IJEDR1504112
International Journal of Engineering Development and Research (www.ijedr.org)650
PSMPV: Patient Self-controllable and Multi-level
Privacy-protecting Cooperative Validation in
Distributed m-Healthcare Cloud Computing System
1Nisar Salim Shaikh, 2Raut S. Y.,
1Student , 2Associative Professor Computer Department. 1Computer Engineering Department,
1PREC, Loni, Ahmednagar, India
________________________________________________________________________________________________________
Abstract - Distributed m-healthcare system computing framework fundamentally encourages effective patient treatment for restorative sharing so as to meet individual wellbeing data among human services suppliers. On the other hand, it realizes the test of keeping both the information classification and patients' character protection at the same time. Numerous current access control and mysterious validation plans can't be direct misused. To take care of the issue, in this paper, a novel approved open security model (OSM) is built up. Patients can approve doctors by setting an entrance tree supporting adaptable limit predicates. At that point, in view of it, by formulating another procedure of characteristic based assigned verifier mark, a patient self-controllable multi-level protection safeguarding agreeable confirmation plan (PSMPA) acknowledging three levels of security and security prerequisite in dispersed m-medicinal services distributed computing framework is proposed. The straightforwardly approved doctors, the by implication approved doctors and the unapproved persons in medicinal conference can separately decode the individual wellbeing data and/or check patients' personalities by fulfilling the entrance tree with their own quality sets. At last, the formal security verification and reenactment results show our plan can oppose different sorts of assaults and far outflanks the past ones as far as computational, correspondence and capacity overhead. Distributed m-human services distributed computing framework altogether encourages effective patient treatment for therapeutic interview by sharing individual wellbeing data among social insurance suppliers. In any case, it realizes the test of keeping both the information secrecy and patients' personality security at the same time. Numerous current access control and mysterious validation plans can't be direct misused. To take care of the issue, in this paper, a novel approved open security model (OSM) is built up. Patients can approve doctors by setting an entrance tree supporting adaptable edge predicates. At that point, taking into account it, by concocting another strategy of quality based assigned verifier mark, a patient self-controllable multi-level protection safeguarding agreeable validation plan (PSMPV) acknowledging three levels of security and protection prerequisite in circulated m-social insurance distributed computing framework is proposed. The specifically approved doctors, the in a roundabout way approved doctors and the unapproved persons in therapeutic meeting can separately translate the individual wellbeing data and/or check patients' characters by fulfilling the entrance tree with their own particular trait sets. At last, the formal security evidence and recreation results represent our plan can oppose different sorts of assaults and far beats the past ones regarding computational, correspondence and capacity overhead.
Index Terms— Validation, access control, security and protection, dispersed distributed computing, m-human services framework.
________________________________________________________________________________________________________
I. INTRODUCTION
Distributed m-healthcare system computing frameworks have been progressively embraced overall including the European Commission exercises, the US Health Insurance Portability and Accountability Act (HIPAA) and numerous different governments for proficient and top notch restorative treatment [1], [2], [3]. In m-human services interpersonal organizations, the individual wellbeing data is constantly shared among the patients situated in particular social groups experiencing the same ailment for common backing, and crosswise over appropriated medicinal services suppliers (HPs) furnished with their own cloud servers for therapeutic advisor [28], [29]. On the other hand, it additionally realizes a progression of difficulties, particularly how to guarantee the security and protection of the patients' close to home wellbeing data from different assaults in the remote correspondence channel, for example, listening in and altering [5], [26].
IJEDR1504112
International Journal of Engineering Development and Research (www.ijedr.org)651
just if the patient and the doctor meet in the physical world. As of late, a patient-driven and fine-grained information access control in multi-proprietor settings is built for securing individual wellbeing records in distributed computing [30]. In any case, it chiefly concentrates on the focal distributed computing framework which is not adequate for effectively handling the expanding volume of individual wellbeing data in m-human services distributed computing framework. In addition, it is insufficient for [30] to just ensure the information classification of the persistent's close to home wellbeing data in the legit however inquisitive cloud server model subsequent to the continuous correspondence between a patient and an expert doctor can lead the enemy to infer that the patient is experiencing a particular sickness with a high likelihood. Tragically, the issue of how to secure both the patients' information secrecy and personality protection in the circulated m-medicinal services distributed computing situation under the noxious model was left untouched.
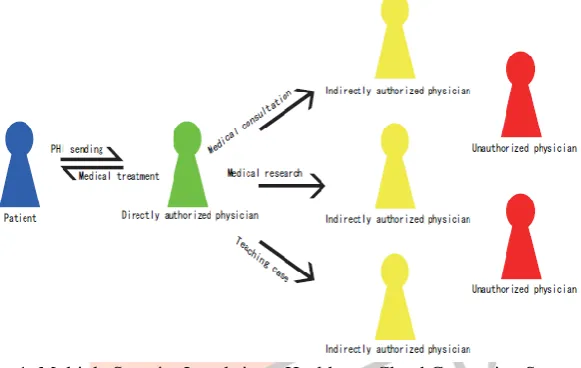
In this paper, we consider at the same time accomplishing information classification and personality security with high effectiveness. As is portrayed in Fig. 1, in appropriated m-human services distributed computing frameworks, every one of the individuals can be ordered into three classifications: the straightforwardly approved doctors with green marks in the nearby medicinal services supplier who are approved by the patients and can both access the tolerant's close to home wellbeing data and check the quiet's character and the in a roundabout way approved doctors with yellow names in the remote social insurance suppliers who are approved by the specifically approved doctors for therapeutic advisor or some examination purposes (i.e., since they are not approved by the patients, we utilize the term 'in a roundabout way approved). They can just get to the individual wellbeing data, however not the persistent personality. For the unapproved persons with red marks, nothing could be gotten. By developing the systems of characteristic based access control [22] and assigned verifier marks (DVS) [21] on de-recognized wellbeing data [27], we understand three distinct levels of security saving necessity specified previously. The fundamental commitments of this paper are outlined as takes after.
Fig. 1: Multiple Security Levels in m-Healthcare Cloud Computing System
1) A novel approved available protection model (OSM) for the multi-level security saving helpful verification is built up to permit the patients to approve relating benefits to various types of doctors situated in circulated human services suppliers by setting an entrance tree supporting adaptable limit predicates.
(2) Based on AAPM, a patient self-controllable multilevel protection safeguarding agreeable validation plan (PSMPV) in the circulated m-human services distributed computing framework is proposed, acknowledging three unique levels of security and protection necessity for the patients.
(3) The formal security evidence and reenactment results demonstrate that our plan far beats the past developments as far as protection safeguarding ability, computational, correspondence and capacity overhead.
Whatever is left of this paper is composed as takes after. We talk about related work in the following segment. In Section II we discussed about literature of medical system. In Section III , the system model of a conveyed m-human services distributed computing framework is outlined. We give some foundation and preliminaries required all through the paper in Section III. At that point, we set up a novel approved available security display.
II LITRATURE REVIWE
IJEDR1504112
International Journal of Engineering Development and Research (www.ijedr.org)652
HIS to pictures and now additionally to information on the sub-atomic level; (7) the enduring increment of new advances to be incorporated, now beginning to incorporate pervasive processing situations and sensor-based innovations for wellbeing observing. Human services are experiencing an outlook change, moving from 'Modern Age Medicine to Information Age Healthcare' (Smith, 1997). This 'outlook change' is forming social insurance frameworks (Haux et.al, 2002) and changing the human services understanding relationship (Ball, 2001). For instance, the World Wide Web has changed the way people in general draw in with wellbeing data (Powell et al., 2003).The presentation of the (PC) amid 1980s to 1990s, which later bolstered by Local Area Network (LAN) has made the utilization of wellbeing data frameworks across the board. . Wellbeing data frameworks suppliers started to reengineer their items and teamed up with different merchants to make it more open. For moment, IBM and Bexter entered joint endeavor, which subsumed the previous Omega and Delta item (Bourke M.K, 1994). Database administration frameworks furnished with inquiry dialects empowered different merchants to get to database. Question dialect intervened interoperability and heterogeneous databases crosswise over sellers.
From the late 1980s, innovation was created so as to make the conveyance of more customized administrations and items at lower costs conceivable. Amid this period, medicinal services associations were moving towards a coordinated consideration. A pattern towards open frameworks and article innovations has as of now been rising amid the '90s, institutional mergers and systems have made new ideas obligatory (Kuhn and Giuse, 2001). In US, the merger of clinics and individual practices into huge coordinated human services systems has been portrayed as an overwhelming pattern (Teich, 1998), while in Europe has been depicted as a decentralized system of social insurance conveyance organizations that gradually replaces healing facilities as focuses of consideration conveyance (Iakovidis , 1998). The pattern towards clinical registering and a patient focused PC based record couldm be seen worldwide in 1980s (Ball, 1999).
TABLE 1. Healthcare Information Systems by Industry Phase at USA (Bourke M.K, 1994)
As anticipated, the doctor's facility data arrangement of prior decades which was for the most part managerial usefulness had turned out to be considerably more centered around the clinical point of view and the patient record, while turning out to be more open in a mechanical and in addition an authoritative sense. It is currently comprehended that information, not frameworks, is the thing that matters (Tuttle, 1999). In addition, the basic issue is individuals – not innovation, and innovation is the empowering agent, not the driver (Ball, 1999).
III PROPOSED SYSTEM Related Work
There exist a progression of developments for approved access control of patients' close to home wellbeing data [8], [9], [10], [11], [15], [16], [18], [19]. As we talked about in the past segment, they essentially consider the issue of information classification in the focal distributed computing structural engineering, while leaving the testing issue of acknowledging distinctive security and protection saving levels as for (w.r.t.) sorts of doctors getting to circulated cloud servers unsolved. Then again, mysterious distinguishing proof plans are rising by abusing nom de plumes other security protecting methods [4], [10], [11], [12], [13], [14], [17], [20], [23], [25]. Lin et. al. proposed SAGE accomplishing the substance arranged protection as well as the logical security against a solid worldwide enemy [12]. Sun et al. proposed an answer for protection and crisis reactions in light of mysterious certification, pseudorandom number generator and confirmation of information [11], [13]. Lu et al. proposed a security saving validation plan in mysterious P2P frameworks in light of Zero-Knowledge Proof [14].
IJEDR1504112
International Journal of Engineering Development and Research (www.ijedr.org)653
namelessness level relies on upon the span of the secrecy set making the unknown validation unfeasible in particular surroundings where the patients are meagerly conveyed.
Fig: 2 A Basic Architecture of E-health system
In this paper, the security and namelessness level of our proposed development is essentially upgraded by partner it to the basic Gap Bilinear Diffie-Hellman (GBDH) issue and the quantity of patients' credits to manage the protection spillage in patient scantily disseminated situations in [6], [7]. All the more fundamentally, without the learning of which doctor in the human services supplier is proficient in treating his ailment, the most ideal route for the patient is to encode his own PHI under a predefined access arrangement instead of dole out every doctor a mystery key. Subsequently, the approved doctors whose trait set fulfills the entrance approach can recuperate the PHI and the entrance control administration additionally turns out to be more proficient. To wrap things up, it is seen that our development basically varies from the trifling mix of property based encryption [22] and assigned verifier mark [21]. As the recreation results show, we all the while accomplish the functionalities of both access control for individual wellbeing data and mysterious verification for patients with altogether less overhead than the paltry blend of the two building pieces above. In this manner, our PSMPA far beats the past plans [21], [30] in proficiently acknowledging access control of patients' close to home wellbeing data and multi-level protection safeguarding helpful confirmation in dispersed m-human services distributed computing frameworks.
System Architecture
The essential e-human services framework delineated in Fig. 2 chiefly comprises of three parts: body region networks (BANs), remote transmission systems and the human services suppliers outfitted with their own particular cloud servers [1], [2]. The understanding's close to home wellbeing data is safely transmitted to the human services supplier for the approved doctors to get to and perform restorative treatment.
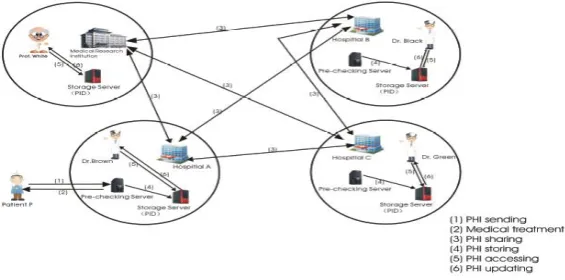
We further show the extraordinary attributes of circulated m-human services distributed computing frameworks where all the individual wellbeing data can be shared among patients experiencing the same sickness for common bolster or among the approved doctors in dispersed social insurance suppliers and restorative examination foundations for medicinal meeting. A run of the mill structural planning of a dispersed m-healthcare distributed computing framework is appeared in Fig. 3. There are three circulated human services suppliers A, B, C and the medicinal exploration foundation D, where Dr. Cocoa, Dr. Dark, Dr. Green and Prof. White are working individually. Each of them has its own cloud server. It is accepted that patient P registers at doctor's facility An, every one of her/his own wellbeing data is put away in healing center A's cloud server, and Dr. Cocoa is one of his specifically approved doctors. For medicinal meeting or other exploration purposes in participation with clinics B,C and restorative examination establishment D, it is required for Dr. Chestnut to create three undefined transcript reenactments of patient P's own wellbeing data and offer them among the disseminated cloud servers of the doctor's facilities B,C and therapeutic examination organization D.
Fig 3: An Architecture Diagram of Distributed m-Healthcare Cloud Computing System
IJEDR1504112
International Journal of Engineering Development and Research (www.ijedr.org)654
In this paper, a novel approved open protection model and a patient self-controllable multi-level protection safeguarding helpful confirmation plan acknowledging three unique levels of security and protection prerequisite in the disseminated m-human services distributed computing framework are proposed, trailed by the formal security evidence and effectiveness assessments which represent our PSMPA can oppose different sorts of pernicious assaults and far beats past plans as far as capacity, computational and correspondence overhead.
V ACKNOWLEDGEMENT
We thank our colleagues from PREC Loni who provided insight and expertise that greatly assisted the research, although they may not agree with all of the interpretations/conclusions of this paper. We would also like to show our gratitude to the Prof.Raut S.Y. for sharing their pearls of wisdom with us during the course of this research. We are also immensely grateful to Prof. Jondhale (H.O.D.) for their comments on an earlier version of the manuscript, although any errors are our own and should not tarnish the reputations of these esteemed persons.
REFERENCES
[1] L. Gatzoulis and I. Iakovidis, “Wearable and portable E-health systems,” IEEE Eng. Med. Biol. Mag., vol. 26, no. 5, pp. 51– 56, Sep.-Oct. 2007.
[2] I. Iakovidis, “Towards personal health record: current situation, obstacles and trends in implementation of electronic healthcare records in europe,” Int. J. Med. Inf., vol. 52, no. 1, pp. 105–115, 1998.
[3] E. Villalba, M. T. Arredondo, S. Guillen, and E. Hoyo-Barbolla, “A new solution for a heart failure monitoring system based on wearable and information technologies in,” in Proc. Int. Workshop Wearable Implantable Body Sens. Netw., Apr. 2006, pp. 150–153.
[4] R. Lu and Z. Cao, “Efficient remote user authentication scheme using smart card,” Comput. Netw., vol. 49, no. 4, pp. 535– 540, 2005.
[5] M. D. N. Huda, N. Sonehara, and S. Yamada, “A privacy management architecture for patient-controlled personal health record system,” J. Eng. Sci. Technol., vol. 4, no. 2, pp. 154–170, 2009.
[6] S. Schechter, T. Parnell, and A. Hartemink, “Anonymous authentication of membership in dynamic groups in,” in Proc. 3rd Int. Conf. Financial Cryptography, 1999, pp. 184–195.
[7] D. Slamanig, C. Stingl, C. Menard, M. Heiligenbrunner, and J. Thierry, “Anonymity and application privacy in context of mobile computing in eHealth,” in Mobile Response, New York, NY, USA: Springer, 2009 pp. 148–157.
[8] J. Zhou and Z. Cao, “TIS: A threshold incentive scheme for secure and reliable data forwarding in vehicular delay tolerant networks,” in Proc. IEEE Global Commun. Conf., 2012, pp. 985–990.
[9] S. Yu, K. Ren, and W. Lou, “FDAC: Toward fine-grained distributed data access control in wireless sensor networks,” in Proc. IEEE Conf. Comput. Commun., 2009, pp. 963–971.
[10] F. W. Dillema and S. Lupetti, “Rendezvous-based access control for medical records in the pre-hospital environment,” in
Proc. 1st ACM SIGMOBILE Int. Workshop Syst. Netw. Support Healthcare
Assisted Living, 2007, pp. 1–6.
[11] J. Sun, Y. Fang, and X. Zhu, “Privacy and emergency response in e-healthcare leveraging wireless body sensor networks,” IEEE Wireless Commun., vol. 17, no. 1, pp. 66–73, Feb. 2010.
[12] X. Lin, R. Lu, X. Shen, Y. Nemoto, and N. Kato, “SAGE: A strong privacy-preserving scheme against global eavesdropping for Ehealth systems,” IEEE J. Sel. Areas Commun., vol. 27, no. 4, pp. 365–378, May 2009.
[13] J. Sun, X. Zhu, C. Zhang, and Y. Fang, “HCPP: Cryptography based secure EHR system for patient privacy and emergency healthcare,” in Proc. 31st Int. Conf. Distrib. Comput. Syst., 2011, pp. 373–382.
[14] L. Lu, J. Han, Y. Liu, L. Hu, J. Huai, L. M. Ni, and J. Ma, “Pseudo trust: Zero-knowledge authentication in anonymous P2Ps,” IEEE Trans. Parallel Distrib. Syst., vol. 19, no. 10, pp. 1325–1337, Oct. 2008.
[15] J. Zhou and M. He, “An improved distributed key management scheme in wireless sensor networks,” in Proc. 9th Int. Workshop Inf. Security Appl., 2008, pp. 305–319.
[16] J. Zhou, Z. Cao, X. Dong, X. Lin, and A. V. Vasilakos, “Securing mhealthcare social networks: challenges, countermeasures and future directions,” IEEE Wireless Commun., vol. 20, no. 4, pp. 12–
21, Aug. 2013.
[17] M. Chase and S. S. Chow, “Improving privacy and security in multi-authority attribute-based encryption,” in Proc. 16th ACM Conf. Comput. Commun. Security, 2009, pp. 121–130.
[18] J. Bethencourt, A. Sahai, and B. Waters, “Ciphertext-policy attribute- based encryption,” in Proc. IEEE Symp. Security Privacy, 2007, pp. 321–334.
[19] N. Cao, Z. Yang, C. Wang, K. Ren, and W. Lou, “Privacy-preserving query over encrypted graph-structured data in cloud computing,” in Proc. 31st Int. Conf. Distrib. Comput. Syst., 2011,
pp. 393–402. [20] F. Cao and Z. Cao, “A secure identity-based multi-proxy signature scheme,” Comput. Electr. Eng., vol. 35, pp. 86–95, 2009.
[21] X. Huang,W. Susilo, Y. Mu, and F. Zhang, “Short designated verifier signature scheme and its identity-based variant,” Int. J. Netw. Security, vol. 6, no. 1, pp. 82–93, Jan. 2008.
[22] V. Goyal, O. Pandey, A. Sahai, and B. Waters, “Attribute-based encryption for fine-grained access control of encrypted data,” in Proc ACM Conf. Comput. Commun. Security, 2006, pp. 89–98.
IJEDR1504112
International Journal of Engineering Development and Research (www.ijedr.org)655
[24] PBC Library, [online] http://crypto.stanford.edu/pbc/times. html, 2006.