A Quality Improvement
Project to Decrease Human
Milk Errors in the NICU
Reena Oza-Frank, PhD, RD, a, b, c Rashmi Kachoria, MPH, a, b James Dail, CLSSBB, MBA, d Jasmine Green, RN, RNC-NIC, BSN, e Krista Walls, RN, RNC-NIC, BSN, e Richard E. McClead Jr, MD, MHAd, e
aCenter for Perinatal Research, bResearch Institute, and dQuality Improvement Services, and eDivision of Neonatology, Nationwide Children's Hospital, Columbus, Ohio; and cDepartment of Pediatrics, College of Medicine, The Ohio State University, Columbus, Ohio
Dr Oza-Frank conceptualized and designed the study, oversaw data analyses, and drafted the initial manuscript; Ms Kachoria carried out the initial analyses and reviewed and revised the manuscript; Mr Dail provided critical comments on the analysis; Ms Green and Walls contributed to data collection and interpretation; Dr McClead conceptualized and designed the study; and all authors approved the fi nal manuscript as submitted.
DOI: 10.1542/peds.2015-4451
Accepted for publication Aug 22, 2016
Address correspondence to Reena Oza-Frank, PhD, RD, Nationwide Children’s Hospital, 700 Children’s Dr, Columbus, OH 43205. E-mail: reena.oza-frank@ nationwidechildrens.org
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2017 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no fi nancial relationships relative to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential confl icts of interest to disclose.
Human milk feeding, considered the optimal nutrition for infants, is recommended by the American Academy of Pediatrics 1 and the World
Health Organization. 2 It is also part
of the Healthy People 2020 national health agenda. 3 For preterm infants,
human milk reduces the incidence of necrotizing enterocolitis, improves feeding tolerance, promotes cognitive development, 4–7 and decreases
respiratory tract infections and sepsis. 8 As a result, many hospitals
have significantly increased their human milk feeding rates over the past 10 years. 9, 10
Similar to national breastfeeding trends, NICU breastfeeding rates have also recently increased. 11 Often,
expressed human/breast milk (EBM) is the only option during the early postnatal period for NICU-admitted infants due to oral feeding restrictions. Ensuring safe EBM in the NICU is a complex process; EBM needs to be
abstract
BACKGROUD AND OBJECTIVE Ensuring safe human milk in the NICU is a complex
process with many potential points for error, of which one of the most serious is administration of the wrong milk to the wrong infant. Our objective was to describe a quality improvement initiative that was
associated with a reduction in human milk administration errors identified over a 6-year period in a typical, large NICU setting.
METHODS: We employed a quasi-experimental time series quality improvement
initiative by using tools from the model for improvement, Six Sigma methodology, and evidence-based interventions. Scanned errors were identified from the human milk barcode medication administration system. Scanned errors of interest were wrong-milk-to-wrong-infant, expired-milk, or preparation errors. The scanned error rate and the impact of additional improvement interventions from 2009 to 2015 were monitored by using statistical process control charts.
RESULTS: From 2009 to 2015, the total number of errors scanned declined
from 97.1 per 1000 bottles to 10.8. Specifically, the number of expired milk error scans declined from 84.0 per 1000 bottles to 8.9. The number of preparation errors (4.8 per 1000 bottles to 2.2) and wrong-milk-to-wrong-infant errors scanned (8.3 per 1000 bottles to 2.0) also declined.
CONCLUSIONS: By reducing the number of errors scanned, the number of
opportunities for errors also decreased. Interventions that likely had the greatest impact on reducing the number of scanned errors included installation of bedside (versus centralized) scanners and dedicated staff to handle milk.
received, stored, and prepared with fortifiers or additives, and the bottles combined/divided before feeding. There is potential for error at any of these steps. When considering the large volume that is handled to feed many infants, each receiving multiple feedings per day, this risk is compounded. 12 Medication errors are
3 times more likely in hospitalized children compared with adults, 13
ranging from 5% to 27% of hospital stays. Because human milk is treated in a similar fashion to medications for hospitalized infants, 14 a similar error
frequency may also extend to human milk handling and administration.15
One of the most serious human milk errors that can occur is administration of the wrong milk to the wrong infant. This can result in the transmission of infectious diseases that may be present in human milk and leads to in-depth infectious disease testing of the donor mom, recipient infant, and recipient mom as well as authorization to disclose results to the recipient’s parents. Wrong human milk administration errors can erode the trust and confidence of patient families and result in increased costs from additional tests. 16
In 2008, the NICU at Nationwide Children’s Hospital (NCH) in Columbus, Ohio began a quality improvement (QI) initiative in an attempt to eliminate errors of the wrong milk being scanned in response to actual breast milk errors reported by nursing staff voluntarily through the hospital event reporting system. The purpose of the initiative was to decrease errors and the number of opportunities for actual errors. 17 This report describes the
interventions targeted at eliminating scanned wrong milk errors and improving overall breast milk safety.
METHODS
Context
NCH is an academic, nonprofit, free-standing children’s hospital located
in Columbus, Ohio. Annually, the total inpatient and outpatient visits at NCH exceed 1.3 million. Neonatal services (neonatology) is a joint venture between NCH and central Ohio maternity hospitals. It is one of the largest neonatal intensive care programs in the United States with >250 neonatal beds. The main campus NICU consists of 114 neonatal beds divided among 3 level IIIC NICUs with >2100 neonates admitted per year. Twenty percent of these infants weigh ≤1500 g at birth, and >30% have major surgical problems. Currently, the NCH NICU consistently administers >6000 human milk feedings monthly, and up to 60% of infants are on human milk at any given time. 18, 19
Interventions
The original breast milk
administration process included handwritten labeling of milk bottles, and preparation/administration of bottles by nursing staff, without dedicated space to thaw, prepare, and warm the bottles. Thus, in response to actual breast milk errors reported by nursing staff voluntarily through the hospital event reporting system in 2008, a multidisciplinary QI team was established. The team consisted of representatives from clinical nutrition and lactation, neonatology (including nursing staff), information systems, and QI services. Using tools from the Institute for Healthcare Improvement Model for Improvement 20 and Six Sigma, 21 the
QI team flowcharted the original process of collecting, storing, and administering breast milk; examined existing policies related to the process; and identified areas in the workflow where the system failed (failure mode effects analysis). 22 The
QI team identified key processes and implemented several strategies to reduce error rates.
First, the QI team revised and updated the EBM storage and handling process. Second, they
sought approval from the hospital administration to purchase the Timeless Medical Systems’ electronic breast milk tracking system (a barcode medication administration system [BCMA] known as “Women and Infants” [W&I]). W&I was chosen because it allows for comprehensive tracking of EBM bottles. The team was confident that the decision to implement W&I would have a dramatic effect on reducing the number of wrong-milk-to-wrong-infant errors. The effort to reduce scanned and actual errors was based on previously defined best practices for breast milk administration. 23, 24
W&I was implemented for use by nurses to check in, prepare, and administer EBM feedings via centralized scanners. At this time, bedside medication barcoding was unavailable in the NICU; therefore, to use W&I optimally, scanners had to be purchased. Because of budgetary constraints, only a limited number of scanners were initially purchased. These were installed in centralized locations throughout the NICU. Training and implementation of W&I took a few months to assess small processes of change needed before full implementation. The partial implementation of W&I in 2009 provided a baseline scanned error rate, which was used to assess subsequent improvement interventions to reduce scanned and actual errors. Scanned errors were then documented and graphed on statistical process control charts.
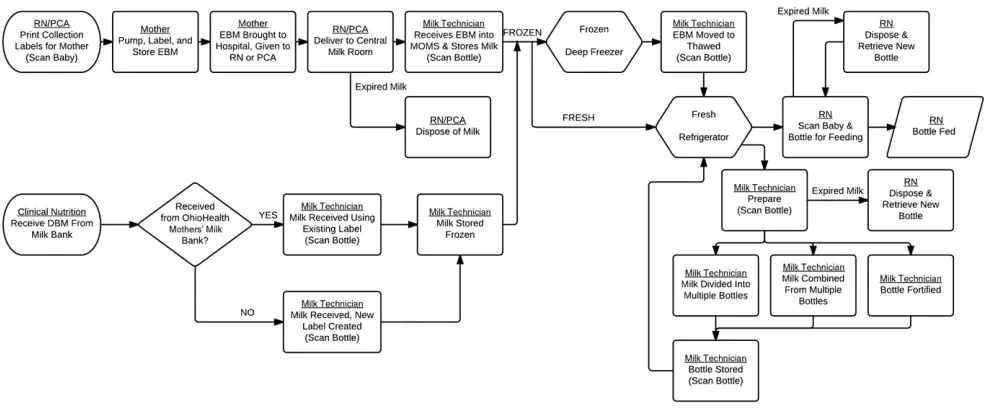
In 2011, another actual wrong-milk-to-wrong-infant error occurred. A full root cause analysis was completed with a detailed timeline of events and identification of individual and system related causal factors. A revised comprehensive human milk handling and storage process (exclusive of donor milk) was developed and audited for compliance ( Fig 1). Moreover, the process for the evaluation and follow-up of wrong human milk administration errors was standardized. In addition, a full-time dedicated milk technician was hired, and plans for a centralized milk room were developed.
Measures and Analysis
The W&I system provides 66 possible scanned error codes. Ten codes were evaluated as “critical errors.” These were grouped into 3 categories: human milk expiration, wrong milk to wrong infant, and human milk preparation ( Table 1). The monthly error rate, the primary outcome metric, was defined as the number of errors scanned in the W&I system divided by the total number of bottles fed per month as
logged in W&I. The scanned error rate and the impact of additional improvement interventions from 2009 to 2015 were monitored by using statistical process control charts. Control charts were generated for the total number of scanned errors, as well as for each individual category of errors. A Laney adjustment was used to account for overdispersion in the data. We used a combination of linear regression, the 6 successively increasing or decreasing points rule, and the 8 consecutive points rule to assess trends and shifts in the data. The first 3 months of
error data were not included in the centerline/control limit calculations because they reflected a W&I system software and hardware training period.
The main process measure was to estimate the concordance between the numbers of bottles fed as reported from either W&I or from medical records. The number of scanned errors compared to the breast milk errors documented in the hospital event reporting system was also measured to determine if the number of voluntarily reported errors followed a similar pattern.
FIGURE 1
Current breast milk management and administration workfl ow, NCH. DBM, donor breast milk; MOMS, barcoding system (BCMA); PCA, patient care assistant; RN, registered nurse.
TABLE 1 Error Codes in the W&I System Identifi ed as Critical Errors
Error Category Human Milk Expiration Wrong Milk/Wrong Infant Human Milk Preparation W&I error message The bottle that you
selected has expired.
This bottle is assigned to another infant.
The bottle that you selected has already been thawed and cannot be refrozen. The bottle cannot be fed
to the infant as it is currently frozen.
The bottle is not from the mother of this infant.
You are attempting to combine fortifi ed and nonfortifi ed bottles. The bottle cannot be
received as it is already expired.
The item does not belong to the person.
You are attempting to combine bottles that have different fortifi cations. The bottle that you
Ethical Issues
This QI work involved implementing evidence-based interventions or best practices designed to reduce and ultimately eliminate human milk administration errors for neonates admitted to NCH neonatal services. Therefore, per human research protection program policy, this QI project was not considered human subjects’ research, and formal approval by the institutional review board was not required.
RESULTS
From 2009 to 2015, the most common scanning errors identified were due to expired milk, wrong-milk-to-wrong-infant, and
preparation errors, respectively ( Fig 2). During this time period, the total number of scanned errors declined from 97.1 errors per 1000 bottles to 10.8 ( Fig 2). Specifically, the number of expired milk error scans declined from 84.0 per 1000 bottles to 8.9. The number of preparation (4.8 per 1000 bottles to 2.2) and wrong-milk-to-wrong-infant errors scanned (8.3 per 1000 bottles to 2.0) also declined. These scanned error rates have been sustained through 2015. The first centerline shift was observed in June 2011, in conjunction with the implementation of bedside scanners ( Fig 3). The second shift was a continuous downward trend observed in 2012 after the implementation of a dedicated full-time milk technician. This trend was interrupted after only 5 points, but then continued after a small 1-point reversal. The application of linear regression to the entire 8-point slope from March 2012 to December 2012 (constrained at the end points to intersect the 2 flat stages, exactly as plotted) yielded a highly significant result (P < .001), making it clear that we do indeed have a valid downward trend. Therefore, we have plotted the centerline to conform accordingly (trend identification with regression
confirmation is built into our control charting tool, so this did not require separate analysis).
Control charts for each individual category of errors scanned indicate that the decrease in errors scanned related to expired milk was associated with the use of magnets on the outside of the breast milk refrigerators and the implementation of dedicated milk technicians
(Supplemental Figs 4–6). Similarly, the decrease in scanned milk
preparation errors was also primarily associated with the hiring of a milk technician. Finally, the decrease in scanned wrong milk errors was associated with the installation of bedside scanners.
In terms of process measures, we found ∼92% to 100% concordance between the number of bottles scanned (data directly from W&I) and the number of bottles fed (abstracted from medical records), indicating W&I is capturing the vast majority of bottles fed on a regular basis. We also examined the number of all documented breast milk errors in the hospital event reporting system to determine if the number
of voluntarily reported breast milk errors also declined. Although the event reporting system began before 2013, the W&I system was not fully implemented on all units administering breast milk until 2012. In 2013, data were categorized with more granularity to allow for more specific categorization of breast milk errors. We found that the number of voluntarily reported events also declined from 58 in 2013 to 29 in 2015.
DISCUSSION
We observed a decrease in the number of wrong milk errors scanned from 2009 to 2015. We also observed a decrease in the number of errors scanned related to breast milk expiration and preparation. Before the W&I system implementation, these errors were unrecognized. Declines in voluntarily reported breast milk errors during the same time period corresponded with the decreases in scanned errors. These decreases in scanned errors were primarily associated with 2 specific interventions: installation of bedside scanners and hiring of staff dedicated
FIGURE 2
to handle milk. Although examining scanned errors does not explicitly indicate a reduction in actual errors, such data indicate reductions in opportunities for actual errors to occur.
Current recommendations and reports of best practices suggest that centralized handling and use of barcode scanning improve human milk patient safety 23, 24 and
contribute to time and cost savings. 12
Thus, our interventions followed these recommended best practices. For example, hiring dedicated staff to handle milk was associated with decreases in milk preparation and expiration scanned errors. Similarly, installation of bedside scanners was associated with decreases in wrong milk errors. Both of these
interventions highlight the need to effectively implement change(s) into the workflow of the unit.
Barcoding is recommended by the Institute of Medicine as a safety intervention and “proactive approach” to prevent problems with patient identification. 25 The Joint
Commission also lists barcoding as a way to meet National Patient Safety Goal 1. 26 In response to
these recommendations, BCMA systems are applicable to breast milk because breast milk is considered medicine. 14 Others have shown
that BCMA systems for human milk reduce wrong milk errors. 17, 24, 27
As our study and other studies have demonstrated, 24 BCMA
has highlighted new, previously unmonitored scanned errors, such
as the potential for feeding expired milk 24 or incorrectly prepared milk.
As with medications, attention must be paid to the expiration date on human milk. 28 With every freeze/
thaw cycle of milk processing, some of the protective properties (such as antibodies) are destroyed, increasing the susceptibility of contamination, overgrowth of harmful bacteria, and risk of infection. 29 As a result,
NICUs must follow conservative shelf-life recommendations to protect their immune-compromised patients. Moreover, incorrect milk preparation, such as combining bottles that have already been fortified, has the potential to expose infants to inappropriate micronutrient concentrations that can cause harm. 30–33
FIGURE 3
A risk of BCMA systems is the potential to develop work-arounds to circumvent the system and bypass safety features. 28 For example,
to facilitate the patient scanning process, staff may place a patient’s printed ID band on a report sheet and scan it instead of the band attached to the patient. Most nurses manage >1 patient at a time, and thus, by not scanning the infant ID band attached to the patient, they risk scanning the wrong patient band. A second example is the ease of skipping the disposal step for expired milk. If an expired bottle is scanned, an error appears on the screen. This should be a hard stop to additional milk preparation and feeding. Ideally, the expired bottle should be disposed before scanning a new bottle for feeding. However, after an expired error is logged, the system does not force disposal of the expired milk. These occurrences of expired milk are monitored and manually reviewed by nursing staff to determine if the proper procedures were followed.
The generalizability of this study is limited, because not all NICUs have a BCMA. The expense associated with implementing a human milk BCMA may be more appropriate for larger units and systems such as ours. Costs associated with the human milk BCMA include software, hardware, and staff time. Conservatively, the initial costs of a human milk BCMA system for a small- to mid-sized NICU could range from $100 000 to $200 000 with an additional $50 000 to $100 000 annually for ongoing support.
The success of this initiative was also influenced by the culture of safety established at NCH in 2009 with the implementation of our “Zero Hero” program to eliminate preventable patient harm. 20, 34
Because the implementation of this safety program preceded the implementation of W&I system, the
clinical staff were already focused on QI and patient safety.
Although we observed a decrease in the scanned human milk error rate, our rate is not 0. Recently, we have begun tracking errors specific to donor breast milk. The local human milk bank implemented the same BCMA technology used by NCH. This allows seamless use of donor milk bottles. Additionally, the W&I system is used not only on our main campus (the focus of this study) but also in the satellite nurseries/NICUs that are managed by NCH in birth hospitals throughout Columbus, Ohio. Error rates at these satellite units have not yet been examined. Finally, NCH has plans to integrate feed orders from the electronic medical record into the W&I system. This integration would allow the milk technicians to have the information for bottle preparation (eg, fortification) within W&I, eliminating the need to manually look up each patient’s feed orders in the medical record (which is our current process).
By reporting human milk errors, an uncommon practice in hospitals, 16, 27, 28
and the strategies to reduce them, our study brings transparency in sharing data to improve outcomes. Sharing data between institutions (“all teach, all learn”) can facilitate rapid spread of best practices, potentially achieving optimal outcomes more quickly. 35 Without a
thorough understanding of the rates of human milk errors, and which human milk errors are occurring at which point(s) in the process, strategies to prevent harm are difficult to implement.
CONCLUSIONS
We have shown a decrease in the number of scanned human milk administration errors after a series of interventions. However, errors still occur. Thus, additional efforts are needed to additionally reduce the scanned error rate to ultimately
eliminate errors. With human milk feeding increasing among infants admitted to the NICU, volumes of milk will continue to increase as will opportunities for errors. Patients and families should be able to trust the proper handling and administration of this aspect of medical care. Thus, continued efforts are needed to improve and disseminate successful strategies to ultimately eliminate human milk administration errors.
ACKNOWLEDGMENTS
We thank Thomas Bartman, MD, PhD, Vicky L. Armstrong, RN, MSN, Christine Smith, BA, RN, IBCLC, ANLC, Margaret R. Holston, RN, BSN, and Margot Ranney, RN, for their support and participation in the initial QI efforts related to this project. We also thank T. Arthur Wheeler, MS, MSES, MBA, for statistical assistance and Andrew Gilleon, BSECE, and Nicholas Foor for assistance accessing data.
ABBREVIATIONS
BCMA: barcode medication administration system EBM: expressed human/breast
milk
NCH: Nationwide Children’s Hospital
QI: quality improvement W&I: Women and Infants
REFERENCES
1. Eidelman AI, Schanler RJ, Johnston M, et al; Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics. 2012;129(3). Available at: www. pediatrics. org/ cgi/ content/ full/ 129/ 3/ e827
2. World Health Organization. Health topics: breastfeeding. Available at: www. who. int/ topics/ breastfeeding/ en/ . Accessed May 28, 2015
2020/ default. aspx. Accessed November 7, 2012
4. Cavell B. Gastric emptying in infants fed human milk or infant formula. Acta Paediatr Scand. 1981;70(5):639–641
5. Furman L, Taylor G, Minich N, Hack M. The effect of maternal milk on neonatal morbidity of very low-birth-weight infants. Arch Pediatr Adolesc Med. 2003;157(1):66–71
6. Lucas A, Cole TJ. Breast milk and neonatal necrotising enterocolitis.
Lancet. 1990;336(8730):1519–1523
7. O’Connor DL, Jacobs J, Hall R, et al. Growth and development of premature infants fed predominantly human milk, predominantly premature infant formula, or a combination of human milk and premature formula. J Pediatr Gastroenterol Nutr. 2003;37(4):437–446
8. Ip S, Chung MGR, Chew P, et al.
Breastfeeding and Maternal and Infant Health Outcomes in Developed Countries. Rockville, MD: US Agency for Healthcare Research and Quality; 2007
9. Centers for Disease Control and Prevention. Breastfeeding report card, 2013. Available at: www. cdc. gov/ breastfeeding/ pdf/ 2013breastfeeding reportcard. pdf. Accessed March 19, 2015
10. Centers for Disease Control and Prevention. Progress in increasing breastfeeding and reducing racial/ ethnic differences - United States, 2000-2008 births. MMWR Morb Mortal Wkly Rep. 2013;62(5):77–80
11. Kachoria R, Oza-Frank R. Trends in breastfeeding initiation in the NICU by gestational age in Ohio, 2006-2012.
Birth. 2015;42(1):56–61
12. Steele C, Czerwin A, Bixby C. Breast milk bar code scanning results in time savings and staff effi ciency. J Acad Nutr Diet. 2015;115(1):23–26
13. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285(16):2114–2120
14. Rodriguez NA, Miracle DJ, Meier PP. Sharing the science on human milk feedings with mothers of
very-low-birth-weight infants. J Obstet Gynecol Neonatal Nurs. 2005;34(1):109–119
15. Miller MR, Robinson KA, Lubomski LH, Rinke ML, Pronovost PJ. Medication errors in paediatric care: a systematic review of epidemiology and an evaluation of evidence supporting reduction strategy recommendations. Qual Saf Health Care. 2007;16(2):116–126
16. Drenckpohl D, Bowers L, Cooper H. Use of the six sigma methodology to reduce incidence of breast milk administration errors in the NICU.
Neonatal Netw. 2007;26(3):161–166
17. Wolford SR, Smith C, Harrison ML. A retrospective two year study of breast milk error prevention in the neonatal intensive care unit. Neonatal Intensive Care. 2013;26(2):41–42
18. Oza-Frank R, Bhatia A, Smith C. Combined peer counselor and lactation consultant support increases breastfeeding in the NICU. Breastfeed Med. 2013;8(6):509–510
19. Oza-Frank R, Bhatia A, Smith C. Impact of peer counselors on breastfeeding outcomes in a nondelivery NICU setting.
Adv Neonatal Care. 2014;14(4):E1–E8
20. Brilli RJ, McClead RE Jr, Crandall WV, et al. A comprehensive patient safety program can signifi cantly reduce preventable harm, associated costs, and hospital mortality. J Pediatr. 2013;163(6):1638–1645
21. Revere L, Black K. Integrating Six Sigma with total quality management: a case example for measuring medication errors. J Health Manag. 2003;48(6):377–391; discussion 392
22. Tech Briefs. Performing failure mode and effect analysis. Available at: www. techbriefs. com/ component/ content/ article/ 1097- et/ applications/ 6134- 15122- 403? limitstart= 0. Accessed June 10, 2015
23. Robbins ST, Meyers R. Infant Feedings: Guidelines for Preparation of Human Milk and Formula in Health Care Facilities. 2nd ed. Chicago, IL: American Dietetic Association; 2011
24. Steele C, Bixby C. Centralized breastmilk handling and bar code scanning improve safety and reduce breastmilk administration errors.
Breastfeed Med. 2014;9(9):426–429
25. Kohn LT, Corrigan JM, Donaldson MS.
To Err Is Human: Building a Safer Health System. Washington, DC: The National Academies Press; 2000
26. The Joint Commission. Standards FAQ details: two patient identifi ers - NPSG - goal 1 - 01.01.01. Available at: www. jointcommission. org/ standards_ information/ jcfaqdetails. aspx? StandardsFaqId= 750#x26ProgramId= 46. Accessed December 7, 2015
27. Dougherty D, Nash A. Bar coding from breast to baby: a comprehensive breast milk management system for the NICU. Neonatal Netw. 2009;28(5):321–328
28. Fleischman EK. Innovative application of bar coding technology to breast milk administration. J Perinat Neonatal Nurs. 2013;27(2):145–150
29. Cossey V, Jeurissen A, Thelissen MJ, Vanhole C, Schuermans A. Expressed breast milk on a neonatal unit: a hazard analysis and critical control points approach. Am J Infect Control. 2011;39(10):832–838
30. Rao R, Georgieff MK. Iron therapy for preterm infants. Clin Perinatol. 2009;36(1):27–42
31. Holick MF, Shao Q, Liu WW, Chen TC. The vitamin D content of fortifi ed milk and infant formula. N Engl J Med. 1992;326(18):1178–1181
32. Botash AS, Nasca J, Dubowy R, Weinberger HL, Oliphant M. Zinc-induced copper defi ciency in an infant.
Am J Dis Child. 1992;146(6):709–711
33. Penniston KL, Tanumihardjo SA. The acute and chronic toxic effects of vitamin A. Am J Clin Nutr. 2006;83(2):191–201
34. Brilli RJ, Allen S, Davis JT. Revisiting the quality chasm. Pediatrics. 2014;133(5):763–765
DOI: 10.1542/peds.2015-4451 originally published online January 11, 2017;
2017;139;
Pediatrics
Richard E. McClead Jr
Reena Oza-Frank, Rashmi Kachoria, James Dail, Jasmine Green, Krista Walls and
A Quality Improvement Project to Decrease Human Milk Errors in the NICU
Services
Updated Information &
http://pediatrics.aappublications.org/content/139/2/e20154451 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/139/2/e20154451#BIBL This article cites 27 articles, 5 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/breastfeeding_sub
Breastfeeding
http://www.aappublications.org/cgi/collection/nutrition_sub
Nutrition
sub
http://www.aappublications.org/cgi/collection/quality_improvement_
Quality Improvement
_management_sub
http://www.aappublications.org/cgi/collection/administration:practice
Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2015-4451 originally published online January 11, 2017;
2017;139;
Pediatrics
Richard E. McClead Jr
Reena Oza-Frank, Rashmi Kachoria, James Dail, Jasmine Green, Krista Walls and
A Quality Improvement Project to Decrease Human Milk Errors in the NICU
http://pediatrics.aappublications.org/content/139/2/e20154451
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2017/01/09/peds.2015-4451.DCSupplemental Data Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.