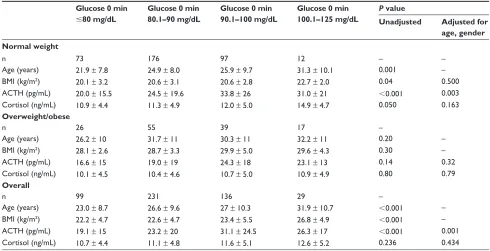
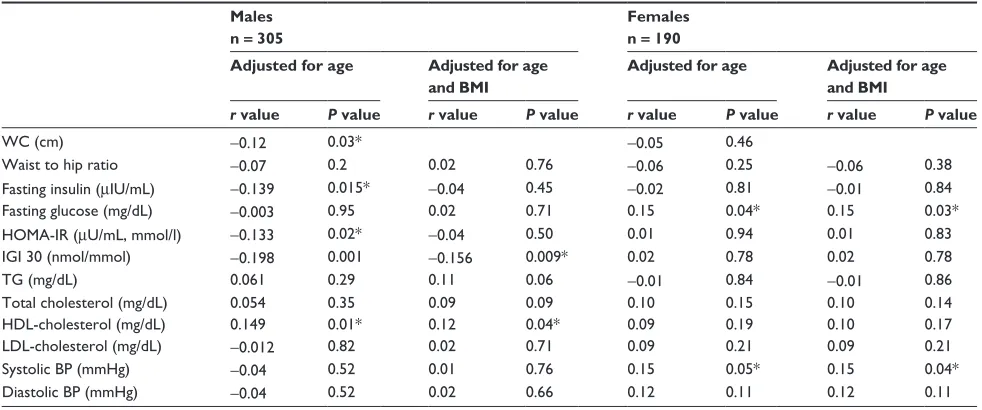
Morning cortisol is lower in obese individuals with normal glucose tolerance
Full text
Figure
Related documents
It has been accepted for inclusion in Scholarly Horizons: University of Minnesota, Morris Undergraduate Journal by an authorized editor of University of Minnesota Morris Digital
The important reasons given by the household respondents for the MDA beneficiaries for not consuming the distributed drugs were either being out of station during MDA
Functional strategies are designed to achieve organizational business strategy and create competitive advantage. In a continuously changing business environment, functional
Prabhakar: A Comparative Study Of Agnikarma By Panchadhatu Shalaka And Lauha Shalaka In The Management Of Heel Pain Due To Calcaneal Spur.. International Ayurvedic medical
Eleven patients did not undergo a muscle biopsy because they were found to have a classical mito- chondrial syndrome and a pathogenic mtDNA mu- tation was found in blood,
10-12 Smaller hospitals in Croatia, as in other countries, must therefore transfer acutely neurotraumatized patients, regardless of how bad their condi- tion might be, to
The study made at Louise Philippe showroom on the topic brand management reveals that from all the varieties of brands of Madura fashion and life style of Aditya Birla
and to children's blood lead (Pb-B) levels and recommended.. the increased use of unleaded
