A Randomised, Controlled Trial o f a
Pharmaceutical Discharge Service.
Tesneem Ditta.
Submitted in requirement for award o f
M.Phil.
School O f Pharmacy
University o f London
ProQuest Number: 10104222
All rights reserved
INFORMATION TO ALL USERS
The quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
uest.
ProQuest 10104222
Published by ProQuest LLC(2016). Copyright of the Dissertation is held by the Author.
All rights reserved.
This work is protected against unauthorized copying under Title 17, United States Code. Microform Edition © ProQuest LLC.
ProQuest LLC
789 East Eisenhower Parkway P.O. Box 1346
A
b st r a c tObjectives
Identification of drug related problems associated with the traditional system of hospital patient discharge. Development and evaluation of a pharmaceutical discharge service with respect to medication errors, patients’ and doctors’ views, and some associated costs and savings.
Methods
Development of the service was followed by a controlled trial. Seventy patients recruited from medical wards were randomly allocated to intervention (pharmaceutical discharge service with a pharmacist undertaking a supplementary drug history, reissuing appropriate medication, discharge counselling and preparing a typed discharge medicines letter for the GP), or control groups (traditional system of doctor-acquired drug history and doctor handwritten information on discharge medication to GP). Domiciliary visits were undertaken three weeks after discharge and the prevalence and severity o f medication errors and the prevalence of intentional changes to medication by doctors was determined. Patients’ and general practitioners’ opinions’ o f the provision of discharge medicines related information was sought and the costs and savings associated with the service were estimated.
did not alter the mean severity of medication errors (p=0.45, Mann-Whitney test), or the prevalence of intentional changes to medication made by doctors after patients were discharged, which occurred in 24% of intervention and 36% of control patients. Fewer intervention group patients reported problems with medication after discharge (p=0.001, chi square test), or having outstanding questions regarding discharge medication (p=0.01, chi square test). Hospital savings of £97.05 were realised by reissuing 80% of suitable medication.
Conclusion
A
c k n o w l e d g e m e n t s.
I would like to thank Nick Barber for his tireless supervision. I would also like to acknowledge the help that I received from Joan Ashby and the staff at Mount Vernon and Watford hospitals and the Royal Pharmaceutical Society of Great Britain since this thesis was supported by the receipt of a Galen award.
Co n t e n t s
ABSTRACT______________________________________________________2 ACKNOWLEDGEMENTS_________________________________________ 4 CHAPTER ONE. INTRODUCTION________________________________ 11 1.1. CLINICAL PHARMACY DEVELOPMENT IN U K. HOSPITALS 11
1.1.1. Ev o l u t io n Of Clinical Ph a r m a c y In U.K . Ho sp it a l s...12
1.1.2. Ev a l u a t io nofc linicalp h a r m a c yse r v ic es... 13
1.2. THE INTERFACE BETWEEN PRIMARY AND SECONDARY CARE. 18 1.2.1. In tr o d u c t io n... 18
1.2.2. Pa tien t Care Sy st e m... 19
1.2.2.1. Admission and Referral...22
1.2.2.2. Discharge...25
1.2.2.3. Following discharge....28
1.2.3. Co m m u n ica tio n Is s u e s... 33
1.2.3.1. Communication Between Health Care Professionals: Hospital - GP Communication....33
1.2.3.2. Communication Between Health Care Professionals : Hospital Pharmacist - Community Pharmacist...36
1.2.3.3. Communication with Patients...37
1.2.4. Po tentia l Solutions To Pr o b le m s... 4 0 1.2.4.1. Rationalisation O f Prescribing...41
1.2.4.2. System Orientated Measures...41
1.2.4.3 Patient Orientated Measures...48
1.2.4.4. Multiple Intervention Approaches....56
1.2.4.5. Selection OF Pa t ie n t s... 59
1.3 N.H.S. REFORMS AND OTHER OPPORTUNITIES FOR PHARMACY 61 1.3.1 .The Na tio n al Health Se r v ic ea n d Reform su p to 1 9 9 5 ... 61
1.3.4. Ot h er Opportuntiiesf o r Ph a r m a c y In v o l v e m e n ta tthe In te r fa c e...63
CHAPTER TWO. PILOTING THE PHARMACEUTICAL DISCHARGE SERVICE_______________________________________________________ 69 2.1. OBJECTIVES OF PILOT STUDY______________________________ 69 2.2. DEVELOPING THE SERVICE AT MOUNT VERNON HOSPTTAL...69
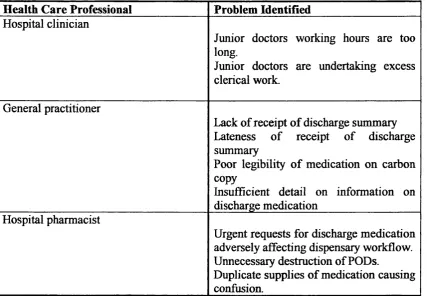
2.2.1. Ba c k g r o u n d... 6 9 2 .2.2. Esta b l ish in g Ne e df o ra Ne w Sy ste m - Pr o b le m sw it h Cu r r e n t Sy s t e m... 71
2.2.3. Dev e l o pin g A Ne w Sy s t e m...74
2 .2.4. No t m c a t io n Of He a l t h Ca r e Pr o fessio n a l s...78
2.3.2.1. Assessment For Drug History Interview...81
2.3.2.2. Drug History Interview...82
2.3.2.3. Checking Patients ’ Own Drugs...83
2.3 .3 . Pharm aceuttcal Disc h a r g ese r v ic epro to co lfo r Disc h a r g e 84 2.3.3.1 Discharge Medication Planning...84
2.3.3.2. Patient Counselling...86
2.4. EVALUATION OF PHARMACEUTICAL DISCHARGE SERVICE ...87
2 .4 .1 . OBJECTIVES... 87
2 .4 .2 . St u d y De sig n...88
2 .4 .3 . Me a s u r e s... 88
2.4.3.1. GP Questionnaire....89
2.4.3.2. Hospital Doctor Questionnaire...89
2.4.3.3. Drug Savings/Reissue Rates...90
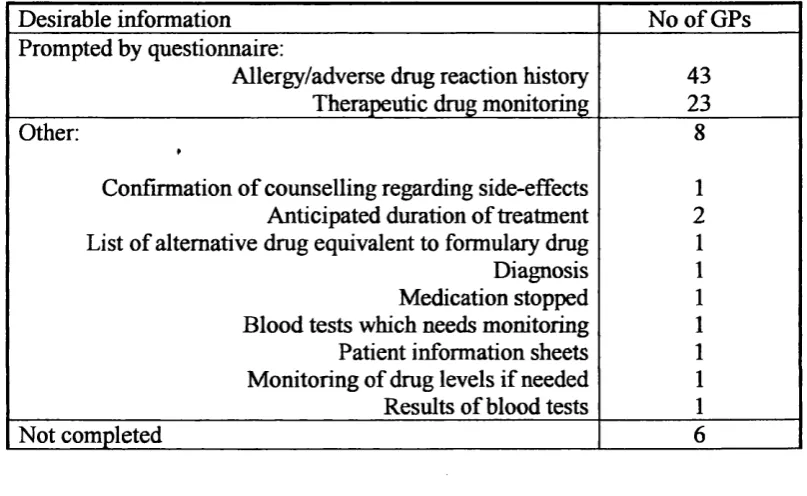
2.5. RESULTS___________________________________________________ 91 2 .5 .1 . GP Qu e st io n n a ir e...91
2 .5 .2 . Ho spita l Docto r Qu e st io n n a ir e...94
2 .5 .3 . Re so u r c e Us e... 96
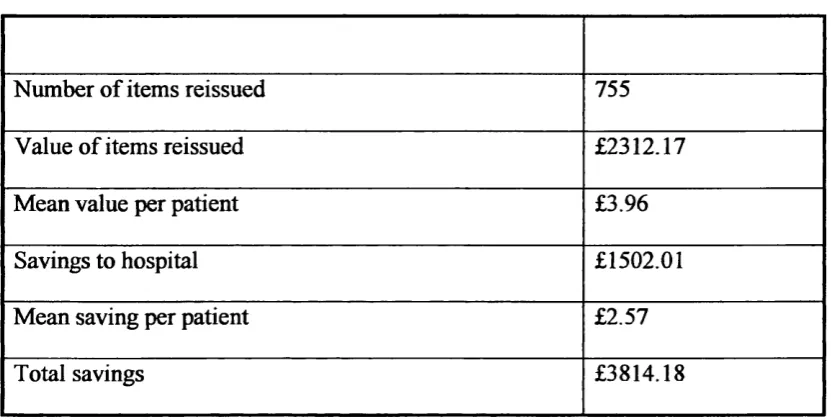
2.5.3.1. Drug Savings...96
2.5.3.2. Reissue ofPODs...97
2.6. DISCUSSION________________________________________________99 CHAPTER THREE. DEVELOPMENT OF METHODS FOR RANDOMISED CONTROL TRIAL_______________________________ 101 1. D^^Ci.^l^GlI^^U^^ D ... 101
3.2. OBJECTIVES______________________________________________102 3 3 . CLARIFICATION OF RESEARCH QUESTIONS________________103 3 .3 .1 . Med ic a t io n Disc r e pa n c ie s... 103
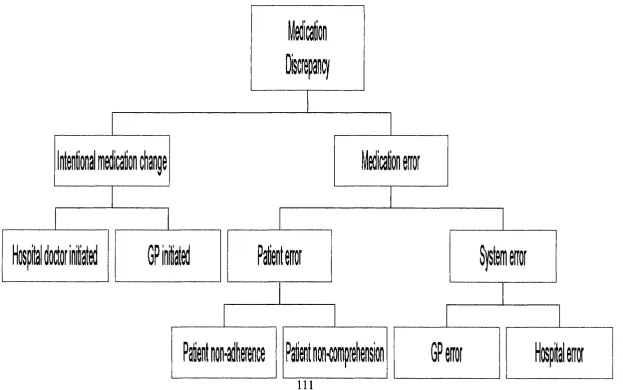
3.4. RESEARCH QUESTIONS AND HYPOTHESES_________________ 112 3 .4 .1 . Me d ic a tio n Disc r e pa n c ies... 112
3 .4 .2 . Asso c ia t e d Co stsa n d Sa v in g s... 116
3 .4 .3 . GP Vie w s... 117
3 .4 .4 . Pa t ie n t s VIEWS... 117
3.5. STUDY DESIGN____________________________________________ 118 3 .5 .1 . St u d y Ra tio n a l e...118
3 .5 .2 . Pa t ie n ta n d Wa r d In c l u s io n Criteria. ... 121
3.5.2.1. Patient Selection Criteria...121
3.5.2.2. Ward Selection Criteria...122
3 .5 .3 . In t e r v e n t io n... 123
3.6. ETHICAL APPROVAL______________________________________ 124 3.7. DEVELOPMENT OF DATA COLLECTION TOOLS_____________126
3.7.1.3. Comments on Study...130
3.7.2. Fir st Pr e-Testof Patien t In ter view Sc h e d u l e...131
3.7.3. Se c o n d Pre-testo f Pa tient In ter view Sc hedu lea n d GP Qu e st io n n a ir e s... 132
3.8. CALCULATION OF SAMPLE SIZE___________________________133 3.9. NOTIFICATION OF HEALTH CARE PROFESSIONALS_________134 3.10. TIMETABLE FOR RECRUITMENT__________________________134 3.11. RCT PROTOCOL._________________________________________ 135 3.11.1. Id en tifica tio na n d Recr uitm entof Pa tien ts... 135
3.11.2. Ob t a in in g Co n se n t... 136
3.11.3. Disc h a r g e...138
3.11.4. Dom iciliary Visit... 138
3.12. ANALYSIS________________________________________________ 140 3.12.1. Me d ic a tio n Disc r e pa n c y An a l y s is... 140
3.12.2. Co st s An a l y s i s... 141
3.12.3. G P s ’ AND Pa t ie n t s’ Vie w s...143
CHAPTER FOUR. RESULTS._____________________ 145 4.1. PATIENT RECRUITMENT___________________________________145 4.1.1 St u d y Popu la tio n... 145
4.1.2. Pa t ie n t s Sa tisfy in g In c l u sio n Criteria...148
4.1.3. Pa t ie n t s Recr uited In t o St u d y... 151
4.2. MEDICATION DISCREPANCIES_____________________________ 152 4.2.1. Pr ev a l e n c eof Med ic a tio n ERr o r s... 152
4.2.2. Ty p e sof Medica tio n Er r o r... 155
4.2.2.1. Patient Errors...155
4.2.2.2 System Errors...156
4.2.3. Descr iptio nof Med ic a tio n Er ro rs... 158
4.2.4. Sev e r it y of Me d ic a tio n Er r o r s... 163
4.2.5. In t e n t io n a l Med ic a tio n Ch a n g e s... 166
4.3. COSTS AND SAVINGS ASSOCIATED WITH THE PHARMACEUTICAL DISCHARGE SERVICE_____________________ 170 4.3.1. Dr u g Co st s...170
4.3.1.1. Medication Changes....170
4.3.1.2. Patient Own Drugs Suitability and Reissue...171
4.3.2. Ph a r m a c y Co s t s...173
4.4. GP SATISFACTION SURVEY.________________________________174 4.4.1. Tim e Ta k e n To Receive Discharge Cor r espo n d en ce... 175
4.4.2. GP Op in io n Of Receipt Of Disc h a rg e In fo r m a tio n... 175
4.4.3. GP Op in io n Of Legibilityof In fo r m a t io n... 177
4 .4.4. G P Opin io no f Com pletenessof Disc h a r g e Su m m a r y...178
4.5.2. Pa tien t Useof Me d ic a t io na n d In fo r m a t io n Re c e iv e do n
Disc h a r g e... 184
4.5.2.1. Primary Respondent...184 4.5.2.2. Medication Taking Habits and Reminders...186 4.5.2.3. Patient Recall o f Receipt ofDischarge Medication and Verbal Information...186 4.5.2.4. Patient Recall and Utilisation o f Written Information...188
4.5 .3 . PATENT Id en tified Pr o blem s With Medicin es Sin c e Discharg e ... 189 4.5 .4 . Pa t e n t Id en tified Un a n s w e r e d Qu e s t o n s On Disc h a r g e
Med ic in e s... 192 4 .5 .5 . Co n t a c t With Ho spit a l Afte r Disc h a r g e... 192
4 .5 .6 . Co n t a c tw ith GP Su r g e r y Af t e rDi s c h a r œ... 195
4#6# * #*##***#*#*#*******#######*##**#*****#**##**#***#*#**#**#*#«*******#*#**####*#*#*###*##«#*#****# 199 CHAPTER FIVE. DISCUSSION _______________________________ 200 5.1. BENEFITS OF A PHARMACEUTICAL DISCHARGE SERVICE. «200 5.2. LIMITATIONS OF RESEARCH AND GENERALISEABILITY..„...,203 5 J . DRAWBACKS OF SCHEME__________________________________206 5.4. DEVELOPMENT OF THE SERVICE_________________________.208
5.5« FURX'HUR RESEARCH^» ««215
CHAPTER SIX. REFERENCES___________________________________ 220 CHAPTER SEVEN. APPENDICES________________________________ 242
Ap p e n d ix 1. Discharcæ Medicin es Letter. ... 2 4 2 Ap p e n d ix 2. Or d e r Fo r mf o r Discharg e Dr u g s... 243 Ap p e n d ix 3. Pa t e n t Dr u g Su m m a r y... 2 4 4 Ap pe n d ix 4. GP Qu e s t o n n a ir e (Mo u n t Ve r n o n Ho spit a l) ... 2 4 6 Ap p e n d ix 5. Ho s p h a l Do c t o r Qu e s t o n n a ir e (Mo u n t Ve r n o n Hospital)
...2 4 7
Ap p e n d ix 6: Pa t e n t Re m in d e r Ch a r t (d o u b l esid e d, f o l d sin toleaflet) ... 2 4 9
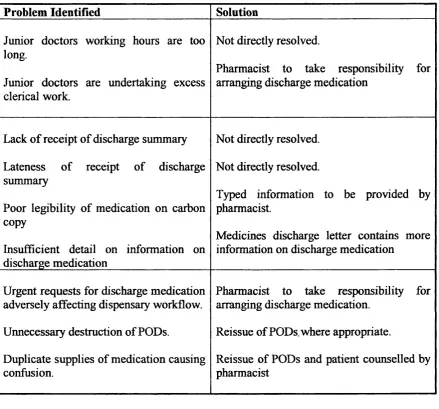
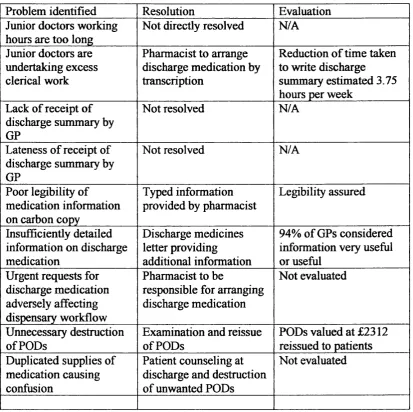
Ta b l e 2. Su m m a r yofsolutionsimplementedtor eso lveproblem s w rra
EXISTING DISCHARGE SYSTEM RELATING TO MEDICATION... 79
Ta b l e 3. GP o pin io nofu se fu l n e ssofph a r m a c ym e d ic a t io nletter. ... 92
Ta b l e 4. Ot h e rin fo r m a tio nc o n sider edd esir a bl eb y G Ps... 92
Ta b l e 5. GP o pin io noftim elinessofreceiptofd isc h a r g e su m m a r y... 92
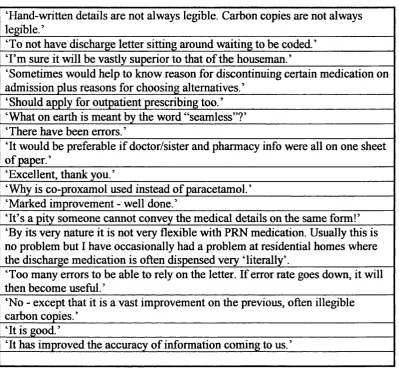
Ta b l e 6. Ad d it io n a l GP c o m m en ts... 93
Ta b l e 7. Va l u e o fr eissu e dpa t ie n t s’ o w nd r u g s’ a n dh o spita lsa v in g s o n DRUG PROCUREMENT COSTS...98
Ta b l e 8. Medica tio nc h a n g esm a d einho spital... 98
Ta b l e 9. Su m m a r yofpilotst u d y; problem sw ithe x k t t n g d is c h a r œsystem RELATING TO MEDICAHON, SOLUHONS THAT WERE IMPLEMENTED AND EVALUATED...100
Ta b l e 10. Su m m a r yofr e a s o n sf o rpatien tsn o tf u l fil lin ge n t r ycriteria. ... 147
Ta b l e 11. Su m m a r yofr e a s o n sf o rn o n-r ec r u itm en to fsu it a b l epa tie n ts. ... 149
Ta b l e 12. Su m m a r yofr e a so n sfo rn o tu n d e r t a k in gh o m ev isit... 149
Ta b l e 13. B N F Ca teg o r yof Dr ug sa sso c ia tedwtthm e d ic a tio ner r o r s. 159 Ta b l e 14. B N F c l a sso fd r u gc h a ng esin tiia tedin t e n t io n a l l y...169
Ta b l e 15. Su m m a r yofa d m issio nd r u g s...172
Ta b l e 16. Su m m a r yofm edica tio nc h ang esm a d ei nh o sp it a l...172
Ta b l e 17. Su m m a r yo fsu itabilitya n dr eissu eofp a t ie n to w nd r u g s 172 Ta b l e 18. Tim etor ec eived isc h a r g es u m m a r y (Pa tien ta n dw a r dg r o u ps) ...176
Ta b l e 19. GP Sa tisfa ctio nw ith Tim elinesso f Receipt (patie n ta n dw a r d g r o u ps) ...176
Ta b l e 20. G P Op in io no n Co m pletenessof Disc h a r g e Su m m a r y...180
Ta b l e 21. Sa tisfa c t io nw ith Vector (patientg r o u p) ...180
Ta b l e 22. Sa tisfa c t io nwtthv ec to r (w a r dg r o u p) ... 180
Ta b l e 23. Ad d it io n a lc o m m entsm a d eb y GPs... 182
Ta b l e 24. Dem o g ra ph icd et a ilsofst u d ypa t ie n ts...185
Ta b l e 25. Med ica tio n Ta k in g Habtts... 185
Ta b l e 26. Pa tien t Reca ll ofw h ich Health Car e Pr o fessio n a l g a v ethem DISCHARGE Me d ic a tio n... 187
Ta b l e 27. Pa t ie n tr ec allofb e in gc o u n selle do nm e d ic a t io nprio rto d is c h a r g e... 187
Ta b l e 28. Pe r s o ntow h o min fo r m atio nsh o w n...190
Ta b l e 29. Pa t ien tid entifiedpr o blem sw ithm e d ic a tio nsin c ed isc h a r g e. ... 190
Ta b l e 30. Pa t ien t Id en t ifie dq u estio n so nd isc h a r g em e d ic a t io n... 193
Ta bl e 31. Ho spit a l Co n t a c t Follo w ing Disc h a r g e... 196
Ta b l e 32. GP Co n t a c t Fo llo w in g Disc h a rg e... 197
Ta b l e 33. Re a s o n s Ctted By Pa tien ts Fo r Co n t a c t in g GP Su r o s r y... 198
Fig u r e 1. Pa t ie n t Care Sy s t e m: Ou tpa tien t Mo d e l... 20
Fig u r e 2. Pa t ie n t Ca r e Sy s t e m : In pa t ie n t Mo d e l...21
Fig ure 4. Fl o w c h a r tto sh o wm edica tio nd isc r e pa n c yc l a ssm c a t t o n
SYSTEM...I l l Fig ur e 5. St u d y De s ig n... 120 Fig u r e 6; Pa t ie n t Rec r u itm en t Ch a r t... 146 Fig ur e 7. Fl o w c h a r tsh o w in gthepr ev alenc ea n d t y peo fm ed ic a tio n
ERRORS i nin t er v e n tio n (I) AND CONTROL C GROUPS OF PATENTS
(SIGNIFICANCE LEVEL P = 0.05)... 154 Fig ur e 8. Me a n Sev er ity Score. Controlg r o u p... 164 Fig u r e 9. Me a n se v er itysc o r e. Inter ventio ng r o u p... 165 Fig ur e 10. Flo w c h a r to fthein tentionalc h a n g e st om e d ic a t io nb y
C
h a pt e rO
n e. I
n t r o d u c t io n.
This thesis describes the development and evaluation of a clinical pharmacist led service of communication of medication related information between primary and secondary care in a U.K. hospital
This chapter describes clinical pharmacy development in United Kingdom hospitals and studies evaluating a common clinical pharmacy service, that of prescription monitoring, are appraised. The primary/secondary healthcare interface is examined in detail to identify problems pertinent to pharmacists and relevant studies are critically discussed. Finally, the current climate within the health service in the U.K. provides a number o f opportunities for pharmacists to develop their role in primary/secondary interface care and these are presented.
1.1. Clinical Pharmacy Development in U.K. Hospitals.
Clinical pharmacy services are provided by many U.K. NHS hospital pharmacy departments. This section summarises the development of clinical pharmacy in the U.K. over the last thirty years and describes some of the services currently provided. Increasingly, evidence of the effectiveness and efficiency of health care services is demanded, and the evidence supporting one clinical pharmacy activity will be examined to determine how and to what extent the service has been evaluated for effectiveness and efficiency.
L L L Evolution Of Clinical Pharmacy In U.K. Hospitals.
Inadequate drug control systems were reported in the late 1960s to cause medication errors and the use of prescription forms that were kept with the patient were advocated It is generally believed that clinical pharmacy evolved when these serious deficiencies in medication prescribing and administration in U.K. hospitals were identified.
responsibility for dosage calculations, and having a contribution to make in the interpretation of assays for drugs in body fluids.
The recommendations of the Nuffield enquiry were taken into account by the Department of Health circular HC(88)54 Many regions in the U.K. formulated service specifications. The Royal Pharmaceutical Society of Great Britain statement of principles for hospital pharmacy includes that ‘pharmacists are professionally, ethically and legally responsible directly to the patient for the quality of care they provide. The pharmacist has a duty of care to the patient to ensure that the medicines they receive are safe, effective and represent an effective use of scarce NHS resources’
L l,2, Evaluation of clinical pharmacy services
Clinical pharmacy has developed extensively in U.K. NHS hospitals. Although standards are set by health authorities, professional bodies and academic organisations on clinical pharmacy practice, the range of services provided may vary considerably between hospitals. Currently, activities undertaken by clinical pharmacists fall into two categories, namely ward based activities and policy level activities. The former includes those services that are offered to patients such as prescription monitoring and counselling, and to doctors, nurses and other health professionals in the form of formal and informal education and training. The latter includes formulary management, clinical trials co-ordination and the provision of financial and prescribing data to clinicians and managers.
A comprehensive survey of clinical pharmacy provided by U.K. NHS hospitals, published in 1994, sampled all U.K. districts and sent questionnaires to all hospital pharmacies that provided comprehensive services i.e. beyond drug supply The authors reported that the most commonly provided service was drug therapy monitoring for acute and long-stay patients, provided by 97% and 93% of respondent hospital pharmacies. Other common services provided included clinical trials support (92%) and formulary management (89%). Pharmacists were also involved in specialist services such as therapeutic drug monitoring, nutrition and pain control. Since prescription monitoring has been reported as being the most frequently provided service, relevant studies will be appraised.
Many studies aiming to evaluate in-patient prescription monitoring have included some measurement of the process such as intervention monitoring, and a few have considered economic factors and acceptability of the service
Intervention recording is undertaken for staff education, medico-legal purposes, to analyse workload and justify staff levels and to measure the contribution of the pharmacist to patient care and cost savings.
of cases as a result. Other surveys have determined time spent on prescription monitoring
Intervention rates and the amount of time pharmacists spend monitoring prescription do not give an indication of the clinical impact o f the intervention. Evaluation of interventions can be undertaken in terms of determining the perceived benefit of the intervention or the perceived reduction in harm to the patient. Another method for describing the need for prescription monitoring focuses on prescription irregularities The first U.K. study evaluating the effectiveness of prescription monitoring was undertaken in 1981 A ward pharmacy service was introduced at a single hospital and a sample of prescriptions before and after the service were reviewed for prescribing errors, which were defined as incompleteness, incorrectness or ambiguity of a prescription item. The authors reported a 46% reduction in the number of errors per patient and a 43% reduction in the number of errors per prescription. Errors were not graded for severity although the authors judged that errors were rarely dangerous but could cause confusion for nurses, and limitations of the study include lack of generaliseability and potential bias. Some studies, attempting to reduce bias, have objectively graded the significance of interventions using non-participant external examiners. In one study investigating the significance of interventions made by pharmacists and technicians, on the wards and in the dispensary of a single hospital over five months, a consultant physician’s opinion was sought on a random number of interventions, although all interventions were recorded by technicians and pharmacists. Of the 1585 interventions, 0.5% were considered to be life-saving, 3.7% to prevent toxicity, and 25% optimised patient care and
improved the standards o f practice Eadon evaluated the quality of interventions made at a cardiothoracic hospital A six point system was used to determine the potential significance of interventions. All interventions were scored by a senior clinical pharmacist with three doctors scoring a random sample of interventions. There was no difference between pharmacist and doctor scores. Using this system, 53% of interventions were reported to lead to an improvement in patient care and 2% prevented major organ failure or significant adverse reaction. Interventions made by 35 pharmacists at six hospitals over twenty eight days were evaluated by an independent assessor (doctor) Interventions were made on 2.9% of all prescriptions and 8% of interventions were judged to have potential for major harm to the patient. The authors did not investigate the costs of providing the service but noted that interventions took an average of 41 minutes per pharmacist per week. The largest study surveyed 210 pharmacists in 311 hospitals over 7 days Of 2706 prescriptions that were questionable, pharmacists intervened on 2095 occasions and their advice was accepted in 96% of instances.
interventions were associated with potential cost avoidance where costs avoidance included reduction in drug costs, savings in drug therapy monitoring, savings attributable to complications associated with drug therapy, and savings relative to a reduction in length of stay, but did not provide financial values. However, interventions were found to rarely save money when based on drug costs alone
Retrospective prescription monitoring may be regarded as a policing role and it is important that doctors and nurses do not perceive pharmacists negatively as a result. A study into junior doctors acceptance of clinical pharmacists found that all doctors questioned rated prescription monitoring by pharmacists as being quite or very useful Doctors also seemed to desire increased contact with pharmacists. Consultants responded favourably to clinical pharmacists in another study, but consultants who did not have a pharmacist on their ward round responded less favourably than those consultants who had a pharmacist on the ward round When surveyed, nurses have had favourable opinions of pharmacists on wards
( 12,13)
Hospital pharmacists have developed services in clinical areas where there is a need for pharmaceutical support. Using prescription monitoring as an example, studies have investigated the process, acceptability and economic considerations. The next section identifies a need for pharmaceutical input at the interface between primary and secondary health care, and how pharmacists have responded.
1.2. The Interface Between Primary And Secondary Care.
1.2A. Introduction.
An increasingly recognised aspect of healthcare services related to the movement of patients between different healthcare environments. The most common example is patient transfer between primary care (community) and secondary care (hospitals). However, movement within the community such as respite care and intermediate care, and also within hospitals as in transfer o f patients from a district general to a specialist hospital are also acknowledged. This thesis specifically explores the primary/secondary healthcare interface.
The importance of close links between primary and secondary healthcare providers is now widely recognised when prescribing drug therapies. Furthermore, adequate information must be communicated to the patient in order to help them to take their medication appropriately. Deficiencies within this complex system exist and descriptions have centred on the patient care system which comprises patient admission or referral, inpatient or outpatient care, discharge and follow-up. Problems at each stage of the patient care system will be discussed in depth and communication deficiencies will be explored. Specific measures purporting to resolve interface problems will be appraised.
1,2,2. Patient Care System,
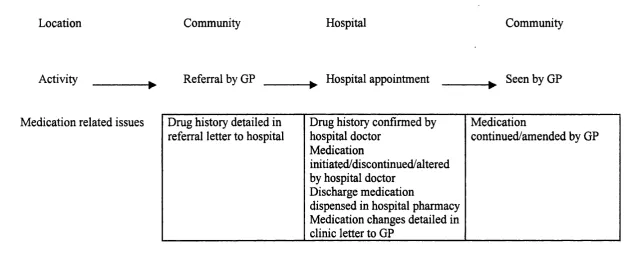
Within most U.K. hospitals, the system for acute health care provision is represented by two models, the inpatient model and the outpatient model (refer to Figures 1 and 2). The outpatient model requires the patient to arrive for consultation with a hospital specialist, usually after referral from their own general practitioner or after discharge from hospital. The consultation commonly takes place within a clinic setting at the hospital and the patient may also interact with clinic nurses, require blood tests or other investigations and be issued with a prescription which may be presented to the hospital pharmacy. The inpatient model is more complex and requires the patient to be admitted onto a hospital ward and occupy a hospital bed. The model consists of an admission stage, which may be preceded by a pre-admission stage, the stay in hospital, discharge and post-discharge. The patient is admitted to the ward as an emergency, via casualty
Figure 1. Patient Care System: Outpatient Model.
Location Community Hospital Community
Activity Referral by GP Hospital appointment Seen by GP
Medication related issues Drug history detailed in referral letter to hospital
Drug history confirmed by hospital doctor
Medication
initiated/discontinued/altered by hospital doctor
Discharge medication
dispensed in hospital pharmacy Medication changes detailed in clinic letter to GP
Medication
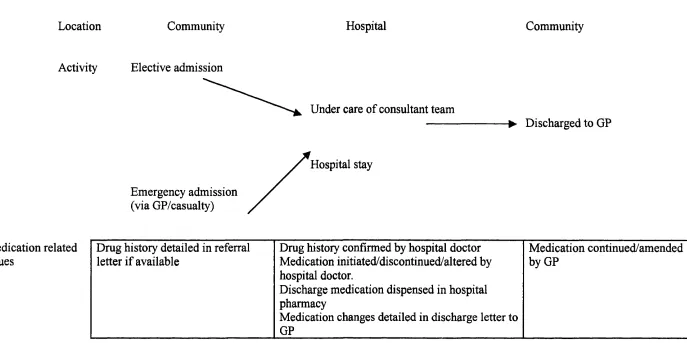
Figure 2. Patient Care System : Inpatient Model.
Location Community
Activity Elective admission
Hospital Community
Emergency admission (via GP/casualty)
Under care of consultant team
Hospital stay
-► Discharged to GP
Medication related issues
Drug history detailed in referral Drug history confirmed by hospital doctor Medication continued/amended
letter if available Medication initiated/discontinued/altered by byGP
hospital doctor.
Discharge medication dispensed in hospital pharmacy
Medication changes detailed in discharge letter to GP
or their own GP, or as an elective admission. Patients may bring some or all of their medication into hospital, and if the GP provides a referral letter, this may document the current drug therapy. On discharge, medication is supplied by the hospital pharmacy upon receipt of a prescription completed by the hospital doctor. The prescription is often an integral part of a discharge summary which includes diagnosis, treatment and further management and is generally completed by hand by a doctor and sent to the GP. In some hospitals, a formal dictated and typed discharge letter is sent to the GP after the patient has been discharged Post- discharge care is generally undertaken by the GP who will continue or amend drug therapy, but the patient may also have to return to hospital for finther investigations or to the outpatient clinic which may result in further modification of drug therapy.
1 .2 .2 1 . Adm ission and Referral
However, hospital clinician acquired drug histories may be inadequate and incomplete and this can be attributed to a number of causes:
• least experienced doctor undertakes drug history,
• lack of familiarity of medication and common dosages by junior doctors, • poor recall of current medication by patients,
• transcription o f drug treatment from instructions on drug containers which may not relate to actual medication consumed,
• patient reluctance to admit poor adherence to treatment to doctor,
• overlooking over-the-counter (OTC) medication as being unimportant by patient and/or doctor,
• patient too ill to communicate effectively,
• lack of time to undertake a full history or chase up missing information (oncall).
As many as 34% of drug charts were found to contain mistakes relating to incorrect transcription of the patient’s regular medication Errors included complete omission of drugs as well as incorrect doses. On admission to an Australian hospital, patients were found to be taking a mean of five drug items, and a mean 0.5 drugs per patient were omitted by the admitting physician, with a further 0.3 errors in dose or dose frequency per patient Inadequate drug histories have the potential to exacerbate problems when patients are subsequently discharged.
Amongst one hundred patients admitted to an ophthalmology unit, the GP notification o f drug history differed from the patient’s actual medication in over 50% of instances Out of 76 patients who were taking prescription medication, 35 patients were taking prescription medication that the GP did not report. Furthermore, patients had been referred to an eye hospital and for thirteen out of the seventeen patients with glaucoma the correct treatment was not notified. The GP referral letters were inaccurate in eighteen out of forty one patients attending a cardiac clinic The drug history was omitted in the GP referral letter for 36% of patients attending a gastro-enterology clinic, and drug history acquisition at the clinic was hampered by the fact that only 13% of patients had brought their medication to the clinic However another study found that drug histoiy was ‘present’ in 88% of referral letters to a medical unit, although the completeness of the drug history was not examined
In terms of accuracy and completeness of drug history, researchers have identified, using a pharmacist undertaken formal drug history interview with the patient’s medicines available to be the gold standard, that telephone contact between the hospital doctor and general practitioner revealed the most information on actual medication, followed by GP referral letter and that hospital drug history records was the least accurate record GP records and hospital records differed in 70% and 76% respectively from the record obtained by interviewing medical patient with their medicines at a general medical clinic
errors/omissions/adverse drug reactions and or interactions in the drug therapy prescribed on admission As a result eight patients were suffering from an adverse drug reaction which was not noted since the offending drug was omitted from the record. In another study, 172 errors were reported and assessed by a multidisciplinary team. Omissions of drugs accounted for 46 of the 172 errors, which in the assessment could have caused deterioration in the patient’s condition, and three errors were assessed as potentially life-threatening In one report, an incomplete drug history led to a patient undergoing unnecessary laparotomy, complicated by pneumothorax
1.2.2.2. Discharge
The processes that occur when patients are discharged are prescription writing, dispensing of medication, receipt of medication by patient and provision of medicines related information to patient and primary care provider, usually the GP. In the UK unstructured discharge letters and separate prescription forms for discharge medication have been replaced by structured, standard forms which include the discharge prescription particularly for initial discharge correspondence, which is sent to the GP when the patient is discharged. Occasionally, these are supplemented by a typed, and detailed dictated summary which is sent later. Waiting for discharge medicines from pharmacy has been given as a reason in 22% of patients in whom the discharge was delayed In general, the delay often occurs earlier in discharge prescription writing process.
Medication is supplied to patients leaving hospital to ensure continuity of treatment. The supply should be sufficient to cover the patient’s needs until they receive a further supply fi'om their GP. Discharge medication is generally prescribed by a doctor, but the proportion of patients receiving a discharge prescription may vary. An investigation into the proportion of discharged surgical patients receiving discharge medications revealed that 30 out of 56 patients were given discharge prescriptions The authors found that the decision as to whether a discharge prescription was required was determined by nursing staff questioning the patient. The high proportion of surgical patients discharged without a prescription may be explained by the likelihood that there may be fewer changes to existing medication in surgical patients compared to medical patients since drugs are the main medical intervention whereas surgery is the primary surgical intervention.
In one study, of 408 patients supplied with discharge medication, only 69% contacted their GP within seven days, and 72% within ten days. There was no contact at one month of discharge in 20% of patients Another study investigated the impact of a change in policy fi'om a fourteen to a seven day supply of discharge medication and a change in format of the discharge letter They found no difference regarding continuity of treatment between a seven and a fourteen day supply.
discharge prescriptions are generally checked against the drug chart by a pharmacist. Delays in patient discharge from hospital are occasionally blamed on delays in the preparation of discharge medication, but this may be due to queries which need to be resolved before the prescription can be dispensed. In Ireland queries occurred in 25% of discharge prescriptions, 88% of which necessitated contact with the prescriber As a result, mean pharmacy processing time rose from eight minutes for a prescription that did not require intervention to twenty five minutes for a prescription where the doctor was contacted. 62% of all errors related to poor prescription writing technique (no strength, no frequency, vague directions, illegible prescriptions and controlled drug errors). Interventions were required before 19% o f discharge prescriptions could be dispensed in a UK hospital 21% of 257 discharge prescriptions dispensed for both acute and long stay medical, elderly care and surgical wards required intervention due to errors or omissions, the most frequent errors were incorrect dose (31%) and omissions (22%)
It has been suggested that discharge prescription monitoring is undertaken by the ward pharmacist instead of by the dispensary pharmacist Wards pharmacists made more interventions than would have been identified by dispensary pharmacists (68 versus 42) and this was attributed in part to their greater knowledge of the patient’s medication plans. Furthermore, a reduction in delay on prescription processing was identified.
Errors in discharge prescription may increase as the total number of drugs prescribed to a patient increases In patients prescribed a mean o f 4.8 (+/- 3.5)
drugs on discharge, there was a mean omission of 1.38 (+/- 2.04) drugs per patient. These omissions were drugs that were prescribed on the inpatient drug chart but not on the discharge prescription and can be regarded as errors in transcription.
1.2.2.3. Following discharge
by other researchers as being either intentional i.e. occurring with professional intent, or unintentional i.e. occurring without professional intent One week after discharge from medical wards an unintentional discrepancy rate of 11% was observed, which rose to 46% six weeks after discharge. The authors concluded that most discrepancies occur in supplies obtained after hospital discharge. In another study almost two thirds of medical patients had changes in medication seven days after hospital, with 34% attributed to an inadequate drug history on admission or counselling on discharge, 43% due to poor communication between hospital and GP, and only 23% of changes having been initiated by the GP Patients had felt that they received adequate information about drug treatment (65%) and had had an opportunity to ask questions about drug treatment (84%). This highlights an anomaly between patients’ satisfaction with information given and problems encountered.
If medical patients experience problems with medicines, then it can be assumed that elderly patients would also have problems. Elderly patients may have other difficulties, especially with memory, manual dexterity and confusion, which combined with a high number of chronic disease states and the likelihood of polypharmacy may exacerbate problems. In one, frequently cited, study, forty five out of fifty elderly patients had deviations in medication within two weeks of discharge Differences in medication were due to cessation of therapy in eleven patients, change in dosage in ten patients an initiation of new drugs in twenty patients. Changes included name of medication from generic to brand, direction for taking, dose and the taking of drugs that had been discontinued by the hospital. Not all changes were made intentionally by the GP. The author
recommended closer links between hospitals and primary care professionals, possibly by a hospital based liaison pharmacist.
To what extent do GPs contribute to medication changes ? In a German study, investigators found that GPs continued 66% of drugs to chronically ill patients on discharge from hospital 21% of drugs were switched to alternative agents (the majority of which were generic switches) and 13% of drugs were discontinued by GPs. In addition, GPs prescribed 18% more drugs than prior to admission. The authors called for greater communication and collaboration between hospitals and GPs not only regarding individual patients but also by establishing joint prescribing committees.
Medication changes occur after discharge, but changes to medication made by general practitioners are generally considered to be acceptable and clinically appropriate. GP initiated changes have been assessed for appropriateness and the authors found that there were changes to medication in 80% of general medical patients within four weeks of hospital discharge. All changes made by GPs were scrutinised and 35% of medication changes made by GPs were considered to have no clinical justification.
medical, elderly and surgical wards respectively). A complexity factor was calculated for each item which considered additional instructions and the number of dose administration times is greater than one. The mean complexity factors were 10,54, 12.57, and 8.58 for elderly, medical and surgical ward patients, indicating more complex discharge prescriptions from medical compared with elderly wards, and less complex discharge prescriptions from surgical compared with elderly wards. The complexity of drugs on admission and medication changes were not considered.
Changes to medication name and dose are not the only relevant differences observed after patient discharge. It has been found that 47% o f medication was inappropriately issued in child resistant containers (CRCs) in elderly patients discharged from a rehabilitation unit, and 28% of prescriptions were inaccurately labelled A new prescription was not issued for 27% of patients and of those issued, new drugs had been initiated in 11% and omitted in 13%. These problems occurred despite an attempt to improve communication to GPs by telephoning the surgery on the day of discharge and posting the discharge summary in addition to giving a copy to the patient to take to their GP.
One problem which becomes apparent after hospital discharge relates to inappropriate duplication of medication. When patients are admitted into hospital, they may be discouraged from bringing in their existing medication. This may result from past experience of confiscation and subsequent destruction of their medication. The extent o f destruction of patients’ own medication is discussed later and it is likely that the patients’ concerns about destruction are well founded.
There are two repercussions when a patient does not bring existing medication into hospital, firstly inadequate recognition of a patient’s current drug regimen by hospital health care workers and secondly, the opportunity for the patient, to continue to medicate with drugs that have been stopped by the hospital once they are discharged home. These points are highlighted in a study where researchers found that eighteen patients were taking forty drugs that had been issued prior to hospital admission, and fifteen patients continued taking twenty six drugs on their own judgement, which included six drugs that had been stopped by the hospital, and twenty that the hospital staff had been unaware of. One example cited was where tiaprofenic acid, which had been stopped in hospital and ranitidine commenced, was restarted by the patient. Comments were made that a five day supply of medication had been made and that five days was insufficient time for GPs to review the prescription and initiate a further supply.
Finally, these problems are not specifically limited to patients moving from one health care environment to another. A study investigated problems experienced by people in the community and found that, o f patients using medication, 52% reported difficulties in using containers, with most difficulties arising from foil covered containers and eyedrop bottles.
1.2.3. Communication Issues.
Communication is a principal factor in promoting effective, seamless provision of pharmaceutical services. Communication issues may be categorised into interaction with health care professionals and interaction between health care professionals and the patient. With regard to inpatients, pharmacy related discharge arrangements in hospitals have been described by two surveys of all hospitals in England in 1995 and 1999*^^^ and of all districts in Wales in 1995 Interim discharge letters are hand written and the discharge prescription may be included or a separate discharge prescription may be written. Inclusion of the discharge prescription is more popular with all types of hospital, namely teaching, general and specialist hospitals.
1.2.31. Communication Between Health Care Professionals: H ospital-GP Communication.
Communication between the hospital and GP occurs on admission and discharge, and problems in communication when patients are admitted or referred to hospital have been described earlier in section 1.2.2.1. This section will focus on communication at the discharge phase. In general the content, format and receipt
Incomplete information provision to GPs may contribute to changes in treatment. With regards to discharge medication, 42% of GPs who had contract with one Kent hospital felt they received too little information and over half felt that this was true of information provided to patients and only 55% of GPs considered that the information was adequate. Inadequacies highlighted included illegible discharge summaries, lack of duration of treatments and lack of information regarding changes in medication. The latter was cited by 88% of GPs. A similar study revealed that 96% of GPs wanted information on medication changes made by hospitals, primarily to facilitate continuity of care. Other reasons cited as to why GPs want information on reasons for changes to treatment are to facilitate patient counselling, to alter or query hospital prescribing and financial considerations. Another study reported a complete absence of information on drugs supplied on discharge in 90% of first communications and second conununications respectively, and under-reporting of drug reactions in hospital The authors did not describe the discharge documentation and it is probable that in this case the discharge prescription was not included in the discharge letter. In a more recent study, discharge treatment was reported in 88% of first and second communications received in one practice and in 78% and 94% of first and second communications received in another practice Medication was not recorded in 18% of discharge correspondence and there were discrepancies in information transmitted via the first and communications where differences occurred in 9 (14%) of communications, with differences in drug name (generic/non-generic), doses and drugs. Data was limited since 62% of second communications were not available for scrutiny. General practitioners have
specified the importance of selected items of information for patients receiving chemotherapy Items considered essential by GPs include details of drugs used (82%), dose of drug (68%), and potential side-effects (41%) and these were covered in 100%, 89% and 5% of discharge letters received. Knowledge of side effects of chemotherapeutic drugs is necessary to ensure appropriate patient monitoring and lack of provision of this data may appear to put the patient at risk.
1.2.3.2. Communication Between Health Care Professionals : Hospital Pharmacist - Community Pharmacist
Few studies have examined the level of communication between hospital and community pharmacists. The available evidence suggests that community pharmacists receive little information when patients are discharged from hospital although to be fair to hospital pharmacists, there is a similar lack of formal communication when patients are admitted to hospital.
care that had worked well The results of these surveys have been confirmed by an observational work sampling study of hospital and community pharmacists which found no contact between hospital and community pharmacists
1.2.3.3. Communication with Patients
Before exploring issues regarding communication with patients at the interface, it is appropriate to first ask why is it necessary to communicate with the patient, who should communicate and also how to communicate effectively and what information to provide.
Why ?
The concept that patients are passive consumers of healthcare with health care professionals acting in a paternalistic manner is outmoded and it is unreasonable to expect people to want to know nothing about their medication. There are a number of valid reasons for providing medicines- related information to patients that apply equally to provision of information on discharge and whenever and wherever medication is prescribed. There is good evidence to support the hypothesis that patient counselling enhances the patient’s ability to take medication by improving their medication knowledge and this will be discussed later. That patients desire more information on their medication is an aspect of patient empowerment. Legislation has also demanded improved patient information. Legal considerations include an obligation on the part of the doctor to give information as patients have the right to receive information on drug
therapy as extolled by the Patient’s Charter. Despite this, it has been argued that physicians and pharmacists maybe reluctant to provide information to patients European legislation recognises a patient’ right to information on medication and since January 1999 there is a legal requirement for all medicines to supplied with a comprehensive information leaflet for patients
Who should be providing information on medication ?
said that elderly patients routinely received medicines related information on discharge, whereas only 4% of patients reported that they had received written information In another study, 95% of nurses believed that patients received discharge medication counselling
How should information be relayed?
Information can be supplied in one of two ways, verbally or printed. Different patient groups have different needs and it also necessary to ‘individualise’ information. Patients may be grouped according to their age or disease state. The problems faced by elderly patients may relate to slower cognitive functioning, reduced short-term memory and impaired visual acuity and manual dexterity. For example, a quarter of elderly patients may be unable to read a standard computer generated medication labels Since elderly patients consume a large proportion on medication (in 1990 43% of prescriptions issued in the U.K. went to elderly patients), research strategies have been adopted to overcome, partly problems faced by the elderly. In addition to having difficulties taking medication, elderly patients may not be able to remember exactly what they ware taking, and one study found that only 10% of patients were able to recall all drugs that they were taking
Counselling has been shown to improve recall of medicines after discharge and errors made with medication after discharge in the elderly Although one early study found no difference in error rates Written information in the form of a computer generated reminder chart improved patients’ knowledge (83% with
chart versus 47% without chart correctly described their medication regimen) and increased compliance which was increased furdierwith verbal counselling
What Happens in Practice ?
Although measures such as counselling and the provision of written information have been advocated, there is evidence that this does not occur in practice. Written information was provided to 14% of outpatients who had received specific drugs Only 32% were informed of side-effects although most patients were told the dose and dosing interval. Patients discharged from medical and surgical wards were shown to have poor knowledge of side-effects or duration of treatment, although most (over 80%) patients were able to read and understand instructions Poor recall of medication was associated with increased age, mental score, and number of drugs prescribed Medicines were correctly described for 75% of drugs prescribed to elderly patients A survey of the reported level of provision of certain services to elderly patients questioned all hospital pharmacies in England and received a 68% response The authors found that 2% of respondent hospitals counselled all elderly patients before discharge, 28% counselled no elderly patients and 27% provided all elderly patients with written information about their medication
1.2,4, Potential Solutions To Problems,
pharmaceutical requirements, including information, can be communicated and maintained in a safe, timely and user-friendly way’ and from the evidence cited earlier it is clear that this does not always occur in practice.
There are three initiatives that can be described which aim to reduce difficulties when patients are moved between primary and secondary care:
1. Rationalisation of prescribing.
2. System orientated measures (improve patient admission/discharge procedures and communication between health care professionals).
3. Patient orientated measures (improve communication between health care professionals and patients).
1.2.4.1. Rationalisation O f Prescribing
Since some medication changes in hospital can be attributed to hospital formulary choices joint prescribing formularies have been proposed. Such formularies may be co-ordinated by an ‘interface pharmacist’ whose responsibilities would include shared care prescribing, interface consensus groups and disease management guidelines. A similar role has been given the title ‘pharmacist facilitator’
1.2.4 2. System Orientated Measures
Improvements in the processes by which patients are admitted to and discharge from hospitals have been achieved by improving and developing communication
pathways and by the use of measures such as dedicated interface roles and protocols.
As discussed earlier, discharge prescription monitoring by ward pharmacists may be beneficial Comparison of drug charts and discharge prescriptions have shown that over half required intervention by a pharmacist In an American study, pharmacist intervention was required in 38% of discharge prescriptions (106) pharmacist screening of discharge prescriptions led to a change of
therapy in 56% of interventions compared with 14% and 17% of interventions made by dispensary pharmacists and clinical pharmacists took less time to resolve problems with an average of 3.5 minutes per prescription for clinical pharmacists and 5.3 minutes per prescription for dispensary staff.
In several hospitals, clinical pharmacists are transcribing the discharge prescription, with the doctor checking and signing the prescription which has improved the efficiency of the discharge process and reduce errors on the discharge prescription
which may due to a perception of the community pharmacist’s relative lack of knowledge of paediatric therapy and of the individual patient’s treatment plans
Circumventing the hospital pharmacy at discharge arguably increase the potential for drug errors. One study assessed discrepancies between the discharge prescription written by the hospital physician, the discharge instruction sheet (DCI) completed by the nurse who also counselled the patient, and the medication dispensed by the community pharmacist, for 388 paediatric patients discharged from an American hospital. In 19% of patients, the discharge prescription, DCI and the dispensed medication were not identical, accounting for 12% of prescriptions. In 5% of initial prescriptions there were omissions or inaccurate information. Hence, providing patients with prescriptions instead of medication may not be advantageous, despite a study where some patients regarded this as their ideal choice due to perceived reduced waiting times, convenience and the possibility of shopping whilst waiting for the prescription to be dispensed. Only 2% of patients commented that prescription queries were more easily resolved in the hospital pharmacy.
Other system improvements are aimed at improving communication between the hospital and the GP and developing communication pathways between the hospital and community pharmacist, but communication between the GP and community pharmacist is also worth consideration.
Communication between hospital and community pharmacists has been proposed as a measure to improve the provision of a seamless approach to pharmaceutical services In 1993, the hospital pharmacists group of the Royal
Pharmaceutical Society produced checklists for hospital admission and discharge, to be completed by community pharmacists to provide information to hospital pharmacists when patients were admitted and vica-versa on discharge Information provided by the community pharmacist included patient demographic data, prescribed and non-prescription medication history and domiciliary circumstances. The hospital pharmacist provided information relating to the patient’s medication plan, whether any existing medication had been stopped or altered and the reasons for such changes, and details of discharge medication. Assessment of the form found that benefits included identification of medicines related problems and subsequent intervention for 25% of elderly patients, o f which 68% were judged to be clinically significant Perceived problems included that the forms were time consuming to complete, there was increased paper workload and there was difficulty in tracking patient transfers. Utilisation of the checklist to solve medication problems may not readily occur When data on 68 Pharmaceutical Society checklists sent from hospital to community pharmacists were analysed, thirty three problems were identified. In twenty five (37%) prescriptions, nine were resolved by contacting the GP and eight were resolved without contacting the GP. It was noted with concern that no intervention was made by community pharmacists in nearly half of the cases where problems were identified including nine cases where drugs were omitted, three cases where there was failure to discontinue drugs, two wrong drugs and two wrong doses. This may indicate a need for training of community pharmacists before the checklists fulfil their full potential. Despite potential advantages, there is evidence that the Pharmaceutical Society checklists are not used extensively in practice
Pharmaceutical Society checklists only 4% responded affirmatively and 72% responded negatively Awareness of the existence of the checklists amongst community pharmacists was poor, at 29% for community and 75% for hospital pharmacists and several potential problems Avith using the form were identified including lack of time. Hospital and community pharmacists did agree on the usefulness of such checklists for specific patient groups such as elderly patients, patients on complex medication regimens and mentally ill patients and the original checklists were designed with vulnerable patient groups in mind. One of the main difficulties of sending patient’s information to the community pharmacist is the potential to limit the patient’s freedom to visit any pharmacy.
Other types of document to enhance the communication of medicines related information, such as typed and written pharmacy information letters have been described. A pharmacy information letter was shown to reduce medication management problems experienced by elderly patients after discharge The letter was completed by a hospital pharmacist and included information on medication changes and drug allergies in addition to listing any problems in opening containers and was given to patients, and sent to the GP, the community pharmacist nominated by the patient and if necessary to the community nurse. Interestingly, the perceived usefulness of the pharmacy information letter differed between health care professionals, with 29%, 79% and 82% of GPs, community pharmacists and community nurses respectively finding the letter useful or very useful. GPs showed a poor positive response to the pharmacy letter, whereas there was a reduction in problems experienced by patients. Perhaps this indicates an unawareness amongst GPs of the problems faced by patients recently discharged
from hospital. In a Canadian study, information was prepared by the hospital pharmacist and forwarded to the GP and community pharmacist The information that was prepared took the form of two summaries, a ‘rationale for inpatient changes’ (RFC) document which detailed medication changes made by hospital personnel and noted the reasons for changes, and a ‘recommendation for future changes’ (RFC) document which included alterations in dose or drug that should be considered for future management. The former document was sent to both GPs and community pharmacists and the latter to GPs only. GP response was mostly positive with an intention to follow the recommendation in 23 out of 27 letters. The two types of summaries were time consuming to prepare, taking an average of 45 minutes for the preparation of the RFC and 91 minutes for the RFC summary.
computer generated discharge prescriptions for surgical patients in the U.S.A. When compared to hand-written discharge drug prescriptions computer generated prescriptions decreased the number of legal and prescribing errors in addition to decreasing dispensary processing times. A study in the USA similarly investigated use of computer generated discharge prescriptions, this time for medical patients (123) computer program was accessed voluntarily by physicians and there was a tendency to use it for older patients. The computer system was regarded as making it easier to order medication by 68% of doctors using the system, and to save time by 41% of doctors. Similar findings were reported in another study
The extension of hospital computer prescribing systems to order discharge medication is reasonable but at the time of the study few hospitals in the U.K. had computerised prescribing. Pharmacists accessing computerised prescribing systems in hospitals increase to order discharge medication was found to increase the efficiency of the discharge process by reducing the proportion of urgent requests and the need for clarification of the discharge prescription Electronic data interchange between GPs and community pharmacists and better IT systems in hospitals are planned, but patient specific electronic communication between primary and secondary health care workers may take longer. The use of fax machines to act as vectors for communication of discharge medication has more potential in the U.K. so that medication summaries prepared by hospital pharmacists can be faxed to GPs and community pharmacists The use of information technologies at the primary/secondary care interface will be discussed further in the discussion in view of recent NHS reforms.
The pharmacist has been promoted as educator, co-ordinator and navigator A dedicated admissions pharmacist uses all of her clinical skills to improve the quality of information regarding medication when patients are admitted into hospital Pharmacists who develop a role in discharge planning have found that they are consulted more about other matters as their ward exposure is increased The title ‘patients’ medicines co-ordinator’ has been given to a pharmacist whose main responsibility is to write discharge prescriptions and counsel patients Benefits have included an estimated reduction of 80 hours per week spent by junior doctors arranging discharge medication and £10,735 saved on the costs of discharge medication to the medical directorate within which the project was undertaken. Discharge co-ordinators are not necessarily pharmacists and comprehensive discharge arrangements require assessment of the patient’s often complex social and nursing needs. A discharge co-ordinator was found to improve the discharge planning service and decrease problems experienced by medical patients after discharge, but did not affect re-admission rates (readmission within seven days of discharge) and the benefits incurred an additional cost
1.2.4.3 Patient Orientated Measures
interventions takes place at all points in the interface, preadmission, admission, discharge and post-discharge. Certain patient groups have been specifically targeted and these include medical, surgical, elderly patients, those with a high number of medication changes and paediatric patients.
1.2.4.3.1 Pre-admission and admission to hospital
Various studies have demonstrated that pharmacists acquire more information on medication than doctors For example, pharmacists documented 31% more items of information that doctors Clarification of drug therapy was necessary in 19% of patients following a pharmacist-undertaken drug history A review of studies reported that pharmacists prepare a more complete drug history than physicians which was due in part to increased documentation of non-prescription medicines This finding has been confirmed by several other studies
Feedback from doctors has been positive, with 76% of junior doctors supporting this role, but a sizeable minority (24%) felt that it was not necessary or practical Further evidence suggests that pharmacists may document more information on drug allergies than physicians
information on drugs than doctors, but does this make a valuable contribution to the overall care of the patient? Several studies have attempted to scrutinise the information obtained by pharmacists in terms of the potential significance
The first study assessing clinical significance of pharmacist acquired drug histories was conducted in Canada and found that 11% of pharmacist acquired information that had been omitted by doctors were deemed clinically important by an expert panel whereas this was estimated to be 70% in another study In the U.K. clinical significance was presumed when 29% of patient interviews necessitated contacting the prescriber and 81% of these resulted in therapy changes
Methods for drug history acquisition have been described Interviewing patients requires the application of sound communication skills such as the ability to control the interview pace, asking questions appropriately and probing answers whilst relating to the patient’s needs Accessing the patient’s notes prior to interviewing patients is useful since relevant background information such as previous medical history can be collated. Some authors advocate a review-of- systems approach to drug history acquisition In general, the following areas have been probed:
• Prescription medication - including name/brand, dose and frequency, indication and date started.
• Non-prescribed medication - including OTC, herbal and homeopathic remedies.