Collaborative Care for Children With
ADHD Symptoms: A Randomized
Comparative Effectiveness Trial
Michael Silverstein, MD, MPHa, L. Kari Hironaka, MD, MPHa, Heather J. Walter, MD, MPHb, Emily Feinberg, ScDa,c, Jenna Sandler, MPHa, Michelle Pellicer, MPHa, Ning Chen, MAa, Howard Cabral, PhD, MPHd
abstract
OBJECTIVES:Although many attention-deficit/hyperactivity disorder (ADHD) care models havebeen studied, few have demonstrated individual-level symptom improvement. We sought to test whether complementing basic collaborative care with interventions that address common reasons for symptom persistence improves outcomes for children with inattention and hyperactivity/impulsivity.
METHODS:We conducted a randomized comparative effectiveness trial of 2 care management systems for 6- to 12-year-old children being evaluated for ADHD (n= 156). All participants received care management with decision support. Care managers in the enhanced care arm also were trained in motivational and parent management techniques to help parents engage in their child’s treatment, address their own mental health needs, and manage challenging child behaviors. We used multivariable models to assess inattention, hyperactivity/impulsivity, oppositionality, and social skills over 1 year.
RESULTS:Both treatment arms generated guideline concordant diagnostic processes in 94% of cases; 40% of children had presentations consistent with ADHD. For the entire sample, there were no differences in symptom trajectories between study arms; mean differences in change scores at 12 months were–0.14 (95% confidence interval–0.34 to 0.07) for inattention;–0.13 (–0.31 to 0.05) for hyperactivity/impulsivity;–0.09 (–0.28 to 0.11) for oppositionality; and 3.30 (–1.23 to 7.82) for social skills. Among children with ADHD-consistent presentations, enhanced arm participants experienced superior change scores for hyperactivity/impulsivity of–0.36 (–0.69 to–0.03), oppositionality–0.40 (–0.75 to –0.05), and social skills 9.57 (1.85 to 17.28).
CONCLUSIONS:Among children with ADHD-consistent presentations, addressing barriers to engagement with care and challenging child behaviors has potential to improve the effectiveness of collaborative care.
WHAT’S KNOWN ON THIS SUBJECT:Collaborative care is known to be an effective system to manage child behavioral health conditions in the primary care setting.
WHAT THIS STUDY ADDS:Among urban children with attention-deficit/hyperactivity disorder, using lay care managers to address barriers to engagement with care and challenging child behaviors has the potential to improve the effectiveness of conventional collaborative care.
Departments ofaPediatrics, andbPsychiatry, Boston University School of Medicine, Boston Medical Center, Boston,
Massachusetts; and Departments ofcCommunity Health Sciences, anddBiostatistics, Boston University School of Public Health, Boston, Massachusetts
Attention-deficit hyperactivity disorder (ADHD) affects 8% to 12% of US school-aged children.1Far more
children, however, demonstrate functionally impairing inattention or hyperactivity/impulsivity, but do not meet full diagnostic criteria for ADHD. Although most children with ADHD symptoms are managed by their primary care provider,2,3
diagnostic processes and treatment plans in this setting often fail to uphold evidence-based standards.4
To address this gap between evidence and practice, a number of ADHD care management models have been developed. These models have focused largely on communication of patient data or assistance with medical decision-making (decision support) and have succeeded in improving guideline adherence for ADHD diagnosis and management.5–7
There is a paucity of literature, however, on the impact of these care models on individual level outcomes.
One approach to improving outcomes is to augment evidence-based models of care with lay-delivered
interventions designed to address specific reasons for lack of clinical improvement. This approach could be particularly important for low-income and minority children, who have limited access to mental health specialists and often receive their care in underresourced settings.8,9
Although many reasons for symptom persistence exist, 3 reasons may be particularly salient for urban children. First, engagement with behavioral health care is often problematic.10–14
Second, low-income parents, particularly those of inattentive or hyperactive/impulsive children, have an increased prevalence of depression and adult ADHD,15which have been
associated with poorer child symptom trajectories.16,17Third, behavioral
comorbidities, particularly
oppositionality, are highly prevalent among low-income populations, and can limit the effectiveness of strategies designed to address core ADHD symptoms.18,19
In this context, we conducted a randomized comparative
effectiveness trial to test the hypothesis that augmenting a basic collaborative care system (whereby primary care clinicians work with specialists via care manager intermediaries) with
interventions to address specific reasons for protracted symptoms could improve outcomes for low-income children with inattention and hyperactivity/impulsivity. Because we were interested in real-world applicability in a Medical Home context,20all care management
processes were conducted by lay providers without formal mental health backgrounds; and study procedures, whenever possible, adhered to principles of effectiveness research.21
Because we were interested in symptomatic improvement among all children presenting to primary care with relevant behavioral concerns, we enrolled subjects at the point of initiation of an ADHD workup, as opposed to the point of diagnosis.
In our 2-arm trial, all participants received care management and decision support, based largely on evidence-based collaborative care models that have been applied to different clinical populations.22,23
Care managers in the enhanced study arm also were trained in motivational interviewing techniques to help parents engage with care for their children, and to seek care for their own behavioral health concerns.24
These care managers also were trained in Triple P’s Primary Care module, a series of techniques effective in reducing coercive parenting and behavioral problems in children.25–27We followed families
for 1 year and measured children’s inattention, hyperactivity/impulsivity, oppositionality, and social skills.
METHODS
Study Design and Setting
We conducted a 2-site, parallel-group comparative effectiveness trial with 1:1 randomization. Both sites were
urban primary care pediatric practices serving low-income
populations: one, within an academic medical center; the other,
a community health center.
Participants
We recruited 6- to 12-year-old children, whose primary care provider initiated an evaluation for ADHD based on parental report of inattentive or hyperactive/impulsive behavior. Those with existing ADHD diagnoses, documentation of autism spectrum or bipolar disorder, and those already receiving care from a pediatric neurologist, psychiatrist, or developmental-behavioral pediatrician were excluded. We restricted our sample to English- and Spanish-speaking families.
Recruitment and Enrollment
We enrolled participants from October 2010 to July 2013. To emulate real-world circumstances, primary care providers initiated evaluations for ADHD at their own discretion, and made referrals via the electronic medical record for care management. A central coordinator offered care management services, irrespective of participation in the trial. Those participating in the trial subsequently met with study staff, who obtained written informed consent.
Randomization
Interventions
Both study arms were modeled on the concept of collaborative care. We retained lay care managers
(bachelor’s or master’s level) without formal mental health training or clinical experience. Care managers’ responsibilities were threefold:first, they obtained symptom reports, by using the Vanderbilt ADHD Diagnostic Rating scales,28from both parents
and teachers. These scales were obtained as part of the initial diagnostic process, and the ongoing monitoring process for those with ADHD-consistent presentations. To obtain teacher ratings, care managers sent forms, along with a signed release, to a centralized school administrator who in turn contacted teachers. Second, care managers received brief training in medical history taking, and obtained clinical information from families on behavioral symptoms and social and family history. Third, care managers served as liaisons between primary care providers and a decision support panel consisting of 1 child
psychiatrist (HJW), 1 developmental-behavioral pediatrician (LKH), and 1 primary care pediatrician.
Decision support focused on whether clinical presentations were consistent with ADHD (combined, inattentive, hyperactive/impulsive, or not-otherwise-specified types), or whether alternative diagnoses should be entertained. An“ADHD-consistent presentation”was defined as meeting
Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, symptom criteria on both the parent and teacher Vanderbilt scales, in the absence of a plausible alternative explanation for the child’s symptoms, as determined from narrative clinical information. If an ADHD diagnosis was confirmed by the primary care provider, the decision support team provided guideline-concordant pharmacological guidance,29and
advice on monitoring and treating to a target symptom score. Decision
support was phrased in nonspecific terms: for example, if a suggestion was made to start a stimulant medication, a specific medication was not named. For those with ADHD-inconsistent presentations, the decision support team provided guidance about diagnostic next steps. The electronic health record provided the medium for communication.
Enhanced care managers received additional training to address 3 common reasons for ADHD symptom persistence: ambivalence toward engagement with behavioral health care,14parental mental health,30and
oppositional child behavior.18To
address thefirst 2, care managers were trained in motivational interviewing31
and followed a standardized script to resolve ambivalence toward treatment. Consistent with previous work,25care
managers used motivational interviewing principles to explore parents’stressors, and to offer referrals to adult behavioral health services if indicated. Last, enhanced care managers were certified by a master trainer in Triple P’s Primary Care module. Whereas basic care managers conducted their work in person only until the initial diagnostic decision support meeting (and by telephone thereafter), enhanced care managers met with clients in person as often as necessary to accomplish these aims.
Intervention Training and Fidelity All enhanced care managers underwent a 5-day training in motivational interviewing conducted by a trainer certified by the
Motivational Interviewing Network of Trainers, and were judged to have appropriate skills on assessment of videotaped interactions with standardized patients. Because our study was an effectiveness trial, we took an unobtrusive approach to care manager supervision andfidelity monitoring.21Skills were maintained
through weekly supervision sessions with a social worker and through annual booster sessions with the motivational interviewing trainer.
During these annual sessions, the trainer assessed skills based on a standard set of criteria consistent with best practices in motivational interviewing.31Triple P training
involved a commercially available training and certification module. We implemented Triple P as it would be in a real-world practice setting and did not deploy any additional training than provided in the original module.
Measures and Outcome Assessment At baseline, we recorded the age and gender of all children. We chose our outcome measures to be congruent with the Multimodal Treatment of ADHD Study,32a seminal study
comparing treatment approaches for children with ADHD. We used the Swanson, Nolan, and Pelham (SNAP-IV) scale to assess behavioral symptoms. This scale, which has a range of 0 to 3, has a factor structure that includes 2 ADHD subscales (inattention and hyperactivity/ impulsivity) and an oppositionality subscale.33We used standard scores
from Social Skills Rating System to assess children’s social skills.34For
adult caregivers, we assessed age, relationship to the child, marital and work status, education, and race and ethnicity. We assessed caregiver depressive symptoms by using the Quick Inventory of Depressive Symptoms35; adult ADHD symptoms,
by using the Adult ADHD Self-Report Scale36; and health literacy, by using
the Brief Test of Functional Health Literacy.37For each measure, we used
published clinical cutpoints.
Our primary outcome was ADHD symptoms, measured by parent SNAP-IV report, 6 and 12 months after randomization. Secondary outcomes included oppositional symptoms and social skills.
Statistical Analysis
We conducted an intention-to-treat analysis, excluding 1 subject who was found to be ineligible
from baseline for inattention, hyperactivity/impulsivity,
oppositionality, and social skills, we used 2-samplet-tests.
By using multivariable linear regression models, we assessed differences in symptom changes across intervention groups, accounting for relevant baseline differences, and enrollment site as afixed effect.38We calculated
standardized effect sizes as the adjusted difference between groups divided by the pooled SD, by using the Cohen d statistic. We conducted stratified analyses to determine if there was differential impact among children whose presentations were consistent, or inconsistent, with ADHD. We assessed effect modification by ADHD-consistent presentation by entering treatment arm–by–ADHD interaction terms into the models. Because outcomes data were missing in only 9% of subjects, we employed no special techniques to handle missing data.
To explore possible intervention mechanisms of action, we
supplemented the intention-to-treat analysis with an as-treated analysis, in which we divided the sample into those receiving no enhanced care sessions, those receiving 1 to 3 sessions, and those receiving 4 to 5 sessions, irrespective of random assignment. We analyzed differences in outcomes via analysis of variance, restricting this analysis to 12-month outcomes because all intervention “doses”had been delivered by this time. We used thex2test to assess differences between study groups in ADHD medication prescription receipt and receipt of specialty behavioral health services. Small cell sizes precluded formal
mediation analyses or multivariable modeling of potential mechanistic pathways.
Sample Size
We estimated our sample size to generate adequate power to test
a clinically significant difference across intervention arms on decreasing SNAP-IV scores over 12 months. We assumed from the Multimodal Treatment of ADHD study that at baseline, SNAP-IV scores would average 2.2 (SD 0.70).39We
assumed that among subjects in the basic arm, follow-up scores would average 1.8 at 6 months and 1.4 at 12 months; in the enhanced arm, 1.7 at 6 months and 1.1 at 12 months, differences in score trajectories considered clinically significant.42,43
We assumed a 2-sidedaof 0.05, 80% power, and 10% loss to follow-up, leading to our goal of randomizing 156 subjects.
The Boston University Medical Center Institutional Review Board approved this study (Clinical Trials.gov NCT01275378).
RESULTS Enrollment
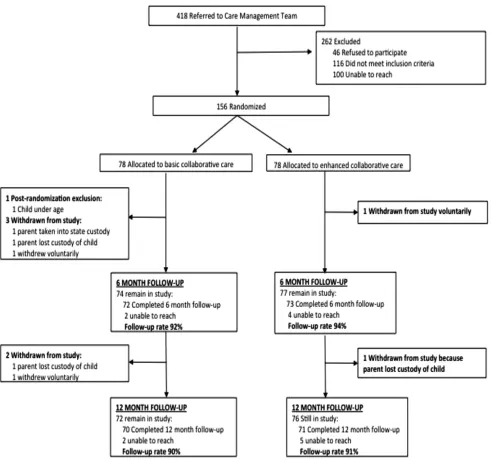
Primary care providers referred 418 children to the central coordinator (Fig 1). Of these, 116 did not meet inclusion criteria, 100 could not be contacted, and 46 refused to
participate. Of the 156 subjects in the trial, 114 were recruited from the hospital clinic. One subject in the basic care arm was found to be ineligible after randomization and excluded. Of the 155 eligible, randomized subjects, 141 (91%) were assessed at the 12-month follow-up point.
Baseline Characteristics Our sample of children was predominantly male (69%), with a mean age of 8.73 years (SD 2.07). The sample was 60% black and 27% Latina. Most baseline characteristics were balanced between the 2 study groups (Table 1); however, whereas 76% of caregivers in the enhanced care arm had attained a high school diploma, 63% in the basic care arm had. Overall, randomization appeared to be effective.
Baseline child inattention, hyperactivity/impulsivity, oppositionality, and social skills scores reflected a study population with the expected behavioral challenges. Based on SNAP-IV norms, 54% of the children in the sample scored in the top 5%, nationally, for inattention; 68%, in the top 5% for hyperactivity/impulsivity; and 31% in the top 5% for oppositionality. The mean rank of children in our sample for social skills was the 23rd percentile nationally. None of these scores differed between intervention groups at baseline.
Process Data
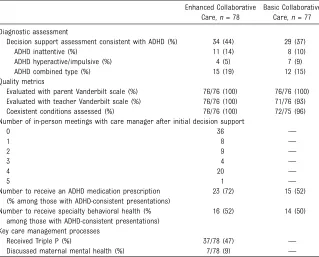
Initial steps of the ADHD diagnostic process for children in both care groups adhered well to established quality metrics, including evaluation with symptom inventories and assessment of comorbid conditions (Table 2). Overall, 40% of cases were judged to be consistent with ADHD. By design, basic care managers did not meet with families in person after initial decision support was
provided; by contrast, enhanced care managers had up to 5 in-person follow-up meetings (mean, 1.58; SD 1.73) with their clients. All enhanced care managers were deemed to have maintained motivational interviewing skills throughout the study period. Thirty-seven study parents (47%) in the enhanced care arm engaged in at least 1 aspect of Triple P; 7 parents (9%) engaged in a discussion about their own mental health. There were no known adverse events in either arm.
Inattention, Hyperactivity/ Impulsivity, Oppositionality, and Social Skills
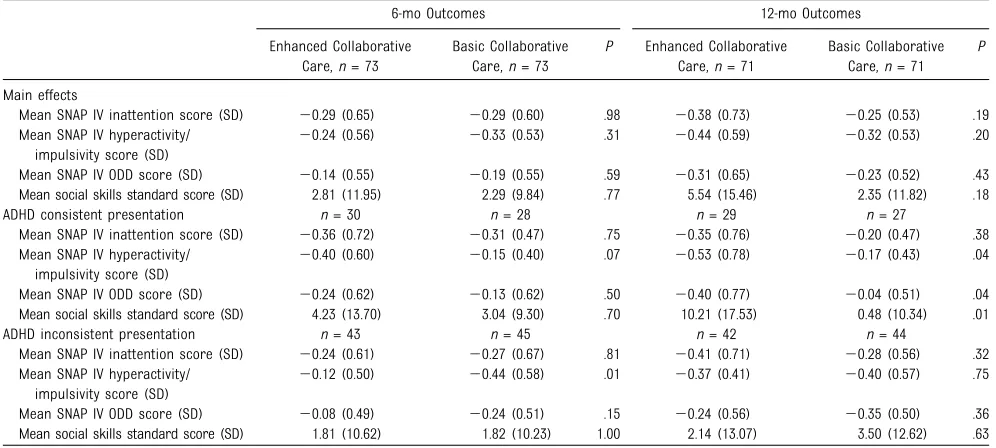
At both 6 and 12 months of follow-up, mean changes in scores for
through 6 and 12 months demonstrated no significant differences across study arms (Table 4).
Subgroup Analyses
Among children with ADHD-consistent presentations, multivariable models estimating differences in symptom changes from baseline demonstrated better trajectories among those receiving enhanced care (Table 4). At
12 months, those in the enhanced arm experienced greater
improvements in hyperactivity/ impulsivity (–0.36; 95% confidence interval [CI]–0.69 to–0.03),
oppositionality (–0.40; 95% CI–0.75 to–0.05), and social skills (9.57; 95% CI 1.85 to 17.28) than those in the basic arm. Effect sizes for these outcomes were moderate to large: 0.57 for hyperactivity/impulsivity, 0.55 for oppositionality, and 0.69 for social skills. Treatment arm-by-ADHD
interaction terms indicated statistically significant effect modification for each of these measures (P= .04 for hyperactivity/impulsivity,P= .02 for oppositionality,P= .01 for social skills).
Intervention Dose, Medication Prescription and Specialty Behavioral Health Care
An unadjusted as-treated analysis suggested better 12-month change scores for inattention (P= .07) and social skills (P= .04) among children FIGURE 1
with ADHD-consistent presentations, whose families received 1 to 3 enhanced care sessions. Whereas the proportion of children with
ADHD-consistent presentations to receive specialty behavioral health services was similar across study arms, there was a clinically
meaningful (but statistically nonsignificant) difference in the proportion of children with ADHD-consistent presentations to be prescribed an ADHD medication (52% in basic care versus 72% in enhanced care;P= .10).
DISCUSSION
Our study tested the comparative effectiveness of 2 collaborative care systems on urban children’s trajectories of inattention, hyperactivity/impulsivity, oppositionality, and social skills. Across the entire sample, there were no differences in outcomes between study arms. However, among children with ADHD-consistent presentations, those in the enhanced care arm experienced better symptom trajectories than those in the basic care arm. Among this subgroup, differences between arms appeared greater in the second half of the follow-up period than thefirst, with moderate to large effect sizes observed.
Consistent with recent novel approaches to pediatric behavioral health,23,41we enrolled children in
our trial based on presenting symptoms, as opposed to ultimate diagnoses. This family-centered approach represents a departure from much of the extant ADHD literature. Furthermore, whereas most studies to date have tested care systems against usual care, our trial is novel in studying whether augmenting collaborative care with lay-delivered strategies to address common reasons for symptom persistence improves outcomes. These dimensions, along with our emphasis on urban, low-income children, make our results relevant to primary care providers, those interested in operationalizing the principles of the Medical Home,20
and those interested in designing care for vulnerable populations.
Because our intervention has multiple facets, determining which TABLE 1 Baseline Characteristics by Study Group
Enhanced Collaborative Care,n= 78
Basic Collaborative Care,n= 77 Mean child age, y (SD) 8.69 (1.95) 8.67 (2.14)
Boys,n(%) 55 (71) 52 (67)
Child SNAP-IV scores (SD)
Inattentive subscale 1.94 (0.56) 1.81 (0.62) Hyperactive/impulsive subscale 1.79 (0.78) 1.78 (0.77) Oppositional defiant subscale 1.31 (0.78) 1.39 (0.74) Social Skills Rating Scale scores (SD) 82.51 (16.65) 84.96 (16.19) Caregiver relation to child,n(%)
Mother 69 (88) 68 (87)
Father 4 (5) 4 (5)
Legal guardian 5 (6) 6 (8)
Mean caregiver age, y (SD) 36.59 (9.30) 37.38 (8.27)
Black,n(%) 48 (62) 46 (59)
Latina,n(%) 19 (24) 23 (29)
US born,n(%) 48 (62) 50 (66)
High school graduate,n(%) 60 (77) 49 (63) Work outside home,n(%) 36 (46) 37 (47) Mean depression score (SD) 6.94 (4.76) 7.60 (5.04) Parent with symptoms of adult ADHD,n(%) 16 (21) 18 (23) Inadequate parental health literacy,n(%) 12 (16) 13 (17) Recruited from hospital site,n(%) 57 (73) 57 (73) Recruited from community health center,n(%) 21 (27) 21 (27)
TABLE 2 Clinical and Process Data
Enhanced Collaborative Care,n= 78
Basic Collaborative Care,n= 77 Diagnostic assessment
Decision support assessment consistent with ADHD (%) 34 (44) 29 (37) ADHD inattentive (%) 11 (14) 8 (10) ADHD hyperactive/impulsive (%) 4 (5) 7 (9) ADHD combined type (%) 15 (19) 12 (15) Quality metrics
Evaluated with parent Vanderbilt scale (%) 76/76 (100) 76/76 (100) Evaluated with teacher Vanderbilt scale (%) 76/76 (100) 71/76 (93) Coexistent conditions assessed (%) 76/76 (100) 72/75 (96) Number of in-person meetings with care manager after initial decision support
0 36 —
1 8 —
2 9 —
3 4 —
4 20 —
5 1 —
Number to receive an ADHD medication prescription (% among those with ADHD-consistent presentations)
23 (72) 15 (52)
Number to receive specialty behavioral health (% among those with ADHD-consistent presentations)
16 (52) 14 (50)
Key care management processes
Received Triple P (%) 37/78 (47) — Discussed maternal mental health (%) 7/78 (9) —
model component was responsible for the observed differences among children with ADHD-consistent presentations is difficult. Because only 9% of enhanced care parents discussed their own mental health, it is unlikely that this component was critical. Similarly, because receipt of specialty behavioral health services was equal across intervention groups, this was also unlikely a key driver of outcomes. By contrast, although there
is no direct evidence that Triple P was responsible for our results, its uptake among enhanced care families was nearly 50%, and it could well explain enhanced care’s preferential impact on hyperactivity/impulsivity. Last, among children with ADHD-consistent presentations in the enhanced care group, there was a clinically meaningful increase in ADHD medication prescriptions. Given that the motivational
interviewing script deliberately focused on medication use, it is possible that motivational interviewing started a cascade of events leading to increased
receptivity to ADHD medication, and that this, in turn, could have led to improved outcomes.
The principal strengths of our study are its comparative effectiveness design and real-world applicability. These particular strengths, however, TABLE 3 ADHD and ODD Symptoms and Social Skills at 6 and 12 Months
6-mo Outcomes 12-mo Outcomes
Enhanced Collaborative Care,n= 73
Basic Collaborative Care,n= 73
P Enhanced Collaborative Care,n= 71
Basic Collaborative Care,n= 71
P
Main effects
Mean SNAP IV inattention score (SD) 20.29 (0.65) 20.29 (0.60) .98 20.38 (0.73) 20.25 (0.53) .19 Mean SNAP IV hyperactivity/
impulsivity score (SD)
20.24 (0.56) 20.33 (0.53) .31 20.44 (0.59) 20.32 (0.53) .20
Mean SNAP IV ODD score (SD) 20.14 (0.55) 20.19 (0.55) .59 20.31 (0.65) 20.23 (0.52) .43 Mean social skills standard score (SD) 2.81 (11.95) 2.29 (9.84) .77 5.54 (15.46) 2.35 (11.82) .18 ADHD consistent presentation n= 30 n= 28 n= 29 n= 27
Mean SNAP IV inattention score (SD) 20.36 (0.72) 20.31 (0.47) .75 20.35 (0.76) 20.20 (0.47) .38 Mean SNAP IV hyperactivity/
impulsivity score (SD)
20.40 (0.60) 20.15 (0.40) .07 20.53 (0.78) 20.17 (0.43) .04
Mean SNAP IV ODD score (SD) 20.24 (0.62) 20.13 (0.62) .50 20.40 (0.77) 20.04 (0.51) .04 Mean social skills standard score (SD) 4.23 (13.70) 3.04 (9.30) .70 10.21 (17.53) 0.48 (10.34) .01 ADHD inconsistent presentation n= 43 n= 45 n= 42 n= 44
Mean SNAP IV inattention score (SD) 20.24 (0.61) 20.27 (0.67) .81 20.41 (0.71) 20.28 (0.56) .32 Mean SNAP IV hyperactivity/
impulsivity score (SD)
20.12 (0.50) 20.44 (0.58) .01 20.37 (0.41) 20.40 (0.57) .75
Mean SNAP IV ODD score (SD) 20.08 (0.49) 20.24 (0.51) .15 20.24 (0.56) 20.35 (0.50) .36 Mean social skills standard score (SD) 1.81 (10.62) 1.82 (10.23) 1.00 2.14 (13.07) 3.50 (12.62) .63
Lower scores indicate fewer symptoms for all SNAP-IV measures; higher scores indicate better social skills. ODD, oppositional defiant disorder.
TABLE 4 Multivariable Symptom Change Models
Outcome Difference in Symptom Score Between Enhanced and Basic Collaborative Care Groups
6 mon= 146 12 mon= 142
Mean Difference (95% CI) Effect Size Mean Difference (95% CI) Effect Size Main effects
SNAP inattention score 0.00 (–0.21 to 0.20) 0.00 20.14 (–0.34 to 0.07) 0.21 SNAP hyperactivity/impulsivity score 0.09 (–0.09 to 0.27) 20.17 20.13 (–0.31 to 0.05) 0.20 SNAP ODD score 0.05 (–0.13 to 0.23) 20.09 20.09 (–0.28 to 0.11) 0.17 Social skills score 0.59 (–2.98 to 4.16) 20.06 3.30 (–1.23 to 7.82) 0.23 ADHD consistent presentation
SNAP inattention score 20.05 (–0.37 to 0.27) 0.08 20.16 (–0.50 to 0.18) 0.24 SNAP hyperactivity/impulsivity score 20.22 (–0.48 to 0.04) 0.49 20.36 (–0.69 to–0.03) 0.57 SNAP ODD score 20.10 (–0.42 to 0.23) 0.18 20.40 (–0.75 to–0.05) 0.55 Social skills score 1.68 (–4.49 to 7.85) 0.13 9.57 (1.85 to 17.28) 0.69 ADHD inconsistent presentation
SNAP inattention score 0.02 (–0.25 to 0.28) 20.05 20.15 (–0.41 to 0.10) 0.19 SNAP hyperactivity/impulsivity score 0.31 (0.08 to 0.54) 20.58 0.03 (–0.18 to 0.24) 20.08 SNAP ODD score 0.14 (–0.06 to 0.34) 20.31 0.09 (–0.13 to 0.31) 20.11 Social skills score 20.01 (–4.35 to 4.32) 0.00 21.14 (–6.46 to 4.17) 20.10
introduce 2 important limitations. Thefirst is that disentangling the impact of individual intervention components, which likely act both independently and
interdependently,42,43often requires
strict standardization in intervention implementation, which is largely impossible in an effectiveness design.44This, combined with the fact
that we would not expect the benefits of enhanced care to accrue through the same pathway for all study participants, limits our ability to isolate key mediating factors of our model. Second, staying true to an effectiveness study design limits us to monitoring interventionfidelity through unobtrusive means,21which
are inherently less exacting than techniques typically used in efficacy trials.
Additionally, our study was
conducted in a single geographic area. Most of our subjects attended school in a district in which there was usually not a single, easily identifiable teacher who knew the child best; therefore, we confined our outcome assessments to parent report. Although a limitation, this approach to measuring outcomes is
consistent with existing studies of collaborative behavioral health care for children,41and previous work
indicates that our outcome measures tend to be stable across parent and teacher reports.39
With these limitations in mind, it appears that adding certain theory-based components to a basic collaborative care system produces no added benefit for a population of
urban children with symptoms of inattention and hyperactivity/ impulsivity. However, among children with presentations
consistent with ADHD, using lay care managers to address barriers to engagement and challenging child behaviors could have some added benefit. Because our positive
findings occurred in a study subgroup, as opposed to the main sample, thesefindings need to be replicated in a larger study, powered not only to confirm intervention impact, but also to decipher its mechanism of action.
ACKNOWLEDGMENTS
We thank Megan Bair-Merritt for her thoughtful review of the manuscript.
This trial has been registered at www.clinicaltrials.gov (identifier NCT01275378). www.pediatrics.org/cgi/doi/10.1542/peds.2014-3221
DOI:10.1542/peds.2014-3221 Accepted for publication Jan 15, 2015
Address correspondence to Michael Silverstein, MD, MPH, Vose Hall 3, Boston Medical Center, Boston, MA 02118. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2015 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:Health Resources and Services Administration, Maternal Child Health Bureau, grant R40MC17181.
POTENTIAL CONFLICT OF INTEREST:The authors have indicated they have no potential conflicts of interest to disclose.
COMPANION PAPER:A companion to this article can be found on page e1042, online at www.pediatrics.org/cgi/doi/10.1542/peds.2015-0070.
REFERENCES
1. Biederman J, Faraone SV. Attention-deficit hyperactivity disorder.Lancet. 2005;366(9481):237–248
2. Stein RE, Horwitz SM, Storfer-Isser A, Heneghan A, Olson L, Hoagwood KE. Do pediatricians think they are responsible for identification and management of child mental health problems? Results of the AAP periodic survey.Ambul Pediatr. 2008;8(1):11–17
3. Stein RE, Horwitz SM, Storfer-Isser A, et al. Attention-deficit/hyperactivity disorder: how much responsibility are pediatricians taking?Pediatrics. 2009; 123(1):248–255
4. Epstein JN, Kelleher KJ, Baum R, et al. Variability in ADHD care in community-based pediatrics.Pediatrics. 2014;134(6): 1136–1143
5. Leslie LK, Weckerly J, Plemmons D, Landsverk J, Eastman S. Implementing the American Academy of Pediatrics attention-deficit/hyperactivity disorder diagnostic guidelines in primary care settings.Pediatrics. 2004;114(1):129–140 6. Epstein JN, Rabiner D, Johnson DE, et al.
Improving attention-deficit/hyperactivity disorder treatment outcomes through use of a collaborative consultation treatment service by community-based pediatricians:
a cluster randomized trial.Arch Pediatr Adolesc Med. 2007;161(9):835–840 7. Epstein JN, Langberg JM, Lichtenstein PK,
Mainwaring BA, Luzader CP, Stark LJ. Community-wide intervention to improve the attention-deficit/hyperactivity disorder assessment and treatment practices of community physicians.
Pediatrics. 2008;122(1):19–27 8. Committee on Psychosocial Aspects of
9. Thomas CR, Holzer CE III. The continuing shortage of child and adolescent psychiatrists.J Am Acad Child Adolesc Psychiatry. 2006;45(9):1023–1031 10. dosReis S, Butz A, Lipkin PH, Anixt JS,
Weiner CL, Chernoff R. Attitudes about stimulant medication for attention-deficit/hyperactivity disorder among African American families in an inner city community.J Behav Health Serv Res. 2006;33(4):423–430
11. dosReis S, Mychailyszyn MP, Myers M, Riley AW. Coming to terms with ADHD: how urban African-American families come to seek care for their children.
Psychiatr Serv. 2007;58(5):636–641 12. Leslie LK, Plemmons D, Monn AR,
Palinkas LA. Investigating ADHD treatment trajectories: listening to families’stories about medication use.
J Dev Behav Pediatr. 2007;28(3):179–188 13. Stevens J, Harman JS, Kelleher KJ. Ethnic and regional differences in primary care visits for attention-deficit hyperactivity disorder.J Dev Behav Pediatr. 2004;25(5): 318–325
14. Radigan M, Lannon P, Roohan P, Gesten F. Medication patterns for attention-deficit/ hyperactivity disorder and comorbid psychiatric conditions in a low-income population.J Child Adolesc
Psychopharmacol. 2005;15(1):44–56 15. Ray GT, Croen LA, Habel LA. Mothers of
children diagnosed with attention-deficit/hyperactivity disorder: health conditions and medical care utilization in periods before and after birth of the child.Med Care. 2009;47(1):105–114 16. Owens EB, Hinshaw SP, Kraemer HC, et al.
Which treatment for whom for ADHD? Moderators of treatment response in the MTA.J Consult Clin Psychol. 2003;71(3): 540–552
17. Hinshaw SP. Moderators and mediators of treatment outcome for youth with ADHD: understanding for whom and how interventions work.Ambul Pediatr. 2007; 7(suppl 1):91–100
18. Jensen PS, Hinshaw SP, Kraemer HC, et al. ADHD comorbidityfindings from the MTA study: comparing comorbid subgroups.J Am Acad Child Adolesc Psychiatry. 2001;40(2):147–158 19. Swanson JM, Kraemer HC, Hinshaw SP,
et al. Clinical relevance of the primary findings of the MTA: success rates based
on severity of ADHD and ODD symptoms at the end of treatment.J Am Acad Child Adolesc Psychiatry. 2001;40(2):168–179 20. Medical Home Initiatives for Children
With Special Needs Project Advisory Committee. The American Academy of Pediatrics. The medical home.Pediatrics. 2002;110(1):184–186
21. Thorpe KE, Zwarenstein M, Oxman AD, et al. A pragmatic-explanatory
continuum indicator summary (PRECIS): a tool to help trial designers.J Clin Epidemiol. 2009;62(5):464–475 22. Unützer J, Katon W, Callahan CM, et al;
IMPACT Investigators. Improving Mood-Promoting Access to Collaborative Treatment. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial.JAMA. 2002;288(22): 2836–2845
23. Kolko DJ, Campo JV, Kilbourne AM, Kelleher K. Doctor-office collaborative care for pediatric behavioral problems: a preliminary clinical trial.Arch Pediatr Adolesc Med. 2012;166(3):224–231 24. Grote NK, Swartz HA, Geibel SL, Zuckoff A,
Houck PR, Frank E. A randomized controlled trial of culturally relevant, brief interpersonal psychotherapy for perinatal depression.Psychiatr Serv. 2009;60(3):313–321
25. Sanders MR. Triple P-Positive Parenting Program: towards an empirically validated multilevel parenting and family support strategy for the prevention of behavior and emotional problems in children.Clin Child Fam Psychol Rev. 1999;2(2):71–90
26. Sanders MR, Bor W, Morawska A. Maintenance of treatment gains: a comparison of enhanced, standard, and self-directed Triple P-Positive Parenting Program.J Abnorm Child Psychol. 2007;35(6):983–998
27. Sanders MR, Markie-Dadds C, Tully LA, Bor W. The triple P-positive parenting program: a comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems.J Consult Clin Psychol. 2000; 68(4):624–640
28. Wolraich ML, Feurer ID, Hannah JN, Baumgaertel A, Pinnock TY. Obtaining systematic teacher reports of disruptive behavior disorders utilizing DSM-IV.
J Abnorm Child Psychol. 1998;26(2): 141–152
29. Subcommittee on Attention-Deficit/ Hyperactivity Disorder; Steering Committee on Quality Improvement and Management. ADHD: clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/ hyperactivity disorder in children and adolescents.Pediatrics. 2011;128(5): 1007–1022
30. Lesesne CA, Visser SN, White CP. Attention-deficit/hyperactivity disorder in school-aged children: association with maternal mental health and use of health care resources.Pediatrics. 2003; 111(5 pt 2):1232–1237
31. Miller W, Rollnick S.Motivational Interviewing: Preparing People for Change. 2nd ed. New York, NY: The Guilford Press; 2002
32. Jensen PS, Arnold LE, Swanson JM, et al. 3-year follow-up of the NIMH MTA study.
J Am Acad Child Adolesc Psychiatry. 2007; 46(8):989–1002
33. Bussing R, Fernandez M, Harwood M, et al. Parent and teacher SNAP-IV ratings of attention deficit hyperactivity disorder symptoms: psychometric properties and normative ratings from a school district sample.Assessment. 2008;15(3): 317–328
34. Gresham FM, Elliot SN. Social skills scale of the Social Skills Rating System (SSRS). In: Rush AJ, First MB, Blacker D, eds.
Handbook of Psychiatric Measures. 2nd ed. Washington, DC: American
Psychiatric Publishing; 2008
35. Rush AJ, Trivedi MH, Ibrahim HM, et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression.
Biol Psychiatry. 2003;54(5):573–583 36. Garland MR. The short form adult
attention deficit/hyperactivity self-report scale is a useful diagnostic measure.
Evid Based Ment Health. 2006;9:38 37. Baker DW, Williams MV, Parker RM,
Gazmararian JA, Nurss J. Development of a brief test to measure functional health literacy.Patient Educ Couns. 1999; 38(1):33–42
multicenter studies: an overview.Ann Intern Med. 2001;135(2):112–123 39. The MTA Cooperative Group. Multimodal
Treatment Study of Children with ADHD. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder.Arch Gen Psychiatry. 1999;56(12):1073–1086 40. MTA Cooperative Group. National
Institute of Mental Health Multimodal Treatment Study of ADHD follow-up: 24-month outcomes of treatment
strategies for attention-deficit/ hyperactivity disorder.Pediatrics. 2004; 113(4):754–761
41. Kolko DJ, Campo J, Kilbourne AM, Hart J, Sakolsky D, Wisniewski S. Collaborative care outcomes for pediatric behavioral health problems: a cluster randomized trial.Pediatrics. 2014;133(4). Available at: www.pediatrics.org/cgi/content/full/133/ 4/e981
42. Lewin S, Glenton C, Oxman AD. Use of qualitative methods alongside
randomised controlled trials of complex healthcare interventions: methodological study.BMJ. 2009;339:b3496
43. Campbell M, Fitzpatrick R, Haines A, et al. Framework for design and evaluation of complex interventions to improve health.
BMJ. 2000;321(7262):694–696 44. Craig P, Dieppe P, Macintyre S, et al.
DOI: 10.1542/peds.2014-3221 originally published online March 23, 2015;
2015;135;e858
Pediatrics
Sandler, Michelle Pellicer, Ning Chen and Howard Cabral
Michael Silverstein, L. Kari Hironaka, Heather J. Walter, Emily Feinberg, Jenna
Comparative Effectiveness Trial
Collaborative Care for Children With ADHD Symptoms: A Randomized
Services
Updated Information &
http://pediatrics.aappublications.org/content/135/4/e858
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/135/4/e858#BIBL
This article cites 38 articles, 10 of which you can access for free at:
Subspecialty Collections
activity_disorder_adhd_sub
http://www.aappublications.org/cgi/collection/attention-deficit:hyper Attention-Deficit/Hyperactivity Disorder (ADHD)
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
http://www.aappublications.org/cgi/collection/medical_home_sub Medical Home
_sub
http://www.aappublications.org/cgi/collection/community_pediatrics Community Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2014-3221 originally published online March 23, 2015;
2015;135;e858
Pediatrics
Sandler, Michelle Pellicer, Ning Chen and Howard Cabral
Michael Silverstein, L. Kari Hironaka, Heather J. Walter, Emily Feinberg, Jenna
Comparative Effectiveness Trial
Collaborative Care for Children With ADHD Symptoms: A Randomized
http://pediatrics.aappublications.org/content/135/4/e858
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.