Left Main Protection During very High
Risk Transcatheter Aortic Valve-in-Valve
Procedure. A Collaborative Registry
Luca Testa
1, Tarun Chakravarty
2, Azeem Latib
3, Fausto Castriota
4, Montone RA
1,
Alberto Cremonesi
4, Antonio Colombo
3, Raj Makkar
2, Francesco Bedogni
11 Ist. Clinico S. Ambrogio, Milan, Italy
2 Cedars-Sinai Heart Institute, Cedars-Sinai Medical Center, Los Angeles, California, USA 3 San Raffaele Hospital, Milan, Italy
4 GVM Care and Research, Maria Cecilia Hospital, Cotignola, Italy
Corresponding author: Dr. Luca Testa, MD, PhD Dept. of Interventional Cardiology, Ist. Clinico S. Ambrogio, Milan, Italy E-mail: [email protected]
Introduction
Surgical aortic valve replacement (SAVR) had a substantial shift toward the use of bio-prostheses rather than mechanical valves.1 Unfortunately bio-prostheses have limited durability, and most are expected to degenerate and eventually fail within 10 to 20 years1. As a result, many patients will suffer from degenerated surgical bio-prosthetic valves. A redo SAVR is often a high-risk procedure that carries significant mortality and morbidity risks, especially because these patients are elderly and have numerous comorbidities2.
Transcatheter aortic valve replacement (TAVR) proved to be an alternative to SAVR for the treatment of severe
symptomatic native aortic valve stenosis in patients at a high or prohibitive surgical risk.3,4 Moreover, several reports have suggested that the use of TAVR for failed surgical aortic bio-prostheses (“valve-in-valve”, TAVR-VIV) is technically feasible5,6,7.
However, surgical bioprostheses have different characteristics. In particular, those included in the present registry pose a higher risk of left main obstruction, as a consequence of very specific features including tall and externally mounted leaflets as well as a relatively high bioprosthesis implant (slightly supra-annular) (Figure 1).
ISSN: 2410-2636 © Barcaray Publishing * Corresponding author. E-mail: [email protected]
Abstract
Background
Surgically implanted aortic bio-prostheses are prone to degeneration and eventually failure within 10 to 20 years. Transcatheter aortic valve replacement “valve-in-valve” (TAVR-VIV) is an effective treatment for patients deemed at prohibitive risk for surgical redo. However, Mitroflow, Freedom, Toronto and Freestyle bioprostheses pose a high risk of left main obstruction and are only marginally represented in the available literature.
Methods and Results
After evaluation of local Heart Team, TAVR-VIV implantation was performed in 20 patients with a failed Mitroflow (8), Freedom (5), Toronto SPV (3), Freestyle (2), Trifecta (1), or Mosaic (1) bioprostheses. Patients/prostheses were divided in type A (mainly stenotic, 8 pts), and type B (mainly regurgitant, 12 pts). All patients were managed protecting the left main ostium.
At 30 days, 2 fatalities (10%) and 2 myocardial infarction (10%) occurred. At a mean follow up of 6 months, 2 further fatalities (cumulative survival rate of 80%) were observed (cumulative incidence of 5%).
Conclusions
This registry specifically focusing on extremely high risk TAVR-VIV is a proof of concept. The protection of the left main during the procedure allows patients initially deemed at highest or even prohibitive risk to be successfully treated and further support the use of bioprostheses at the time of the surgical treatment.
Keywords: degenerated aortic bioprosthesis, valve in valve, left main occlusion.
Citation: Testa L, Chakravarty T, Latib A et. al. Left Main protection during very high risk Transcatheter Aortic Valve-in-Valve procedure. A Collaborative Registry. International Cardiovascular Forum Journal.
2016;6:29-35. http://dx.doi.org/10.17987/icfj.v6i0.169
Figure 1. The Sorin Pericarbon Freedom™ stentless valve (Sorin Group, Saluggia, Italy) is a truly stentless valve formed from two sheets of bovine pericardium. It is available since 1994. The Mitroflow Aortic Pericardial Heart Valve™ consists of a single piece of bovine pericardium that is preserved with glutaraldehyde and sewn onto a polyester covered polymer stent. A radiopaque, silicone sewing ring is attached to the outer perimeter of the inflow side of the valve. The Freestyle Valve (Medtronic Inc, Minneapolis, MN, USA) is a stentless bioprosthesis remarkably similar to a native valve in terms of hemodynamic features. Toronto SPV™ bioprosthetic aortic valve (St. Jude Medical, Inc., St. Paul, MN, USA) is a stentless bioprosthesis. To perform the implantation, an incision has to be done at least 1 cm above the native sinotubular edge, and the native valve must be excised. Thus the native aortic wall is sutured to the bioprosthetic valve, and the aorta resewn. The Mosaic Tissue Valve (Medtronic Inc, Minneapolis, MN, USA) is a porcine derived stentless valve. Leaflets are secured to a flexible stent, covered by a fine fabric intended to facilitate the suture.The Trifecta Valve (St. Jude Medical, Inc., St. Paul, MN, USA) is a stented bioprosthesis in which leaflets are manufactured using bovine pericardial tissue.All these valves are designed for subcoronary, slightly suprannular implantation using interrupted or continuous suture techniques at the inflow side.
Previous experience, reported an ostial coronary obstruction rate in 7.7% of the Mitroflow cases and in 50% of the Freedom 7. We thus report on a multicenter registry of TAVR-VIV implantation for these highest risk degenerated bio-prostheses. Moreover, we hereby describe the technique of Left Main (LM) protection that has been implemented to avoid the LM acute occlusion.
Methods
Patients
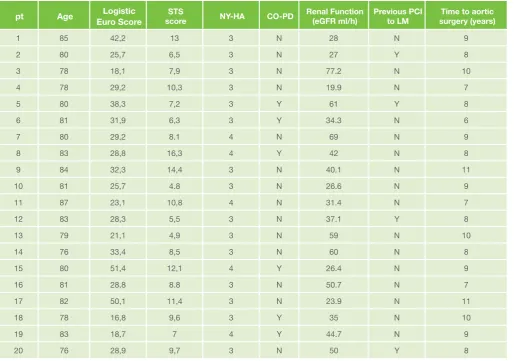
Twenty patients with degenerated Mitroflow, Freedom, Toronto or Freestyle bioprostheses have been included in the present registry and prospectively followed up (Table 1). Before the procedure a collegial evaluation of the “heart team” including cardiologists, interventional cardiologists, anesthesiologist and cardiac surgeons was made to determine surgical eligibility. Clinical criteria for high risk were considered: age ≥ 75 years, coronary artery disease, malignancy, hepatic cirrhosis, frailty, chronic obstructive pulmonary disease, severe pulmonary hypertension, porcelain aorta, low ejection fraction, diabetes, renal failure, peripheral obstructive artery disease. Logistic Euroscore and STS score were calculated.
At the time of enrolment, all patients had symptomatic heart failure (NYHA class III-IV), despite intensive medical therapy. Echocardiographic criteria for bioprosthesis dysfunction were:
aortic valve area < 1 cm2 and/or aortic regurgitation grade > 3. Use of transthoracic or transesophageal echocardiogram was left to the common practice of the enrolling center. Use of 3D echo was discretional.
Once a consensus over the therapeutic approach and informed written consent were obtained, the evaluation of the patient was performed to select the vascular access and to assess the presence of coronary artery disease. Where indicated percutaneous coronary revascularization was performed before TAVI.
General Procedures
The choice of third generation 18-Fr CoreValve Revalving System™ (Medtronic, Minneapolis, MN, USA), Edwards Sapien or Sapien XT implantation was left to operator discretion as well as the arterial access selection. General anesthesia or sedation was left to the anesthesiologist’s discretion. A temporary pacemaker was positioned in all patients in the absence of a previous permanent one. Transcatheter prosthesis size was chosen according to nominal internal diameter of the failed bioprosthesis and double checked with the mobile app available at www.europcr. com. (http://www.pcronline.com/About/2014/Valve-Atlas-app). Transthoracic echocardiography was performed post-procedure and at hospital discharge. Clinical follow-up evaluation was performed at 30 days, 3 and 6 months, then yearly. A CT scan has been performed in all cases as a routine work up in order to evaluate the arterial accesses as well as the anatomy of the aortic root with specific focus on the height of the LM and the size of the left cusp: cases in which the LM height was below 10 mm were considered at highest risk of LM occlusion, in particular in the presence of a relatively small aortic root. Double antiplatelet therapy was administered in all patients. ASA was continued indefinitely and clopidogrel (75 mg/day) for the following 6 months. For patients previously treated with percutaneous coronary intervention, dual antiplatelet therapy was continued as planned.
Left Main protection technique
left to operators discretion although in all cases a half dose of unfractioned heparin, according to weight and renal function, was administered after positioning the smaller sheath, while the full dose was reached after positioning the 18-F sheath.
Figure 2. Case example. Top left panel: aortogram showing the very shallow LM ostium with respect to the radiopaque ring of a Mitroflow 21 bioprosthesis. Top mid panel: guiding catheter and
2 intracoronary wires (LAD and LCx). Top right panel: first step of CRS deployment. Bottom left panel: left coronary angiogram showing the patency of the LM. Bottom right panel: once the guiding catheter has been taken out, aortogram still shows the patency of the LM. CRS: CoreValve Revalvyng System; LAD: left anteriore descending; LCx: left circumflex; LM: left main.
Definitions
From a clinical point of view patients have been selected according to the criteria listed above. From an angiographic/ imaging point of view, patients having an aortic bioprosthesis with tall and externally mounted leaflets as well as a relatively high implant or even supraannular, such as (Mitroflow, Freedom, Toronto SPV, Freestyle, Trifecta, Mosaic) were deemed at highest risk when the LM height was <10mm.
The criteria of the American Society of Echocardiography were used to assess the mechanism of failure of the bioprosthetic valve (9). A certain degree of both stenosis and regurgitation was always present, “Combined Stenosis-Regurgitation”, however, patients were categorized according to the predominant mechanism of failure, either in the “Stenosis” group or in the “Regurgitation” group. End point definitions were according to VARC-2 consensus document criteria 10. Safety as well as efficacy end points were recorded in hospital, at 30 days and at last follow up.
Table 1. Clinical characteristics at baseline
pt Age Euro ScoreLogistic scoreSTS NY-HA CO-PD Renal Function(eGFR ml/h) Previous PCI to LM surgery (years)Time to aortic
1 85 42,2 13 3 N 28 N 9
2 80 25,7 6,5 3 N 27 Y 8
3 78 18,1 7,9 3 N 77.2 N 10
4 78 29,2 10,3 3 N 19.9 N 7
5 80 38,3 7,2 3 Y 61 Y 8
6 81 31,9 6,3 3 Y 34.3 N 6
7 80 29,2 8.1 4 N 69 N 9
8 83 28,8 16,3 4 Y 42 N 8
9 84 32,3 14,4 3 N 40.1 N 11
10 81 25,7 4.8 3 N 26.6 N 9
11 87 23,1 10,8 4 N 31.4 N 7
12 83 28,3 5,5 3 N 37.1 Y 8
13 79 21,1 4,9 3 N 59 N 10
14 76 33,4 8,5 3 N 60 N 8
15 80 51,4 12,1 4 Y 26.4 N 9
16 81 28,8 8.8 3 N 50.7 N 7
17 82 50,1 11,4 3 N 23.9 N 11
18 78 16,8 9,6 3 Y 35 N 10
19 83 18,7 7 4 Y 44.7 N 9
20 76 28,9 9,7 3 N 50 Y 8
Statistical analysis
Numerical values are expressed as mean ± standard deviation. All reported probability values were 2-tailed, and p<0.05 considered statistically significant. Analyses were performed with the SPSS statistical software package (version 19).
Results
The baseline clinical characteristics of the patients are reported in Table 1. Eight patients had a predominantly stenosed degenerated bioprosthesis; the remaining 12, predominantly regurgitant. General anesthesia was chosen in 6 patients, deep sedation in the remaining 14. In all cases a percutaneous transfemoral approach was used and hemostasis obtained by means of Prostar XL10™ or 2 Proglide™.
CoreValve Revalving System™ (CRS) 26 mm was implanted in the majority of patients (n=12, 60%), CRS 23mm in 2 patients (10%), and Edwards Sapien/Sapien XT (ES) 23mm in the remaining cases (n=6, 30%). No patient needed a second implant.
Procedural outcome
Valve-in-valve implantation was successful with immediate restoration of satisfactory valve function in all patients.
However, in 4 cases [1 CRS 26 into a predominantly
regurgitant Pericarbon Freedom 21 (pt 11 in Table 2), another CRS 26 into a predominantly stenosed Pericarbon Freedom 21 (pt 16 in Table 2), a ES 23 into a predominantly regurgitant Mitroflow 21 (pt 2 in Table 2), and a ES 23 into a predominantly stenosed Toronto 21, pt 3 in Table 2), the deployment of a stent to the ostial LM was necessary to restore adequate flow. In these cases, a severe impairment of the flow through the LM was observed but not a total occlusion. Despite prompt intervention and stent deployment, two patients experienced a non Q-wave myocardial infarction and a longer stay in the intensive care unit. Common features of these patients were: small bioprosthesis with a relatively small aortic root, and a very shallow LM with a reduced size of the left Valsalva sinus. These two patients had a particularly shallow left main ostium, i.e. 11 mm. No procedural death occurred. No intra and periprocedural cerebrovascular events occurred. Two patients died (10%) during hospitalization. They were both admitted with severely regurgitant bioprosthesis (Freedom and Freestyle, respectively) and died from multi organ failure (see Table 3 for clinical events) although no complications occurred during the procedure. No cases of acute kidney injury were observed.
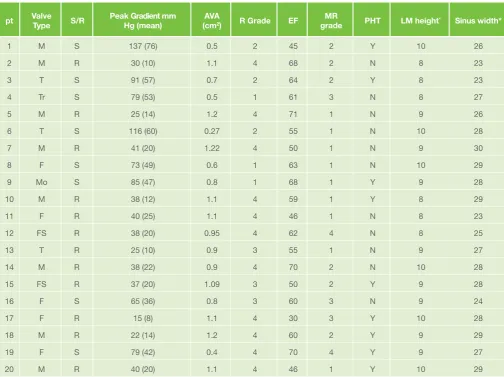
Table 2. Baseline anatomical characteristics
pt Valve Type S/R Peak Gradient mm Hg (mean) (cmAVA2) R Grade EF gradeMR PHT LM height* Sinus width*
1 M S 137 (76) 0.5 2 45 2 Y 10 26
2 M R 30 (10) 1.1 4 68 2 N 8 23
3 T S 91 (57) 0.7 2 64 2 Y 8 23
4 Tr S 79 (53) 0.5 1 61 3 N 8 27
5 M R 25 (14) 1.2 4 71 1 N 9 26
6 T S 116 (60) 0.27 2 55 1 N 10 28
7 M R 41 (20) 1.22 4 50 1 N 9 30
8 F S 73 (49) 0.6 1 63 1 N 10 29
9 Mo S 85 (47) 0.8 1 68 1 Y 9 28
10 M R 38 (12) 1.1 4 59 1 Y 8 29
11 F R 40 (25) 1.1 4 46 1 N 8 23
12 FS R 38 (20) 0.95 4 62 4 N 8 25
13 T R 25 (10) 0.9 3 55 1 N 9 27
14 M R 38 (22) 0.9 4 70 2 N 10 28
15 FS R 37 (20) 1.09 3 50 2 Y 9 28
16 F S 65 (36) 0.8 3 60 3 N 9 24
17 F R 15 (8) 1.1 4 30 3 Y 10 28
18 M R 22 (14) 1.2 4 60 2 Y 9 29
19 F S 79 (42) 0.4 4 70 4 Y 9 27
20 M R 40 (20) 1.1 4 46 1 Y 10 29
Table 3. Clinical Events (see text for definitions)
At 30 days
N (%) Cumulative event rate at last follow up N (%)
Death 2(10) 4 (20)
Myocardial infarction 2 (10) 2 (10)
Stroke 0 (0) 0 (0)
New onset renal failure 0 1 (5)
Definitive pacemaker 0 1 (5)
Echocardiographic findings post-TAVR
In patients with predominantly stenotic bioprosthesis, transaortic gradient significantly decreased from a mean of 90.6+24.09 mmHg to 19.6+4.07 mmhg (p<0.001), while the valve area increased from 0.57+0.1 to 1.6+0.2 (p=NS). Left ventricular ejection fraction did not significantly change before and after procedure. Post procedural regurgitation grade was mild in two cases (Table 4).Notably, in patients with predominantly regurgitant bioprosthesis, regurgitation grade post implantation was 1 or 2 in all cases. Ejection fraction did not significantly change (Table 4).
Follow up
At a mean follow up of 6 months (median 90 days), two further fatalities, as a consequence of severe respiratory insufficiency, and a pacemaker implantation for new complete AV block occurred. There were no additional strokes, myocardial infarcts, major bleeds or repeat valve interventions (Table 3). Echocardiographic parameters at last follow up showed a persistent good result after valve implantation (Table 4). New York Heart Association class at last follow up was 1-2 in all patients.
Discussion
The gold standard treatment for low and moderate risk severe aortic stenosis remains the surgical aortic valve replacement 11 and the valve of choice is often a bio-prosthesis, to avoid the risks associated with lifelong oral anticoagulation 12. With time, however, this advantage is offset by degeneration of the bio-prosthetic valve tissue, eventually resulting in the failure of bio-prostheses with either severe stenosis or valvular regurgitation 11. A surgical redo is often limited by a prohibitive risk of mortality and morbidity 13. In this scenario the use of transcatheter valves has shown to be highly successful with a very favorable risk-benefit profile 14, although there are some specific bioprostheses that have been associated with an extremely high risk of acute left main occlusion during the procedure. Of note, data specifically focusing on this population of patients/failed bioprostheses are extremely limited 15.
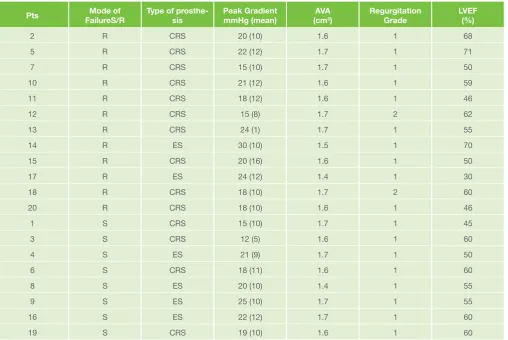
Table 4. Echocardiographic Characteristics at last follow up
Pts FailureS/RMode of Type of prosthe-sis Peak GradientmmHg (mean) (cmAVA2) RegurgitationGrade LVEF(%)
2 R CRS 20 (10) 1.6 1 68
5 R CRS 22 (12) 1.7 1 71
7 R CRS 15 (10) 1.7 1 50
10 R CRS 21 (12) 1.6 1 59
11 R CRS 18 (12) 1.6 1 46
12 R CRS 15 (8) 1.7 2 62
13 R CRS 24 (1) 1.7 1 55
14 R ES 30 (10) 1.5 1 70
15 R CRS 20 (16) 1.6 1 50
17 R ES 24 (12) 1.4 1 30
18 R CRS 18 (10) 1.7 2 60
20 R CRS 18 (10) 1.6 1 46
1 S CRS 15 (10) 1.7 1 45
3 S CRS 12 (5) 1.6 1 60
4 S ES 21 (9) 1.7 1 50
6 S CRS 18 (11) 1.6 1 60
8 S ES 20 (10) 1.4 1 55
9 S ES 25 (10) 1.7 1 55
16 S ES 22 (12) 1.7 1 60
19 S CRS 19 (10) 1.6 1 60
We hereby describe the results of a multicenter independent prospective registry in which patients presenting with a failed highest risk aortic bioprosthesis have been successfully treated with a simple technique of left main protection.
This precaution of positioning a guiding catheter and one or two intracoronary wires makes the valve in valve procedure feasible and effective [see figure 1], although in all but four cases [CRS 26 into a predominantly regurgitant Pericarbon Freedom 21, CRS 26 into a predominantly stenosed Pericarbon Freedom 21, a ES 26 into a predominantly regurgitant Mitroflow 21, and a ES 26 into a predominantly stenosed Toronto 21) an abrupt LM occlusion occurred and a rapid intervention was necessary to restore an adequate blood flow through the left main. The predisposition for this ominous complication is related to the spatial geometry of the surgical valve leaflets inside the aortic sinuses, i.e. it is a composite not only of the type of valve, but of the “virtual ring” of the post of the valve in relationship with the side of tubular junction, the sinuses, and the coronary orifices. In other words, the same valve in a large aortic root or with large sinuses or with high coronary ostia does not pose the same risk as a small calcified route with low coronary sinuses. In this scenario the different features, in particular the height of the external frame, of self-expandable bioprostheses as compared to the balloon expandable deserve a consideration. From one hand the taller frame may pose a higher risk of LM occlusion in a context of small sinuses/tubular junction and shallow coronary orifices, however, the possibility of a “fine tuning” before the final deployment or even the possibility to retrieve the bioprosthesis can be of great value. In the present registry we did not observe differences and the possible explanation relies on the experience of the participating centers that have chosen the prosthesis they are more confident with for the specific cases.
Those cases in which despite the protection an acute LM occlusion occurred share some common features, such as a small bioprosthesis, a small sinus width (<24 mm), and a very shallow LM (height of LM was 9 mm in 1 patient and 8 mm in the other 3 patients).
The presence of the catheter and the wire could be considered a sort of “safety net”: it does allow a prompt management of a possible flow impairment through the LM and it probably keeps the leaflet of the degenerated bioprosthesis far from the LM. The latter, however, could be only temporarily effective, as suggested by cases of delayed LM occlusion, i.e. once the catheter has been taken out15. In these cases, even the alternative approach of positioning an undeployed stent into the coronary bed, would be ineffective8.
Bioprostheses that showed the highest risk of left main occlusion share some technical features such as: tall and externally mounted valve leaflets and a relatively high implant (slightly supraannular). The mode of degeneration seems to have no impact on the risk of LM occlusion. On the other hand, it has been suggested that a severely stenotic degenerated bioprosthesis is associated with a worse outcome as compared to a regurgitant one 14. Thus, a clear knowledge of the technical features of the degenerated bioprosthesis is mandatory to plan the procedure. Information regarding the height of the leaflet, the height of the coronary ostia, the inner and outer dimensions of the prosthesis must be clearly addressed and, for those information that cannot be retrieved by the manufacturer’s Instruction For Use, a Computed Tomography is mandatory to complete the pre-procedural work up.
Nonetheless, even with a complete collection of available information, including the mode of degeneration,
echocardiographic and CT-scan parameters, bioprosthesis size, valve position with respect to the aortic annulus, and valve type (stented vs. stentless), the VIV procedure remains technically demanding.
Of note, there are some key points that should always be considered6. The use of transesophageal echocardiography (TEE), particularly when dealing with a stentless valve, can be of great value. However, the majority of the cases is nowadays done in mild sedation rather than in general anesthesia, thus the implementation of TEE could be limited in favor of a less invasive approach, considering that a rapid conversion to open heart surgery is actually anecdotic11.
The predilation should be avoided in cases of severe regurgitation and considered only when crossing a severely stenotic bioprosthesis is impossible. On the other hand, in some cases, a post dilation is needed. The issue of advanced Atrio Ventricular block and subsequent Pace Maker implantation is less relevant as compared to the setting of native aortic valve stenosis6, as well as the incidence of permanent left bundle branch block17.
No large scale randomized controlled trial comparing redo SAVR and VIV in patients with failed bioprostheses have been done. Data coming from a recent European Database show that the rate of major complications after surgical redo is still high, thus supporting the VIV as a concrete alternative in patients in which there is a reasonable chance to obtain a good procedural result and a favorable impact at least on the quality of life18. Limitation of the present study.
This is not a randomized controlled trial, thus there is no direct comparator to the strategy that has been tested. The chance of a selection bias is high as the criteria of highest risk are mainly based on a very limited specific literature and there is no consensus over this subject, however, participating centers have very large experience in the field of transcatheter heart valve treatment; on the other hand, this high expertise could mean that the clinical outcomes may not be generalisable to all the TAVR centers.
Conclusion
In selected patients with aortic bio-prosthesis degeneration, the acute occlusion of left main following a valve-in-valve procedure is a rare and ominous complication with very high mortality. This complication has been shown to be more frequent with specific types of bioprostheses. The systematic use of left main protection with a guiding catheter and intracoronary wire seems to be helpful to ensure an adequate level of safety and should be advocated in all cases in which the risk of acute left main occlusion is very high. Nonetheless, only a larger study, involving centers at a different level of expertise, may provide conclusive data concerning the long term clinical outcomes. These findings further support the use of bioprostheses at the time of surgical aortic valve replacement as even in highest risk settings a transcatheter approach can overcome the risk of left main occlusion.
Declarations of Interest
Acknowledgements
The authors agree to abide by the requirements of the Statement of publishing ethics of the International Cardiovascular Forum Journal19
References
1. Brown JM, O’Brien SM, Wu C, Sikora JA, Griffith BP, Gammie JS. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: changes in risks, valve types, and outcomes in the Society of Thoracic Surgeons National Database. J Thorac Cardiovasc Surg. 2009;137:82–90. doi: 10.1016/j.jtcvs.2008.08.015.
2. Maganti M, Rao V, Armstrong S, Feindel CM, Scully HE, David TE. Redo valvular surgery in elderly patients. Ann Thorac Surg. 2009;87:521–525. doi: 10.1016/j.athoracsur.2008.09.030
3. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria JE, Herrmann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–1607. doi: 10.1056/NEJMoa1103510.
4. Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Williams M, Dewey T, Kapadia S, Babaliaros V, Thourani VH, Corso P, Pichard AD, Bavaria JE, Herrmann HC, Akin JJ, Anderson WN, Wang D, Pocock SJ. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–2198. doi: 10.1056/NEJMoa1008232.
5. Webb JG, Wood DA, Ye J, Gurvitch R, Masson JB, Rodes-Cabau J, Osten M, Horlick E, Wendler O, Dumont E, Carere RG, Wijesinghe N, Nietlispach F, Johnson M, Thompson CR, Moss R, Leipsic J, Munt B, Lichtenstein SV, Cheung A. Transcatheter valve-in-valve implantation for failed bioprosthetic heart valves. Circulation. 2010;121:1848 –1857. doi: 10.1161/CIRCULATIONAHA.109.924613.
6. Bedogni F, Laudisa ML, Pizzocri S, Tamburino C, Ussia GP, Petronio AS, Napodano M, Ramondo A, Presbitero P, Ettori F, Santoro G, Klugman S, De Marco F, Brambilla N, Testa L. Transcatheter valve-in-valve implantation using Corevalve Revalving System for failed surgical aortic bioprostheses. JACC Cardiovasc Interv. 2011;4:1228-34. doi: 10.1016/j. jcin.2011.10.002.
7. Dvir D, Webb J, Brecker S, Bleiziffer S, Hildick-Smith D, Colombo A, Descoutures F, Hengstenberg C, Moat NE, Bekeredjian R, Napodano M, Testa L, Lefevre T, Guetta V, Nissen H, Hernández JM, Roy D, Teles RC, Segev A, Dumonteil N, Fiorina C, Gotzmann M, Tchetche D, Abdel-Wahab M, De Marco F, Baumbach A, Laborde JC, Kornowski R. Transcatheter aortic valve replacement for degenerative bioprosthetic surgical valves: results from the global valve-in-valve registry. Circulation. 2012;126:2335-44. doi: 10.1161/CIRCULATIONAHA.112.104505.
8. Chakravarty T, Jilaihawi H, Nakamura M, Kashif M, Kar S, Cheng W, Makkar R. Pre-emptive positioning of a coronary stent in the left anterior descending artery for left main protection: a prerequisite for transcatheter aortic valve-in-valve implantation for failing stentless bioprostheses?. Catheter Cardiovasc Interv. 2013;824:E630-6. doi: 10.1002/ccd.25037 9. Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed
MD, Gaasch WH, Lytle BW, Nishimura RA, O’Gara PT, O’Rourke RA, Otto CM, Shah PM, Shanewise JS. Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2008;118:e523–e661. doi: 10.1161/CIRCULATIONAHA.108.190748 10. Kappetein AP, Head SJ, Généreux P, Piazza N, van Mieghem NM,
Blackstone EH, Brott TG, Cohen DJ, Cutlip DE, van Es GA, Hahn RT, Kirtane AJ, Krucoff MW, Kodali S, Mack MJ, Mehran R, Rodés-Cabau J, Vranckx P, Webb JG, Windecker S, Serruys PW, Leon MB. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document. J Am Coll Cardiol. 2012;60:1438-54. doi: 10.1016/j. jacc.2012.09.001
11. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA, O’Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM 3rd, Thomas JD, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Creager MA, Curtis LH, DeMets D, Guyton RA, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Stevenson WG, Yancy CW; American College of Cardiology; American College of Cardiology/American Heart Association; American Heart Association. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.J Thorac Cardiovasc Surg. 2014 Jul;1481:e1-e132. doi: 10.1016/j.jtcvs.2014.05.014.
12. Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur Heart J 2003;24:1231– 1243.
13. Jaussaud N. Risk of reoperation for aortic bioprosthesis disfunction. J Heart Valve Dis 2009; 18:256-261.
14. Dvir D; Webb J; Bleiziffer S; Pasic M; Waksman R; Kodali S; Barbanti M; Latib A; Schaefer U; Rodés-Cabau J; Treede E; Piazza N; Hildick-Smith D; Himbert D; Walther T; Hengstenberg C; Nissen H; Bekeredjian R; Presbitero P; Ferrari E; Segev A; deWeger A; Windecker S; NE Moat; Napodano M; Wilbring M; Cerillo AG; Brecker S; Tchetche D; Lefèvre T; De Marco F; Fiorina C; Petronio AS; Teles RC; Testa L; Laborde JC; Leon MB; Kornowski R for the Valve-in-Valve International Data Registry Investigators JAMA. 2014;3122:162 doi:10.1001/jama.2014.7246. 15. Gurvitch R, Cheung A, Bedogni F, Webb JG. Coronary obstruction
following transcatheter aortic valve-in-valve implantation for failed surgical bioprostheses. Catheter Cardiovasc Interv. 2011;773:439-444. doi: 10.1002/ccd.22861
16. Khawaja MZ, Haworth P, Ghuran A, Lee L, de Belder A, Hutchinson N, Trivedi U, Laborde JC, Hildick-Smith D. Transcatheter aortic valve implantation for stenosed and regurgitant aortic valve bioprostheses CoreValve for failed bioprosthetic aortic valve replacements. J Am Coll Cardiol. 2010;55:97-101. doi: 10.1016/j.jacc.2009.06.060.
17. Testa L, Latib A, De Marco F, De Carlo M, Agnifili M, Latini RA, Petronio AS, Ettori F, Poli A, De Servi S, Ramondo A, Napodano M, Klugmann S, Ussia GP, Tamburino C, Brambilla N, Colombo A, Bedogni F. Clinical Impact of Persistent Left Bundle Branch Block afterTranscatheter Aortic Valve Implantation with CoreValve Revalving System. Circulation. 2013, 12712:1300-7. doi: 10.1161/CIRCULATIONAHA.112.001099
18. Onorati F, Biancari F, De Feo M, Mariscalco G, Messina A, Santarpino G, Santini F, Beghi C, Nappi G, Troise G, Fischlein T, Passerone G, Heikkinen J, Faggian G. Mid-term results of aortic valve surgery in redo scenarios in the current practice: results from the multicentre European RECORD (REdo Cardiac Operation Research Database) initiative. Eur J Cardiothorac Surg. 2014 Mar 30. [Epub ahead of print]. doi: 10.1093/ejcts/ ezu116.
19. Shewan LG, Coats AJS, Henein M. Requirements for ethical publishing in biomedical journals. International Cardiovascular Forum Journal 2015;2:2 DOI: 10.17987/icfj.v2i1.4
Acronym List
SAVR: surgical aortic valve replacement TAVR: trasncatheter aortic valve replacement VIV: valve in valve
LM: left main
STS: Society of thoracic surgeon ES: Edwards Sapien/Sapien XT
TEE: transesophageal echocardiography NYHA: New York Heart association CT: computed tomography ASA: acetil salycilic acid