STUDY OF PATTERN OF URINARY SEDIMENTS IN
RENAL DISEASES
DISSERTATION
SUBMITTED TO THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY
CHENNAI
In partial fulfillment of the requirements for the degree of
M.D. (PATHOLOGY)
BRANCH – III
DEPARTMENT OF PATHOLOGY
TIRUNELVELI MEDICAL COLLEGE HOSPITAL
TIRUNELVELI – 627011
CERTIFICATE
This is to certify that the dissertation titled “STUDY OF PATTERN OF
URINARY SEDIMENTS IN RENAL DISEASES”, is a bonafide work done by
Dr.MOHAN MURUGESAN, Post Graduate Student, Department of Pathology,
Tirunelveli Medical College, Tirunelveli – 627011, in partial fulfillment of the
university rules and regulations for the award of MD DEGREE in PATHOLOGY
BRANCH-III, under my guidance and supervision, during the academic period
from 2014 – 2017.
Prof. SITHY ATHIYA MUNAVARAH. M.D.,
Dean,
CERTIFICATE
I hereby certify that this dissertation entitled “STUDY OF PATTERN OF
URINARY SEDIMENTS IN RENAL DISEASES” is a record of work done by
Dr.MOHAN MURUGESAN, in the Department of Pathology, Tirunelveli
Medical College, Tirunelveli, during his postgraduate degree course period from
2014- 2017. This work has not formed the basis for previous award of any
degree.
Prof. K. SHANTARAMAN. M.D.,
Department of pathology, Tirunelveli Medical College, Tirunelveli- 627011.
Prof. K. SHANTARAMAN. M.D.,
DECLARATION
I solemnly declare that the dissertation titled “STUDY OF PATTERN OF
URINARY SEDIMENTS IN RENAL DISEASES” was done by me at
Tirunelveli Medical College, Tirunelveli – 627011, during the period 2014 - 2017
under the guidance and supervision of Prof. K.SHANTARAMAN.M.D., to be
submitted to The Tamil Nadu Dr. M.G.R. Medical University towards the partial
fulfillment of requirements for the award of MD DEGREE in PATHOLOGY
BRANCH-III.
Place : Tirunelveli
Date :
Dr.MOHAN MURUGESAN, Post Graduate Student, Department of Pathology, Tirunelveli Medical College,
ACKNOWLEDGEMENT
I thank Professor Dr. SITHY ATHIYA MUNAVARAH. M.D., Dean,
Tirunelveli Medical College, for having permitted me to conduct the study and
use the hospital resources in the study.
I express my heartfelt gratitude to Professor Dr. SHANTARAMAN.K.
M.D., Professor and Head, Department of Pathology, for his inspiration, advice
and guidance in making this work complete.
I am extremely thankful to Professors Dr. VALLIMANALAN. S. M.D.,
Dr. SWAMINATHAN . K. M.D., Dr. SURESH DURAI. J. M.D., Dr. ARASI
RAJESH.M.D., DR.VASUKI.M.D., Additional Professors, Department of
Pathology, for guiding me academically and professionally during the period of
study. I also thank the Assistant Professors, for their encouragement and support.
I sincerely thank Professor Dr. RAMASUBRAMANIAN. V. M.D., D.M.,
and faculties of the Department of Nephrology for providing me the patients for
my study and guiding me during the period of study.
I also thank all the lab technicians especially Mr. Balamurugan and
Mrs. Premalatha for their valued assistance and my fellow postgraduates for their
cooperation which enormously helped me in the study. I am also indebted to thank
all the patients and their caring relatives for without their humble cooperation, this
ABBREVIATIONS
GFR GLOMERULAR FILTERATION RATE
SLE SYSTEMIC LUPUS NEPHRITIS
RBCs RED BLOOD CORPUSCLES
WBCs WHITE BLOOD CORPUSCLES
HDL HIGH DENSITY LIPOPROTEIN
RTECs RENAL TUBULAR EPITHELIAL CELLS
THG TAMM HORSFALL GLYCOPROTEIN
MCD MINIMAL CHANGE DISEASE
FSGS FOCAL SEGMENTAL GLOMERULOSCLEROSIS
IgAN IgA NEPHROPATHY
HPF HIGH POWER FIELD
MPGN MEMBRANOPROLIFERATIVE
GLOMERULONEPHRITIS
LN LUPUS NEPHRITIS
DN DIABETIC NEPHROPATHY
AIN ACUTE INTERSTITIAL NEPHRITIS
NSAIDS NON STEROIDAL ANTI INFLAMMATORY DRUGS
CIN CHRONIC INTERSTITIAL NEPHRITIS
AN ANALGESIC NEPHROPATHY
ATN ACUTE TUBULAR NECROSIS
IMH ISOLATED MICROSCOPIC HAEMATURIA
AKI ACUTE KIDNEY INJURY
AKIN ACUTE KIDNEY INJURY NETWORK
LPF LOW POWER FIELD
S.D. STANDARD DEVIATION
CONTENTS
1. INTRODUCTION 1
2. AIMS AND OBJECTIVES 3
3. REVIEW OF LITERATURE 4
4. MATERIALS AND METHODS 49
5. RESULTS AND OBSERVATION 55
6. DISCUSSION 72
7. SUMMARY AND CONCLUSION 80
8. BIBLIOGRAPHY
1
INTRODUCTION
Urinary microscopy is an integral part of the clinical evaluation of patients
with kidney disorders and frequently is used to differentiate a number of clinical
conditions (eg, nephrotic syndrome, nephritic syndrome). The findings also can
guide medical interventions and improve patient management. The examination of
the urinary sediment, coupled with the assessment of proteinuria, allows the
identification of different urinary profiles, which can be caused by various
clinical conditions. These urinary profiles are: the nephrotic pattern; the nephritic
pattern; the nephrotic and nephritic pattern; the sediment pattern with many renal
tubular epithelial cells; the sediment pattern with increased numbers of
erythrocytes and the leukocyturia. Hyaline cylindruria with a few erythrocytes
and leukocytes may be seen in normal subjects. The concentration of creatinine in
serum is the most widely used and commonly accepted measure of renal function
in clinical medicine. The clinical utility of the serum creatinine concentration
centers on its relation to the glomerular filtration rate (GFR). In renal patients, the
serum creatinine level may remain normal with abnormal urinalysis as in case of
non proliferative glomerulonephritis; increased in level with abnormal urinalysis
as seen in diseases like proliferative glomerulonephritis, acute kidney injury with
acute tubular necrosis; increased level with normal urinalysis as seen in cases of
hypertensive nephrosclerosis and ischemic renal diseases.
Urinary sediment scoring system can be used to assess the role of urine
2
tubular epithelial cell casts constitute two parameters needed for calculating a
score.
Renal diseases are seldom diagnosed in the early stages because the
biochemical parameters are not elevated until late.Investigations for detection of
early stages of renal disease are of immense importance. Urinalysis yields a lot of
valuable information regarding the functioning of the kidney, when properly
performed, hence is called “liquid renal biopsy”.Properly conducted urine
examination can indicate subtle changes in renal function. Urine examination is
simple and cost effective. It has added values in the diagnostic workup of renal
diseases. Several systemic diseases like diabetic mellitus, systemic lupus nephritis
(S.L.E) causes significant damage to kidneys where regular monitoring is required
for detection of renal injury. In these conditions, which necessitates repeated
3
AIMS AND OBJECTIVES
1. To describe the various patterns of urinary sediments in patients with renal
diseases.
2. To correlate these urine sediment patterns described with type and severity
of renal damage namely the histopathological patterns in renal biopsy,
4
REVIEW OF LITERATURE
The earliest microscopic examination of urine was done by Nicolaus
Fabricius de Peiresc [1] in 1630, to study the nature of the urinary stones. Pierre
Rayer and Eugene Napoleon Vigla introduced urine microscopy into clinical
practice[1].Their study was comprehensive and of paramount importance. They
explained about the handling of urine sample, microscope, and the importance of
correlating microscopic examination with biochemical parameters. They
described in detail about the crystals, and squamous epithelial cells, mucus, pus
cells, erythrocytes, lipids, sperm and yeasts. They mentioned about thin and light
lamellae which was probably casts and also described the urinary findings in
normal subjects and many pathological conditions. They stated that apparently
normal urine can contain erythrocytes or leukocytes which can be identified only
with the microscope, thus presenting the concepts of microscopic hematuria and
pyuria. In acute nephritis plenty of blood corpuscles, mucus globules, squamous
epithelial cells, and fibrin strands. In patients with nephrotic syndrome, thin
lamellae of amorphous material probably casts, mucus globules, lipids, blood
corpuscles, uric acid crystals, scanty phosphates. In acute and chronic
pyelonephritis, pus globules, blood corpuscles, necrotic cellular debris, uric acid
crystals or crystals of triple phosphate. Finally, the association between lipiduria
and albuminuria. All these observations were done during a period in which
microscopy as a diagnostic tool was at its initial stages. In 1837, Gabriel Gustav
5
tubules[1]. In 1842 Johann Franz Simon, described them in urine[1]. Henry Bence
Jones, discovered light chain proteinuria[1]. He described urinary casts and
explained the association between casts, Bright's disease and albuminuria.
Thomas Addis in 1920, performed microscopic examination of urine in patients of
glomerulonephritis serially over the years and detected that an abundant sediment
containing large numbers of erythrocytes (RBCs), leucocytes(WBCs), epithelial
cells and casts could become more and more scanty over time[1]. This specified
the transformation of an active disease into a chronic process. For quantification
of urinary sediments Addis introduced collection of timed urine samples and the
use of counting chambers, which was termed as "Addis count"[1]. Based on the
results Bright's disease was classified into three types, that is, haemorrhagic,
degenerative, and arteriosclerotic. Addis also defined broad renal failure casts in
renal failure patients in a period in which biochemical tests were not readily
available as they are today. In 1960s urinary sediments were studied using new
microscopic techniques. The final evidence to previous in vitro studies that
Tamm-Horsfall glycoprotein is the matrix of casts was provided by McQueen
using immunofluorescent-labelled antibodies [1]. In early 1950s phase contrast
microscopy was discovered and recommended for urinalysis in 1968 by Robert
Kark[1].In early 1970s transmission electron microscopy was used to identify
amyloid fibrils in urine samples of patients with renal amyloidosis, and then in
acute tubular necrosis. Few years later scanning electron microscope was utilised
6
The examination of the urinary sediment, which is an integral part of urinalysis, is
an irreplaceable tool for the diagnosis and monitoring of the diseases of the
kidneys and the urinary tract [2,3]. However, reliable results can be obtained only
by using the correct methodology.
Collection of urine :
International guidelines suggest the procedures for urine collection [4,5]. For
routine examination any fresh specimen of urine is adequate. It is best to collect
an early morning specimen, which is voided when the patient first arises from a
night’s sleep, as it is the most concentrated single specimen, and it has the lowest
pH, which tends to preserve the formed elements well. The second urine of the
morning, is usually concentrated and acidic, and without the lysis of the elements
which can occur in overnight urine due to the prolonged permanence in the
bladder[6]. Highly alkaline urine favours the lysis of leukocytes[7], casts [8] and
precipitation of phosphates which can mask other urinary elements. In order to
minimize contamination, hands and external genitalia must be cleaned with water,
for females, spreading of the labia of vagina, for males the retraction of the
foreskin of the glans. The midstream technique is the recommended procedure in
which the first portion of the urine is discarded, since it may be contaminated with
cellular elements and bacteria from the external urinary tract and genital area [5].
Macroscopic examination:
Macroscopic inspection reveal the presence of turbidity and of abnormal
changes of the urine colour. Turbidity is caused by large numbers of squamous
7
urates[9] in majority of cases. However, pathological samples are often perfectly
clear. Therefore, the absence of turbidity in itself is not a reliable criterion to
judge a urine sample. Abnormal urine colour can be due to a large number of
causes (Tables1 and 2)[10]. In some conditions such as gross haematuria,
bilirubinuria, or chyluria , the examination of the urinary sediment allows us to
identify the cause of abnormal urine colour. It is best to examine the samples
within 3 hours of collection, to avoid bacterial overgrowth, dissolution of casts
and cells, and contamination from the environment. This is because in some
instances leukocytes can lyse in less than 1 hour especially in samples with a high
pH ( > 7.0) and/or a low specific gravity ( < 1.010). This can be prevented by
refrigeration of the samples at + 2 °C to + 8 °C[4,5]. However at these temperatures
phosphates and urates may precipitate with a masking of important sediments. A
possible alternative is the use of preservatives such as formaldehyde[11],
[image:20.595.79.561.549.685.2]glutaraldehyde[12] and cellfix[13].
Table 1 : The main causes of abnormal urine colour.
ENDOGENOUS CAUSES EXOGENOUS CAUSES
Haemoglobin Vegetable derived substances
Myoglobin Alimentary pigments
Bilirubin , biliverdin Drugs
8
Table 2 : Differentiation of the causes of changes in the colour of the urine.
COLOR CAUSES
Reddish brown Increased urobilinogen or porphyrins
Bright red Large amount of fresh blood
Pink Small amount of blood
Smoky brown Blood pigments
Brownish yellow or green Bile pigments
Milky white Chyluria
International guidelines recommend standardized procedures for
centrifugation and the subsequent steps of urine preparation and examination.
Centrifugation is used to concentrate the formed elements of the urine, but if it is
not performed properly, it may introduce relevant biases, mainly due to partial
recovery of the elements present in the urine. Gadeholt [14] showed that the best
recovery of erythrocytes and leukocytes was obtained at 2,500 r.p.m. (~ 1,120 g),
whilst a lower recovery was found at 1,000 and 3,000 r.p.m, using a centrifuge
with a radius of 16 cm and a centrifugation time of 5 min. Therefore, the yield is
strongly influenced by the speed of centrifugation. Other factors are the duration
of centrifugation and the volume of urine centrifuged. Hence the same
combination of speed and duration of centrifugation, as well as the same volume
of urine is to be used for obtaining reproducible results[15].The speed of
centrifugation is most often expressed as rotations per minute (rpm) or as “relative
centrifugal force” (RCF) or “g”. To calculate this, one must know the radius of the
centrifuge used. The RCF is obtained by the following formula [4]:
9
where: r = the radius in cm from the center of the spindle to the bottom of the
tube;
N = rotations per minute.
Centrifugation is important, for instance, for erythrocytic casts which, in
patients with isolated microscopic haematuria, we find in low numbers even in
centrifuged samples. After centrifugation, the supernatant is discarded. While in
many laboratories this is still done by pouring off but international guidelines
recommend removing a standardized volume of urine. This helps to standardize
the procedure and increases its reproducibility. To resuspend the pellet, the test
tubes were agitated gently by hand. A standardized volume of the resuspended
urine should be transferred to the slide.
Microscopic examination:
The urinary sediment is to be examined after obtaining the results for urine
protein level mainly. The knowledge of the dipstick results are also important
because it helps to direct the examination of the urinary sediment. At high specific
gravity, erythrocytes and leukocytes become smaller and at a specific gravity of ≤
1.010, erythrocytes and leukocytes swell and can undergo considerable lysis [16].
In addition, cytoplasmic Brownian movements and loss of nuclear segmentation
of leukocytes occurs [17]. In fact, a negative dipstick for haemoglobin, leukocyte
esterase, nitrites, or albumin has a high probability of being associated with
negative microscopy, while a dipstick positive for one or more such analytes
directs microscopy investigation towards the search of erythrocytes, leukocytes,
10
haemoglobin or leukocyte esterase but with no or only few erythrocytes or
leukocytes at microscopy, suggests cell lysis, which may be due to low urinary
specific gravity and/or high pH. In such a case, microscopy without dipstick
would give a false negative result. On the contrary, a case with negative dipstick
for haemoglobin or leukocyte esterase but with microscopy positive for
erythrocytes or leukocytes may be due to the presence in the urine of ascorbic acid
(which reduces the sensitivity of the pad for haemoglobin) or of cephalotine
(which reduces the sensitivity of the pad for leukocyte esterase) [2,3].
Once the slide is put under the microscope, it is to be examined without
delay to avoid changes due to the heat caused by the light beam of the microscope
or the drying up of the sample. The slide is to be examined at low magnification.
This is essential for an overview of the sample, and to analyse the distribution of
the elements. Casts tend to collect at the edges. Then, proceed to higher
magnification to identify the elements properly. Since these usually lie on
different planes, frequent adjustments of focus are necessary. For every case,
examine at least 20 random low and high microscopic fields. The following
microscopic particles were examined:
- erythrocytes (glomerular or non glomerular )
- leukocytes
- renal tubular epithelial cells
- transitional epithelial cells
- squamous epithelial cells
11
- casts with their subtypes
- other elements
The microscope for the examination of the urinary sediment must be of
good quality and equipped with at least a low magnification (e.g., x 100) and a
high magnification (x 400). Bright field microscopy has traditionally been used
for the analysis of urinary sediment, and is still widely used today [18]. However,
with this type of microscopy, all the elements of the urinary sediment are poorly
differentiated from the background with some exception for lipids, crystals, and
waxy casts. Therefore, particles with low refractive index such as hyaline casts
and erythrocytes with low haemoglobin content can easily be missed. In addition,
cellular details are poorly distinguishable. Some improvement may be obtained by
downward adjustment of the condenser, by closing the diaphragm of the
condenser. The urine can contain different types of cells, some of which derive
from the circulation, while others derive from the epithelia of the urinary system.
Other cells, such as podocytes [19] , basophilic leukocytes, platelets or monocytes
have also been described in urine. However, they were identified with
sophisticated techniques.
Erythrocytes :
Erythrocytes are a frequent finding in urine. Erythrocyte diameter,
refractivity index and morphology can vary under various conditions. The
diameter of erythrocytes ranges from 4.0 to about 10 μm, and influenced by
changes in specific gravity (or osmolality), increasing as specific gravity
12
about ≤ 1.010, the erythrocytes tend to undergo lysis, a fact which can cause false
negative results and discrepancies between microscopy and dipstick for
haemoglobin. The refractivity index of erythrocytes varies according to their
haemoglobin content. When this is very low, the erythrocyte is hardly discernible,
especially with bright field microscopy. In such a case, a thin cell membrane is the
only identifiable structure (the so-called “ghost cell”).
The morphology of urinary erythrocytes ranges from perfectly round cells
to particles with very changed shape. Fairley and Birch in 1982 [24] confirmed that
altered erythrocytes were typical of patients with Bright’s disease (i.e.,
glomerulonephritis).These investigators were the first to report in modern times
that in haematuria of glomerular origin, erythrocytes have an abnormal shape (the
so-called “dysmorphic erythrocytes”) , while in haematuria of non-glomerular
origin, erythrocytes have a normal appearance, similar to that of erythrocytes seen
in peripheral blood smears (the so-called “isomorphic erythrocytes”). Pollock
C.et.al confirmed the utility of examining urinary erythrocyte morphology [20].
The evaluation of urinary erythrocytes morphology is associated with certain
limitation [21] with lack of univocal criteria to define a haematuria as glomerular or
non-glomerular. In fact, the discriminating cut off was as low as 10% [22]. Koene
R.A.P.et.al.[23] defined a haematuria as glomerular when more than two
erythrocyte subtypes were found in the same sample. Köhler H.et.al. [25] defined it
when ≥ 5% “acanthocytes” were seen, which are doughnut-shaped dysmorphic
erythrocytes with one or more vesicle-like protrusions, which can be identified
13
The wide spectrum of appearances that erythrocytes may have in the urine,
in the category of both dysmorphic and isomorphic erythrocytes may lead to low
inter-observer reproducibility [26].
A non glomerular haematuria can be found in patients with a glomerular
disease due to gross haematuria [27], renal insufficiency, increased diuresis after
furosemide administration or necrotizing glomerulonephritis [28]. Haematuria is
considered as glomerular when we find ≥ 40% dysmorphic erythrocytes and /or ≥
5% acanthocytes [25] and/or ≥ 1 erythrocytic casts/50 low power fields. With this
approach, Fogazzi G.B.et al. have been able to find a close correlation with the
presence of glomerular changes at renal biopsy were present[29].
The cause of glomerular erythrocyte dysmorphism is not entirely known.
In vitro experiments have shown that neither osmolality nor pH changes of
solutions in which erythrocytes are suspended are sufficient to cause dysmorphic
morphology [30]. On the contrary, this can be produced if osmolality or pH
changes are coupled with the passage of erythrocytes through membranes with
pores having a diameter of 3.0 μm. In addition, erythrocytes develop dysmorphic
features if they are serially incubated with different solutions corresponding to
those of the different tubular segments, and finally are also incubated with a
solution containing a haemolytic substance, derived from red cell lysate [31]. These
data led to the hypothesis that in vivo erythrocytes become dysmorphic as a
consequence of a dual injury [32]. The first injury is thought to result from the
passage through “gaps” in the glomerular basement membrane, while the second
14
pH/osmolality changes or unidentified substances interfere with the ability of the
cells to regain their original shape. Rarely, urinary erythrocytes may have
morphological changes due to causes unrelated to glomerular diseases. Urinary
erythrocytes may have morphological changes due to causes unrelated to
glomerular diseases like in cases of haematuria caused by sickle cell disease,
whose urine can show sickle erythrocytes [33, 34], and in patients with urological
haematuria and concomitant iron deficiency anaemia, whose urine can contain
anisocytes and poikilocytes [35].
Leukocytes:
Neutrophils are the leukocytes most frequently found in the urinary
sediment. Typically they appear as round granular cells, granules representing
cytoplasmic organelles. Their diameter ranges from about 7.0 to 15.0 μm.
However, substantial differences in diameter and morphology may be caused by
differences in urine specific gravity or osmolality. In diluted urine, the cell is
larger and in case of concentrated urine, the identification of the lobulated nucleus
may be difficult. Occasionally, for unknown reasons, neutrophils may show blebs
protruding from the cell body or may have an elongated shape. On microscopic
examination of the sample, neutrophils undergo degeneration and transform into
larger cells with irregular shape and a thin transparent granular cytoplasm, hardly
distinguishable from the background. Neutrophils may also appear in clumps,
which is seen especially in urinary tract infection. Bacterial urinary tract infection
is the most frequent cause of neutrophiluria. They are seen in a wide spectrum of
15
interstitial nephritis, polycystic kidney disease, or urologic disorders. In women,
neutrophils may be found in the urine because of contamination by genital
secretions with presence of large amounts of squamous epithelial cells with or
without bacteria, Candida, or Trichomonas vaginalis.
Eosinophils too may be present in the urine. They can definitely be
identified only by using special stains like May-Grünwald-Giemsa, Wright’s or
Hansel’s stains. Eosinophiluria can be found in a wide spectrum of diseases
including acute interstitial nephritis caused by methicillin[37] urinary tract
infection, prostatitis, extracapillary glomerulonephritis, Henoch- Schonlein
purpura nephritis, acute allograft rejection or urinary schistosomiasis.
Eosinophiluria is now considered as an unspecific finding of much less diagnostic
importance [38].
Lymphocytes can be identified with certainty only with specific or general
stain preparations, such as Papanicolou’s stain. Lymphocyturia is considered as
an early and sensitive marker of acute cellular rejection in renal allograft
recipients [39,40,41]. It is also common in chyluria, a condition which is
characterized by “milky” urine [42].
Renal tubular epithelial cells:
The different segments of the renal tubules are lined by different types of
epithelial cells. Their size ranges from about 9.0 to 25.0 μm. Most of the renal
tubular epithelial cells (RTECs) in the urinary sediment are derived from the
proximal segments. These are round to oval or rectangular, have a large central or
16
abundant organelles, and a mean diameter of about 14.0 μm .Other RTECs from
distal tubules, are polygonal with a central nucleus and are smaller, and those
deriving from the collecting ducts have a columnar shape with a nucleus in the
basal position containing prominent nucleoli. At times, RTECs show degenerative
changes or appear in aggregates which indicates a particularly severe tubular
damage. RTECs are usually accompanied by elements indicative of parenchymal
renal disease such as casts, dysmorphic erythrocytes or lipids. RTECs are found in
disorders that primarily involve the tubules, such as acute tubular necrosis [43, 44],
acute interstitial nephritis [45] or acute rejection of a renal allograft. However, they
may also be seen in the urine of patients with glomerular diseases, as a
consequence of the tubular damage caused by inflammation and/or proteinuria.
Transitional epithelial cells:
Transitional epithelial cells derive from the urothelium, which lines the
urinary tract from the calyces to the bladder in women, and to the proximal
urethra in men. Transitional cells of the urothelium may have various shapes, but
they are mostly of ovoid or club-like appearance, having a central or peripheral
nucleus with one or two nucleoli, and a thin cytoplasm. Their longitudinal
diameter ranges from about 10.7 to 38.0 μm .Ovoid cells may at times be difficult
to distinguish from round or ovoid renal tubular cells. However, ovoid deep
transitional cells have a thinner cytoplasmic rim than renal tubular cells, and are
not associated with other particles suggestive of renal damage such as casts or
dysmorphic erythrocytes. Transitional cells are seen in large quantities (i.e. one or
17
layers of the urothelium such as urolithiasis, bladder carcinoma, or
hydronephrosis [46].
Squamous epithelial cells:
Squamous epithelial cells found in the urine mostly derive from the
superficial layers of vaginal epithelium. They are the largest cells in the urinary
sediment, their diameter ranging from about 17.0 to 118.0 μm. These cells are
quadrangular to polygonal in shape, and have a broad cytoplasm containing few
granules and a small central nucleus. Frequently, squamous cells are folded or are
aggregated in clumps.
Occasionally, bacteria are attached to their cell membrane , reflecting
colonization by bacteria. This process is thought to be an indispensable step
preceding urinary tract infection. If urine contains large numbers of squamous
cells, free nuclei of these cells are often seen, which represent remnant debris after
cell degeneration. Squamous cells are constantly shed from the urethra and
vagina, and small numbers are almost invariably present in the urinary sediment
of females. If urine is not collected properly (without spreading the labia and
without discarding the first portion of the voided urine), or if there is a vaginal
discharge, the squamous cells can be so abundant that proper analysis of the
18
Lipids:
In the urine sediment lipids appear as free lipid droplets, oval fat bodies,
fatty casts or cholesterol crystals. Free lipid droplets, isolated or in aggregates,
appear as translucent round particles of very variable size, with a bright yellow
colour. The oval fat bodies are macrophages [47] or renal tubular epithelial cells
with lipid droplets[48] . Fatty casts are cylinders which contain lipid droplets in
their matrix. The amount of lipids can vary from a few and isolated droplets to
tightly packed droplets, which mask the matrix of the cast. Cholesterol crystals are
thin, colourless and transparent plates with well-defined edges, which can be
isolated or in aggregates. Lipid droplets can usually be identified without
difficulty. However, larger fat globules may be confused with isomorphic
erythrocytes, yeasts or round calcium oxalate crystals. Lipids can also be
identified by stains such as Oil-Red O or Sudan III. Lipiduria can be found in
several renal diseases, but especially in nephrotic syndrome . In this condition,
lipiduria is due to free cholesterol, cholesterol esters, triglycerides, free fatty acids
and phospholipids, the main lipoprotein being represented by HDL[49]. However,
they may also be found in patients with non-nephrotic proteinuria, in some
patients with non- glomerular diseases [50] or in patients with polycystic kidney
disease and low grade proteinuria [51]. In the latter condition, the lipid droplets are
thought to derive from renal cysts containing degraded blood. In patients with
glomerular diseases, lipids enter the urine because of abnormal glomerular
19
tubular cells and transported for hydrolysis into lysosomes. Then, they re-enter the
tubular urine by active expulsion , or as a result of cellular breakdown.
Casts:
Casts are cylindrical elements of variable diameter and length which form
in the distal tubules and collecting ducts of the kidneys. They can also form in the
branching collecting ducts, as demonstrated by the occasional finding of branched
casts. The matrix of casts is made of Tamm-Horsfall glycoprotein (THG) which is
synthesized and secreted by the cells of the thick ascending limb of Henle’s loop.
THG contains 616 amino acids and carbohydrates, which account for
approximately 30% of its molecular weight. THG is the major protein of the
normal urine but its biologic role is still unclear [52]. Under several physiological
and pathological conditions, fibrils of THG tend to aggregate and to interweave
within the tubular lumen, forming a cylindrical structure. The formation of this is
favoured by low intratubular pH, high osmolality and high sodium concentration,
or by interaction with myoglobin, haemoglobin, Bence-Jones protein and other
substances. Initially, the forming cast remains anchored to the tubular cells by fine
fibrils, but subsequently it is washed away by the tubular urine flow and finally
reaches the bladder as a cast[53].
Casts may be hyaline, if they consist of THG only, or complex if they also
contain other elements. In fact, whichever particles are passing through the
tubular lumen during the formation of the cast (e.g., cells, lipids, granules, crystals
or microorganisms)they can be trapped in its matrix. This explains the large
20
significance .The final morphology of casts also depends on the diameter of
tubules in which they were formed. When the tubules are dilated, as in tubular
atrophy or renal obstruction, large casts are seen in the urine, a finding which is
therefore indicative of renal failure.
Since casts are formed in the renal tubules, all particles they contain derive
from the kidneys. Unfortunately, several types of casts of diagnostic importance
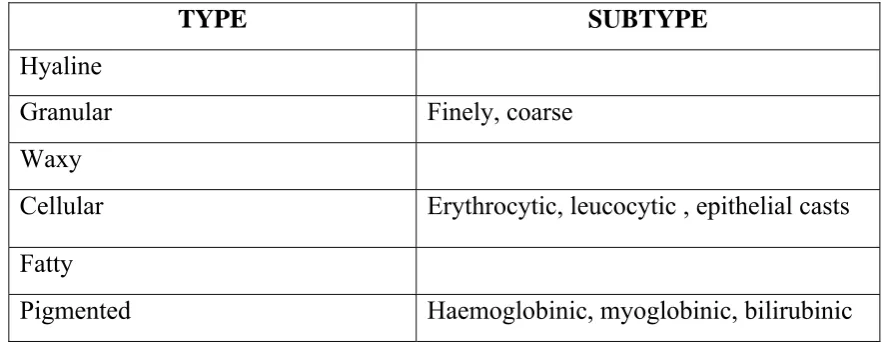
[image:33.595.86.528.310.481.2]are often not recognized in community or hospital based laboratories [54, 55].
Table 3: Classification of casts.
TYPE SUBTYPE
Hyaline
Granular Finely, coarse
Waxy
Cellular Erythrocytic, leucocytic , epithelial casts
Fatty
Pigmented Haemoglobinic, myoglobinic, bilirubinic
Hyaline casts:
Hyaline casts contain only THG, which confers a low refractive index.
Consequently, these casts may be overlooked if only bright field microscopy is
used. Variable amounts of hyaline casts can be found in the normal subject. They
can also be seen in subjects without renal disease after physical exercise, during
episodes of fever or dehydration, or during acute congestive heart failure.
Moreover, Imhof et al. [56] found transient abundant hyaline cylindruria after a
21
However, hyaline casts are also found in renal diseases, mostly in combination
with other types of casts [36] .
Granular casts:
Typical granular casts have their surface covered by granules which vary in
number and size. Granules can be fine or coarse, and clear, dark or pigmented.
Granules of casts are lysosomes containing reabsorbed ultrafiltered proteins
which, due to active expulsion from the tubular cell or tubular cell damage, fall
into the tubular lumen, where they are trapped in the matrix of the forming cast.
However, since granular casts are also found in renal diseases without proteinuria
such as acute tubular necrosis [57], it is accepted that granules might also derive
from cellular degeneration. Coarse granules are formed by degenerated cells such
as leukocytes or renal tubular epithelial cells [53]. The above mechanisms explain
why granular casts are usually not seen in the urine of normal subjects and why
their finding strongly indicates the presence of a renal disease. Granular casts,
together with renal tubular epithelial cell casts, are a distinguishing finding in
patients with acute tubular necrosis . However, they are also frequent in patients
with glomerulonephritis [36].
Waxy casts:
Waxy casts derive their name from their appearance, which is reminiscent
of melted wax. They have a high refractive index, dark colour, broad diameter and
hard, frequently indented and cracked edges. Occasionally, their surface is not
smooth but somewhat irregular. It has been claimed that waxy casts may derive
22
frequent finding in patients with renal failure, both acute and chronic. In few
patients with glomerular diseases without significant differences between
proliferative and non- proliferative histologic types [36].
Cellular casts:
Casts may contain different types of cells, namely erythrocytes, leukocytes
or renal tubular epithelial cells (RTEC). Therefore, cell-containing casts are
classified as erythrocytic, leukocytic and RTEC casts. The erythrocytes within the
cast may be so tightly packed that the matrix of the cast can hardly be seen and
individual erythrocytes can hardly be discernible. Alternatively, only a few
erythrocytes may be trapped in the hyaline matrix. The erythrocytes within the
casts can have a normal or reduced haemoglobin content (so-called “ghost”
erythrocytes), and can be either isomorphic or, more rarely, dysmorphic.
Erythrocytic casts are a marker of glomerular bleeding and should be examined in
all patients with isolated microscopic haematuria of unknown origin. In patients
with overt glomerulonephritis, erythrocytic casts are found in 85% of cases [23],
which depends on the types of glomerular disease investigated and on the
methodology used to search them. The prevalence being significantly higher in
proliferative disorders than in non proliferative ones. Together with dysmorphic
erythrocytes, erythrocytic casts are a distinguishing feature of the nephritic
sediment. Very rarely they may be found in patients with haematuria caused by
acute interstitial nephritis. The degradation of erythrocytes within the casts leads
to the formation of so-called haemoglobin casts, whose clinical significance is the
23
Leukocytic casts can contain variable amounts of leukocytes, from few to
so many that the matrix of the cast is completely masked .Leukocytes may be well
preserved or degenerated, in which case they are hardly distinguishable from renal
tubular epithelial cells. Leukocytic casts are found in patients with active
proliferative lupus glomerulonephritis [58], other glomerular diseases [36] or acute
interstitial nephritis.
Renal tubular epithelial cells (RTEC) casts, which are also known as
epithelial casts, can contain variable amounts of RTECs, from few to many .These
cells are identical to RTECs seen outside casts, which have a well evident nucleus
and a granular cytoplasm. However, when the cells are degenerated, these
distinguishing details are lost and differentiation between leukocytic casts and
RTEC casts can be impossible.
RTEC casts are found in all conditions associated with severe tubular
damage such as acute tubular necrosis [54] and acute interstitial nephritis of
whatever cause. However, these casts are a very frequent finding also in patients
with glomerular diseases.[36]
Fatty casts:
Fatty casts can contain lipid droplets (isolated or in clumps), oval fat
bodies or cholesterol crystals. The lipid droplets within the casts may be few,
small and scattered or so abundant and packed that they completely mask the
matrix of the cast. Cholesterol plates may at times protrude from the edges of the
24
sediment. Therefore, they are typical of patients with nephrotic range proteinuria
but also seen in patients without nephrotic range proteinuria [36].
Pigmented casts:
Pigmented casts includes haemoglobin, myoglobin and bilirubin casts.
Haemoglobin casts derive from erythrocytes which have undergone degeneration.
Haemoglobin casts have a typical brownish to reddish-brown colour and a
granular appearance.
Their identification is facilitated by careful focusing, which may reveal the
remnants of erythrocyte membranes. In typical cases, haemoglobin casts are
associated with erythrocytic casts and erythrocytes, and indicate renal bleeding.
Myoglobin casts have a brown to reddish-brown colour similar to that of
haemoglobin casts. The surface can be either smooth or granular, but careful
focusing does not show any remnants of erythrocytes. The knowledge of the
clinical context is indispensable to distinguish myoglobin casts from haemoglobin
casts. Myoglobin casts are seen in the urine of patients with acute renal failure
associated with rhabdomyolysis, which occurs in crush syndrome [59]. Casts of any
type i.e., hyaline, granular, waxy or cellular, may be stained by the typical yellow
colour of bilirubin. Bilirubin casts are observed in the urine of patients with
25
Other elements :
Pseudocasts:
Pseudocasts are particles which morphologically resemble casts without
being formed in the renal tubules. Many particles in the urine can resemble casts.
Among these crystals (especially when in clusters or aggregates), cells, mucus and
most frequently, contaminants such as cloth or synthetic fibres. Compared to
casts, pseudocasts may show harder edge, more irregular contours, more variable
size , unusual colours, differing from the colour due to haemoglobin, myoglobin
or bilirubin.
Mucus :
Mucus is a substance derived from the secretion of the accessory glands.
Usually, mucus appears as ribbon-like threads with irregular contours and fibrillar
structure. The fibrils tend to be larger and more loosely textured than fibrils seen
in hyaline casts. Less frequently, mucus threads aggregate to form large masses or
networks of fine fibrils. Occasionally, threads of mucus resemble hyaline casts
(pseudocasts). Cells may be trapped in mucus which leads to a grossly
inhomogeneous distribution across the slide .
Crystals:
Crystals are a frequent finding. There are many types of urinary crystals ,
such as common crystals like uric acid, amorphous urates and amorphous
phosphates, calcium oxalate, calcium phosphate, triple phosphate. Pathological
26
crystals due to drugs and other crystals like hippuric acid, calcium carbonate,
ammonium biurate.
Micro-organisms :
Several organisms can be identified in urinary sediments. Rods may be
isolated, in pairs or in long chains. The same is true for cocci . Rods and cocci are
easily identifiable, but sometimes cocci may be confused with amorphous urates
or phosphates but can be differentiated based on movement typical for cocci.
Bacteria may adhere to squamous epithelial cells, or clump into masses of
variable size. Urinary infection can reasonably be suspected if bacteria are present
in freshly voided midstream urine, particularly if numerous leukocytes are also
present. In women, bacteria and leukocytes in the urine can be due to
contamination from vaginal secretions, as a consequence, for instance, of
vaginitis. This situation is usually associated with massive amounts of squamous
epithelial cells with or without Candida and/or Trichomonas vaginalis. In urinary
tract infections with involvement of the kidney, besides leukocytes and bacteria,
leukocytic casts and even bacterial casts can be found. Yeasts are unicellular
organisms which reproduce by budding. Candida albicans is the most frequent
yeasts found in the urine. Candida appears as pale-green cells with smooth and
well-defined walls. The nucleus is at times visible, and the cytoplasm is
homogenous without apparent organelles. Round Candida cells may resemble
erythrocytes and some types of monohydrated calcium oxalate crystals, but
Candida are often nucleated and, especially, show budding. After letting the urine
27
clumps, can be seen. The most frequent cause of Candida in the urine sediment is
contamination by vaginal discharge in women with vaginitis. In this condition,
Candida is usually associated with massive amounts of squamous epithelial cells,
bacteria, and leukocytes .Candida, however, can also cause a true urinary
infection, especially in patients with diabetes mellitus, structural abnormalities of
the urinary tract, in-dwelling catheters, prolonged antibiotic treatment or
immunosuppression. Under these conditions, Candida in the urine may reflect
invasive candidiasis, which may cause urethritis, cystitis or renal infection. In case
of renal involvement, candidal casts can be found in the urine.
Patterns of urinary sediments:
Normal individual:
Many studies have been carried out on the urine sediment of normal
subjects. All studies showed that erythrocytes, leukocytes, renal tubular epithelial
cells and casts could be present. Casts ranged from zero to variable numbers[60].
Casts were almost invariably of the hyaline type, even though granular casts or
even epithelial casts could be found. Birch et al. studied the erythrocyturia of 376
healthy adult subjects [61]. Using samples centrifuged at 750 g for 5 min, a
Fuchs-Rosenthal counting chamber and a phase contrast microscope, it was found that
males gave a median count of 2,500 erythrocytes/mL (range 250-13,000/mL) and
a modal count of 2,000 cells/mL. Females gave a median count of 4,000
erythrocytes/ mL (range 250-16,000) and a modal count of 3,000/mL. Counts did
not appear to be age dependent. Since the 95% percentile was 8,000
28
8,000 erythrocytes/mL. Pollock et al. studied the excretion of erythrocytes of 27
healthy volunteers [20]. After centrifugation at 2,000 rotations per minute for 4
minutes, the cells were counted in a Fuchs-Rosenthal chamber using phase
contrast microscopy. The excretion rate of erythrocytes was < 1,000/mL (95%
confidence). Loh et al. studied the excretion of erythrocytes and leukocytes of 419
children [62]. Using uncentrifuged urine, a Neubauer counting chamber and phase
contrast microscopy, it was found that 95% of children excreted < 14 × 10 6
erythrocytes/L (i.e. < 14,000/mL) and < 4 × 106 leukocytes/L (i.e. < 4,000/mL).
Erythrocyturia was significantly higher in children aged 2-5 years, and leukocyte
excretion was significantly higher in females than in males (2.5 × 106/L versus 1.2
× 106/L). Interestingly, in the studies of Birch et al. [61] and of Loh et al. [62], the
morphology of erythrocytes was also evaluated. This was found to be consistently
dysmorphic, i.e. of glomerular origin. These results were confirmed partially by
Fasset et al., who studied 50healthy adult subjects and found that most subjects
had red cells similar to those seen in patients with glomerulonephritis, but many
also had some non- glomerular red cells [63]. Thus, these studies described give
very different figures in the excretion of erythrocytes and leukocytes in the urine
of the normal subject, and explains the different definitions of pathologic
microscopic haematuria which can be found in the literature [64, 65].The difference
in results may be partially explained by the methods used to collect, prepare and
analyse the urine samples were not the same in the different studies, and there
were large differences in the number of subjects studied. The difference in the
29
to the lack of consistent results, and may explain why several laboratories do not
provide normal values for urinary erythrocytes and leukocytes. Without these
figures, it is impossible to define microscopic haematuria or pathological
leukocyturia correctly, which is done by a careful selection of the subjects to be
studied and by using a standardized method for urine collection, handling and
analysis.
Minimal change disease and focal segmental glomerulosclerosis:
The urine findings in MCD and FSGS are those of the nephrotic syndrome
namely, marked proteinuria associated with variable numbers of renal tubular
epithelial cells (RTECs), marked cylindruria (hyaline, hyaline-granular, granular
and RTEC casts), and lipiduria. In MCD, lipiduria is less frequent than in other
glomerular diseases and microscopic haematuria is absent or mild. In primary
FSGS, microscopic haematuria is more frequent and less mild than in MCD. Any
deviation from the above patterns is suspicious. For instance, the sudden
appearance of RTECs and RTEC casts associated with a rapid decline of renal
function may point to superimposition of acute tubular necrosis, which in
nephrotic patients is often the consequence of hypovolaemia. The sudden
appearance of a severe microscopic haematuria and leukocyturia, accompanied by
a rise in serum creatinine, may suggest the presence of superimposed acute
interstitial nephritis, which occasionally is the result of diuretic treatment. The
sudden appearance of gross haematuria, particularly in the presence of unilateral
30
Membranous nephropathy:
Proteinuria in the nephrotic range is usually associated with microscopic
haematuria, heavy cylindruria, and lipiduria. The sudden appearance of gross
haematuria, with or without unilateral enlargement of the kidney, is suggestive of
renal vein thrombosis, which in membranous nephropathy is more frequent than
in any other glomerular disease. Rapid transformation into a full-blown nephritic
sediment, accompanied by a rise in serum creatinine, is suggestive of a possible,
although rare, superimposition of extra capillary proliferation [66].
IgA Nephropathy:
Proteinuria in nephrotic range with a mild to very severe haematuria , a
mild to moderate leukocyturia and few renal tubular epithelial cells . Erythrocytic
casts and fatty casts are the most frequent, being followed by renal tubular
epithelial cell casts and leukocytic casts, which are rare. Ibels et al. [67], who
studied 174 patients with IgA Nephropathy, and found increased red cells and
increased white cells in 94% and 46% of samples, respectively. Interestingly, they
also found that the total number of casts and the number of hyaline-granular casts
at presentation correlated significantly with the worsening of serum creatinine at
follow-up. Microscopic haematuria (defined as > 5% RBCs/HPF) was a marker of
IgAN also in the study by Nakayama et al.[68], who found it in 92% of 364
patients. These authors also observed that there was a significant correlation
between the total number of hyaline, granular, erythrocytic, leukocytic and fatty
casts and of oval fat bodies in the urine and the severity of the histological lesions.
31
isolated microscopic haematuria. Interestingly, when the morphology of urinary
red blood cells was evaluated in this disease, a mixed haematuria, containing
isomorphic and dysmorphic erythrocytes in the same proportion was found by
some investigators [24], while others found mainly dysmorphic erythrocytes or ≥
5% acanthocytes [25].
Membranoproliferative glomerulonephritis:
A wide spectrum of urinary changes is possible in MPGN of whatever
type. These include isolated dysmorphic microscopic haematuria, microscopic
haematuria and proteinuria, nephrotic syndrome and macroscopic haematuria.
Thus, the finding of a nephritic or of a nephritic and nephrotic sediment is not
uncommon in patients with MPGN. Interestingly, in a large study on the
prognostic factors of primary MPGN [69], it was found that the presence of
granular casts in the urine at baseline correlated significantly with the logarithm of
serum creatinine, the degree of proteinuria and albuminaemia, and with acute
tubular damage, mesangial sclerosis, and glomerular crescents or necrosis at renal
biopsy. In addition, it was found that patients with urinary granular casts had a
significantly higher probability of progression to end stage renal failure at 3 years
than the patients without granular casts.
Acute post-streptococcal glomerulonephritis:
In the acute phase, the urinary findings correspond to those of a full-blown
nephritic syndrome .However, as in lupus nephritis, diffuse and active glomerular
changes may occasionally be associated with normal or only mildly altered
32
disappear by the end of the first year, but in some isolated microscopic haematuria
may persist for years.
Extra capillary glomerulonephritis:
In the active phase, extra capillary glomerulonephritis is typically
associated with rapidly progressive renal failure, mild to moderate proteinuria and
the most severe haematuria which can be observed in patients with
glomerulonephritis. When the glomerular lesions heal with appropriate therapy,
erythrocytes and erythrocytic casts usually decrease to complete disappearance.
Thus, in extracapillary glomerulonephritis, the examination of the urinary
sediment is a valuable tool for the evaluation of the activity or inactivity of the
disease, with relapses frequently being heralded by the appearance of an active
sediment and a rise in the number of urinary erythrocytes. One must be aware that
these findings can be observed in whatever type of extra capillary
glomerulonephritis, including Goodpasture’s syndrome. Interestingly, the latter
condition can occasionally occur with only mild microscopic haematuria with or
without mild proteinuria, in spite of a clear cut linear deposition of IgG in the
kidney [71].
Lupus nephritis:
The finding of persistent proteinuria > 0.5 g/24 hours (or > 3+ if
quantification is not available) or of cellular casts including red blood cell,
haemoglobin, tubular, granular, or mixed in the urine sediment, are among the
criteria of the American College of Rheumatology for the diagnosis of systemic
33
patients with known or suspected lupus should undergo urinalysis at regular
intervals[73].The examination of the urinary sediment with the assessment of
proteinuria and of serum creatinine is mandatory for the identification of renal
flares and the guidance of therapeutic intervention [74]. Urinary sediment
examination is also useful for recognizing the severity of the renal disease. As a
general rule, the milder the renal lesions the fewer the urinary changes, and vice
versa [75], though there are exceptions however. Thus, in active class III and class
IV lupus nephritis, discrete to severe proteinuria is almost invariably present,
while the sediment reflects the inflammatory injury of the glomerulus.
Consequently, it comprises a frequent and moderate to severe erythrocyturia, mild
to moderate leukocyturia, a few RTECs, and abundant and pleomorphic
cylindruria, including erythrocytic casts in the vast majority of patients. However,
rare cases of active lupus nephritis with minor urinary changes and inactive
sediment can occur.
When the disease is controlled by therapy, the former elements usually
decrease or disappear. Reappearance of erythrocyturia and, especially, of cellular
casts, quite often indicates imminent relapse. In patients with the LN class V,
proteinuria is usually, but not always, marked. In contrast with class III and IV
LN, microscopic haematuria, leukocyturia, erythrocytic casts and leukocytic casts
may be either absent or mild. A change in the amount of proteinuria and/or the
character of the urinary sediment may indicate a change in the type of glomerular
lesions with transformation into another class [75]. In a lupus patient with a
34
absence of inflammatory changes of the sediment correctly, since this finding
usually indicates that progressive renal failure is due to non-immune mechanisms
which will not respond to immunosuppression.
Schönlein-henoch purpura nephritis:
A minority of patients have only dysmorphic microscopic haematuria,
which can be transient and of short duration. About 50% of patients have
persistent microscopic haematuria and proteinuria. In patients with nephrotic
syndrome, there is usually mild haematuria associated with abundant cylindruria
and fatty particles. In patients with nephritic syndrome and extracapillary
proliferation at renal biopsy, the sediment shows severe erythrocyturia and
cylindruria including erythrocyte/haemoglobin casts. About 20% of patients,
however, present with both nephrotic and nephritic sediment. In some patients,
urinary changes recur or worsen during, or shortly after, skin rash recurrences [76].
Diabetic nephropathy:
Initially, only microalbuminuria is found, the detection of which
necessitates the use of specific methods such as immunochemical assays utilizing
anti-albumin antibodies, high performance liquid chromatography, or appropriate
dipsticks. In advanced stages, non-selective proteinuria develops .Urinary
sediment is usually defined as unremarkable in DN, apart from some occasional
erythrocytes. However, a number of studies have shown that microscopic
haematuria is not uncommon in diabetic nephropathy, being found in 15% to 35%
of patients with biopsy-proven DN associated with type 2 diabetes mellitus [77,78].
35
found in 62% of patients with clinically diagnosed DN, a prevalence which
increased to 82% when three consecutive samples from the same patients were
analyzed [79]. Interestingly, ≥ 5% acantocyturia, a marker of glomerular bleeding,
was found in only 4% of diabetic patients in contrast with 75% of patients with
glomerulonephritis. This finding makes the origin of microscopic haematuria in
DN largely unclear. Besides microscopic haematuria, it should be remembered
that the appearance of an active urine sediment with many erythrocytes,
leukocytes and pleomorphic cylindruria in a diabetic patient should always be
considered as a possible sign of superimposed proliferative and active
glomerulonephritis such as IgAN, acute post-infectious glomerulonephritis, or
extracapillary glomerulonephritis [80]. Leukocyturia associated with bacteriuria is
suggestive of urinary tract infection which, in diabetes, is frequent and may be
associated with pneumaturia i.e., the passage of gas into the urine due to bacteria
such as Escherichia coli and Enterobacter aerogenes [81]. Another complication of
urinary tract infection in diabetics is septic papillary necrosis, which can present
with flank pain, gross haematuria and papillary fragments in the urine. Candida is
also frequently found in the urine of diabetic patients.
Nephropathies due to plasma cell dyscrasias:
In patients with myeloma cast nephropathy, proteinuria is mainly due to the
excretion of monoclonal light chains (the so-called Bence Jones proteinuria),
which are identified by immunefixation. It is important to remember that light
chains are not detected by dipsticks commonly used for urinalysis. In fact, these
36
light chains. On microscopy, myeloma cells appears with oval to round eccentric
nuclei showing peripheral clumping of nuclear chromatin, prominent nucleoli and
a high nucleus/cytoplasm ratio. Myeloma casts i.e., casts surrounded by
multinucleated cells, may also be seen [82].Patients with amyloidosis or light chain
deposition disease usually have proteinuria in the nephrotic range, which is
mainly of the glomerular type. Thus, the urinary sediment usually contains
abundant cylindruria (hyaline, hyaline-granular, granular, and RTEC cell casts)
and lipiduria. In amyloidosis, microscopic haematuria is usually absent. In both
amyloidosis and light chain deposition disease, the appearance of a nephritic
sediment may herald the superimposition of extra capillary proliferation.
Acute interstitial nephritis:
In AIN caused by antibiotics especially beta lactam drugs the proteinuria is
usually mild. Leukocyturia and haematuria are found in all patients in the
full-blown phase. Eosinophiluria seems to be always present. In AIN due to
non-steroidal anti-inflammatory drugs ( NSAIDS), due to the concomitant glomerular
disease, proteinuria is a constant finding, and frequently it is in the nephrotic
range with leukocyturia, haematuria or casts (hyaline, granular, waxy, containing
leukocytes but not erythrocytes) on sediment examination. In AIN associated with
bacterial infections, proteinuria is frequent but is usually < 1.5g/24 hours.
Microscopic haematuria is almost invariably seen but leukocyturia is rare.Of the
idiopathic forms, AIN associated with uveitis is the best characterized variety.
Proteinuria of < 1 g/24 hours is almost invariably present, which is caused by
37
both, but it may even be normal. In only a few patients has eosinophiluria been
found.
Two aspects of urinary sediment in AIN deserve a separate comment.
Eosinophiluria is usually considered as a marker of AIN. Old studies support this
view as well as several case reports in which AIN was caused by a wide spectrum
of drugs including ciprofloxacin, omeprazole, vancomycin, fluindione, or
linezolid. However ,one should consider that AIN encompasses a heterogeneous
group of diseases, and that eosinophiluria has a different prevalence in the
different forms. In fact, it seems to be more frequent in AIN associated with
antibiotics than in other types. In addition, with the use of Hansels’s stain, which
is more specific and sensitive than traditional Wright’s stain, eosinophiluria has
been found in a wide spectrum of disorders, including several types of
glomerulonephritis, prostatitis, chronic pyelonephritis, renal cholesterol
embolism, urinary schistosomiasis, etc. It is commonly thought that erythrocytic
casts are so rare in AIN that their presence should suggest the diagnosis of a
glomerular disease [83, 84]. Interestingly, erythrocytic cylindruria was associated
with many erythrocytic casts within the tubules at renal biopsy. In addition,
erythtrocytic casts have been found in 4/12 patients (33%) with AIN by Köhler et
al. [25]. Thus, the possibility that erythrocytic casts can be found in the urine of
38
Chronic interstitial nephritis:
In spite of the heterogeneous nature of CRIN, the urinary changes are
rather uniform. They are represented by the excretion of proteins of low molecular
weight such as β2- microglobulin, concentration and/or acidification defects, and
loss of glucose, bicarbonate, uric acid, phosphate and amino acids. The urinary
sediment may be normal or only mildly changed, containing sparse leukocytes
and a few hyaline or hyaline-granular casts, while microscopic haematuria is
uncommon. Analgesic nephropathy (AN) is the best studied form of CRIN. It is
characterized by early urinary concentration and acidification defects, with
proteinuria which is usually < 1 g/24 h, microscopic haematuria, as well as
leukocyturia. A sudden appearance or a worsening of haematuria and
leukocyturia, or even the appearance of gross haematuria in association with
lumbar colicky pain may indicate renal papillary necrosis. This event can also be
seen in diabetic patients usually in conjunction with a urinary tract infection,
sickle cell disease, renal tuberculosis, and urinary tract obstruction. When
papillary necrosis is suspected, fragments of the necrotic papilla should be looked
for in the urine, especially by the use of a filter paper or a gauze .A worsening of
haematuria with or without atypical urothelial cells may also be due to
uroepithelial cancer, whose incidence is increased in AN. Therefore, in patients
with AN the serial examination of urinary sediment is useful to reveal possible
39
Acute tubular necrosis:
In ATN, urine sediment shows variable numbers of RTECs, both necrotic
and viable, at times even fragments of the tubular epithelium, and abundant
cylindruria (granular casts and RTEC casts). In addition, depending on the cause
of the tubular damage, other particles can be seen. These other particles are
important in identifying the cause of the acute kidney injury. Thus the presence of
brownish pigmented casts in urine which does not contain erythrocytes suggests
ATN from myoglobinuria or haemoglobinuria. The presence of a massive
crystalluria can suggest ethylene glycol poisoning (which causes atypical
spindle-like monohydrate calcium oxalate crystals) [85], acute uric acid nephropathy
(which causes uric acid crystals), or ATN due to intra-renal precipitation of a
drugs in which the crystalluria can be either morphologically atypical (which may
be caused by sulfadiazine, amoxycillin, acyclovir, indinavir, felbamate, etc.) or
due to calcium oxalate (which may be caused by vitamin C, naftidrofuryl oxalate,
or orlistat).
The presence of severe haematuria associated with erythrocytic casts
strongly suggests a primary or secondary proliferative glomerulonephritis in an
active phase [86]. In addition to all this, in recent times, several urinary biomarkers
have been proposed for the early diagnosis of ATN and are currently under
investigation. These include interleukin 18, kidney injury molecule 1, and tubular
enzyme such as the intestinal form of alkaline phosphatase, N-acetyl-β
40
Interpretation of sediment findings:
The nephrotic sediment is observed in patients with nephrotic syndrome.
This is a condition characterized by proteinuria of > 3.5 g/24 hour associated with
hypoalbuminaemia, hypercholesterolaemia, and variable oedema. In most
instances, nephrotic syndrome is caused by glomerulopathies which at renal
biopsy have little or no evidence of glomerular inflammation (e.g., absence of
intra- or extra-capillary cell proliferation, necrotizing lesions, or insudation with
polymorphs and/or mononuclear cells).Any glomerular disease may cause a
nephrotic syndrome, but the most common are minimal change disease (MCD),
focal segmental glomerulosclerosis (FSGS), idiopathic membranous nephropathy,
diabetic nephropathy, membranous lupus nephritis, amyloidosis and light chain
deposition disease. Lipiduria and marked cylindruria, especially fatty casts and
renal tubular epithelial cell (RTEC) casts, are the hallmarks of the nephrotic
sediment. Microscopic haematuria is variable according to the type of
glomerulopathy. Usually, it is absent or mild in minimal change disease, while it
is more frequent in focal segmental glomerulosclerosis and idiopathic
membranous nephropathy, and it is variable in diabetic nephropathy. In these
conditions, leukocyturia is uncommon and, if present, mild .Although lipiduria is
the distinguishing feature of the nephrotic sediment, this is not invariably present .
Lipids enter the urine because of impaired glomerular basement membrane
permeability, their passage through the glomerular barrier being also influenced
by the selectivity of proteinuria (the higher the selectivity the lower the lipiduria).
![Table 4 : Quantification of urinary sediments. [102]](https://thumb-us.123doks.com/thumbv2/123dok_us/182521.52296/66.595.69.552.100.299/table-quantification-urinary-sediments.webp)
![Table 6: Correlation coeffecient and its interpretation.[103]](https://thumb-us.123doks.com/thumbv2/123dok_us/182521.52296/68.595.86.547.129.271/table-correlation-coeffecient-and-its-interpretation.webp)
![Table 12: Urine sediment scoring by Lakhmir S.Chawla.et.al.2008 [93]](https://thumb-us.123doks.com/thumbv2/123dok_us/182521.52296/79.595.98.518.72.239/table-urine-sediment-scoring-lakhmir-s-chawla-et.webp)