infants ultimately proven to have meningitis. The most consistent complaints presented are fever and altered function of the central nervous system, which can be as striking as seizures, or as unimpressive as drowsiness and lethargy. The data in Table I suggest that there should be no reluctance to perform a lum- bar puncture readily, on the assumption that the benefits to be gained far outweigh the potential harm of the procedure. This assumption is supported in part by the observation that the puncture-related com- plication rate in a group of children treated for tuberculous meningitis with repeated intrathecal administration of streptomycin was six children during a 12-year period. Unfortunately, there is no denominator from which to calculate incidence, but the authors,13 as well as others14 relate the com- plication to the use of unstyletted needles. In our emergency room, we are aware of no complications, whereas approximately 3.3%
of all lumbar punctures allow a diagnosis of bacterial meningitis. With such an ac- ceptable risk-benefit ratio, lumbar punc- tures are performed without hesitation in our institution.
B. EXAMINATION OF CEREBROSPINAL FLUID
1. Detection of Bacteria
(H.
influenzae, Pneumococcus, and Meningococcus)amined by detecting microorganisms or observing the host's response to the invad- ing bacteria. The classic method of bacteria detection uses a gram stain of the CSF. When this stain is made on fluid containing 10j bacteria per milliliter, there will be, on the average, one organism per oil immer- sion field. Since disease may occur at organism densities lower than this, the efficacy of this test improves through maneuvers which increase the organism concentration. Centrifuging the CSF and staining the pellet are the simplest of these; however, H. influenzae requires a force of 10,000 x g for ten minutes in order to sedi- ment. With the standard clinical laboratory centrifuge, which develops a maximum of 1,000 x g, 60 minutes of centrifugation may be necessary.
The current definitive procedure for the detection of bacteria in CSF, growth of the organism in culture, depends upon sev- eral factors, namely, that the organisms be alive in the CSF, that they not be killed in transit, and that the culture medium be able to support growth. Differentiation of bacteria in the laboratory depends on spe- cific differences in the metabolism of the
TABLE I
SIGNS AND SYMPTOMS OF BACTERIAL ~ ~ E N ~ N C ~ T ~ S
Presenting Complaints
Fever Vomiting Irritability Listlessness Convulsions Headache Stiff neck Anorexia
Rash
Total in study Reference
BACTERIAL MENINGITIS
various pathogenic bacteria. Because of dif- ferences in their biosynthetic ability, some pathogens require intracellular metabolites for growth (i.e., NAD+ for H , influenme). Yet, differences in their catabolic capabili- ties form the basis for the commonly used fermentation tests. An extension of this concept will test the CSF directly for bacterium specific metabolic properties or metabolites, e.g., the use of imniunoelectro- phoresis to detect bacterial antigens. This method produces a false-negative rate (in culture-positive cases ) of 10%,15s l 6 lower
than the false-negative rate of 19% in the interpretation of gram stains.17
2. Detection of Bacterial Products
Antigen detection has the main advan- tage of not requiring living or even intact bacteria: this factor makes the test particu- larly valuable in cases where the admin- istration of broad-spectrum antibiotics may alter the expected CSF findings. An analo- gous approach, yet to be explored, detects bacterial specific enzymes in the CSF. These large protein molecules are specific by definition, and may not leave the CSF immediately, because of their large size.
3. Host Inflammatory Response
The basic premise used to detect host response to bacterial invasion assumes that the response is inflammatory-a situation which makes diagnosis extremely difficult in the leukopenic patient. The factor most commonly used as an index for inflammation of the leptomeninges is the presence of leukocytes in the CSF. The total number of leukocytes in the CSF in bacterial menin- gitis ranges from 200 to 20,00O/cu mm. The majority (greater than 50%) are acute inflammatory cells, namely, polymorpho- nuclear leukocytes. The distinction between leukocytes must be made with an appropri- ate stain (methylene blue or Wright's). It should be remembered that the spectrum of response occurring in aseptic meningitis may overlap with that of a bacterial menin- gitis. In this instance, the diagnosis of pyogenic meningitis rests on the demon- stration of the existing, or recently past
presence of bacteria. However, when the diagnosis is unknown at the initial time the child is presented, there are two courses of action. One of these is to treat the child as if bacterial meningitis is present, with- out waiting for the results of the culture. This course assumes that transportation and subsequent cultivation of the micro- organism have been without error and that the specific cause will, in a few days, be demonstrated. But this is not always the case; a situation can occur where the child has dramatically improved, following the institution of parenteral antibiotic therapy, yet 48 hours later all cultures appear sterile. At that time, we have to weigh the prob- ability of existing bacterial meningitis missed by the usual diagnostic tests, versus the risk imposed by hospitalization and parenteral administration of antibiotics for seven to ten days. This risk ratio defies generalization, as it depends on many fac- tors, from the expertise of bacteriology technicians to the prevailing nursing prac- tices. The often recommended other course of action is to perform serial CSF examina- tions at six-hour intervals without admin- istering antibiotics.
591
BACTERIAL MENINGITISsixth dayls or even the second week1" of illness.
Disruption of the continuity of the blood- CSF barrier is another consequence of the inflammatory response. An increase in the CSF protein content provides the most common indication of this disruption. Since subclassification shows the spinal fluid pro- tein in meningitis to mirror the plasma pro- tein, this remains the least informative of the
CSF
indicators of bacterial meningitis.4. Noninflamrnatory Host Response
One of the oldest CSF indices of bac- terial meningitis, a lowered CSF:blood glucose ratio, is probably one of the least understood. A cellular inflammatory re- sponse can lower the CSF glucose content in the absence of bacteria. In addition, CSF glucose concentration can decrease sec- ondary to irradiation of the head (with body shielded), or heatstroke, or pyogenic meningitis in aplastic animals. This sug- gests that either the decrease in CSF glu- cose concentration is independent of the cellular inflammatory process, or is the result of the early vascular changes in the inflammation. Available data indicate that the lowered CSF glucose content is due to
a change in the metabolic properties of the central nervous system. This metabolic change can result, conceivably, from micro- organism "toxins" acting at a subcellular level. Toxin-induced metabolic damage can act at one of the several levels of cellular organization. Present data suggest that sev- eral factors operate, yet the quantitative contribution of each remains indefinite. Interference of glucose transport from blood to brain is probably one of the opera- tive factors in decreased glucose flow from the brain to the CSF. However, an in- creased CSF lactate content probably re- flects increased lactate production by CNS tissue involved in meningitis.20121 This in- tensified production may alter cerebral metabolism over and above that due to distorted glucose transport. Increased CSF lactate content does not occur in aseptic meningitis, but is of limited clinical useful- ness because of techniques necessary in handling the samples. Although determina- tion of the CSF lactate concentration might prove most valuable in distinguishing a partially treated bacterial from a viral meningitis, because of an insdlicient data base, it currently offers no more than the determination of the CSF glucose concen- tration.
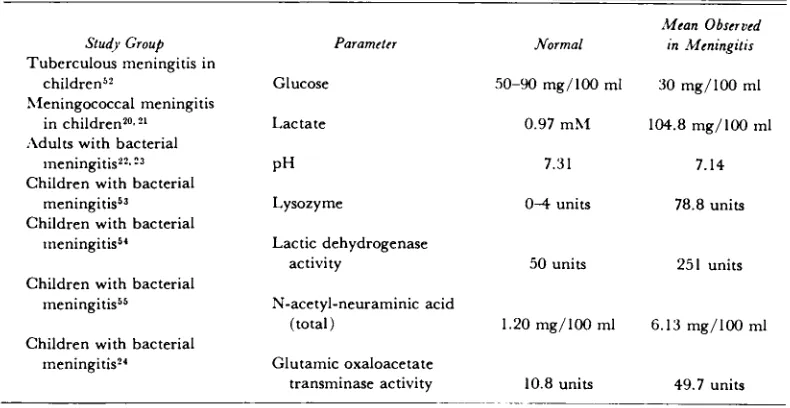
TABLE I1
NONINFLAMMATORY CSF RESPONSES TO BACTERIAL MENINGITIS
Study Group
Tuberculous meningitis in children5?
~leningococcal meningitis in ~ h i l d r e n ? ~ , ? ~ ;\dults with bacterial
~ n e n i n g i t i s ~ ? . ~ ~ Children with bacterial
r n e n i n g i t i ~ ~ ~ Children with bacterial
~neningitis~'
Children with bacterial ~ n e n i n g i t i s ~ ~
Children with bacterial meningitis?'
Parameter
LMcon Observed Normal in Menin,eifis
Glucose 50-90 rng/100 ml 30 rng/100 rnl
Lactate 0.97 m?rf 104.8 rng/100 ml
Lysozyme 0 4 units 78.8 units
Lactic dehydrogenase
activity 50 units 251 units
N-acetyl-neuraminic acid
(total) 1.20 rng/100 rnl 6.13 rng/100 ml
Glutarnic oxaloacetate
DIAGNOSIS
AND
TREATMENT592
An increase in
CSF
lactic acid concentra- tion can lower theCSF
pH when it exceedsCSF
buffering capacity, and this does occur in bacterial meningitis, and tends to cor- relate with theCNS
symptom^.^^^^^ But, again, it adds little information to that already conventionally obtained, whereas determination ofCSF
pH requires an an- aerobic sample obtained in a respiratory steady state.Like the measurement of lactate,
CSF
pH might also be helpful in distinguish- ing partially treated bacterial from viral meningitis, yet no experience exists to confirm this suggestion. More notably, perhaps the magnitude and duration of the depressed
CSF
pH may be of prognostic significance by reflecting quan- titatively the degree to which meningitis affects the metabolism of the developing brain. Tbis infers that if the brain remains metabolically abnormal for a long periodof time, normal growth and development will be disturbed, and subsequent function will be abnormal. Table I1 summarizes some metabolic changes observed in
CSF
in bacterial meningitis.
Along this line of reasoning, one may look for other evidence in the
CSF
of altered metabolism in cerebral cellular elements. This premise suggests that meta- bolically abnormal cerebral tissue will be less likely to develop into tissue with normal function. In this regard,CSF
glu- tamic oxaloacetic transaminase (GOT) has been found to aid in the identification of potentially fatal outcome in m e n i n g i t i ~ . ~ ~ The source of this enzyme is probably cerebral tissue with some blood contribu- tion. As might be expected, elevation in CSF GOT is associated with stormy clinical illness and death, with the symptoms ex- plicable on the basis of vascular thrombosis and cerebral necrosis (Table 11).Ill. MORBID ANATOMICAL CHANGES
Floyd Gilles, M.D.
The bacterial mode of access to the sub- arachnoid space is a source of concern to the physician. Does the child have a bac- teremia from a distant cryptogenic source, which spreads to his leptomeninges? Or, is there a direct route to the leptomeninges from a parameningeal site such as the ear or paranasal sinus? Is there a direct pas- sage from skin to leptomeninges via a con- genital dermal sinus tract, such as those in the midline of the vertebral column or the head (or, less frequently, via a congenital defect in the central nervous system cover- ings around the middle ear or along the cribiform plate)?
CNS
dysfunction encountered by the clinician during leptomeningitis falls into several categories: seizures, changes in consciousness, elevation of intracranial pressure, focal and/or symmetrical upper motor neuron deficits, asymmetrical upper motor neuron deficits, lower motor deficits(i.e., cranial nerve palsies), hydrocephalus, deficits associated with herniation, and unsuspected complications of therapy.
BACTERIAL MENINGITIS
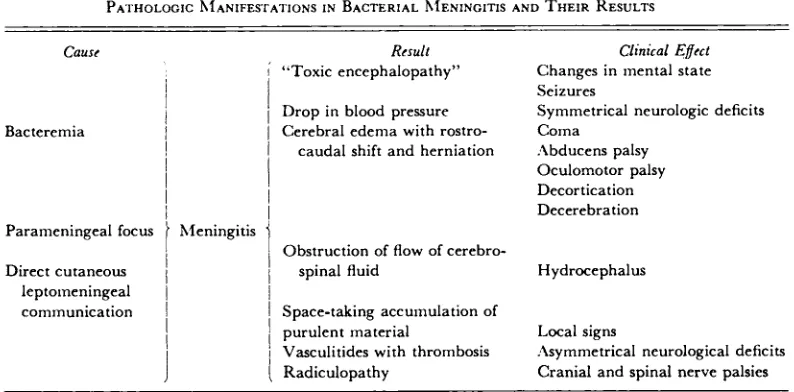
TABLE 111
PATHOLOGIC ~ I A N I F E S ~ A T I O N S I N BACTERIAL ~ ~ E N I N G I T I S A N D THEIR RESULTS
Cause Result Clinical Effect
I "Toxic encephalopathy" Changes in mental state
I
I
1
Drop in blood pressure Seizures Symmetrical neurologic deficitsBacteremia 1 / Cerebral edema with rostro- Coma
1 caudal shift and herniation .\bducens palsy
I
1
1
Oculomotor palsy! Decortication
1 1 Decerebration
Parameningeal focus
1
hfeningitisI Obstruction of flow of cerebro-
Direct cutaneous 1
1
spinal fluid Hydrocephalus lepto~neningeal I 1communication I I Space-taking accu~nulation of
1
1
purulent material Local signsI
Vasculitides with thrombosis Radiculopathy :\symmetrical neurological deficits Cranial and spinal nerve palsiesThe child with leptomeningitis and vas- effects produce a caudal shift of midline culitis in and around the medulla is sus- structures, with their entrapment in the ceptible to cardiovascular instability. With tentorial notch or foramen magnum and failure of adequate perfusion pressure, or concomitant herniation of parahippocampal with sudden transient cessation of cardiac gyri and/or cerebellum. This shift results function, flow first ceases in arteries and in dramatic and ominous changes in con- arterioles farthest from the heart and with sciousness or postual reflexes (decortica- the restoration of normal perfusion pres- tion or decerebration). Caudal shift of the sure, the last region to be relieved of stasis brain stem results in palsy of the abducens is the same vascular bed. Multiple sym- nerve, secondary to its stretching between metrical or bilateral necroses occurring the point of penetration of arachnoid, and simultaneously within the brain, usually its point of dural penetration via Dorello's result from a deficit in systemic perfusion, canal. Palsy of the oculomotor nerve can or a defect in drainage from a functional occur by stretching or by direct compres- occlusion of one or more of the great sion by parahippocampal gyri.
sinuses, such as that occurring with sinus Acute ventricular dilatation correlates thrombosis. Frequently following hypoper- with obstruction of cerebrospinal fluid cir- fusion, isocortical lesions, more or less sym- culation by thick, inflammatory exudate in metrical in topography and in size, are the aqueduct; at the outlets of the fourth encountered in the region of the terminal ventricle, or in the leptomeningeal spaces. portions of the anterior, middle, and pos- No cases of postmeningitic hydrocephalus terior cerebral arteries, primarily in the have been related to obstruction of the parietal and occipital lobes. The cerebellum, Pacchionian granulations alone.
ilarly involved.
C
DIAGNOSIS AND TREATMENT 594 lent material may loculate in the ventricles
and function as a mass lesion, and/or con- tinually seed the leptomeninges. Such ac- cumulations can arise by direct extension from the leptomeninges via the choroid fissure to the choroid plexus, or may be the result of direct seeding of the choroid plexus during bacteremia. Once in the ven- tricular system, organisms may be ex- tremely hard to eliminate, short of the use of direct drainage.
Overt vasculitis further complicates lep- tomeningitis. Large numbers of inflamma- tory cells may accumulate between the endothelium and internal elastic lamina of small arteries and arterioles, to the point of obliteration of the lumen.
I n other cases, direct invasion of blood vessel walls by organisms can produce ne- crosis, inflammation, and thrombosis. Prop-
agation of the thrombus results in exten- sion of the necrosis.
Inflammation and necrosis occur within cranial and spinal rootlets traversing the exudate-filled leptomeninges, and consti- tute the basis for the radiculopathy fre- quently associated with leptomeningitis.
Although the pia of the leptomeninges is usually relatively resistant to direct in- vasion by micro-organisms, bacterial sub- stances must diffuse across that mem- brane, for subpial astrocytosis is frequently encountered in children surviving more than a few days. Rarely, however, transpial invasion by bacteria occurs, and is accom- panied by a local cerebritis.
This pathogenetic sequence was synthe- sized from the postmortem material avail- able at the Children's Hospital Medical Center and the l i t e r a t ~ r e . ~ j - * ~
IV. NEUROLOGICAL ASPECTS: THEIR
DIAGNOSIS AND TREATMENT
M. J. Bresnan, M.D.
The comments made here apply to meningitis in general, although it should be noted that meningococcal meningitis has a lower complication rate in all series, and H. influenzae and pneumococcal men- ingitis seem to have comparable compli- cation rates. H. influenzae dominates most series because of its frequency in child- hood.l7, 29
A. SEIZURES
Seizures occur in up to 30% of cases and a r e most common in meningitis due to H. infEuenzae. Three basic kinds of seizures can be recognized: ( 1 ) In- termixed focal and generalized seizures of short duration and low frequency, are usually not a clinical problem, therefore, overmedication should be avoided. Because such seizures may have a metabolic basis, a careful watch should focus on electrolyte and, especially, water balance. ( 2 ) Recur-
rent and prolonged seizures of varying focality are very difficult to control, and have a poor prognosis. ( 3 ) Focal recurrent seizures should bring to mind the possible complication of subdural effusion, or venous or arterial thrombosis with infarction.
The first consideration in treating seizures should be the maintenance of a clear air- way, administration of oxygen, suction, aids to metabolic homeostasis (especially correction of respiratory acidosis), and, pri- marily, maintenance of blood pressure. The following drugs are of acute value: ( 1) Di- azepam (Valium), 1 mg per year of age intravenously to a maximum of 10 mg, given as a bolus. (Supplied as 10 mg in
595
BACTERIAL MENINGITISmglkg intravenously over 30 minutes (less than 25 mumin; less than
1
gm per dose.)(4)
Paraldehyde,0.3
ml/kg, per rectum.Avoid short-acting barbiturates, e.g., sodium amytal, and repeated combinations of diazepam and phenobarbital, because of the dangers of acute respiratory depression or cardiac arrest. Because large doses of diphenylhydantoin intravenously can pro- duce hypotension, blood pressure must be monitored.
Basic maintenance doses are, phenobar- bital,
5
mg/kg/day and, dilantin, 6 mg/ kg/day, but higher dosages ( u p to double) may be necessary for short pe- riods. These medications can be gradu- ally reduced and abandoned over several days after the acute phase of the illness if EEGs do not show seizure discharges; clinical seizures are not present, and there are no gross neurological residua. If these criteria are not met, longer term anticon- vulsants are indicated.B. CEREBRAL EDEMA
Brain swelling is believed to contribute to the obtundation and coma so typical of meningitis. In all series, as with most neu- rological illnesses, the deeper the coma, the poorer the prognosis. Despite the presence of increased intracranial pressure, papilledema is unusual and, if found, focal complications should be searched for, such as abscess or subdural efision. In uncom- plicated cases, CSF pressures return to normal in 48 hours. Sixth nerve palsies, a frequent accompaniment of pressure, are not of localizing value, and should not pre- clude lumbar puncture. However, even though lumbar puncture is essential, and rarely causes problems, it is advisable to remove as little fluid as is necessary.
Corticosteroids are standard treatment for cerebral edema, and have been used in meningitis, but it is unclear whether they were used to treat edema or to counter inflammation. Interestingly, prednisolone seems i n e f f e ~ t i v e , ~ ~ while dexamethasone (Decadron), the current choice of most
neurologists for edema, appeared to lower the complication rate in one series3' The authors discount this, as their control group seemed more critically ill and had higher concentrations of spinal fluid glutamic oxaloacetic transaminase. The dose used in that study was lower than the usual to con- trol cerebral edema. In the context of ade- quate antibiotics, steroids do not seem to increase the complication rate significantly yet they have not seemed of sufEcient value to have a place in the routine treatment of meningitis.
If used, the dose of dexamethasone is
2 to 4 mg intravenously, followed by 1 to
2 mg every six hours, depending on the size of the patient. Mannitol can be used for acute focal edema, but its action is shortlived, and its effect on fluid balance complicated.
The
dose is1.5
to2
gmlkg in- travenously over10
to15
minutes. Glycerol is a safer, easier agent to use and must be given by mouth. It is useful for main- tenance, as it does not seem to have a rebound effect. Glycerol dosage is 1 to2
gm/kg every four to six hours by naso- gastric tube in all obtunded patients.
C. FOCAL NEUROLOGICAL COMPLICATIONS
1. Subduml Effusion
In the past 20 years, pediatricians have recognized the need for searching for sub- dural effusions during the course of men- ingitis. Frequently, persistent or recurrent fever has been used as an indication for the performance of subdural taps, but this indi- cation is questionable. More important signs seem to be persistent lethargy, coma, increasing head size, or an area of trans- illumination in infants. Persistent focal seizures also suggest effusions, and may remit with tapping. The incidence of such effusions in some series of meningitis in children has been as high as %.* This frequency is related to the diligence
O Dr. McKay has commented that the 50% inci-
DIAGNOSIS AND TREATMENT 596
of the physician, and the age of the pa- tients being most common in infants under 18 months of age, when such taps are easily performed. Despite this high incidence, only 10% to
15%
of effusions are sympto- matic.If symptomatic, treatment consists of re- moving 15 to 20 ml per side per day until dry. Persistent, large collections of two to three weeks' duration are usually associated with neurological sequelae related to in- trinsic disease of the underlying hemi- sphere. There is some suggestions that stripping of membranes may improve the p r o g n o s i ~ . ~ ~
2. Subdural Empyema
True empyema, i.e., pus, as opposed to infected effusion, is very rare. Although empyema is associated with the same signs as significant subdural effusion, it correlates with hectic fever. There are usually predis- posing factors to empyema in conjunction with meningitis, especially sinusitis and otitis. In suspicious cases, skull x-rays prove valuable. The treatment is surgical evalua- tion ( usually debridement ) , and prolonged administration of antibiotic^.^'. 3 5
3. Arteritis
Neuropathologists have noted the pres- ence of arteritis in all varieties of meningitis for many years. Although related to basillar inflammation in general, it affects arteries of varying sizes. Recently, arteritis has commanded increasing attention as a pos- sible cause of neurological complications, and because of improved possibilities for its clinical demonstration. This is best done by angiography, which in careful hands, is associated with a very low morbidity.36 Clinically, these children usually will have a hemiparesis, associated in many cases with a hemianopsia, findings distinctly un- usual with uncomplicated subdural collec- tions. Persistent focal seizures are present as well. No data on treatment are available. Maintenance of blood pressure, and, thereby, cerebral perfusion pressure, seems important.
4. Venous Thrombosis (Phlebitis)
Venous occlusion as a complication of meningitis seems to be less common than formerly, not only because of antibiotics and their earlier use, but also due to careful fluid management and the prevention of dehydration. The signs are usually in- tractable focal seizures with a hemiparesis, often involving the arm more than the leg. The appearance of significant numbers of red blood cells in the CSF may announce such a thrombosis, because of the associ- ated hemorrhagic infarction. There is no specific treatment.
5. Abscess
Abscesses occupying a large space are very rare. Their appearance resembles that of subdural empyema secondary to a parameningeal focus, such as otitis, mas- toiditis, sinusitis, and osteomyelitis. Clinic- ally, late focal signs and increased intra- cranial pressure appear, and may be asso- ciated with papilledema. Positive Techne- tium 99 brain scans and focal delta rever- sals on EEG prove especially helpful in early diagnosis. Treatment consists of sur- gical evacuation and prolonged antibiotics.
D. LATE COMPLICATIONS AND SEQUELAESp6
597
BACTERIAL MENINGITISIQ's compared to siblings, occur in up to Obviously, long-term follow-up of chil- 20% of "normal" survivors. These may or dren who have recovered from meningitis may not have an abnormal
EEG,
which, in is important, even in those children who turn, may or may not be associated with seem to have made a successful recov- s e i z u r e ~ . ~ ~ 3EV.
TREATMENT OF BACTERIAL MENINGITIS: ANTIMICROBIAL
AND GENERAL
Arnold 1. Smith, M.D.
The fundamental goal of therapy is to permit normal growth and development of the child. This goal needs to be reaffirmed because the achievement of a low mortality rate by increasing the number of survivors has also increased the number of damaged children. Preservation of life is certainly the first and most dramatic step in allowing the infant to achieve his potential, yet we have not begun to realize a reduction in
the long-term morbidity of this d i ~ e a s e . ~ ~ ~ ~ Treatment, like the approach to diagnosis,
can consider two areas: removing the or- ganisms ( H. influenza, pneumococcus and meningococcus in "simple" meningitis of infancy) and aiding the host.
A. ANTIMICROBIAL THERAPY
Clearance of the organism from the sub- arachnoid space is considered of prime im- portance in therapy, as the presence of organisms in that anatomic location is the "first cause" in the sequence of pathophysi- ological events. Net microorganism removal depends upon the clearance rate being greater than the rate of multiplication. Antibiotics "clear the infection" by decreas- ing or stopping the rate of bacterial growth. The host then removes the microorganisms, and organizes the inflammatory exudate. For antibiotics to perform efficiently, they must come into contact with the bacterium. This apparently over simplified statement is of prime importance, due to the special na- hue of the CNS, behind its "blood-brain bar- rier." Penetration of antibiotics through this banier varies with each antimicrobial agent,
as well as with the integrity of the barrier. For example, ampicillin, the current agent of choice, achieves a CSF concentration which is 30% of the simultaneous blood con- centration, early in the course of the men- ingitis. Later, as the inflammatory responses subside, the concentration in the CSF may, somewhat surprisingly, fall to
5%
of that in blood (Table IV). Such a dramatic fall might easily reduce the CSF antibiotic con- centration to less than that which is anti- bacterial: a phenomenon which may operate in cases reported as ampicillin failures. The pragmatic solution to the problem has been to increase the ampicillin dosage, a process which has now reached the current prac- tice of administering ampicillin intraven- ously at a dosage of 400 mg/kg/day (an approach tolerated because of the large ratio of efficacy to toxicity). This mega dosage schedule focuses on keeping ampi- cillin present at a concentration which will'TABLE IV
Number of
Study Patients 'Mean Percent of Serum Concentration
56 5 Day I W.O%
Day 3 39.2%
Day 6 27.7%
Day 9 12.2%
5 7 20 Day 1-4 10.97,
5 8 5 Day-unstated 4.7%
59 34 Day &3 35.7%
Day 4-9 32.8Tc
DIAGNOSIS AND TREATMENT 598 neutralize, if not kill, the last microorgan-
ism liberated from the fibrinous exudate, as it is debrided by the resolving inflamma- tory process. Cessation of antibiotic therapy before eliminating the last organism risks the proliferation of microorganisms faster than their clearance and the resultant re- currence of clinical disease. Thus, the dura- tion of antibiotic therapy, even in our current mega dosages, proves important to ultimate outcome. We continue therapy until the patient is afebrile for five days. If at that time, the spinal fluid contains 50 or less mononuclear leukocytes per cubic mil- limeter, and the protein concentration less than 50 mg/100 ml, antibiotic therapy is discontinued. In most infants, this means 10 to 14 days of antibiotic therapy. Conse- quently, the last few days of antibiotic treatment are the most critical when one uses antimicrobials of the penicillin class, because of the increasing blood-brain bar- rier. In other words, as the child improves, more effort should be devoted to making sure that appropriate blood levels of ampi- cillin are present: a recommendation op- posite that of the neurotic habit of "tapering antibiotics."
Many problems in delivery of penicillin- type antimicrobials to the subarachnoid space are obviated by the use of chloram- phenicol, a bacteriostatic agent which at- tains a significant CSF concentration re- gardless of the degree of meningeal inflam- m a t i ~ n . ~ ~ ? ~ ~ Although there are no con- trolled studies of comparison of ampicillin and chloramphenicol, it is noteworthy that most cases of "ampicillin failure" have responded to c h l ~ r a m p h e n i c o l . ~ ~ - ~ ~ The rationale for the common use of am- picillin lies in its freedom from toxicity, as opposed to the hematologic toxicity accom- panying the use of chloramphenicol. How- ever, the benefits of lower toxicity accrued from the use of ampicillin, must be bal- anced against its potential for antimicrobic failure.
B. AIDING THE HOST
The importance of "supportive therapy"
must be emphasized in the treatment of bacterial meningitis. The goal of this aspect of therapy is to maintain the child's homeo- stasis until internal "autoregulation" can take over. The delivery of oxygenated blood to the brain has first priority, if cerebral metabolism and subsequent devel- opment is to be minimally deranged. In the absence of direct measurements, bed- side monitoring is accomplished through observation of blood pressure, central venous pressure, hematocrit, and arterial Po,. Maintenance of these physiologic parameters with the appropriate replace- ment fluid (blood, saline, or plasma), and with an adequate ambient Po,, is as im- portant as appropriate antibiotic therapy. The delivery of bactericidal leukocytes, antibiotics, metabolic substrates, and anti- bacterial proteins is directly dependent on an appropriate cerebral blood flow.
Other pathophysiological alterations also occur commonly in bacterial meningitis. They can be a further detriment to intrinsic cerebral metabolism, as well as a detriment to all factors promoting bacterial clearance. These alterations, occurring in 10% to 50% of all patients, consist of: (1) h y p ~ g l y c e m i a , ~ ~
( 2 ) hypo~alcemia,~5 ( 3 ) hypo or hyperther- mia, and ( 4 ) hypo or hypers~molarity.~~
One must remember the possibility of metabolic complications occurring, as they are readily treatable.
We can decrease the morbidity of bac- terial meningitis only through promoting microorganism clearance ( antibiotics ) ; aid- ing the host in clearing the organisms, and maintaining cerebral metabolism.
REFERENCES
1. Bennett, J.: Minutes, ad hoc meeting on poly- saccharide vaccines. Infectious Diseases Branch, National Institute of Allergy and Infectious Diseases. September 30, 1972. 2. Michaels, R. H.: Increase in influenza1 menin-
gitis. N. Eng. J. Med., 285:686, 1971. 3. Parke, J. C. Jr., Schneerson, R., and Robbins,
599
BACTERIAL MENINGITIS
4. Fraser, D. W., Darby, C. P., Koehler, R. E.,Jacobs, C. F., and Feldman, R. A.: Risk factors in bacterial meningitis: Charleston County, South Carolina. J. Infect. Dis., 127: 271, 1973.
5. Sell, S. H. W., Merrill, R. E., Doyne, E. O., and Zimsky, E. P.: Long-term sequelae of Hemo- philus influenme meningitis. Pediatrics, 49: 206, 1972.
6. Sproles, E. T., 111, Azerrad, J., Williamson, C., and Merrill, R. E.: Meningitis due to Hemo- philus influenme: Long-term sequelae. J. Pediat., 75:782, 1969.
7. Turk, D. C.: Distribution of Hemophilus in- flmm in healthy human communities. Turk, D. C., and May, J. R., eds.: Hemo- philus infiuenzae: Its clinical importance, ed. 1. London: English Universities Press,
1967, p. 20.
8. Good, P. G., Fousek, M. D., Grossman, M. F., and Boisvert, P. L.: A study of the familial spread of Hemophilus influenme, type b. Yale J. Biol. Med., 15:913, 1943.
9. Harding, A. L., Anderson, P., Howie, V. M., Ploussard, J. H., and Smith, D. H.: Hemo- philus influenme isolated from children with otitis media. Sell, S. H., and Karzon, D. T., eds.: Hemophilus influenure. Nashville, Tennessee: Vanderbilt University Press, in press.
10. Greenfield, S., and Feldman, H. A.: Familial carriers and meningococcal meningitis. N. Eng. J. Med., 277:497, 1967.
11. Leedom, J. M., Ivler, D., Mathies, A. W., Thrupp, L. D., Fremont, J. C., Wehrle, P. F., and Portney, B.: The problem of sulfa- diazine-resistant meningococci. Antimicrob. Agents. Chemother., 6:281, 1966.
12. Austrian.: Pneumococcal infections in sickle cell anemia. h e r . J. Dis. Child., 173:614, 1972.
13. Choremis, C., Economos, D., and Papadetos, C.: Intraspinal epidermoid tumors in patients treated for tuberculous meningitis. Lancet, 2:437, 1956.
14. McQueen, J. A,, and Ducker, T. B.: Intraspinal tumors ( epidermoid ) resulting from lumbar punctures with open needles. J. S. Carolina Med. Assoc., 67:107, 1971.
15. Ingram, D. L., Anderson, P., and Smith, D. H.: Countercurrent immunoelectrophoresis in the diagnosis of systemic disease caused by Hemophilus influenme b. J. Pediat., 81: 1156, 1972.
16. Coonrod, J. D., and Rytel, M. W.: Determina- tion of the etiology of bacterial meningitis by counter-immunoelectrophoresis. Lancet, 1:1154, 1972.
17. Dodge, P. R., and Swartz, M. N.: Bacterial meningitis: A review of selected aspects 11. N. Eng. J. Med., 272:1003, 1965.
18. Quick, D. T., Thompson, J. M., and Bond, J. 0.: The 1962 epidemic of St. Louis encephalitis in Florida. IV. Clinical features of cases occuring in the Tampa Bay area. Amer. J. Epidemiol., 181:415, 1965. 19. Karzon, D. T., Eckert, G. L., Barron, A. L.,
et al.: Aseptic meningitis due to Echovirus 4. Amer. J. Dis. Child., 101:610, 1961. 20. Posner, J. B., and Plum, F.: Independence of
blood and CSF lactate. Arch. Neurol., 16: 492, 1967.
21. DeSanctis, A. G., Killian, J., and Garcia, T.: Lactic acid of spinal fluid in meningitis: Practical diagnostic and prognostic value. Amer. J. Dis. Child., 46:239, 1933. 22. Shearer, C., and Parsons, T. R.: The reaction
of the spinal fluid during cerebrospinal fever. Quart. J. Med., 14:120, 1921.
23. Prockop, L. D.: Cerebrospinal fluid lactic acid. Neurology, 18: 189, 1968.
24. Belsey, M. A.: CSF glutamic oxdoacetic trans- aminase in acute bacterial meningitis. Amer. J. Dis. Child., 117:288, 1969.
25. Adams, R. D., Kubik, C. S., and Bonner, F. J.: The clinical and pathological aspects of i d u - enzal meningitis. Arch. Pediat., 65:408,1948. 26. Wertham, F.: The cerebral lesion in purulent meningitis. Arch. Neurol. Psych., 26:549, 1931.
27. Smith, J. F., and Landing, B. H.: Mechanisms of brain damage in H. influenza1 meningitis. J. Neuropath. Exp. Neurol., 19:248, 1960. 28. Rorke, L. B., and Pitts, F. W.: Purulent
meningitis: the pathologic basis of clinical manifestations. Clin. Pediat. 2:64, 1983. 29. Wehrle, P. F., Mathies, Jr., A. W., and Lee-
dom, J. M.: The critically ill child: Manage- ment of acute bacterial meningitis. Pediatrics, 44:991, 1969.
30. deLemos, R. A., and Haggerty, R. J.: Corti- costeroids as an adjunct to treatment in bacterial meningitis: A controlled clinical trial. Pediatrics, 44:30, 1969.
31. Belsey, M. A,, HofFpavir, C. W., and Smith, M. H. D.: Dexamethasone in the treatment of acute bacterial meningitis: The effect of study design on the interpretation of results. Pediatrics, 44: 503, 1969.
32. McKay, R. J., Jr., Ingraham, F. D., and Matson, D. D.: Subdural fluid complicating bacterial meningitis. JAMA, 152:387, 1953. 33. Benson, P., Nyhan, W. L., and Shimazu, H.:
The prognosis of subdural eftisions com- plicating pyogenic meningitis. J. Pediat., 57: 670, 1960.
34. Coonrod, J. D., and Dans, P. W.: Subdural empyema. Amer. J. Med., 5385, 1972. 35. LeBeau, J., Creissard, P., Harispe, L., and
DIAGNOSIS
ANDTREATMENT
36. Thomas, V. H., and Hopkins, I. J.: Arterio-graphic demonstration of vascular lesions in the study of neurologic deficit in advanced Haemophilus influenme meningitis. Develop. Med. Child. Neurol., 14:783, 1972. 37. Schwartz, J. F.: Ataxia in bacterial meningitis.
Neurology, 22: 1071, 1972.
38. Sell, S. H. W., Webb, W. W., Pate, J. E., and Doyne, E. 0.: Psychological sequelae of bacterial meningitis: Controlled studies. Pediatrics, 49: 212, 1972.
39. Roy, T. E., Krieger, E., and Craig, G., et al.: Studies on the absorption of chloramphenicol in relation to the treatment of meningitis. Antibiot. Chemother., 2 5 0 5 , 1952.
40. Schoenbach, E. B., Spencer, H. C., and Monnier, J.: Treatment of H. influenme meningitis with aureomycin and chloram- phenicol. Amer. J. Med., 12:263, 1952. 41. Haltalin, K. C., and Smith, J. B.: Reevaluation
of ampicillin therapy for Hemophilus in- fluenzae meningitis. Amer. J. Dis. Child., 122:328, 1971.
42. Gold, A. J., Lieberman, E., and Wright, H. T.: Bacteriologic relapse during ampicillin treat- ment of Hemophilus influenme meningitis. J. Pediat., 74:779, 1969.
43. Shackelford, P. G., Bobinski, J. E., Feigin, R. D., and Cherry, J. D.: Therapy of Henw- philus influenme reconsidered. N. Eng. J. Med., 287:634, 1972.
44. Yeung, C. Y., Lee, V. W. Y., and Young, M. B.: Hypoglycemia in neonatal sepsis. J. Pediat., 77:812, 1970.
45. Gonzalez, C. F., Finberg, L., and Bluestein, D. D.: Electrolyte concentration during acute infections. h e r . J. Dis. Child., 107:476, 1964.
46. Nyhan, W. L., and Cooke, R. E.: Symptomatic hypoantremia in acute infections of the cen- children. Canad. Med. Assn. J., 90:615, 1964. 47. Gossage, J. D.: Acute purulent meningitis in children. Canad. Med. Assn. J., 90:615,1964.
48. Seriki, 0.: Pyogenic meningitis in infancy and childhood. Clin. Pediat., 9: 17, 1970. 49. Haggerty, R. J., and Zizi, M.: Acute bacteri-
al meningitis. Advances Pediat., 13:129, 1964.
50. Carpenter, R. R., and Petersdorf, R. G.: The clinical spectrum of bacterial meningitis. Amer. J. Med., 33:262, 1962.
51. Kneebone, G. M.: Purulent meningitis in child- hood. Med. J. Aust., 48:124, 1961. 52. Sifontes, J. E., Williams, R. D., Lincoln, E. M.,
and Clemons, H.: Observations on the glu- cose content of the cerebrospinal fluid in patients with tuberculous meningitis. Amer. Rev. Tuberc., 67:732, 1953.
53. Rabe, E. F., and Curnen, E. C.: Occurrence of lysozyrne in the cerebrospinal fluid and serum of infants and children. J. Pediat., 38:147, 1951.
54. Neches, W., and Platt, M.: Cerebrospinal fluid LDH in 287 children including 53 cases of meningitis of bacterial and nonbacterial etiology. Pediatrics, 41: 1097, 1968. 55. O'Toole, R. D., Goode, L., and Howe, C.:
Neuraminidase activity in bacterial menin- gitis. J. Clin. Invest., 50:979, 1971. 56. Taber, L. H., Yow, M. D., and Nieberg, F. G.:
The penetration of broad-spectrum anti- biotics into the CSF. Ann. N.Y. Acad. Sci., 145:473, 1967.
57. Barrett, F. F., Eardley, W. A., Yow, M. D., and Leverett, H. A.: Ampicillin in the treat- ment of acute suppurative meningitis. J.
Pediat., 69:343, 1966.
58. Stark, G.: Treatment of ventriculitis in hydro- cephalic infants: Intrathecal and intraven- tricular use of the new penicillins. Develop. Med. Child, Neurol., 15:36, 1968.
1973;52;586
Pediatrics
David H. Smith, David L. Ingram, Arnold L. Smith, Floyd Gilles and M. J. Bresnan
BACTERIAL MENINGITIS: A Symposium
Services
Updated Information &
http://pediatrics.aappublications.org/content/52/4/586
including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or in its
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
1973;52;586
Pediatrics
David H. Smith, David L. Ingram, Arnold L. Smith, Floyd Gilles and M. J. Bresnan
BACTERIAL MENINGITIS: A Symposium
http://pediatrics.aappublications.org/content/52/4/586
the World Wide Web at:
The online version of this article, along with updated information and services, is located on
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.