Jharna Ghosh IJSRE Volume 06 Issue 02 February 2018 Page 7847 Volume||6||Issue||02||February-2018||Pages-7847-7857||ISSN(e):2321-7545 Website: http://jsae.in
Index Copernicus Value- 76.10 DOI: http://dx.doi.org/10.18535/ijsre/v6i2.07
Effectiveness of Slow breathing relaxation exercise in controlling pain during early
mobilisation among CABG patients in a selected hospital, kolkata, WB.
Authors
Jharna Ghosh
Associate Prof. Woodlands college of Nursing,,Kolkata
ABSTRACT
The investigator conducted a study to assess “Effectiveness of Slow Breathing Relaxation Exercise in controlling pain during early mobilization among CABG patients in a selected hospital, Kolkata, West Bengal”. The objective of the study is to assess the pain with or without practising slow breathing relaxation exercise during early mobilization among CABG patients and to determine the association between pain score and selected variables among experimental and control group. The investigator adopted purposive research sampling technique with time-series research design. The total sample size was 60 – having 30 in each of experimental and control group. Here the investigator used two tools for data collection – selected variables and universal pain scale (simple descriptive numerical pain scale) to assess pain score. The data were analyzed using both descriptive and inferential statistics. Investigator found that the mean pain score of experimental group reduced gradually after practising slow breathing relaxation exercise during different stages of mobilization (rest, sitting, standing and walking) as opposed to the control group. The findings of the study revealed that the „t‟ value was not significant before mobilization i.e.at rest (1.78) but was significant at sitting (2.58), at standing (10.37) and at walking (27.20) step of mobilization at 0.05 level of significance. Therefore effectiveness of slow breathing relaxation exercise in controlling pain during early mobilization is established. The findings of the study have implications on nursing education, administration, practice and in research.
BACKGROUND OF STUDY
The incidence, prevalence, morbidity and mortality from coronary artery disease (CAD) among Asian Indians have been reported to be higher than among Europeans, Americans and other Asians, irrespective of whether they live in India or abroad. In 2010, of all projected worldwide deaths, 23 million are expected to
be because of cardiovascular diseases.6
Every year, some 427,000 patients in the United States have coronary artery bypass graft surgery (CABG) Whether the surgery is done with the patient on or off the cardiopulmonary bypass (CPB) machine.
India is experiencing a rapid health transition with rising burden of Non-Communicable Diseases. According to WHO report (2002) cardiovascular disease (CVDs) will be the largest cause of death and
disability in India by 2020 and is expected to affect over 65 million Indians by 2015.7
OBJECTIVES OF THE STUDY
To assess the Pain with practicing slow breathing relaxation exercise during early mobilization of patients who have undergone CABG in experimental group at
Jharna Ghosh IJSRE Volume 06 Issue 02 February 2018 Page 7848
Sitting
Standing
Walking
To assess the Pain without practicing slow breathing relaxation exercise during early mobilization of
patients who have undergone CABG in control group at
Rest
Sitting
Standing
Walking
To find out the effectiveness of breathing exercise in terms of reduction of pain in experimental group.
To determine the association between pain score and selected demographic variables in experimental
and control group.
HYPOTHESES:
H1 –The mean pain score of CABG patients who practice slow breathing relaxation exercise during
mobilization is lower than those who do not practice at 0.05 level of significance.
H2 - There is significant association between pain score and the selected variables in experimental group
and control group at 0.05 level of significance.
VARIABLES:
Dependant Variables: pain- score
Independent Variable: Slow breathing relaxation exercise
RESEARCH METHODOLOGY Research approach
Quasi Experimental approach
RESEARCH DESIGN
Quasi – experimental time series design
Experimental group: R E -- O1xO2xO3x O4
20 mins (O 1 =pain score at rest
O2=pain Score at sitting,
O3=pain score at standing,
O4 = Pain score at walking)
X= treatment; Slow breathing relaxation exercise for 2- 3 minutes before each step of mobilization)
Control group: RC-- O5-O6-O7- O8
20 mins (O5 =pain score at rest,
O6=pain score atsitting,
Jharna Ghosh IJSRE Volume 06 Issue 02 February 2018 Page 7849
O8 = pain score at walking)
(--)= No treatment given to control group before each step of mobilization
Tool and Techniques for Data Collection
Table-2
Data collection Tools and Techniques
S/L NO Tools Variables Techniques
Tool -1
Tool -2
Demographic profile
Demographic data Illness data
Pain scale (Simple descriptive numerical pain scale)
Age, sex, and, education, occupation
Duration of illness, type of CABG, Site of graft taken, no. of graft taken, no. of pacing wire, No. of chest drain, No. of
invasive lines was
present, day of Extubation, and no. of wounds
Pain score
Record analysis
Record analysis
Pain assessment
ANALYSIS OF DATA
Part A – Demographic characteristics of the samples N= 60
Figure- 2 : Distribution of Age of the samples
Data presents in the figure-2 highlights that among 60 samples, 2(3.33%) are in age group of 30-45 years, 35(38.33%) are in the age group of 46-60 years and 25(35.33%) are in the age group of 61-75 years.
It has been observe that the majority of age distribution of the samples are within (46-60 year) where as very minor age distribution within (30-45 years)in both experimental and control group.
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00%
30 - 45 years 46 - 60 years 61 - 75 years
P
e
rcent
ag
e
Age Groups
Experimental
Jharna Ghosh IJSRE Volume 06 Issue 02 February 2018 Page 7850 Demographic characteristics of the samples
N=60
Figure-3: Distribution of sex of the sample
Data presented in the figure-3 highlights that, among 60 samples, male participants are majority in both experimental 29 (96.67%) and control 30 (100%) groups as compare to female 1 (3.33%).
It is observed that the incidents of ischaemic disease are higher among male than female.
Demographic characteristics of the samples
N = 60
Figure-4: Distribution of educationof thesamples
The data reveals in the figure-4 that, in terms of education majority 22 (73.33%) of participants in experimental group and 24 (80%) in control group are graduates whereas the secondary educational level 4 (13.33%) in experimental group and 2 (6.67%) in control group.
Demographic characteristics of the samples
Figure-5: Distribution of occupation of the sample
0.00% 20.00% 40.00% 60.00% 80.00% 100.00% 120.00%
Male Female
P
e
rcent
ag
e
Sex Types
Experimental
Control
0.00% 20.00% 40.00% 60.00% 80.00%
Secondary H.S. Graduate
P
e
rcent
ag
e
Education Levels
Experimental
Control
0.00% 10.00% 20.00% 30.00% 40.00% 50.00%
Service Business Retired
P
er
cent
ag
e
Occupation Types
Experimental
Jharna Ghosh IJSRE Volume 06 Issue 02 February 2018 Page 7851
According to occupation data, figure-5 represents that majority of participants are service holder in both groups 13(43.33%) equally, whereas least are retired persons 7(23.33%) in experimental group and businessman 7(23.33%) in control group.
Demographic characteristics of the samples Part B –Distribution of Illness data of the samples
N=60
Sample characteristics Experimental Group (N=30) Control Group (N=30)
Variable Values Frequency (f) Percentage (%) Frequency (f) Percentage (%)
Duration of Illness
< 1 year 5 17% 4 13%
1 - 2 years 7 23% 7 23%
> 2 years 18 60% 19 63%
Types of CABG On Pump 6 20% 5 17%
Off Pump 24 80% 25 83%
Sites of graft taken
Saphenous 29 97% 28 93%
Radial 5 17% 2 7%
Thoracic 24 80% 24 80%
No. of grafts taken
One 2 7% 2 7%
Two 7 23% 11 37%
Three 12 40% 12 40%
Four 9 30% 5 17%
No. of chest drains
One 2 7% 1 3%
Two 17 57% 22 73%
Three 11 37% 7 23%
No. of pacing wire
One 20 67% 18 60%
Two 10 33% 12 40%
Day of extubation 1st post-op 30 100% 30 100%
2nd post-op 0 0% 0 0%
No. of invasive lines
PAP 30 100% 30 100%
ABP 30 100% 30 100%
Peripheral Lines 30 100% 30 100%
Urinary Catheter 30 100% 30 100%
No. of wounds
Sternal side 30 100% 29 97%
Hand 5 17% 2 7%
Both legs 28 93% 29 97%
Data presented in table-3 highlights that majority of sample’s duration of illness more than 2years in compare to less than one year in both group.
According to type of CABG, majority of samples are under off pump CABG than on pump in both group. Table-4 reveals that most of the graft are taken from Saphenous-29(97%)in both group where as radial grafts are taken very least -5(17%) in experimental group and 1(3%) in control group.
Table-4 also shows that majority 30(100%) of wounds are from Sternal wounds in both groups whereas radial wounds were 5 (17%) in experimental and 1(3%) in control group.
Jharna Ghosh IJSRE Volume 06 Issue 02 February 2018 Page 7852
According to number of pacing wires, majority of the samples having one pacing wires 20(67%) in experimental group and 18(60%) in control group in compare to two pacing wire in both group 22(37%). The table-4 also highlights that number of invasive lines and day of extubation data are 100% equal in both experimental and control group.
Section-2
This section deals with the findings related to the difference of pain score between experimental group practicing slow breathing relaxation exercise and control group not practicing slow breathing relaxation exercise with 1st, 2nd, 3rd and 4th observation during early mobilization.
Findings related to MD, SD, un-paired ‘t’ test has been calculated between observed pain score at 1st, 2nd, 3rd
and 4th observation respectively.
To find out the difference in the pain score among CABG 3rd post operative day’s patients in experimental
and control group the following research and null hypothesis is stated.
H1 – The mean pain score of CABG patients who practice slow breathing relaxation exercise is lower than
those who do not practice during early mobilization at 0.05 level of significance.
H01-There is no significant difference in mean pain score of patients who practice slow breathing relaxation
exercise than those who do not practice during early mobilization at 0.05 level of significance
Findings related to MD, SD, un-paired ‘t’ test has been calculated between observed pain score at 1st, 2nd, 3rd
and 4th observation respectively.
N=60
Figure- 6 : Distribution of mean pain scores between experimental and control group during four step of mobilization.
The figure highlights the mean pain score of experimental group who practice slow breathing relaxation
exercise is lower than those who do not during four step of mobilization.
4.13
3.80
2.33
0.60
3.93 4.20
5.07
6.27
0.00 1.00 2.00 3.00 4.00 5.00 6.00 7.00
At Rest Sitting Standing Walking
Experimental
Jharna Ghosh IJSRE Volume 06 Issue 02 February 2018 Page 7853 Table-4
Mean, mean difference, standard deviation and ‘t’ value of pain score in experimental and control group
Un-paired ‘t’ value calculated between experimental group practicing slow breathing relaxation exercise and control group not practicing slow breathing relaxation exercise in respect of pain score with 1st, 2nd, 3rd and
4th observations among 3rd post operative CABG patients during early mobilization.
N=60
Step Observation Mean Pain
Score SD
Mean Difference
Standard
Error df
tabulated 't' value
Observed 't' value
1 At Rest
Experimental (O1) 4.13 0.72
0.20 0.20 58 2.00 1.01
Control (O5) 3.93 0.81
2 Sitting
Experimental (O2) 3.80 0.60
0.40 0.15 58 2.00 2.58 *
Control (O6) 4.20 0.60
3 Standing
Experimental (O3) 2.33 1.04
2.73 0.26 58 2.00 10.37 *
Control (O7) 5.07 1.00
4 Walking
Experimental (O4) 0.60 0.92
5.67 0.21 58 2.00 27.20 *
Control (O8) 6.27 0.68
df(58)= 2.00, p<= 0.05 df ( 58) =2.66 , p<= 0.01 * = Significant value
Data presented in the Table-5 shows that the difference of mean pain score (4.13) in experimental group than the mean pain score (3.93) in control group in 1st observation with mean difference (0.20) before intervention and mobilizationis not significant from ‘t’ value of 1.01 for df (58) at 0.05 level of significance. It is also reveals that the homogeneity of the samples.
In 2nd observations the mean pain score (3.80) in experimental group is lower than the mean pain score (4.20) in control group with mean difference (0.40) which is significant as evident from ‘ t’ value of 2.58for df (58) at 0.05 level of significance.
In 3rd observations mean pain score (2.33) in experimental group is lower than the mean pain score (5.07) in
control group with mean difference (2.73) which is significant as evident from ‘ t’ value of 10.37 for df (58) at 0.05 level of significance.
In 4th observation data shows the mean pain score (0.6) in experimental group is significantly lower than the
mean pain score (6.27) in control group with mean difference(5.67) which is very much significant as evident from ‘t’ value of (27.20) for df (58 ) at o.05 level of significance.
Thus it is concluded that obtained mean difference of pain score in 1st observation is not significant but in
2nd, 3rd and 4th observations between experimental and control group of CABG3rd post operative day’s patients during early mobilization after practicing slow breathing relaxation exercise is a true difference , not by chance. Therefore, null hypothesis is rejected andresearch hypothesis (H1) is accepted.
This indicates that practicing slow breathing relaxation exercise is effective in controlling pain during early
mobilization among CABG 3rd post operative day’s patients.
Section 3
Jharna Ghosh IJSRE Volume 06 Issue 02 February 2018 Page 7854 H2 - There is significant association between pain score and the selected demographic variables in experimental group and control group at 0.05 level of significance.
H02 - There is no significant association between pain score and the selected demographic variables in experimental group and controlat 0.05 level of significance
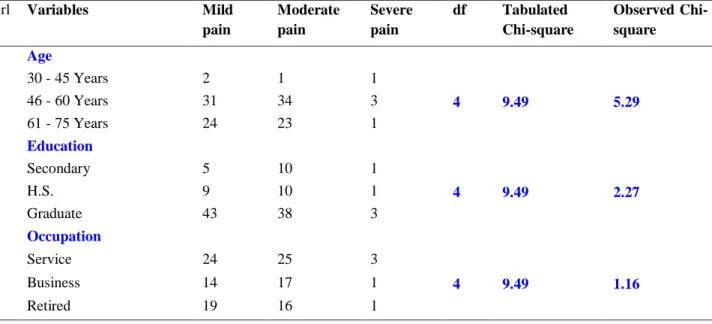
Table -5 Chi-square value between the pain score and selected demographic variables among experimental group.
n=30
X2 ( 4) = 9.49 , p<= 0.05
The data presented in the table 6 shows that the calculated chi-square value is lower than the table value in respect of age, education and occupation which is not found statistically significant at 0.05 level of significance.
No association is calculated for sex and pain score due to non-availability of female participants.
Table-5 ( cont.)- Chi- square value between the pain score and selected demographic variables among experimental group
n=30
Srl #
Variables Mild
pain
Moderate pain
Severe pain
df Chi-square
value
Chi-square value
4 Duration of Illness
< 1 Year 10 9 1
4 9.49 1.32
1 - 2 Years 14 12 2
> 2 Years 33 37 2
5 Type of CABG
On Pump 13 10 1
2 5.99 0.11
Off Pump 44 48 4
6 Site of grafts taken
Saphenous 55 56 5
4 9.49 0.41
Radial 10 9 1
Srl #
Variables Mild
pain
Moderate pain
Severe pain
df Tabulated
Chi-square
Observed Chi-square
1 Age
30 - 45 Years 2 1 1
4 9.49 5.29
46 - 60 Years 31 34 3
61 - 75 Years 24 23 1
2 Education
Secondary 5 10 1
4 9.49 2.27
H.S. 9 10 1
Graduate 43 38 3
3 Occupation
Service 24 25 3
4 9.49 1.16
Business 14 17 1
Jharna Ghosh IJSRE Volume 06 Issue 02 February 2018 Page 7855
Thoracic 44 49 3
7 Number of grafts taken
One 6 1 1
6 12.59 1.74
Two 13 13 2
Three 24 27 1
Four 14 17 1
8 Number of chest drains
One 4 3 1
4 9.49 0.34
Two 33 33 2
Three 20 22 2
9 Number of pacing wire
One 37 35 4
2 5.99 0.56
Two 20 23 1
10 Number of wounds
Sternal 57 58 5
4 9.49 0.53
Hand 10 9 1
Legs 55 58 3
X2 ( 4) = 9.49,X2 ( 2)= 5.9 9 , X2 ( 6)= 12.59, p<= 0.05
Data presented in the table 5 shows that there is no association with pain score and selected illness demographic variable as evident from table value and calculated value at 0.05 level of significance.
Hence null hypothesis H02 is accepted and research hypothesis H2 is rejected.
No chi-square association with number of invasive lines and day of extubation is done as there is no variation.
Table 6-Chi- square value between the pain score and selected demographic variables among control group n=30
Srl #
Variables Mild
pain
Moderate pain
Severe pain
df Chi-square
value
Chi-square value
1 Age
30 - 45 Years 1 1 2 4 9.49 7.62
46 - 60 Years 2 40 26
61 - 75 Years 1 24 23
2 Education
Secondary 1 6 5 4 9.49 1.54
H.S. 1 10 9
Graduate 2 49 37
3 Occupation
Service 2 34 20 4 9.49 2.05
Business 1 15 16
Retired 1 16 15
X2 ( 4) = 9.49 , p<= 0.05,
The data presented in the table 7 shows that there are no significant association between the pain score and selected demographic variables (age, sex, education and occupation) among control group as calculated chi-square value is lower than tabulated value at 0.05 level of significance.
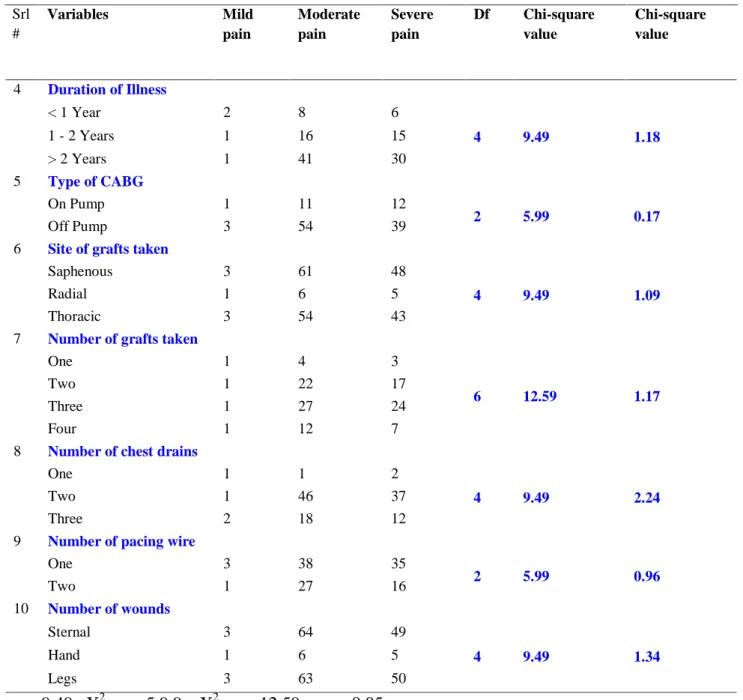
Jharna Ghosh IJSRE Volume 06 Issue 02 February 2018 Page 7856 Table 6 (Contd…) Chi-square value between the pain scores and selected illness demographic profiles among control group
n=30
Srl #
Variables Mild
pain
Moderate pain
Severe pain
Df Chi-square
value
Chi-square value
4 Duration of Illness
< 1 Year 2 8 6
4 9.49 1.18
1 - 2 Years 1 16 15
> 2 Years 1 41 30
5 Type of CABG
On Pump 1 11 12
2 5.99 0.17
Off Pump 3 54 39
6 Site of grafts taken
Saphenous 3 61 48
4 9.49 1.09
Radial 1 6 5
Thoracic 3 54 43
7 Number of grafts taken
One 1 4 3
6 12.59 1.17
Two 1 22 17
Three 1 27 24
Four 1 12 7
8 Number of chest drains
One 1 1 2
4 9.49 2.24
Two 1 46 37
Three 2 18 12
9 Number of pacing wire
One 3 38 35
2 5.99 0.96
Two 1 27 16
10 Number of wounds
Sternal 3 64 49
4 9.49 1.34
Hand 1 6 5
Legs 3 63 50
X2 ( 4) = 9.49, X2 ( 2) = 5.9 9 , X2 ( 6) = 12.59 , p<= 0.05
Data presented in the table 7 shows that there are no association with pain score and selected illness demographic variable as evident from table value and calculated value at 0.05 level of significance. Hence null hypothesis (H02) is accepted and research hypothesis (H2) is rejected.
No chi-square association with number of invasive lines and day of extubation is done with pain score as there is no variation.
CONCLUSIONS:
From the study findings it was concluded that:
The slow breathing relaxation exercise is helpful in controlling pain during early mobilization among
patients having undergone coronary artery bypass surgery .
Jharna Ghosh IJSRE Volume 06 Issue 02 February 2018 Page 7857 REFERENCE:
1. Asian Journal of Cardiovascular Nursing.Nayak S. Baby.Identify the risk factors and effectiveness of
pulmonary rehabilitation.2009. June; vol-17.No-2
2. Lewis MS(2001) Medical Surgical Nursing for clinical management.5th ed. Baltimore.Philadephia
3. Bruner& Suddharth. Medical Surgical Nursing. 11th edition. Kluwer& Kluwer publication.New Delhi
4. Black.J.M. and Jacob M K (1997) .Medical Surgical Nursing.5th edition. Baltimore. Philadelphia
5. Potter Patrica C. Perry . Fundamental of Nursing 6th edition. St.laws. Mosby publication
6. Asian Journal of Cardiovascular Nursing. Chatterjee Nirmalya..Cardiovascular disorder in India.
2012. June; vol-20 .No-2
7. WHO. Cardiovascular disease: Prevention and Control. Available at
http//:www.google/WHO/CVD.htm.Accessed December.2012
8. K. park. Text Book of Social Medicine. 20th edition. Baranashidas publication.New delhi
9. Soler. et aI.( 20I0). Post operative patients on efficacy of pain management with drug. Available at
http://scholar.google.co.in/scholar?q=Soler.et.al+2010+post+operative+pain+management+with+dru g
10.Louise Rose.et al (2011).Survey of assessment and management of paon for critically ill adults.
11.Polit and Hungler. Nursing research principles and methods. 6th edition. Philadelphia. Lippincott.
12.Basavan Thappa B T. Nursing Theories. 1st ed. New Delhi. Jypee publication
13.R Narang, N Bordoloi. Relationship between CAD calcification score using Cine Fluroscopy and
Exercise stress test.available at http:// www.pubmed/ relaxation techniques.htm
14.Lauri Barclay. Off-pump CABG as safe as on-pump but has higher revascularization rates.Availabe
at http://www.medscape.com/medical_news.htm