ARTICLE
Managing Attention-Deficit/Hyperactivity Disorder in
Primary Care: A Systematic Analysis of Roles
and Challenges
Thomas J. Power, PhDa,b, Jennifer A. Mautone, PhDa, Patricia H. Manz, PhDc, Leslee Frye, MSa, Nathan J. Blum, MDa,b
aThe Center for Management of ADHD, Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania;bDepartment of Pediatrics, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania;cSchool Psychology Program, Lehigh University, Bethlehem, Pennsylvania
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.This study was designed to investigate the perceptions of primary care
providers about their roles and the challenges of managing attention-deficit/hyper-activity disorder and to evaluate differences between providers who serve families primarily from urban versus suburban settings.
METHODS.The ADHD Questionnaire was developed to assess primary care provider
views about the extent to which clinical activities that are involved in the manage-ment of attention-deficit/hyperactivity disorder are appropriate and feasible in pri-mary care. Participants were asked to rate each of 24 items of the questionnaire twice: first to indicate the appropriateness of the activity given sufficient time and resources and second to indicate feasibility in their actual practice. Informants used a 4-point scale to rate each item for appropriateness and feasibility.
RESULTS.An exploratory factor analysis of primary care provider ratings of the
appro-priateness of clinical activities for managing attention-deficit/hyperactivity disorder identified 4 factors of clinical practice: factor 1, assessing attention-deficit/hyperac-tivity disorder; factor 2, providing mental health care; factor 3, recommending and monitoring approved medications; and factor 4, recommending nonapproved med-ications. On a 4-point scale (1 ⫽ not appropriate to 4⫽ very appropriate), mean ratings for items on factor 1, factor 2, and factor 3 were high, indicating that the corresponding domains of practice were viewed as highly appropriate. Feasibility challenges were identified on all factors, but particularly factors 1 and 2. A significant interaction effect, indicating differences between appropriateness and feasibility as a function of setting (urban versus suburban), was identified on factor 1. The
chal-lenges of assessing attention-deficit/hyperactivity disorder were greater for urban than for suburban primary care providers.
CONCLUSIONS.Primary care providers believe that it is highly appropriate for them to have a role in the management of
deficit/hyperactivity disorder. Feasibility issues were particularly salient related to assessing attention-deficit/hyperactivity disorder and providing mental health care. The findings highlight the need not only for additional training of primary care providers but also for practice-based resources to assist with school communica-tion and collaboracommunica-tion with mental health agencies, especially in urban practices.
A
TTENTION-DEFICIT/HYPERACTIVITY DISORDER (ADHD)is the most commonly occurring disruptive behavior disorder encountered by clinicians in primary care. This condition is estimated to occur among 3% to 10% of school-aged children.1,2 In addition, ADHD often coexists with mental health and learning disorders. Amongclinic-referred children with ADHD, it is estimated that 50% have oppositional defiant disorder or conduct disorder, 30% have an anxiety disorder, 25% have a depressive disorder, and 25% have a learning disability.3Although the
prevalence of comorbid conditions in primary care settings is somewhat lower than rates in clinic-referred samples, the prevalence is still high (eg, 40% oppositional defiant disorder, 10% depressive disorders).2,4
www.pediatrics.org/cgi/doi/10.1542/ peds.2007-0383
doi:10.1542/peds.2007-0383
Key Words
ADHD, primary care, feasibility Abbreviations
ADHD—attention-deficit/hyperactivity disorder
AAP—American Academy of Pediatrics PCP—primary care provider
AQ-PCP—ADHD Questionnaire for Primary Care Providers
A major venue for the delivery of services to children with ADHD in the United States is primary care.5–7The
American Academy of Pediatrics (AAP) has affirmed the critical role of primary care providers (PCPs) in the de-livery of services to children with ADHD. The AAP, through its Committee on Quality Improvement, has issued guidelines for assessment and treatment of this disorder.1,8These guidelines highlight the importance of
obtaining information from the child, parents, and teachers about ADHD and potential comorbid conditions in conducting an assessment of ADHD. Also, the guide-lines emphasize that treatment planning ought to rep-resent a collaborative effort among the family, school, and health systems and that treatment, including phar-macologic and/or behavioral methods, should be de-signed to improve specified academic and behavioral targets.
Most primary care pediatricians report that they are aware of the AAP guidelines, and⬎75% have reported that they incorporate the guidelines into their practice9;
however, when asked about specific components of the guidelines, only 35% reported using all 4 assessment components recommended by the AAP.9 When PCPs
have been offered support and education, the AAP guidelines generally have been implemented success-fully; however, even in these situations, several obsta-cles have been encountered, including a lack of clarity about how to interpret discrepant findings from parent and teacher reports, limited knowledge of community resources, and limited information about how to identify children who are in need of psychoeducational evalua-tion and how to obtain these evaluaevalua-tions from the school.10,11In addition, providers often report that lack of
time, reimbursement issues, lack of training, and the challenges of communicating with schools make it diffi-cult to manage ADHD in the context of primary care practice.10,12 Furthermore, research has shown that the
challenges of providing care to families who are served in clinics that are funded primarily by public insurance differ from those that arise among families who are served in practices that are financed mainly through private insurance.12
Although PCPs are assuming a greater role in the management of ADHD, there continues to be a substan-tial gap between existing need and the capacity to pro-vide ADHD services in the context of primary care prac-tice. Improved understanding of what PCPs believe is appropriate for them to do compared with what is fea-sible may help to identify effective strategies to facilitate the delivery of ADHD services in primary care. Several studies have investigated the feasibility of providing ADHD services in the context of primary care, and a recent study found that PCPs who served predominately families from low-income communities experienced greater challenges in caring for children with ADHD than PCPs who served more affluent families12;
how-ever, the research generally has not assessed feasibility in the context of what PCPs view as appropriate for them to do and has used surveys with unknown reliability. This study is unique in that we (1) developed a standardized and reliable instrument for assessing PCP perceptions of
both the appropriateness and the feasibility of a wide range of clinical activities related to the assessment and treatment of ADHD, (2) compared ratings of appropri-ateness and feasibility as a method of identifying chal-lenges in managing ADHD, and (3) compared the views of PCPs who practice in low-income urban communities versus suburban settings to understand whether these groups differ with regard to their roles and challenges in treating children with ADHD.
METHODS
Development of the ADHD Questionnaire for Primary Care Providers
The ADHD Questionnaire for Primary Care Providers (AQ-PCP) was developed to assess PCP views about the extent to which clinical activities that are involved in the management of ADHD are appropriate and feasible in the context of primary care. The items in this question-naire were developed on the basis of (1) a careful review of the AAP guidelines for assessing ADHD, (2) a review of research on the roles of PCPs in providing care to children with ADHD in the context of primary care, and (3) a series of focus groups with PCPs.
Focus groups were conducted across 4 practices (2 urban and 2 suburban) and included 29 PCPs who were employed within the extensive primary care network of the Children’s Hospital of Philadelphia (CHOP). Ques-tions posed during the focus groups included the follow-ing: “What is your role in the assessment and treatment of ADHD?” “How do you view your role (what is appro-priate for you to do)?” and, “What are the major chal-lenges you encounter in serving children with ADHD?” The focus group discussions centered on 5 themes: (1) roles and challenges related to assessment; (2) roles and challenges related to treatment; (3) communication problems in working with schools and mental health agencies; (4) barriers to care, including time and reim-bursement; and (5) supports that might be useful (eg, education of PCPs, consultation with ADHD experts, support in linking with school, provision of family ther-apy in primary care setting).
Study Participants
The study was conducted in 27 primary care practices that are affiliated with CHOP. Among these practices, 23 provided services primarily to children and families who resided in the outskirts of the Philadelphia and sur-rounding region (referred to as suburban practices). The remaining 4 practices were based in the city and served as resident training sites (urban practices). The question-naire was administered to 181 PCPs (134 suburban, 46 urban), who all were board certified in pediatrics. Ques-tionnaires from 121 PCPs were returned.
Procedures
The study was exempted from review by the human subjects committee of the institutional review board at CHOP because the survey contained no information that could potentially identify a child. In addition, no infor-mation that could be used to identify the informant (PCP) was obtained, with the exception of name of practice. The Medical Director of Primary Care Services informed PCPs about the study via e-mail. Subsequently, a letter and packet of questionnaires were sent to site managers requesting that they distribute the AQ-PCP to each PCP in the practice. Practice managers and selected practice leaders were contacted periodically to remind them to urge PCPs to submit their surveys. In addition to this method, surveys were administered at a regularly
scheduled meeting that included ⬃65% of the urban-based PCPs. PCPs were not reimbursed for their partici-pation in this study.
Statistical Analyses
To organize the large volume of data and identify salient constructs underlying the 24 items of the AC-PCP, we conducted a factor analysis. The factors that were iden-tified in the analysis represent groups of clinical activities that are related to one another and thus reflect salient roles or domains of practice for PCPs associated with the management of ADHD. Given the uncertainty about the underlying constructs of the AQ-PCP, an exploratory as opposed to a confirmatory factor analysis was con-ducted. A series of common factor analyses using squared multiple correlations as the initial communality estimates were conducted to identify the latent structure of the AQ-PCP.13–15Determination of the most
parsimo-nious factor structure was assessed using both orthogo-nal (varimax) and oblique (promax) rotation methods. Factor analysis yields pattern coefficients or factor load-ings; the magnitude of these coefficients is indicative of the strength of the association between the item on the AQ-PCP and the proposed factor. Pattern coefficients
ⱖ0.40 were predetermined to indicate a significant as-sociation between the item on the AQ-PCP and the proposed factor. Factor structures were evaluated
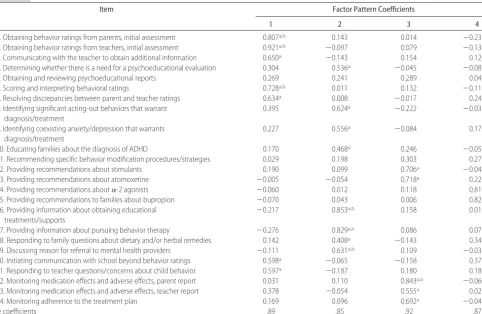
ac-TABLE 1 Four-Factor Structure of the AQ-PCP
Item Factor Pattern Coefficients
1 2 3 4
1. Obtaining behavior ratings from parents, initial assessment 0.807a,b 0.143 0.014 ⫺0.235
2. Obtaining behavior ratings from teachers, initial assessment 0.921a,b ⫺0.097 0.079 ⫺0.138
3. Communicating with the teacher to obtain additional information 0.650a ⫺0.143 0.154 0.126
4. Determining whether there is a need for a psychoeducational evaluation 0.304 0.536a ⫺0.045 ⫺0.085
5. Obtaining and reviewing psychoeducational reports 0.269 0.241 0.289 0.049
6. Scoring and interpreting behavioral ratings 0.728a,b 0.011 0.132 ⫺0.115
7. Resolving discrepancies between parent and teacher ratings 0.634a 0.008 ⫺0.017 0.242
8. Identifying significant acting-out behaviors that warrant diagnosis/treatment
0.395 0.624a ⫺0.222 ⫺0.031
9. Identifying coexisting anxiety/depression that warrants diagnosis/treatment
0.227 0.556a ⫺0.084 0.178
10. Educating families about the diagnosis of ADHD 0.170 0.468a 0.246 ⫺0.051
11. Recommending specific behavior modification procedures/strategies 0.029 0.198 0.303 0.273
12. Providing recommendations about stimulants 0.190 0.099 0.706a ⫺0.045
13. Providing recommendations about atomoxetine ⫺0.005 ⫺0.054 0.718a 0.221
14. Providing recommendations about␣-2 agonists ⫺0.060 0.012 0.118 0.819a,b
15. Providing recommendations to families about bupropion ⫺0.070 0.043 0.006 0.825a,b
16. Providing information about obtaining educational treatments/supports
⫺0.217 0.853a,b 0.158 0.015
17. Providing information about pursuing behavior therapy ⫺0.276 0.829a,b 0.086 0.077
18. Responding to family questions about dietary and/or herbal remedies 0.142 0.408a ⫺0.143 0.343
19. Discussing reason for referral to mental health providers ⫺0.111 0.631a,b 0.109 ⫺0.038
20. Initiating communication with school beyond behavior ratings 0.598a ⫺0.065 ⫺0.158 0.375
21. Responding to teacher questions/concerns about child behavior 0.597a ⫺0.187 0.180 0.186
22. Monitoring medication effects and adverse effects, parent report 0.031 0.110 0.843a,b ⫺0.066 23. Monitoring medication effects and adverse effects, teacher report 0.378 ⫺0.054 0.555a 0.021
24. Monitoring adherence to the treatment plan 0.169 0.096 0.692a ⫺0.048
␣coefficients .89 .85 .92 .87
cording to standard criteria16: (1) eigenvalues of the
un-rotated factors areⱖ1.0; (2) the rotated factor solution meets criteria for Cattell’s17 scree test; (3) each factor
demonstrates adequate internal consistency, with␣ co-efficients ⱖ.70; (4) the final factor solution minimizes intercorrelations among retained, unit-weighted factors and items with appreciable loadings (ⱖ0.40) on⬎1 fac-tor; and (5) the proposed factors are clinically meaning-ful.
Once the factor structure of the AQ-PCP was identi-fied, the mean rating of the items on each factor was computed (range: 1– 4). A mean rating of ⱖ3.0 for a factor (corresponding with a rating of “much” on the scale) was interpreted as indicating that the factor or domain of practice was viewed as highly appropriate for PCPs. A series of t tests was conducted to determine whether there were differences between PCPs who worked in suburban versus urban practices with regard to their perceptions of the appropriateness of each do-main of practice. For these 4 tests of significance, the␣ level was adjusted to .0125 to account for the multiple comparisons. For cases in which significant differences were identified, effect sizes (Cohen’s d18) were
com-puted.
The challenge faced by PCPs in implementing their roles in the management of ADHD was operationalized as the difference between perceptions of appropriateness and feasibility. A series of repeated measures analyses of variance were conducted to determine whether the dif-ference between mean item ratings for appropriateness and feasibility for each of the 4 factors was significant. The␣level was adjusted to .0125 in conducting these 4 analyses. Effect sizes were calculated by using Cohen’sd, adjusted for the correlation between scores for appropri-ateness and feasibility.19
RESULTS
Participant Characteristics
In the 23 suburban practices, the percentage of children who were eligible for Medicaid ranged from 2% to 32% (mean: 10%). Eligibility for Medicaid in the 4 urban practices ranged from 62% to 70% (mean: 66%). In the suburban practices, the ethnic/racial composition of all children served was 13% black, 2% Asian, 2% Latino, 70% white, and 13% other or unknown. In the urban practices, the ethnic/racial composition of all children was 85% black, 1% Asian, 2% Latino, 7% white, and 5% other or unknown. In both the suburban and urban practices, 50% of the children served were female.
There was essentially no difference between the ur-ban and suburur-ban practices with regard to the percent-age of PCPs in full-time practice (ⱖ80% of a full-time equivalent). In the suburban practices, 61% of the PCPs were in full-time practice, whereas in the urban settings 58% were in full-time practice. Also, PCPs in the subur-ban and ursubur-ban practices were similar with regard to mean number of years of experience in the CHOP pri-mary care system (5.7 and 6.6 years, respectively). Ap-proximately 95% of the urban PCPs were involved in resident education, whereas ⬍10% of the PCPs in the
suburban practices were involved in resident teaching activities.
There were no missing data for 108 (89%) cases. Eleven of the cases contained ⱕ3 missing responses (⬍15% of items), and these cases were retained in the study. For these cases, missing data were imputed via multiple regression. The remaining 2 cases contained missing responses forⱖ15% of the items, so these scales were discarded. Completed surveys were returned by 119 clinicians (66% of total number of PCPs sent ques-tionnaires), including 82 (61%) in suburban practice and 37 (80%) in urban practice.
Factor Analysis of the AQ-PCP
A series of factor analyses was conducted, and it was determined that a 4-factor (oblique) solution best met the criteria described for factor retention. In other words, the factor analysis indicated that the AQ-PCP assesses 4 constructs or domains of PCP practice related to the management of ADHD. This factor solution ac-counted for a total variance of 61%. Table 1 presents the pattern coefficients (factor loadings) for the 4 constructs that emerged from the factor analysis. All but 2 of the AQ-PCP items showed significant factor loadings (ie,
ⱖ0.40) and were retained in the final solution. The first factor, which accounted for 45% of the total scale vari-ance, contained 7 items with factor loadingsⱖ0.40. The
␣ coefficient for this factor was .89, indicating a high level of internal consistency reliability. This factor, which was labeled “assessing ADHD,” contained items related to obtaining information from parents and teach-ers for the purpose of assessing ADHD.
The second factor, accounting for 7% of total vari-ance, included 8 items. The ␣coefficient for this factor was high (.85). This factor, referred to as “providing mental health care,” consisted of items related to edu-cating families about psychosocial and educational treat-ments and determining the presence of comorbid con-ditions.
The third factor, accounting for 5% of total variance, comprised 5 items and had a high ␣ coefficient (.92). This factor, labeled “recommending and monitoring Food and Drug Administration [FDA]–approved medi-cations for ADHD,” consisted of items that pertained to the use of stimulants and atomoxetine and monitoring medication effectiveness using parent and teacher rating scales.
The fourth factor, accounting for 3% of total variance, contained 2 items. The internal consistency reliability for this factor also was high (.87). This factor, referred to as “recommending non–FDA-approved medications for ADHD,” consisted of items related to the use of ␣-2 agonists and bupropion in managing ADHD.
Levels of Appropriateness for Each Factor
The distribution of scores on factors 1 and 2 did not deviate substantially from normality, but there were severe deviations from normality on the other 2 factors. Given that the size of the sample was relatively large, it is not likely that the nonnormality of the distributions for factors 3 and 4 exerted a meaningful impact on the analyses.20Levene’s test of homogeneity of variance was
nonsignificant for each factor when comparing the dis-tributions for urban and suburban PCPs, supporting the use of analyses of variance.
Table 3 presents the mean rating for each factor. As indicated, mean ratings for factors 1, 2, and 3 were high (ⱖ3.0), particularly for factors 2 and 3 (3.28 and 3.33, respectively), indicating that the corresponding domains of practice were viewed as highly appropriate for PCPs; however, the mean rating for factor 4 was low (⬍2.0), indicating that this domain of practice (recommending non–FDA-approved medications for ADHD) generally was viewed as lacking in appropriateness for PCPs.
Table 3 also indicates the mean appropriateness rating for each item of the AQ-PCP. There was considerable variability among mean item ratings within each factor. For example, mean item ratings ranged from 2.61 to 3.55 for factor 1. Obtaining behavior ratings from par-ents and teachers was viewed as a highly appropriate activity for PCPs, whereas initiating communication with school professionals, responding to teacher ques-tions about child behavior, and resolving discrepancies between parent and teacher ratings were viewed as hav-ing lower levels of appropriateness. With regard to factor 2 (providing mental health care), all of the mean item ratings were high, except responding to family questions about diet and identifying comorbid anxiety and depres-sion. All of the items related to factor 3 (recommending and monitoring FDA-approved medications) had high mean ratings, and the 2 items on factor 4 (recommend-ing and monitor(recommend-ing non–FDA-approved medications) had low mean ratings. Differences between urban and suburban PCPs were not significant at the .0125 level on any of the factors.
Feasibility Challenges Related to Each Factor
Scores on each factor for ratings of feasibility were com-puted. The␣coefficients for each of the feasibility factors were high (⬎.80), which supported the internal consis-tency reliability of these dimensions. Mean item ratings of feasibility were examined for each of the 4 factors. The distribution of mean item ratings of feasibility on all factors, except factor 4, did not deviate substantially from normality. Given the relatively large sample size, it
is not likely that the nonnormality of the distribution for factor 4 had a meaningful impact on the analyses.20
The difference between mean item ratings for appro-priateness and feasibility was significant for each factor (factor 1, F1,117 ⫽ 170.82,P ⬍.001; factor 2, F1,117 ⫽
103.59, P ⬍ .001; factor 3, F1,117 ⫽ 82.14, P ⬍ .001;
factor 4, F1,117⫽11.60,P⬍.001). Effect sizes were large
TABLE 2 Unit-Weighted Interfactor Correlations for the AQ-PCP
Factor Factor
2 3 4
1 0.56 0.73 0.44
2 — 0.67 0.53
3 — — 0.48
TABLE 3 Mean Factor and Item Appropriateness Ratings for the AQ-PCP
Factor/Item Mean SD
Factor 1: assessing ADHD 3.07 0.67
1. Obtaining behavior ratings from parents, initial assessment
3.55 0.65
2. Obtaining behavior ratings from teachers, initial assessment
3.50 0.71
3. Communicating with the teacher to obtain additional information
3.03 0.88
6. Scoring and interpreting behavioral ratings 3.08 0.93 7. Resolving discrepancies between parent and
teacher ratings
2.76 0.99
20. Initiating communication with school beyond behavior ratings
2.61 0.84
21. Responding to teacher questions/concerns about child behavior
2.88 0.91
Factor 2: providing mental health care 3.28 0.56 4. Determining whether there is a need for a
psychoeducational evaluation
3.46 0.72
8. Identifying significant acting-out behaviors that warrant diagnosis/treatment
3.19 0.83
9. Identifying coexisting anxiety/depression that warrants diagnosis/treatment
2.89 0.93
10. Educating families about the diagnosis of ADHD
3.67 0.56
16. Providing information about obtaining educational treatments/supports
3.38 0.76
17. Providing information about pursuing behavior therapy
3.39 0.69
18. Responding to family questions about dietary and/or herbal remedies
2.74 0.97
19. Discussing reason for referral to mental health providers
3.53 0.63
Factor 3: recommending and monitoring FDA-approved medications for ADHD
3.33 0.76
12. Providing recommendations about stimulants
3.42 0.86
13. Providing recommendations about atomoxetine
3.16 1.05
22. Monitoring medication effects and adverse effects, parent report
3.48 0.78
23. Monitoring medication effects and adverse effects, teacher report
3.18 0.87
24. Monitoring adherence to the treatment plan 3.38 0.79 Factor 4: recommending non–FDA-approved
medications for ADHD
1.88 0.93
14. Providing recommendations about␣-2 agonists
1.95 1.02
15. Providing recommendations to families about bupropion
1.79 0.95
Items that did not load on any factor
5. Obtaining and reviewing psychoeducational reports
3.22 0.89
11. Recommending specific behavior modification procedures/strategies
for factors 1 and 2 (1.01 and 0.93, respectively), moder-ate for factor 3 (0.44), and small for factor 4 (0.20). These findings suggested that PCPs experience chal-lenges with implementing clinical activities in each of the 4 domains of ADHD practice but especially in the domains related to factor 1 (assessing ADHD) and factor 2 (providing mental health care).
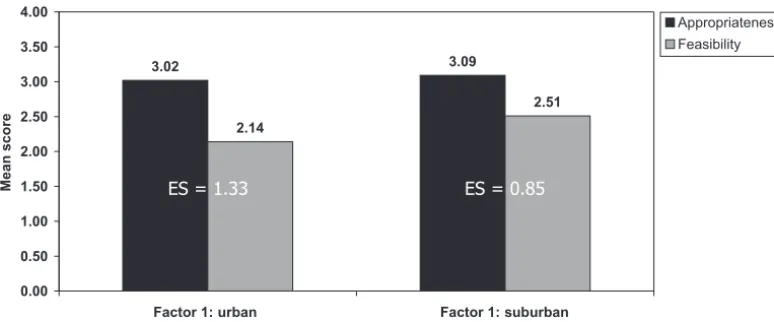
A significant interaction effect, indicating differences between appropriateness and feasibility as a function of setting (urban versus suburban), was identified on factor 1 (F1,117⫽7.75,P⫽.006), and the interaction effect on
factor 3 just failed to reach significance using the ad-justed␣level of .0125 (F1,117⫽5.96,P⫽.016). Figure
1 illustrates the interaction effect for factor 1. The dif-ference between appropriateness and feasibility was greater for urban PCPs (effect size of 1.33) than for suburban PCPs (effect size of 0.85). Figure 2 illustrates the interaction effect for factor 3. Once again, the differ-ence between appropriateness and feasibility was greater for urban PCPs (effect size: 0.64) than for suburban PCPs (effect size: 0.36). The interaction effect for factors 2 and 4 was not significant.
DISCUSSION
This study describes the development of a standardized and reliable method for examining PCP perceptions of the appropriateness and feasibility of a wide range of clinical activities that pertain to the assessment and treatment of ADHD. Unique aspects of the study are that we systematically compared ratings of appropriateness and feasibility to identify practice challenges, and we contrasted the views of PCPs from urban and suburban settings. The findings demonstrated that urban PCPs ex-perienced more challenges in providing certain aspects of ADHD care than suburban PCPs, but both urban and suburban PCPs generally rated ADHD clinical activities as being appropriate for them.
The factor analysis of the AQ-PCP identified 4 reliable constructs, referring to domains of practice in the manage-ment of ADHD in primary care (assessing ADHD, providing mental health care, recommending and monitoring FDA-approved medications for ADHD, and recommending non– FDA-approved medications for ADHD). In general, each of these domains, with the exception of using non–FDA-approved medications, was viewed as highly acceptable
3.02 3.09 2.14 2.51 0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 n a b r u b u s 1: r o t c a F n a b r u 1: r o t c a F Mean score Appropriateness Feasibility 5 8 . 0 = S E 3 3 . 1 = S E FIGURE 1
Differences between mean item ratings of appropriateness and feasibility as a function of setting for factor 1 (assessing ADHD). ES indicates effect size. Items were rated on a 4-point scale (1⫽not at all; 2⫽somewhat; 3⫽much; 4⫽very).
3.10 3.43 2.61 3.16 0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 n a b r u b u s 3: r o t c a F n a b r u 3: r o t c a F Mean score Appropriateness Feasibility
ES = 0.64 ES = 0.36
FIGURE 2
and within the scope of practice of PCPs. The findings of this study affirm the appropriateness of situating services for children with ADHD in primary care and the general acceptability of ADHD clinical activities to PCPs. At the same time, this study highlights the limits of primary care practice related to managing ADHD and identifies several challenges that need to be addressed, particularly within urban primary care practices that serve low-income com-munities.
Although assessing ADHD generally was viewed by PCPs as within their scope of practice, there was sub-stantial variability in their ratings of the items on this factor. PCPs reported that it is highly appropriate for them to obtain rating scales from parents and teachers to assess ADHD; however, initiating communication with school professionals (in addition to requesting rating scales) and responding to questions from teachers were viewed as less appropriate, suggesting that PCPs may need assistance from other members of the practice when communication with the school is needed.
Factor 2, referring to providing mental health care, included primarily items related to educating families about psychosocial and educational treatments and as-sessing for the presence of comorbid conditions, such as behavior disorders, emotional disorders, and learning disabilities. PCPs generally believed that the range of activities included in this factor was within their scope of practice. It is noteworthy that views about the appropri-ateness of screening for anxiety and depression were relatively low, suggesting that PCPs may need education or additional resources to assist them in screening for internalizing problems.
The items on factor 2 did not pertain to the actual provision of mental health services such as behavior therapy and family counseling. The 1 item on the AQ-PCP that referred to the provision of behavior therapy (item 11, recommending specific behavior modification strategies to families) did not load on factor 2 or any of the other factors; however, this item had a relatively high rating for appropriateness, suggesting that it gener-ally was viewed as being within the scope of practice for PCPs.
All of the items related to recommending and moni-toring FDA-approved medications (stimulants and ato-moxetine) were within the acceptable range, indicating that these activities are within the scope of practice of PCPs. The 2 items related to recommending non–FDA-approved medications (bupropion and␣-2 agonists) had low ratings of appropriateness, suggesting that PCPs gen-erally would prefer to refer to specialists (eg, child and adolescent psychiatrists, developmental-behavioral pe-diatricians, pediatric neurologists) when the first-line medications for ADHD are not successful in treating this disorder.
Providers reported that they experience significant challenges in managing ADHD. The challenges were par-ticularly strong related to factor 1 (assessing ADHD), which contained several items related to obtaining in-formation from schools, and factor 2 (providing mental health care). The challenges in these domains high-lighted the problems experienced by PCPs in
collaborat-ing with schools and makcollaborat-ing appropriate referrals to mental health providers, which have been identified as barriers in previous studies.10,21On presenting the
find-ings of this study to a focus group of PCPs, the providers highlighted the need for additional training related to assessment, school collaboration, family education, and collaboration with mental health providers; however, it was clear that continuing education was not sufficient to address the feasibility issues faced by PCPs. A recurrent theme among urban providers during this discussion was the need for a team member or a “point person” (eg, nurse, school liaison, mental health specialist) to assist in collaborating with schools, educating families, arranging for appropriate and affordable mental health care, and facilitating follow-up with mental health providers. Also, PCPs indicated that it would be helpful to have ADHD experts available in person or by telephone to assist with medication issues, questions about comorbidity, and ap-propriate referrals. Furthermore, there was some discus-sion about the need for a practice-based family behavior therapist.
This investigation affirmed the findings of the study by Leslie et al12that there are differences between urban
and suburban providers with regard to the management of ADHD. The findings illustrated in Figs 1 and 2 point out 2 significant feasibility problems for urban practitio-ners: urban PCPs experience substantially greater chal-lenges with assessing ADHD and using FDA-approved medications than suburban PCPs. Subsequent focus groups with PCPs indicated that these challenges reflect the problems that urban PCPs experience with getting information from urban schools and obtaining feedback on a consistent basis from parents and teachers in mon-itoring medications.
In comparing the findings of urban and suburban PCPs in this study, it should be noted that these groups differed with regard not only to the demographics of the children served (eg, race/ethnicity, socioeconomic sta-tus) but also to the involvement of providers in resident education. Practicing in an academic context has been found to be associated with a greater likelihood of im-plementing AAP guidelines9; therefore, the greater
fea-sibility issues reported by urban PCPs as compared with suburban PCPs may be attributable to factors that are associated with poverty (eg, higher psychosocial stress among families, greater challenges faced by schools) as well as factors that are related to the PCPs (eg, frustra-tion in trying to implement the relatively high standards of the AAP guidelines in an urban setting).
Also, as indicated, the urban and suburban PCPs dif-fered with regard to both patient demographics and the involvement of PCPs in resident training. Suburban PCPs generally were not involved in resident training, whereas urban PCPs were. It is possible that the chal-lenges faced by urban PCPs who are not involved in resident education differ in some ways from those who are trainers. Also, urban PCPs who practice in clinics that are not affiliated with tertiary care hospitals such as CHOP may have fewer resources, which could make it more challenging for them to manage ADHD than their colleagues who practice in hospital-affiliated programs. One additional limitation is that the urban PCPs in this study may have had more opportunities for continuing education about the management of ADHD than the suburban PCPs.
CONCLUSIONS
The findings of this study demonstrated that PCPs have 4 major roles related to the management of ADHD: assessing the disorder, providing mental health care, recommending and monitoring FDA-approved tions, and recommending non–FDA-approved medica-tions. Providers indicated that each of these roles, with the exception of recommending non–FDA-approved medications, is appropriate for them and within their scope of practice. Feasibility issues were identified par-ticularly related to assessing ADHD and providing ADHD-related mental health care for children and fam-ilies (eg, teaching behavior management strategies). The challenges of assessing ADHD seemed to be strongly related to the problems that PCPs experience with get-ting information from schools and communicaget-ting with educational professionals. Urban PCPs reported much more difficulty with assessing ADHD and medicating children using FDA-approved drugs than their col-leagues in suburban practice. The findings highlight the need not only for additional training of PCPs but also for practice-based resources to assist with school communi-cation and collaboration with mental health agencies.
ACKNOWLEDGMENTS
This study was supported by funding through the Chair’s Initiative in the Department of Pediatrics at CHOP.
We are extremely grateful to Trude Haecker, Maggie Swietlik, and Jeanie Kim Carpenter for assistance in conducting this study.
REFERENCES
1. American Psychiatric Association.Diagnostic and Statistical Man-ual of Mental Disorders.4th ed. Text revision. Washington, DC: American Psychiatric Association; 2000
2. Brown RT, Freeman WS, Perrin JM, et al. Prevalence and assessment of attention deficit/hyperactivity disorder in pri-mary care settings. Pediatrics. 2001;107(3). Available at: www.pediatrics.org/cgi/content/full/107/3/e43
3. Barkley RA.Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. 3rd ed. New York, NY: Guilford; 2006
4. Costello EJ, Costello AJ, Edelbrock C, et al. Psychiatric disor-ders in pediatric primary care: the new hidden morbidity.
Psychiatry.1988;45:1107–1116
5. Burns BJ, Costello EJ, Angold A, et al. Children’s mental health service use across service sectors.Health Aff (Millwood).1995; 14:147–159
6. Leaf PJ, Alegria M, Cohen P, et al. Mental health service use in the community and schools: results from the four-community MECA study. J Am Acad Child Adolesc Psychiatry. 1996;35: 889 – 897
7. Rappley MD, Gardiner JC, Jetton JR, Houang RT. The use of methylphenidate in Michigan.Arch Pediatr Adolesc Med.1995; 149:675– 679
8. American Academy of Pediatrics, Subcommittee on Attention-Deficit/Hyperactivity Disorder and Committee on Quality Im-provement. Clinical practice guideline: treatment of the school-aged child with attention-deficit/hyperactivity disorder.
Pediatrics.2001;108:1033–1043
9. Rushton JL, Fant KE, Clark SJ. Use of practice guidelines in the primary care of children with attention-deficit/hyperactivity dis-order.Pediatrics.2004;114(1). Available at: www.pediatrics.org/ cgi/content/full/114/1/e23
10. Leslie LK, Weckerly J, Plemmons D, Landsverk J, Eastman S. Implementing the American Academy of Pediatrics attention-deficit/hyperactivity disorder diagnostic guidelines in primary care settings.Pediatrics.2004;114:129 –140
11. Polaha J, Cooper SL, Meadows T, Kratochvil CJ. The assess-ment of attention-deficit/hyperactivity disorder in rural pri-mary care: the portability of the American Academy of Pedi-atrics guidelines to the “real world.” Pediatrics.2005;115(2). Available at: www.pediatrics.org/cgi/content/full/115/2/e120 12. Leslie LK, Stallone K, Weckerly J, McDaniel AL, Monn A.
Implementing the ADHD guidelines in primary care: does one size fit all?J Health Care Poor Underserved.2006;17:302–327 13. Browne MW. An overview of analytic rotation in exploratory
factor analysis.Multivariate Behav Res.2001;36:111–150 14. Gorsuch RL. Exploratory factor analysis. In: Nesselroade JR,
Cattell RB, eds.Handbook of Multivariate Experimental Psychology. 2nd ed. New York, NY: Plenum; 1988:231–258
15. Wegener DT, Fabrigar LR. Analysis and design for nonexperi-mental data. In: Reis HT, Judd CM, eds.Handbook of Research Methods in Social and Personality Psychology. New York, NY: Cam-bridge University Press; 2000:412– 450
16. McDermott PA. National standardization of a uniform multi-situational measure of child and adolescent psychopathology.
Psychol Assess.1993;5:413– 424
17. Cattell RB. The scree test for the number of factors.Multivariate Behav Res.1966;1:245–276
18. Cohen J.Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Erlbaum; 1988
19. Ray JW, Shadish WR. How interchangeable are different esti-mators of effect size?J Consult Clin Psychol.1996;64:1316 –1325 20. Tabachnick BG, Fidell LS. Using Multivariate Statistics. 5th ed.
Boston, MA: Pearson; 2006
21. Guevara J, Fuedtner C, Romer D, et al. Fragmented care for inner-city minority children with attention-deficit/hyperactivity disorder.
DOI: 10.1542/peds.2007-0383
2008;121;e65
Pediatrics
Blum
Thomas J. Power, Jennifer A. Mautone, Patricia H. Manz, Leslee Frye and Nathan J.
Systematic Analysis of Roles and Challenges
Managing Attention-Deficit/Hyperactivity Disorder in Primary Care: A
Services
Updated Information &
http://pediatrics.aappublications.org/content/121/1/e65
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/121/1/e65#BIBL
This article cites 11 articles, 3 of which you can access for free at:
Subspecialty Collections
activity_disorder_adhd_sub
http://www.aappublications.org/cgi/collection/attention-deficit:hyper
Attention-Deficit/Hyperactivity Disorder (ADHD)
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior
Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2007-0383
2008;121;e65
Pediatrics
Blum
Thomas J. Power, Jennifer A. Mautone, Patricia H. Manz, Leslee Frye and Nathan J.
Systematic Analysis of Roles and Challenges
Managing Attention-Deficit/Hyperactivity Disorder in Primary Care: A
http://pediatrics.aappublications.org/content/121/1/e65
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.