A Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Study
of SLI381 (Adderall XR) in Children With Attention-Deficit/Hyperactivity
Disorder
Joseph Biederman, MD*; Frank A. Lopez, MD‡; Samuel W. Boellner, MD§; and Mark C. Chandler, MD储
ABSTRACT. Objective. SLI381 (Adderall XR) is a 2-component extended-release capsule formulation of Adderall designed to produce a therapeutic effect that lasts throughout the day with 1 morning dose. The pri-mary objective of this study was to assess the efficacy and safety of SLI381 compared with placebo in the treat-ment of attention-deficit/hyperactivity disorder (ADHD) in children in a naturalistic school and home setting. A secondary objective was to assess the diurnal variation in responses based on morning and afternoon assessments. Methods. A multicenter, randomized, double-blind, parallel-group, placebo-controlled trial was conducted at 47 sites. After a 1-week washout of any previous stimu-lant medication, patients were randomized to receive single-daily morning doses of placebo or SLI381 10 mg, 20 mg, or 30 mg for 3 weeks. Participants aged 6 to 12 years inclusive who satisfied Diagnostic and Statistical Manual of Mental Disorders, Fourth Editioncriteria diag-nosis of ADHD were included. The primary efficacy parameter was the Conners Global Index Scale for Teach-ers. Secondary efficacy parameters included the Conners Global Index Scale for Parents, the Clinical Global Im-pressions Scale for improvement, and the Parent Global Assessment for improvement. Safety was assessed by recording adverse events, laboratory tests, and vital signs at each visit during the study. Physical examinations and electrocardiograms were performed at the screening and the end of the study.
Results. Five hundred eighty-four children were ran-domized, 563 were included in the intent-to-treat popu-lation, and 509 completed the entire study. Intention-to-treat analysis of Conners Global Index Scale for Teachers and Conners Global Index Scale for Parents scores re-vealed significant improvement in morning, afternoon, and late afternoon behavior for all active treatment groups versus placebo. All active treatment groups showed significant dose-related improvement in behav-ior from baseline. Both the Clinical Global Impressions Scale for improvement and Parent Global Assessment for improvement showed all doses of SLI381 to be superior to placebo at treatment end and both confirmed the dose-response relationship between improvement and the SLI381 dose. The incidence of spontaneously reported
adverse events was low and similar for active treatments and placebo.
Conclusions. SLI381 produced consistent, dose-re-lated improvements on all measures of efficacy. The ex-tended-release nature of the SLI381 formulation was shown by continued, significant improvement in after-noon assessments by teachers and afterafter-noon and late afternoon assessments by parents. The time course and therapeutic effects of SLI381 suggests that this medica-tion is an efficacious once-daily treatment for children with ADHD. Pediatrics 2002;110:258 –266; attention-deficit/hyperactivity disorder, amphetamine, Adderall XR, randomized, controlled trial.
ABBREVIATIONS. ADHD, attention-deficit/hyperactivity disor-der; ECG, electrocardiogram; DISC, Diagnostic Interview Sched-ule for Children; CGIS-T, Conners Global Index Scale for Teachers; CGIS-P, Conners Global Index Scale for Parents; CGI, Clinical Global Impressions Scale for improvement; PGA, Parent Global Assessment for Improvement; ITT, intention-to-treat; ANCOVA, analysis of covariance.
A
ttention-deficit/hyperactivity disorder (ADHD) is a common neurobehavioral disorder affect-ing from 4% to 12% of school-aged children.1This disorder is characterized by developmentally inappropriate levels of inattention, hyperactivity, and impulsivity,2 and is associated with significant
impairment across multiple domains of function-ing, including academic and occupational achieve-ment, family and peer relationships, and low self-esteem.3–7
Numerous randomized, controlled trials have shown stimulant medications to be highly effective in ameliorating the symptoms of ADHD.8 –10
How-ever, their use can be problematic because of the need for multiple daily dosing in most individuals. In-school dosing in pediatric patients may lead to ridicule by peers and further negative impact on self-esteem, compliance, and treatment satisfaction. In addition, many patients may require medication coverage that extends into homework time and or-ganized recreational activities. This denotes a com-pelling need for more effective once-daily dosage forms of stimulant medications that last throughout the school day and into the evening.
Adderall (Shire US Inc, Valley Stream, NY), a sin-gle-entity amphetamine drug product consisting of a mixture of neutral salts of dextroamphetamine sul-fate, amphetamine sulsul-fate, the dextro isomer of am-phetamine saccharate, and d,l-amam-phetamine
aspar-From *Massachusetts General Hospital, Boston, Massachusetts; ‡Children’s Developmental Center, Maitland, Florida; §Clinical Study Centers, Little Rock, Arkansas; and储North Carolina Neuropsychiatry, Chapel Hill, North Carolina on behalf of the SLI381.301 Study Group.
Received for publication Jul 11, 2001; accepted Feb 20, 2002.
Reprint requests to (J.B.) Pediatric Psychopharmacology Unit, Massachu-setts General Hospital, 15 Parkman St—ACC 725, Boston, MA 02114. E-mail: [email protected]
tate, is effective in treating the symptoms of ADHD.11–16 To address the need for a once-daily
dosing option for more patients, a 2-component extended-release formulation (SLI381 capsules [Catalytica Pharmaceuticals, Inc, Greenville, NC]) of Adderall has been developed that is designed to produce pulsed-release of amphetamine salts yield-ing a therapeutic effect that lasts throughout the day and into the evening with 1 morning dose.
The SLI381 capsule formulation is composed of 2 types of Microtrol beads combined in a 50:50 ratio within 1 capsule. The immediate release beads are designed to release drug content in a time course similar to Adderall. The delayed release beads are designed to release drug content 4 to 6 hours after oral administration of the capsule. With the inclusion of the delayed-release component, the 2-unit formu-lation, given once a day, is expected to produce similar pharmacokinetic and pharmacodynamic ef-fects as immediate release Adderall given twice daily.
A pilot study compared the bioavailability of 3 composite 20-mg experimental extended release for-mulations with a single-dose administration against the reference, Adderall 10 mg bid with a 4-hour interval.17 The selected SLI381 formulation was
bio-equivalent to Adderall in terms of the d- and l-amphetamine extent and rate of absorption, and the time to maximum concentration values for d- and l-amphetamine were not different from those ob-served for Adderall bid with a 4-hour interval.
This multicenter study was designed to assess the safety and efficacy of SLI381 in a naturalistic school and home setting. This naturalistic environment al-lows efficacy and safety results to be extrapolated to the clinical pediatric population most likely to re-ceive stimulant treatment for ADHD. A randomized, double-blind, parallel group design with up to 3 weeks of exposure permits between-group differ-ences in clinical manifestations of childhood ADHD and in acute safety and tolerability to be evaluated. The primary objective of this study was to assess the efficacy and safety of SLI381 compared with pla-cebo in the treatment of ADHD in children. The secondary objective was to assess diurnal variation in responses to SLI381 based on morning and after-noon assessments. This study was conducted in com-pliance with institutional review board and informed consent regulations.
METHODS Participants
Children aged 6 to 12 years who satisfiedDiagnostic and Statis-tical Manual of Mental Disorders, Fourth Editioncriteria for a pri-mary diagnosis of hyperactive-impulsive or combined subtypes of ADHD were recruited for the study. Participants were required to be in a school setting in which the same teacher was able to make assessments of both morning and afternoon behavior. The teacher had to be able to spend sufficient time with a participant to make valid assessments in both the morning and afternoon. Participants who were home-schooled were not permitted to enroll.
Children were either known to be responsive to stimulants or naı¨ve to stimulant treatment. Participants incapable of under-standing or following the instructions given in the study, known nonresponders to stimulant medication, and those with a comor-bid psychiatric diagnosis (psychosis, bipolar illness, pervasive
developmental disorder, severe obsessive compulsive disorder, severe depressive or severe anxiety disorder) were excluded from the study. Participants with a history of seizure (exclusive of febrile seizure), tic disorder, or a family history of Tourette’s disorder, those with a documented allergy or intolerance to Adderall, and participants taking clonidine, anticonvulsant drugs, pemoline (within 30 days), medications that affect blood pressure or heart rate, steroids, or other medications that have central nervous system effects or affect performance (such as sedating antihistamines and decongestant sympathomimetics, either oral or topical) also were excluded. Other exclusion criteria included a concurrent chronic or acute illness or condition that might con-found results or increase risk to the participant, history of sus-pected substance abuse disorder, or living with someone with a current diagnosed substance abuse disorder.
Study Design
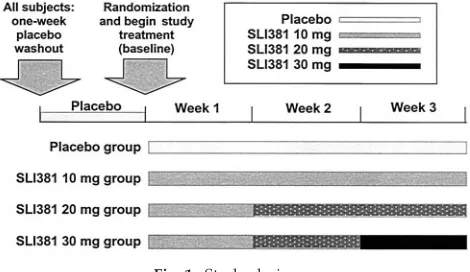
This was a multicenter, randomized, double-blind, placebo-controlled, parallel group, study of 3 doses of SLI381. After screen-ing (Visit 1), participants returned for a washout visit (Visit 2) in which vital signs were measured and any current stimulant treat-ment (if any) was discontinued. All participants receive placebo treatment in a single-blind fashion for a 1-week washout phase. At Visit 3 (baseline visit), participants were randomly allocated in a 2:2:2:3 ratio to 1 of 4 treatment groups: SLI381 10 mg/d, SLI381 20 mg/d, SLI381 30 mg/d, or placebo.
The study design used a dose-escalation regimen for the SLI381 treatment groups, in which all children received SLI381 10 mg for the first week of treatment, those randomized to the 20-mg and 30-mg groups received 20 mg for the second week of treatment, and those randomized to the 30-mg group received 30 mg for the third week of treatment (Fig 1). Patients returned at weekly inter-vals for safety and efficacy assessments. During each of the study weeks, patients were also assessed by their teachers at school and by their parents at home for efficacy using standard ADHD rating scales (see “Measurements”).
Physical examinations and laboratory tests, including hematol-ogy, blood chemistry, and urinalysis, were performed at baseline and endpoint. A full vital signs check, including oral temperature, pulse, and sitting blood pressure, was performed at screening. For all other visits, only pulse and sitting blood pressure were mea-sured. In addition, a 12-lead electrocardiogram (ECG) was per-formed at screening and study endpoint. Adverse events were collected beginning at the time of informed consent by investiga-tor interview.
Measurements
During the screening visit (Visit 1), ADHD was established by 1) a psychiatric examination which reviewed Diagnostic and Sta-tistical Manual of Mental Disorders, Fourth Editionand criteria, and 2) the National Institutes of Mental Health Diagnostic Interview Schedule for Children Version 4.0 (DISC-4.0).18One interviewer from each center was trained to administer the DISC-4.0 before the initiation of the study.
Beginning with the washout week, teachers completed the Con-ners Global Index Scale (teacher’s version; CGIS-T) on 3 specified days (Monday, Wednesday, and Friday), in the morning and afternoon of each day (⬃10:00amand 2:00pm). Parents completed the Conners Global Index Scale (parent’s version; CGIS-P) once
per week on either Saturday or Sunday. They rated the child 3 times during the day (at⬃10:00am, 1:00pm, and after 4:00pm). Parents were also given a diary to record observations of their child’s behavior during the week to aid in completing the Parent’s Global Assessment, which was completed at baseline (washout week) and the final visit. Adverse event information was re-corded, and drug compliance was assessed by capsule counts at each weekly study visit.
The primary efficacy parameter was the average of morning and afternoon CGIS-T total scores at study endpoint (or last treat-ment week). This included a total of up to 6 assesstreat-ments, 3 for morning and 3 for afternoon. In addition, the averages of the CGIS-T scores were calculated separately for both morning and afternoon assessments to evaluate the drug effect versus placebo for morning and afternoon separately.
Secondary efficacy parameters included CGIS-P and 2 global assessments of overall improvement by the investigator (the Clin-ical Global Impressions Scale for improvement [CGI]), and by parents (the Parent Global Assessment for improvement [PGA]). Average total scores were calculated separately for morning, af-ternoon, and late afternoon CGIS-P; only the improvement score of the CGI and PGA were examined in the study.
Adverse events were recorded by COSTART term and rated as mild, moderate, or severe. Compliance was measured by capsule counts at the end of each visit.
Statistical Analysis
To detect a standardized treatment difference of 0.47 between a single SLI381 treatment group and the placebo group at 90% power (2-tailed) and an␣level of 0.05, it was necessary to enroll at least 120 participants in the placebo group and 80 participants in each of the 3 treatment groups (10, 20, and 30 mg/d). Assuming a 20% attrition rate over the course of the study, a total of 450 participants were targeted for inclusion in the study.
The primary efficacy analysis was conducted using the inten-tion-to-treat (ITT) population and a 2-way analysis of covariance (ANCOVA) model with a general linear approach. This ANCOVA model used the average of CGIS-T total scores over the last treat-ment week assessed (ie, study endpoint), as the dependent vari-able, and the treatment (four levels) and study site as the inde-pendent variable. The corresponding baseline score (obtained during the single-blind washout week) of the primary endpoint was included as a covariate in the statistical model. SAS PROC GLM (Windows version 6.12) was used for this analysis. If statis-tically significant treatment effect was disclosed (P⬍.05) by the 2-way ANCOVA, Dunnett’s test for multiple mean comparisons was used to compare the differences between treatment groups and the placebo group.
A similar analytic approach to the CGIS-T total scores was adopted for each individual treatment week and for secondary efficacy measures and subgroup population comparisons. For the CGIS-T, those assessments conducted before noon, exclusive, were operationally categorized as morning assessments; those
assess-ments that were conducted after noon, inclusive, were operation-ally categorized as afternoon assessments. Similarly, for the CGIS-P, morning assessments were those conducted before noon, afternoon assessments were those conducted from noon to 4:00 pm, and late afternoon assessments were operationally categorized as those conducted on or after 4:00pm. Because participants as-signed to SLI381 20 mg and 30 mg received their doses in a dose escalation fashion, a 3-way analysis of variance with split-plot design was used to analyze weekly averages of the CGIS-T total scores without data imputation for participants who completed the study to evaluate the dose titration effect. Safety-related infor-mation was analyzed comparatively for active versus placebo groups, using 1-way analysis of variance, to examine differences in changes from baseline to end of study.
RESULTS Study Population
Six hundred forty-nine participants were enrolled in the study and entered the lead-in placebo washout phase. Of these participants, 584 were randomized to the double-blind treatment phase, which was con-ducted at 47 sites. One hundred twenty-four, 121, 129, and 210 participants were randomized to the SLI381 30 mg/d, 20 mg/d, and 10 mg/d groups, and to the placebo group, respectively. The numbers of participants in each treatment group who completed the study were 112 (90.3%), 105 (86.8%), 119 (92.2%), and 173 (82.4%), respectively. The disposition of par-ticipants withdrawn from the study is shown in Ta-ble 1.
Across the treatment groups, the majority of par-ticipants were boys (72.9%– 80.4%) and white (70.0%– 82.1%) (Table 2). The mean age, weight, and height of these children were comparable across treatment groups. The majority (⬎90%) of the chil-dren were diagnosed as ADHD combined type in each of the treatment groups, and the distribution of the disorder types was balanced among the treat-ment groups. Although the study protocol called for only those with diagnoses of either combined or hyperactive subtypes to be eligible for participation, 12 participants diagnosed as inattentive were ran-domized to treatment. These participants were in-cluded in the efficacy and safety analyses because they represented only 2% of the total randomized and were distributed across all 4 groups. The average
TABLE 1. Disposition of Participants Enrolled in the Study
Entire Study Dropout Before Randomization
Randomized Treatment
SLI381 30 mg
SLI381 20 mg
SLI381 10 mg
Placebo
Entered 649 65
Randomized 584 NA 124 121 129 210
Completed 509 NA 112 105 119 173
Discontinued 140 65 12 16 10 37
Reason
Adverse events 17 2 5 4 0 6
Consent withdrawn 53 27 4 7 4 11
Protocol violation 13 7 2 1 2 1
Lost to follow up 11 3 0 2 0 6
Lack of efficacy 13 NA 0 1 2 10
Other* 33 26 1 1 2 3
Number of patients for assessment
Efficacy (ITT population) 563 NA 120 112 128 203
Safety 649 65 124 121 129 210
NA indicates not applicable.
duration of the disorder ranged from 2.5 to 2.9 years across the treatment groups, and 30.4% to 37.5% were treatment naı¨ve.
Compliance
Noncompliance was defined as taking ⬍80% or
⬎120% of study medication during any outpatient evaluation period (visit to visit). For the ITT popula-tion, drug compliance among the treatment groups was similar across the 2 phases, ranging from 97.8% to 98.8% during the washout phase and from 97.2% to 98.2% during the double-blind treatment phase. Similar patterns were observed for the following subgroups: boys versus girls, age groups (6 – 8 years vs 9 –12 years), race, and ADHD subtype.
Efficacy
Primary Efficacy: Teacher Ratings
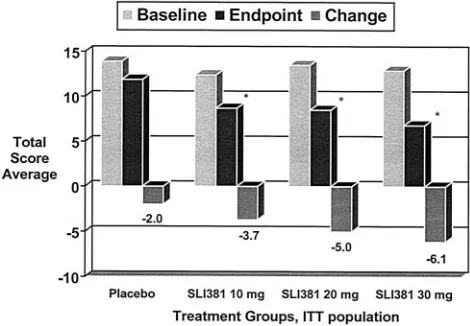
The primary efficacy measure was the average of the CGIS-T total scores obtained at study endpoint, including both the morning and afternoon assess-ments, and the baseline score obtained during the placebo washout week was the covariate in the ana-lytical model (Fig 2). Two-way analysis of variance showed a trend toward a difference across study sites in the baseline values (P ⫽.053), but no differ-ence in baseline scores across treatment groups (P⫽
.402). All active treatment groups showed significant improvements in CGIS-T scores from baseline to study endpoint. The magnitude of changes from baseline to study endpoint was⬃6 to 1 in unit point for SLI381 groups compared with placebo, a roughly fivefold relative improvement of ADHD behavior at school in participants receiving active treatment. The 2-way ANCOVA at endpoint showed a highly
sig-nificant treatment effect (P ⬍ .0001), a significant effect of baseline covariate (P⬍.0001), and site effect was not significant (P⫽.2778). Dunnett’s test, which adjusted the P value for multiplicity, disclosed fur-ther that at the study endpoint, differences in CGIS-T total score were negative for each SLI381 dose group in comparison to placebo and highly significant (P⬍
.001).
In addition, difference scores relative to placebo indicated a dose-response relationship for the SLI381 doses, with the largest improvement associated with the 30-mg group and the smallest improvement with the 10-mg group. Figure 3 illustrates the dose rela-tionship between the 3 SLI381 treatment groups Fig 2. CGIS-T total score average at baseline, study endpoint, and change for average of both morning and afternoon assessments. *P⬍.001 compared with placebo by Dunnett test following AN-COVA with baseline score as covariate.
TABLE 2. Summary of Demographic and Baseline Information (ITT,N⫽563)
Characteristic Treatment Group
SLI381 30 mg
N⫽120
SLI381 20 mg
N⫽112
SLI381 10 mg
N⫽128
Placebo
N⫽203
Male,n(%) 96 (80.0) 90 (80.4) 100 (78.1) 148 (72.9)
Female,n(%) 24 (20.0) 22 (19.6) 28 (21.9) 55 (27.1)
Race,n(%)
Caucasian 84 (70.0) 92 (82.1) 98 (76.6) 156 (76.8)
Black 20 (16.7) 9 (8.0) 11 (8.6) 27 (13.3)
Hispanic 11 (9.2) 10 (8.9) 12 (9.4) 14 (6.9)
Asian/Pacific Islander 1 (0.8) 0 (0) 1 (0.8) 2 (1.0)
Native American 0 (0.0) 0 (0) 1 (0.8) 0 (0)
Other 4 (3.3) 1 (0.9) 5 (3.9) 4 (2.0)
Age (y) mean 8.8⫾1.77 8.4⫾1.70 8.5⫾1.58 8.6⫾1.73
Height (in) mean 53.1⫾4.99 52.3⫾4.52 52.3⫾4.18 52.9⫾4.38
Weight (lb) mean 72.6⫾23.01 70.9⫾24.09 73.2⫾25.60 74.4⫾25.84
ADHD duration (y) mean 2.9⫾2.30 2.6⫾2.29 2.5⫾2.16 2.7⫾2.28
ADHD subtype,n(%)
Combined 112 (93.3) 104 (92.9) 117 (91.4) 190 (93.6)
Hyperactive 6 (5.0) 6 (5.4) 8 (6.3) 8 (3.9)
Inattentive 2 (1.7) 2 (1.8) 3 (2.3) 5 (2.5)
Previous prescription,n(%)
Stimulant 80 (66.7) 73 (65.2) 78 (60.9) 112 (55.2)
Other 0 (0) 4 (3.6) 1 (0.8) 4 (2.0)
No previous prescription 37 (30.8) 34 (30.4) 48 (37.5) 76 (37.4)
Not listed 3 (2.5) 1 (0.9) 1 (0.8) 11 (5.4)
Comorbid conditions present,n(%) 37 (30.8) 31 (27.7) 41 (32.0) 61 (30.0)
CGIS-T baseline score, mean 11.2⫾6.9 12.1⫾6.7 11.5⫾6.3 10.6⫾6.6
when the responses are corrected for the correspond-ing placebo response.
The CGIS-T total scores were also calculated sep-arately for the morning and afternoon assessments (Table 3). The findings were very similar to the CGIS-T scores averaged across morning and after-noon, indicating that SLI381 doses from 10 to 30 mg per day were effective during both morning and afternoon.
The time course of improvements in each treat-ment group is depicted in Fig 4. The improvetreat-ments in CGIS-T were consistent and dose-related at each treatment week as well as at study endpoint. Im-provement during week 1 was similar between SLI381 treatment groups, and better than placebo group. During week 2, the 20-mg and 30-mg groups continued to improve, whereas the response of the 10-mg group remained relatively unchanged. During the third week the 30-mg group continued to im-prove, the improvements in the 10-mg and 20-mg groups showing a plateau effect. At all time points the improvements in the SLI381 treatment groups were statistically superior to the improvements in the placebo group.
For participants eligible for the ITT analysis, sub-group analyses of the CGIS-T total scores were per-formed for boys versus girls and for participants with and without previous stimulant therapy for ADHD. The trend of response to SLI381 treatment was similar among boys and girls and consistent with those of the entire ITT population. Patients who were naı¨ve to ADHD treatment responded as consis-tently and positively as those who were treated with stimulants before study participation.
Parent Ratings
The results of the parent evaluation, using the parent version of the CGIS, revealed similar efficacy (Fig 5; Table 4). The mean magnitude of changes from baseline to study endpoint was⬃2.5 to 1 in unit point for SLI381 groups compared with placebo, a 1.5-fold relative improvement of ADHD behavior at home for participants on active treatment. The changes from baseline in the morning and late after-noon assessments were almost identical, indicating that the SLI381 was still effective in the early evening (defined as on and from 4:00pm).
Global Assessments
Two other secondary measures which gave global assessments of overall improvement, one by the in-vestigator (CGI) and the other by the parents (PGA), both showed the superiority of SLI381 therapy over placebo, and both confirmed the dose-response rela-tionship between improvement and SLI381 dose (Fig 6).
Safety
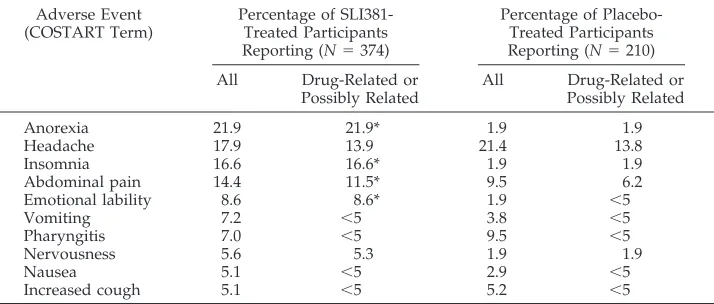
Postrandomization, 263 (70.3%) SLI381-treated participants and 119 (56.7%) placebo-treated partici-pants reported adverse events. The majority (69%) of adverse events were mild; 28% were moderate, and 4% were severe. The most frequently reported ad-verse events are shown in Table 5. Adad-verse events Fig 3. Dose-response relationship in CGIS-T total score average.
Fig 4. Time course of average CGIS-T total scores. *P⬍.001 all SLI381 treatment groups compared with placebo.
Fig 5. CGIS-P total score average at baseline, study endpoint, and change for average of all assessment times (morning, afternoon, and late afternoon). *P⬍.001 compared with placebo by Dunnett test following ANCOVA with baseline score as covariate. TABLE 3. Changes From Baseline to Study Endpoint for
CGIS-T Total Score Average for Morning and Afternoon Assess-ments
Treatment Group
Morning Assessment Afternoon Assessment
Baseline Change From Baseline
Baseline Change From Baseline
Placebo 10.1 ⫺0.7 11.4 ⫺1.2
SLI381 10 mg 11.2 ⫺5.0* 11.8 ⫺5.4*
SLI381 20 mg 11.5 ⫺5.4* 12.7 ⫺6.8*
SLI381 30 mg 10.7 ⫺5.8* 11.6 ⫺7.2*
that occurred more frequently in the SLI381 groups were anorexia (21.9% vs 1.9% in the SLI381 and placebo groups, respectively), insomnia (16.6% vs 1.9%), abdominal pain (14.4% vs 9.5%), emotional lability (8.6% vs 1.9%), vomiting (7.2% vs 3.8%), and nervousness (5.6% vs 1.9%). Adverse events that had similar incidence rates with SLI381 and placebo treatment were headache (17.9% vs 21.4%), pharyn-gitis (7.0% vs 9.5%), and increased coughing (5.1% vs 5.2%). Severe adverse events reported after the start of double-blind therapy in⬎1% of participants were insomnia (1.6%), anorexia (1.3%), and emotional la-bility (1.1%), all of which occurred in SLI381-treated participants. There was no clear evidence for a dose-relationship in the incidence of adverse events across the 3 SLI381 treatment groups with the exception of anorexia.
Fifteen participants were withdrawn from the study during double-blind treatment because of ad-verse events (placebo: 6; SLI381–20 mg: 4; SLI381–30 mg: 5). Within the participants who were treated with SLI381, the adverse events that most frequently caused withdrawal included anorexia (3 partici-pants), abdominal disturbances (2 participartici-pants), and nausea (2 participants).
The occurrence of abnormal laboratory values was low and similar in both placebo- and SLI381-treat-ment groups. No apparent trends were seen and most were considered to be clinically insignificant. No clinically significant changes in group mean ECG parameters were observed over the duration of the study; in all cases where abnormalities occurred, findings were deemed harmless, clinically insignifi-cant, or normal by pediatric cardiologists. In regard to vital signs, no significant changes were seen be-tween treatment groups and no significant changes occurred over time.
DISCUSSION
The primary objective of this study was to evaluate the efficacy and safety of SLI381,a single-dose, long-acting formulation of Adderall for the treatment of ADHD in naturalistic school and home settings. This study is one of the largest ADHD medication trials conducted to date, with efficacy assessments of nearly 600 patients. Overall, the findings from this study indicate that: 1) SLI381 10 mg per day gave a significant improvement in treatment of ADHD com-pared with placebo; 2) the maximum effect was reached within the first week of dosing; 3) dose increase by 10 mg at weekly intervals to a maximum Fig 6. Investigator (CGI) and parent (PGA) global improvement
ratings at study endpoint. All comparisons to placebo significant (P⬍.001).
TABLE 4. Changes From Baseline to Study Endpoint for CGIS-P Total Score Average for Morn-ing, Afternoon, and Late Afternoon Assessments
Treatment Group Morning
Assessment
Afternoon Assessment
Late Afternoon Assessment
Baseline Change Baseline Change Baseline Change
Placebo 13.2 ⫺1.7 13.7 ⫺2.0 14.3 ⫺1.4
SLI381 10 mg 12.4 ⫺3.5* 12.5 ⫺4.3* 12.6 ⫺3.7*
SLI381 20 mg 13.1 ⫺4.7† 13.0 ⫺5.1† 14.2 ⫺4.7†
SLI381 30 mg 12.5 ⫺5.7† 13.0 ⫺7.0† 13.3 ⫺5.8†
*P⬍.05 versus placebo using 2-samplettest (without Dunnett test). †P⬍.001 versus placebo using 2-samplettest (without Dunnett test).
TABLE 5. Percent Incidence of the Most Frequently Reported Adverse Events Postrandomization
Adverse Event (COSTART Term)
Percentage of SLI381-Treated Participants Reporting (N⫽374)
Percentage of Placebo-Treated Participants Reporting (N⫽210) All Drug-Related or
Possibly Related
All Drug-Related or Possibly Related
Anorexia 21.9 21.9* 1.9 1.9
Headache 17.9 13.9 21.4 13.8
Insomnia 16.6 16.6* 1.9 1.9
Abdominal pain 14.4 11.5* 9.5 6.2
Emotional lability 8.6 8.6* 1.9 ⬍5
Vomiting 7.2 ⬍5 3.8 ⬍5
Pharyngitis 7.0 ⬍5 9.5 ⬍5
Nervousness 5.6 5.3 1.9 1.9
Nausea 5.1 ⬍5 2.9 ⬍5
Increased cough 5.1 ⬍5 5.2 ⬍5
of 30 mg per day resulted in further improvements that occurred within the first week of each increase in dose; 4) participants treated with SLI381 30 mg per day showed approximately a 5 unit points relative improvement in ADHD behavior, as measured by CGIS-T, over those receiving placebo; and 5) SLI381 was well tolerated. These results document that SLI381 is a safe and effective once-daily dosage form of stimulant medication that lasts throughout the school day and into the early evening.
The findings that one early morning dose of SLI 381 was effective throughout the morning and after-noon as reported by parents and teachers confirm, in the naturalistic setting of home and school, previous results in a laboratory setting.19,20 The previous
study examined pharmacokinetic and pharmacody-namic parameters of three fixed doses of SLI381 com-pared with placebo and Adderall 10 mg in an analog classroom setting and found SLI381 20 mg and 30 mg to produce rapid improvements in behavior and cog-nition by 1.5 hours postdose. These improvements were sustained for up to 12 hours, strongly support-ing a duration of action that covers the school day.
The long acting clinical effects of SLI381 clearly eliminate the need for in school administration. Con-sidering the inherent problems associated with in-school dosing of stimulant medications for ADHD (ie, many schools do not have nursing staff available to administer these medicines; many parents and children do not want to receive their treatment in school because of the potential stigmatizing effects of such procedures; and the medicolegal concerns asso-ciated with the storage and administration of sched-uled medicines in school) the availability of a safe and effective long acting stimulant such as SLI381 is likely to greatly facilitate the treatment of the large number of afflicted youth with ADHD.
Such benefits of SLI381 not only will increase pa-tient privacy and compliance, but are also important to secure a steady clinical effect throughout the school day. Despite the well-documented efficacy of stimulant drugs in the treatment of ADHD, the short duration of action of the immediate release prepara-tions has been associated with therapeutic peaks and valleys with their potential for breakthrough symp-toms in between doses and likely adverse impact on treatment satisfaction.
Of equal clinical relevance is the finding docu-menting that the clinical benefits of SLI381 extend beyond the school day to include time-points after 4:00 pm. Such results indicate that the duration of action of SLI381 should allow for pharmacological support of homework activities, after school athletic and social activities, as well as family life— critical components of the child’s life.
A clear dose-response relationship was evident across all efficacy assessments, with increased im-provement at successive increases in dose. In fact, the main efficacy endpoint, the CGIS-T total score aver-age, reached normalized values for the SLI381 30-mg group. In the absence of dose-limiting adverse effects when treating patients with ADHD, much thought should be given to increasing the dose to an optimal level. Although lower doses may not be
subthera-peutic, this study demonstrates that optimal results were seen at the 30-mg dose of SLI381.
Study medication was very well tolerated and the incidence of adverse events compares favorably with that of immediate-release compounds. There was lit-tle evidence of a dose-response relationship in safety parameters across the SLI381 treatment groups. Thus, increasing the dose had no apparent influence on tolerability. The exception to this may be in the incidence of reported anorexia. However, posthoc analysis of reported anorexia showed that treatment naı¨ve participants had significantly more problems with this (33.6% reporting) than did those partici-pants with prior experience with ADHD medications (16.2% reporting). Because this was a shot-term trial of 3 weeks duration, it can not be determined from these data whether the reported incidence of this adverse event would abate over time. A 24-month, open-label trial is ongoing and may better define the long-term adverse event profile of this medication.
Noteworthy is the clean cardiovascular profile of SLI381 as evidenced by repeated ECG measure-ments. This is important to emphasize in light of recent concerns regarding potential cardiovascular effects of stimulant medications.
Subgroup analyses showed the same, positive im-provements for boys and girls with ADHD. In fact, considering the sizeable representation of girls, this study represents one of the largest clinical trials of girls with ADHD ever conducted. Although almost all of the available literature on ADHD is limited to boys with this disorder, recent work documents that ADHD is equally disabling in boys and girls with ADHD.21Thus, the findings of similar benefits
asso-ciated with SLI381 treatment in boys and girls with ADHD are very encouraging and extend to females the well-documented therapeutic benefits of psycho-stimulants in the treatment of ADHD.
Although the majority of patients in this study had previous exposure to stimulant medication, a sub-stantial minority (⬃34%) were treatment naı¨ve. The subgroup analyses showed the same, positive im-provements for patients with a history of stimulant treatment as for those with no previous exposure to stimulant medication. This demonstrates the efficacy of SLI381 across both patient groups.
Because our sample included a narrow develop-mental window of children 6 to 12 years, it is unclear whether our results will generalize to older age groups. Considering the wide range of benefits asso-ciated with the long duration of action of SLI381, it is likely that other age groups will also benefit from this pharmacologic profile. Clearly, additional clini-cal trials are needed to document the efficacy and safety of SLI381 in adolescents and adults with ADHD.
CONCLUSION
SLI381 is a safe and efficacious treatment in chil-dren for the treatment of ADHD. The extended-re-lease nature of this new formulation of mixed am-phetamine salts allowed adequate control of the signs and symptoms of ADHD using a once-a-day dosing schedule. Dose-related improvements in chil-dren’s behavior at school and home when compared with placebo were seen after the administration of 1 SLI381 dose of 10 mg to 30 mg in the morning, in both morning and afternoon as measured by both teacher and parent ratings, and continued into late afternoon as measured by parent ratings. SLI381 was effective in participants with previous experiences of stimulant treatment for ADHD, and in participants who were naı¨ve to ADHD treatment. The use of this extended-release formulation would simplify medi-cation schedules for children who are in school, and could improve compliance. Dosing in the morning before the child left for school would ensure protec-tion against ADHD symptoms during and beyond the school day.
ACKNOWLEDMENT
This study was supported by Shire Pharmaceutical Develop-ment Inc, Rockville, Maryland.
APPENDIX SLI381.301 Study Investigators
Howard Abikoff, PhD, New York University Child Study Cen-ter, New York, New York
Paul J. Ambrosini, MD, Medical College of Pennsylvania, Phil-adelphia, Pennsylvania
L. Eugene Arnold, MD, Ohio State University, Columbus, Ohio Joseph Biederman, MD, Massachusetts General Hospital, Bos-ton, Massachusetts
Jeffery L. Blumer, MD, University Hospitals of Cleveland, Cleveland, Ohio
Samuel W. Boellner, MD, Clinical Study Centers, L.L.C., Little Rock, Arkansas
Larry Brown, MD, Children’s Hospital of Philadelphia, Phila-delphia, Pennsylvania
Ronald T. Brown, PhD, Medical University of South Carolina, Charleston, South Carolina
Charles D. Casat, MD, Behavioral Health Center, Charlotte, North Carolina
Mark C. Chandler, MD, North Carolina Neuropsychiatry, PA, Chapel Hill, North Carolina
Edward, Cherlin, MD, Valley Clinical Research, El Centro, Cal-ifornia
C. Keith Conners, PhD, Duke University Medical Center, Durham, North Carolina
Daniel Connor, MD, University of Massachusetts Medical Cen-ter, WorcesCen-ter, Massachusetts
Daniel Coury, MD, Pediatric Clinical Studies Center, Colum-bus, Ohio
Andrew J. Cutler, MD, Coordinated Research of Florida, Winter Park, Florida
W. Burleson Daviss, MD, Dartmouth-Hitchcock Medical Cen-ter, Lebanon, New Hampshire
Carlos Figueroa, MD, Advanced Psychiatric Group, Rosemead, California
L. Matthew Frank, MD, Dominion Psychiatric Associates, Vir-ginia Beach, VirVir-ginia
Laurence L. Greenhill, MD, New York State Psychiatric Insti-tute, New York, New York
Saul Helfing, MD, Oregon Center for Clinical Investigations, Inc, Lake Oswego, Oregon
Sharon L. Hirsch, MD, Childrens Memorial Hospital, Chicago, Illinois
Joseph P. Horrigan, MD, University of North Carolina, Chapel Hill, North Carolina
James Hudziak, MD, University of Vermont/ Fletcher Allen Healthcare, Burlington, Vermont
Martin Kremenitzer, MD, Associated Neurologists, PC, Dan-bury, Connecticut
Kara Lewis, MD, Barrow Neurologic Group, Phoenix, Arizona Robert S. Lipetz, DO, Encompass Clinical Research, Spring Valley, California
Thomas M. Lock, MD, State University of New York, Buffalo, New York
Peter D. Londborg, MD, Seattle Clinical Research Center, Seat-tle, Washington
Frank A. Lopez, MD, Children’s Development Center, Mait-land, Florida
Keith McBurnett, PhD, University of Chicago, Chicago, Illinois James T. McCracken, MD, UCLA Neuropsychiatric Institute, Los Angeles, California
Denis Mee-Lee, MD, Hawaii Clinical Research Center, Hono-lulu, Hawaii
Jeffery Newcorn, MD, Mt. Sinai Medical Center, New York, New York
Donna Palumbo, PhD, University of Rochester School of Med-icine, Rochester, New York
Anil Patel, MD, The Damluji Research Center, Vista, California Steven R. Pliszka, MD, University of Texas Health Science Center, San Antonio, Texas
George Realmuto, MD, University of Minnesota Medical School, Minneapolis, Minnesota
Murray Rosenthal, DO, Behavioral and Medical Research, LLC, San Diego, California
Richard L. Rubin, MD, Miami Research Associates, Miami, Florida
Keith Saylor, PhD, Neuroscience, Inc, Bethesda, Maryland Ward T. Smith, MD, Pacific Northwest Clinical Research, Port-land, Oregon
Michael Sternberg, MD, Advanced Research Center, Wood-bridge, Virginia
Harvey Tilker, PhD, Four Rivers Clinical Research, Inc, Paducah, Kentucky
Sharon Wigal, PhD, University of California at Irvine, Irvine, California
Mark Wolraich, MD, Vanderbilt University, Nashville, Tennes-see
Daniel R. Wynn, MD, Consultants in Neurology, LTD, North-brook, Illinois
REFERENCES
1. American Academy of Pediatrics, Committee on Quality Improvement and Subcommittee on Attention-Deficit/Hyperactivity Disorder. Clini-cal practice guideline: diagnosis and evaluation of the child with attention-deficit/hyperactivity disorder.Pediatrics.2000;105:1158 –1170 2. American Psychiatric Association.Diagnostic and Statistical Manual for Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994
3. Biederman J, Faraone S, Milberger S, et al. A prospective 4-year fol-low-up study of attention-deficit hyperactivity and related disorders.
Arch Gen Psychiatry.1996;53:437– 446
4. Biederman J, Mick E, Faraone SV. Normalized functioning in youths with persistent attention-deficit/hyperactivity disorder.J Pediatr.1998; 133:544 –551
5. Barkley RA. Developmental course, adult outcome, and clinic-referred ADHD adults. In: Barkley RA, ed. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment.2nd ed. New York, NY: Guilford Press; 1998:186 –224
6. Mannuzza S, Klein R, Bessler A, Malloy P, Lapadula M. Adult outcome of hyperactive boys: educational achievement, occupational rank, and psychiatric status.Arch Gen Psychiatry.1993;50:565–576
7. Barkley RA, Fischer M, Edelbrock CS, Smallish L. The adolescent out-comes of hyperactive children diagnosed by research criteria: I. An 8-year prospective follow-up study.J Am Acad Child Adolesc Psychiatry.
1990;29:546 –557
8. Swanson JM, McBurnnet K, Wigal T, et al. Effect of stimulant medica-tion on children with attenmedica-tion deficit disorder: a “review of reviews.”
Exceptional Children.1993;60:154 –162
life cycle.J Am Acad Child Adolesc Psychiatry.1996;35:409 – 432 10. Greenhill LL, Halperin JM, Abikoff H. Stimulant medications.J Am Acad
Child Adolesc Psychiatry.1999;38:503–512
11. Swanson JM, Wigal S, Greenhill LL, et al. Analog classroom assessment of Adderall in children with ADHD.J Am Acad Child Adolesc Psychiatry.
1998;37:519 –526
12. Pelham WE, Aronoff HR, Midlam JK, et al. A comparison of Ritalin and Adderall: efficacy and time-course in children with attention-deficit/ hyperactivity disorder. Pediatrics. 1999;103(4). Available at: http:// www.pediatrics.org/cgi/content/full/103/4/e43
13. Pelham WE, Gnagy EM, Chronis AM, et al. A comparison of morning-only and morning/late afternoon Adderall to morning-morning-only, twice-daily, and three times-daily methylphenidate in children with attention-deficit/hyperactivity disorder.Pediatrics.1999;104:1300 –1311 14. Manos MJ, Short EJ, Findling RL. Differential effectiveness of
methyl-phenidate and Adderall in school-age youths with attention-deficit hyperactivity disorder.J Am Acad Child Adolesc Psychiatry. 1999;38: 813– 819
15. Pliszka SR, Browne RG, Olvera RL, Wynne SK. A double-blind, place-bo-controlled study of Adderall and methylphenidate in the treatment of attention-deficit/hyperactivity disorder.J Am Acad Child Adolesc Psy-chiatry.2000;39:619 – 626
16. Ahmann PA, Theye FW, Berg R, Linquist AJ, Van Erem AJ, Campbell LR. Placebo-controlled evaluation of amphetamine mixture–
dextro-amphetamine salts and dextro-amphetamine salts (Adderall): efficacy rate and side effects.Pediatrics.2001;107(1). Available at: http://pediatrics. org/ cgi/content/full/107/1/e10
17. Michaels MA, Weston IE, Zhang Y, Tulloch SJ. Pharmacokinetics of SLI381, a two-component extended-release formulation of mixed am-phetamine salts, administered in fasted and fed states, and sprinkled on food. Poster presented at the 41st Annual Meeting of the NIMH New Clinical Drug Evaluation Unit Program; May 29, 2001; Phoenix, AZ 18. Shaffer D, Fisher P, Lucas CP, Dulcan MK, Schwab-Stone ME. NIMH
Diagnostic Interview for Children Version IV (NIMH DISC-IV): descrip-tion, differences from previous versions, and reliability of some com-mon diagnoses.J Am Acad Child Adolesc Psychiatry.2000;39:28 –38 19. McCracken JT, Biederman J, Greenhill LL, et al. Analog classroom
assessment of SLI381 for the treatment of ADHD. Poster presented at the 47th Annual Meeting of the American Academy of Child and Adolescent Psychiatry; October 26, 2000; New York, NY
20. McGough JJ, Greenhill LL, Biederman J, et al. PK/PD analyses of SLI381 in pediatric ADHD. Poster presented at the 47th Annual Meeting of the American Academy of Child and Adolescent Psychiatry; October 27, 2000; New York, NY
21. Biederman J, Faraone SV, Mick E, et al. Clinical correlates of ADHD in females: findings from a large group of girls ascertained from pediatric and psychiatric referral sources.J Am Acad Child Adolesc Psychiatry.
1999;38:966 –975
MEDICAL STUDENTS SUE OVER RESIDENCY SYSTEM
“A class-action lawsuit to be filed in Washington challenges the matching program on antitrust grounds. The suit says the defendants, including 7 medical organizations and more than 1,000 private hospitals, have used the program to keep residents’ wages low and hours long. Almost all first-year residents make less than $40,000 a year and often work 100-hour weeks.
If the suit is successful, the nation’s health care system faces an enormous financial liability and the prospect of being forced to change the way that gener-ations of doctors have been trained.
More than 80% of first-year residency positions are offered exclusively through the program, known formally as the National Resident Matching Program. The matches are based on ranked lists submitted by hospitals and the 15,000 or so students, and both sides agree in advance to accept the match. . . There is no room for negotiations about wages, hours, or other terms of employment. As a conse-quence, the plaintiffs say, the hospitals, which share detailed salary information with each other, can force residents to accept below-market wages for 3 to 8 years, depending on specialty, of their residencies.
The stakes in the new suit are high. The complaint does not specify how much money the plaintiffs seek, but they claim to represent a class of 200,000 residents. If residents’ fair market salaries were determined to be $100,000, say, the sums at issue for a single year would exceed $12 billion, and because this is an antitrust case, the damages would be automatically tripled.”
New York Times.May 7, 2002
DOI: 10.1542/peds.110.2.258
2002;110;258
Pediatrics
Joseph Biederman, Frank A. Lopez, Samuel W. Boellner and Mark C. Chandler
Disorder
SLI381 (Adderall XR) in Children With Attention-Deficit/Hyperactivity
A Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Study of
Services
Updated Information &
http://pediatrics.aappublications.org/content/110/2/258
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/110/2/258#BIBL
This article cites 14 articles, 2 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/therapeutics_sub Therapeutics
http://www.aappublications.org/cgi/collection/pharmacology_sub Pharmacology
ctivity_disorder_adhd_sub
http://www.aappublications.org/cgi/collection/attention-deficit:hypera Attention-Deficit/Hyperactivity Disorder (ADHD)
l_issues_sub
http://www.aappublications.org/cgi/collection/development:behaviora Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.110.2.258
2002;110;258
Pediatrics
Joseph Biederman, Frank A. Lopez, Samuel W. Boellner and Mark C. Chandler
Disorder
SLI381 (Adderall XR) in Children With Attention-Deficit/Hyperactivity
A Randomized, Double-Blind, Placebo-Controlled, Parallel-Group Study of
http://pediatrics.aappublications.org/content/110/2/258
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.