ARTICLE
Longitudinal Changes of Brain-Type Natriuretic
Peptide in Preterm Neonates
Ralph L. da Graca, MDa,b, Denise C. Hassinger, MDa,b, Patrick A. Flynn, MDa,c, Cristina P. Sison, PhDd, Mirjana Nesin, MDa,b, Peter A.M. Auld, MDa,b
aDepartment of Pediatrics, New York Presbyterian Hospital, Weill Medical College of Cornell University, New York, New York;bDivision of Newborn Medicine, New York
Presbyterian Hospital, Weill Medical College of Cornell University, New York, New York;cDivision of Pediatric Cardiology, New York Presbyterian Hospital, Weill Medical
College of Cornell University, New York, New York;dDepartment of Statistics, North Shore-Long Island Jewish Health System, Manhasset, New York
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.To determine age-related concentrations of brain-type natriuretic peptide in preterm infants using bedside Triage brain-type natriuretic peptide test and correlate it to the presence or absence of the patent ductus arteriosus and venti-latory support.
METHODS.Serum brain-type natriuretic peptide levels were measured in infants who
were born at⬍32 weeks’ gestation from birth to 2 months of age. Serial echocar-diograms were performed, until closure of the patent ductus arteriosus, or until discharge. Brain-type natriuretic peptide levels were correlated to the day of life, gestational age, presence or absence of the patent ductus arteriosus, and the degree of ventilatory support. Nineteen preterm infants (gestational age: 24 –31 weeks; birth weight: 645–1670 g) were enrolled prospectively during the first 2 weeks of life. Serum brain-type natriuretic peptide levels (pg/mL) were determined in 177 blood samples, and 87 paired echocardiograms were performed.
RESULTS.Significant negative correlation was found between brain-type natriuretic
peptide levels and the day of life and remained significant when the patients were stratified by gestational age (ⱕ28 weeks and ⬎28 weeks). Higher brain-type natriuretic peptide levels correlated with increasing grade of the patent ductus arteriosus. Significant differences in brain-type natriuretic peptide levels were seen with increasing ventilatory support. Comparisons between the size of patent ductus arteriosus and the degree of ventilatory support to brain-type natriuretic peptide levels revealed that the size of the patent ductus arteriosus was the major determinant of both brain-type natriuretic peptide levels and the degree of ven-tilatory support.
CONCLUSIONS.Similar to term infants, brain-type natriuretic peptide levels of preterm infants are related to the chronological age and decline during the first month of life. Rapid bedside Triage brain-type natriuretic peptide is a potentially valuable and practical assay in determining the hemodynamic changes in preterm infants.
www.pediatrics.org/cgi/doi/10.1542/ peds.2005-1387
doi:10.1542/peds.2005-1387
Key Words
B-type natriuretic peptide, Triage BNP, prematurity, preterm infants, patent ductus arteriosus
Abbreviations
BNP— brain-type natriuretic peptide N-BNP—N-terminal BNP CHF— congestive heart failure PDA—patent ductus arteriosus GA— gestational age
NCPAP—nasal continuous positive airway pressure
IQR—interquartile range DOL— day of life
RDS—respiratory distress syndrome
Accepted for publication Dec 27, 2005 Address correspondence to Ralph L. da Graca, MD, UMDNJ-New Jersey Medical School, Department of Anesthesiology, 185 S Orange Ave, MSB E-538, Newark, NJ 07103. E-mail: [email protected]
B
RAIN NATRIURETIC PEPTIDE(BNP) is 1 of the cardiac natriuretic peptides that are responsible for the reg-ulation of physiologic vascular changes in response to pressure or fluid overload. Originally described in ex-tracts of porcine brain,1it is present in the human brainbut secreted mainly by ventricular myocytes in response to stretching. BNP contains 108 amino acid residues that release an active 32–amino acid molecule and an inac-tive N-terminal fragment. This hormone and other car-diac peptides induce vasodilation, natriuresis, and diure-sis and acts to antagonize the effects of the renin-angiotensin-aldosterone system.1,2
In adults, both BNP and N-terminal BNP (N-BNP) are highly sensitive and specific diagnostic and prognostic markers for the evaluation and treatment of congestive heart failure (CHF). It also has been used to evaluate acute dyspnea, left ventricular end-diastolic dysfunction, pulmonary hypertension, and myocardial infarction and even predict sudden cardiac death in patients with CHF.3–6Normal values of plasma N-BNP and N-terminal
atrial natriuretic peptide have been reported in healthy individuals from the perinatal period to adulthood.7–9
Reports also have discussed the use of N-BNP in corre-lation with the patent ductus arteriosus (PDA), in rela-tion to therapy (nonsteroidal anti-inflammatory medi-cations and surgery), and in CHF in children with congenital heart disease.10–12
Recently, a new blood test, Triage BNP (Biosite Diag-nostics, San Diego, CA), has been approved by the Food and Drug Administration for bedside diagnosis of CHF in adults. This test can be performed on as little as 250L of whole blood and measures the active form of BNP within 15 minutes. To our knowledge, the usefulness and the normal values of BNP levels that are determined by Triage BNP have not been established in preterm neonates. The objective of this study was to determine physiologic changes of BNP in premature neonates, us-ing bedside Triage BNP, from birth to 2 months of age and assess its relationship to the PDA and ventilatory support. The premature infant has a likelihood of car-diopulmonary and vascular morbidity that is specific to this patient population; therefore, it is difficult to obtain true normative data. Bedside Triage BNP is a potential clinical tool in the treatment of premature infants with PDA and respiratory distress. Ultimately, BNP levels may help clinicians to follow progression of disease and aid in the clinical decision-making of when closure of the PDA is necessary.
METHODS
This was a prospective observational longitudinal study. The study was approved by Institutional Review Board of the Weill Medical College of Cornell University. Writ-ten parental consent was obtained before study enroll-ment. All infants who were⬍32 weeks’ gestational age (GA) and admitted directly or transferred to the NICU at
New York Presbyterian Hospital of the Weill Cornell Medical Center were eligible for enrollment. Because infants who are ⬍32 weeks’ GA frequently have more clinical implications for PDA therapy, near-term and infants who were 32 to 34 weeks’ GA were excluded. Infants with any genetic disorder, congenital anomalies, or congenital heart disease other than PDA also were excluded from the study. Limitations to enrollment in-cluded ability to obtain consent, precondition of a single investigator performing collection, correct calibration of Triage BNP device, and availability of the echocardiog-rapher. Blood samples were collected in correlation to other blood draws to avoid excessive blood draws spe-cifically for study purposes. BNP measurements were performed on day of enrollment and 3 times a week during the first 2 months of life. An echocardiogram was performed on the day of enrollment and every 4 to 5 days until documented closure of the PDA was noted or the patient was discharged. BNP measurements were paired with echocardiograms and performed within 1 hour of each other. Echocardiography was performed by a single cardiologist throughout the duration of the study.
Although subjective, PDA grade was used to stan-dardize each echocardiogram evaluation during the course of the study. A PDA grade (left atrial to aorta ratio, ductal diameter, and diastolic flow in the descend-ing aorta) was determined for each evaluation to assess the severity of PDA: 0, closed; 1, small; 2, moderate; 3, large.13,14For assessment of the correlation with the
se-verity of respiratory distress at the time of BNP determi-nations, the following ventilatory rating scale was used for the purpose of this study: 0, room air; 1, nasal can-nula or nasal continuous positive airway pressure (NCPAP) with or without oxygen; 2, conventional ven-tilation requiringⱕ30% fraction of inspired oxygen; 3, conventional ventilation/high-frequency oscillatory ventilation requiring ⬎30% fraction of inspired oxy-gen). Assigning a ventilatory rating score allowed us to determine indirectly whether BNP and/or the grade of PDA correlated with the degree of respiratory distress. The plan of care for each patient was determined by the attending neonatologist, and BNP values were not avail-able to the cardiologist and the clinical team.
Measurement of Plasma BNP
mixture through the diagnostic lane to a zone of immo-bilized murine monoclonal antibody against the ring structure of BNP, binding the BNP fluorescent antibody complex. The unbound fluorescent antibodies were washed away by excess plasma. The Triage BNP device quantifies the fluorescence intensity of the BNP assay zone using an internal calibration curve. The assay re-quired⬃15 minutes.
Because hemolysis can affect BNP values, the BNP levels from whole blood that was obtained by venipunc-ture and from the catheter were compared in patients who had an indwelling vascular catheter. The measured difference was within 5%. Most samples were obtained by venipuncture.
Statistical Analysis
Analysis of variance was conducted to compare BNP levels over time across various groups, such as gender (male versus female), race, GA, ventilatory rating, and PDA size. Bonferroni-like adjustments were applied for pairwise comparisons on finding significant group differ-ences.
It was determined that a natural log transformation of the data conformed to the standard analysis of variance assumptions. Accordingly, all analyses were conducted using the log-transformed data but were reported in their original untransformed units to facilitate interpre-tation. For descriptive purposes, Spearman correlations were calculated to describe overall correlation between BNP and day of life. The2test was used to determine
association between categorical variables. These analyses were conducted under the weak (statistical) assumption of independence of daily measurements. The analysis of covariance method (Bland and Altman) was applied to determine correlations within patients.15
Sample Size Considerations
The sample size for this study was based on feasibility and not on any formal statistical power calculations. The number of patients in this study was limited to the available data collected during the specified study period and by difficulties in enrolling premature infants in a no-benefit research study.
RESULTS
Demographics
From June 2003 to March 2004, 19 premature infants were enrolled prospectively in the study. The demo-graphics of the study infants are shown in Table 1. There were no significant differences when comparing birth weights and GA with gender and race. All infants were enrolled during the first 2 weeks of life: 16 on day of life (DOL) 0 to 2, 1 on DOL 4, and 2 on DOL 13. Infants were followed until 2 months of age or until discharge. On average, infants were followed for 25.5 days (median: 20
days; range: 8 –72 days). Serum BNP levels were deter-mined in 177 samples. Eighty-seven paired echocardio-grams were performed from enrollment until docu-mented closure of the PDA. Because in most infants the PDA closed before 2 months of age, more BNP levels than echocardiograms were obtained. The median num-ber of BNP measurements was 8 per infant (range: 4 –22). The median number of echocardiograms was 3 per infant (range: 1–10). Infants with large PDA had more echocardiograms performed and BNP measure-ments than infants with early PDA closure. Four patients received a trial of indomethacin: 3 for asymptomatic and 1 for symptomatic PDA. One asymptomatic PDA failed to close, and the patient with symptomatic PDA ultimately required surgery.
During the course of the study, 12 of the 19 infants received surfactant therapy, 11 of the 12 infants were intubated and on ventilatory support at the time of enrollment, and 2 infants required high-frequency ven-tilation. The remaining 8 infants required either NCPAP or cannula with oxygen at the time of enrollment; only 1 of the 8 who received surfactant was placed onto NCPAP. Respiratory support that was required at the time of the testing was recorded and compared with serum BNP levels and the results of echocardiogram. Among the 19 enrolled infants, 7 had sepsis confirmed by a positive blood culture, 1 had meningitis, and 2 developed necrotizing enterocolitis. All enrolled patients survived their NICU course.
Correlation Between BNP and Postnatal Age
Figure 1 illustrates the distribution of logarithmic values of BNP during the first 2 months of life. The actual BNP levels (pg/mL) according to DOL are expressed as
me-TABLE 1 Demographics and Clinical Characteristics of Preterm Infants
Preterm Infants, % (n⫽19)
Mean⫾SD Range
Gestational age, wk 27.6⫾2.59 24–31
ⱕ28 12 (63)
⬎28 7 (37)
Birth weight, g 1055⫾294 645–1670
Male gender 14 (74)
Female gender 5 (26)
Ethnicity
White 9 (48)
Black 5 (26)
Hispanic 5 (26)
Antenatal steroids 19 (100)
Surfactant 12 (63)
Chorioamnionitis/PROM 7 (37) Cesarean births 18 (95) Apgars
1 minute 5.3⫾3.2 0–9
5 minute 7.4⫾1.4 5–9
dian with interquartile range (IQR; 25%–75%): DOL 0 to 1, 362 (94 –780); DOL 2 to 3, 196 (115–1146); DOL 4 to 5, 159 (25–1060); DOL 6 to 7, 70 (23–227); DOL 8 to 10, 81 (17–289); DOL 11 to 14, 64 (24 –191); DOL 15 to 30, 43 (12–158); DOL⬎30, 16 (6 – 48). BNP levels dur-ing the first few DOL were higher and declined expo-nentially over time. A significant negative correlation was seen between BNP and DOL (r⫽ ⫺0.34;P⫽.001). Correlations remained significant when infants were stratified according to GA (r⫽ ⫺0.34 [P ⫽ .0001] for ⱕ28 weeks andr⫽ ⫺0.47 [P⫽.0015] for⬎28 weeks. No significant difference was found when the 2 GA groups were compared with each other.
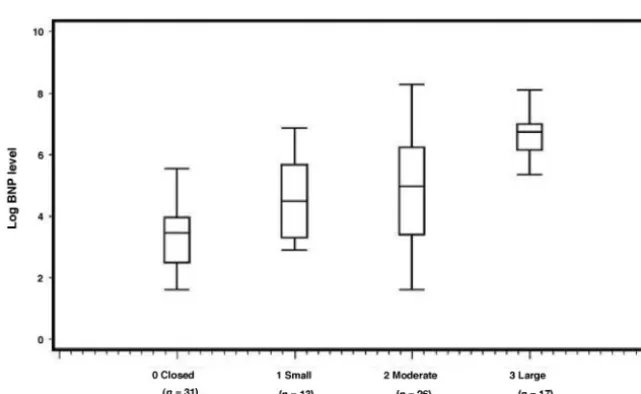
Correlation Between BNP and Grade of PDA
BNP levels were paired to echocardiogram results and correlated to the grade of PDA (0, 1, 2, and 3). Eighty-seven paired samples were obtained during the study.
The following BNP levels (pg/mL) were obtained for each PDA grade (median [IQR (25%–75%)]: grade 0, 31 (12–52); grade 1, 88 (27–285); grade 2, 145 (30 – 498); and grade 3, 833 (470 –1060). Figure 2 depicts the dis-tribution of logarithmic values of BNP levels according to the PDA grade. Significant differences in BNP levels were seen with increasing grade of PDA (P⬍.0001). In pairwise comparisons, significant differences were seen between PDA grades: 0 and 1,P⬍ .014; 0 and 2, P⬍
.001; 0 and 3,P⬍.001; 1 and 3,P⬍.001; and 2 and 3,
P⬍.001.
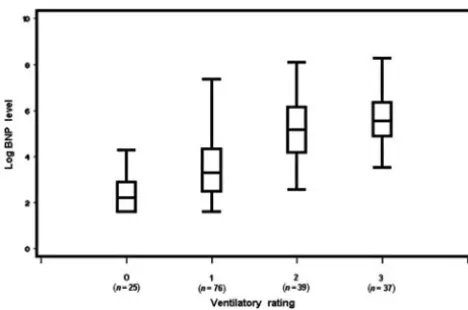
Correlation Between BNP and Ventilatory Support
The following BNP levels (pg/mL) were obtained for different ventilatory ratings (median [IQR (25%–75%)]: rating 0, 9 (5–18); rating 1, 27 (12–75); rating 2, 176 (65– 470); and rating 3, 256 (132–573). Figure 3 illus-trates the distribution of logarithmic BNP values
accord-FIGURE 1
Exponential changes of logarithmic BNP levels (pg/ mL) in preterm neonates over time (n⫽177 observa-tions). Values are expressed as median with IQR (25%– 75%).
FIGURE 2
ing to the degree of ventilatory support. Significant in-creases in the BNP levels were seen across increased degree of ventilatory support (P ⬍ .0001). In pairwise comparisons, significant differences were detected be-tween ventilatory ratings: 0 and 1,P⬍.001; 0 and 2,P ⬍.001; 0 and 3,P⬍.001; 1 and 2,P⬍.001; and 1 and 3,P⬍.001). No difference was seen between 2 and 3 (P ⫽.720). Therefore, intubated patients represent a simi-lar group in relation to their BNP values, and in addi-tional subanalysis, we combined their measurements.
Correlation of BNP, Grade of PDA, and Degree of Ventilatory Support
To determine whether there are significant correlations among BNP levels, PDA, and ventilatory support, we divided 87 sets of observations into 2 ventilatory groups: nonintubated (ventilatory ratings 0 and 1) and intubated (ventilatory ratings 2 and 3) and compared them with the size of the PDA: high-grade PDA (grade 3) and lower grade PDA (grades 0, 1, and 2). When grade 3 PDA was diagnosed by echocardiogram, 14 (82%) of 17 observa-tions noted that these infants tended to be intubated (ventilatory ratings 2 and 3), in contrast to 29 (41%) of 70 observations of patients with lower grades of PDA (0, 1, and 2) that required intubation (P⫽.003).
Table 2 illustrates the relationship of logarithmic val-ues of BNP levels, grade of PDA, and ventilatory rating to each other. BNP values are expressed as mean⫾ SEM
and median (25%–75% IQR). Significant correlation was seen when comparing increasing size of the PDA with the degree of ventilatory support. Within lower PDA grades, BNP levels were significantly higher in the intubated than in the nonintubated infants. However, regardless of ventilatory support, no significant differ-ence was seen in patients with high-grade PDA (grade 3). The overall patterns of change in BNP levels between PDA groups depended on the degree of ventilatory sup-port (P⬍.02)
DISCUSSION
Rapid diagnostic tests are becoming a point of care in neonatal and adult medicine. Before such a test can be introduced into clinical practice, it is important to estab-lish normative values and identify patient populations that may benefit from a test. In this study, we used bedside Triage BNP to measure postnatal changes of BNP levels in premature infants. Our results are similar to other published literature using N-terminal atrial natri-uretic peptide and N-BNP tests that require larger blood volumes and the results of which are not available im-mediately.7–9
We have demonstrated after an initial increase on DOL 1 and 2 (that most likely represents perinatal vas-cular adaptation from fetal to neonatal circulation), BNP levels in premature infants declined exponentially dur-ing the first 2 months of life and reached similar values that have been reported in healthy adults and children (Fig 1).7,8In contrast to healthy term infants, daily BNP
levels in premature infants show greater variability over time.9The difficulty in correlating BNP to the size of the
PDA during the perinatal transition more likely corre-lates with changes in pulmonary arterial pressure and adaptation to normal circulation.16However, the greater
variability of BNP levels over time likely is related to cardiopulmonary morbidities (delayed closure of PDA, respiratory distress syndrome [RDS], fluid overload, etc) that are associated with prematurity. Our results showed no difference when patients were stratified by GA and indicate that comorbidities may be more relevant for the varying changes in the BNP levels than GA. In addition to the cardiopulmonary factors, other circulatory changes (septic shock) may affect BNP levels. Data from animal studies17and adult literature18indicate that
cyto-kines (especially IL-6) may play a role in the upregula-tion of natriuretic peptides in ventricular myocytes and the release of prostaglandins in circulation that may
TABLE 2 Correlations of BNP, Grade of PDA, and Ventilatory Rating
Ventilatory Rating (Nonintubated) Ventilatory Rating (Intubated) P
PDA grade 0, 1, 2 BNP: 63.4⫾17; median: 26 (12–52) (n⫽41) BNP: 519⫾157; median: 168 (88–300) (n⫽29) ⬍.0001 PDA grade 3 BNP: 783⫾115; median: 849 (558–941) (n⫽3) BNP: 1061⫾261; median: 759 (389–1240) (n⫽14) NS
P ⬍.002 ⬍.01
NS indicates nonsignificant.
FIGURE 3
relate to ductal opening. Because a significant number (37%) of premature infants in our study were exposed to chorioamnionitis or developed infections, the role of cytokines in the regulation of BNP production may be relevant for the clinical course in premature infants and their ability to undergo postnatal vascular adaptation.
Our results confirm already reported findings that the magnitude of PDA is the major determinant of elevated BNP.10,11Infants who developed a large PDA (grade 3)
have significantly higher levels of BNP than infants without PDA or with small- or moderate-sized PDA (Fig 2). Infants with moderate (grade 2) PDA may represent a nonhomogeneous group, as indicated by the wide SD of BNP levels (Fig 2). Some patients in this group had high BNP levels, indicating hemodynamically significant PDA, whereas the others with the same grade of PDA had lower levels of BNP and likely hemodynamically insignificant PDA. Alternatively, elevated BNP levels in an infant with small- or moderate-sized PDA may have other reasons for elevated BNP level: cardiac abnormal-ities (eg, myocarditis, ventricular dysfunction) or vascu-lar cause other than postnatal circulatory adaptation (eg, persistent pulmonary hypertension of the newborn, fluid overload, transfusion).19,20
A positive correlation was established between ventilatory support and BNP levels (Fig 3). The likely explanation for these findings was the presence of a hemodynamically significant PDA. The increased degree of left-to-right shunting, pulmonary congestion with de-creased lung compliance, and eventual progression to CHF have been described in RDS.21,22Our study confirms
these findings: infants with the highest grade of PDA (grade 3) had both higher BNP levels and a higher de-gree of ventilatory support (Table 2). It is likely that this group of infants would benefit from therapeutic inter-vention (eg, closure of PDA, fluid restriction).
Table 2 further describes infants with lower grades of PDA that required higher ventilatory support (intu-bated). These infants more likely had lung disease and therefore showed relatively lower BNP values. As de-scribed earlier, this likely is a nonhomogeneous group, and selected infants within this group may have evi-dence for elevated BNP levels other than the PDA. A significant difference between this group and infants who were not intubated and had low PDA grade sug-gests that significant respiratory disease may be second-ary to a delayed decline in the pulmonsecond-ary vascular re-sistance.16
Despite a small sample size and the various comor-bidities that are associated with prematurity, we were able to establish a range of BNP values in premature infants during the first 2 months of life using a bedside device with immediate availability of results. Our study showed that the natural progression of circulatory changes over time was not related to GA but rather to comorbidities that premature infants experience during
this period.10,11,16,19–22 Even in an extremely premature
infant, BNP levels declined after the first few DOLs when the PDA was closed and RDS was not severe. BNP levels correlated best with the size of the PDA. Infants who have a large PDA and require a high degree of ventila-tory support tend to have higher BNP levels and may represent a target group that would benefit from closure of the PDA.23 The importance of the utilization of BNP
has not been shown to be diagnostic in this population. It is important to do additional studies and possibly multicenter trials to establish true normative ranges in premature infants, especially in the case in which BNP levels may serve as an indicator for earlier intervention (surgical ligation or medical therapy). However, it is important to emphasize that BNP levels should be used as an adjunct to clinical assessment and echocardiogra-phy and cannot be used independently in medical deci-sion-making. In addition, Triage BNP may serve as a quick, reliable, and inexpensive tool to follow progres-sion of cardiopulmonary and vascular disease and help to determine when echocardiography is required in such critically ill infants.
REFERENCES
1. Sudoh T, Kangawa K, Minamino N, Matsuo H. A new natri-uretic peptide in porcine brain.Nature.1998;332:78 – 81 2. Levin ER, Gardner DG, Samson WK. Natriuretic peptides.
N Engl J Med.1998;339:321–328
3. Troughton RW, Frampton CM, Yandle TG, Espiner EA, Nich-olls MG, Richards AM. Treatment of heart failure guided by plasma aminoterminal brain natriuretic peptide (N-BNP) con-centrations.Lancet.2000;355:1126 –1130
4. Mueller C, Scholer A, Laule-Kilian K. Use of B-type natriuretic peptide in the evaluation and management of acute dyspnea.
N Engl J Med.2004;350:647– 654
5. Nagaya N, Nishikimi T, Uematsu M. Plasma brain natriuretic peptide as a prognostic indicator in patients with primary pul-monary hypertensionCirculation.2000;102:865– 870
6. Wang TJ, Larson MG, Levy D. Benjamin. Plasma natriuretic peptide levels and the risk of cardiovascular events and death.
N Engl J Med.2004;350:655– 663
7. Yoshibayashi M, Kamiya T, Saito Y. Plasma brain natriuretic peptide concentrations in healthy children from birth to adolescence: marked and rapid increase after birth.Eur J En-docrinol.1995;133:207–209
8. Daggubati S, Parks JR, Overton RM, Cintron G, Schocken DD, Vesely DL. Adrenomedullin, endothelin, neuropeptide Y, atrial, brain, and C-natriuretic prohormone peptides compared as early heart failure indicators. Cardiovasc Res. 1997;36: 246 –255
9. Mir TS, Laux R, Hellwege HH. Plasma concentrations of ami-noterminal pro atrial natriuretic peptide and amiami-noterminal pro brain natriuretic peptide in healthy neonates: marked and rapid increase after birth.Pediatrics.2003;112:896 – 899 10. Puddy VF, Amirmansour C, Williams AF, Singer DR. Plasma
brain natriuretic peptide as a predictor of haemodynamically significant patent ductus arteriosus in preterm infants.Clin Sci (Lond).2002;103:75–77
concentrations of N-terminal pro-brain natriuretic peptide in control children from the neonatal to adolescent period and in children with congestive heart failure.Pediatrics.2002;110(6). Available at: www.pediatrics.org/cgi/content/full/110/6/e76 13. Skinner J. Diagnosis of patent ductus arteriosus.Semin
Neona-tol.2001;6:49 – 61
14. Evans N. Diagnosis of patent ductus arteriosus in the preterm newborn.Arch Dis Child.1993;68:58 – 61
15. Bland JM, Altman DG. Calculating correlation coefficients with repeated observations: correlation within subjects. BMJ. 1995; 310:446
16. Ikemoto Y, Nogi S, Teraguchi M, Kojima T, Hirata Y, Kobayashi Y. Early changes in plasma brain and atrial natriuretic peptides in premature infants: correlation with pulmonary arterial pres-sure.Early Hum Dev.1996;46:55– 62
17. Tanaka T, Kanda T, Takahashi T, Saegusa S, Moriya J, Kuraba-yashi M. Interleukin-6-induced reciprocal expression of SERCA and natriuretic peptides mRNA in cultured rat ventric-ular myocytes.J Int Med Res.2004;32:57– 61
18. Witthaut R, Busch C, Fraunberger P, et al. Plasma atrial natri-uretic peptide and brain natrinatri-uretic peptide are increased in septic
shock: impact of interleukin-6 and sepsis-associated left ventric-ular dysfunction.Intensive Care Med.2003;29:1696 –1702 19. Reynolds EW, Ellington JG, Vranicar M, Bada HS. Brain-type
natriuretic peptide in the diagnosis and management of per-sistent pulmonary hypertension of the newborn. Pediatrics.
2004;114:1297–1304
20. Walther T, Stepan H, Faber R. Dual natriuretic peptide re-sponse to volume load in the fetal circulation.Cardiovasc Res.
2001;49:817– 819
21. Pesonen E, Heldt GP, Merritt TA. Atrial natriuretic factor and pulmonary status in premature infants with respiratory distress syndrome preliminary investigation:Pediatr Pulmonol.1993;15: 362–364
22. Pesonen E, Merritt AT, Heldt G. Correlation of patent ductus arteriosus shunting with plasma atrial natriuretic factor con-centration in preterm infants with respiratory distress syn-drome.Pediatr Res.1990;27:137–139
DOI: 10.1542/peds.2005-1387
2006;117;2183
Pediatrics
Nesin and Peter A.M. Auld
Ralph L. da Graca, Denise C. Hassinger, Patrick A. Flynn, Cristina P. Sison, Mirjana
Longitudinal Changes of Brain-Type Natriuretic Peptide in Preterm Neonates
Services
Updated Information &
http://pediatrics.aappublications.org/content/117/6/2183
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/117/6/2183#BIBL
This article cites 22 articles, 6 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/cardiology_sub
Cardiology
http://www.aappublications.org/cgi/collection/neurology_sub
Neurology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2005-1387
2006;117;2183
Pediatrics
Nesin and Peter A.M. Auld
Ralph L. da Graca, Denise C. Hassinger, Patrick A. Flynn, Cristina P. Sison, Mirjana
Longitudinal Changes of Brain-Type Natriuretic Peptide in Preterm Neonates
http://pediatrics.aappublications.org/content/117/6/2183
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.