Ectodermal dysplasia is a rare abnormality of ectodermal structures and can be found mainly in boys. Its occurrence among newborn ranges from 1:10,000 to 1:100,000. It is defined as abnormali− ties in two or more ectodermal structures, with symptoms of trichodysplasia, dyshydrosis, ony− chodysplasia, and dental anomalies [1]. Clinical recognition of ectodermal dysplasia always requires X−ray imaging diagnostics, preferably pantomographic imaging [2, 3]. Although the symptoms of dysplasia have been described for more than 150 years, the very name of ectodermal dysplasia was proposed in 1929. The author of the term, A.A. Weech, divided it into two main vari− ants: anhydrotic dysplasia, later termed ‘major
form’ by Franceschetti, and hydrotic dysplasia – ‘minor form’ [4]. The hydrotic form is inherited in the autosomal dominant mode, and is character− ized by oligodontia, deformed nails, sparse fair hair, lack of eyebrows and eyelashes, brown skin pigmentation, and excessive skin thickness on palms and feet. Anhydrotic dysplasia is nowadays also called hypohydrotic due to a non−total lack of sweat glands. Besides the hydrotic form, ectoder− mal dysplasia may also be characterized by light pigmentation of the skin, wrinkled skin, frequent co−occurrence of lack of eyebrows and eyelashes, protruding forehead, narrow nose, ear deformation (so called ‘satyr’s ear’), thick lips, and atypical conical shape of retained teeth. All these features
B
OGUMIŁAF
RĄCZAK1, D
ANUTAG
ÓRNIAK2, H
ALINAE
Y−C
HMIELEWSKA1, E
WAS
OBOLEWSKA1Difficulties in the Prosthetic Treatment of Patients
with Ectodermal Dysplasia – Case Report
Trudności w leczeniu protetycznym pacjentów
z zespołem ektodermalnym – opis przypadków
1Katedra i Zakład Protetyki Stomatologicznej Pomorskiej Akademii Medycznej w Szczecinie 2Katedra i Zakład Ortodoncji Pomorskiej Akademii Medycznej w Szczecinie
Dent. Med. Probl. 2009, 46, 1, 126–130 ISSN 1644−387X
CLINICAL CASE
© Copyright by Wroclaw Medical University and Polish Stomatological Association
Abstract
Ectodermal dysplasia is a syndrome characterized by abnormalities in ectodermal structures. Its occurrence among newborn ranges from 1:10,000 to 1:100,000. The main clinical symptoms of ectodermal dysplasia are the inabili− ty to perspire (anhydrosis), poor hair (hypotrichosis), and oligodontia of deciduous and permanent teeth. Facial fea− tures exhibit a more or less intense underdevelopment of the middle and lower part of the face, caused by agene− sia of alveolar processes. In this paper the authors present two cases of ectodermal dysplasia: (1) a 2.5 year old child with full symptoms of dysplasia and (2) an 18 year old patient with oligodontia of numerous permanent teeth (Dent. Med. Probl. 2009, 46, 1, 126–130).
Key words:anhydrotic ectodermal dysplasia, symptoms, early treatment.
Streszczenie
Charakterystyczną cechą dysplazji ektodermalnej jest niedorozwój tkanek pochodzenia ektodermalnego. Częstotliwość występowania dysplazji ektodermalnej według różnych autorów wynosi od 1 : 10.000 do 1 : 100.000 urodzonych dzieci. Zespół dysplazji ektodermalnej charakteryzują trzy główne objawy kliniczne: niepotliwość, słabe owłosienie, braki zawiązków zębów mlecznych i stałych. W rysach twarzy stwierdza się bardziej lub mniej nasilony niedorozwój środkowego i dolnego piętra twarzy, spowodowany niewykształceniem wyrostków zębo− dołowych. Autorzy przedstawiają dwa przypadki pacjentów z dysplazją ektodermalną: dziecka 2,5−letniego z pełnoobjawowym zespołem ektodermalnym oraz pacjenta 18−letniego z licznymi brakami zębów stałych (Dent. Med. Probl. 2009, 46, 1, 126–130).
contribute to the characteristic senile facial appearance of children with ectodermal dysplasia. The dysplasia is accompanied by body hyperther− mia with fevers and seizures, especially in infants. Patients also suffer from difficulties within eating and chewing, as well as with speech [5−7]. Many authors reported a family occurrence of hypohy− drotic dysplasia, X−chromosomal recessively inherited. Female carriers have less intense symp− toms, while full symptoms can be observed in men. In this mode of inheritance, a female carrier may transmit the mutated gene to half of her chil− dren, regardless of sex. A male carrier has healthy sons and daughters that are carriers [7, 8].
In this paper the authors present the proce− dures in early and late orthodontic and prosthetic treatment of patients with hypohydrotic dysplasia. Children with ectodermal abnormalities require, beside the dental treatment, also an increased psy− chological support. Oligodontia and presence of atypical teeth lead to alienation and loneliness. The child becomes shy, aloof, and hence has prob− lems with proper psychoemotional development. Usually children with dysplasia are also less active and less talkative than healthy children [6, 8]. Oligodontia affects biting off the food and chew− ing, thus leading to worse nutrition [9]. Considering all the aformentioned problems, early orthodontic and prosthetic treatment helps the pre− vent negative effects on the child’s body and psy− che. Full rehabilitation requires long−term treat− ment and teamwork from the pedodontist, ortho− dontist, prosthodontist and oral surgeon [10]. Children are very appreciative patients and per− fectly adapt to dentures.
The mode of treatment depends on the patient’s age, the number of missing teeth and the quality of existing teeth, position on the dental arch, and the type of co−existing dental and occlusal anomalies [11]. It should be emphasised that a lack of orthodontic and prosthetic rehabilitation during the growth of the child leads to the disfunction of muscles and therefore to an increase in malocclu− sion and deteriorated facial features. This in turn may lead to difficulties in later treatment [12].
A dynamic development in prosthetic care has resulted in new solutions for patients that require movable dentures. Such dentures should be con− structed and incorporated into the stomatognathic system so they do not constitute an iatrogenic fac− tor, but instead have a therapeutic and preventive function. A good denture needs good basic mate− rial. One should consider physicochemical prop− erties and also the reaction of the material in the oral cavity. Dental surgeons are mainly interested in the deposition of plaque and bacteria on the denture surface, and also the allergizing proper−
ties of prosthetic materials. No less important, both for the dental surgeon and the patient, is the appearance of the denture and the durability of its colour [13]. Acrylic may be a potential pathogen− ic factor for the adjacent mucous membrane of the oral cavity. 20−70% patients using movable den− tures experience prosthetic stomatopathies. The alternative solution may be acetal resin, charac− terized by a high resistance to abrasion, perfect stretchability and mechanical strength, high resilience, low thermal conduction, and appropri− ate rigidity. It is also thought to be non−toxic and non−allergic [13, 14].
Case Report
Case no. 1
A 2.5 year old boy was directed to the Orthodontics Institute at the Pomeranian Medical Academy from the Medical Genetics Department at the Child Health Center in Warsaw. The child was hospitalized due to unexplained recurring fevers. Interviews with the child’s family revealed the occurrence of ectodermal dysplasia in his mother and sister.
During clinical examination typical symptoms were observed: dry and bright hypoplastic skin with a decreased perspiration, weak hair and con− siderable oligodontia. Also typical facial features were observed: shorter middle and lower section of the face, caused by an abnormal development of alveolar processes and lack of some teeth; deeper chin furrow and everted lower lip; facial skin with visible inflammations in the area of deep−set eyes (Fig. 1).
Fig. 1. 2.5 year old patient M.Ś. before the beginning of treatment
Ryc. 1. 2,5−letni pacjent M.Ś. przed rozpoczęciem leczenia
Intraorally, two teeth with atypical structures were observed. The pantomographic image did not show any remnants of any other deciduous teeth, only poorly visible probable buds of permanent teeth: 11, 21, 23, 31 and 41 (Figs. 2, 3).
Prosthetic and orthodontic treatment was applied. After the vertical dimension of occlusion had been determined, upper and lower denture were made. The vertical dimension of occlusion was very difficult to determine (Figs. 5, 6). The dentures were made using Kalot’s method and artificial teeth with flat cusps. Due to the early age of the patient, the dentures were a form of ortho− dontic appliance. The dentures were equipped with orthodontic elements enabling the correction of dental appliances and having a positive effect on the development of the jaw (Fig. 6). The patient easily accepted the dentures and his new appear− ance (Fig. 7). However, dentures for children require changes throughout the growth and devel− opment of the stomatognathic system, and thus the child remains under the constant care of an ortho− dontist and prosthodontist.
Case no. 2
An 18 year old man was directed to the Orthodontic Department at the PMU in Szczecin from a local practice in Gryfice. The patient had not had any orthodontic or prosthetic treatment before. The family interview revealed a less pro− nounced form of ectodermal dysplasia in a cousin.
During clinical examination, typical symp− toms were observed: dry, bright and hypoplastic skin with decreased perspiration, weak hair, con− siderable oligodontia. The middle and lower sec− tion of his face was shortened due to the abnor− malities in alveolar processes. The chin furrow was deeper than normal, lower lip everted. The excess frontal tubers, saddle nose, thick and evert− ed lips were observed. The symmetry of the face was maintained (Fig. 8). Intraoral examination showed narrow edges of alveolar processes and the underdevelopment of the jaw and mandible. Two retained deciduous teeth: 55 and 75, and 11 permanent teeth were observed in the jaw: two central incisors, two fillings, one bicuspid, and two molars; and in the mandible: two fillings and two molars (Figs. 9, 10).
Fig. 2.Intraoral picture of the patient. Remaining two deciduous teeth of a characteristic cone like shape
Ryc. 2.Wewnątrzustne zdjęcie pacjenta. Pozostające zęby mleczne o charakterystycznym stożkowatym kształcie
Fig. 3.Patient with a visible occlusion rim
Ryc. 3. Pacjent z widocznym wzornikiem zwarciowym
Fig. 5. 2.5 year old patient M.Ś. after the completion of the first part of treatment
Ryc. 5. 2,5−letni pacjent M.Ś. po realizacji pierwszej części leczenia
Fig. 4.2.5 year old patient M.Ś. after completing the first part of treatment
Ryc. 4. 2,5−letni pacjent M.Ś. po zakończeniu pierw− szego etapu leczenia
The patient was given orthodontic treatment with a partially fixed braces in the upper arch in order to line incisors, close the diastema and restoration of the site for lateral incisors. After removal of the braces, retentive treatment was applied, and upper and lower denture were made from acetal resin. The patient is under constant prosthetic and orthodontic care.
Discussion
The emotional development of children often depends on the acceptance from the environment. A child at kindergarten age with visible physical defects has serious problems with being accepted by peers. A considerable number of missing teeth also impairs the basic functions of the stomatog− nathic system and affects the development of the jaw and dental arches, leading to facial and occlusal anomalies.
Children with ectodermal dysplasia frequently experience psychological problems. They are less active, more shy and often very silent. Due to the great number of missing teeth, young patients have problems with biting off and chewing food, which affects their nutrition and speech. The feel− ing of being different has a disadvantegous effect both psychoemotional development which often leads to serious trauma. Early orthodontic and prosthetic rehabilitation that restores the correct function of the stomatognathic system not only improves speech, but also enables proper psychoe− motional development. In mature patients, it is possible to carry out reconstruction with implants, which to a great extent improves the function of prosthetic appliances.
It should be mentioned here that patients with ectodermal dysplasia should be under the treatment and observation of a team of specialists (pediatri− cian, dermatologist, pedodontist, orthodontist, pro− sthodontist) during the whole time of growth.
Conclusions
Patients with ectodermal dysplasia require multi−specialized treatment. Interdisciplinary treatment should be implemented in the earliest stage of the child’s growth. Orthodontic and pros− thetic treatment is necessary for correct develop− ment of the stomatognathic system and the psyche of the young patient.
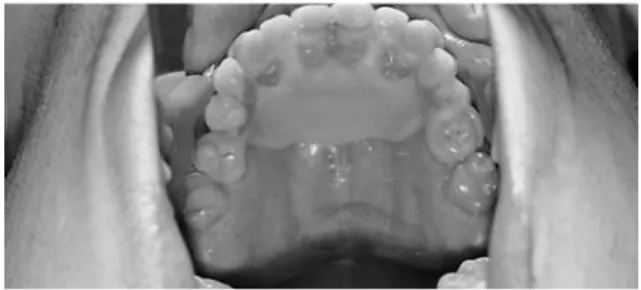
Fig. 7.Intraoral picture of the patient. Upper dental arch
Ryc. 7.Wewnątrzustne zdjęcie pacjenta. Łuk zębowy górny
Fig. 8.Intraoral picture of the patient. Lower dental arch
Ryc. 8.Wewnątrzustne zdjęcie pacjenta. Łuk zębowy dolny
Fig. 9.Intraoral picture of the patient during treatment
Ryc. 9.Wewnątrzustne zdjęcie pacjenta podczas leczenia
Fig. 10.Patient S.H. after treatment. Upper dental arch
Ryc. 10.Pacjent S.H. po zakończeniu leczenia. Łuk zębowy górny
Fig. 6.18 year old patient S.H. before the beginning of treatment
Ryc. 6. 18−letni pacjent S.H. przed rozpoczęciem leczenia
References
[1] ZADURSKAM., CHABEREKS., KUBANIM., SIEMIŃSKA−PIEKARCZYK B., NASTALSKAE., LASKOWSKAM.: Ocena struktury morfologicznej kości u pacjentów z dysplazją ektodermalną. Prot. Stomatol. 2005, 55, 163−168. [2] BIEDZIAKB.: Występowanie wad zgryzu u pacjentów z oligodoncją. Dent. Med. Probl. 2004, 41, 483−488. [3] BIEGAŃSKI T., CZARNY−RATAJCZAK M.: Podłoże genetyczne oraz obrazy radiologiczne osteochondrodysplazji
wywołanych zaburzeniami transportu siarczanów. Pol. J. Radiol. 2002, 67, 94−99.
[4] BIEDZIAKB.: Etiologia i występowanie agenezji zębów – przegląd piśmiennictwa. Dent. Med. Probl. 2004, 41, 531–535.
[5] ROUSETT−CARON M.M., DELFOSSE C., NOULE M., BEAUVENTRE L., LAFFORGUE P.: Hypodontia, oligodontia, anodontia and syndromem of developmental anomalies. Dent. Med. Probl. 2003, 40, 109−115.
[6] JAKÓB−DOLEŻALK., KNYCHALSKA−KARWANZ., PIĄTKOWSKAE.: Wrodzona dysplazja entodermalna. Czas. Stomat. 2000, 53, 523−530.
[7] ROSNOWSKA−MAZURKIEWICZ A., WOJTASZEK−SŁOMIŃSKA A.: Anhydrotyczna dysplazja ektodermalna. Ortop. Szczęk. Ortod. 2000, 3, 17−22.
[8] ROSNOWSKA−MAZURKIEWICZA., WOJTASZEK−SŁOMIŃSKAA.: Ocena wzrostu twarzowej części czaszki u pacjentów z anhydrotyczną dysplazją ektodermalną. Ortop. Szczęk. Ortod. 2001, 2, 3−7.
[9] REMISZEWSKIA.: Przyczynek do zagadnienia występowania dysplazji ektodermalnej u dzieci. Ped. Pol. 1983, 58, 299−305.
[10] GROTOWSKI T. A.: Rehabilitacja implantoprotetyczna w przypadkach hipodoncji siekaczy górnych bocznych. Obserwacje wieloletnie. Magazyn Stomatol. 2006, 16, 6, 50−55.
[11] WIŚNIEWSKA G., MAJEWSKI S., MATRASZEK H.: Rehabilitacja pacjentów z wrodzonym brakiem zawiązków zębowych. Magazyn Stomatol. 2000, 10, 4, 50−53.
[12] CIECHOWICZK., MATEŃKOD., FEDERT., KUBANIM., ZADURSKAM.: Zespołowe leczenie ortodontyczno−chirur− giczno−protetyczne pacjentów z zespołem ektodermalnym. Protet. Stomatol. 2007, 57, 157−162.
[13] FRĄCZAKB., SOBOLEWSKAE., KIJAKE., ŻWIRM.: Wpływ pH śliny na strukturę żywicy acetalowej. Nowocz. Tech. Dentyst. 2007, 59−65.
[14] SOBOLEWSKAE., FRĄCZAKB., CZARNOMYSY−FUROWICZD., EY−CHMIELEWSKAH., KARAKULSKAJ.: Bacteria adhe− sion to the surface of various prosthetic materials. Ann. Acad. Med. Stet. 2007, 53, 68−71.
Address for correspondence:
Bogumiła Frączak
Katedra i Zakład Protetyki Stomatologicznej PAM Powstańców Wielkopolskich 72
70−111 Szczecin Poland
Tel.: +48 91 466 17 15
E−mail: [email protected] Received: 23.02.2009
Revised: 5.03.2009 Accepted: 6.04.2009
Praca wpłynęła do Redakcji: 23.02.2009 r. Po recenzji: 5.03.2009 r.