An Index of Child Well-being in the European Union
Full text
Figure

Related documents
However, the results observed in Figures 9-16 for Ka-band and V-band both uplink and downlink at 0.001% and 0.01% unavailability of time, interference will occur in all 37 locations
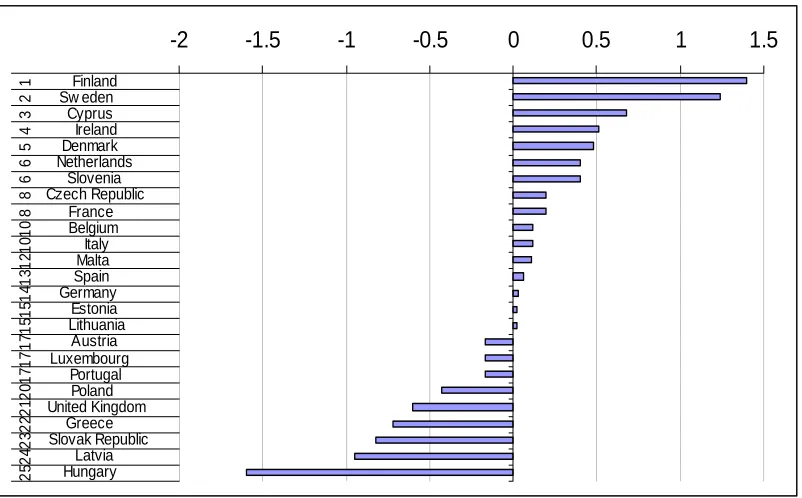
Finland Sweden Netherlands Lithuania Luxembourg Spain Denmark Latvia Poland Austria Czechia France Estonia Croatia Slovenia Ireland Romania Slovakia United Kingdom Belgium
Without prejudice to legal requirements, or to any limitations imposed by CaixaBank that may be applicable, permission is hereby expressly refused for any type of use or
Mirya Holman received her PhD from Claremont Graduate University in American Politics and Public Policy and her BA from Loyola University New Orleans in Political Science and
In the current study, application of Adper Single Bond Plus following two types of surface treatments yielded the highest bond strength with no significant
Other previous studies (i.e. The current study was intended to integrate the various factors of knowledge sharing’s attitudes in the context of the hotel industry. The study aims
The best linear unbiased estimator (BLUE) for the population mean under moving extreme ranked set sampling (MERSS) is derived for general location and scale parameters of
Once your complete thesis meets your advisor’s approval, you can distribute copies to all committee members and schedule the thesis defense meeting..
