PERIAPICAL MICROSURGERY: A 4-D ANALYSIS OF HEALING PATTERNS
Daniel Crossen
A thesis submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Science in the School
of Dentistry (Endodontics).
Chapel Hill 2018
Approved By:
Peter Z Tawil
Thiago Morelli
ABSTRACT
Daniel Crossen: Periapical Microsurgery: A 4-D Analysis of Healing Patterns (Under the direction of Peter Tawil)
This study analyzed the volumetric healing pattern of the buccal plate after
periapical microsurgery over time, with focus on the bucco-lingual thickness of bone
and the regression of the surface contour of the cortical plate. Twelve surgical sites
were analyzed in vivo at least one year following periapical. Volumetric healing was analyzed by converting pre-operative and post-operative CBCT images into digital
3-Dimensional models; then registering the models to be able to analyze the changes in
volume over time. Analysis was completed using the software “GeoMagic,” which
allowed for registration of the volumes, calculation of volume change, and a calculation
of the margin of error. Results showed the reduction of bucco-lingual thickness and the
regression of the cortical plate to be within the margin of error in all cases. It is
therefore concluded that periapical microsurgery does not cause thinning of the
ACKNOWLEDGEMENTS
This research was supported by a grant from the AAE Foundation for
Endodontics. It was also supported by the 2016-2017 Dr Shizuko Yamauchi
Endodontics Graduate Student Award, given by the Yamauchi family and the Dental
Foundation of North Carolina, INC.
Thesis Mentor: Dr. Peter Z. Tawil
Thesis Advisor: Dr. Thiago Morelli
Thesis Advisor: Dr. Donald Tyndall
UNC Dept of Endodontics: Dr. Ashraf Fouad, Donna Perdue, Cindy Hynes, Neldy
Pagan
ITK-SNAP software: http://www.itksnap.org
GeoMagic Software: https://www.3dsystems.com/software
TABLE OF CONTENTS
List of Tables . . . vii
List of Figures . . . viii
List of Pictures . . . ix
Thesis Introduction . . . 1
References . . . 3
Review of Literature . . . 4
i: Periapical Microsurgery a: History . . . 4
b: Microsurgical Technique . . . 6
c: Indications . . . 8
d: Tissue Considerations . . . 10
e: Traditional Outcome Measurements/Criteria . . . 12
f: Gap of Knowledge . . . 13
ii: CBCT a: Development and Implementation of CBCT in the Dental Office . . . 14
b: CBCT use in the evaluation of healing after periapical microsurgery . . . 16
c: CBCT as used in this study . . . 17
iii: 3-D Software a: ITK-SNAP and Conversion to .STL . . . 18
b: Geomagic . . . 19
Formatted Sections for the Journal of Endodontics
i: Introduction . . . 26
ii: Materials and Methods . . . 28
iii: Results . . . 31
iv: Discussion . . . 34
v: Conclusion . . . 35
References . . . 37
Thesis Conclusion . . . 41
LIST OF TABLES
LIST OF FIGURES
Figure 1 - Boxplot of the volume change of the buccal cortical plate . . . 33
Figure 2 - Graphic representation of the volume change in mm3 compared
to the average error in mm . . . 34
Figure 3 - Graphic representation of the time elapsed between periapical
LIST OF PICTURES
Picture 1 - Screenshot of a pre-operative .STL file after segmentation using ITK-SNAP . . . 42
Picture 2 - Screenshot of .STL after being imported into “GeoMagic” . . . 43
Picture 3 - Screenshot of a post-op .STL file after segmentation using ITK-SNAP . . . 44
Picture 4 - Screenshot of post-operative .STL after importation into “GeoMagic.” . . . 45
Picture 5 - Screenshot of color map from “GeoMagic” showing changes
in surface contour between pre-operative and post-operative .STL volumes . . . 46
Picture 6 - Cross-sectional image from “GeoMagic” . . . 47
Picture 7 - Selection of area of interest using “GeoMagic” . . . 48
THESIS INTRODUCTION
Endodontics has been defined as the diagnosis, prevention, and treatment of
apical periodontitis. Non-surgical root canal treatment, often referred to as “getting a
root canal,” is often the first line of treatment for apical periodontitis if the tooth is to be
retained. When infection persists or returns, further treatment is warranted (1). This
further treatment is divided into two categories: non-surgical root canal retreatment, and
apical surgery. Modern surgical techniques and materials are referred to as “periapical
microsurgery” (2). While the ability of the periapex to heal following non-surgical
removal of microbes has been demonstrated since Kakehashi, Stanley, and
Fitzgerald’s seminal article in 1965 (3), the healing of the periapex following apical
surgery has not been as well studied.
Although studies have consistently shown healing to occur following apical
surgery, they have focused simply on the reduction of the apical lesion and
regeneration of the lamina dura (4-7), or, in some of the cone-beam computed
tomography (CBCT) studies, the Hounsfield units of the periapical area (8). Even then,
the sample population sizes have been small enough to render the power of the study
too small to achieve statistical significance in many of their findings. To date no study
has analyzed the volumetric patterns of healing, including their effects on the cortical
plate and bucco-lingual ridge thickness. Until recently, this would have been
counterparts (9), and without surgical re-entry, there was no way to analyze healing in vivo. However, modern CBCT now allows us to examine hard tissue changes in vivo utilizing a non-invasive approach (10). By measuring the volume and bucco-lingual
thickness of healed bone, clinicians will have the knowledge of whether grafting is
prudent at the time of periapical microsurgery in order to prevent later grafting requiring
surgical re-intervention should implants be necessary at a future date.
The aim of this study was to evaluate the volumetric healing of hard tissue over
time after periapical microsurgery; with specific focus on the bucco-lingual thickness of
bone and the surface contour of the cortical plate. The study converted CBCT images
into 3-D models using the software, “ITK-SNAP” (11), and then overlaid, or registered
the models made prior to surgery with those made 1-5 years after surgery, and
calculated the changes in bone volume using the software “Geomagic.” Analysis was
REFERENCES
1. Friedman S. Considerations and concepts of case selection in the management of post‐treatment endodontic disease (treatment failure). Endodontic Topics. 2002;1:54-78. 2. Tawil P, Saraiya V, Galicia J, Duggan D. Periapical Microsurgery: The Effect of Root
Dentinal Defects on Short- and Long-term Outcome. JOURNAL OF ENDODONTICS. 2015;41:22-27.
3. KAKEHASHI, S., STANLEY, H., & FITZGERALD, R. (1965). Effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology, 20(3), 340-340.
4. Lingaraj JB, Kotrashetti SM, Gupta N. Healing assessment of osseous defects of periapical lesions with use of freeze dried bone allograft. Journal of Maxillofacial and Oral Surgery. 2009;8:362-365.
5. Tanomaru-FIlho M, Jorge ÉG, Guerreiro-Tanomaru JM, Reis JMS, Spin-Neto R, Gonçalves M. Two- and tridimensional analysis of periapical repair after endodontic surgery. Clinical Oral Investigations. 2015;2014;19:17-25.
6. Rud, J., Andreasen, J.O., Mo¨ ller Jensen, J.E., 1972. Radiographic criteria for the assessment of healing after endodontic surgery. Int. J. Oral Surg. 1, 195–214.
7. Molven, O., Halse, A., Grung, B., 1987. Observer strategy and the radiographic
classification of healing after endodontic surgery. Int. J. Oral Maxillofac. Surg. 16, 432– 439.
8. Kaya S, Yavuz I, Uysal I, Akku Z. Measuring bone density in healing periapical lesions by using cone beam computed tomography: A clinical investigation. Journal of
Endodontics. 2012;38:28-31.
9. Ford TRP. The radiographic detection of periapical lesions in dogs. Oral Surgery, Oral Medicine, Oral Pathology. 1984;57:662-667.
10. Peters CI, Peters OA. Cone beam computed tomography and other imaging techniques in the determination of periapical healing. Endodontic Topics. 2012;26:57-75.
REVIEW OF LITERATURE
i: Periapical Microsurgery
a: History
Periapical microsurgery is integral to the practice of a modern endodontist (1). A
longitudinal cohort study in Florida showed that 13% of the population has received
endodontic treatment of some form, and that 3% of those procedures were surgical in
nature. So while surgical endodontic treatment may seem rare, as less than one half of
one percent of the population has had an apical surgery (2), the total number of
endodontic surgeries per year in the US alone is approximately 300,000, which affects
quite a substantial number of individuals (3). The same survey showed that less than
5% of all surgical endodontic procedures are completed by general dentists, while over
70% of non-surgical endodontic procedures are performed by general dentists. A
survey of practicing endodontists showed that surgical procedures make up 7.2% of all
treatments in the modern endodontic practice (4). As such, surgical procedures are
integral to the practicing endodontist both in establishing a rapport of specialist-level
knowledge and skill, as well as to the financial well-being of a practice.
Surgical endodontic procedures are first mentioned in the literature at the
beginning of the 20th century. As early as 1903, (5) and also in 1906 (6) a technique was described for surgically removing the “roughened” (resorbed) root end and
surface and filling using burs. This later came to be known as an “apicoectomy,” or
literally the removal of the apex of the root. Schamberg’s detailed description of the
procedure included packing the surgical site with iodoform or carbolated gauze, and
having the patient return for multiple visits until granulation tissue was no longer present
at the site. Only after this was complete did Schamberg advocate obturation (filling) of
the canal. Later, Hartzell advocated complete disinfection and obturation of the canal
prior to surgery (7,8). Hartzell’s techniques were considerably less time-consuming
than prior techniques, and as such were more likely to become widely used among
practitioners at the time. Hartzell claimed a failure rate of less than 7% in cases
completed this way.
At the time, it was already well-known that the apical seal of gutta percha and
eugenol-based sealer was not optimal. As such, within a decade, efforts were made to
replace the apical obturation material with amalgam, in the hopes that the apical seal
could be improved and leakage would decrease. Lucas outlined this retro-preparation
and retro-fill using amalgam in a series of articles from 1916-1919 (9,10,11). Following
resection of the root tip, this was completed by using a small round bur to remove the
apical gutta percha and to create retention for the amalgam, then placing, condensing,
and burnishing the amalgam into the preparation. In the same series, Lucas also
described what later came to be known as the “pack and whack” procedure. For
mandibular anterior teeth, he recommended that the teeth be obturated with copper
amalgam prior to surgery. Then during surgery, there was no need for a
retro-preparation and retro-fill, but only the apicoectomy. During the next few decades, there
and outlined repeatedly. For example, the use of a bevel was adopted to allow for
better visualization and easier preparation. While Hartzell had reported success rates in
excess of 90%, reviews in the literature showed the long-term success of these
techniques to be closer to 60% (12). Most practitioners recognized this lower success
rate, inferior to that of non-surgical endodontic retreatment. Combined with the
increased invasiveness, recovery time, and esthetic concerns of apical surgery when
compared to surgical retreatment, apicoectomy was not nearly as common as
non-surgical retreatment. This trend continues today (3) even though the success rate of
modern surgical treatment is considerably higher (12,13), especially in certain scenarios
that will be further explained later (14).
b: Microsurgical Technique
In the 1990’s, significant advances were made that considerably changed the
way endodontic surgery was done (15). The advent of the Dental Operating
Microscope allowed for greater magnification and direct light delivery to the surgical site.
This in turn led to the ability to visualize and access the periapical area without the need
for large flaps or large osteotomies (13). Using the dental operating microscope in
combination with transillumination, even the dentinal defects and microcracks present at
the periapex are able to be visualized (16). This increased ability to illuminate and
magnify the surgical site, combined with the ability to visualize the periapical area and
structures therein, have prompted some authors to state that the use of the dental
operating microscope is a must when performing periapical microsurgery, and all
Ultrasonic handpieces allow for a root end preparation without the use of rotary
handpieces and burs. Traditional rotary instrumentation precludes the instrument from
having bends in the shank, as the entire shank must rotate. Without the necessary
rotation of traditional burs, ultrasonic handpieces are able to be designed in such a
manner so as to fit around the various anatomical impediments, and prepare deep into
the canal without the removal of large amounts of circumferential dentin. In addition,
the manufacturer is able to place a bend near the tip of the ultrasonic instrument, which
allows for the instrument to be used in a smaller osteotomy, and on a flat root-end
surface (18). These techniques, combined with the use of proper direct vision or
micro-mirrors, allow for root-end preparation without the need for a large osteotomy or large
bevel. Smaller bevels decrease the amount of exposed dentinal tubules, which
decreases the chance of leakage into the system (13,19).
Another important aspect of the modern microsurgical technique is the use of a
biocompatible root-end obturation material. In 1990, Dorn and Gartner showed that the
use of IRM or SuperEBA as a root-end filling material resulted in a significant
improvement in 10-year outcomes when compared to amalgam (20). The advent of
Mineral Trioxide Aggregate (MTA) showed extreme promise in histological studies, with
cementum formation on the remaining root surface and even directly on the MTA in the
area of the root-end filling (21,22,23). Today, various materials are used, including
Bioceramics, MTA, SuperEBA, and IRM. Various studies have shown no significant
difference of the long-term clinical outcome between these materials (24,25). However,
histologic studies in animals have shown improved healing after surgery with the use of
number of inflammatory cells present in the periapex of a tooth treated with MTA is
clinically relevant. While one human outcome study did show improved outcome with
the use of MTA over SuperEBA and IRM (28), the choice of retrofilling material was not
randomized, decreasing the level of evidence supported by the study.
In combination, the widespread use of a dental operating microscope, ultrasonic
root-end preparation, and obturation with newer root-end filling materials has greatly
increased the long-term outlook for surgical root canal treatment (15). While traditional
apicoectomy success rates were seen at 45-60%, the modern technique has shown
long-term success rates in excess of 90% (12,13).
c: Indications
While success rates are influenced by myriad factors, primary non-surgical root
canal therapy generally has a long-term overall success rate of approximately 90% (29).
For the other 10% of cases, a decision must be made as to how to treat the tooth to
best eliminate the existing cause of pathology, as well as to prevent apical periodontitis
from recurring in the future. Generally, there are three options for a tooth with apical
periodontitis that has already undergone endodontic therapy: non-surgical retreatment,
surgical endodontic treatment, or extraction of the tooth in question.
While extraction of the offending tooth is a sure way to eliminate apical
periodontitis, replacing the dentition is a difficult and expensive process, with long-term
survival rates similar to those of endodontic treatment (30). The similar survival rate,
combined with the increased expense of implant replacement therapy, make implant
replacement the least cost-effective of the three options when dealing with apical
Non-surgical root canal retreatment is the most common method for dealing with
apical periodontitis in teeth with prior endodontic treatment (3). Statistically, the success
rate of non-surgical retreatment is significantly lower than that of primary root canal
treatment (29), and is lower than that of surgical endodontic treatment (25). Yet
non-surgical retreatment continues to be the modality of choice for revision of previously
treated teeth. This is due to myriad factors, and is often based on subjective decisions
rather than knowledge of the literature and comparable success rates of the
procedures. Typically, the provider faced with the decision to treat surgically or
non-surgically has no knowledge of the treatment details of the original root canal treatment.
While radiographically, the obturation may appear adequate, if improper aseptic
technique was used, bacterial contamination may have been present throughout the
entire procedure. Furthermore, the correct cleaning and sealing of fins, accessory
canals, and isthmuses cannot be assured if knowledge of prior treatment is not
available. Finally, patient preference often comes into play. Non-surgical root canal
retreatment is something patients feel comfortable with, as they have already
undergone non-surgical primary root canal treatment. However, periapical microsurgery
is still a surgery, and many patients prefer to avoid surgery, if possible (32).
With the advances to periapical microsurgery over the past three decades, the
success rates of periapical microsurgery are greatly improved compared to the success
rates of traditional apicoectomy (33,34). In fact, periapical microsurgery success rates
now exceed those of non-surgical retreatment (25), especially in cases where the
natural anatomy of the root canal system has been significantly altered during
periapical microsurgery has a much more predictable outcome. In addition, if a cyst is
suspected, the ability of non-surgical retreatment to resolve the cyst is questionable,
and periapical microsurgery once again has a much more predictable outcome (35).
The use of longer ultrasonic tips allows for deeper root end preparations and fillings,
even up to 9mm, which is generally the length of the entire canal following resection,
rendering the argument of needing non-surgical retreatment initially to cleanse the
canal system a moot point. As such, in these scenarios, and possibly in others, the
prudent clinician may see periapical microsurgery as a preferable alternative to
non-surgical retreatment; both in regards to a predictable outcome, and in long-term cost to
the patient (15,31).
d: Tissue Considerations
A better understanding of the biological processes that guide healing will lead to
a better understanding of the procedure, and ways that it may be further improved. For
both surgical and non-surgical root canal therapy, the goal is healing of the periapical
tissues, including the bone surrounding the root tip. Often, prior to treatment, these
tissues have been severely damaged, with bone replaced by granulation tissue.
Surgical treatment removes the inflamed tissue, but also often removes some of the
healthy bone surrounding the affected area, potentially complicating the natural healing
mechanisms needed to produce a healthy cortical plate and adequate bone volume
(36-39). While studies have shown that healing occurs after surgery, and that the
cortical plate is usually restored, the volumetric healing, especially concerning the
bucco-lingual thickness of bone and the surface contour of the cortical plate, has not
bucco-lingual thickness of bone to a point where the periodontal support is
compromised for the tooth in question, or even the adjacent teeth. It is also unknown if
a change in the contour of the cortical plate occurs which may compromise future
implant placement if needed in the surgical site or adjacent sites. Such knowledge is
paramount when treatment planning surgical cases; especially cases where the
prognosis may be less than favorable.
Following extraction of teeth, ridge preservation by means of bone grafting and
sometimes barrier placement has become commonplace, showing clear benefits in the
literature (40). Grafting is seen as necessary to maintain adequate bone thickness for
future implant placement (40). Yet in the realm of surgical root canal treatment, bone
grafting is not common at all, and the effects on outcome remain unclear (41, 42).
Some give the argument that bone grafting would raise the cost of treatment, making
the procedure less attractive, as it is often regarded as a cost-saving measure when
compared to implant replacement strategies. Yet the cost difference is not extensive,
and surgical therapy would still cost significantly less for the patient, especially in areas
involving a prosthesis with multiple units (31). If surgical root canal therapy is being
performed as a “last resort” to save the tooth, then the necessity of grafting to facilitate
future implant placement should be a prominent concern in the mind of the prudent
clinician. Lin argues that the periapex is very different from the cervical periodontium,
and grafting may not aid in restoring the periodontal ligament or the cementum (42).
However, both PDL and cementum are present in the periodontium, and grafting has
been shown in the periodontal literature to have a high success rate. Lin also states
he concedes that there is a paucity of controlled studies to compare the types or sizes
of lesions, or if there are any factors which would precipitate a need for guided tissue
regeneration (42). In 2013, Song et al established that an apico-marginal defect is one
of these situations, and that there is a significant benefit from using guided tissue
regeneration following apical surgery in these cases (43). In these studies, the
outcome measured was resolution of the periapical radiolucency, not maintenance of
bone volume. It is possible that a discrepancy still exists.
e: Traditional Outcome Measurements/Criteria
The methods and criteria for evaluating outcomes of surgical endodontic therapy
evolved with the procedure. In 1972, Jorgen Rud proposed a system of classifying
periapical healing after endodontic surgery that is still widely in use today (44). The
system looks at the change in the periapical radiolucency at the surgical site over time.
In short, elimination of the periapical radiolucency is classified as “complete healing”; a
persistent periapical radiolucency without symptoms, particularly when lamina dura is
visible around the apex, is classified as “incomplete healing” or scar formation;
“uncertain healing” is the classification for a periapical radiolucency that has decreased
in size, yet still persists; and “unsatisfactory healing” is the term given when no
regeneration of bone or lamina dura has occurred, or when symptoms persist.
Another system to evaluate apical periodontitis is the periapical index (PAI),
developed by Dag Orstavik in 1986. Unlike Rud’s system, the periapical index is not
specific to surgical treatment. But the ordinal scale developed by Orstavik has been
shown to have excellent inter-observer reliability, and has been suggested as the
primarily due to the fact that the subjectivity of diagnosis is reduced by the more
well-defined criteria present in the PAI scale, as well as the ability of evaluators to be blinded
while using the technique (45).
In both of the above systems, healing is assessed using 2-dimensional
radiography. Unfortunately, the surgical site is not 2-dimensional, and traditional
radiography does not give a full understanding of healing at the surgical site. In fact, for
a periapical radiolucency to be visible in 2-dimensional radiography, the cortical plate
must be perforated (46). As such, if there is persistent inflammation around the
periapex, but not extensive enough to perforate the cortical plate, this may persist totally
unknown to the provider. It can also be difficult when using 2-dimensional radiography
to differentiate between overlapping structures, evaluate missed canals that
approximate each other closely, or visualize iatrogenic error in a bucco-lingual
dimension. As such, a new system was proposed to evaluate healing in 3-dimensions
using cone-beam computed tomography (CBCT). In this system, healing of the
resection plane, periapex, and cortical plate is assessed via the different 2-D slices of
the CBCT volume (47).
f: Gap of Knowledge
Using traditional radiography, the 3-dimensional healing pattern of the surgical
site was impossible to visualize in vivo, and thus not completely understood. Even
more recent studies using modern 3-dimensional radiography have only focused on the
elimination of the periapical radiolucency, the regeneration of PDL and lamina dura, and
the reformation of the cortical plate. These signs are an indication of a reduction in
However, to date no studies have focused on the area around the lesion. Little to
nothing is known about the mechanisms or patterns by which the cortical plate heals. It
is possible that even when the cortical plate regenerates, it regenerates with a
significant narrow defect. It is also possible that while the cortical plate regenerates
within the lesion, there is a loss of bucco-lingual thickness around the lesion.
ii: CBCT
a: Development and Implementation of CBCT in the Dental Office
Until recently, 3-dimensional analysis of healing following surgical endodontic
treatment was impossible without surgical re-entry. While 3-dimensional imaging has
been available in medicine since the invention of computed tomography in 1972, the
technology was too expensive to be economically feasible in dentistry. Ironically, the
earliest machines for computed tomography were designed for evaluation of the head
only (49) although the resolutions of the early scanners were far too low for endodontic
applications. The method of acquiring a CT image went through changes over the
subsequent decades. First, fan-beam computed tomography allowed for more efficient
scanning by allowing multiple detectors to operate simultaneously. This is the method
still currently used for medical CT imaging. The advent of cone-beam computed
tomography (CBCT) in 1998 allowed for 3-dimensional imaging of a limited field at a
greatly reduced cost and radiation dose compared to the previously established
fan-beam computed tomography (50).
To give more details, medical CT imaging is accomplished using a fan-shaped
x-ray beam that makes progressive helical rotations around the subject with the radiation
are stacked together to simulate a 3-dimensional object. Using the narrow fan-shaped
beam source, each slice is a separate scan, requiring many rotations around the
subject. Cone-beam CT, on the other hand, acquires images using a round collimated
x-ray source, with the x-rays diverging from the source in a cone-shaped fashion
towards the sensor. By so doing, the need for multiple rotations is eliminated, and the
entire process can be completed with a single rotation of 180 or 360 degrees (51).
Thus, the advantages of CBCT over traditional fan-beam CT imaging are a reduction in
radiation dose, a reduction in time required to record the image, and a reduction in cost.
The disadvantages of CBCT are the decreased ability to analyze soft tissue, and the
increase in scatter radiation (52) and, at times, patient motion.
During the 1990’s, the placement of dental implants for tooth replacement
became much more common, and the demand for 3-dimensional dental imaging in the
dental office grew considerably. The reduced cost of CBCT machines allowed for the
implementation of 3-dimensional radiography in the dental office (49). These CBCT
units soon became popular for their applications in the field of endodontics. The ability
of 3-dimensional radiography to aid in the diagnosis and detection of abnormal
anatomy, internal and external resorption, missed canals (53,54,55), perforations,
separated instruments, transported canals, the extent of periapical radiolucency, and
the proximity of anatomical structures (56), has led the American Association of
Endodontists to issue a position statement to clarify that clinicians should consider a
limited-field CBCT “should be considered the imaging modality of choice for diagnosis in
patients who present with contradictory or nonspecific clinical signs and symptoms
imaging modality of choice for presurgical treatment planning to localize root
apex/apices and to evaluate the proximity to adjacent anatomical structures.” (57)
b: CBCT Use in the Evaluation of Healing after Periapical Microsurgery
Until very recently, there has been a paucity of research involving evaluation of
healing following periapical microsurgery using CBCT. This is likely due to the
established healing indices using 2-dimensional radiography being well established and
in use for decades (44,45). While CBCT has a much higher sensitivity for detecting
periapical radiolucencies compared to periapical radiographs when compared to
histopathological findings as the gold standard (58,59), some providers noted that
CBCT often appears to demonstrate a small periapical radiolucency in teeth that seem
to be otherwise healthy, and even in teeth with vital pulps. More recent research has
shown that while this does occur, these radiolucencies tend to be smaller than 1-2mm in
diameter, and that a radiolucency larger than 2mm in diameter is indeed indicative of
periapical pathology (60). It has been shown that while dental students and residents
may disagree on the presence or absence of periapical radiolucency on CBCT,
experienced clinicians have a much higher inter-observer reliability. While there may
always be error, additional training will help to reduce this error (61).
Recently, a method of evaluating the healing of the periapical radiolucency in
three dimensions was proposed (47). Using multiple indices, this method measures the
healing in two dimensions around the periapex, the surgical entry point, and the cortical
plate. By combining the indices, a general picture of the three-dimensional healing can
be inductively reasoned. The study also showed the inter-observer reliability of CBCT
post-surgery. However, no volumetric analysis of healing was completed in this or other
studies, nor is there currently any method of evaluating the surgical site healing in a
volumetric fashion.
To date, CBCT research on healing following periapical microsurgery has been
focused on patient-focused outcomes, ignoring the possible effects on related structures
and possible future sequelae. The elimination of periapical radiolucency and
reformation of the cortical plate may correlate well with a reduction in symptoms (48),
but they do not show volumetric changes of the bone and supporting structures. The
use of CBCT for this purpose is the most prudent option currently available. Its use and
reliability are established (47); it has been shown to be as accurate as surgical re-entry
and direct visualization in most situations (62), and it is a non-invasive approach (63)
with relatively low radiation risk (64).
c: CBCT as Used in This Study
In this study, all radiographic volumes were made using cone-beam computed
tomography. This method was chosen for the advantages mentioned earlier; mainly
the decrease in radiation, decrease in time required for image acquisition, and a
reduction in cost. With one exception (Participant #06), all volumes were made using
the Kodak 9000 3D® (Carestream Dental, Stuttgart, Germany). The Kodak 9000 3D®
was chosen for its high resolution in limited field imaging, with a relatively low radiation
dose required to produce the image as compared to other models (64,65). The
average CBCT volume to evaluate apical surgery from the Kodak 9000 is equivalent to
approximately 4 bitewings, or regular dental x-rays (64,66). This is the same amount of
radiation as a person receives during a 90-minute plane flight (67). When considering
the low radiation from modern CBCT units with limited field in combination with the
added diagnostic ability they provide, it is scientifically reasonable that studies
recommend CBCT over traditional PA evaluation for post-op evaluation. (63,68).
The volumes for participant #06 were made using the Orthophos XG 3D®
(Sirona, Bensheim, Germany). In this case, the pre-operative volume had been made
using the Orthophos XG 3D®, and in order to achieve proper registration, the
post-operative volume needed to be made on the same machine.
Although the effective radiation dose using the Kodak 9000 3D® is relatively low,
equivalent to only 1-5 days of background radiation (64), all efforts were made to protect
vulnerable populations. As such, participants were excluded from the study if they were
pregnant at the follow-up examination, or if they were undergoing radiation therapy.
iii: 3-D Software
a: ITK-SNAP and Conversion to .STL
As stated before, CBCT machines do not create 3-dimensional models of the
subject they have captured. What they create is a series of 2-dimensional images, or
slices. Specifically, in the case of the Kodak 9000 3D®, a series of 470 2-dimensional
images are created. In order for two volumes to be registered, they must first be
converted into 3-dimensional models.
To accomplish this task in this study, the volumes were exported in
uncompressed DICOM format. The DICOM volumes were then processed using the
software “ITK-SNAP” and the areas of interest converted into .STL files, which are true
was developed specifically for this purpose (69) and has been used for segmentation in
previous publications in the orthodontic literature (70). Segmentation using ITK-SNAP
works by manually selecting a 3-dimensional portion of the volume, setting a grey-level
threshold to eliminate scatter, selecting several points within the selection to guide the
segmentation, and allowing the software to essentially “connect the dots.” By selecting
multiple points, one is assured that the segmentation will not include structures that are
not connected to the main structure being analyzed, such as the opposing arch, or
distant scatter from metal objects. Once the segmentation has been completed, the
object is exported in .STL format, a format commonly used in 3-D modeling and 3-D
printing. (See picture 1, picture 3 in appendix.) While the Kodak 9000 3D® saves
images in 32-bit format, the maximum grayscale ITK-SNAP is able to process is 16-bit.
This was not seen as an issue when creating .STL files, as after segmentation is
complete, the object has essentially 1-bit of depth, meaning the grayscale has been
erased and the object has been completely defined.
b: Geomagic
Once the volumes were converted into .STL format, the software “GeoMagic”
was used to register, or overlay the volumes similarly to subtraction radiography, and
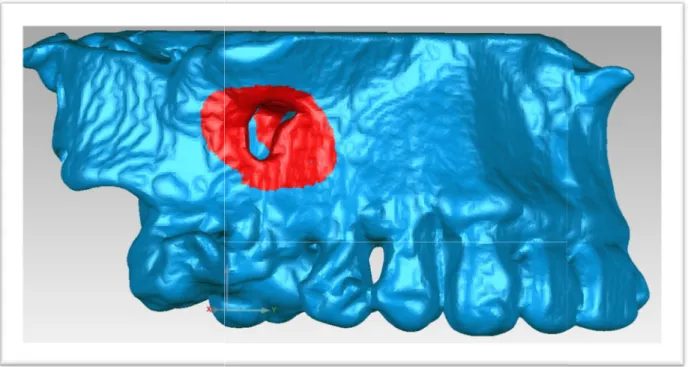
analyze the changes. (See picture 2, picture 4 in appendix.) Once registration was
completed, a color map of the registered images was created to show the changes in
surface contour between pre-operative and post-operative volumes. (See picture 5 in
appendix.) Cross-sectional images were also created to measure the change in
bucco-lingual thickness. (See picture 6 in appendix.) To calculate the volume change in the
the calculations. (See picture 7 in appendix.) While GeoMagic is marketed directly to
the medical field for applications such as this (71), the software is new enough that to
REFERENCES
1. von Arx T. Apical surgery: A review of current techniques and outcome. The Saudi Dental Journal. 2011;23:9-15.
2. Boykin, M. J., Gilbert, G. H., Tilashalski, K. R., & Shelton, B. J. (2003). Incidence of endodontic treatment: A 48-month prospective study. Journal of Endodontics, 29(12), 806-809. doi:10.1097/00004770-200312000-00005
3. American Dental Association, Survey Center, 2005-06 Survey of Dental Services Rendered and Distribution of Dentists in the United States by Region and State, 2005. https://www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/05_sdsr2014 0404t121935.pdf?la=en accessed 2/24/2016
4. Lin, S., Sabbah, W., Sedgley, C., & Whitten, B. (2015). A survey for endodontists in today's economy: Exploring the current state of endodontics as a profession and the relationship between endodontists and their referral base. Journal of Endodontics, 41(3), 325-332. doi:10.1016/j.joen.2014.11.007
5. Moorehead FR. Removal of roughened apex. Dent Cosmos1903;45:163.
6. Schamberg M: The surgical treatment of chronic alveolar abscess. Dent Cosmos 48:15, 1906. Cited in Pathways of the Pulp, 10th edition pg 720.
7. Hartzell TB. Root-tip amputation and external drainage for dental abscesses. Trans Natl Dent Assoc 1908;207–8.
8. Hartzell TB. Root tip amputation. Dominion Dent J 1911;23:473–82.
9. Lucas CD. Root resection and apical canal filling after resection. Dent Summary 1916; 36:201–7.
10. Lucas CD. Indications and technic for root resection. Dent Summary 1918;38:39–42.
11. Lucas CD. Technic of root resection. J Natl Dent Assoc 1919;6:793–800.
12. Setzer, F. C., Shah, S. B., Kohli, M. R., Karabucak, B., & Kim, S. (2010). Outcome of endodontic surgery: A meta-analysis of the Literature—Part 1: Comparison of traditional root-end surgery and endodontic microsurgery. Journal of Endodontics, 36(11), 1757-1765. doi:10.1016/j.joen.2010.08.007
13. Tsesis I, Rosen E, Schwartz-Arad D, Fuss Z. Retrospective evaluation of surgical endodontic treatment: traditional versus modern technique. J Endod 2006;32:412–6.
14. Gorni FGM, Gagliani MM. The Outcome of Endodontic Retreatment: A 2-yr Follow-up. Journal of Endodontics. 2004;30:1-4.
16. Tawil P, Saraiya V, Galicia J, Duggan D. Periapical Microsurgery: The Effect of Root Dentinal Defects on Short- and Long-term Outcome. Journal of Endodontics.
2015;41:22-27.
17. Wu, M.K., Dummer, P.M.H., Wesselink, P.R., 2006. Consequences of and strategies to deal with residual post-treatment root canal infection. Int. Endod. J. 39, 343–356.
18. Gagliani, M., Taschieri, S., Molinari, R., 1998. Ultrasonic root-end preparation: influence of cutting angle on the apical seal. J. Endodont. 24, 726–730.
19. Mehlhaff DS, Harshall JG, Baumgartner JC. Comparison of ultrasonic and high-speed-bur root-end preparations using bilaterally matched teeth. Journal of Endodontics. 1997;23:448-452.
20. Dorn SO, Gartner AH. Retrograde filling materials: A retrospective success-failure study of amalgam, EBA, and IRM. Journal of Endodontics. 1990;16:391-393.
21. von Arx, T., Britain, S., Cochran, D.L., Schenk, R.K., Nummikoski, P.V., Buser, D., 2003. Healing of periapical lesions with complete loss of the buccal bone plate: a histologic study in the canine mandible. Int. J. Periodont. Restor. Dent. 23, 157–167.
22. Baek, S.H., Plenk, H., Kim, S., 2005. Periapical tissue responses and cementum regeneration with amalgam, SuperEBA, and MTA as root-end filling materials. J. Endodont. 31, 444–449.
23. Bernabe´, P.F., Gomes-Filho, J.E., Rocha, W.C., Nery, M.J., Otoboni-Filho, J.A., Dezan-Junior, E., 2007. Histological evaluation of MTA as a root-end filling material. Int. Endod. J. 40, 758–765.
24. Kim S, Song M, Shin S, Kim E. A Randomized Controlled Study of Mineral Trioxide Aggregate and Super Ethoxybenzoic Acid as Root-end Filling Materials in Endodontic Microsurgery: Long-term Outcomes. JOURNAL OF ENDODONTICS. 2016;42:997-1002. 25. Chong BS, Pitt Ford TR, Hudson MB. A prospective clinical study of Mineral Trioxide
Aggregate and IRM when used as root‐end filling materials in endodontic surgery. International Endodontic Journal. 2003;36:520-526.
26. Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of a mineral trioxide aggregate when used as a root-end filling material. J Endod 1993;19:591–5.
27. Torabinejad M, Smith PW, Kettering JD, Pitt Ford TR. Comparative investigation of marginal adaptation of mineral trioxide aggregate and other commonly used rootend filling materials. J Endod 1995;21:295–9.
28. von Arx, T., Ha¨ nni, S., Jensen, S.S., 2007. Clinical and radiographic assessment of various predictors for healing outcome 1 year after periapical surgery. J. Endodont. 33, 123–128
30. Setzer FC, Kim S. Comparison of Long-term Survival of Implants and Endodontically Treated Teeth. Journal of Dental Research. 2014;93:19-26.
31. Kim, S. G., & Solomon, C. (2011). Cost-effectiveness of endodontic molar retreatment compared with fixed partial dentures and single-tooth implant alternatives. Journal of Endodontics, 37(3), 321-325.
32. Friedman S. Considerations and concepts of case selection in the management of post‐treatment endodontic disease (treatment failure). Endodontic Topics. 2002;1:54-78.
33. Hepworth, M.J., Friedman, S., 1997. Treatment outcome of surgical and non-surgical management of endodontic failures. J. Can. Dent. Assoc. 63, 364.
34. Christiansen, R., et al. (2009). "Randomized clinical trial of root-end resection followed by root-end filling with mineral trioxide aggregate or smoothing of the orthograde gutta-percha root filling--1-year follow-up." Int Endod J 42(2): 105-114.
35. Nair PNR. New perspectives on radicular cysts: Do they heal? International Endodontic Journal. 1998;31:155-160.
36. Hirsch, JM, Ahlstrom U, Henrickson PA, et al: Periapical Surgery. Int J Oral Surg 8:173, 1979
37. HARRISON, J., & JUROSKY, K. (1991). wound-healing in the tissues of the periodontium following periradicular surgery .1. the incisional wound. Journal of Endodontics, 17(9), 425-435.
38. Harrison, J. W., & Jurosky, K. A. (1991). Wound healing in the tissues of the periodontium following periradicular surgery. 2. the dissectional wound. Journal of Endodontics, 17(11), 544-552.
39. HARRISON, J., & JUROSKY, K. (1992). wound-healing in the tissues of the
periodontium following periradicular surgery .3. the osseous excisional wound. Journal of Endodontics, 18(2), 76-81.
40. Vignoletti, F., Matesanz, P., Rodrigo, D., Figuero, E., Martin, C., & Sanz, M. (2012). Surgical protocols for ridge preservation after tooth extraction. A systematic review.
Clinical Oral Implants Research, 23(5), 22-38.
41. Taschieri S, Del Fabbro M, Testori T, Weinstein R. Efficacy of Xenogeneic Bone Grafting With Guided Tissue Regeneration in the Management of Bone Defects After Surgical Endodontics. Journal of Oral and Maxillofacial Surgery. 2007;65:1121-1127.
42. Lin, L, Chen, M, Ricucci, D, Rosenberg. Guided Tissue Regeneration in Periapical Surgery. Journal of Endodontics. 2010;36:618-625.
43. Song, M., Kim, S., Shin, S., Kim, H., & Kim, E. (2013). The influence of bone tissue deficiency on the outcome of endodontic microsurgery: A prospective study. Journal of Endodontics, 39(11), 1341-1345.
45. Orstavik D, Ørstavik D, Kerekes K, Kerekes K, Eriksen HM, Eriksen HM. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endodontics & dental traumatology. 1986;2:20-34.
46. Bender IB. Factors influencing the radiographic appearance of bony lesions. Journal of Endodontics. 1982;8:161-170.
47. von Arx, T., Janney, S., Hanni, S., & Bornstein, M. (2016). Evaluation of new cone-beam computed tomographic criteria for radiographic healing evaluation after apical surgery: Assessment of repeatability and reproducibility. Journal of Endodontics, 42(2), 236-242.
48. Andreasen JO, Rud J. Correlation between histology and radiography in the assessment of healing after endodontic surgery. Int’l Journal of Oral Surgery. 1972;1:161-173.
49. Sukovic P. Cone beam computed tomography in craniofacial imaging. Orthodontics & Craniofacial Research. 2003;6:31-36.
50. Mozzo P, Procacci C, Tacconi A, Martini PT, Andreis IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. European radiology. 1998;8(9):1558-64.
51. Scarfe WC, Farman AG, Levin MD, Gane D. Essentials of maxillofacial cone beam computed tomography. The Alpha omegan. 2010;103(2):62-7.
52. Scarfe WC, Farman AG. What is cone-beam CT and how does it work? Dental clinics of North America. 2008;52(4):707-30.
53. Bauman R, Scarfe W, Clark S, Morelli J, Scheetz J, Farman A. Ex vivo detection of mesiobuccal canals in maxillary molars using CBCT at four different isotropic voxel dimensions. International endodontic journal. 2011;44(8):752-8.
54. Blattner TC, George N, Lee CC, Kumar V, Yelton CD. Efficacy of cone-beam computed tomography as a modality to accurately identify the presence of second mesiobuccal canals in maxillary first and second molars: a pilot study. Journal of endodontics. 2010;36(5):867-70.
55. Vizzotto MB, Silveira PF, Arus NA, Montagner F, Gomes BP, da Silveira HE. CBCT for the assessment of second mesiobuccal (MB2) canals in maxillary molar teeth: effect of voxel size and presence of root filling. Int’l endodontic journal. 2013;46(9):870-6.
56. Jacobs R. Dental cone beam CT and its justified use in oral health care. JBR-BTR. 2011;94:254-265.
57. Special Committee to Revise the Joint AAEAPSouoCiE. AAE and AAOMR Joint Position Statement: Use of Cone Beam Computed Tomography in Endodontics 2015 Update. Oral surgery, oral medicine, oral pathology and oral radiology. 2015;120(4):508-12.
59. Paula-Silva F, Wu M, Leonardo MR, Bezerra da Silva L, Wesselink PR. Accuracy of Periapical Radiography and Cone-Beam Computed Tomography Scans in Diagnosing Apical Periodontitis Using Histopathological Findings as a Gold Standard. Journal of Endodontics. 2009;35:1009-1012.
60. Pope O, Sathorn C, Parashos P. A Comparative Investigation of Cone-beam Computed Tomography and Periapical Radiography in the Diagnosis of a Healthy Periapex. JOURNAL OF ENDODONTICS. 2014;40:360-365.
61. Parker JM, Mol A, Rivera EM, Tawil PZ. Cone-beam Computed Tomography Uses in Clinical Endodontics: Observer Variability in Detecting Periapical Lesions. Journal of Endodontics. 2017 Feb 1;43(2):184-7.
62. Grimard BA, Hoidal MJ, Mills MP, Mellonig JT, Nummikoski PV, Mealey BL. Comparison of clinical, periapical radiograph, and cone-beam volume tomography measurement techniques for assessing bone level changes following regenerative periodontal therapy.
Journal of Periodontology. 2009;80:48-55.
63. Peters CI, Peters OA. Cone beam computed tomography and other imaging techniques in the determination of periapical healing. Endodontic Topics. 2012;26:57-75.
64. Ludlow, J. B. (2009). Dosimetry of the kodak 9000 3D small FOV CBCT and panoramic unit. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology, 107(4), e29-e29.
65. Rottke D, Patzelt S, Poxleitner P, Schulze D. Effective dose span of ten different cone beam CT devices. Dentomaxillofacial Radiology. 2013;42:20120417.
66. Li, G. (2013). Patient radiation dose and protection from cone-beam computed tomography. Imaging Science in Dentistry, 43(2), 63-69.Lin L, Chen MY-, Ricucci D, Rosenberg PA. Guided Tissue Regeneration in Periapical Surgery. Journal of Endodontics. 2010;36:618-625.
67. Zanotti-Fregonara, P., & Hindié, E. (2011). Radiation risk from airport x-ray backscatter scanners: Should we fear the microsievert? Radiology, 261(1), 330-331.
68. Low, K.M.T., Dula, K., Bu¨ rgin, W., von Arx, T., 2008. Comparison of periapical
radiography and limited cone-beam tomography in posterior maxillary teeth referred for apical surgery. J. Endodont. 34, 557–562.
69. Yushkevich PA, Piven J, Hazlett HC, et al. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage. 2006;31:1116-1128.
70. Cevidanes LHS, Styner MA, Proffit WR. Image analysis and superimposition of 3-dimensional cone-beam computed tomography models. American Journal of Orthodontics & Dentofacial Orthopedics. 2006;129:611-618.
FORMATTED SECTIONS FOR THE JOURNAL OF ENDODONTICS
i. Introduction
Surgical endodontic treatment is an integral part of the modern endodontic
practice (1,2). Over 300,000 surgical endodontic procedures are completed annually in
the United States alone (3). While apical surgery has been practiced for over 100 years
(4,5,6,7), advances in the 1990’s changed the way the procedure was done (8), giving
rise to the term “periapical microsurgery” (9). These changes include use of the dental
operating microscope (8,10,11), the advent of ultrasonic root-end preparation, the
corresponding decrease in the need for bevel preparation (10,12,13), and the use of
biocompatible root-end fillings, rather than amalgam as used traditionally (14,15,16).
Using these new techniques, the success rate of surgical endodontic therapy went from
45-60% with traditional apicoectomy to over 90% with periapical microsurgery (10,17).
It has been established in the literature that at a histological level the periapical
tissues, cortical plate, and gingiva experience a rapid healing following periapical
microsurgery (20,21,22). As a histological evaluation following surgery is not
appropriate, outcomes following periapical microsurgery are most often measured using
the criteria developed by Jens Rud in 1972 (18) or the periapical index proposed by
Orstavik in 1986 (19). These systems utilize 2-dimensional imaging to analyze the
healing of the periapex. As such, they are limited in their ability to diagnose the
quantify the volumetric changes to hard tissues in and adjacent to the surgical site.
Thus, to date outcome studies have focused on the presence or absence of healing
(9,10,15-19), and the reformation of the cortical plate (23), and not on the volumetric
healing and corresponding site maintenance.
Site maintenance is an important consideration when performing periapical
microsurgery. While guided tissue regeneration has not been shown to improve
outcomes following surgery (24,25) except in certain cases, such as an apico-marginal
defect (26), a lack of adequate site preservation may hinder future implant placement in
the surgical site. It is plausible that it could even affect implant placement in adjacent
sites if osteoclastic activity remodels the cortical plate adjacent to the site while the infill
happens in the osteotomy. While an elimination of the periapical radiolucency on
2-dimensional radiographs corresponds with the reformation of the cortical plate (27), it is
unknown how much the bucco-lingual thickness of the bone at the surgical site is
restored. Even studies using cone-beam computed tomography (CBCT) have focused
on the resolution of the periapical radiolucency (28,29,30) and not on the bucco-lingual
thickness of the bone.
The purpose of this study was to evaluate the 3-dimensional, or volumetric,
healing of the surgical site after at least one year (time being the fourth dimension), with
focus on the bucco-lingual width of the bone and the surface contour of the cortical
plate. One year follow-up has been shown to correlate well with long-term
ii. Materials and Methods a. Recruitment
Participants were identified from a pool of patients who had been treated at the
University of North Carolina – Chapel Hill between the years 2011-2016 and who had a
CBCT made within three months prior to the date of surgery. Patients were contacted
for a follow-up visit regarding their surgery. Upon completion of the routine follow-up
visit, all patients who met the inclusion/exclusion criteria were offered the opportunity to
participate in the study.
Inclusion criteria were as follows:
1. Patient ASA I or ASA II
2. Patient age 18-65 at time of surgery
3. Periapical microsurgery completed 1-6 years prior to date of recall exam
4. CBCT made within 3 months prior to date of surgery
Exclusion criteria were as follows:
1. Patient ASA III or higher
2. Apico-marginal defect present at time of surgery
3. Tooth in question responds positively to percussion or palpation
4. Tooth in question displays isolated probing defect >5mm
5. Patient pregnant
In total, 61 patients were identified for follow-up. Of the 61, 11 patients had the
tooth extracted prior to follow-up, 11 patients were unable to be contacted, and 3
refused the follow-up visit. This left 36 patients who were scheduled for the follow-up
exam. Of the 35 patients, 5 did not show up to their follow-up appointment and were
unable to be rescheduled, 2 did not meet the inclusion criteria, and 16 had their original
CBCT lost following a hard-drive failure. This left a total of 13 participants in the study.
Consent was obtained from those who agreed to participate, and a pregnancy
test was administered to any potential participant where pregnancy was a possibility.
All tests were negative.
b. CBCT Exposure
A limited-field CBCT was made of the surgical site. CBCT allows for accurate
examination of hard-tissue in-vivo without the need for surgery (36,37). It has also been
shown to have a high inter-observer agreement (23). With the exception of one
participant, all CBCT volumes were made using the Kodak 9000 3D® (Carestream
Dental, Stuttgart, Germany). The Kodak 9000 has a high resolution in limited field
imaging with a relatively low radiation dose compared with similar models (38,39). One
participant had CBCT made using the Orthophos XG 3D® (Sirona, Bensheim,
Germany). This unit was chosen as the pre-operative CBCT for the patient had been
made on the unit, and as such the post-operative CBCT needed to be made on the
c. Segmentation and Registration
CBCT does not directly produce a 3-dimensional image. What it creates is a
series of 2-dimensional images, which can be stacked to simulate a 3-dimensional
object (40). This series of images is most often stored in the DICOM format. For
volumetric analysis, the DICOM images must be converted into a true 3-dimensional
object; a process known as segmentation. In this study, segmentation was completed
using the software ITK-SNAP (41), which has been used in the orthodontic literature for
this purpose (42). Following segmentation, the area of interest was stored as a .STL
file, a common file used for 3-D illustration and modeling. (See picture 1, picture 3 in
appendix.)
After segmentation, the pre-operative and post-operative 3-D models were
registered using the software “GeoMagic” (43). (See picture 2, picture 4 in appendix.)
Registration is the process whereby the objects are analyzed, certain reference points
established (in the case of GeoMagic, many reference points,) and the two objects are
overlaid similarly to subtraction radiography so that the changes may be analyzed. The
main difference between registration and subtraction radiography is that with
registration, the changes can be analyzed volumetrically, and not just in two
dimensions.
Using GeoMagic, the registered volumes were analyzed for changes. The
volume change of the buccal bone was quantified using the cortical plate surface as a
iii. Results
Of the 14 subjects, 2 were excluded following segmentation when it was
determined that the volumes could not be registered due to excessive scatter from
implant restorations and screws used during surgical reconstruction. Thus, 12 subjects
were included for data analysis in this study.
Among the twelve participants, 3 (25%) were male and 9 (75%) female. 2
(16.7%) had received bisphosphonate therapy within the two years prior to surgery. 6
participants were 50 or younger, and 6 were older than 50. Median time post-surgery
was 25 months.
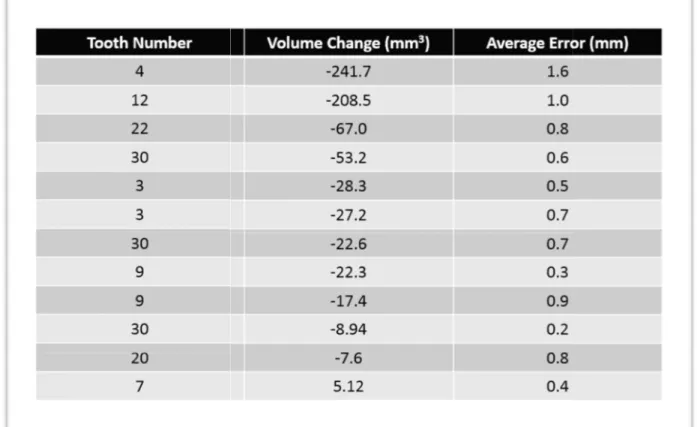
Volumetric analysis showed the median volume change of the buccal cortical
plate to be -24.9mm3 (IQR -8.94 – -67mm3), with an average linear error of 0.7mm
(Table 1, Figure 1). The average linear error is the software’s estimate of how closely
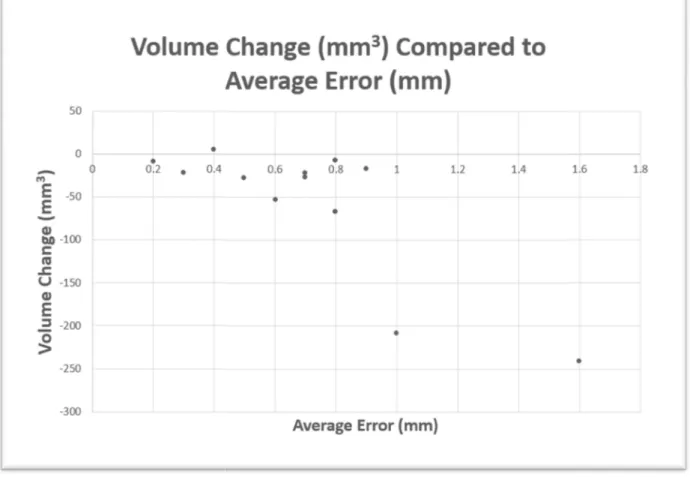
aligned the volumes are following registration. In other words, 24.9mm3 of bone loss occurred in and around the surgical site. Subjects with volume change higher than the
IQR also had greater average error of registration (Figure 2). All linear bucco-lingual
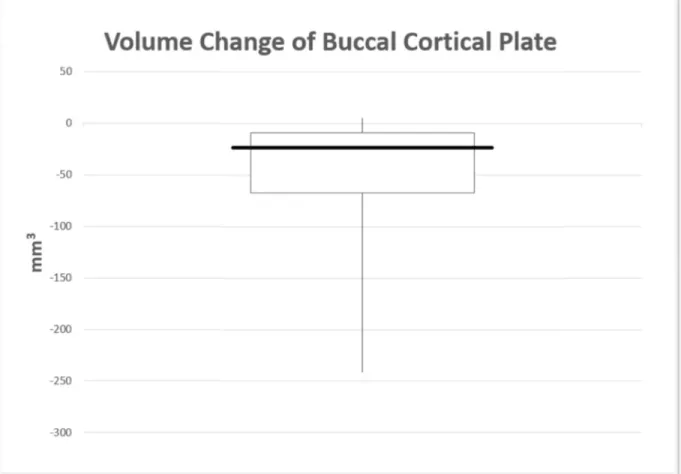
Figure 1: Boxplot of the volume change of the buccal cortical plate. Median volume change -24.9mm3 (IQR
5.12mm3
: Boxplot of the volume change of the buccal cortical plate. Median volume (IQR -8.94mm3 – -67mm3), total range of values
Figure 2: Graphic representation of the volume change in mm
error in mm. The two samples with greatest volume change also had the greatest average error.
iv. Discussion
Although the reported success rate of periapical microsurgery is consistently
90% (10,17), the prudent clinician will concern him/herself with the potential of an
adverse outcome and the reasonable methods known to either avoid that outcome or
prepare for it. While ridge preservation following extraction has shown clear benefi
(44), the potential need for site maintenance following periapical surgery has hitherto
remained unclear (24,45).
representation of the volume change in mm3 compared to the average
The two samples with greatest volume change also had the greatest
Although the reported success rate of periapical microsurgery is consistently
90% (10,17), the prudent clinician will concern him/herself with the potential of an
adverse outcome and the reasonable methods known to either avoid that outcome or
prepare for it. While ridge preservation following extraction has shown clear benefi
(44), the potential need for site maintenance following periapical surgery has hitherto
compared to the average The two samples with greatest volume change also had the greatest
Although the reported success rate of periapical microsurgery is consistently over
90% (10,17), the prudent clinician will concern him/herself with the potential of an
adverse outcome and the reasonable methods known to either avoid that outcome or
prepare for it. While ridge preservation following extraction has shown clear benefits
The results of this study show that there is little to no regression of the buccal
cortical plate (and resultant thinning of the alveolus) following apical surgery. While
25mm3 of bone loss may seem significant if imagined as a cube approximately 3mm in
length, this is an inaccurate view of the results. Total bone regression was measured
over the surgical site, an area of approximately 12mm x 16mm, or almost 200mm2. Seen in
this light, a loss of 25mm3 of bone is equivalent to less than 0.25mm of cortical plate
regression. This theory is confirmed, as we were unable to measure any linear
bucco-lingual change in thickness, as the changes were within the average error of the
registrations.
One limitation of this study is that the software GeoMagic has not been validated
for this purpose on dry skulls. Validation using dry skulls and known volume change
could establish a better understanding of the average error and the ratio of the affect of
average error on volume change calculations. Another limitation is that during the
surgical procedure, the root tip and some of the cortical bone are removed, which
changes the volume of the hard tissue at the surgical site. This problem could be
remedied by taking the CBCT image immediately following surgery. Other limitations
include a small sample size and a lack of controls. Even with these limitations, the
results were consistent, and confirm the results of studies that were symptom-based
mentioned prior.
v. Conclusion
While the use of GeoMagic has not been previously validated in an endodontic
model, it has been used previously in the orthodontic literature (42). And though the
microsurgery, and in the absence of grafting materials or membranes, healing occurs
with little to no regression of the buccal cortical plate and resultant thinning of the
alveolar bone. Future research in this area could involve validation of the software
using dry skulls, or a comparison of .STL quality among different CBCT units. Research
could also be furthered by having a larger patient pool and a more stringent set of
inclusion/exclusion criteria to evaluate only patients without metal restorations in the
area to decrease scatter radiation. However, this would be very difficult, as most
endodontically-treated teeth have received a metal-base or zirconia crown, both of
REFERENCES
1. von Arx T. Apical surgery: A review of current techniques and outcome. The Saudi Dental Journal. 2011;23:9-15.
2. Lin S, Sabbah, W, Sedgley, C, Whitten B. A Survey for Endodontists in Today's Economy: Exploring the Current State of Endodontics as a Profession and the
Relationship between Endodontists and Their Referral Base. Journal of Endodontics. 2015;41:325-332.
3. Suvey Center, American Dental Association [Internet]. Chicago, IL: ADA, c2005-2006. Survey of Dental Services Rendered and Distribution of Dentists in the United States by Region and State; 2005 [cited 2/24/2016]. Available from:
https://www.ada.org/~/media/ADA/Science%20and%20Research/HPI/Files/05_sdsr2014 0404t121935.pdf?la=en
4. Schamberg ML. The surgical treatment of chronic alveolar abscess. Dent Cosmos. 1906;48:15-24.
5. Moorehead FR. Removal of roughened apex. Dent Cosmos. 1903;45:163.
6. Hartzell TB. Root-tip amputation and external drainage for dental abscesses. Trans Natl Dent Assoc 1908; 207–8.
7. Hartzell TB. Root tip amputation. Dominion Dent J 1911; 23:473–82.
8. Kim S, Kratchman S. Modern Endodontic Surgery Concepts and Practice: A Review.
Journal of Endodontics. 2006;32:601-623.
9. Tawil, Peter Z., Saraiya, Veeral M., Galicia, Johnah C., Duggan, Derek J. Periapical Microsurgery: The Effect of Root Dentinal Defects on Short- and Long-term Outcome.
Journal of Endodontics. 2015;41:22-27.
10. Tsesis I, Rosen E, Schwartz-Arad D, Fuss Z. Retrospective Evaluation of Surgical Endodontic Treatment: Traditional versus Modern Technique. Journal of Endodontics. 2006;32:412-416.
11. Wu MK, Dummer PMH, Wesselink PR. Consequences of and strategies to deal with residual post-treatment root canal infection. International Endodontic Journal. 2006;39:343-356.
12. Gagliani, M., Taschieri, S., Molinari, R. Ultrasonic root-end preparation: influence of cutting angle on the apical seal. Journal of Endodontics. 1998;24:726–730.
13. Mehlhaff DS, Harshall JG, Baumgartner JC. Comparison of ultrasonic and high-speed-bur root-end preparations using bilaterally matched teeth. Journal of Endodontics. 1997;23:448-452.
15. Kim S, Song M, Shin S, Kim E. A Randomized Controlled Study of Mineral Trioxide Aggregate and Super Ethoxybenzoic Acid as Root-end Filling Materials in Endodontic Microsurgery: Long-term Outcomes. Journal of Endodontics. 2016;42:997-1002. 16. Chong BS, Pitt Ford TR, Hudson MB. A prospective clinical study of Mineral Trioxide
Aggregate and IRM when used as root‐end filling materials in endodontic surgery.
International Endodontic Journal. 2003;36:520-526.
17. Setzer, FC, Shah, SB, Kohli, MR, Karabucak, B, Kim, S. Outcome of Endodontic Surgery: A Meta-analysis of the Literature—Part 1: Comparison of Traditional Root-end Surgery and Endodontic Microsurgery. Journal of Endodontics. 2010;36:1757-1765.
18. Rud, J., Andreasen, J.O., Möller Jensen, J.E. Radiographic criteria for the assessment of healing after endodontic surgery. Int. J. Oral Surg. 1972;1:195–214.
19. Orstavik D, Ørstavik D, Kerekes K, Kerekes K, Eriksen HM, Eriksen HM. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endodontics & Dental Traumatology. 1986;2:20-34.
20. Harrison J, Jurosky K. Wound-Healing in the Tissues of the Periodontium Following Periradicular Surgery. 1. The Incisional Wound. Journal of Endodontics. 1991;17:425-435..
21. Harrison J, Jurosky K. Wound-Healing in the Tissues of the Periodontium Following Periradicular Surgery. 2. The Dissectional Wound. Journal of Endodontics. 1991;17:544-552..
22. Harrison J, Jurosky K. Wound-Healing in the Tissues of the Periodontium Following Periradicular Surgery. 3. The Osseous Excisional Wound. Journal of Endodontics.
1992;18:76-81.
23. von Arx, T, Janner, S, Hänni, S, Bornstein, M. Evaluation of New Cone-beam Computed Tomographic Criteria for Radiographic Healing Evaluation after Apical Surgery:
Assessment of Repeatability and Reproducibility. Journal of Endodontics. 2016;42:236-242.
24. Taschieri S, Del Fabbro M, Testori T, Weinstein R. Efficacy of Xenogeneic Bone Grafting With Guided Tissue Regeneration in the Management of Bone Defects After Surgical Endodontics. Journal of Oral and Maxillofacial Surgery. 2007;65:1121-1127.
25. Lin S, Sabbah, W, Sedgley, C, Whitten B. A Survey for Endodontists in Today's Economy: Exploring the Current State of Endodontics as a Profession and the
Relationship between Endodontists and Their Referral Base. Journal of Endodontics. 2015;41:325-332.
26. Song, M, Kim, Sahng G, Shin, S, Kim, H, Kim, E. The Influence of Bone Tissue
Deficiency on the Outcome of Endodontic Microsurgery: A Prospective Study. Journal of Endodontics. 2013;39:1341-1345..